Unusual Patterns of Solitary Sacral Plasmacytoma - AJNR · Unusual Patterns of Solitary Sacral...
2
566 Unusual Patterns of Solitary Sacral Plasmacytoma Charles F. Lanzieri ,1.2 Michael Sacher,l Paul Solodnik,l George Hermann,l Burton A. Cohen,l and Jack G. Rabinowitz1 Solitary plasmacytomas are usually lytic and expansile and presen t in the ilium or long bones because of local pain or swelling [1]. Peripheral neuropathy can occur, probably sec- ondary to a neurotoxic substance secreted by the neoplastic plasma cells [2]. Solitary sclerotic plasmacytomas are quite unusual and unreported in the sacrum . This report describes two cases of solitary nonmass-pro- ducing plasmacytomas in the sacrum-one lucent and one sclerotic-that presented with neurological findings in the distribution of the sacral and lumbar nerves. Case Reports Case 1 A 50-year-old man with a 3-month history of progressive weakness and paresthesis in all four quadrants was referred for radiologic evaluation . On physical examination, marked weakness and de- creased pain and vibratory sen sation were present in all extremities. Laboratory studies were within normal limits, including the serum protein electrophoresis , and there was no evidence of Bence Jones proteinuria. Electromyographic studies showed diffuse nonspecific sensory and motor neuropathy. A complete myelogram showed no abnor- B Fig. 1.-Serial sections through sacrum taken at approximately Sl (A), S2 (B), and S3 (e) after IV contrast injection. A destructive sacral mass with loss of cortex is seen anteriorty. Perineural fat surrounding sacral nerve roots is apparently not violated and nerve roots themselves are Recei ved March 20, 1985; accepted after revision June 20,1985 . malities. CT of the lumbar spine and sacrum (Fig . 1) showed a destructive disease within the sacrum but with little if any mass effect upon the sacral nerve root s. The skeletal survey failed to show other destructive lesions. Biopsy of the sacrum revealed plasmacytoma. Case 2 A 40-year-old man presented with an 18-month history of back pain and more recent onset of occasional sphincter incontinence. The physical examination was remarkable for slight weakness and de- creased reflexes in the lower extremities. Sphincter tone was normal. The laboratory studies were unremarkable, including serum protein electrophoresis; there was no evidence of Bence Jones proteinuria. The electromyographic studies showed sensory and motor neurop- athy in the lower extremities. The complete myelogram was normal. CT was performed to evaluate the greater sciatic foramina and revealed a non mass-producing sclerotic process within the sacrum (Fig . 2) . The skeletal survey failed to show other lesions. The sacral biopsy was compatible with plasmacytoma. Discussion The classical radiographic description of multiple myeloma emphasizes multiple "punched-out" areas of bone destruc- c identifiable at several levels. Severe neurological findings referable to the sacral and other nerves were produced despite this apparent lack of physical pressure or mass effect. 1 Departmen t of Radiology, Mount Sinai Hospital and School of Medicine of the City University of New York , New York, NY 10029. 2 Present address: Department of Radiology, Th e Cleveland Clinic Foundation, 9500 Euclid Ave., Cleveland, OH 44106. Address reprint requests to C. F. Lanzieri. AJNR 8:566-567, May/June 1987 0195-6108/87/0803-0566 © American Society of Neuroradiology
-
Upload
phamnguyet -
Category
Documents
-
view
218 -
download
0
Transcript of Unusual Patterns of Solitary Sacral Plasmacytoma - AJNR · Unusual Patterns of Solitary Sacral...
566
Unusual Patterns of Solitary Sacral Plasmacytoma Charles F. Lanzieri ,1.2 Michael Sacher,l Paul Solodnik,l George Hermann,l Burton A. Cohen,l and Jack G. Rabinowitz1
Solitary plasmacytomas are usually lytic and expansile and present in the ilium or long bones because of local pain or swelling [1]. Peripheral neuropathy can occur, probably secondary to a neurotoxic substance secreted by the neoplastic plasma cells [2]. Solitary sclerotic plasmacytomas are quite unusual and unreported in the sacrum.
This report describes two cases of solitary nonmass-producing plasmacytomas in the sacrum-one lucent and one sclerotic-that presented with neurological findings in the distribution of the sacral and lumbar nerves.
Case Reports
Case 1
A 50-year-old man with a 3-month history of progressive weakness and paresthesis in all four quadrants was referred for radiologic evaluation. On physical examination, marked weakness and decreased pain and vibratory sensation were present in all extremities. Laboratory studies were within normal limits, including the serum protein electrophoresis , and there was no evidence of Bence Jones proteinuria.
Electromyographic studies showed diffuse nonspecific sensory and motor neuropathy. A complete myelogram showed no abnor-
B
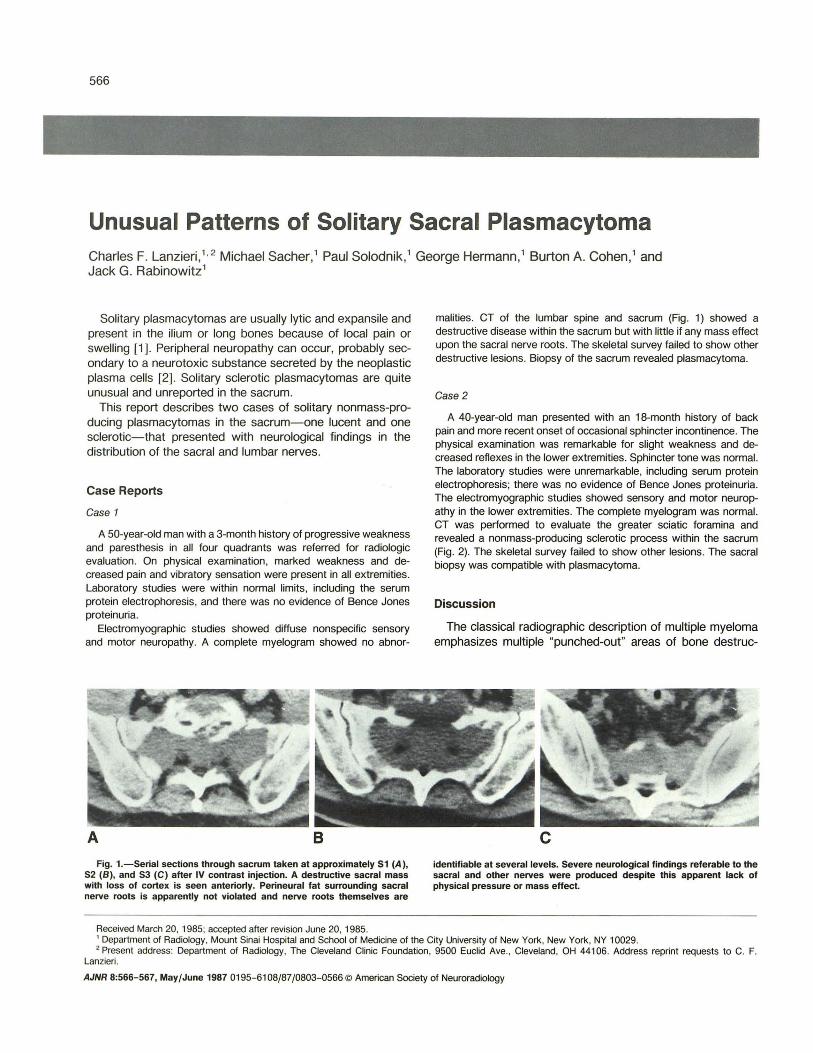
Fig. 1.-Serial sections through sacrum taken at approximately Sl (A), S2 (B), and S3 (e) after IV contrast injection. A destructive sacral mass with loss of cortex is seen anteriorty. Perineural fat surrounding sacral nerve roots is apparently not violated and nerve roots themselves are
Received March 20, 1985; accepted after revision June 20,1985.
malities. CT of the lumbar spine and sacrum (Fig . 1) showed a destructive disease within the sacrum but with little if any mass effect upon the sacral nerve roots. The skeletal survey failed to show other destructive lesions. Biopsy of the sacrum revealed plasmacytoma.
Case 2
A 40-year-old man presented with an 18-month history of back pain and more recent onset of occasional sphincter incontinence. The physical examination was remarkable for slight weakness and decreased reflexes in the lower extremities. Sphincter tone was normal. The laboratory studies were unremarkable, including serum protein electrophoresis; there was no evidence of Bence Jones proteinuria. The electromyographic studies showed sensory and motor neuropathy in the lower extremities. The complete myelogram was normal. CT was performed to evaluate the greater sciatic foramina and revealed a non mass-producing sclerotic process within the sacrum (Fig. 2). The skeletal survey failed to show other lesions. The sacral biopsy was compatible with plasmacytoma.
Discussion
The classical radiographic description of multiple myeloma emphasizes multiple "punched-out" areas of bone destruc-
c identifiable at several levels. Severe neurological findings referable to the sacral and other nerves were produced despite this apparent lack of physical pressure or mass effect.
1 Department of Radiology, Mount Sinai Hospital and School of Medicine of the City University of New York , New York, NY 10029. 2 Present address: Department of Radiology, The Cleveland Clinic Foundation, 9500 Euclid Ave., Cleveland, OH 44106. Address reprint requests to C. F.
Lanzieri.
AJNR 8:566-567, May/June 1987 0195- 6108/87/0803-0566 © American Society of Neuroradiology

AJNR :8, May/June 1987 SOLITARY SACRAL PLASMACYTOMA 567
Fig. 2.-Axial CT image through body of sacrum shows sclerotic, nonexpansile replacement of sacrum by infiltrating plasmacytoma. Sacral canal and neural foramina are not encroached upon.
tion, lytic expansile lesions, or generalized osteoporosis. The disease usually presents between the ages of 45 and 70 years with a peak in the sixth decade. Abnormal serum electrophoresis, Bence Jones proteinuria, and diffuse bone marrow infiltration complete the diagnostic findings [1, 3, 4].
Solitary nonsclerotic plasmacytomas may present as one of two recognized radiographic forms. The first is described as a cystic expansile bony tumor with a narrow zone of transition. It may exhibit internal trabeculations and can be mistaken for a giant cell tumor. The other radiographic type is purely destructive with an appearance similar to an osteolytic metastasis. It also has a narrow zone of transition and often exhibits expanding or "blow-out" features [5-7].
Solitary sclerotic plasmacytomas are rare , constituting less than 3% of all plasmacytomas in most series [2 , 6]. This type tends to be nonexpansile with a narrow zone of transition. An association between sclerotic plasmacytomas and peripheral neuropathy has been repeatedly noted [2, 5-8]. A rib, a vertebral body, the sternum, or the iliac bone are the most frequently involved structures.
Sacral involvement by solitary plasmacytoma of any type is unusual. In one large series of 61 solitary tumors the sacrum was involved in a single case [6]. Other recent series include no examples of solitary sacral lesions [9, 10]. Most often the ilium, long bones, and vertebral bodies are affected. The diagnosis of a solitary plasmacytoma depends on the presence of a normal skeletal survey, bone marrow aspiration , serum protein electrophoresis, and absence of Bence Jones proteinuria [3] .
The association of peripheral neuropathy and SOlitary plas-
macytoma, especially in the sclerotic type, is an interesting one. The peripheral neuropathy associated with multiple myeloma is well documented [1 1] and occurs in about 3% of patients. However, it occurs in about 50% of patients with solitary plasmacytomas [2] . The peripheral neuropathy associated with plasmacytomas tends to be uniform in type with motor weakness more prominently manifested than sensory loss [2]. It usually begins distally and spreads proximally in a symmetrical pattern . In the cases in which nerve biopsy has been performed, demyelination was seen [2] . It has been suggested that the neoplastic plasma cells secrete a substance toxic to peripheral nerves. In vitro studies have demonstrated an antimyelin antibody in the monoclonal protein fraction of patients with monoclonal protein and peripheral neuropathy [12] .
It is well known that disease in the sacrum or its related spaces may produce symptoms related to the sacral or sciatic nerves because of mass effect, and that CT is essential in evaluation of the sacrum [13] . The present cases emphasize these points. In the first case, sacral and peripheral neuropathy were found in the presence of minimal demonstrable compression of the sacral roots . Similar symptoms were found in the second case. It is tempting to postulate that a localized form of peripheral neuropathy may be present. To our knowledge, isolated sclerotic myeloma of the sacrum has not been previously reported .
REFERENCES
1. Dahlin DC. Bone tumors, 2nd ed. Springfield, III : Thomas, 1967 2. Kelly JJ, Kyle RA, Miles JM, Dyala PJ. Osteosclerotic myeloma and
peripheral neuropathy. Neurology 1983;133 : 202- 21 0 3. Himmelfarb E, Sebes J, Rabinowitz J. Unusual roentgenographic presen
tations of multiple myeloma. J Bone Joint Surg 1974;56(9) : 1723- 1728 4. Rodriguez AR , Lutcher CL, Coleman FW. Osteosclerotic myeloma. JAMA
1976;236(16): 1872-1874 5. Hermann G, Sherry H, Rabinowitz J. Solitary plasmacytoma associated
with peripheral neuropathy. Skel Radio/1981 ;6 :217-219 6. Gootnick LT. Solitary myeloma: review of sixty-one cases. Radiology
1945;45 :385-391 7. Read D, Warlow C. Peripheral neuropathy and solitary plasmacytoma. J
Neurol Neurosurg Psychiatry 1978;41 : 177 -184 8. Takasuki K, Uchiyama T, Sagawa K, Yodoi J. Plasma cell dyscrasia with
polyneuropathy and endocrine disorder. Topics in hematology. Proceedings of the 16th International Congress of Hematology. Tokyo, September 1976
9. Tony D, Griffith TW, Laramore GE, et al. Solitary plasmacytoma of bone and soft tissues. Radiology 1980;135 : 195-198
10. Whelan MA, Hilal SK, Gold RP, Luken MG, Michelson WJ. Computed tomography of the sacrum: 2. pathology. AJNR 1982 ;3 :555-559
11 . Silverstein A, Doniger D. Neurologic complications of myelomatosis. Arch Neuro/1 963 ;9 :534-544
12. Latov N, Sherman WH , Nemni R. Plasma-cell dyscrasia and peripheral neuropathy with a monoclonal antibody to peripheral nerve myelin . N Engl J Med 1980;303 :61 8-623
13. Lanzieri CF, Hilal SK. Computed tomography of the sacral plexus and sciatic nerve in the greater sciatic foramen. AJNR 1984;5:315- 318, AJR 1984;143: 165-168



![Research Article Prognostic Significance of Serum Free Light … · 2019. 7. 31. · the progression of MGUS [ ], solitary plasmacytoma [ ], and smoldering myeloma [ ]intomultiplemyeloma.](https://static.fdocuments.net/doc/165x107/60b139df8dfefb1baa01f551/research-article-prognostic-significance-of-serum-free-light-2019-7-31-the.jpg)