Untreated preoperative depression is not associated with postoperative arrhythmias in CABG patients;...
7
REPORTS OF ORIGINAL INVESTIGATIONS Untreated preoperative depression is not associated with postoperative arrhythmias in CABG patients La de ´pression pre ´ope ´ratoire non traite ´e n’est pas associe ´e a ` des arythmies postope ´ratoires chez les patients subissant un PAC Rita Katznelson, MD • W. Scott Beattie, MD, PhD • George N. Djaiani, MD • Matthew Machina, MSc • Ronit Lavi, MD • Vivek Rao, MD, PhD • Shahar Lavi, MD Received: 23 July 2013 / Accepted: 7 October 2013 / Published online: 12 November 2013 Ó Canadian Anesthesiologists’ Society 2013 Abstract Purpose The mechanism by which depression affects postoperative outcome may involve arrhythmias. The purpose of this study was to evaluate whether untreated depression is associated with an increased incidence of postoperative arrhythmias in patients undergoing coronary artery bypass graft surgery (CABG). Methods One hundred seven patients were assessed for signs of depression with the Prime-MD Patient Health Questionnaire (brief PHQ) one week before surgery and subsequently underwent Holter monitoring for 48-72 hr postoperatively. The incidences of atrial fibrillation (AF); supraventricular tachycardia (SVT); ventricular tachycardia (VT), defined as three or more consecutive beats at a cycle length less than 600 msec; ventricular fibrillation (VF); and average heart rate (HR) were recorded in patients with and without signs of depression. Results The incidence of preoperative untreated depression was 27% (29/107). Twenty patients had mild depression (brief PHQ score of 5-9), seven patients had moderate depression (a score of 10-14), and two patients had severe depression (a score of 20). The incidences of postoperative AF, SVT, and non-sustained VT in depressed and non-depressed patients were 37.9% vs 35.9%, respectively (P = 0.50), 34.4% vs 52.5%, respectively (P = 0.07), and 17.2% vs 37.1%, respectively (P = 0.04). The average (SD) postoperative HR was similar in both groups [95 (12) beatsÁmin -1 in depressed patients and 92 (10) beatsÁmin -1 in non-depressed patients, (P = 0.25)]. Multivariate regression analysis showed that older age, but not depression, was a risk factor for postoperative arrhythmia. Conclusions Preoperative untreated depression is not related to postoperative arrhythmia in the early postoperative period in patients undergoing elective CABG. This trial was registered at clinicaltrials.gov (number: NCT00622024). Re ´sume ´ Objectif Le me ´canisme par lequel la de ´pression affecte le pronostic postope ´ratoire pourrait impliquer des arythmies. L’objectif de cette e ´tude e ´tait d’e ´valuer si une de ´pression non traite ´e e ´tait associe ´e a ` une incidence accrue d’arythmies postope ´ratoires chez les patients subissant un pontage aortocoronarien (PAC). Author contributions Rita Katznelson, W. ScottBeattie, Vivec Rao, and Shahar Lavi contributed to the conception of the study. Rita Katznelson, W. Scott Beattie, George N. Djaiani, Vivec Rao, and Shahar Lavi contributed to the study design. Rita Katznelson, Ronit Lavi, Vivec Rao, and Shahar Lavi contributed to the acquisition of data. Rita Katznelson, Matthew Mashina, Ronit Lavi, and Shahar Lavi contributed to the analysis of data. Rita Katznelson, W. Scott Beattie, George N. Djaiani, Matthew Mashina, Ronit Lavi, Vivec Rao, and Shahar Lavi contributed to the interpretation of data. Rita Katznelson and Shahar Lavi participated in drafting the manuscript. W. Scott. Beattie, George N. Djaiani, Matthew Mashina, Ronit Lavi, and Vivec Rao contributed to manuscript revisions. R. Katznelson, MD (&) Á W. Scott Beattie, MD, PhD Á G. N. Djaiani, MD Á M. Machina, MSc Department of Anesthesia and Pain Management, Toronto General Hospital, Toronto, ON, Canada e-mail: [email protected] R. Lavi, MD Department of Anesthesia and Perioperative Medicine, University of Western Ontario, London, ON, Canada V. Rao, MD, PhD Department of Cardiac Surgery, Toronto General Hospital, Toronto, ON, Canada S. Lavi, MD Division of Cardiology, Department of Medicine, University of Western Ontario, London, ON, Canada 123 Can J Anesth/J Can Anesth (2014) 61:12–18 DOI 10.1007/s12630-013-0051-3
Transcript of Untreated preoperative depression is not associated with postoperative arrhythmias in CABG patients;...

REPORTS OF ORIGINAL INVESTIGATIONS
Untreated preoperative depression is not associatedwith postoperative arrhythmias in CABG patients
La depression preoperatoire non traitee n’est pas associee a desarythmies postoperatoires chez les patients subissant un PAC
Rita Katznelson, MD • W. Scott Beattie, MD, PhD • George N. Djaiani, MD •
Matthew Machina, MSc • Ronit Lavi, MD • Vivek Rao, MD, PhD •
Shahar Lavi, MD
Received: 23 July 2013 / Accepted: 7 October 2013 / Published online: 12 November 2013
� Canadian Anesthesiologists’ Society 2013
Abstract
Purpose The mechanism by which depression affects
postoperative outcome may involve arrhythmias. The
purpose of this study was to evaluate whether untreated
depression is associated with an increased incidence of
postoperative arrhythmias in patients undergoing coronary
artery bypass graft surgery (CABG).
Methods One hundred seven patients were assessed for
signs of depression with the Prime-MD Patient Health
Questionnaire (brief PHQ) one week before surgery and
subsequently underwent Holter monitoring for 48-72 hr
postoperatively. The incidences of atrial fibrillation (AF);
supraventricular tachycardia (SVT); ventricular
tachycardia (VT), defined as three or more consecutive
beats at a cycle length less than 600 msec; ventricular
fibrillation (VF); and average heart rate (HR) were
recorded in patients with and without signs of depression.
Results The incidence of preoperative untreated
depression was 27% (29/107). Twenty patients had mild
depression (brief PHQ score of 5-9), seven patients had
moderate depression (a score of 10-14), and two patients
had severe depression (a score of 20). The incidences of
postoperative AF, SVT, and non-sustained VT in depressed
and non-depressed patients were 37.9% vs 35.9%,
respectively (P = 0.50), 34.4% vs 52.5%, respectively
(P = 0.07), and 17.2% vs 37.1%, respectively (P = 0.04).
The average (SD) postoperative HR was similar in both
groups [95 (12) beats�min-1 in depressed patients and 92
(10) beats�min-1 in non-depressed patients, (P = 0.25)].
Multivariate regression analysis showed that older age, but
not depression, was a risk factor for postoperative
arrhythmia.
Conclusions Preoperative untreated depression is not
related to postoperative arrhythmia in the early
postoperative period in patients undergoing elective
CABG. This trial was registered at clinicaltrials.gov
(number: NCT00622024).
Resume
Objectif Le mecanisme par lequel la depression affecte
le pronostic postoperatoire pourrait impliquer des
arythmies. L’objectif de cette etude etait d’evaluer si une
depression non traitee etait associee a une incidence
accrue d’arythmies postoperatoires chez les patients
subissant un pontage aortocoronarien (PAC).
Author contributions Rita Katznelson, W. ScottBeattie, Vivec Rao,and Shahar Lavi contributed to the conception of the study. RitaKatznelson, W. Scott Beattie, George N. Djaiani, Vivec Rao, andShahar Lavi contributed to the study design. Rita Katznelson, RonitLavi, Vivec Rao, and Shahar Lavi contributed to the acquisition ofdata. Rita Katznelson, Matthew Mashina, Ronit Lavi, and ShaharLavi contributed to the analysis of data. Rita Katznelson, W. ScottBeattie, George N. Djaiani, Matthew Mashina, Ronit Lavi, VivecRao, and Shahar Lavi contributed to the interpretation of data. RitaKatznelson and Shahar Lavi participated in drafting the manuscript.W. Scott. Beattie, George N. Djaiani, Matthew Mashina, Ronit Lavi,and Vivec Rao contributed to manuscript revisions.
R. Katznelson, MD (&) � W. Scott Beattie, MD, PhD �G. N. Djaiani, MD � M. Machina, MSc
Department of Anesthesia and Pain Management, Toronto
General Hospital, Toronto, ON, Canada
e-mail: [email protected]
R. Lavi, MD
Department of Anesthesia and Perioperative Medicine,
University of Western Ontario, London, ON, Canada
V. Rao, MD, PhD
Department of Cardiac Surgery, Toronto General Hospital,
Toronto, ON, Canada
S. Lavi, MD
Division of Cardiology, Department of Medicine, University of
Western Ontario, London, ON, Canada
123
Can J Anesth/J Can Anesth (2014) 61:12–18
DOI 10.1007/s12630-013-0051-3
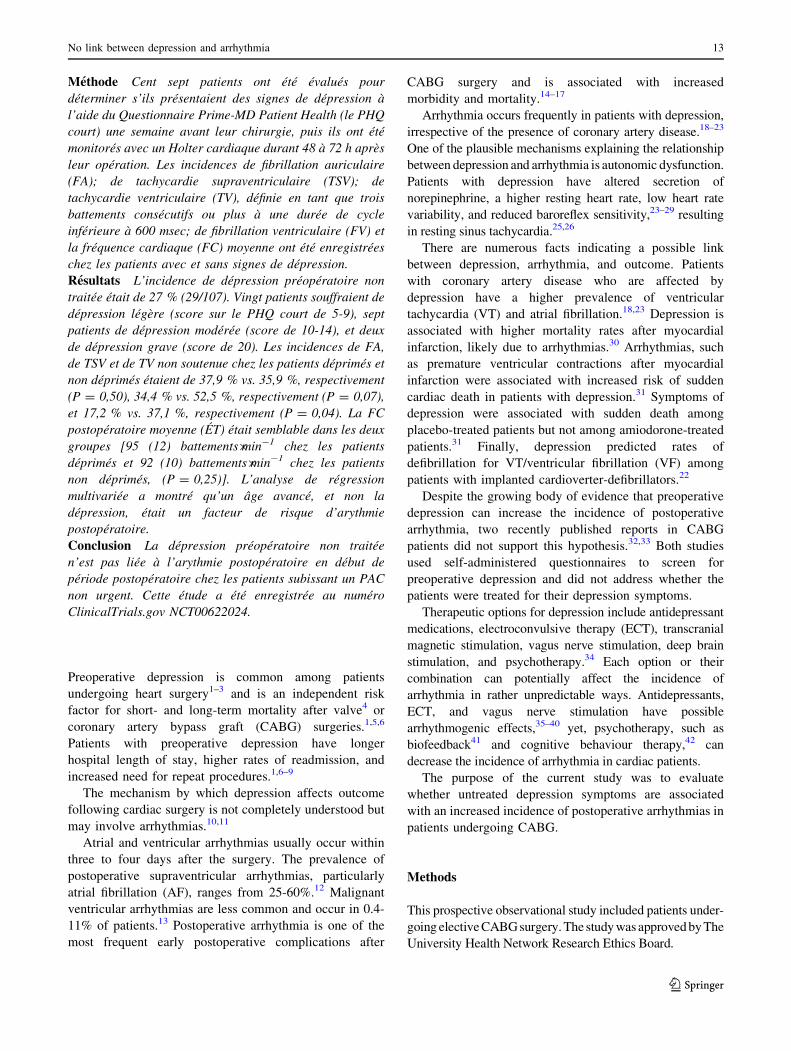
Methode Cent sept patients ont ete evalues pour
determiner s’ils presentaient des signes de depression a
l’aide du Questionnaire Prime-MD Patient Health (le PHQ
court) une semaine avant leur chirurgie, puis ils ont ete
monitores avec un Holter cardiaque durant 48 a 72 h apres
leur operation. Les incidences de fibrillation auriculaire
(FA); de tachycardie supraventriculaire (TSV); de
tachycardie ventriculaire (TV), definie en tant que trois
battements consecutifs ou plus a une duree de cycle
inferieure a 600 msec; de fibrillation ventriculaire (FV) et
la frequence cardiaque (FC) moyenne ont ete enregistrees
chez les patients avec et sans signes de depression.
Resultats L’incidence de depression preoperatoire non
traitee etait de 27 % (29/107). Vingt patients souffraient de
depression legere (score sur le PHQ court de 5-9), sept
patients de depression moderee (score de 10-14), et deux
de depression grave (score de 20). Les incidences de FA,
de TSV et de TV non soutenue chez les patients deprimes et
non deprimes etaient de 37,9 % vs. 35,9 %, respectivement
(P = 0,50), 34,4 % vs. 52,5 %, respectivement (P = 0,07),
et 17,2 % vs. 37,1 %, respectivement (P = 0,04). La FC
postoperatoire moyenne (ET) etait semblable dans les deux
groupes [95 (12) battements�min-1 chez les patients
deprimes et 92 (10) battements�min-1 chez les patients
non deprimes, (P = 0,25)]. L’analyse de regression
multivariee a montre qu’un age avance, et non la
depression, etait un facteur de risque d’arythmie
postoperatoire.
Conclusion La depression preoperatoire non traitee
n’est pas liee a l’arythmie postoperatoire en debut de
periode postoperatoire chez les patients subissant un PAC
non urgent. Cette etude a ete enregistree au numero
ClinicalTrials.gov NCT00622024.
Preoperative depression is common among patients
undergoing heart surgery1–3 and is an independent risk
factor for short- and long-term mortality after valve4 or
coronary artery bypass graft (CABG) surgeries.1,5,6
Patients with preoperative depression have longer
hospital length of stay, higher rates of readmission, and
increased need for repeat procedures.1,6–9
The mechanism by which depression affects outcome
following cardiac surgery is not completely understood but
may involve arrhythmias.10,11
Atrial and ventricular arrhythmias usually occur within
three to four days after the surgery. The prevalence of
postoperative supraventricular arrhythmias, particularly
atrial fibrillation (AF), ranges from 25-60%.12 Malignant
ventricular arrhythmias are less common and occur in 0.4-
11% of patients.13 Postoperative arrhythmia is one of the
most frequent early postoperative complications after
CABG surgery and is associated with increased
morbidity and mortality.14–17
Arrhythmia occurs frequently in patients with depression,
irrespective of the presence of coronary artery disease.18–23
One of the plausible mechanisms explaining the relationship
between depression and arrhythmia is autonomic dysfunction.
Patients with depression have altered secretion of
norepinephrine, a higher resting heart rate, low heart rate
variability, and reduced baroreflex sensitivity,23–29 resulting
in resting sinus tachycardia.25,26
There are numerous facts indicating a possible link
between depression, arrhythmia, and outcome. Patients
with coronary artery disease who are affected by
depression have a higher prevalence of ventricular
tachycardia (VT) and atrial fibrillation.18,23 Depression is
associated with higher mortality rates after myocardial
infarction, likely due to arrhythmias.30 Arrhythmias, such
as premature ventricular contractions after myocardial
infarction were associated with increased risk of sudden
cardiac death in patients with depression.31 Symptoms of
depression were associated with sudden death among
placebo-treated patients but not among amiodorone-treated
patients.31 Finally, depression predicted rates of
defibrillation for VT/ventricular fibrillation (VF) among
patients with implanted cardioverter-defibrillators.22
Despite the growing body of evidence that preoperative
depression can increase the incidence of postoperative
arrhythmia, two recently published reports in CABG
patients did not support this hypothesis.32,33 Both studies
used self-administered questionnaires to screen for
preoperative depression and did not address whether the
patients were treated for their depression symptoms.
Therapeutic options for depression include antidepressant
medications, electroconvulsive therapy (ECT), transcranial
magnetic stimulation, vagus nerve stimulation, deep brain
stimulation, and psychotherapy.34 Each option or their
combination can potentially affect the incidence of
arrhythmia in rather unpredictable ways. Antidepressants,
ECT, and vagus nerve stimulation have possible
arrhythmogenic effects,35–40 yet, psychotherapy, such as
biofeedback41 and cognitive behaviour therapy,42 can
decrease the incidence of arrhythmia in cardiac patients.
The purpose of the current study was to evaluate
whether untreated depression symptoms are associated
with an increased incidence of postoperative arrhythmias in
patients undergoing CABG.
Methods
This prospective observational study included patients under-
going elective CABG surgery. The study was approved by The
University Health Network Research Ethics Board.
No link between depression and arrhythmia 13
123

The study took place from August 2008 until August
2011 and included 120 consecutive patients. All
participants provided informed consent. Inclusion criteria
were patients undergoing elective CABG and aged
18-75 yr. Exclusion criteria were history of arrhythmias
(AF, supraventricular tachycardia [SVT], VT, VF, perma-
nent pacemaker, and/or defibrillator), history of psychiatric
disorders (schizophrenia, mania, psychosis), treatment for
depression in the last six months prior to surgery,
pulmonary hypertension, and left ventricular ejection
fraction \ 40%.
One week before surgery, a trained research assistant
assessed patients in the anesthesia preoperative clinic for
signs of depression using the brief version of Prime-MD
Patient Health Questionnaire (brief PHQ). The depression
module of the brief PHQ scores each of the nine DSM-IV
depression criteria as ‘‘0’’ (not at all) to ‘‘3’’ (nearly every
day). Scores of 5, 10, 15, and 20 represent mild, moderate,
moderately-severe, and severe depression, respectively.43
The brief PHQ is a screening tool for depression symptoms
recommended by the American Heart Association to
identify depression in cardiac patients.44 Patients with a
PHQ score C 10 were referred to psychiatry consult
postoperatively.
Starting immediately after surgery, Holter monitoring
was applied for 48-72 hr. Holter electrocardiogram (ECG)
recordings were scanned by a MARS�8000 Arrhythmia
Review Station (Wipro GE Healthcare) and interpreted by
a Holter technician and a cardiologist who were blinded to
the results of the depression assessment.
The primary outcome was the proportion of patients with
postoperative ventricular or supraventricular arrhythmias.
The following arrhythmias were recorded: number and
frequency of episodes of AF, SVT, VT (defined as three or
more consecutive beats at a cycle length less than 600
msec), and VF, and average heart rate.
Based on the psychiatric assessment, all patients were
divided into two groups: patients with signs of depression
(depression score C 5) and patients without signs of
depression (depression score \ 5). The incidence of
postoperative arrhythmias was compared between the
groups.
Sample size calculation
Our sample size was based on an incidence of post CABG
atrial fibrillation of 40% in patients with no depression.12
Although the incidence of depression in patients with
coronary artery disease before CABG may be 40%,45 we
made a conservative assumption that only 25% of our
patients would have preoperative depression.
A sample size of 108 patients (unequal n in the two
groups, 25% of patients having untreated depression) has
80% power to detect a relative risk of 1.77 with a
significance level of 0.05.
We estimated an attrition rate of 10%; therefore, the
final sample size was 120 patients.
Statistical analysis
A simple 2 x 2 contingency table was constructed to
evaluate the presence of ventricular and /or supraventricular
arrhythmias (dichotomous outcome) based on the Holter
monitor assessment after surgery in patients with and
without untreated depression.
Single predictor and multivariable logistic regression
models were used to calculate the effect of preoperative
untreated depression on postoperative arrhythmia. Untreated
depression and other variables shown to have marginal
association (P\0.20) in the single predictor analysis were
included in the multivariable model. The following variables
were included in the multivariable model: age, sex,
preoperative use of beta- and calcium channel blockers,
cardiopulmonary bypass time, postoperative use of inotropic
agents, and depression scores. Stata� ver. 12.1 (StataCorp
LP, College Station, TX, USA) was used to analyze the data.
Results
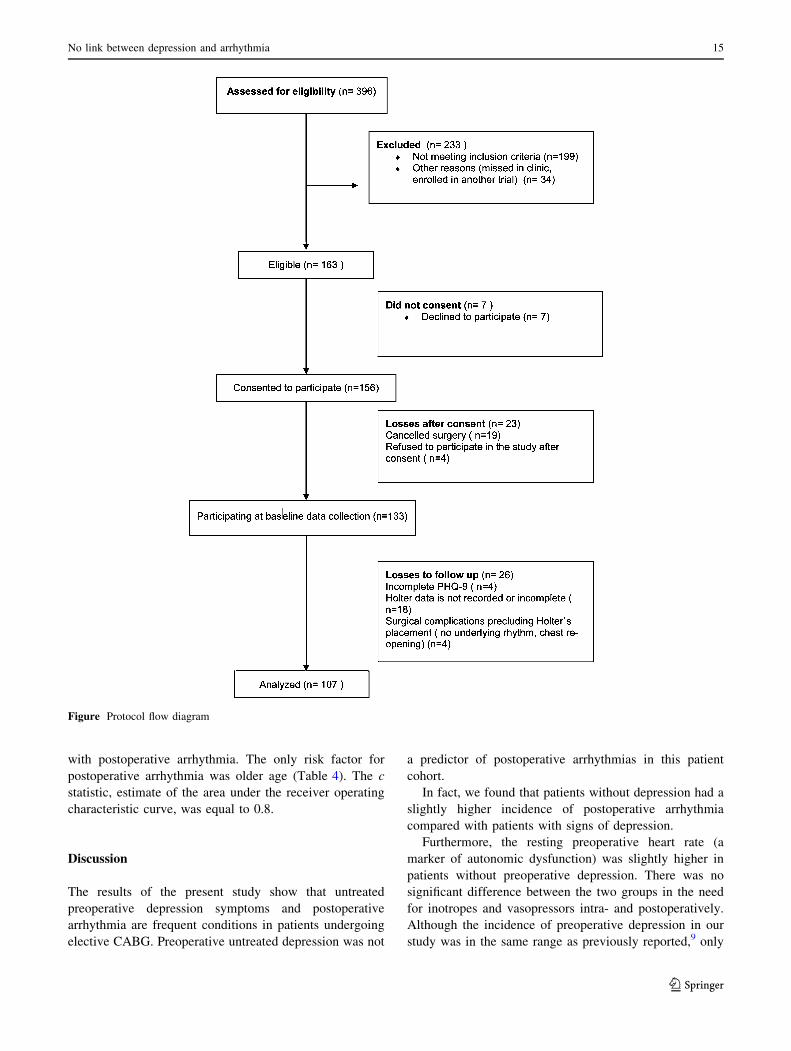
One hundred seven patients completed the study (Figure).
The incidence of preoperative untreated depression was
27% (29/107). Twenty patients were found to have mild
depression (brief PHQ score of 5-9), seven patients had
moderate depression (a score of 10-14), and two patients
had severe depression (a score of 20).
The depression group included more females, and the
patients in this group had lower hemoglobin and creatinine
levels. Patients without signs of depression had a higher
preoperative heart rate and a higher incidence of
preoperative myocardial infarction (Table 1). There was
no difference between groups in surgical characteristics or
in the incidence of intraoperative use of inotropes and
vasoactive drugs (Table 2).
None of the patients developed sustained VT or VF. The
incidence of non-sustained VT was 31.8%, and the
incidence of postoperative atrial fibrillation was 36.4%.
Overall, there were more arrhythmias in the no
depression group. There was no difference between
groups in the incidence of postoperative atrial fibrillation
and supraventricular arrhythmias (Table 3). None of the
patients developed sustained VT or VF, but the incidence
of non-sustained VT was higher in the patients without
depression. Multivariate logistic regression analysis
showed that preoperative depression is not associated
14 R. Katznelson et al.
123
with postoperative arrhythmia. The only risk factor for
postoperative arrhythmia was older age (Table 4). The c
statistic, estimate of the area under the receiver operating
characteristic curve, was equal to 0.8.
Discussion
The results of the present study show that untreated
preoperative depression symptoms and postoperative
arrhythmia are frequent conditions in patients undergoing
elective CABG. Preoperative untreated depression was not
a predictor of postoperative arrhythmias in this patient
cohort.
In fact, we found that patients without depression had a
slightly higher incidence of postoperative arrhythmia
compared with patients with signs of depression.
Furthermore, the resting preoperative heart rate (a
marker of autonomic dysfunction) was slightly higher in
patients without preoperative depression. There was no
significant difference between the two groups in the need
for inotropes and vasopressors intra- and postoperatively.
Although the incidence of preoperative depression in our
study was in the same range as previously reported,9 only
Figure Protocol flow diagram
No link between depression and arrhythmia 15
123

nine patients fulfilled the criteria for moderate-severe
depression. Therefore, the majority of patients in our
cohort with mild depression symptoms simply did not
reach the trigger threshold for autonomic dysfunction and
neurotransmitter imbalance contributing to postoperative
arrhythmia.
We excluded patients who were at high risk for
postoperative arrhythmia. These included patients with a
history of arrhythmia prior to surgery, poor left ventricular
function, and pulmonary hypertension. The incidence of
postoperative arrhythmia (AF and non-sustained VT) in the
current cohort was similar to that in previous reports.13,17,46
Table 1 Baseline characteristics
Suspected
depression*
No
depression
P value
(n = 29) (n = 78)
Age (yr) 63.0 (9.6) 64.6 (9.4) 0.45
Sex (female) 8 (27.5%) 2 (2.5%) 0.004
BMI (kg�m-2) 27.7 (4.4) 28.5 (5.6) 0.5
Preoperative heart rate
(beats�min-1)
63 (10) 68 (15) 0.03
Preoperative pulse Pressure
(mmHg)
54 (13) 57 (18) 0.27
Hypertension 23 (79.3%) 54 (69.2%) 0.3
Diabetes 8 (27.5%) 35 (44.8%) 0.12
PVD 4 (13.8%) 9 (11.5%) 0.7
Previous MI 4 (13.8%) 28 (35.9%) 0.03
Stroke 1 (3.4%) 7 (8.9%) 0.4
COPD 1 (3.4%) 4 (5.1%) 1.0
Alcohol use C 2 drinks/day 29 (6.9%) 4 (5.1%) 0.6
Beta blockers 21 (72.4%) 47 (60.2%) 0.27
Ca channel blockers 4 (13.8%) 14 (17.9%) 0.7
Preoperative Hb (g�dL-1) 138 (13) 144 (12) 0.05
Preoperative creatinine (lM) 73 (38) 88 (22) 0.01
Preoperative potassium
(mEq�L-1)
4.2 (0.3) 4.1 (0.4) 0.2
Data are expressed as mean (SD) or number (%). BMI = body mass
index; Hb = hemoglobin; PVD = peripheral vascular disease;
MI = myocardial infarction; COPD = chronic obstructive
pulmonary disease. *Prime-MD Patient Health Questionnaire score C 5
Table 2 Intraoperative data
Suspected
Depression*
No
depression
P value
(n = 29) (n = 78)
Number of coronary artery
grafts, median (min; max)
3 (1;4) 3 (1;4) 0.9
CPB time (min) 78 (28) 79 (23) 0.8
Aortic cross clamp time (min) 63 (27) 61 (19) 0.7
Intraoperative dopamine 12 (41.3%) 18 (23%) 0.06
Intraoperative epinephrine 1 (3.4%) 7 (8.9%) 0.3
Intraoperative norepinephrine 5 (17.2%) 17 (21.8%) 0.6
Intraoperative vasopressin 1 (3.4%) 4 (5.1%) 0.6
Intraoperative milrinone 0 2 (2.5%) 0.5
Data are expressed as mean (SD) or number (%) unless otherwise
indicated. CPB = cardiopulmonary bypass. *Prime-MD Patient
Health Questionnaire score C 5
Table 3 Postoperative arrhythmia
Suspected
depression*
No
depression
P value
(n = 29) (n = 78)
Heart rate (average)
(beats�min-1)
95 (12) 92 (10) 0.25
AF 11 (37.9%) 28 (35.9%) 0.5
AF time [ 3 min 8 (27.5%) 13 (16.7%) 0.27
SVT 10 (34.4%) 41 (52.5%) 0.07
VT 5 (17.2%) 29 (37.1%) 0.04
All arrhythmias 20 (68.9%) 69 (88.4%) 0.02
Postoperative amiodarone 9 (31%) 26 (33.3%) 0.2
Postoperative beta blockers 21 (72.4%) 48 (61.5%) 0.12
Postoperative Ca channel
blockers
1 (3.4%) 2 (2.5%) 0.6
Cardioversion 0 2 (2.5%) 0.5
Postoperative norepinephrine 10 (34.4%) 25 (32.0%) 0.49
Postoperative epinephrine 1 (3.4%) 6 (7.7%) 0.39
Postoperative dopamine 13 (33.3%) 37 (47.4%) 0.03
Postoperative vasopressin 2 (6.9%) 9 (11.5%) 0.38
Postoperative milrinone 0 2 (2.6%) 0.5
Data are expressed as mean (SD) or number (%). AF = atrial
fibrillation; SVT = supraventricular tachycardia; VT = ventricular
tachycardia. *Prime-MD Patient Health Questionnaire score C 5
Table 4 Multivariate logistic regression for postoperative
arrhythmias (ventricular and supraventricular)
Odds
Ratio
Standard
Error
z score P value Confidence
intervals
Suspected
Depression*
0.27 0.23 -1.48 0.1 0.05 (1.5)
Age 1.13 0.05 2.63 0.008 1.03 (1.24)
Female sex 1.9 2.8 0.47 0.5 0.12 (32.6)
CPB time [ 90 min 1.8 1.6 0.6 0.5 0.27 (1.6)
Preoperative Ca
channel blockers
3.1 4.5 0.93 0.3 0.25 (45)
Preoperative beta
blockers
0.8 0.8 -0.2 0.8 0.1 (6.0)
Postoperative
dopamine
1.7 1.6 0.59 0.6 0.27 (10.7)
CPB = cardiopulmonary bypass. *Prime-MD Patient Health
Questionnaire score C 5
16 R. Katznelson et al.
123

One of the mechanisms explaining the association
between depression and arrhythmia is the arrhythmogenic
effect of antidepressant medications. Both tricyclic
antidepressants and selective serotonin reuptake inhibitors
may prolong the QT interval, affect heart rate variability,
and cause arrhythmias.35–38 In addition, non-
pharmacological modalities, such as ECT and vagus
nerve stimulation, can trigger arrhythmias by affecting
the QT interval or causing heart block.39,40 To avoid this
confounding factor, patients who were treated for
depression were excluded from our study. Similar to
previous studies, we confirmed that older age is an
independent risk factor for postoperative arrhythmia and
that there was no positive association between depression
and arrhythmia in patients with coronary artery disease.
A recent report by Turagam et al.47 showed that patients
who survived sudden cardiac death and have a history of
depression are not at higher risk of recurrent arrhythmia
and death than those with no history of depression.
In a study by Beresnevaite et al.,32 109 male patients
undergoing CABG were evaluated for preoperative
depression and postoperative complications. They did not
find any association between preoperative depression and
early postoperative complications, including arrhythmia.
The authors did not elaborate on their definition of
postoperative arrhythmia or on the diagnostic criteria
they used. In a study by Tully et al.,33 222 patients
undergoing cardiac surgery were assessed for preoperative
depression and anxiety. The primary outcome in this study
was atrial fibrillation. The diagnosis was done with Holter
monitoring applied for the first three postoperative days
and thereafter with daily electrocardiograms until
discharge. They found that anxiety, but not preoperative
depression, had an association with postoperative atrial
fibrillation. The authors did not comment on ventricular
arrhythmias in their patient cohort. As previously
mentioned, there was no discussion in any of these
studies regarding the presence or absence of preoperative
antidepressant therapy in the studied patients.
The results of our study extend the prior observations.
Ours is a novel study using Holter monitoring specifically
to diagnose the incidence of both supraventricular and
ventricular postoperative arrhythmia in patients screened
preoperatively for untreated depression. Therefore, we
consider our results to be robust enough to conclude that
untreated preoperative depression symptoms are not
associated with postoperative arrhythmias.
The definition of depression was based on the results of
a brief PHQ, which is a screening tool to identify patients
with high risk for depression. Although high scores of the
brief PHQ have high specificity and sensitivity for major
depression, it cannot substitute psychiatric assessment for
clinical diagnosis of depression. We did not perform a
formal psychiatric examination in our patients and,
therefore, our findings should be limited to only those
patients defined as high risk for depression. The Holter
monitor was applied for only 48-72 hr, and thus, there may
have been arrhythmias after this period. Nevertheless, the
incidence within the first 48-72 hr was high enough to
confirm our findings. We included all types of arrhythmias
in our study, some with a very short duration; therefore,
some of the recorded arrhythmias are less likely to be
clinically significant.
The results of our study cannot be applied to patients
with a known history of arrhythmia and those who were
treated with antidepressant medications or other
therapeutic modalities in the perioperative period.
Although preoperative depression is a known independent
risk factor for postoperative morbidity and mortality, it is
unlikely that the negative effect of untreated depression
symptoms on postoperative outcomes is related to arrhythmia
in the early postoperative period.
Funding Dean’s Fund, University of Toronto, Canada.
Competing interests None declared.
References
1. Burg MM, Benedetto MC, Rosenberg R, Soufer R. Presurgical
depression predicts medical morbidity 6 months after coronary
artery bypass graft surgery. Psychosom Med 2003; 65: 111-8.
2. Blumenthal JA, Lett HS. Depression and cardiac risk.
J Cardiopulm Rehabil 2005; 25: 78-9.
3. Phillips-Bute B, Mathew JP, Blumenthal JA, et al. Relationship
of genetic variability and depressive symptoms to adverse events
after coronary artery bypass graft surgery. Psychosom Med 2008;
70: 953-9.
4. Ho PM, Masoudi FA, Spertus JA, et al. Depression predicts
mortality following cardiac valve surgery. Ann Thorac Surg
2005; 79: 1255-9.
5. Pignay-Demaria V, Lesperance F, Demaria RG, Frasure-Smith
N, Perrault LP. Depression and anxiety and outcomes of
coronary artery bypass surgery. Ann Thorac Surg 2003; 75:
314-21.
6. Connerney I, Shapiro PA, McLaughlin JS, Bagiella E, Sloan RP.
Relation between depression after coronary artery bypass surgery
and 12-month outcome: a prospective study. Lancet 2001; 358:
1766-71.
7. Baker RA, Andrew MJ, Schrader G, Knight JL. Preoperative
depression and mortality in coronary artery bypass surgery:
preliminary findings. ANZ J Surg 2001; 71: 139-42.
8. Tully PJ, Baker RA, Turnbull D, Winefield H. The role of
depression and anxiety symptoms in hospital readmissions after
cardiac surgery. J Behav Med 2008; 31: 281-90.
9. Tully PJ, Baker RA. Depression, anxiety, and cardiac morbidity
outcomes after coronary artery bypass surgery: a contemporary
and practical review. J Geriatr Cardiol 2012; 9: 197-208.
10. Tully PJ. Psychological depression and cardiac surgery: a
comprehensive review. J Extra Corpor Technol 2012; 44: 224-32.
11. Sher Y, Lolak S, Maldonado JR. The impact of depression in heart
disease. Curr Psychiatry Rep 2010; 12: 255-64.
No link between depression and arrhythmia 17
123

12. Maisel WH, Rawn JD, Stevenson WG. Atrial fibrillation after
cardiac surgery. Ann Intern Med 2001; 135: 1061-73.
13. Knotzer H, Dunser MW, Mayr AJ, Hasibeder WR. Postbypass
arrhythmias: pathophysiology, prevention, and therapy. Curr
Opin Crit Care 2004; 10: 330-5.
14. Jongnarangsin K, Oral H. Postoperative atrial fibrillation.
Cardiol Clin 2009; 27: 69-78.
15. Mayr A, Knotzer H, Pajk W, et al. Risk factors associated with
new onset tachyarrhythmias after cardiac surgery–a retrospective
analysis. Acta Anaesthesiol Scand 2001; 45: 543-9.
16. Sapin PM, Woelfel AK, Foster JR. Unexpected ventricular
tachyarrhythmias soon after cardiac surgery. Am J Cardiol
1991; 68: 1099-100.
17. Almassi GH, Schowalter T, Nicolosi AC, et al. Atrial fibrillation
after cardiac surgery: a major morbid event? Ann Surg 1997; 226:
501-11.
18. Carney RM, Freedland KE, Rich MW, Smith LJ, Jaffe AS.
Ventricular tachycardia and psychiatric depression in patients
with coronary artery disease. Am J Med 1993; 95: 23-8.
19. Lange HW, Herrmann-Lingen C. Depressive symptoms predict
recurrence of atrial fibrillation after cardioversion. J Psychosom
Res 2007; 63: 509-13.
20. Lown B, DeSilva RA. Roles of psychologic stress and autonomic
nervous system changes in provocation of ventricular premature
complexes. Am J Cardiol 1978; 41: 979-85.
21. Mallik S, Krumholz HM, Lin ZQ, et al. Patients with depressive
symptoms have lower health status benefits after coronary artery
bypass surgery. Circulation 2005; 111: 271-7.
22. Whang W, Albert CM, Sears SF Jr, et al. Depression as a predictor for
appropriate shocks among patients with implantable cardioverter-defibrillators: results from the Triggers of Ventricular Arrhythmias
(TOVA) study. J Am Coll Cardiol 2005; 45: 1090-5.
23. Catipovic-Veselica K, Galic A, Jelic K, et al. Relation between
major and minor depression and heart rate, heart-rate variability,
and clinical characteristics of patients with acute coronary
syndrome. Psychol Rep 2007; 100: 1245-54.
24. Louis WJ, Doyle AE, Anavekar SN. Plasma noradrenaline
concentration and blood pressure in essential hypertension,
phaeochromocytoma and depression. Clin Sci Mol Med Suppl
1975; 2: 239S-42S.
25. Lechin F, van der Dijs B, Orozco B, et al. Plasma
neurotransmitters, blood pressure, and heart rate during supine-
resting, orthostasis, and moderate exercise conditions in major
depressed patients. Biol Psychiatry 1995; 38: 166-73.
26. Carney RM, Rich MW, teVelde A, Saini J, Clark K, Freedland
KE. The relationship between heart rate, heart rate variability and
depression in patients with coronary artery disease. J Psychosom
Res 1988; 32: 159-64.
27. Johansson M, Ehnvall A, Friberg P, Myredal A. Arterial
baroreflex dysfunction in major depressive disorder. Clin Auton
Res 2010; 20: 235-40.
28. Francis JL, Weinstein AA, Krantz DS, et al. Association between
symptoms of depression and anxiety with heart rate variability in
patients with implantable cardioverter defibrillators. Psychosom
Med 2009; 71: 821-7.
29. Watkins LL, Grossman P. Association of depressive symptoms
with reduced baroreflex cardiac control in coronary artery
disease. Am Heart J 1999; 137: 453-7.
30. Carney RM, Blumenthal JA, Catellier D, et al. Depression as a
risk factor for mortality after acute myocardial infarction. Am J
Cardiol 2003; 92: 1277-81.
31. Irvine J, Basinski A, Baker B, et al. Depression and risk of sudden
cardiac death after acute myocardial infarction: testing for the
confounding effects of fatigue. Psychosom Med 1999; 61:
729-37.
32. Beresnevaite M, Benetis R, Taylor GJ, Jureniene K, Kinduris S,
Barauskiene V. Depression predicts perioperative outcomes
following coronary artery bypass graft surgery. Scand
Cardiovasc J 2010; 44: 289-94.
33. Tully PJ, Bennetts JS, Baker RA, McGavigan AD, Turnbull DA,
Winefield HR. Anxiety, depression, and stress as risk factors for
atrial fibrillation after cardiac surgery. Heart Lung 2011; 40: 4-11.
34. Mavrides N, Nemeroff C. Treatment of depression in
cardiovascular disease. Depress Anxiety 2013; 30: 328-41.
35. Vieweg WV, Wood MA, Fernandez A, Beatty-Brooks M, Hasnain
M, Pandurangi AK. Proarrhythmic risk with antipsychotic and
antidepressant drugs: implications in the elderly. Drugs Aging
2009; 26: 997-1012.
36. Deshmukh A, Ulveling K, Alla V, Abuissa H, Airey K. Prolonged
QTc interval and torsades de pointes induced by citalopram. Tex
Heart Inst J 2012; 39: 68-70.
37. Johnson EM, Whyte E, Mulsant BH, et al. Cardiovascular
changes associated with venlafaxine in the treatment of late-life
depression. Am J Geriatr Psychiatry 2006; 14: 796-802.
38. Licht CM, de Geus EJ, van Dyck R, Penninx BW. Longitudinal
evidence for unfavorable effects of antidepressants on heart rate
variability. Biol Psychiatry 2010; 68: 861-8.
39. Yamaguchi S, Nagao M, Ikeda T, et al. QT dispersion and rate-
corrected QT dispersion during electroconvulsive therapy in
elderly patients. J ECT 2011; 27: 183-8.
40. Singleton AH, Rosenquist PB, Kimball J, McCall WV. Cardiac
rhythm disturbance in a depressed patient after implantation with
a vagus nerve stimulator. J ECT 2009; 25: 195-7.
41. Patron E, Messerotti Benvenuti S, Favretto G, et al. Biofeedback
assisted control of respiratory sinus arrhythmia as a biobehavioral
intervention for depressive symptoms in patients after cardiac
surgery: a preliminary study. Appl Psychophysiol Biofeedback
2013; 38: 1-9.
42. Chevalier P, Cottraux J, Mollard E, et al. Prevention of
implantable defibrillator shocks by cognitive behavioral
therapy: a pilot trial. Am Heart J 2006; 151: 191.
43. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a
brief depression severity measure. J Gen Intern Med 2001; 16:
606-13.
44. Lichtman JH, Bigger JT Jr, Blumenthal JA, et al. Depression and
coronary heart disease: recommendations for screening, referral,
and treatment: a science advisory from the American Heart
Association Prevention Committee of the Council on
Cardiovascular Nursing, Council on Clinical Cardiology,
Council on Epidemiology and Prevention, and Interdisciplinary
Council on Quality of Care and Outcomes Research: endorsed by
the American Psychiatric Association. Circulation 2008; 118:
1768-75.
45. Pirraglia PA, Peterson JC, Williams-Russo P, Gorkin L,
Charlson ME. Depressive symptomatology in coronary artery
bypass graft surgery patients. Int J Geriatr Psychiatry 1999; 14:
668-80.
46. Magyar-Russell G, Thombs BD, Cai JX, et al. The prevalence of
anxiety and depression in adults with implantable cardioverter
defibrillators: a systematic review. J Psychosom Res 2011; 71:
223-31.
47. Turagam MK, Velagapudi P, Szabo A, Visotcky A, Kocheril AG.
Survivors of sudden cardiac death with history of depression are
not at significantly greater risk of recurrent arrhythmias and
death. Int J Cardiol 2012; 157: 445-6.
18 R. Katznelson et al.
123