UNIVERSITY OF OTAGO ARTHRITIS RESEARCH THEME · Dunedin!Patient!Update!Meeting ... gout and...
49
Transcript of UNIVERSITY OF OTAGO ARTHRITIS RESEARCH THEME · Dunedin!Patient!Update!Meeting ... gout and...
Arthritis Research Theme 2013 Report 1
UNIVERSITY OF OTAGO ARTHRITIS RESEARCH THEME
2013 ANNUAL REPORT
Contents Directors Introduction ............................................................................................................................ 2
Aims of the Arthritis Research Theme .................................................................................................... 3
Core members and associate members ................................................................................................. 4
Press releases ......................................................................................................................................... 5
Otago scientists find genetic link between sugary drinks and gout ................................................... 5
Crippling costs ..................................................................................................................................... 7
New Otago research shows early Māori probably suffered from gout ............................................ 11
Vitamin C does not alleviate gout as previously thought ................................................................. 13
Osteoarthritis improved by extra physiotherapy programmes ........................................................ 14
Footwear and knee injuries being studied ....................................................................................... 16
Juicy bits ............................................................................................................................................... 17
Smoking and Rheumatoid arthritis ................................................................................................... 17
Complementary and alternative medicine – what does your doctor think? .................................... 18
Living with dry mouth ....................................................................................................................... 20
Soft Tissue X-‐rays in Scleroderma ..................................................................................................... 22
Meetings ............................................................................................................................................... 24
Conference Presentations .................................................................................................................... 28
2013 publications ................................................................................................................................. 28
Theme members highlights of 2013 ..................................................................................................... 35
Dunedin Patient Update Meeting ..................................................................................................... 35
Update from the ACR/EULAR Gout Classification Criteria Project .................................................... 35
Grants received in 2013 ........................................................................................................................ 36
Postgraduate students (completed) ..................................................................................................... 37
Current Postgraduate Students ............................................................................................................ 37
Student travel Awards .......................................................................................................................... 39
Summer students ................................................................................................................................. 41
Non-‐additive gene interactions with sugar-‐sweetened beverage consumption and the risk of Gout .......................................................................................................................................................... 41
Joint infections in patients with rheumatic diseases ........................................................................ 42
Dexterity in rheumatoid arthritis: Pilot testing a novel measurement glove and investigating correlates .......................................................................................................................................... 46

Arthritis Research Theme 2013 Report
2
Directors Introduction
The Arthritis Research Theme has had another successful year. Two theme meetings have
been held, both in Dunedin. The first meeting in May was attended by ~40 people including
representatives from Arthritis New Zealand. Professor Ric Day was the invited speaker from
the University of New South Wales. He gave an excellent talk on allopurinol and gout
management. His visit has strengthened the collaboration with Dan Wright, Murray Barclay
and myself. Once again students contributed a number of outstanding presentations to the
meeting. The second theme meeting was held in December. This was a combined meeting
with the Renal Theme and the Gut Health Network. Two summer students have been funded
by the theme and have completed their 10 weeks of research investigation. Two PhD students
were also supported to attend international meetings to present their research
A close relationship has continued with Arthritis New Zealand with attendance by Arthritis
New Zealand representatives at theme meetings. Theme members have also provided articles
in the quarterly newsletter “Juice” which is sent to all Arthritis New Zealand members.
Throughout 2013, theme members have continued strong contributions to international
Arthritis research endeavours, publishing more than 90 papers in top rheumatology and
scientific journals.
We look forward to another successful year in 2014.
Lisa Stamp
Steering Committee: Assoc Prof Tony Merriman, Dr Paul Hessian, Dr Simon Stebbings, Prof Murray Barclay, Prof Lisa Stamp, Assoc Prof Will Taylor, Prof John Highton, Dr Gareth Treharne
Arthritis Research Theme 2013 Report
3
Aims of the Arthritis Research Theme
1. To strengthen research into rheumatic diseases within the University of Otago by
encouraging basic, translational, clinical, and epidemiological research relevant to the
range of rheumatic diseases
2. To foster collaborative research between disciplines both within and beyond the
University in order to promote world class research
3. Increase external research funding in the broad field of arthritis.
Pa`ents with
Arthri`s
Environmental causes of arthri`s
Way drugs work in arthri`s
Improving treatment of arthri`s
Measuring outcomes in arthri`s
Gene`c risk of arthri`s
Inflammatory mechanisms of
arthri`s

Arthritis Research Theme 2013 Report
4
Core members and associate members Members Associate
Members DUNEDIN Medicine -‐ Dr Simon Stebbings, Prof John Highton, Dr Paul
Hessian, Debra McNamara, Dr Hamish Osborne, A/Prof Michael Schultz
Arthritis NZ – David Cox, Dr Natalia Valentino
Psychology -‐ Dr Gareth Treharne, Dr Nicola Swain
Physiology -‐ Dr Andrew Bahn
Pharmacy -‐ Prof Stephen Duffell, Dr Dan Wright , Shan Pan*
Biochemistry -‐ A/Prof Tony Merriman, Mandy Phipps-‐Green
Surgical Sciences – Dr Rebecca Roberts, Dr Mary Wallace
Physiotherapy -‐ Prof David Baxter, Lesley Ward*
Oral health -‐ A/Prof Anita Nolan
Orthopaedics –A/Prof Haxby Abbott
CHRISTCHURCH Medicine-‐ Prof Lisa Stamp, Pip Aimer*, Jill Drake, Janine Francis, Claire Heppenstall
CDHB – Dr Peter Chapman, Dr John O’Donnell Kaikoura Medical Center – Andrea Judd
Clinical Pharmacology -‐ Prof Murray Barclay, A/Prof Matt Doogue
Pathology -‐ Prof Tony Kettle General Practice – Dr Ben Hudson
WELLINGTON Medicine – A/Prof Andrew Harrison, A/Prof William Taylor, Dr Rebecca Grainger
Malaghan Institute -‐ Dr Jacqui Harper; Michael Woodhouse MP
Arthritis Research Theme 2013 Report
5
Press releases
Otago scientists find genetic link between sugary drinks and gout
Thursday, 12 September 2013
University of Otago and Auckland scientists have for the first time discovered a human gene
variant that can “turn bad” when affected by sugary drinks, raising the risk of developing the
common and debilitating arthritic disease gout.
Associate Professor Tony Merriman from the Department
of Biochemistry at the University of Otago says: “This
study shows that sugary drinks reverse the benefits of a
gene variant which would usually protect against gout.
The evidence is now even stronger against sugary drinks.”
Gout is caused by high levels of uric acid in the blood.
The acid crystallises in the joints and the painful inflammatory response is gout. It is the most
common form of arthritis in New Zealand, with particularly high rates in men; 3.7% in
European men, 11.7% in Māori men and 13.5% in Pacific men. The disease has strong links
with other 'metabolic' diseases such as diabetes, heart and kidney disease.
The study, which appeared today online in the international journal Annals of the Rheumatic
Diseases, shows that when the variant of the gene SLC2A9 behaves correctly, it helps
transport uric acid out of the blood stream and facilitates its excretion through the kidney.
“But when people with this gene variant consume sugary drinks, it takes on Jekyll and Hyde
characteristics; the apparent function of the gene variant reverses, such that we think uric acid
is instead transported back into the blood-stream and the risk of gout is increased.
“So, not only does sugar raise uric acid in the blood due to processing in the liver, but it also
appears to directly interfere with excretion of uric acid from the kidney. This was a quite
unpredictable interaction,” he says.
Arthritis Research Theme 2013 Report
6
US researchers studying gout have so far proven that high-fructose corn syrup sweetened soft
drinks increase the risk of gout for people of European ancestry. The second major finding of
the new Otago study was that consuming sugar-sweetened soft drinks also increases the risk
of gout in New Zealanders, including for Māori and Pacific people, independent of their
weight.
“Each daily 300ml serving of sugar-sweetened drink increases the chance of gout by 13%,”
Associate Professor Merriman says.
The Otago researchers examined blood samples to specifically focus on the SLC2A9 gene in
1634 people of European, Maori and Pacific ancestry recruited between 2007 and 2012.
Study participants were recruited mainly from Auckland and Christchurch, through hospitals,
community focal points, such as marae, and workplaces. A similar study was also done in
Tairawhiti (East Coast) in partnership with Ngati Porou Hauora.
Participants also answered a question about their sugar-sweetened soft drink and fruit juice
consumption, and medical information was collected to verify whether or not they had gout.
Within the sample, 5% of European, 14.4% of Māori and 16.6% of Pacific Island people were
drinking more than 1 litre of sugar-sweetened soft and/or fruit juice drink per day.
In the study done in Tairawhiti, the message about the importance of avoiding sugary soft
drinks and fruit juice was actively promoted from an early stage. This resulted in those
participants with gout drinking almost one serving less of these drinks per day compared to
others in New Zealand.
Dr Merriman says gout attacks can be prevented by the prescribed daily use of the medicine
allopurinol, which lowers the production of uric acid in the blood. As a result of the new
research, he further recommends that in addition to taking this medicine people with gout
should not drink any sugary drinks.
The research was funded by the Health Research Council of New Zealand and Arthritis New
Zealand.

Arthritis Research Theme 2013 Report
7
Crippling costs
Reprinted from the Otago Magazine Issue 35 June 2013
It is estimated that arthritis costs the New Zealand health-care system more than $700 million
each year. The University’s Arthritis Research Theme is bringing together researchers to help
find ways to improve the lives of the growing number of New Zealanders affected by this
condition.
Imagine not being able to dress yourself or to turn on a tap to
brush your teeth. Imagine waking daily to debilitating pain.
This is what life is like for many people affected by arthritis.
More than half-a-million New Zealanders suffer from one of a
wide range of conditions covered by the term “arthritis”,
including osteoarthritis, gout and ankylosing spondylitis.
While not all arthritis sufferers are elderly, as our population
ages the number of sufferers is increasing – as is the cost to
society. An economic study commissioned in 2010 by
Arthritis New Zealand found that the annual health-care costs
for arthritis conditions totalled almost $700 million.
Arthritis Research Theme 2013 Report
8
The prevalence of arthritis and its financial impact were two reasons the University of Otago
set up the Arthritis Research Theme in 2011. Other compelling reasons included an
impressive group of researchers already working on arthritis-related issues and a commitment
by the University to support research with impact. A University of Otago Research Theme
signals developing, or potential, research excellence in areas of strength within the
University.
Director, Christchurch-based Professor Lisa Stamp, says the establishment of the Arthritis
Research Theme is a constructive and practical development for people with arthritis. “It not
only highlights the significant amount of internationally-recognised research being done
across the University into all forms of arthritis, but also encourages further clinical research in
an area that affects so many New Zealanders and millions more worldwide.”
Researchers are working on providing answers to some of the key challenges faced by
doctors treating patients with arthritis. Their work spans genetic studies, assessing the risk of
developing rheumatic diseases such as rheumatoid arthritis, gout and spondyloarthritis;
pharmacogenomic studies, predicting responses to different drugs; through to basic science
laboratory studies of the pathophysiology of inflammatory arthritis. There are also a number
of clinical studies including the development of outcome measures and therapeutic clinical
trials.
Stamp says the ultimate aim of Theme members is to improve outcomes for those living with
the painful and crippling condition. “There is no cure for arthritis so a lot of our work focuses
on how to best treat people and ways to minimise their suffering.’’
Stamp’s own research interests include how to tailor drug treatments for rheumatic conditions
such as gout and rheumatoid arthritis (RA) for individual patients. One of her findings – that
doses of the standard gout drug, Allopurinol, could be safely lifted above existing clinical
guidelines to effectively manage the disease in some patients – has had a significant impact
on clinical practice. Another – showing that measuring blood levels of the commonly-used
drug Methotrexate in RA patients is not useful in telling how well the disease is being
controlled – has also been internationally influential.
Practical research outputs such as these are likely to increase as the Theme matures. Stamp
cites a study on smoking as an example of hands-on work already being undertaken.
“A laboratory-based project examining the effects of cigarette smoking on the inflammation
in the joints of RA patients has now been extended to a clinical study funded by the Health
Arthritis Research Theme 2013 Report
9
Research Council, investigating why RA patients find it difficult to stop smoking. In
collaboration with Arthritis New Zealand, we are piloting a smoke-stop programme
developed specifically for people with RA. The laboratory study indicated that an increase in
some inflammatory genes in the joint tissue of smokers returned to normal after the patient
stopped smoking, suggesting there may be direct benefits to quitting.’’
Other projects include studies looking at:
o the genetics of rheumatic diseases, involving patients from Auckland,
Wellington, Christchurch and Hamilton
o the success of folic acid supplementation in patients with rheumatoid arthritis
o high rates of Wegener’s granulomatosis in Canterbury, compared to rates in
the Northern Hemisphere
o the effect of vitamin C on gout
Dunedin-based Associate Professor Tony Merriman, whose work revolves around the
genetics of arthritis, believes one of the biggest benefits of the Theme is bringing together
researchers with different areas of expertise.
“A lot of the work by Theme members focuses on how to make life better for people with
arthritis. The genetics research is understanding what is causing it. Both these things are
important and complement each other perfectly. “Gene researchers have found that 60 to 70
per cent of the reason people either get rheumatoid arthritis, or not, is due to their genes. One
example is the CTLA4 gene, which has been found to be a factor in rheumatoid arthritis. This
gene is being targeted with a drug called Abatacept to prevent or alleviate the condition.
Genetics just gives us more information about what’s going on in the body.’’
Another benefit, says Merriman, is regular meetings, bringing together researchers from
University of Otago centres around the country. “I’m involved in an international study on the
relatively rare condition of giant cell arteritis. There’ve been very few genetic studies done on
it and, for gene studies, you need thousands of people. I did a presentation on this study at a
Theme meeting and lots of people there put their hands up and said ‘I’ll get involved’.
Because of that buy-in, New Zealand is now going to provide 500 of the 2,000 samples from
Australasia.’’
Merriman says he and Theme colleagues, including Stamp, are also involved in work on more
common arthritic conditions, such as gout. “In one gout study we are looking at how genes
Arthritis Research Theme 2013 Report
10
and the environment work together in that condition. Sugary drinks and alcohol raise uric acid
levels which lead to painful attacks. We’ve found that a particular gene is important in
helping the kidney get rid of uric acid.
“There are two versions of this gene, one good at getting rid of the acid and the other which is
not. Interestingly, we’ve found that if people have the good version of the gene but drink
more than a litre of sugary drink a day, they can reverse the effect of the good gene version.
It’s very practical stuff, as well as improving our understanding.’’
Merriman is a mid-career researcher who is getting recognition on the world stage for his
work. Likewise, Stamp has hit her career stride and has many years of productive work in
front of her, but there are researchers at all career stages involved in the Theme.
“Professor John Highton is a very senior researcher who has driven rheumatology research at
the University since the mid-’70s and has trained a number of the other Theme members,”
says Stamp.
“Rheumatology research at the University of Otago, and in New Zealand generally, has been
greatly strengthened in recent years by enthusiastic and productive mid- and early-career
researchers. These researchers are providing a foundation for the Theme to increase research
collaborations across departments and faculties within the University, including the strong
support of postgraduate student study.’’
Supporting early-career researchers is also a key focus, Stamp says. “Students are an integral
part of Theme activities. We have a number of students pursuing PhD and master’s thesis
research. Bachelor of Medical Science students are also involved. In addition, the Theme
completed its first year by sponsoring two summer students who under took a 10-week
arthritis-related research project.
“Student involvement is critical to the on-going success of the Theme. They are the next
generation of researchers and we need to stimulate interest and energy for them to continue in
finding answers to important questions about rheumatology.’’
KIM THOMAS

Arthritis Research Theme 2013 Report
11
New Otago research shows early Māori probably suffered from gout
Monday, 21 October 2013
Discoveries of early Māori skeletal remains showing tell-tale signs of gout have been
corroborated by new evidence that dispels the myth that the disease was largely an upper
class European affliction that did not affect any indigenous populations.
Researching historic newspapers and records of
missionaries, early physicians and accounts by Captain
James Cook and his crew, University of Otago PhD
student Anna Gosling has found suggestions that Māori
suffered from gout around the time of European
settlement.
However, European observers did not recognise the disease among Māori as being gout, often
referring to it in early reports of health as rheumatism, a term to describe general
inflammatory joint diseases.
"Most of the papers discussing gout in Māori talk about gout as if it is a disease primarily
related to transitions to modern lifestyles and the adoption of a westernised diet such as soft
drinks, alcohol and highly processed foods," she says.
"However, the archaeological evidence for gout found earlier at Wairau Bar, and then at
another prehistoric site from Mangere, Auckland, contradicts this. And in this review of early
literature, not only were we able to find suggestion of gout among Māori during the 19th
century in historic newspapers and other sources, but we have also put forward some ideas as
to why this idea of a lack of gout among Māori during this time has been perpetuated."
The paper, recently published in the journal Rheumatology, builds on the work of Otago
biological anthropologist Hallie Buckley and others, who reported skeletal evidence of gout
in the koiwi from Wairau Bar and examined prior to repatriation in 2009.
Arthritis Research Theme 2013 Report
12
Ms Gosling says gout had long been perceived as a disease of the aristocracy – a disease of
affluence and sumptuous lifestyles.
"The Europeans who were reporting on the presence of certain diseases among the Māori may
not have recognised the disease which the Māori were suffering as being gout because Māori
were not living lifestyles of luxury and excess as seen in the upper echelons of European
society at the time. This may be the basis for the high rate of ‘rheumatism’ being reported by
such observers," she says.
This study and the skeletal evidence shows that genetic factors play a significant role and are
likely to have meant that Māori had suffered from gout well before first European contact.
She believes there needs to be more awareness that gout is a disease which has affected Māori
and Pacific peoples since very early on – probably since before they first arrived on the
shores of New Zealand.
"While lifestyle, particularly diet, can contribute to the likelihood of developing gout, there is
also a genetic component, which seems particularly strong among Māori and Pacific
Islanders.
"This is something which both the clinicians, who treat gout, and the sufferers of gout, should
be aware of. There is a precedent which dates back hundreds, possibly thousands of years
(across the Pacific), for Māori and other Pacific peoples suffering gout. Given the importance
of ancestry among Māori and Pacific communities, the link with tupuna means that gout is
not just a result of how the patient is living, and an awareness of this may hopefully help
promote the message that effective modern drugs are available to prevent gout," says Ms
Gosling.
Arthritis Research Theme 2013 Report
13
Vitamin C does not alleviate gout as previously thought
Friday, 17 May 2013
Latest research from the University of Otago, Christchurch, has shown vitamin C does not
significantly lower uric acid levels in gout patients, despite previous studies touting its
benefit.
Professor Lisa Stamp and her colleagues found while vitamin C supplementation, alone or in
combination with gout drug allopurinol, appears to have a weak effect on lowering uric acid
levels in some gout patients, it does not reduce uric acid (urate) levels to a clinically
significant degree in patients with established gout.
The research is published in the latest edition of the American College of Rheumatology
(ACR) journal, Arthritis & Rheumatism.
Gout is an inflammatory arthritis that causes excruciating pain and swelling triggered by the
crystallization of uric acid within the joints. Medical evidence reports that long-term gout
management requires treatment with medications that lower urate levels by inhibiting uric
acid production (allopurinol) or increasing uric acid excretion (probenecid) through the
kidneys.
“While current treatments are successful in reducing the amount of uric acid in the blood,
there are many patients who fail to reach appropriate urate levels and need additional
therapies. Vitamin supplementation is one such alternative therapy and the focus of our
current study, which looked at the effects of vitamin C on urate levels in patients with gout,”
says Professor Stamp.
Her team recruited gout patients who had urate levels greater than the ACR treatment target
level of 0.36 mmol/L (6 mg/100 mL). Of the 40 participants with gout, 20 patients already
taking allopurinol were given an additional 500 mg dose of vitamin C daily or had the dose of
allopurinol increased, while another 20 patients not already taking allopurinol were either

Arthritis Research Theme 2013 Report
14
started on allopurinol or vitamin C (500 mg/day). Researchers analysed blood levels of
vitamin C (ascorbate), creatinine and uric acid at baseline and week eight.
Findings show a modest vitamin C dose for eight weeks did not lower urate levels to a
clinically significant degree in gout patients, but did increase ascorbate. The results differ
from previous research which found that vitamin C reduced urate levels in healthy individuals
without gout, but with high levels of uric acid (hyperuricaemia).
In fact, the Stamp et al. study found reduction of uric acid was significantly less in gout
patients taking vitamin C compared to those who started or increased their dose of
allopurinol.
Professor Stamps says: “though vitamin C may reduce risk of developing gout, our data does
not support using vitamin C as a therapy to lower uric acid levels in patients with established
gout. Further investigation of the urate lowering effects of a larger vitamin C dose in those
with gout is warranted.”
Osteoarthritis improved by extra physiotherapy programmes
Wednesday, 24 July 2013
Manual physiotherapy or regular exercise programmes make a significant difference for
people with painful osteoarthritis in the knee and hip joints, and are cost-effective, new
research from the University of Otago shows.
The randomised clinical trial involved 207 Dunedin
patients over one year and used three protocols of
treatment provided by physiotherapists in addition to
usual care by their GP.
One group was given seven manual physiotherapy
sessions, in addition to usual care, for 40-50 minutes
over nine weeks, followed by two boosters after a further seven weeks. The second group
Arthritis Research Theme 2013 Report
15
involved a programme of exercise both in the clinic and at home, while the third group was
treated with a combination of manual and exercise therapy. A control group received only
usual care from their GP or other health providers.
Lead researcher Associate Professor Haxby Abbott of the Centre for Musculoskeletal
Outcomes Research says that the results show that individually supervised exercise therapy or
manual therapy provided by a physiotherapist, in addition to usual care, improve pain and
physical function for at least one year.
“However, given a time constraint of a 40-50 minute clinic visit, there is no additional benefit
gained from providing both manual and exercise therapy on top of usual care for
osteoarthritis,” Associate Professor Abbott says.
A further study, published this week in the international journal Osteoarthritis and Cartilage,
looked at the economics of the additional treatment in this trial. It found that both additional
exercise therapy and manual therapy are more cost effective for the health system and for
individuals than just applying usual care management to osteoarthritis.
“Exercise therapy provided the best cost-effectiveness from a health system perspective,
while manual therapy was best, and was actually cost-saving, from a societal perspective,” he
says.
“On our main measure, we found that additional manual therapy provided the best symptom
relief of the three treatments we studied. On the other hand, the exercise programme also
produced very good results on physical tests and on quality of life gains. So each has its
strengths, there is no clear best choice for everyone. What’s clear is that either is better than
usual care only.”
The researchers conclude at present there is quite low use of non-surgical and non-drug
therapies for osteoarthritis in primary care, and these studies point to a way of preventing or
delaying pain and disability at significant cost effectiveness for society and the health system.
“These results suggest that GPs should refer patients with hip or knee arthritis for individually
supervised exercise or manual therapy provided by a physiotherapist, in addition to
continuing to provide usual care.”
The researchers say the Management of Osteoarthritis trial demonstrates for the first time the
value of individually prescribed and supervised programmes involving manual care or
exercise in relieving symptoms of hip or knee osteoarthritis.
Arthritis Research Theme 2013 Report
16
The exercise programme involved stationary cycling, muscle strengthening, stretching and
balance and agility exercises both in the clinic and at home.
Both the Management of Osteoarthritis trial and the economic evaluation have been published
in the international journal Osteoarthritis and Cartilage.
The studies were funded by the Health Research Council of New Zealand and the Lottery
Grants Board.
Footwear and knee injuries being studied By Tim Miller on Sun, 3 Nov 2013 Otago Daily Times
Knee injuries plague professional athletes and weekend battlers alike and a study by
researchers at the University of Otago is looking at the reason behind all the weak knees.
Department of Physiotherapy lecturer Gisela Sole said
knee injuries were very common in many sports, such as
netball, football, and rugby.
Knee injuries often resulted in the sportsperson not
being able to return to the same level of achievement
and could increase the risk for knee arthritis later on, Dr
Sole said.
Statistics from ACC show there were more than 4400
claims for knee injuries from playing sport in the Otago
region from June, 2012 to June, 2013. These claims cost
more than $5 million.
Dr Sole is leading a study which focuses on whether the
type of footwear people wear has an effect on knee injuries.
''Past studies have focused mainly on issues such as muscle strength, balance and co-
ordination, and exercise programmes . . . What has been overlooked in the past, is that
footwear may also have an influence on the knee movements,'' she said.
Volunteers were needed to help with the study and the researchers were looking for females
aged between 18 and 35 who take part in a land-based sport at least twice a week.
Woman had a higher risk of non-contact knee injuries than men, which was why the study
would focus on them, she said.
Arthritis Research Theme 2013 Report
17
As part of the study, volunteers will wear shoes with special inserts. Their movements will be
followed by infrared cameras tracking markers placed on the subject.
The movement will show how the knee is affected when landing from a 20cm drop.
Anyone interested in taking part in the study can contact Dr Gisela Sole, by emailing
[email protected], or by phoning 479-7936.
Juicy bits Theme members’ contributions to ‘Juice”, now re-named “Joint Support”, the Arthritis NZ Members News Letter
Smoking and Rheumatoid arthritis Dr Paul Hessian, Senior Research Fellow. Department of Medicine, University of Otago
Arthritis NZ The Juice Member’s Newsletter | March 2013
Epidemiological studies investigating the patterns and causes of
rheumatoid arthritis (RA) have established cigarette smoking as an
important environmental risk factor for developing RA. There is
also evidence that smoking increases the severity of RA once the
disease is established. Part of the explanation for smoking’s effect
is now clear. Smoking causes the modification of certain proteins
[a process known as citrullination]. In patients with a particular
genetic makeup, this induces immunity to the modified proteins and eventually the onset of
RA. It is easy to say that that is all the evidence required and the informed decision is “Stop
smoking reduce the risk or the severity”. However there is still more to be gained from an in-
depth understanding of smoking’s effect. Not all those who smoke develop RA, even if they
have the “right” genetic makeup; and immunity to modified/citrullinated proteins can occur
completely independent of genetic makeup. These anomalies indicate that other factors
influence the effects of smoking and modulate the development of RA.
Our recent research has investigated the effect of smoking on joint synovial tissue, a hotspot
for the inflammation associated with RA. Dendritic cells (DCs) are very important cells in the
immune system, normally tasked with surveillance and response to infection. There is also a
critical role for these cells in diseases like RA. Our work shows that a subgroup of the DCs in
joint tissue are extremely sensitive to at least one of the chemical compounds found in
cigarette smoke, a polycyclic aromatic hydrocarbon. In patients that were smokers, smoke

Arthritis Research Theme 2013 Report
18
exposure activates the aryl hydrocarbon receptor transcription factor system in DCs,
ultimately turning on and off other genes. One consequence is reduced production of a key
inflammatory mediator, intereleukin-6, used by DCs for signalling to the immune system.
There is more to work out about the consequences of DCs responding to cigarette smoke.
However a very practical outcome is that in RA patients who have quit smoking, this effect
on the synovial DCs is rapidly lost. So while the work does not yet explain the lasting effect
of smoking on increasing the risk of getting RA, it does show that stopping smoking will have
some immediate impact on inflammation in the very tissues targeted by rheumatoid
inflammation. That has to have some additional benefit for patients.
The work has been part of a PhD thesis investigation by Dr Marina Kazantseva completed in
collaboration with Professor Lisa Stamp (Christchurch) and Professor John Highton
(Dunedin)
Complementary and alternative medicine – what does your doctor think? Dr Rebecca Grainger University of Otago Wellington
Arthritis NZ The Juice Member’s Newsletter | September 2013
Most shopping malls have a “health store” that sells a wide variety
of tablets, supplements or creams with supposed health benefits.
Your neighbour swears by her chiropractor for her back pain.
Remedies for joint pain are advertised in magazines. All these are
examples of “Complementary and alternative medicines” or CAM.
CAM includes a wide variety of health care approaches with a
history of use or origins outside of mainstream medicine. There are
two broad subgroups of CAM; natural products and mind and body
therapies. Natural products include herbs, vitamins, mineral and supplements. These are
often marketed directly to the public. Mind and body practices are usually administered or
taught by a practitioner and include yoga, massage, acupuncture, meditation, movement
practices (Feldenkrais method, Pilates) and manipulation therapy (chiropractic, osteopathy).
Some practices do not fit neatly into either of these broad groups and include ayurvedic
medicine, traditional chinese medicine, homeopathy and naturopathy. Needless to say there
are a bewildering number of CAM practices available in our communities.
People with musculoskeletal disorders and arthritis are amongst the highest users of CAM
with international and New Zealand data suggesting that up to 40% of people with arthritis
Arthritis Research Theme 2013 Report
19
use CAM at some time. Perhaps this is because many musculoskeletal disorders are chronic
and conventional medical practices cannot relieve all symptoms. Many people do not tell
their doctors that they use CAM. In studies patients report that they do not tell because they
are not asked, consider that there is no reason for a doctor to know, or they fear disapproval.
But do doctors disapprove of CAM use by their patients? The international data suggests that
some doctors hold positive attitudes to CAM but what do Rheumatologists in New Zealand
think about CAM?
We surveyed all 58 practising rheumatologists in New Zealand and heard back from 36
(62%). We asked about six categories of CAM relevant to people with arthritis - Spinal
manipulation (e.g. chiropractic), Acupuncture, Energy medicine (e.g. reiki), Meditation
practices (e.g. Yoga), Glucosamine +/- Chondroitin, and Body work (e.g. Massage, Shiatsu).
We asked Rheumatologists about their familiarity with, the benefit of and likelihood of
recommendation of each of these groups of CAM.
About half of the Rheumatologists responding reported that they were familiar with
Glucosamine, acupuncture, spinal manipulation, meditation practices however most were not
familiar with Energy Medicine. This means that many Rheumatologists feel they are NOT
familiar with CAM therapies and this may be one reason why Rheumatologists do not ask
their patients about CAM therapies. There are now a number of free on-line resources where
up to date, scientifically valid information about CAM therapies can be accessed. These
include the National Centre for Complementary and Alternative Medicine
(www.nccam.nih.gov) and the Cochrane Library (www.cochrane.org). Next time you are
thinking about trying a CAM therapy, do some research and discuss this with your doctor.
Perhaps your doctor can use this chance to learn something too.
For most therapy types the proportion of Rheumatologists who would recommend a CAM
therapy to patients was very similar to proportion that believed the therapy to be beneficial.
For example Meditation practices were believed to be the beneficial by about two-thirds of
Rheumatologists and were recommended to patients by two–thirds of Rheumatologists. If
CAM works, Rheumatologists seem to suggest patients use it.
The majority of Rheumatologists reported that Glucosamine/Chondroitin therapy was not
beneficial for people with joint problems. Interestingly almost 70% of Rheumatologists had
previously recommended Glucosamine +/- Chondroitin treatment to their patients. Why is
there this discrepancy? The first studies of Glucosamine for the pain of knee osteoarthritis
Arthritis Research Theme 2013 Report
20
found that patients taking glucosamine or a placebo tablet both had improvements in pain and
function, with patients taking glucosamine doing a little better than patients taking placebo.
These studies had some problems – they were small, used one brand of glucosamine – and the
extra benefit for glucosamine was only just above what patients feel is a measureable benefit.
Subsequent larger, better-designed trials did not find any benefit for glucosamine over
placebo. More recently a special type of analysis that puts together all the studies of
glucosamine in osteoarthritis and measures the benefits has concluded that the benefits of
taking glucosamine for symptoms of knee osteoarthritis are not bigger than the benefits of
taking a placebo. In short, Glucosamine doesn't work. The results of our study suggest that
Rheumatologists in New Zealand do keep up to date with new research and change their
practices accordingly.
One of the major challenges for all doctors when considering where CAM therapies may fit
into medical care is the lack of robust research testing if CAM therapies actually work and are
safe. Many CAM therapies have not been tested in this way. Arthritis New Zealand has
recognized this and research into CAM therapies for arthritis is one of the key targets for
research funding from Arthritis New Zealand. Hopefully these studies will help doctors and
patients make informed decisions about CAM therapies.
Living with dry mouth
Anita Nolan Professor of Oral Medicine and Head of Oral Health, AUT University, Auckland
Arthritis NZ The Juice Member’s Newsletter | June 2013
Saliva plays a huge role in the health and comfort of mouths. It rinses
and moistens the mouth, initiates food digestion and prevents disease
of the teeth and the lining of the mouth (oral mucosa). The sensation
of a dry mouth (xerostomia) occurs when the amount of saliva in the
mouth is too little or its composition is altered. For many people with
autoimmune arthritis, dry mouth is a common problem. In most cases
there needs to be a 50% reduction in salivary production before it
becomes noticeable. Unfortunately, at that stage, some damage to the
mouth and teeth may have already occurred.
The single greatest cause of a reduction in salivary flow is medication. More than 1800 drugs
have been reported to cause dry mouth and these include antihistamines, blood pressure
medication and sedatives. Auto-immune diseases that are associated with dry mouth include
Arthritis Research Theme 2013 Report
21
rheumatoid arthritis, systemic lupus erythematosus, systemic sclerosis, mixed connective
disease and, most notably, Sjogren’s syndrome. Sjogren’s syndrome, also known as “Sicca
syndrome” is an autoimmune condition where immune cells attack the glands that produce
both saliva and tears, leading to severe and uncomfortable dry mouth and eyes.
Dry mouth can manifest in a number of ways. This can be a sensation of dryness, change in
taste, difficulty eating and swallowing and swelling of salivary glands due to infections and
blockages. One of the most detrimental effects of dry mouth is its effect on tooth decay. A
study in Europe showed that 62% of people with Sjogren’s syndrome had devastating tooth
loss compared with 20% of age and sex-matched people who did not have the condition. It
was noted that 66% of these patients with Sjogren’s syndrome had lost their teeth before the
age of 45 years compared with just 10% of the control population.
Dry mouth has been described as “a neglected symptom”. It remains undiagnosed and,
therefore, untreated in about half of patients. With respect to Sjogren’s syndrome, potential
barriers to appropriate diagnosis and treatment include the diverse symptomatology and
presentations of the condition, a lack of awareness of the condition and a perception that the
condition is mild and that therapy is either not available or necessary. A recent study in the
Otago region demonstrated that dentists, medical GPs and pharmacists all reported a lack of
knowledge of dry mouth management and did not feel confident to treat patients with this
disorder.
Pilot research is currently being undertaken to quantify the level of decayed, missing and
filled teeth in New Zealand people with Sjogren’s Syndrome. Preliminary results suggest that
early and excessive tooth loss is, like in Europe, a feature of the condition in New Zealand.
This research will help to plan the management of oral health needs for peoplewith dry mouth
in the future.
There have been numerous studies that have shown that the dry mouth associated with
Sjogren’s syndrome negatively affects their quality of life. However, to date, research has
consisted mainly of pre-determined questions, criteria and scores. It is increasingly
recognised that questionnaires may not be able to describe what patients actually experience
in their daily battle with chronic dry mouth. It is essential that clinicians gain a greater
understanding of the daily challenges faced by sufferers to enable them to manage this
chronic condition effectively. For this reason, a study is being conducted in New Zealand in
which participants describe daily events and reflections they perceive to be linked to dry

Arthritis Research Theme 2013 Report
22
mouth. Their observations are recorded in a daily diary (recorded for a month) and in an
interview. The analysed data will provide an evidence-related, personal-experience-based
conceptual framework of the impact of dry mouth on the psychological, physical, social,
financial aspects of Sjogren’s syndrome sufferers’ lives, together with any other, as-yet-
unknown aspects. To date themes that have emerged are the lengthy journey to getting a
diagnosis and the impact of the condition on dietary choice, sleep, social and family life and
work. It is clear from this research that clinicians have much to learn from those who live
with a chronic dry mouth.
Finally, for those who suffer from dry mouth, the European Association of Oral Medicine
recommends that you visit your dental hygienist and dentist regularly. You should try to
avoid food and drinks that are sweet, carbonated or acidic. Ensure that any lozenges, mints or
chewing gums you use are sugar free. The use of fluoride rich gels and tooth pastes will help
protect your teeth. Saliva substitute gels will help to lubricate your mouth at night and
between meals. Drink plenty of water at meals and throughout the day. Smoking and
excessive consumption of alcohol, as well as inadequate fluid intake, can worsen dry mouth.
Soft Tissue X-rays in Scleroderma Professor John Highton, Department of Medicine, University of Otago
Arthritis NZ The Juice Member’s Newsletter | December 2013
For Rheumatologists it has been gratifying to experience recent progress
in treating Rheumatic diseases. Patients in NZ definitely have more
options for effective treatment in the 21st century. In order to provide
good treatment it is not only necessary to have effective medicines but
also to have good measures of disease progression so that the impact of
treatment can be measured. Treatment can then be given, and adjusted if
there is insufficient impact on the relevant disease measurements. For Rheumatoid arthritis
this approach has been characterised as “Treat to Target”. Despite recent progress there are
still many challenges. One of these is to find ways of improving treatment for patients with
Scleroderma. This will require not only better medicines but also better ways of measuring
the progress of this unpleasant condition.
In Scleroderma there is an autoimmune attack on blood vessels and fibrosis that is most
obvious in the skin. In the hands this results in compromise of the blood flow to the fingers.
Patients find that they get Raynaud’s phenomenon where the fingers become white and
Arthritis Research Theme 2013 Report
23
bloodless on exposure to cold. Sometimes this is accompanied by damage to the tissues in
the fingers. The fibrotic element of Scleroderma results in thickening and tightening of the
skin restricting movement of the fingers. In some cases deposits of calcium can form under
the skin. The net result is changes that can be seen quite easily but the challenge is how to
measure these changes.
We have previously looked at which measurements in the hand can be used to track changes
in shape and movement due to diseases like Rheumatoid Arthritis and Scleroderma. We
devised a hand anatomic index comprised of simple measurements that could be made with
callipers and a tape measure. Together with my colleague Prof Peter Roberts-Thomson in
Adelaide, and his daughter Alice, an occupational therapist, we were able to show that the
hand index could show significant differences in the hands of patients with the limited form
of Scleroderma compared to the more general form of the disease.
More recently we have investigated the use of X-rays to visualise the changes that
Scleroderma causes in hands. Plain X-rays are able to show some of the changes. However,
conventional X-rays are best at showing bones and we were looking for a method that is
better at visualising soft tissues like skin. Professor Doyle from our Radiology Department
suggested that such a method is in fact widely available as the X-rays used in mammography
for breast cancer screening are adapted for visualising changes in the soft tissues. We
therefore undertook a study to see if the use of digital mammographic X-rays would show
more changes in the fingers of patients with Scleroderma.
At the recent NZRA meeting in Hamilton we presented the findings in the first 20 patients
studied with this somewhat novel application of mammographic X-rays. We were able to
demonstrate that this method is more sensitive for picking up early calcification of tissues. It
is also sufficiently sensitive to show the thickness of the skin that can also be measured from
the images displayed on the computer monitor. We were a bit surprised to be able to see the
internal structure of the finger pulps that contain a framework of connective tissue partitions
that also appear to be thickened, another change that would contribute to tethering of the skin
and immobility of the tissues.
We have been interested to see that the use of X-rays designed specifically to visualise soft
tissues can show greater detail of the changes in fingers due to Scleroderma. We think that
there is some potential for using this method to develop a scoring system to measure the
Arthritis Research Theme 2013 Report
24
changes that occur progressively in Scleroderma and bring us closer to being able to
determine which treatments may have an impact on the disease.
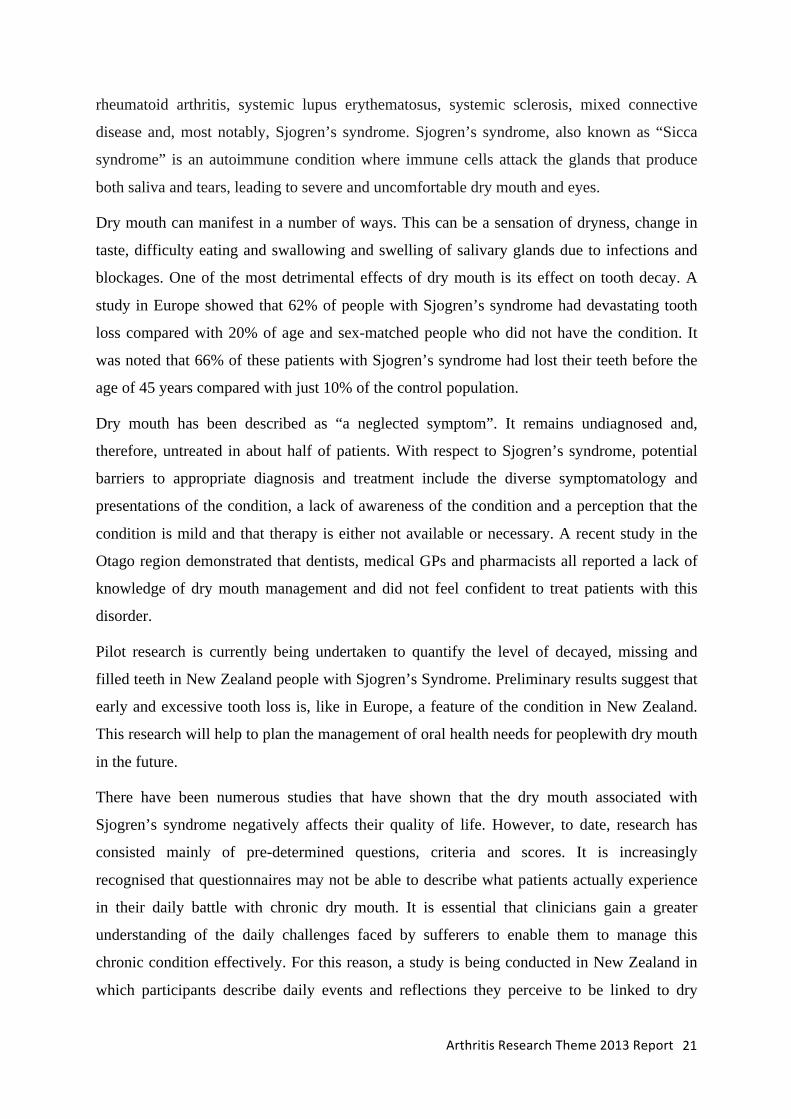
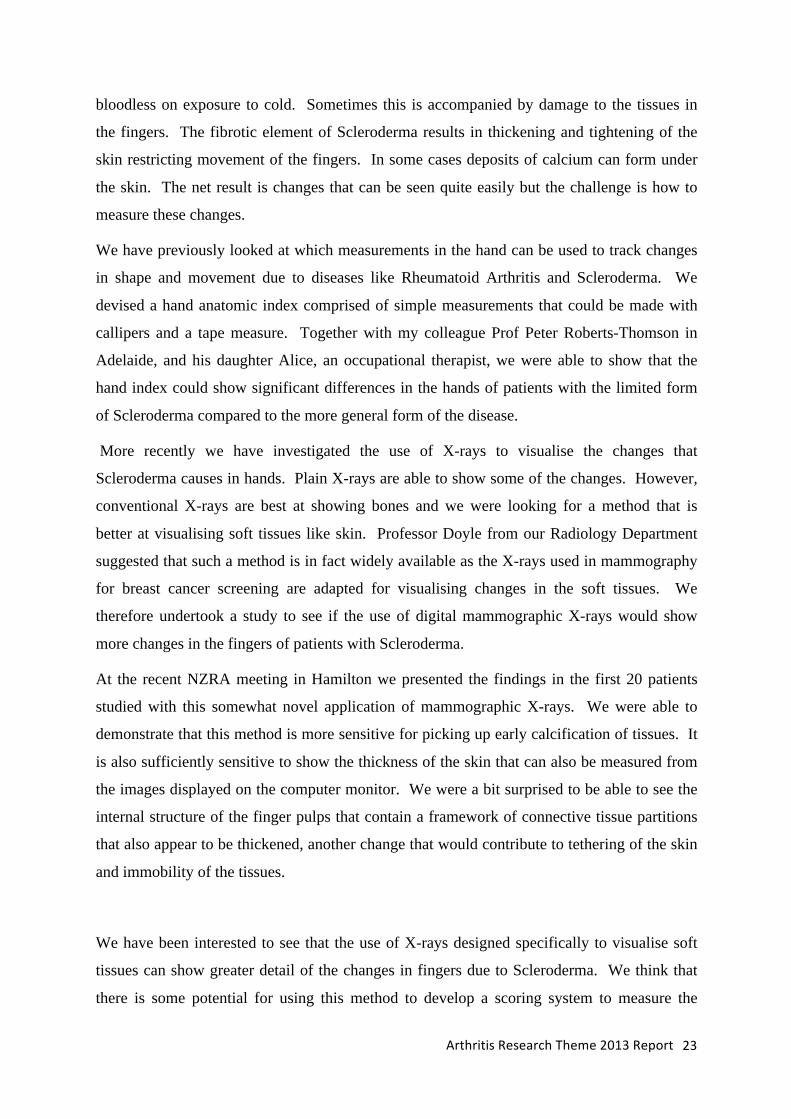
The left picture is the middle finger from a patient with Scleroderma. The right picture by
comparison shows normal appearances. In the left picture there is loss of tissue from the
finger tip, calcium in the tissues and thickening of the skin and internal fibrous structure of
the finger.
Meetings
Thursday May 1st 2013 1000 – 1600 Auditorium, Toitu, Otago Settlers Museum
Guest Speaker: Professor Ric Day
Richard Day is Professor of Clinical Pharmacology at UNSW and St
Vincent's Hospital Sydney. He has a clinical practice in Clinical
Pharmacology, Clinical Toxicology, and Rheumatology. He has
particular interests in promoting the quality of use of medicines
(QUM). He was chair of PHARM for the Federal Government of
Australia 1999-08, was a Director and President of the DIA (2009-
11), was co-chair of the Medication Safety Taskforce for the
Australian Safety and Quality Council, is chair of NSW Medication
Safety Expert Advisory Committee, was chair of the NPS (National Prescribing Service)
R&D committee (2008-10) and is co-chair of the electronic medication management
reference committee for the National e-Health Transition Authority. He is the senior
academic advisor to the Masters in Medical Science in Drug Development in the Faculty of
Arthritis Research Theme 2013 Report
25
Medicine at UNSW. This distance education programme is dedicated to excellence in
medicines and device development. His research focuses upon QUM and the
pharmacotherapy of gout, diabetes, infectious and psychotic diseases. He is also researching
methods of enhancing the safe use of medicines using electronic medication management and
decision support tools as one of six Chief Investigators on NH&MRC Programme Grants
(2009-13) (2014-2018).
Meeting Attendees (May 2013) * indicates student
University of Otago, Christchurch
Medicine Janine Francis, Jill Drake, Lisa Stamp, Murray Barclay, Pip Aimer*, Caitlin Batt*, Nicole Coman-Wright*
University of Otago, Dunedin
Medicine John Highton, Paul Hessian, Debra McNamarra, Anna Wiles, Mary Wallace, Tony Poole, T Ing-aram*
Biochemistry Tony Merriman, Mansour Zamanpoor*, Humaira Rasheed*, Tanya Flynn*, Mandy Phipps-Green, Ruth Topless, Vidyaliny Yugaraja, Murray Cadzow, Marilyn Merriman
Pharmacy Dan Wright, Shan Pan*, Vittal Shivva*, Stephen Duffull, Ashishek Gulati*, Cury Ribeiro Daniel*
Physiotherapy David Baxter, Cathy Chapple, Mari Ramakrishnan, Susan Baxter*
Psychology Gareth Treharne, Lesley Ward*, Jessica Leov* Physiology Andrew Bahn, Claudia Knake* University of Otago, Wellington
Medicine Rebecca Grainger,
Arthritis NZ Natalia Valentino, David Cox
Arthritis Research Theme 2013 Report
26
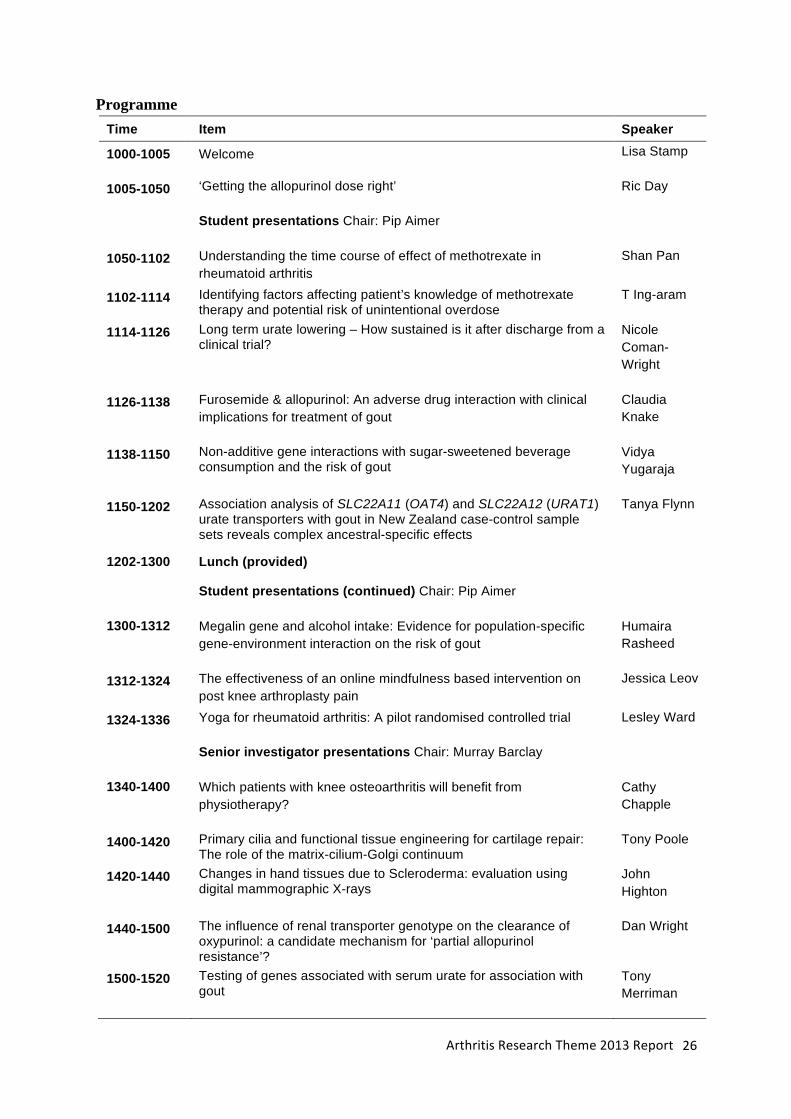
Programme Time Item Speaker
1000-1005 Welcome Lisa Stamp
1005-1050 ‘Getting the allopurinol dose right’ Ric Day
Student presentations Chair: Pip Aimer
1050-1102 Understanding the time course of effect of methotrexate in rheumatoid arthritis
Shan Pan
1102-1114 Identifying factors affecting patient’s knowledge of methotrexate therapy and potential risk of unintentional overdose
T Ing-aram
1114-1126 Long term urate lowering – How sustained is it after discharge from a clinical trial?
Nicole Coman-Wright
1126-1138 Furosemide & allopurinol: An adverse drug interaction with clinical implications for treatment of gout
Claudia Knake
1138-1150 Non-additive gene interactions with sugar-sweetened beverage consumption and the risk of gout
Vidya Yugaraja
1150-1202 Association analysis of SLC22A11 (OAT4) and SLC22A12 (URAT1) urate transporters with gout in New Zealand case-control sample sets reveals complex ancestral-specific effects
Tanya Flynn
1202-1300 Lunch (provided)
Student presentations (continued) Chair: Pip Aimer
1300-1312 Megalin gene and alcohol intake: Evidence for population-specific gene-environment interaction on the risk of gout
Humaira Rasheed
1312-1324 The effectiveness of an online mindfulness based intervention on post knee arthroplasty pain
Jessica Leov
1324-1336 Yoga for rheumatoid arthritis: A pilot randomised controlled trial Lesley Ward
Senior investigator presentations Chair: Murray Barclay
1340-1400 Which patients with knee osteoarthritis will benefit from physiotherapy?
Cathy Chapple
1400-1420 Primary cilia and functional tissue engineering for cartilage repair: The role of the matrix-cilium-Golgi continuum
Tony Poole
1420-1440 Changes in hand tissues due to Scleroderma: evaluation using digital mammographic X-rays
John Highton
1440-1500 The influence of renal transporter genotype on the clearance of oxypurinol: a candidate mechanism for ‘partial allopurinol resistance’?
Dan Wright
1500-1520 Testing of genes associated with serum urate for association with gout
Tony Merriman
Arthritis Research Theme 2013 Report
27
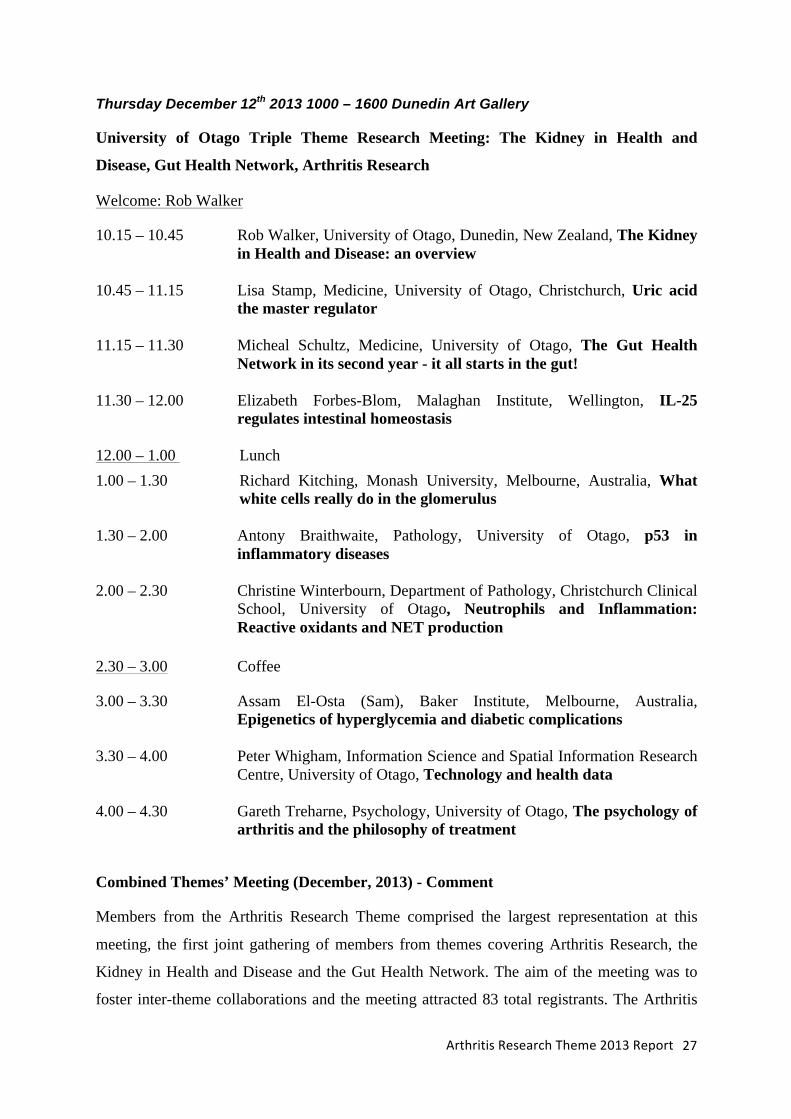
Thursday December 12th 2013 1000 – 1600 Dunedin Art Gallery
University of Otago Triple Theme Research Meeting: The Kidney in Health and
Disease, Gut Health Network, Arthritis Research
Welcome: Rob Walker
10.15 – 10.45 Rob Walker, University of Otago, Dunedin, New Zealand, The Kidney in Health and Disease: an overview
10.45 – 11.15 Lisa Stamp, Medicine, University of Otago, Christchurch, Uric acid
the master regulator 11.15 – 11.30 Micheal Schultz, Medicine, University of Otago, The Gut Health
Network in its second year - it all starts in the gut! 11.30 – 12.00 Elizabeth Forbes-Blom, Malaghan Institute, Wellington, IL-25
regulates intestinal homeostasis 12.00 – 1.00 Lunch 1.00 – 1.30 Richard Kitching, Monash University, Melbourne, Australia, What white cells really do in the glomerulus 1.30 – 2.00 Antony Braithwaite, Pathology, University of Otago, p53 in
inflammatory diseases 2.00 – 2.30 Christine Winterbourn, Department of Pathology, Christchurch Clinical
School, University of Otago, Neutrophils and Inflammation: Reactive oxidants and NET production
2.30 – 3.00 Coffee
3.00 – 3.30 Assam El-Osta (Sam), Baker Institute, Melbourne, Australia, Epigenetics of hyperglycemia and diabetic complications
3.30 – 4.00 Peter Whigham, Information Science and Spatial Information Research
Centre, University of Otago, Technology and health data 4.00 – 4.30 Gareth Treharne, Psychology, University of Otago, The psychology of
arthritis and the philosophy of treatment
Combined Themes’ Meeting (December, 2013) - Comment
Members from the Arthritis Research Theme comprised the largest representation at this
meeting, the first joint gathering of members from themes covering Arthritis Research, the
Kidney in Health and Disease and the Gut Health Network. The aim of the meeting was to
foster inter-theme collaborations and the meeting attracted 83 total registrants. The Arthritis
Arthritis Research Theme 2013 Report
28
Research Theme invited Professor Antony Braithwaite (Pathology) to speak on his work with
the p53 protein and provide background to a p53-arthrits-related project for which funding is
being sought. Also on behalf of the theme, Professor Lisa Stamp presented on Uric acid as a
master regulator of inflammation in gout while Dr Gareth Treharne gave his insight into the
psychology of arthritis and the philosophy of treatment.
Conference Presentations Members from the Arthritis Research Theme were present at and presented at the major local
and international Rheumatology meetings
American College of Rheumatology Annual Scientific Meeting San Diego
Australian Rheumatology Association Annual Scientific Meeting, Perth
Asia Pacific League of Associations of Rheumatology Annual Scientific Meeting Bali
International Society of Critical Health Psychology (ISCHP) 8th Biennial Conference
New Zealand Rheumatology Association Annual Scientific Meeting Hamilton
British Society for Rheumatology: Annual Conference ICC Birmingham UK
Symposium on Yoga Therapy and Research, Boston, USA
Symposium on Yoga Research, Boston, USA
PhysioForward Conference, Dunedin, New Zealand
2013 publications Abbott, J. H., Robertson, M. C., Chapple, C., Pinto, D., Wright, A. A., Leon de la Barra, S., Baxter, G. D., Theis, J.-C., Campbell, A. J., on behalf of the MOA Trial Team. (2013). Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee: A randomized controlled trial. 1: Clinical effectiveness. Osteoarthritis & Cartilage, 21(4), 525-534.
Abbott, J. H., Foster, M., Hamilton, L., Ravenwood, M., & Tan, N. (2013). Validity of pain drawings for predicting psychological status outcome in patients with recurrent or chronic low back pain. Journal of Manual & Manipulative Therapy. Advance online publication. doi: 10.1179/2042618613Y.0000000046
Anderson-Lister, G., & Treharne, G. J. (2013). 'Healthy' individuals' perceptions of type 1 and type 2 diabetes cause and management: A ‘think-aloud,’ mixed-methods study using video-based vignettes. Journal of Health Psychology. Advance online publication. doi: 10.1177/1359105313490315
Arthritis Research Theme 2013 Report
29
Batt, C., Phipps-Green, A. J., Black, M. A., Cadzow, M., Merriman, M. E., Topless, R., … Harrison, A., Highton, J., … Stamp, L., … Merriman, T. R. (2013). Sugar-sweetened beverage consumption: A risk factor for prevalent gout with SLC2A9 genotype-specific effects on serum urate and risk of gout. Annals of the Rheumatic Diseases. Advance online publication. doi: 10.1136/annrheumdis-2013-203600 Brown, M., Levack, W., McPherson, K. M., Dean, S. G., Reed, K., Weatherall, M., & Taylor, W. J. (2013). Survival, momentum, and things that make me "me": Patients' perceptions of goal setting after stroke. Disability & Rehabilitation. Advance online publication. doi: 10.3109/09638288.2013.825653 Campbell, A., Hocking, C., & Taylor, W. J. (2013). The experience of having psoriasis through the lens of the International Classification of Functioning, Disability and Health (ICF). Australasian Journal of Dermatology. Advance online publication. doi: 10.1111/ajd.12103 Chin, P. K. L., Vella-Brincat, J. W. A., Walker, S. L., Barclay, M. L., & Begg, E. J. (2013). Dosing of dabigatran etexilate in relation to renal function and drug interactions at a tertiary hospital. Internal Medicine Journal. Advance online publication. doi: 10.1111/imj.12170
Chin PK, Barclay ML, Begg EJ. Rifampicin and dabigatran etexilate: a place for laboratory coagulation monitoring. British Journal of Clinical Pharmacology 2013; 75(2): 554-5.
Clay, L., Treharne, G. J., Hay-Smith, E. J. C., & Milosavljevic, S. (2013). Is workplace satisfaction associated with self-reported quad bike loss of control events among farm workers in New Zealand? Applied Ergonomics. Advance online publication. doi: 10.1016/j.apergo.2013.07.003
Cury Ribeiro, D., Sole, G., Abbott, J. H., & Milosavljevic, S. (2013). Validity and reliability of the Spineangel® lumbo-pelvic postural monitor. Ergonomics. Advance online publication. doi: 10.1080/00140139.2013.781233 Dalbeth, N., Fransen, J., Jansen, T. L., Neogi, T., Schumacher, H. R., & Taylor, W. J. (2013). New classification criteria for gout: A framework for progress. Rheumatology. Advance online publication. doi: 10.1093/rheumatology/ket154
Dalbeth, N., House, M. E., Horne, A., Te Karu, L., Petrie, K. J., McQueen, F. M., & Taylor, W. J. (2013). The experience and impact of gout in Māori and Pacific people: A prospective observational study. Clinical Rheumatology, 32(2), 247-251. Dalbeth, N., House, M. E., Gamble, G. D., Home, A., Pool, B., Purvis, L., … Merriman, M., Cadzow, M., Phipps-Green, A., Merriman, T. R. (2013). Population-specific influence of SLC2A9 genotype on the acute hyperuricaemic response to a fructose load. Annals of the Rheumatic Diseases, 72(11), 1868-1873. Dalbeth, N., House, M. E., Gamble, G. D., Home, A., Purvis, L., Stewart, A., Merriman, M., Cadzow, M., Phipps-Green, A., Merriman, T. (2013). Population-specific effects of SLC17A1 genotype on serum urate concentrations and renal excretion of uric acid during a fructose load. Annals of the Rheumatic Diseases. Advance online publication. doi: 10.1136/annrheumdis-2013-203767
Darlow, B., Dowell, A., Baxter, G. D., Mathieson, F., Perry, M., & Dean, S. (2013). The enduring impact of what clinicians say to people with low back pain. Annals of Family Medicine, 11(6), 527-534. Dimitroulas, T., Douglas, K. M. J., Panoulas, V. F., Toms, T., Smith, J. P., Treharne, G. J., … Kitas, G. D. (2013). Derangement of hemostasis in rheumatoid arthritis: Association
Arthritis Research Theme 2013 Report
30
with demographic, inflammatory and metabolic factors. Clinical Rheumatology. Advance online publication. doi: 10.1007/s10067-013-2283-6
Dobson, F., Hinman, R. S., Roos, E. M., Abbott, J. H., Stratford, P., Davis, A. M., … Hansen, P., Bennell, K. L. (2013). OARSI recommended performance-based tests to assess physical function in people diagnosed with hip or knee osteoarthritis. Osteoarthritis & Cartilage, 21(8), 1042-1052.
Doecke, J. D., Simms, L. A., Zhao, Z. Z., Huang, N., Hanigan, K., Krishnaprasad, K., Roberts, R. L., … Gearry, R. B., … Radford-Smith, G. L. (2013). Genetic susceptibility in IBD: Overlap between ulcerative colitis and Crohn's disease. Inflammatory Bowel Diseases. Advance online publication. doi: 10.1097/MIB.0b013e3182810041
Duffull, S. B., & Isbister, G. K. (2013). Predicting the requirement for N-acetylcysteine in paracetamol poisoning from reported dose. Clinical Toxicology. Advance online publication. doi: 10.3109/15563650.2013.830733 Duffull, S. B., & Wright, D. F. B. (2013). What do we learn from repeated population analyses? British Journal of Clinical Pharmacology. Advance online publication. doi: 10.1111/bcp.12233
Dyke J, Hendry K, Hill J, Schultz M, Mason E, Glue P. Management of a Cluster of Foreign Body Ingestion Incidents in Patients with Borderline Personality Disorder. Open J Psychiatry 2013 (in press) Falvey, J. D., Bentley, R. W., Merriman, T. R., Hampton, M. B., Barclay, M. L., Gearry, R. B., & Roberts, R. L. (2013). Macrophage migration inhibitory factor gene polymorphisms in inflammatory bowel disease: An association study in New Zealand Caucasians and meta-analysis. World Journal of Gastroenterology, 19(39), 6656-6664. Gosling, A. L., Matisoo-Smith, E., & Merriman, T. R. (2013). Gout in Māori: Modern affliction or ancestral trait? [Editorial]. Rheumatology. doi: 10.1093/rheumatology/ket299 Grainger, R., & Walker, J. (2013). Rheumatologists' opinions towards complementary and alternative medicine: A systematic review. Clinical Rheumatology. Advance online publication. doi: 10.1007/s10067-013-2379-z
Gulati A, Isbister G, Duffull SB. Scale reduction of a systems coagulation model with an application to modelling pharmacokinetic pharmacodynamic data. CPT Pharmacometrics Syst Pharmacol (In press) Hatah, E., Braund, R., Duffull, S. B., & Tordoff, J. (2013). General practitioners' views of pharmacists' current and potential contributions to medication review and prescribing in New Zealand. Journal of Primary Health Care, 5(3), 223-233.
Hatah, E., Braund, R., Tordoff, J., & Duffull, S. B. (2013). A systematic review and meta-analysis of pharmacist-led fee-for-services medication review. British Journal of Clinical Pharmacology. Advance online publication. doi: 10.1111/bcp.12140 Hatah, E., Tordoff, J., Duffull, S. B., & Braund, R. (2013). Pharmacists' performance of clinical interventions during adherence support medication reviews. Research in Social & Administrative Pharmacy. Advance online publication. doi: 10.1016/j.sapharm.2013.04.008
Hendrick, P., Milosavljevic, S., Hale, L., Hurley, D. A., McDonough, S. M., Herbison, P., & Baxter, G. D. (2013). Does a patient's physical activity predict recovery from an episode of acute low back pain? A prospective cohort study. BMC Musculoskeletal Disorders, 14(1), 126.
Arthritis Research Theme 2013 Report
31
Heydon, S, Duffull S. Pharmacy at Otago: The First 50 Years. The school, the profession and the people. New Zealand’s National School of Pharmacy, Dunedin (2013).
Hughes, K., Flynn, T., de Zoysa, J., Dalbeth, N., & Merriman, T. R. (2013). Mendelian randomization analysis associates increased serum urate, due to genetic variation in uric acid transporters, with improved renal function. Kidney International. Advance online publication. doi: 10.1038/ki.2013.353
Hyland, G., Hay-Smith, J., & Treharne, G. (2013). Women's experiences of doing long-term pelvic floor muscle exercises for the treatment of pelvic organ prolapse symptoms. International Urogynecology Journal. Advance online publication. doi: 10.1007/s00192-013-2202-z
Ingegnoli, F., Ardoino, I., Boracchi, P., Cutolo, M., EUSTAR co-authors, including Highton, J., & Stebbings, S. (2013). Nailfold capillaroscopy in systemic sclerosis: Data from the EULAR scleroderma trials and research (EUSTAR) database. Microvascular Research, 89, 122-128. doi: 10.1016/j.mvr.2013.06.003
Jamsen KM, Duffull SB, Tarning J, Price RN, Simpson JA. A robust design for identification of the Parasite Clearance Estimator. Malaria Journal (In press).
John, H., Hale, E. D., Treharne, G. J., Kitas, G. D., & Carroll, D. (2013). A randomized controlled trial of a cognitive behavioural patient education intervention vs a traditional information leaflet to address the cardiovascular aspects of rheumatoid disease. Rheumatology, 52(1), 81-90.
Jones, G. T., Bown, M. J., Gretarsdottir, S., Romaine, S. P. R., Helgadottir, A., Yu, G., … Jin, C., … Phillips, L. V., Williams, M. J. A., Topless, R., Merriman, T. R., … Lewis, D. R., … van Rij, A. (2013). A sequence variant associated with Sortilin-1 (SORT1) on 1p13.3 is independently associated with Abdominal Aortic Aneurysm. Human Molecular Genetics. Advance online publication. doi: 10.1093/hmg/ddt141 Kazantseva, M. G., Hung, N. A., Highton, J., & Hessian, P. A. (2013). MMP expression in rheumatoid inflammation: The rs11568818 polymorphism is associated with MMP-7 expression at an extra-articular site. Genes & Immunity. Advance online publication. doi: 10.1038/gene.2012.65 Kemp R, Dunn E, Schultz M. Immunomodulators in Inflammatory Bowel Disease: An Emerging Role for Biologic Agents. BioDrugs. 2013 Jun 8. (In press) Kini GP, McAlindon ME, Schultz M, Collett J, Murray IA. Capsule endoscopy of a very refractory celiac disease. Journal of Gastroenterology Hepatology 2013,28:1254 Koning, M., Ailabouni, R., Gearry, R. B., Frampton, C. M. A., & Barclay, M. L. (2013). Use and predictors of oral complementary and alternative medicine by patients with inflammatory bowel disease: A population-based, case-control study. Inflammatory Bowel Diseases. Advance online publication. doi: 10.1097/MIB.0b013e31827f27c8 Korell, J., & Duffull, S. B. (2013). A semi-mechanistic red blood cell survival model provides some insight into red blood cell destruction mechanisms. Journal of Pharmacokinetics & Pharmacodynamics. Advance online publication. doi: 10.1007/s10928-013-9322-4 Korell, J., Duffull, S. B., Dalrymple, J. M., Drake, J., Zhang, M., Barclay, M. L., & Stamp, L. K. (2013). Comparison of intracellular methotrexate kinetics in red blood cells with the kinetics in other cell types. British Journal of Clinical Pharmacology. Advance online publication. doi: 10.1111/bcp.12209
Arthritis Research Theme 2013 Report
32
Korell, J., Stamp, L. K., Barclay, M. L., Dalrymple, J. M., Drake, J., Zhang, M., & Duffull, S. B. (2013). A population pharmacokinetic model for low-dose methotrexate and its polyglutamated metabolites in red blood cells. Clinical Pharmacokinetics. Advance online publication. doi: 10.1007/s40262-013-0052-y
Lawitz E, Mangia A, Wyles D, Rodriguez-Torres M, Hassanein T, Gordon SC, Schultz M, et al. Sofosbuvir for Previously Untreated Chronic Hepatitis C Infection. New England Journal of Medicine 2013(epub ahead of print) Lee JC, Espéli M, Anderson CA, Linterman MA, Pocock JM, Williams NJ, Roberts R, et al. (2013).Human SNP links differential outcomes in inflammatory and infectious disease to a FOXO3-regulated pathway. Cell. 2013 155(1):57-69.
Mansi, S., Milosavljevic, S., Tumilty, S., Hendrick, P., & Baxter, G. D. (2013). Use of pedometer-driven walking to promote physical activity and improve health-related quality of life among meat processing workers: A feasibility trial. Health & Quality of Life Outcomes, 11, 185. doi: 10.1186/1477-7525-11-185
McDonough, S. M., Tully, M. A., Boyd, A., O'Connor, S. R., Kerr, D. P., O'Neill, S. M., … Baxter, G. D., Hurley, D. A. (2013). Pedometer-driven walking for chronic low back pain: A feasibility randomized controlled trial. Clinical Journal of Pain. Advance online publication. doi: 10.1097/AJP.0b013e31827f9d81
Merriman, T. R., & Flynn, T. J. (2013). Molecular genetics of hyperuricaemia and gout. In eLS. John Wiley & Sons. doi: 10.1002/9780470015902.a0025153
Milne, V., Kearns, R., & Harrison, A. Patient age, ethnicity and waiting times determine the likelihood of non-attendance at a first specialist rheumatology assessment. International Journal of Rheumatic Diseases. 2014 Jan;17(1):19-25. Mulligan, H., Treharne, G. J., Hale, L. A., & Smith, C. (2013). Combining self-help and professional help to minimize barriers to physical activity in persons with multiple sclerosis: A trial of the "Blue Prescription" approach in New Zealand. Journal of Neurologic Physical Therapy, 37, 51-57. Nasir, B. F., Griffiths, L., Nasir, A., Roberts, R., Barclay, M., Gearry, R., & Lea, R. A. (2013). Perianal disease combined with NOD2 genotype predicts need for IBD-related surgery in Crohn's disease patients from a population-based cohort. Journal of Clinical Gastroenterology, 47(3), 242-245. Nasir, B. F., Griffiths, L. R., Nasir, A., Roberts, R., Barclay, M., Gearry, R. B., & Lea, R. A. (2013). An envirogenomic signature is associated with risk of IBD-related surgery in a population-based Crohn’s disease cohort. Journal of Gastrointestinal Surgery. Advance online publication. doi: 10.1007/s11605-013-2250-1. Ngu, J. H., Wallace, M. C., Merriman, T. R., Gearry, R. B., Stedman, C. A. M., & Roberts, R. L. (2013). Association of the HLA locus and TNF with type I autoimmune hepatitis susceptibility in New Zealand Caucasians. SpringerPlus, 2(1), 355.
Nyberg J, Bazzoli C, Ogungbenro K, Aliev A, Leonov S, Duffull S, Hooker AC, Mentre F. Methods and software tools for design evaluation in population pharmaockinetics-pharmacodynamics. British Journal of Clinical Pharmacology (In press). Peplow, P. V., & Baxter, G. D. (2013). Testing infrared laser phototherapy (810 nm) to ameliorate diabetes: Irradiation on body parts of diabetic mice. Lasers in Surgery & Medicine, 45(4), 240-245.
Arthritis Research Theme 2013 Report
33
Peplow, P. V., & Baxter, G. D. (2013). Translational approach to treating diabetes using acupuncture or electroacupuncture. In J. D. Adams Jr & E. J. Lien (Eds.), Traditional Chinese medicine: Scientific basis for its use (pp. 313-338). Cambridge, UK: Royal Society of Chemistry. doi: 10.1039/9781849737852-00313
Pinto D, Robertson MC, Abbott JH, Hansen P, Campbell AJ for the MOA Trial Team Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee. 2: economic evaluation alongside a randomized controlled trial Osteoarthritis & Cartilage. 2013; 21(10):1504-13. Rasheed, H., Phipps-Green, A., Topless, R., Hollis-Moffatt, J. E., Harré Hindmarsh, J., Franklin, C., Stamp, L. K., Merriman, T. R. (2013). Association of the lipoprotein receptor-related protein 2 gene with gout and non-additive interaction with alcohol consumption. Arthritis Research & Therapy, 15, R177. doi: 10.1186/ar4366 Pinto, D., Robertson, M. C., Abbott, J. H., Hansen, P., Campbell, A. J., on behalf of the MOA Trial Team. (2013). Manual therapy, exercise therapy, or both, in addition to usual care, for osteoarthritis of the hip or knee. 2: Economic evaluation alongside a randomized controlled trial. Osteoarthritis & Cartilage. Advance online publication. doi: 10.1016/j.joca.2013.06.014
Roberts, R. L., Wallace, M. C., Jones, G. T., van Rij, A. M., Merriman, T. R., Harrison, A., … Stamp, L. K., … Highton, J., Stebbings, S. M. (2013). Prevalence of HLA-B27 in the New Zealand population: Effect of age and ethnicity. Arthritis Research & Therapy, 15, R158.
Roberts, R. L., Wallace, M. C., Wright, D. F. B., Cadzow, M., Dalbeth, N., Jones, P. B., Stamp, L. K., Harrison, A. A., Black, M. A., Merriman, T. R. (2013). Frequency of CYP2C9 polymorphisms in Polynesian people and potential relevance to management of gout with benzbromarone. Joint Bone Spine. Advance online publication. doi: 10.1016/j.jbspin.2013.07.006 Schmitt, J. S., & Abbott, J. H. (2013). Patient global ratings of change did not adequately reflect change time over time: A clinical cohort study. Physical Therapy. Advance online publication. doi: 10.2522/ptj.20130162
Shaw JP, Print A, Duffull SB. Development of a Postgraduate Educational Program for Pharmacist Prescribers in New Zealand. J Pharm Pract Res 2013;43:122-7.
Shivva, V., Korell, J., Tucker, I. G., & Duffull, S. B. (2013). An approach for identifiability of population pharmacokinetic–pharmacodynamic models. CPT: Pharmacometrics & Systems Pharmacology, 2. Advance online publication. doi: 10.1038/psp.2013.25 Shivva V, Korell JK, Tucker IG, Duffull SB. Choice of parameterisation affects identifiability for population models. Journal of Pharmacokinetics and Pharmacodynamics (In press)
Smith, C. M., Hale, L. A., Olson, K., Baxter, G. D., & Schneiders, A. G. (2013). Healthcare provider beliefs about exercise and fatigue in people with multiple sclerosis. Journal of Rehabilitation Research & Development, 50(5), 733-744. Stamp, L. K., O'Donnell, J. L., Frampton, C., Drake, J. M., Zhang, M., & Chapman, P. T. (2013). Clinically insignificant effect of supplemental vitamin C on serum urate in patients with gout: A pilot randomized controlled trial. Arthritis & Rheumatism, 65(6), 1636-1642.
Arthritis Research Theme 2013 Report
34
Stamp, L. K., Wells, J. E., Pitama, S., Faatoese, A., Doughty, R. N., Whalley, G., Richards, A. M., Cameron, V. A. (2013). Hyperuricaemia and gout in New Zealand rural and urban Māori and non- Māori communities. Internal Medicine Journal, 43(6), 678-684. Stamp, L. K., & Barclay, M. (2013). Therapeutic drug monitoring in rheumatic diseases: Utile or futile? Rheumatology. Advance online publication. doi: 10.1093/rheumatology/ket355
Stamp, L. K., Hazlett, J., Highton, J., & Hessian, P. A. (2013). Expression of methotrexate transporters and metabolizing enzymes in rheumatoid synovial tissue. Journal of Rheumatology. Advance online publication. doi: 10.3899/jrheum.130066 International Genetics of Ankylosing Spondylitis Consortium (IGAS), including Stebbings, S. (2013). Identification of multiple risk variants for ankylosing spondylitis through high-density genotyping of immune-related loci. Nature Genetics, 45(7), 730-738.
tan Nguyen, H., Merriman, T. R., & Black, M. A. (2013). CNVrd, a read-depth algorithm for assigning copy-number at the FCGR Locus: Population-specific tagging of copy number variation at FCGR3B. PLOS ONE, 8(4), e63219. doi: 10.1371/journal.pone.0063219 Tarr GP, Smith RA, John RA, Crowley AP, Kok JB, Lee HN, Mustafa MH, Sii KM, Son SE, Weaver LJ, Cameron C, Dockerty JD, Murray IA, Schultz M. Perceived risks and benefits of surveillance colonoscopy in people undergoing surveillance for family history of colorectal cancer. New Zealand Medical Journal. 2013 Sep 13;126(1382):58-69. Taylor, W. J., Brown, M., Aati, O., Weatherall, M., & Dalbeth, N. (2013). Patient preferences for core outcome domains for chronic gout studies do not support the validity of composite response criteria. Arthritis Care & Research. Advance online publication. doi: 10.1002/acr.21955 Taylor, W. J., & Robinson, P. C. (2013). Classification criteria: Peripheral spondyloarthropathy and psoriatic arthritis. Current Rheumatology Reports, 15(4), 317. Teruel, M., McKinney, C., Balsa, A., Pascual-Salcedo, D., Rodriguez-Rodriguez, L., Ortiz, A. M., … Merriman, T., … Martin, J. (2013). Association of CD247 polymorphisms with rheumatoid arthritis: A replication study and a meta-analysis. PLOS ONE, 8(7), e68295. doi: 10.1371/journal.pone.0068295 Tucker, I. G., Norris, P. T., & Duffull, S. B. (2013). What is the best way to deliver therapeutics and who decides? [Editorial]. Therapeutic Delivery, 4(7), 763-765. van Egmond R, Barclay ML, Chin PKL, Sies CW, Florkowski CM. Biological variation of TPMT enzyme activity: when has a significant change taken place? Annals of Clinical Biochemistry 2013; 50(5): 473-478
van Egmond R, Barclay ML, Chin PKL, Sies CW, Florkowski CM. Pre-analytical stringency: what factors may confound interpretation of TPMT enzyme activity? Annals of Clinical Biochemistry 2013; 50(5): 479-484. Wassinger CA, Sole G, Osborne H. Clinical measurement of scapular upward rotation in response to acute subacromial pain. Journal of Orthopaedics Sports Physical Therapy. 2013;43(4):199-203.
Ward, L., Stebbings, S., Cherkin, D., & Baxter, G. D. (2013). Yoga for functional ability, pain and psychosocial outcomes in musculoskeletal conditions: A systematic review and meta-analysis. Musculoskeletal Care. Advance online publication. doi: 10.1002/msc.1042

Arthritis Research Theme 2013 Report
35
Ward, L. (2013) Yoga: A useful and effective therapy for musculoskeletal disorders? Physical Therapy Reviews, 18, 4, 235-238.
Wright, D. F. B., Stamp, L. K., Merriman, T. R., Barclay, M. L., Duffull, S. B., & Holford, N. H. G. (2013). The population pharmacokinetics of allopurinol and oxypurinol in patients with gout. European Journal of Clinical Pharmacology. 69(7):1411-21 Wright, D. F. B., & Duffull, S. B. (2013). A bayesian dose-individualization method for warfarin. Clinical Pharmacokinetics, 52(1), 59-68. doi: 10.1007/s40262-012-0017-6 Wright, D. F. B., Al-Sallami, H. S., & Duffull, S. B. (2013). Is the dose of dabigatran really more predictable than warfarin? [Letter]. British Journal of Clinical Pharmacology. Advance online publication. doi: 10.1111/bcp.12144
Yeo, T. W., Lampah, D. A., Rooslamiati, I., Gitawati, R., Tjitra, E., Kenangalem, E., … Duffull, S. B., Anstey, N. A. (2013). A randomized pilot study of L-arginine infusion in severe falciparum malaria: Preliminary safety, efficacy and pharmacokinetics. PLOS ONE, 8(7), e69587.
Yeoh, N., Burton, J. P., Suppiah, P., Reid, G., & Stebbings, S. (2013). The role of the microbiome in rheumatic diseases. Current Rheumatology Reports, 15(3), 314.
Zhang M, Moore GA, Barclay ML, Begg EJ. A simple HPLC method for simultaneous determination of three triazole antifungals in human plasma. Antimicrobial Agents and Chemotherapy 2013; 57(1): 484-489
Theme members highlights of 2013
Dunedin Patient Update Meeting Disseminating the outcomes of research involving patients is an important aspect of research
efforts. One avenue utilized is the annual Dunedin Patient Update meeting, which in 2013
was held on the afternoon of December 5th. Among presentations, Dr Simon Stebbings
considered whether bacteria in the mouth cause arthritis, PhD student Lesley Ward presented
her results on the feasibility and safety of an 8-week relaxation-based yoga intervention for
patients with rheumatoid arthritis, Dr Rebecca Roberts summarized her genetic studies of the
HLA-B27 gene in New Zealand and medical student T Ing-aram presented on patient advice
and understanding of methotrexate dosage.
Update from the ACR/EULAR Gout Classification Criteria Project
This project is on track to present its main findings at the ACR Annual Scientific Meeting in
late 2014. Twenty-five sites from 16 countries have so far submitted data on 480 participants
to the SUGAR study. A systematic review of imaging for the diagnosis of gout has been
completed and was presented at the ACR ASM in San Diego in November. The main
findings were that DECT and US have good test accuracy for the diagnosis of gout in well-
established disease but insufficient data limit the strength of conclusions that can be drawn. A
Arthritis Research Theme 2013 Report
36
diagnostic accuracy preference survey will be conducted over the New Zealand summer, and
the results from all these studies will be discussed in detail at a 2-day consensus meeting
immediately prior to the EULAR Congress June 2014 in Paris. At this meeting, chaired by
Associate Professor William Taylor, an invited panel of 20 gout experts from Europe and
North America will integrate the data analysis with their clinical experience to confirm new
criteria for the diagnosis of gout. The new criteria will then be tested in existing data-sets to
check accuracy and feasibility.
Grants received in 2013 Ribeiro D and Sole, G - Jack Thomson Arthritis Grant: Can we optimize rotator cuff motor control? Exploring novel rehabilitation exercises for shoulder osteoarthritis treatment. $10,127 Roberts RR and Stamp LK – Arthritis New Zealand. Using pharmacogenetics to predict response to allopurinol. $20,067
Sole G, Ribeiro D, Sole C, and Mündermann A. Physiotherapy New Zealand: Do footwear variations influence the magnitude and direction of forces across the knee in people who have sustained a knee injury? Amount: $7,618 Stamp LK, Hessian PA and Highton J – Health Research Council of New Zealand. Predicting response to biologics using gene expression profiles and cytokines. $1.2M Treharne G, Stamp LK, Valentino N and Stebbings S.– University of Otago Research Grants. Qualitative follow-up investigation of a piloted smoking cessation intervention for people with rheumatoid arthritis. $20,000
Hessian PA and Stamp LK MBIE/Cawthron Institute Subcontract Healthy food ingredients from shellfish and algae. $705, 950
Harcombe HJ, Abbott JH, Derrett S, Paul C, Davie G, Gwynne-Jones D. - Arthritis New Zealand. Hip and knee joint replacement surgery in New Zealand: Equity of access according to region, age, ethnicity, socio-economic status and rurality. $49,838 Woodley, S J, Chapple, CM, Flack, N and Nicoholson, HD. Jack Thompson Arthritis Grant Award Can prehabilitation improve patient outcomes following hip joint replacement? $26,230 Wright DFB, Chin PKL, Jensen BP, Zhang M, Duffull SB, Begg EJ. NZ Pharmacy Education and Research Foundation. Individualised dabigatran dosing and anticoagulant monitoring to improve patient outcomes. $5125
Schultz M, Butt GA, Rodrigues E, Kemp R. NZSG AbbVie Research Grant How do NOD2 mutations associated with Crohn’s disease modify the response of the intestinal epithelium to commensal bacteria? $35,000 Schultz M, Regenbrecht H, Walmsley R, Ho C. Healthcare of Otago Charitable Trust Putting the Patient First: IBDsmart – A mobile platform for the management of patients with Inflammatory Bowel Disease. $18,000
Arthritis Research Theme 2013 Report
37
Postgraduate students (completed) Tracey Daysh-Andrew MHealSc. (Rehabilitation). Evaluation of the Offender Reintegration Process for Work and Income clients being released from Manawatu Prison Health Unit into Primary Care Services. Supervisor: William Taylor.
Aimee Chisnall MSc. The role of SLC2A9 variants in hyperuricaemia and gout. Supervisor: Tony Merriman
Abhishek Gulati PhD. Application of pharmacometric methods to systems pharmacology. Supervisors: Stephen Duffull, Geoff Isbister.
Matire Harwood PhD. Understanding and Improving Stroke Recovery for Maori and Their Whanau. Supervisors: William Taylor, Kathryn McPherson, Harry McNaughton, Papaarangi Reid, Bridget Robson. Ernieda MD Hatah PhD. Investigating medication review services provided by community pharmacists. Supervisors: Rhiannon Braund, Stephen Duffull, June Tordoff. Kimberley Hughes MSc. 'The Causative relationship between Serum Urate, kidney function and phenotypic parameters. Supervisor: Tony Merriman Chakradhar Lagishetty PhD. Covariates in pharmacometrics. Supervisors: Stephen Duffull and Parry Guilford Daniel Ribeiro PhD. Exploring the measurement properties and effectiveness of a postural monitor and feedback device. Supervisors: Milosavljevic S, Haxby Abbott, Giesla Sole. Stephanie Thompson MhealSc. (Rehabilitation). Awarded with distinction. Effect of the rehabilitation setting on motivation post stroke. Supervisors: William Taylor and Mark Weatherall.
Daniel Wright PhD. Model-based drug dosing. Supervisors: Stephen Duffull, Nick Holford.
Current Postgraduate Students Pip Aimer - Identifying and overcoming the barriers to smoking cessation in rheumatoid arthritis. PhD supervisors: Lisa Stamp, Gareth Treharne, Vicky Cameron, Simon Stebbings
Hesham Al-Sallami - Optimising patient care by individualising drug doses. PhD Supervisors: Stephen Duffull and Natalie Medlicott
Piyanan Assawasuwannakit – How patient compliance impacts on drug pharmacokinetics and pharmacodynamics. PhD Supervisors: Rhiannon Braund and Stephen Duffull
Caitlin Batt - Prevalence of Fructose Malabsorption in Gout. BMedSci supervisors: Lisa Stamp and Richard Gearry Susan Baxter – Walking as an intervention for people with rheumatoid arthritis. PhD supervisor: Gareth Treharne Paul Chin - Aspects of renal function and dabigatran and gentamicin drug clearance. PhD supervisors Evan Begg and Murray Barclay Eng Wee Chua - Understanding adverse drug reactions or responses using genomic sequencing (UDRUGS). PhD supervisors Martin Kennedy, Murray Barclay, Ruth Savage
Arthritis Research Theme 2013 Report
38
Emily Davidson - Measurement of change in self-identity after traumatic brain injury. PhD supervisors: William Levack, William Taylor
Tahzeeb Fatima - Gout: The relationship with metabolic disease. PhD supervisor Tony Merriman
Tanya Flynn - Causes of gout; genetic and social understandings. PhD supervisor: Tony Merriman
Anna Gosling - Hyperuricaemia in the Pacific: a biological anthropological perspective. PhD supervisors: Tony Merriman and Lisa Matisoo-Smith
Nyugen Hoang – Statistical methods for the analysis of copy number variants. PhD supervisors: Tony Merriman and Mik Black
Roisin Hegarty – Daily fatigue and psychological well-being among people with rheumatoid arthritis. MSc supervisor: Gareth Treharne
Sally Heppenstall Validation of the InterRai RUGS-III in three New Zealand District Health Boards. MHealSc. Supervisors: Will Taylor and Sally Keeling.
Elizabeth Kemp - The psychometric properties of the Patient Specific Functional Scale in patients with lower limb conditions. MPhty Supervisors: Haxby Abbott and Will Taylor
Cherie le Lievre Is the Participation and Environment Measure for Children and Youth (PEM-CY) valid in a general New Zealand population? MHealSc. Supervisors: Fiona Graham and Will Taylor. Liu, Lizhou - Non-pharmocological interventions for knee osteoarthritis: evaluation of the effectiveness of walking versus walking plus laser acupuncture. Degree required supervisors: David Baxter, Suzanne McDonough, Margot Skinner.
Beth Mayland – Anxiety and outcomes of upper limb injury. PhD supervisor: Gareth Treharne
Valerie Milne - Social and geographic barriers to accessing rheumatology services. PhD supervisors: Andrew Harrison and Robin Kearns
Jarrod Moors - Health and well-being in Pacific teenagers. MSc supervisor Tony Merriman Shan Pan – Development of a population pharmacokinetic-pharmacodynamic (PKPD) model for methotrexate and methotrexate polyglutamates in red blood cells. PhD supervisors: Steve Duffull, Julia Korrell and Lisa Stamp
Humaira Rasheed – Relationship of gout with dyslipidemia. PhD supervisor: Tony Merriman Shamin Mohd Saffian – The dose individualisation of warfarin. Supervisors: Steve, Dan Wright, Paul Chin
Salahudeen – Anticholinergic indices for commonly prescribed medicines. Supervisors: Prasad Nishtala, S Duffull
Warren Scott – Beliefs about exercise among men with rheumatoid arthritis. MSc supervisor: Gareth Treharne
Vittal Shiva – Development of population pharmacokinetic model for ketones. PhD Supervisors: Stephen Duffull and Ian Tucker
Lesley Ward - Yoga for musculoskeletal conditions. PhD supervisors: David Baxter and Simon Stebbings
Arthritis Research Theme 2013 Report
39
Catherine Willett A Pilot Study of Low-Dye taping in Rugby Union Players – perceptions of tolerability MHealSci supervisor Hamish Osborne
Mansour Zamanpour - Genetic basis for negative relationship between rheumatoid arthritis and schizophrenia. PhD supervisor: Tony Merriman
Student travel Awards
The theme supported two PhD students to attend the International meeting to present their
research. The selection panel included Paul Hessian, Andrew Harrison and Tony Merriman,
Lesley Ward attended two meetings in the USA and Pip Aimer attended a meeting in the UK.
Reports on these are below.
Lesley Ward - PhD candidate, School of Physiotherapy and Department of Medicine
With the assistance of financial aid from the Arthritis
Research Theme, I attended the Symposium on Yoga
Research (SYR), and the Symposium on Yoga Therapy and
Research (SYTAR), in Boston, USA. SYR and SYTAR are
the premier international conferences for academic yoga
research and professional education into yoga therapy. For
the first time, SYR and SYTAR were held in conjunction with each other, offering a unique
opportunity to attend both conferences.
My attendance was the first time New Zealand has been represented at SYR and SYTAR; and
I was fortunate to be accepted to present at both conferences. At SYR, I gave a poster
presentation on the results of my Delphi survey, which involved establishing international
guidelines for the components and reporting of yoga interventions for musculoskeletal
conditions. This poster was very well received, with a lot of interest in the development of
this area of research. Additionally, a number of researchers who participated in the Delphi
survey were attending the conference, and it was an excellent opportunity to network with
them, and discuss future directions for this phase of research.
At SYTAR, I gave a 15-minute oral platform presentation, reporting on my pilot feasibility
study of yoga for people with rheumatoid arthritis. Again, my talk was well received, and
people very interested at the research occurring here in New Zealand. My mentor for my pilot
Arthritis Research Theme 2013 Report
40
study was attending SYTAR, offering the opportunity to discuss study results and suggestions
for future research.
It was very rewarding to attend these international conferences, share my work, and receive
peer feedback that my PhD research is of international interest and standing. Networking
opportunities at both conferences were excellent, and collaborations were established for
future research projects. Specifically, I have been asked to collaborate on publications with
two separate researchers in Germany, and a researcher in the USA. Collaborative work will
begin once I have submitted my PhD thesis, in early 2014.
My attendance at SYR and SYTAR is one of the highlights of my PhD. I thank the Arthritis
Research Theme for their financial support of my attendance at these events, and look
forward to on-going research collaboration with ART members.
Pip Aimer - PhD candidate, Department of Medicine, University of Otago, Christchurch
I was very fortunate to attend the ISCHP conference that was held
21-24 July 2013 at Bradford, United Kingdom. The conference is
held every two years and provides an opportunity for researchers
from all over the world to explore emerging and on-going issues in
relation to health and healthcare. This moderately small conference
with about 150 attendees, included health psychologists, health
service providers, users, activists, students, and scholars in a diverse range of disciplines, but
whom all take a critical approach to health, illness and healthcare. The conference had a very
collaborative, welcoming and inclusive feeling to it, and provided researchers with an
opportunity to present their research in a diverse range of presentation formats: including
exhibitions, stage performances, posters, speakers, and various presentation challenges: such
as a 5-minute challenge (with a maximum of only 5 slides), and the entertaining Pecha Kucha
(20 pictorial slides for 20 seconds each). The symposiums were held in 4 parallel sessions,
specifically aimed at stimulating debate and enthusiasm for critical health psychology.
I was selected to present a ‘5-minute challenge’ talk on my PhD research: identifying the
barriers to smoking cessation in rheumatoid arthritis. The ‘challenge’ was to be able to

Arthritis Research Theme 2013 Report
41
express my research topic into the strictly enforced presentation time, not an easy feat! This
qualitative research study was focused on the health issue of smoking cessation and the
chronic illness of rheumatoid arthritis (RA). Smoking has recently been identified as a
significant environmental risk factor for developing rheumatoid arthritis. In addition to this,
continued smoking may intensify disease activity in RA and lessen responsiveness to
medications. However, there is little research to-date on smoking cessation support
specifically aimed at people with RA. The aims of this study were to identify specific RA-
related barriers to smoking cessation. The transcripts from focus groups and individual
interviews were analysed thematically using a critical realist approach and therefore fits with
the research ethos of ISCHP.
I definitely took advantage of the pre-conference workshop that offered group discussion and
pragmatic advice on publishing in critical health psychology. The conference symposiums
covered diverse topics such as Care and Aging; Recovering Beauty; Health promotion in
global contexts; Health Disparities and Inequalities; Healthcare Services and Social
Interaction; Living with Difference; and Recovery Programmes. It was a busy 4 days with so
many interesting speakers including key-note addresses on ‘Disability studies and critical
health psychology: comrades in arms?’ and ‘No rest for the aged? Individual responsibility
for staying alive in the twenty first century’. Overall, the conference was a fantastic
opportunity to meet and talk to other researchers, many who are starting out or completing
PhD’s. West Yorkshire was fabulous, especially inviting with the heat wave that England
was experiencing at the time.
Summer students The Arthritis Research Theme utilised extra funding provided by the University and supported students for summer research projects; Vidya Yugaaja (Biochemistry), Imogen Nolan (Medicine, Christchurch) and Mike Wilson (Psychology).
Non-additive gene interactions with sugar-sweetened beverage consumption and the risk of Gout
Vidya Yugaraja, Supervisor: Tony Merriman
Background: Gout is a multi-factorial disease resulting from high urate in the blood.
Consumption of sugar sweetened beverages (SSB), which contain large amounts of fructose
increase serum urate levels and the risk of gout. There is evidence for a non-additive

Arthritis Research Theme 2013 Report
42
interaction between SSB consumption and the gout risk gene SLC2A9. The aim of this study
was to find any further genes that interact with SSB consumption to influence serum urate
levels and the risk of gout.
Methods: Approved data from 5,365 individuals in the Atherosclerosis Risk in Communities
(ARIC) study was used to perform a in silico partial genome-wide association study. New
Zealand multi-ancestral gout cases (n=809) and controls (n=925) were then genotyped for
DKK2 single nucleotide polymorphism (SNP) rs12498707 using Taqman technology.
STATA (version 8.0) was used for statistical analysis.
Results: rs12498707 SNP in the DKK2 gene was identified. Increasing SSB consumption
was associated with increased urate levels in the ARIC Caucasian group only when the minor
allele (A) was present (∆SU=0.004mmol/L, p=3.1x10-4). SSB consumption ≥4/day was
shown to interact with the DKK2 variant to increase in serum urate concentrations in ARIC
Caucasain subjects (β=0.042, p=9.4x104). However, there was no statistically significant
evidence for a similar interaction on the risk of gout in the NZ sample set (NZ Caucasian;
OR=2.39, p=0.29, Eastern Polynesian; OR=1.34, p=0.62, Western Polynesian; OR=0.88,
p=0.84).
Conclusion: There was a gene-environment (GxE) interaction between the DKK2 variant
(rs12498707) and SSB consumption (≥4/day) to increase serum urate concentrations in the
ARIC Caucasian population. While statistical significance could not be replicated for the risk
of gout in the NZ gout case-control sample set, the trend suggests that the minor allele
associates with an increased risk of gout in the Caucasian group.
Joint infections in patients with rheumatic diseases
Imogen Nolan, Supervisor(s): Professor Lisa Stamp and Professor
Steve Chambers
This study examined the population within Canterbury from 2006-
2013 who developed a joint infection. This is a very serious
medical condition caused by spread of bacteria from the blood or a
nearby infection, which can destroy a joint within a matter of days
if left untreated. Joint infections are relatively rare, however they are estimated to cost over
$5,000,000 per year for inpatient stays in addition to outpatient appointments, GP visits,
allied health physiotherapy and occupational therapy support and loss of productivity. People
Arthritis Research Theme 2013 Report
43
with abnormal joints, such as those with arthritis, are at an increased risk of developing a joint
infection. Furthermore, they are often on drugs which suppress the immune system,
potentially increasing the risk even more. Immunosuppressive drugs for arthritis include
steroids like prednisone, a group called disease modifying anti-rheumatic drugs (DMARD’s),
and newer agents called ‘biologics’ which are synthetic antibodies against specific parts of
the immune system involved in an autoimmune disease process. In this study we wanted to
describe the characteristics of people in Canterbury who developed joint infections and
identify any risk factors. We also wanted to examine the people who had pre-existing
abnormal joints, particularly those with various types of arthritis like rheumatoid arthritis
(RA), and those with crystals deposition diseases namely gout (monosodium urate crystals)
and pseudogout (calcium pyrophosphate dihyrate crystals). We aimed to describe these
groups and identify whether immunosuppressive medications were putting them at risk.
The patients who had joint infections from 2006-2013 were identified from a database kept
by the infectious diseases department in Christchurch Public Hospital. There were two groups
to look at, those who had an infection in a native joint, and those who had an infection in a
prosthetic joint replacement. Patients with confirmed infection were included if they lived in
Canterbury and were 18 years of age or above. If the patient was admitted more than once for
the same infection, information was recorded for the first admission only. Data on the joint
infection event and the patient’s medical history were obtained from the Health Connect
South hospital records and paper patient files for those admitted in 2008 and prior.
The native joint group included 199 patients who had a joint infection between 2006-2013.
158 (80%) of these patients had no joint disease before the infection, however 7 patients had
RA, 23 patients had crystal disease and 3 people had other types of autoimmune disease. The
mean age was 57.6 years. The type of bacteria which caused the infections were similar
across all groups with Staphylococcus aureus being most common (46.5%), followed by
coagulase-negative Staphylococcus (CNS) (7.5%), pyogenic Streptococci (10%), other
Streptococci (4%) and ‘other’ organisms (12%). There was no growth in 13% of cases and no
aspirate done in 7%.
In the prosthetic joint group, 181 patients were included. 140 (77%) of these patients had no
prior joint disease, 10 had RA, 25 had crystal disease and 6 had an ‘other’ autoimmune
disease. The mean age for this group was 68.5 years. The causative organisms were similar to
the native joint group however proportions were different, with higher CNS, mixed growth
and ‘other’ bugs. S. aureus was still the most common (34%), followed by CNS (23%), other
Arthritis Research Theme 2013 Report
44
Streptococci (5%), mixed growth (4%) and others (18%). There was no growth in 7% and no
aspirate done in 2%. Rates were comparable across all groups except the RA group where S.
aureus accounted for a higher 70% infections.
The rates per year of all joint infections per the Canterbury population (aged 18 and over)
were calculated using population data from NZ statistics. The rate remained relatively stable
at 0.01% of the population per year between 2006-2013, identical to some published
estimates of rates for industrialised countries. The rate increased overall by 0.003% over the 8
years.
The major risk factor for joint infection development in both groups was a preceding medical
intervention. In the native joint group 6% of the patients without pre-existing arthritis had a
steroid injection into the joint within 6 weeks prior to the infection. More patients in the RA
(14%) and the crystal disease groups (9%) had preceding steroid injections. 16% of the ‘no
arthritis’ group had surgery within 6 months of the joint infection compared with none in the
RA group and 9% in the crystal disease group. In the prosthetic joint group 33% had previous
joint surgery, with the crystal disease group having a higher rate at 40%. There were no cases
of steroid injection. Other risk factors like heart or lung disease and diabetes were also
recorded. 29% and 32% of people in the native and prosthetic groups respectively had at least
one of these.
Gout and pseudogout do not suppress the immune system. However it is unclear whether the
presence of crystals in the joint per se is a risk factor for an infection. When an individual
presents with suspected joint infection, a sample of the joint fluid is taken to identify the
bacteria and this is also the method used to identify joint crystals, so we investigated this
further. Joint fluid was examined for crystals in almost half (48%) of the native joint patient
samples and crystals were observed in 13%. However in the 13 patients with known gout, the
joint fluid was examined for crystals in only 6. Crystals were also found in 1 patient with
previously undiagnosed gout, 8 cases of undiagnosed pseudogout and 1 case where both
crystal types were identified for the first time. In the prosthetic joint group the joint fluid was
examined for crystals in less aspirates (22%) and a larger proportion (31%) were positive for
crystals. In the 17 patients with previously diagnosed gout and 1 with pseudogout, 6 (35%)
had joint fluid examined for crystals. 7 cases of undiagnosed pseudogout and 1 case of both
gout and pseudogout were also identified for the first time.
Arthritis Research Theme 2013 Report
45
There were 3 medication classes which we examined as possible risk factors for joint
infection. Out of the 7 people in the native joint group who had RA, 4 (57%) were on
prednisone, 5 (71%) were on a DMARD, and 1 (14%) was on a biologic. Out of the 22 people
in the crystal disease group 3 (14%) were on prednisone and 1 (4.5%) was on a DMARD, in
the ‘other’ group 1 person was on prednisone and 2 were on a DMARD. Out of the 10
prosthetic joint group patients with RA, 8 (80%) were on prednisone, 6 (60%) were on a
DMARD, and 3 (30%) were on a biologic agent. Of the 25 people with crystal disease 2 (8%)
were on prednisone with none on a DMARD, and in the ‘other’ group there were 5 people on
prednisone and 4 people on a DMARD.
While we wanted to identify whether being on an immune suppressant medication altered the
likelihood of developing an infection, this proved to be difficult due to the small number of
patients receiving these drugs. The most heavily immune suppressed patients were as
expected, those with RA. These patients made up 3.5% of the native infection group and
5.5% of the prosthetic group. The prevalence of RA is generally accepted to be 1-2%
although previous NZ studies have estimated 3.1%, 3.5%, 2.5%, 0.4% and 0.53%. Thus it is
difficult to say whether there is a difference in the prevalence in the population who develop a
joint infection. It was a surprise that not more patients with RA were identified, and that there
were such large numbers of patients with crystal deposition disease. In Canterbury, taking
into account the different rates for Māori and non-Māori populations, the overall rate of gout
is ~3.3%. Pseudogout rates are unknown. In our study the rates of crystal deposition diseases
in the native group were gout (8%) and total crystal disease (12%). In the prosthetic group
rates were gout (10%) and total crystal disease (14%).
Overall the results were surprising as most variables were similar across those with and
without pre-existing arthritis. We also identified less RA patients than expected, which could
possibly indicate that the medications used in this disease to suppress the immune system are
less likely to lead to joint infection than previously thought. The high rates of crystal disease
was also interesting, and may be due to increasing rates of these diseases in the whole
population or due to the presence of crystals in a joint predisposing to infection. The major
limitation of this study was sample size and the possibility that some cases of joint infection
were not included in the original database used. The next step will be to carry out a more
thorough search to ensure all cases in this time period were identified, and to then extend the
study to the years prior to 2006 to increase the sample size and reach statistical significance
for the identified risk factors.

Arthritis Research Theme 2013 Report
46
Dexterity in rheumatoid arthritis: Pilot testing a novel measurement glove and investigating correlates Mike Wilson; Supervisor(s): Dr Gareth Treharne and Prof
Elizabeth Franz (Department of Psychology), Advisor: Dr
Simon Stebbings (Department of Medicine)
A key treatment outcome for rheumatoid arthritis (RA) patients
is an improved ability to perform everyday tasks, most of
which require dexterity. Current measures of dexterity
generally use: a) the time needed to complete a task; b) assessment of ability to complete a
task in a prescribed manner; c) self-report questionnaires or d) grip strength to assign a level
of dexterity. The aim of this summer project was to pilot a new measurement device that uses
accelerometers. Over the summer the suitability of this device has been piloted with healthy
control participants and algorithms for calculating accurate assessment of dexterity have been
developed.
A procedure was developed and refined which included 10 tasks, 3 unilateral and 7 bilateral,
mainly derived from other validated dexterity and functional measures such as the Sequential
Occupational Dexterity Assessment and the Health Assessment Questionnaire (HAQ). The
tasks were: 1) picking up a pen; 2) writing a sentence; 3) turning a round door knob; 4)
opening a previously opened jar; 5) opening a child-proof pill bottle; 6) patting the head
while rubbing the stomach; 7) a repeated flexion to extension movement of the index finger;
8) buttoning and unbuttoning a man’s shirt; 9) buttoning and unbuttoning a lady’s shirt and
10) opening the wrapper of a sweet.
Participants also completed a standard grip strength test using a hand dynamometer, the HAQ
and the Quick Disabilities of the Arm Shoulder and Hand questionnaire to validate data
generated by the accelerometer device. The tasks were standardised by, for example setting
an exact distance to reach the pen and the amount of force required to open the jar. The
accelerometry recordings can be used to segment components of the tasks that remain
constant, as shown in Figure 1 for the recording of an example participant opening a jar.
The procedure was trialled on 29 participants without arthritis. The sample had a mean age of
39.9 (SD 14.2) years. The procedure was also trialled on one participant with RA and no
feasibility issues were encountered. Data were collected on anxiety, depression, illness
perceptions, diet, exercise, smoking status, sleep quality, and any medications and
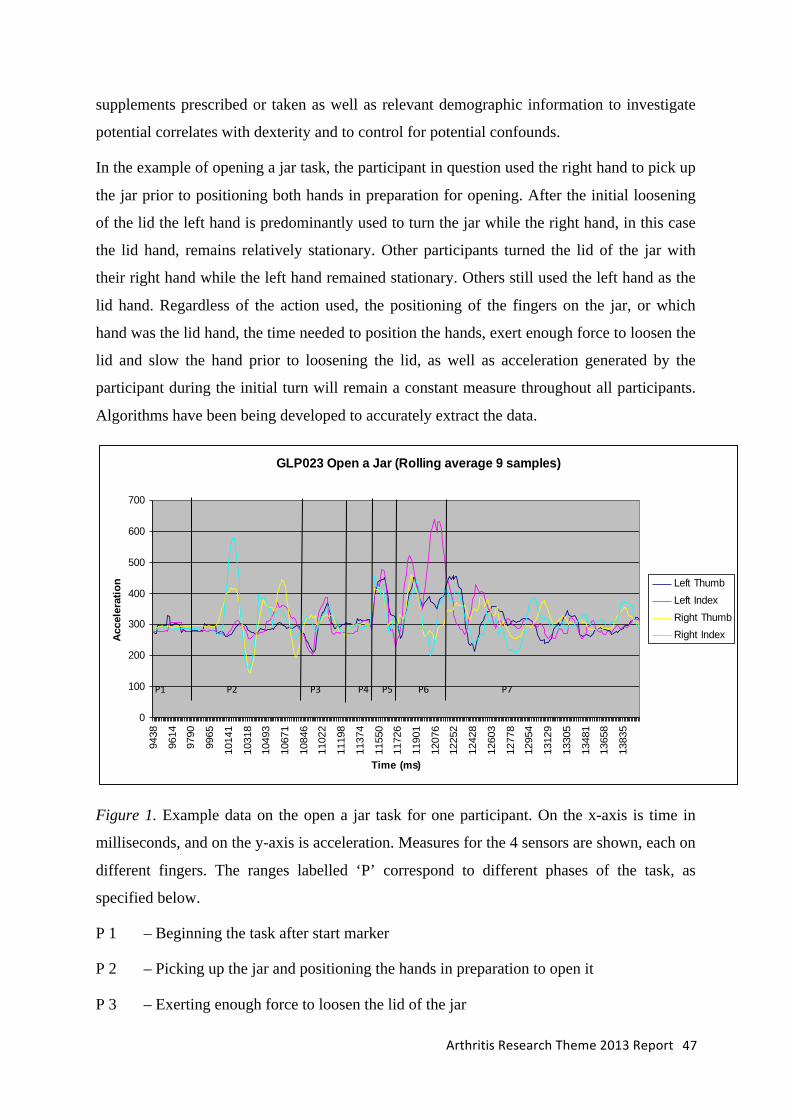
Arthritis Research Theme 2013 Report
47
supplements prescribed or taken as well as relevant demographic information to investigate
potential correlates with dexterity and to control for potential confounds.
In the example of opening a jar task, the participant in question used the right hand to pick up
the jar prior to positioning both hands in preparation for opening. After the initial loosening
of the lid the left hand is predominantly used to turn the jar while the right hand, in this case
the lid hand, remains relatively stationary. Other participants turned the lid of the jar with
their right hand while the left hand remained stationary. Others still used the left hand as the
lid hand. Regardless of the action used, the positioning of the fingers on the jar, or which
hand was the lid hand, the time needed to position the hands, exert enough force to loosen the
lid and slow the hand prior to loosening the lid, as well as acceleration generated by the
participant during the initial turn will remain a constant measure throughout all participants.
Algorithms have been being developed to accurately extract the data.
Figure 1. Example data on the open a jar task for one participant. On the x-axis is time in
milliseconds, and on the y-axis is acceleration. Measures for the 4 sensors are shown, each on
different fingers. The ranges labelled ‘P’ correspond to different phases of the task, as
specified below.
P 1 – Beginning the task after start marker
P 2 – Picking up the jar and positioning the hands in preparation to open it
P 3 – Exerting enough force to loosen the lid of the jar
GLP023 Open a Jar (Rolling average 9 samples)
0
100
200
300
400
500
600
700
9438
9614
9790
9965
1014
1
1031
8
1049
3
1067
1
1084
6
1102
2
1119
8
1137
4
1155
0
1172
6
1190
1
1207
6
1225
2
1242
8
1260
3
1277
8
1295
4
1312
9
1330
5
1348
1
1365
8
1383
5
Time (ms)
Acc
eler
atio
n Left ThumbLeft IndexRight ThumbRight Index
P1 P2 P3 P4 P5 P6 P7
Arthritis Research Theme 2013 Report
48
P 4 – Acceleration generated once the lid was loose
P 5 – Deceleration generated after the lid has moved
P 6 – Acceleration generated from second turn
P 7 – Deceleration from second turn
P2 to 7 – Time taken to complete the entire task
Research is continuing on the suitability of the device as a measure of dexterity in a larger
sample of RA patients. Ethical approval has been granted by the University of Otago Human
Ethics Committee (Health) and locality approval is still in the process of being given by
Health Research South to recruit RA patients from the Dunedin Hospital Rheumatology
Department. The pilot phase with healthy controls has ensured the protocol runs smoothly
whilst also providing normative data on the general population.
This preliminary investigation indicates that the dexterity measuring device has the ability to
delineate between a number of components that make up an individual task. This segmenting
provides an accurate assessment of which component(s) of a task RA patients have the most
difficulty with.
![Ankylosing spondylitis and related conditions - NHS Wales1].pdf · Condition Ankylosing spondylitis Ankylosing spondylitis and related conditions This booklet provides information](https://static.fdocuments.net/doc/165x107/5d53eb2788c993a4728b841d/ankylosing-spondylitis-and-related-conditions-nhs-1pdf-condition-ankylosing.jpg)