
Update on Colorectal Cancer - sialliance.health.nz · Update on Colorectal Cancer Dr Christopher...
51
Update on Colorectal Cancer Dr Christopher Jackson Medical Oncologist Southern Blood and Cancer Service
Transcript of Update on Colorectal Cancer - sialliance.health.nz · Update on Colorectal Cancer Dr Christopher...
Update on Colorectal Cancer
Dr Christopher Jackson
Medical Oncologist
Southern Blood and Cancer Service
CRC Update – September 2010
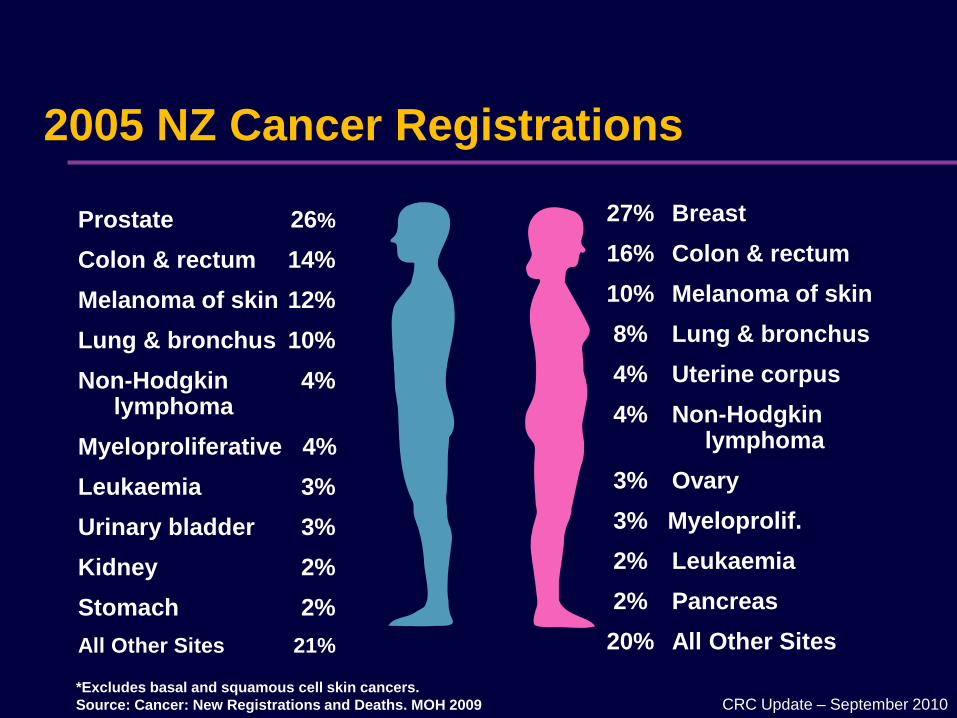
2005 NZ Cancer Registrations
*Excludes basal and squamous cell skin cancers.
Source: Cancer: New Registrations and Deaths. MOH 2009
27% Breast
16% Colon & rectum
10% Melanoma of skin
8% Lung & bronchus
4% Uterine corpus
4% Non-Hodgkinlymphoma
3% Ovary
3% Myeloprolif.
2% Leukaemia
2% Pancreas
20% All Other Sites
Prostate 26%
Colon & rectum 14%
Melanoma of skin 12%
Lung & bronchus 10%
Non-Hodgkin 4% lymphoma
Myeloproliferative 4%
Leukaemia 3%
Urinary bladder 3%
Kidney 2%
Stomach 2%
All Other Sites 21%

Age standardised incidence of Colorectal Cancer
NZ, UK and Aus 2004/5
0
100
200
300
400
500
600
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85+
Age category
Incid
en
ce p
er
100,0
00 p
op
ula
tio
n
NZ total UK total Aus total
NZHIS 2005; Aus Institute of Health and Welfare; Cancer Research UK

0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
40.0
1961
1963
1965
1967
1969
1971
1973
1975
1977
1979
1981
1983
1985
1987
1989
1991
1993
1995
1997
1999
2001
2003
2005
Year
Mo
rta
lity
pe
r 1
00
,00
0
Age standardised death rates, NZ 1961-2005
Lung
Colorectal
Breast
Prostate
Melanoma
Cervix
NZ HIS 2005

CRC Update – September 2010
Disease-specific funding
Colorectal Cancer
5-FU / Capecitabine
Oxaliplatin
Irinotecan
Breast Cancer
FEC / FAC + G-CSF
Docetaxel / Paclitaxel
Tam / AIs
Herceptin adjuvant / advanced
Vinorelbine
Capecitabine
Cetuximab
Bevacizumab
Panitumumab
SIR Spheres
Raltitrexed Gemcitabine

CRC Update – September 2010
Risk factors
Personal / Family history
Ulcerative colitis
Hyperinsulinism: RR 1.30
Alcohol: > 2pints/d, 4 glasses wine / d: RR 1.41
Obesity: RR 1.5 if BMI > 25
Vitamin B6 inversely related to colon cancer risk: RR 0.51
– Unclear whether supplementation or diet important
Exercise: RR 0.33-0.60
Diet – Western Diet
Red meat > 300g / week
Vitamin D, Calcium controversial
Association does not prove causation

CRC Update – September 2010
All cancers come from polyps
CRC Update – September 2010
Common symptoms
Change in bowel habit – loose stool
Rectal bleeding
Narrow stool
Abdominal pain
Bloating
Anaemia
Constitutional symptoms are LATE signs
Pain is uncommon
80% of rectal bleeding will be benign

CRC Update – September 2010
Good staging critical
Colonoscopy
Biopsy
CT
MRI
PET
CRC Update – September 2010
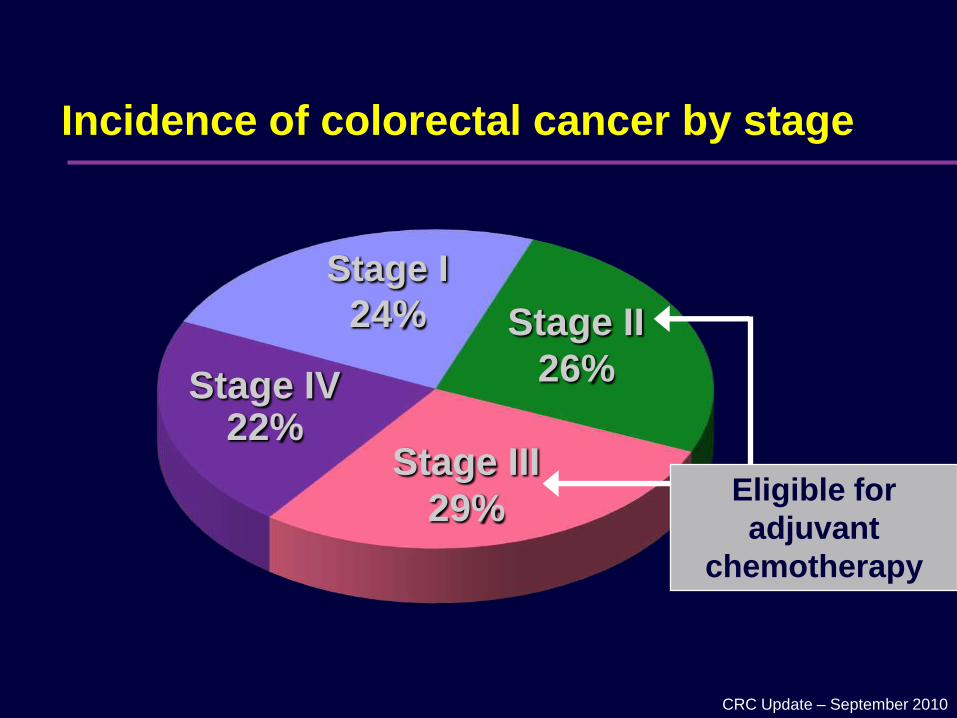
Incidence of colorectal cancer by stage
Stage I
24% Stage II
26%
Stage III
29%
Stage IV22%
Eligible for
adjuvant
chemotherapy
CRC Update – September 2010
Types of surgery

CRC Update – September 2010
Adjuvant Chemotherapy
Stage IIIStage IIStage I
Worsening Survival
No Adjuvant
TherapyAdjuvant TherapyPossible Adjuvant Therapy
Traditional view of relapse risk & adjuvant therapy
CRC Update – September 2010
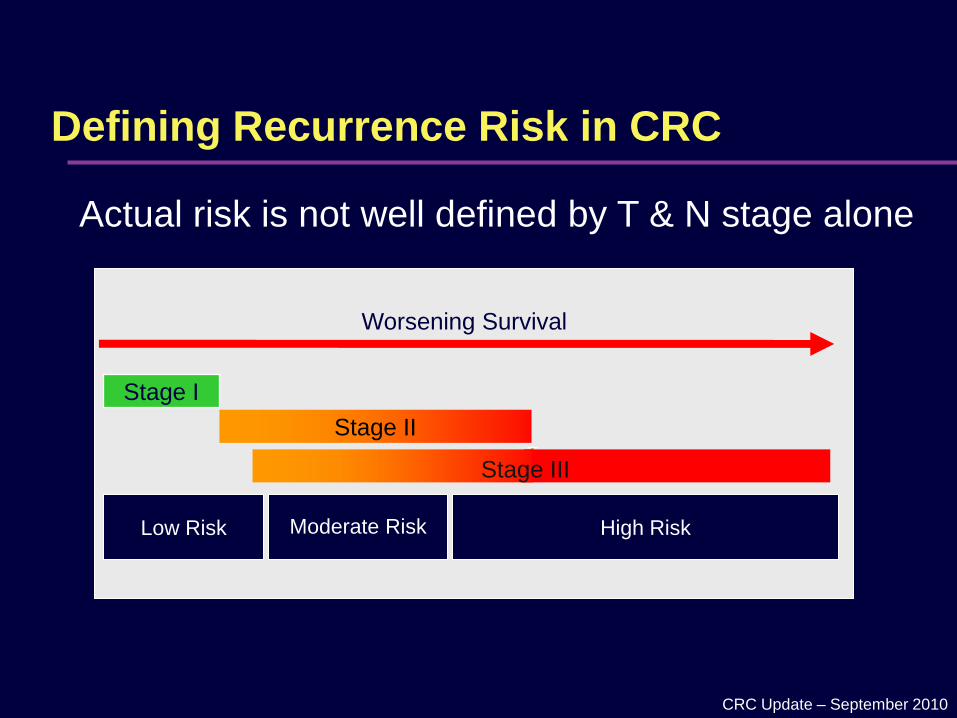
Stage I
Worsening Survival
Low Risk High RiskModerate Risk
Stage III
Defining Recurrence Risk in CRC
Actual risk is not well defined by T & N stage alone
Stage II
Stage III
CRC Update – September 2010
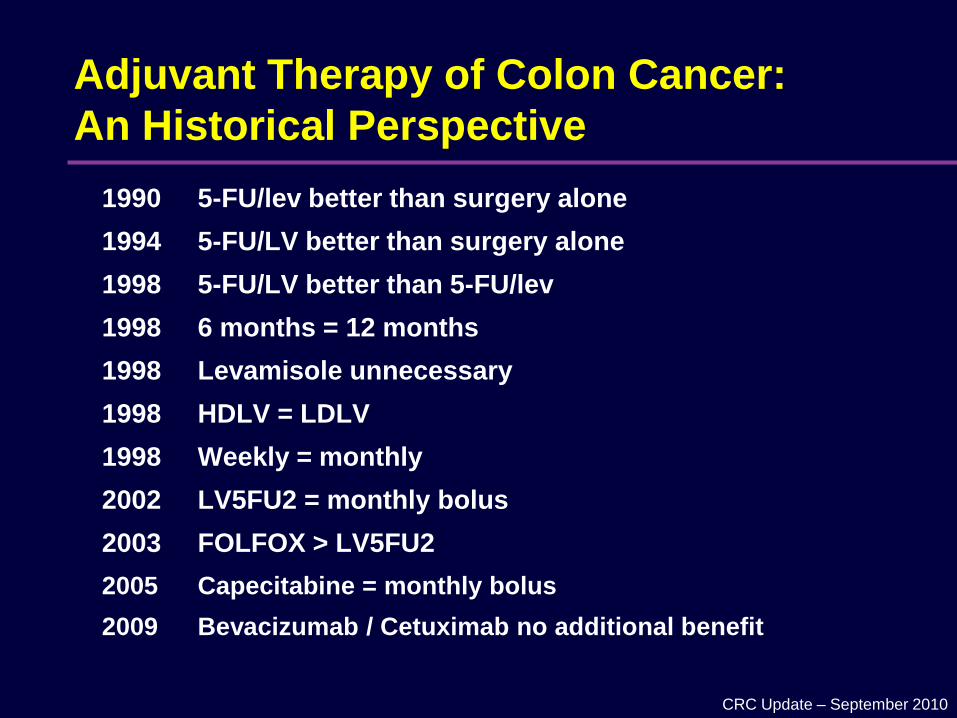
Adjuvant Therapy of Colon Cancer:
An Historical Perspective
1990 5-FU/lev better than surgery alone
1994 5-FU/LV better than surgery alone
1998 5-FU/LV better than 5-FU/lev
1998 6 months = 12 months
1998 Levamisole unnecessary
1998 HDLV = LDLV
1998 Weekly = monthly
2002 LV5FU2 = monthly bolus
2003 FOLFOX > LV5FU2
2005 Capecitabine = monthly bolus
2009 Bevacizumab / Cetuximab no additional benefit
CRC Update – September 2010
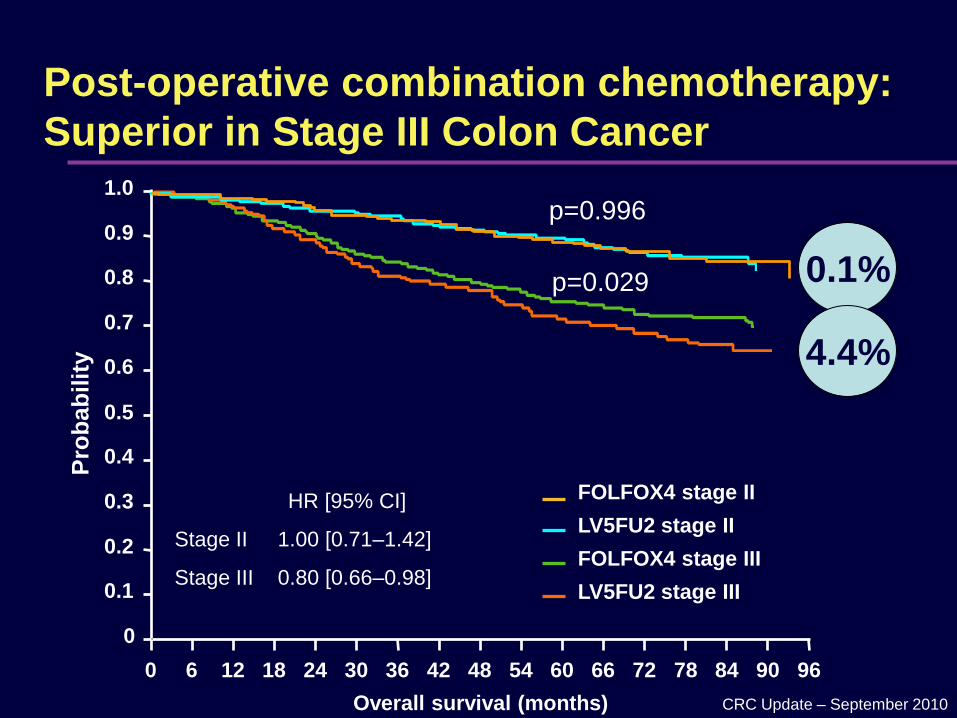
Post-operative combination chemotherapy:
Superior in Stage III Colon Cancer
FOLFOX4 stage II
LV5FU2 stage II
FOLFOX4 stage III
LV5FU2 stage III
Overall survival (months)
Pro
bab
ilit
y
1.0
0.8
0.6
0.4
0.2
0
0.9
0.7
0.5
0.3
0.1
0 6 12 18 24 6030 36 42 48 54 66 9672 78 84 90
HR [95% CI]
Stage II 1.00 [0.71–1.42]
Stage III 0.80 [0.66–0.98]
0.1%
4.4%
p=0.996
p=0.029

CRC Update – September 2010
Relative toxicities of differing regimens
%Bolus 5-
FUInfused 5-FU Bolus 5-FU Capecitabine
Diarrhoea 9 4 11 13
Stomatitis 7 2 14 2
Nausea/Vomiting 3 1 3 3
PPE 0 0 <1 17
Neutropenia 16 7 26 2
CRC Update – September 2010
Management of toxicity
Early recognition!!!
– Importance of specialist nursing
Interruption of treatment
Delay
Dose reduction
Loperamide, Codeine, Octreotide, Steroids??
Anti-biotics
Pyridoxine
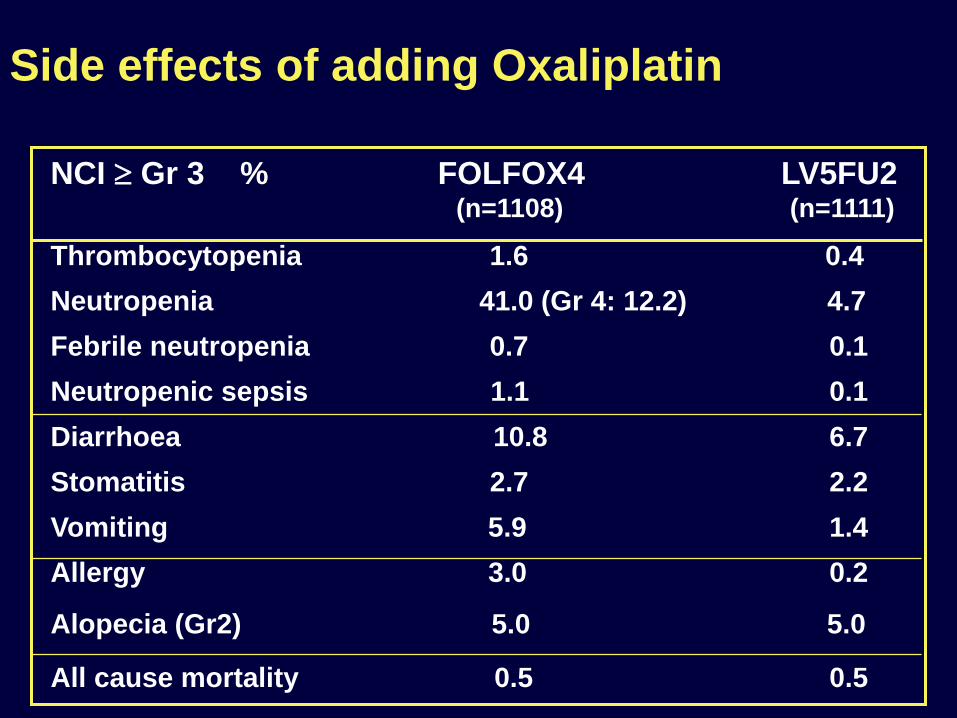
Side effects of adding Oxaliplatin
NCI Gr 3 % FOLFOX4 LV5FU2(n=1108) (n=1111)
Thrombocytopenia 1.6 0.4
Neutropenia 41.0 (Gr 4: 12.2) 4.7
Febrile neutropenia 0.7 0.1
Neutropenic sepsis 1.1 0.1
Diarrhoea 10.8 6.7
Stomatitis 2.7 2.2
Vomiting 5.9 1.4
Allergy 3.0 0.2
Alopecia (Gr2) 5.0 5.0
All cause mortality 0.5 0.5

CRC Update – September 2010
Long-term Neuropathy
0
10
20
30
40
50
60
During
Tx
6
months
1-year 2-year 3-year 4-year
Grade 1
Grade 2
Grade 3
Evaluable patients n=811
Grade 0 84.3%
Grade 1 12.0%
Grade 2 2.8%
Grade 3 0.7%

CRC Update – September 2010
Adjuvant chemotherapy in the elderly
CRC Update – September 2010
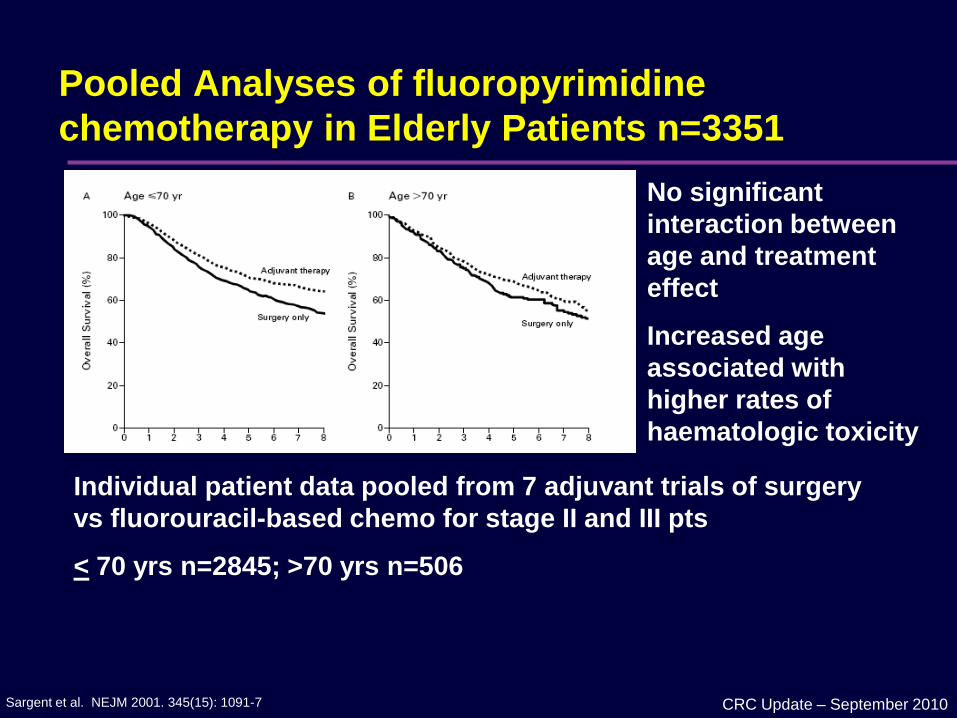
Pooled Analyses of fluoropyrimidine
chemotherapy in Elderly Patients n=3351
Sargent et al. NEJM 2001. 345(15): 1091-7
Individual patient data pooled from 7 adjuvant trials of surgery
vs fluorouracil-based chemo for stage II and III pts
< 70 yrs n=2845; >70 yrs n=506
No significant
interaction between
age and treatment
effect
Increased age
associated with
higher rates of
haematologic toxicity

CRC Update – September 2010
Adjuvant chemo in elderly
André T et al. JCO 2009;27:3109-3116; QUASAR Collab Group Lancet 2007; 370:2020-29
CRC Update – September 2010
Rectal cancer: pre-operative therapy
CRC Update – September 2010
Pre-operative therapy
Advanced disease
CRC Update – September 2010
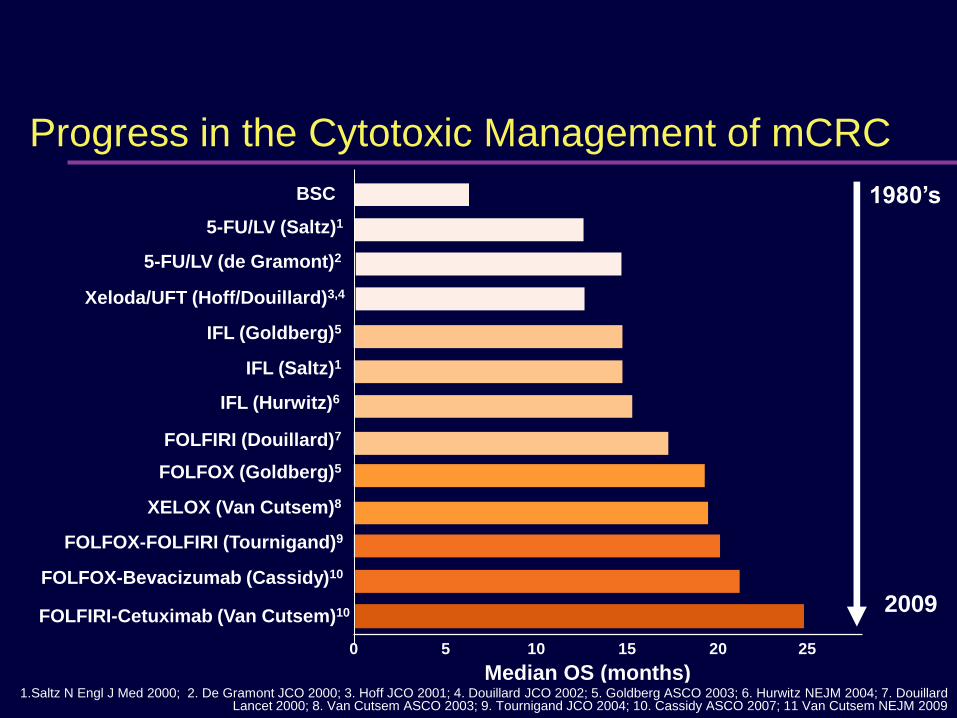
Progress in the Cytotoxic Management of mCRC
FOLFOX-FOLFIRI (Tournigand)9
5-FU/LV (Saltz)1
Xeloda/UFT (Hoff/Douillard)3,4
5-FU/LV (de Gramont)2
IFL (Goldberg)5
IFL (Saltz)1
FOLFIRI (Douillard)7
FOLFOX (Goldberg)5
XELOX (Van Cutsem)8
0 252015105
IFL (Hurwitz)6
Median OS (months)
BSC 1980’s
2009
1.Saltz N Engl J Med 2000; 2. De Gramont JCO 2000; 3. Hoff JCO 2001; 4. Douillard JCO 2002; 5. Goldberg ASCO 2003; 6. Hurwitz NEJM 2004; 7. Douillard Lancet 2000; 8. Van Cutsem ASCO 2003; 9. Tournigand JCO 2004; 10. Cassidy ASCO 2007; 11 Van Cutsem NEJM 2009
FOLFIRI-Cetuximab (Van Cutsem)10
FOLFOX-Bevacizumab (Cassidy)10
CRC Update – September 2010
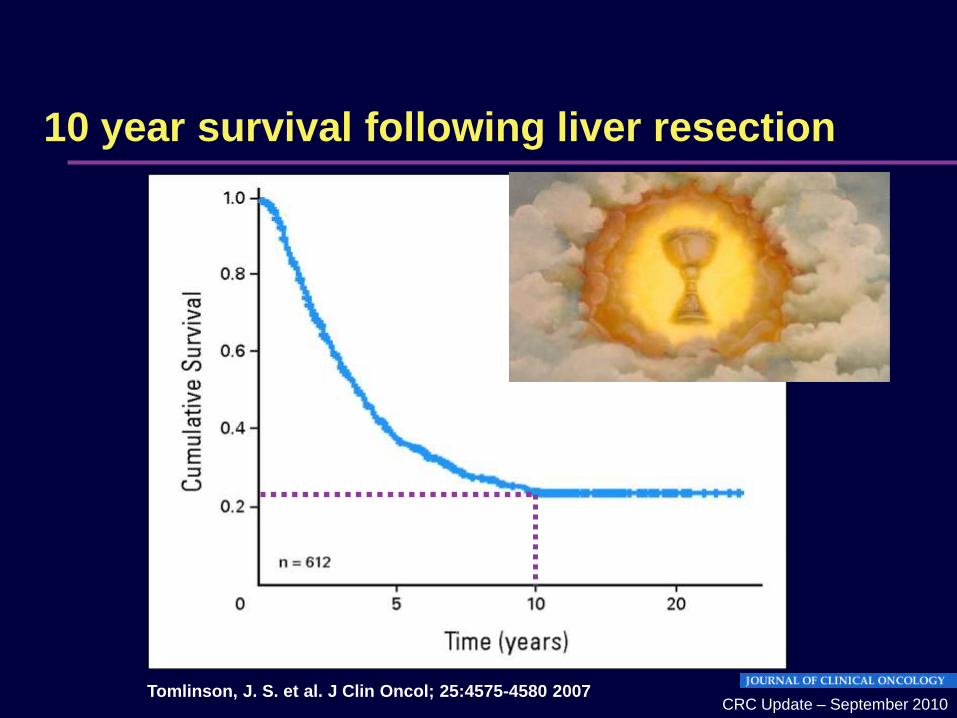
10 year survival following liver resection
Tomlinson, J. S. et al. J Clin Oncol; 25:4575-4580 2007

CRC Update – September 2010
OPTIMOX 1 Neurotoxicity FOLFOX4 vs 7
0
2
4
6
8
10
12
14
16
18
1 3 5 7 9
11
13
15
17
19
21
23
cycles
% o
f patients
FOLFOX4
FOLFOX7

CRC Update – September 2010
Anti-VEGF
Reduces
interstitial fluid pressure
vessel density
Increases
drug delivery
Anti-VEGF antibody ‘normalises’ the tumour
vasculature
Jain R. Nature Med 2001;7:987–9; Willett CG, et al. Nat Med 2004;10:145–7;
Tong R, et al, Cancer Res 2004;64:3731–6
CRC Update – September 2010
Bevacizumab-Related Toxicities
• Hypertension (about 10%)
• Venous Thromboembolism
• Arterial Thromboembolism (increased risk 2->4.5%)
• Bleeding
• Proteinuria
• Delayed Wound Healing
• GI Perforation (about 2%)
1Hurwitz H, et al. N Engl J Med 2004;350:2235–42 2Novotny W, et al. J Clin Oncol 2004;22 (July 15 Suppl.): Abstract 3529 3Hambleton J, et al. J Clin Oncol 2004;22 (July 15 Suppl.): Abstract 3582
4Scappaticci et al J Surg Oncol. 2005 Sep 1;91(3):173-80.
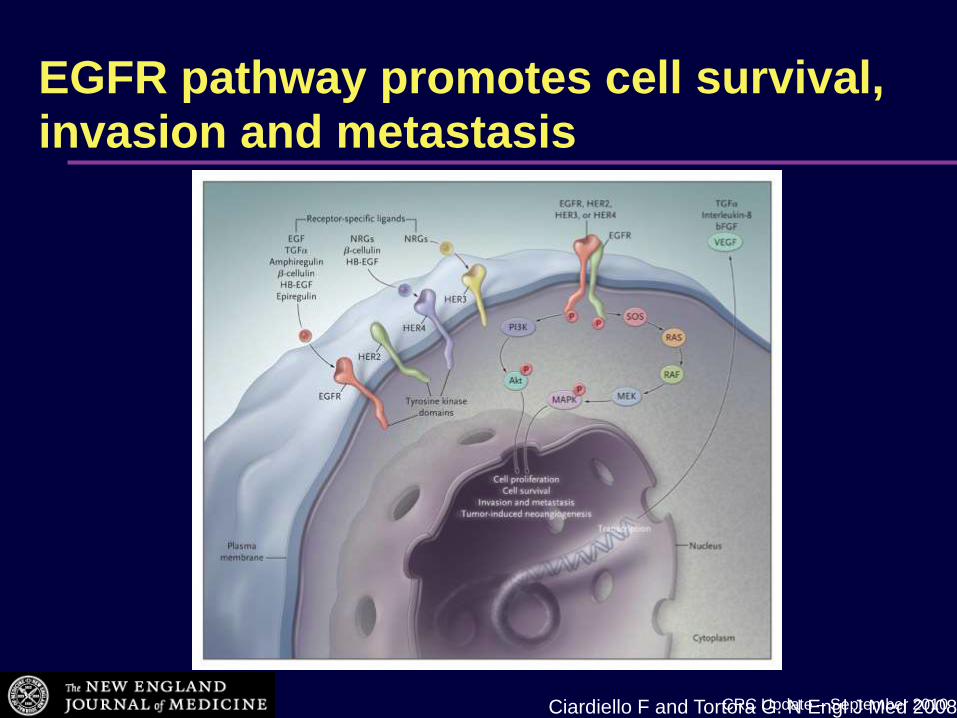
CRC Update – September 2010Ciardiello F and Tortora G. N Engl J Med 2008
EGFR pathway promotes cell survival, invasion and metastasis

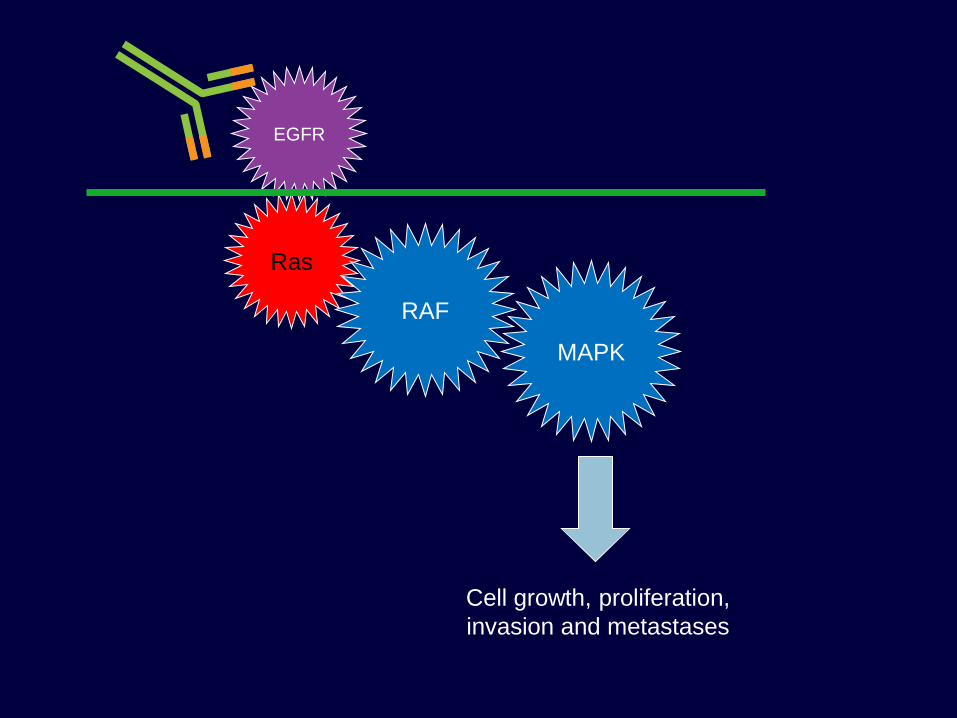
Ras
RAF
MAPK
EGFR
Cell growth, proliferation,
invasion and metastases

Ras
RAF
MAPK
EGFR
Cell growth, proliferation,
invasion and metastases
Ras
RAF
MAPK
EGFR
Cell growth, proliferation,
invasion and metastases
CRC Update – September 2010
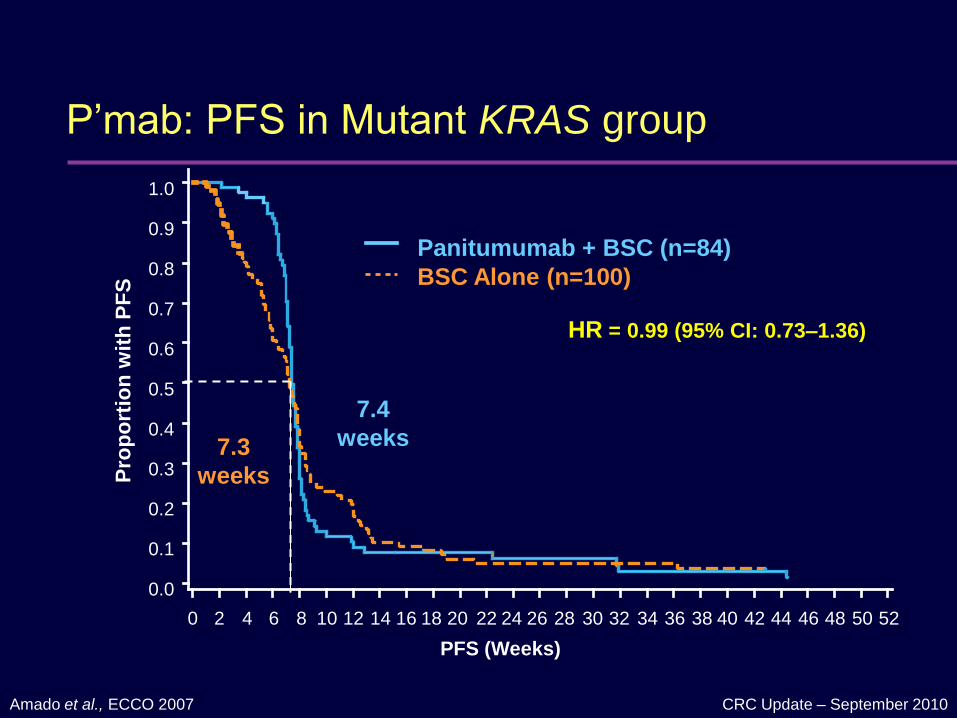
P’mab: PFS in Mutant KRAS group
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pro
po
rtio
n w
ith
PF
S
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
PFS (Weeks)
36 38 40 42 44 46 48 50 52
Panitumumab + BSC (n=84)
BSC Alone (n=100)
HR = 0.99 (95% CI: 0.73–1.36)
Amado et al., ECCO 2007
7.4
weeks7.3
weeks

CRC Update – September 2010
P’mab: PFS in WT KRAS group
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
PFS (Weeks)
36 38 40 42 44 46 48 50 52
Panitumumab + BSC (n=124)
BSC Alone (n=119)
HR = 0.45 (95% CI: 0.34–0.59)
Stratified log-rank test, p < 0.0001
Pro
po
rtio
n w
ith
PF
S
Amado et al., ECCO 2007
7.3
weeks
12.3 weeks

EGFR inhibitor-induced skin reactions
1 2 3 4 5 6 7 8 9
Post-inflammatory effectsAcne-like rash
Paronychia
Dry skin
Pruritus
Fissura
Hydrocolloid
dressing
or
Propylene
glycol +/-
salicylic acid
Anti-septic
soaks
Silver nitrate
(pyogenic
granuloma)
THERAPY SUGGESTIONS
Topical anti-acne
creams (drying
effect)
+/- tetracyclines
+/- antihistamines
Emollients
Pictures provided by S Segaert and E Van Cutsem (Leuven, Belgium).
CRC Update – September 2010
NICE appraisal – Cost per QALY
Bevacizumab: £88,364
– Additional median survival 6 weeks; 10% addit response
Cetuximab: £58,870
– Additional 10 weeks progression-free survival in chemo-refractory group
NICE threshold: £30,000
CRC Update – September 2010
Managing toxicity: CTCAE grading
G1: Mild
G2: Moderate
G3: IV, or hospitalisation (25% DR)
G4: Life threatening (50% DR or stop)
G5: RIP
A question of how soon, how severe,
and the treatment context

Primary and secondary prevention

CRC Update – September 2010
Colorectal cancer – screening
4 trials examining FOBT effect on CRC mortality
Biennial testing; FOBT Colonoscopy
Age range 45-70
Cochrane meta-analysis:

CRC Update – September 2010
Lifestyle advice – diet
JAMA 2007: Meyerhardt
1009 patients
Dietary patterns and relapse rates
Effect as strong as adjuvant chemotherapy; cumulative not exclusive
US PPP trial as supportive evidence
– Dietary intervention independent of obesity, T2DM
CRC Update – September 2010
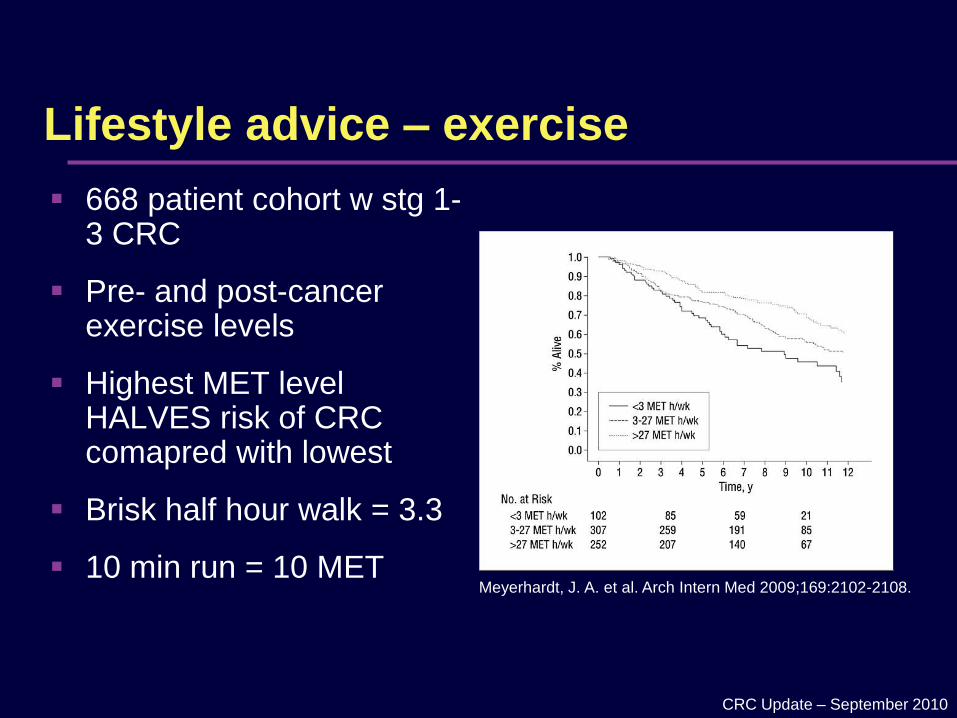
Lifestyle advice – exercise
668 patient cohort w stg 1-3 CRC
Pre- and post-cancer exercise levels
Highest MET level HALVES risk of CRC comapred with lowest
Brisk half hour walk = 3.3
10 min run = 10 MET Meyerhardt, J. A. et al. Arch Intern Med 2009;169:2102-2108.

CRC Update – September 2010
Lifestyle advice – general
Hyperinsulinism: RR 1.30
Obesity: RR 1.5 if BMI > 25
– Lose weight
Alcohol: > 2pints/d, 4 glasses wine / d: RR 1.41
– Drink less
Vitamin B6 inversely related to colon cancer risk: RR 0.51
– Vitamin supplements? (or healthy diet)
Cases
CRC Update – September 2010
Case 1 – SM
34 yo f. Noted rectal bleeding, attributed to haemorrhoids. On rectal
examination there was a palpable mass at 5cm. She has no significant
comorbidities and takes no medications, and has no family history of cancers.
CT scan shows bone and liver mets
Biopsy confirms adenocarcinoma
? Radiotherapy
? Surgery
? Chemo
CRC Update – September 2010
Case 2 – CW
62 year old female
Emergency presentation
pT4a N0 (0/22) V1 G2 adenocarcinoma sigmoid
CEA = 9, CT scan clear
? Other staging investigations
? Benefit of chemo
? Colonoscopy
Summary
CRC Update – September 2010
Summary
CRC 2nd most common, incidence and deaths
Early detection saves lives
Change in bowel habit needs investigation
Good staging critical
Adjuvant therapy in stage 2 & 3 benefit of 4-20%
Treatment of stage four quadruples survival time
Toxicity management requires early recognition
Aggressive multi-modal therapy in selected patients with stage 4 disease can result in cure
Several lifestyle and prevention options available
We can do better!

NZ Summary – How do we stack up?
Ease of access to colonoscopy
Screening
Rapid specialist access ? / Access to adjuvant therapy
Full access to advanced drug therapy /
Comprehensive bowel cancer programme /

Colorectal Cancer.
New Zealand’s Cancer.













![SERIOUS SKIN INFECTIONS - sialliance.health.nz · frequently implicated organisms are Staphylococcus aureus and Streptococcus pyogenes [166]. Skin infections are more likely to develop](https://static.fdocuments.net/doc/165x107/5e56d81254256d30696d75aa/serious-skin-infections-frequently-implicated-organisms-are-staphylococcus-aureus.jpg)


