UnitedHealthcare Plans - Broker Home Pagebroker.uhc.com/assets/OR KA (51+) Medical & Pharmacy...
12
UnitedHealthcare Plans Key Accounts 51+ Medical and Pharmacy Plans Effective January 1, 2014 OREGON – Key Accounts A variety of plan designs, ranging from network-based solutions that promote consumer engagement to traditional designs that focus on primary care.
Transcript of UnitedHealthcare Plans - Broker Home Pagebroker.uhc.com/assets/OR KA (51+) Medical & Pharmacy...
UnitedHealthcare Plans
Key Accounts 51+ Medical and Pharmacy Plans
Effective January 1, 2014
OREGON – Key Accounts
A variety of plan designs, ranging from network-based solutions that promote consumer engagement to traditional designs that focus on primary care.

Plan Categories DefinitionFlat Copay} Flat Copay plans for PCP and specialist o ce visits
Premier } Split Copay plans that incorporate the UnitedHealth Premium® designation program for specialists
Premier FlexPoint } Split Copay plans that incorporate the UnitedHealth Premium designation program for specialists.
Applicable specialist copayment for limited number of visits
HSA} High-deductible plans that are HSA-eligible and can integrate Optum HSA accounts
Consumer} Plan designs that engage members in their health care decisions
UnitedHealthcare Navigate®
} Network-only plans that utilize a PCP to manage and direct a member’s care
UnitedHealthcare Navigate Balanced®
} Network-only plans that utilize a PCP to manage and direct a member’s care while also oering lower coverage for visits to a network specialist without a referral
Navigate HSA} Navigate plans that are HSA-eligible and can integrate Optum HSA accounts
Navigate Balanced HSA } Navigate Balanced plans that are HSA-eligible and can integrate Optum HSA accounts
$0 Copay for Children} Family-friendly Flat Copay and Navigate plans with a $0 PCP network copayment for children under age 19
Non-Differential PPO } Coinsurance plans for employees outside the UnitedHealthcare network service area
Pharmacy } Pharmacy plans with 3 or 4 tiers can be paired with medical plans
1
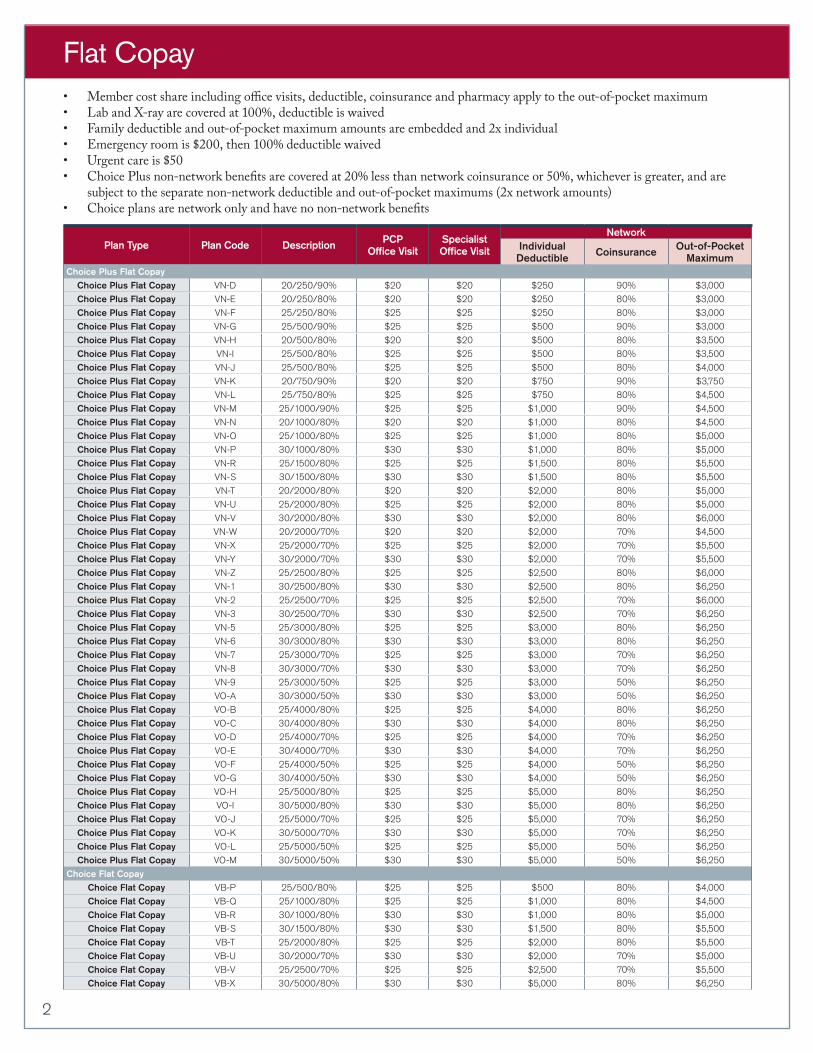
• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Lab and X-ray are covered at 100%, deductible is waived• Family deductible and out-of-pocket maximum amounts are embedded and 2x individual• Emergency room is $200, then 100% deductible waived• Urgent care is $50• Choice Plus non-network bene�ts are covered at 20% less than network coinsurance or 50%, whichever is greater, and are
subject to the separate non-network deductible and out-of-pocket maximums (2x network amounts)• Choice plans are network only and have no non-network bene�ts
Flat Copay
Plan Type Plan Code Description PCP Office Visit
Specialist Office Visit
NetworkIndividual Deductible Coinsurance Out-of-Pocket
MaximumChoice Plus Flat Copay
Choice Plus Flat Copay VN-D 20/250/90% $20 $20 $250 90% $3,000
Choice Plus Flat Copay VN-E 20/250/80% $20 $20 $250 80% $3,000
Choice Plus Flat Copay VN-F 25/250/80% $25 $25 $250 80% $3,000
Choice Plus Flat Copay VN-G 25/500/90% $25 $25 $500 90% $3,000
Choice Plus Flat Copay VN-H 20/500/80% $20 $20 $500 80% $3,500
Choice Plus Flat Copay VN-I 25/500/80% $25 $25 $500 80% $3,500
Choice Plus Flat Copay VN-J 25/500/80% $25 $25 $500 80% $4,000
Choice Plus Flat Copay VN-K 20/750/90% $20 $20 $750 90% $3,750
Choice Plus Flat Copay VN-L 25/750/80% $25 $25 $750 80% $4,500
Choice Plus Flat Copay VN-M 25/1000/90% $25 $25 $1,000 90% $4,500
Choice Plus Flat Copay VN-N 20/1000/80% $20 $20 $1,000 80% $4,500
Choice Plus Flat Copay VN-O 25/1000/80% $25 $25 $1,000 80% $5,000
Choice Plus Flat Copay VN-P 30/1000/80% $30 $30 $1,000 80% $5,000
Choice Plus Flat Copay VN-R 25/1500/80% $25 $25 $1,500 80% $5,500
Choice Plus Flat Copay VN-S 30/1500/80% $30 $30 $1,500 80% $5,500
Choice Plus Flat Copay VN-T 20/2000/80% $20 $20 $2,000 80% $5,000
Choice Plus Flat Copay VN-U 25/2000/80% $25 $25 $2,000 80% $5,000
Choice Plus Flat Copay VN-V 30/2000/80% $30 $30 $2,000 80% $6,000
Choice Plus Flat Copay VN-W 20/2000/70% $20 $20 $2,000 70% $4,500
Choice Plus Flat Copay VN-X 25/2000/70% $25 $25 $2,000 70% $5,500
Choice Plus Flat Copay VN-Y 30/2000/70% $30 $30 $2,000 70% $5,500
Choice Plus Flat Copay VN-Z 25/2500/80% $25 $25 $2,500 80% $6,000
Choice Plus Flat Copay VN-1 30/2500/80% $30 $30 $2,500 80% $6,250
Choice Plus Flat Copay VN-2 25/2500/70% $25 $25 $2,500 70% $6,000
Choice Plus Flat Copay VN-3 30/2500/70% $30 $30 $2,500 70% $6,250
Choice Plus Flat Copay VN-5 25/3000/80% $25 $25 $3,000 80% $6,250
Choice Plus Flat Copay VN-6 30/3000/80% $30 $30 $3,000 80% $6,250
Choice Plus Flat Copay VN-7 25/3000/70% $25 $25 $3,000 70% $6,250
Choice Plus Flat Copay VN-8 30/3000/70% $30 $30 $3,000 70% $6,250
Choice Plus Flat Copay VN-9 25/3000/50% $25 $25 $3,000 50% $6,250
Choice Plus Flat Copay VO-A 30/3000/50% $30 $30 $3,000 50% $6,250
Choice Plus Flat Copay VO-B 25/4000/80% $25 $25 $4,000 80% $6,250
Choice Plus Flat Copay VO-C 30/4000/80% $30 $30 $4,000 80% $6,250
Choice Plus Flat Copay VO-D 25/4000/70% $25 $25 $4,000 70% $6,250
Choice Plus Flat Copay VO-E 30/4000/70% $30 $30 $4,000 70% $6,250
Choice Plus Flat Copay VO-F 25/4000/50% $25 $25 $4,000 50% $6,250
Choice Plus Flat Copay VO-G 30/4000/50% $30 $30 $4,000 50% $6,250
Choice Plus Flat Copay VO-H 25/5000/80% $25 $25 $5,000 80% $6,250
Choice Plus Flat Copay VO-I 30/5000/80% $30 $30 $5,000 80% $6,250
Choice Plus Flat Copay VO-J 25/5000/70% $25 $25 $5,000 70% $6,250
Choice Plus Flat Copay VO-K 30/5000/70% $30 $30 $5,000 70% $6,250
Choice Plus Flat Copay VO-L 25/5000/50% $25 $25 $5,000 50% $6,250
Choice Plus Flat Copay VO-M 30/5000/50% $30 $30 $5,000 50% $6,250
Choice Flat CopayChoice Flat Copay VB-P 25/500/80% $25 $25 $500 80% $4,000
Choice Flat Copay VB-Q 25/1000/80% $25 $25 $1,000 80% $4,500
Choice Flat Copay VB-R 30/1000/80% $30 $30 $1,000 80% $5,000
Choice Flat Copay VB-S 30/1500/80% $30 $30 $1,500 80% $5,500
Choice Flat Copay VB-T 25/2000/80% $25 $25 $2,000 80% $5,500
Choice Flat Copay VB-U 30/2000/70% $30 $30 $2,000 70% $5,000
Choice Flat Copay VB-V 25/2500/70% $25 $25 $2,500 70% $5,500
Choice Flat Copay VB-X 30/5000/80% $30 $30 $5,000 80% $6,250
2
Plan Type Plan Code Description PCP Office Visit
Premium Designated Specialist Office Visit
Non-Premium Designated Specialist Office Visit
Network
Individual Deductible Coinsurance
Out-of-Pocket
MaximumChoice Plus Premier
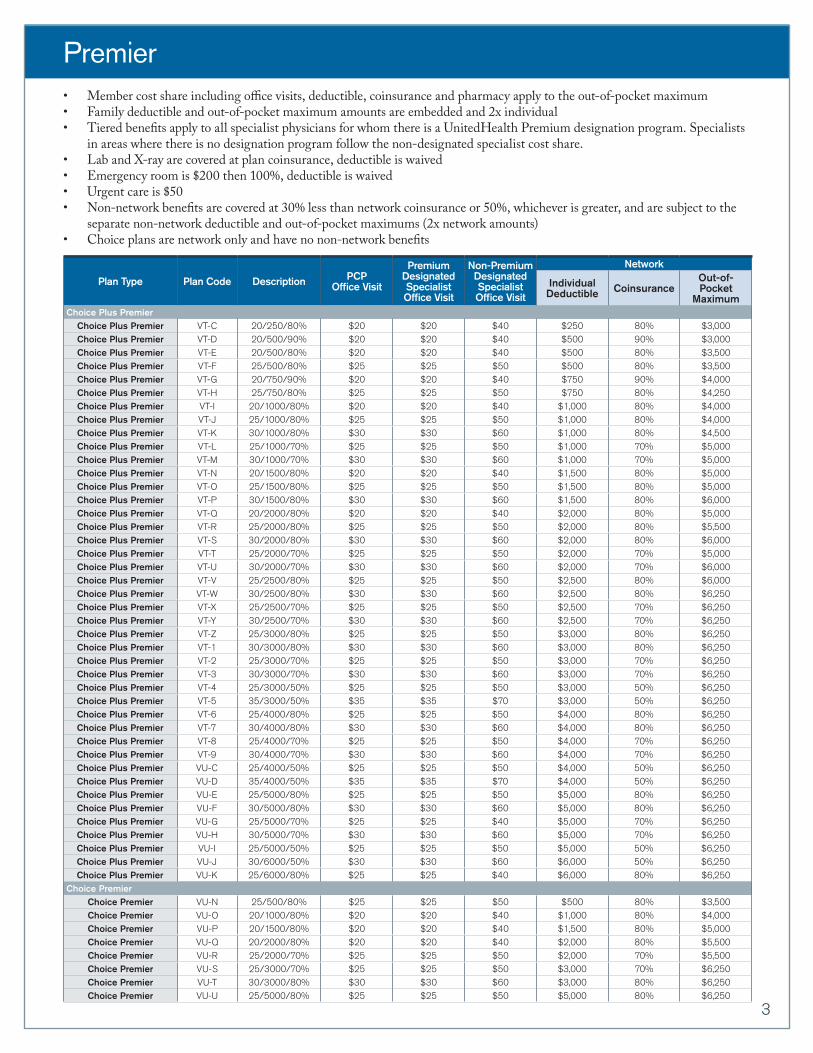
Choice Plus Premier VT-C 20/250/80% $20 $20 $40 $250 80% $3,000Choice Plus Premier VT-D 20/500/90% $20 $20 $40 $500 90% $3,000Choice Plus Premier VT-E 20/500/80% $20 $20 $40 $500 80% $3,500Choice Plus Premier VT-F 25/500/80% $25 $25 $50 $500 80% $3,500Choice Plus Premier VT-G 20/750/90% $20 $20 $40 $750 90% $4,000Choice Plus Premier VT-H 25/750/80% $25 $25 $50 $750 80% $4,250Choice Plus Premier VT-I 20/1000/80% $20 $20 $40 $1,000 80% $4,000Choice Plus Premier VT-J 25/1000/80% $25 $25 $50 $1,000 80% $4,000Choice Plus Premier VT-K 30/1000/80% $30 $30 $60 $1,000 80% $4,500Choice Plus Premier VT-L 25/1000/70% $25 $25 $50 $1,000 70% $5,000Choice Plus Premier VT-M 30/1000/70% $30 $30 $60 $1,000 70% $5,000Choice Plus Premier VT-N 20/1500/80% $20 $20 $40 $1,500 80% $5,000Choice Plus Premier VT-O 25/1500/80% $25 $25 $50 $1,500 80% $5,000Choice Plus Premier VT-P 30/1500/80% $30 $30 $60 $1,500 80% $6,000Choice Plus Premier VT-Q 20/2000/80% $20 $20 $40 $2,000 80% $5,000Choice Plus Premier VT-R 25/2000/80% $25 $25 $50 $2,000 80% $5,500Choice Plus Premier VT-S 30/2000/80% $30 $30 $60 $2,000 80% $6,000Choice Plus Premier VT-T 25/2000/70% $25 $25 $50 $2,000 70% $5,000Choice Plus Premier VT-U 30/2000/70% $30 $30 $60 $2,000 70% $6,000Choice Plus Premier VT-V 25/2500/80% $25 $25 $50 $2,500 80% $6,000Choice Plus Premier VT-W 30/2500/80% $30 $30 $60 $2,500 80% $6,250Choice Plus Premier VT-X 25/2500/70% $25 $25 $50 $2,500 70% $6,250Choice Plus Premier VT-Y 30/2500/70% $30 $30 $60 $2,500 70% $6,250Choice Plus Premier VT-Z 25/3000/80% $25 $25 $50 $3,000 80% $6,250Choice Plus Premier VT-1 30/3000/80% $30 $30 $60 $3,000 80% $6,250Choice Plus Premier VT-2 25/3000/70% $25 $25 $50 $3,000 70% $6,250Choice Plus Premier VT-3 30/3000/70% $30 $30 $60 $3,000 70% $6,250Choice Plus Premier VT-4 25/3000/50% $25 $25 $50 $3,000 50% $6,250Choice Plus Premier VT-5 35/3000/50% $35 $35 $70 $3,000 50% $6,250Choice Plus Premier VT-6 25/4000/80% $25 $25 $50 $4,000 80% $6,250Choice Plus Premier VT-7 30/4000/80% $30 $30 $60 $4,000 80% $6,250Choice Plus Premier VT-8 25/4000/70% $25 $25 $50 $4,000 70% $6,250Choice Plus Premier VT-9 30/4000/70% $30 $30 $60 $4,000 70% $6,250Choice Plus Premier VU-C 25/4000/50% $25 $25 $50 $4,000 50% $6,250Choice Plus Premier VU-D 35/4000/50% $35 $35 $70 $4,000 50% $6,250Choice Plus Premier VU-E 25/5000/80% $25 $25 $50 $5,000 80% $6,250Choice Plus Premier VU-F 30/5000/80% $30 $30 $60 $5,000 80% $6,250Choice Plus Premier VU-G 25/5000/70% $25 $25 $40 $5,000 70% $6,250Choice Plus Premier VU-H 30/5000/70% $30 $30 $60 $5,000 70% $6,250Choice Plus Premier VU-I 25/5000/50% $25 $25 $50 $5,000 50% $6,250Choice Plus Premier VU-J 30/6000/50% $30 $30 $60 $6,000 50% $6,250Choice Plus Premier VU-K 25/6000/80% $25 $25 $40 $6,000 80% $6,250
Choice PremierChoice Premier VU-N 25/500/80% $25 $25 $50 $500 80% $3,500Choice Premier VU-O 20/1000/80% $20 $20 $40 $1,000 80% $4,000Choice Premier VU-P 20/1500/80% $20 $20 $40 $1,500 80% $5,000Choice Premier VU-Q 20/2000/80% $20 $20 $40 $2,000 80% $5,500Choice Premier VU-R 25/2000/70% $25 $25 $50 $2,000 70% $5,500Choice Premier VU-S 25/3000/70% $25 $25 $50 $3,000 70% $6,250Choice Premier VU-T 30/3000/80% $30 $30 $60 $3,000 80% $6,250Choice Premier VU-U 25/5000/80% $25 $25 $50 $5,000 80% $6,250
Premier• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Family deductible and out-of-pocket maximum amounts are embedded and 2x individual• Tiered bene�ts apply to all specialist physicians for whom there is a UnitedHealth Premium designation program. Specialists
in areas where there is no designation program follow the non-designated specialist cost share.• Lab and X-ray are covered at plan coinsurance, deductible is waived• Emergency room is $200 then 100%, deductible is waived• Urgent care is $50• Non-network bene�ts are covered at 30% less than network coinsurance or 50%, whichever is greater, and are subject to the
separate non-network deductible and out-of-pocket maximums (2x network amounts)• Choice plans are network only and have no non-network bene�ts
3
Plan Type Plan Code Description
PCP Office Visit
Premium Designated Specialist Office Visit
Non-Premium Designated Specialist Office Visit
Office Visit
Limits
Network
Individual Deductible Coinsurance
Out-of-Pocket
MaximumChoice Plus Premier FlexPoint
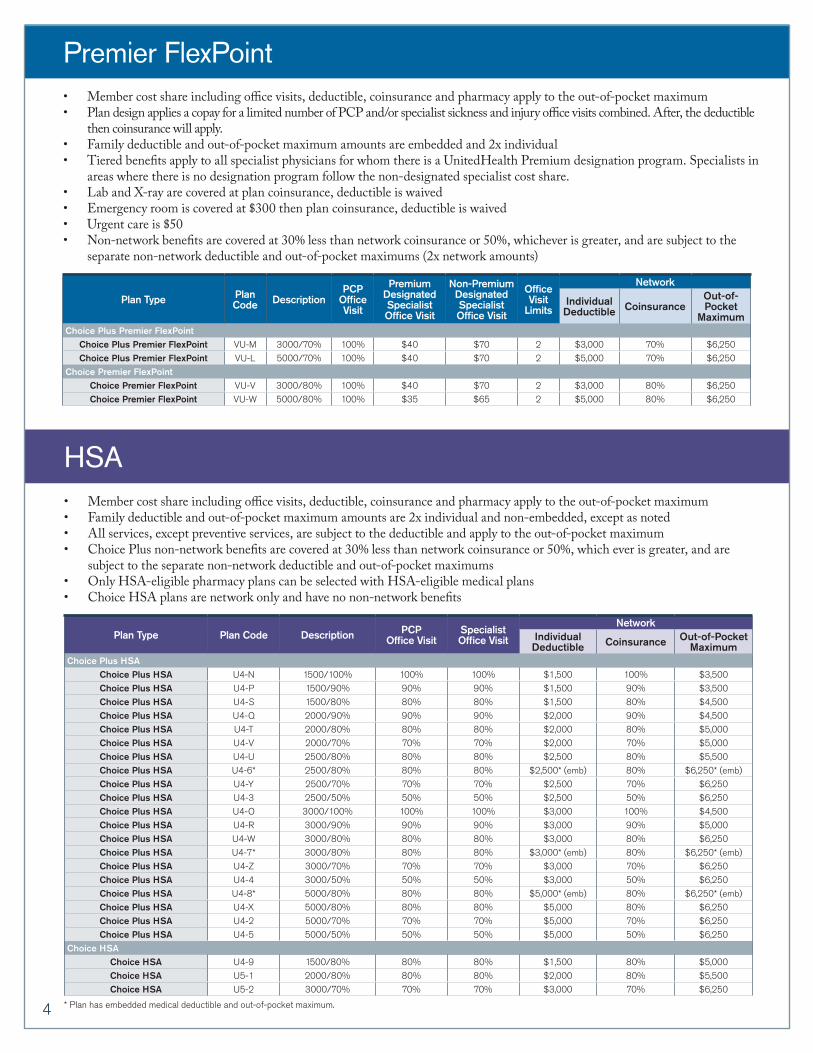
Choice Plus Premier FlexPoint VU-M 3000/70% 100% $40 $70 2 $3,000 70% $6,250
Choice Plus Premier FlexPoint VU-L 5000/70% 100% $40 $70 2 $5,000 70% $6,250
Choice Premier FlexPointChoice Premier FlexPoint VU-V 3000/80% 100% $40 $70 2 $3,000 80% $6,250
Choice Premier FlexPoint VU-W 5000/80% 100% $35 $65 2 $5,000 80% $6,250
Premier FlexPoint• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum • Plan design applies a copay for a limited number of PCP and/or specialist sickness and injury o ce visits combined. After, the deductible
then coinsurance will apply.• Family deductible and out-of-pocket maximum amounts are embedded and 2x individual• Tiered bene�ts apply to all specialist physicians for whom there is a UnitedHealth Premium designation program. Specialists in
areas where there is no designation program follow the non-designated specialist cost share.• Lab and X-ray are covered at plan coinsurance, deductible is waived• Emergency room is covered at $300 then plan coinsurance, deductible is waived• Urgent care is $50• Non-network bene�ts are covered at 30% less than network coinsurance or 50%, whichever is greater, and are subject to the
separate non-network deductible and out-of-pocket maximums (2x network amounts)
Plan Type Plan Code Description PCP Office Visit
Specialist Office Visit
NetworkIndividual Deductible Coinsurance Out-of-Pocket
MaximumChoice Plus HSA
Choice Plus HSA U4-N 1500/100% 100% 100% $1,500 100% $3,500
Choice Plus HSA U4-P 1500/90% 90% 90% $1,500 90% $3,500
Choice Plus HSA U4-S 1500/80% 80% 80% $1,500 80% $4,500
Choice Plus HSA U4-Q 2000/90% 90% 90% $2,000 90% $4,500
Choice Plus HSA U4-T 2000/80% 80% 80% $2,000 80% $5,000
Choice Plus HSA U4-V 2000/70% 70% 70% $2,000 70% $5,000
Choice Plus HSA U4-U 2500/80% 80% 80% $2,500 80% $5,500
Choice Plus HSA U4-6* 2500/80% 80% 80% $2,500* (emb) 80% $6,250* (emb)
Choice Plus HSA U4-Y 2500/70% 70% 70% $2,500 70% $6,250
Choice Plus HSA U4-3 2500/50% 50% 50% $2,500 50% $6,250
Choice Plus HSA U4-O 3000/100% 100% 100% $3,000 100% $4,500
Choice Plus HSA U4-R 3000/90% 90% 90% $3,000 90% $5,000
Choice Plus HSA U4-W 3000/80% 80% 80% $3,000 80% $6,250
Choice Plus HSA U4-7* 3000/80% 80% 80% $3,000* (emb) 80% $6,250* (emb)
Choice Plus HSA U4-Z 3000/70% 70% 70% $3,000 70% $6,250
Choice Plus HSA U4-4 3000/50% 50% 50% $3,000 50% $6,250
Choice Plus HSA U4-8* 5000/80% 80% 80% $5,000* (emb) 80% $6,250* (emb)
Choice Plus HSA U4-X 5000/80% 80% 80% $5,000 80% $6,250
Choice Plus HSA U4-2 5000/70% 70% 70% $5,000 70% $6,250
Choice Plus HSA U4-5 5000/50% 50% 50% $5,000 50% $6,250
Choice HSAChoice HSA U4-9 1500/80% 80% 80% $1,500 80% $5,000
Choice HSA U5-1 2000/80% 80% 80% $2,000 80% $5,500
Choice HSA U5-2 3000/70% 70% 70% $3,000 70% $6,250
* Plan has embedded medical deductible and out-of-pocket maximum.
HSA• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Family deductible and out-of-pocket maximum amounts are 2x individual and non-embedded, except as noted• All services, except preventive services, are subject to the deductible and apply to the out-of-pocket maximum• Choice Plus non-network bene�ts are covered at 30% less than network coinsurance or 50%, which ever is greater, and are
subject to the separate non-network deductible and out-of-pocket maximums• Only HSA-eligible pharmacy plans can be selected with HSA-eligible medical plans• Choice HSA plans are network only and have no non-network bene�ts
4
Plan Type Plan Code Description PCP Office Visit
Specialist Office Visit
NetworkIndividual Deductible Coinsurance Out-of-Pocket
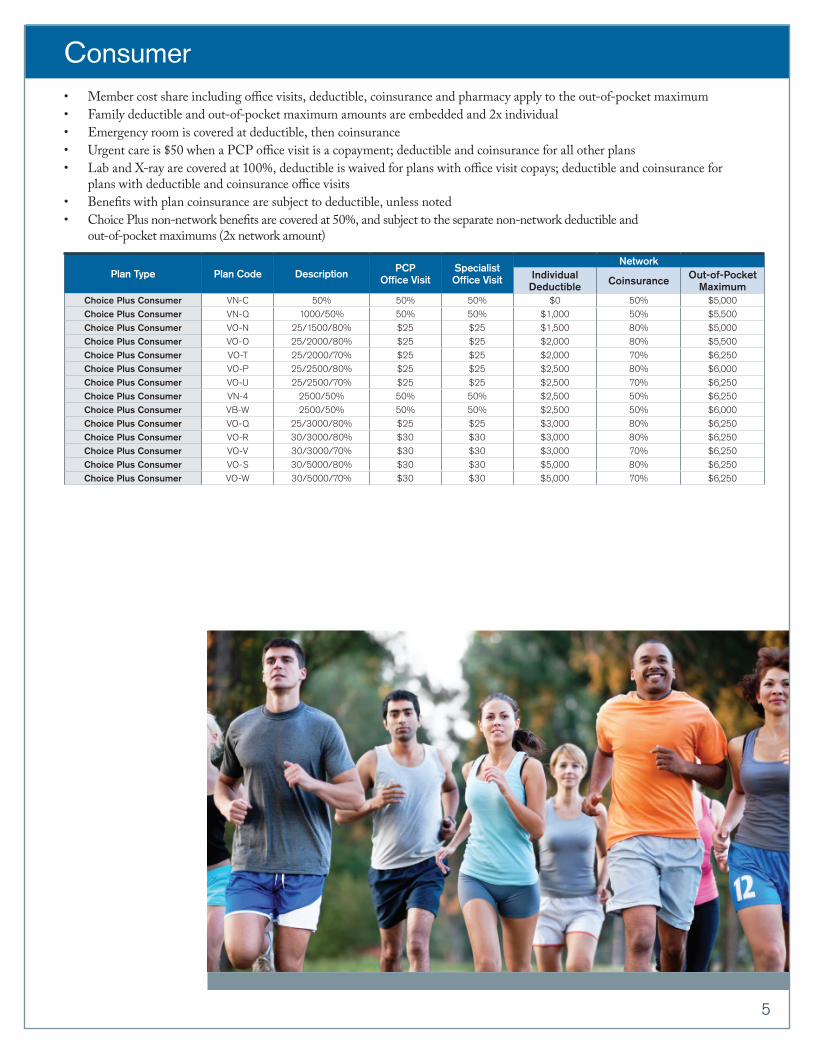
MaximumChoice Plus Consumer VN-C 50% 50% 50% $0 50% $5,000
Choice Plus Consumer VN-Q 1000/50% 50% 50% $1,000 50% $5,500
Choice Plus Consumer VO-N 25/1500/80% $25 $25 $1,500 80% $5,000
Choice Plus Consumer VO-O 25/2000/80% $25 $25 $2,000 80% $5,500
Choice Plus Consumer VO-T 25/2000/70% $25 $25 $2,000 70% $6,250
Choice Plus Consumer VO-P 25/2500/80% $25 $25 $2,500 80% $6,000
Choice Plus Consumer VO-U 25/2500/70% $25 $25 $2,500 70% $6,250
Choice Plus Consumer VN-4 2500/50% 50% 50% $2,500 50% $6,250
Choice Plus Consumer VB-W 2500/50% 50% 50% $2,500 50% $6,000
Choice Plus Consumer VO-Q 25/3000/80% $25 $25 $3,000 80% $6,250
Choice Plus Consumer VO-R 30/3000/80% $30 $30 $3,000 80% $6,250
Choice Plus Consumer VO-V 30/3000/70% $30 $30 $3,000 70% $6,250
Choice Plus Consumer VO-S 30/5000/80% $30 $30 $5,000 80% $6,250
Choice Plus Consumer VO-W 30/5000/70% $30 $30 $5,000 70% $6,250
Consumer• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Family deductible and out-of-pocket maximum amounts are embedded and 2x individual• Emergency room is covered at deductible, then coinsurance• Urgent care is $50 when a PCP o ce visit is a copayment; deductible and coinsurance for all other plans• Lab and X-ray are covered at 100%, deductible is waived for plans with o ce visit copays; deductible and coinsurance for
plans with deductible and coinsurance o ce visits• Bene�ts with plan coinsurance are subject to deductible, unless noted• Choice Plus non-network bene�ts are covered at 50%, and subject to the separate non-network deductible and
out-of-pocket maximums (2x network amount)
5
Plan Type Plan Code Description
PCP Office Visit
Specialist Office Visit
with Referral
Specialist Office Visit
without Referral
Network
Individual Deductible Coinsurance
Coinsurance without Referral
Out-of-Pocket
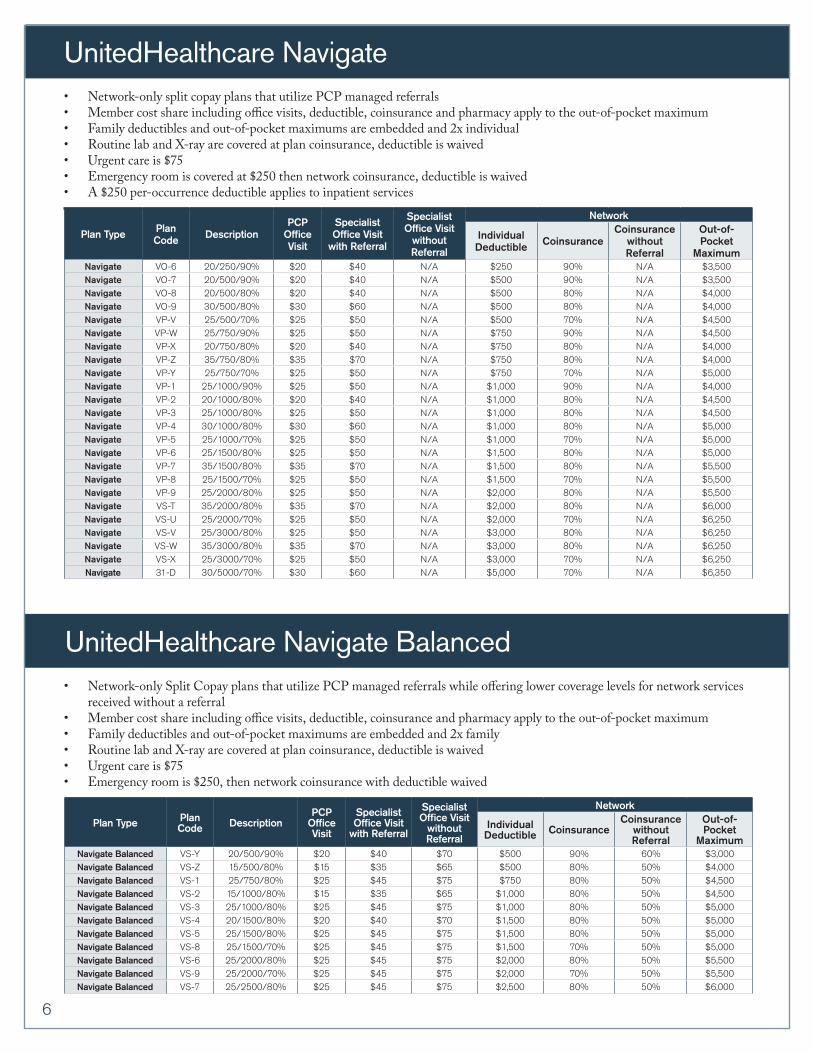
MaximumNavigate VO-6 20/250/90% $20 $40 N/A $250 90% N/A $3,500Navigate VO-7 20/500/90% $20 $40 N/A $500 90% N/A $3,500Navigate VO-8 20/500/80% $20 $40 N/A $500 80% N/A $4,000Navigate VO-9 30/500/80% $30 $60 N/A $500 80% N/A $4,000Navigate VP-V 25/500/70% $25 $50 N/A $500 70% N/A $4,500Navigate VP-W 25/750/90% $25 $50 N/A $750 90% N/A $4,500Navigate VP-X 20/750/80% $20 $40 N/A $750 80% N/A $4,000Navigate VP-Z 35/750/80% $35 $70 N/A $750 80% N/A $4,000Navigate VP-Y 25/750/70% $25 $50 N/A $750 70% N/A $5,000Navigate VP-1 25/1000/90% $25 $50 N/A $1,000 90% N/A $4,000Navigate VP-2 20/1000/80% $20 $40 N/A $1,000 80% N/A $4,500Navigate VP-3 25/1000/80% $25 $50 N/A $1,000 80% N/A $4,500Navigate VP-4 30/1000/80% $30 $60 N/A $1,000 80% N/A $5,000Navigate VP-5 25/1000/70% $25 $50 N/A $1,000 70% N/A $5,000Navigate VP-6 25/1500/80% $25 $50 N/A $1,500 80% N/A $5,000Navigate VP-7 35/1500/80% $35 $70 N/A $1,500 80% N/A $5,500Navigate VP-8 25/1500/70% $25 $50 N/A $1,500 70% N/A $5,500Navigate VP-9 25/2000/80% $25 $50 N/A $2,000 80% N/A $5,500Navigate VS-T 35/2000/80% $35 $70 N/A $2,000 80% N/A $6,000Navigate VS-U 25/2000/70% $25 $50 N/A $2,000 70% N/A $6,250Navigate VS-V 25/3000/80% $25 $50 N/A $3,000 80% N/A $6,250 Navigate VS-W 35/3000/80% $35 $70 N/A $3,000 80% N/A $6,250 Navigate VS-X 25/3000/70% $25 $50 N/A $3,000 70% N/A $6,250 Navigate 31-D 30/5000/70% $30 $60 N/A $5,000 70% N/A $6,350
UnitedHealthcare Navigate• Network-only split copay plans that utilize PCP managed referrals• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Family deductibles and out-of-pocket maximums are embedded and 2x individual • Routine lab and X-ray are covered at plan coinsurance, deductible is waived• Urgent care is $75• Emergency room is covered at $250 then network coinsurance, deductible is waived• A $250 per-occurrence deductible applies to inpatient services
Plan Type Plan Code Description
PCP Office Visit
Specialist Office Visit
with Referral
Specialist Office Visit
without Referral
Network
Individual Deductible Coinsurance
Coinsurance without Referral
Out-of-Pocket
MaximumNavigate Balanced VS-Y 20/500/90% $20 $40 $70 $500 90% 60% $3,000Navigate Balanced VS-Z 15/500/80% $15 $35 $65 $500 80% 50% $4,000Navigate Balanced VS-1 25/750/80% $25 $45 $75 $750 80% 50% $4,500Navigate Balanced VS-2 15/1000/80% $15 $35 $65 $1,000 80% 50% $4,500Navigate Balanced VS-3 25/1000/80% $25 $45 $75 $1,000 80% 50% $5,000Navigate Balanced VS-4 20/1500/80% $20 $40 $70 $1,500 80% 50% $5,000Navigate Balanced VS-5 25/1500/80% $25 $45 $75 $1,500 80% 50% $5,000Navigate Balanced VS-8 25/1500/70% $25 $45 $75 $1,500 70% 50% $5,000Navigate Balanced VS-6 25/2000/80% $25 $45 $75 $2,000 80% 50% $5,500Navigate Balanced VS-9 25/2000/70% $25 $45 $75 $2,000 70% 50% $5,500Navigate Balanced VS-7 25/2500/80% $25 $45 $75 $2,500 80% 50% $6,000
• Network-only Split Copay plans that utilize PCP managed referrals while oering lower coverage levels for network services received without a referral
• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Family deductibles and out-of-pocket maximums are embedded and 2x family• Routine lab and X-ray are covered at plan coinsurance, deductible is waived• Urgent care is $75• Emergency room is $250, then network coinsurance with deductible waived
UnitedHealthcare Navigate Balanced
6
Plan Type Plan Code Description
PCP Office Visit
Specialist Office Visit
with Referral
Specialist Office Visit
without Referral
Network
Individual Deductible Coinsurance
Coinsurance without Referral
Out-of-Pocket
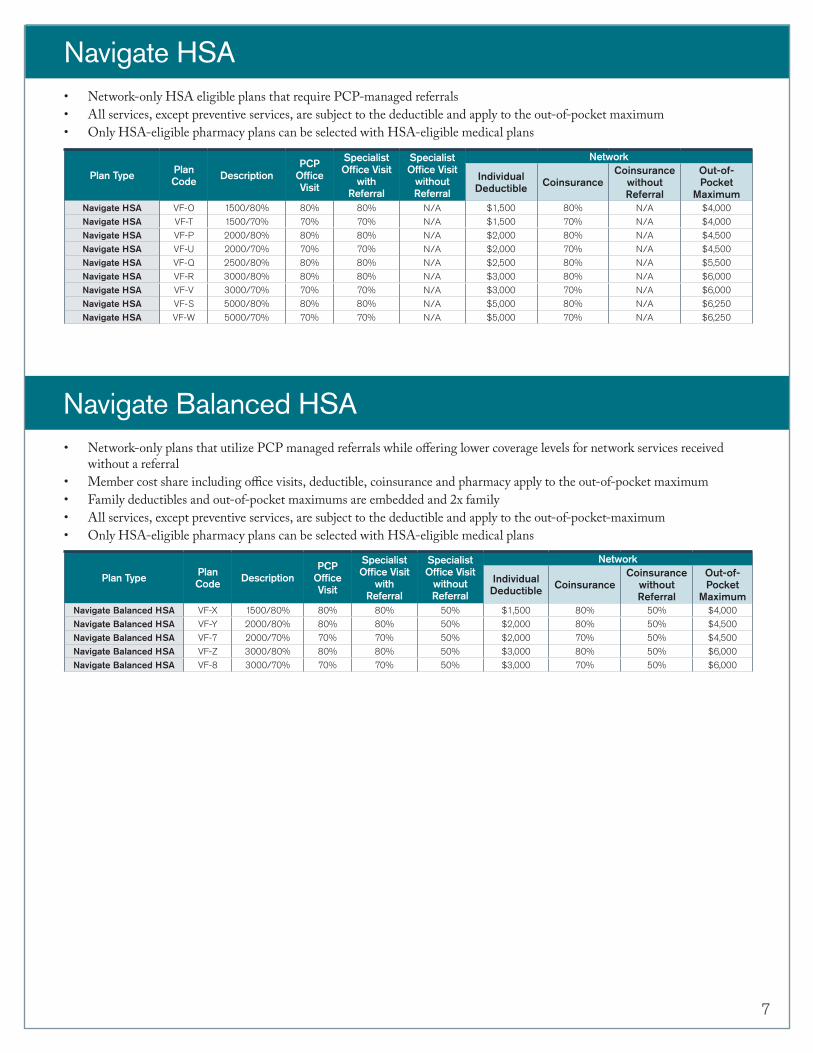
MaximumNavigate HSA VF-O 1500/80% 80% 80% N/A $1,500 80% N/A $4,000
Navigate HSA VF-T 1500/70% 70% 70% N/A $1,500 70% N/A $4,000
Navigate HSA VF-P 2000/80% 80% 80% N/A $2,000 80% N/A $4,500
Navigate HSA VF-U 2000/70% 70% 70% N/A $2,000 70% N/A $4,500
Navigate HSA VF-Q 2500/80% 80% 80% N/A $2,500 80% N/A $5,500
Navigate HSA VF-R 3000/80% 80% 80% N/A $3,000 80% N/A $6,000
Navigate HSA VF-V 3000/70% 70% 70% N/A $3,000 70% N/A $6,000
Navigate HSA VF-S 5000/80% 80% 80% N/A $5,000 80% N/A $6,250
Navigate HSA VF-W 5000/70% 70% 70% N/A $5,000 70% N/A $6,250
Navigate HSA• Network-only HSA eligible plans that require PCP-managed referrals• All services, except preventive services, are subject to the deductible and apply to the out-of-pocket maximum• Only HSA-eligible pharmacy plans can be selected with HSA-eligible medical plans
Plan Type Plan Code Description
PCP Office Visit
Specialist Office Visit
with Referral
Specialist Office Visit
without Referral
Network
Individual Deductible Coinsurance
Coinsurance without Referral
Out-of-Pocket
MaximumNavigate Balanced HSA VF-X 1500/80% 80% 80% 50% $1,500 80% 50% $4,000
Navigate Balanced HSA VF-Y 2000/80% 80% 80% 50% $2,000 80% 50% $4,500
Navigate Balanced HSA VF-7 2000/70% 70% 70% 50% $2,000 70% 50% $4,500
Navigate Balanced HSA VF-Z 3000/80% 80% 80% 50% $3,000 80% 50% $6,000
Navigate Balanced HSA VF-8 3000/70% 70% 70% 50% $3,000 70% 50% $6,000
• Network-only plans that utilize PCP managed referrals while oering lower coverage levels for network services received without a referral
• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Family deductibles and out-of-pocket maximums are embedded and 2x family• All services, except preventive services, are subject to the deductible and apply to the out-of-pocket-maximum• Only HSA-eligible pharmacy plans can be selected with HSA-eligible medical plans
Navigate Balanced HSA
7
Plan Type Plan Code Description
PCP Office Visit
Children’s PCP
Office Visit
Children’s Office
Visit Age Limit
Specialist Office Visit
Network
Individual Deductible Coinsurance
Out-of-Pocket
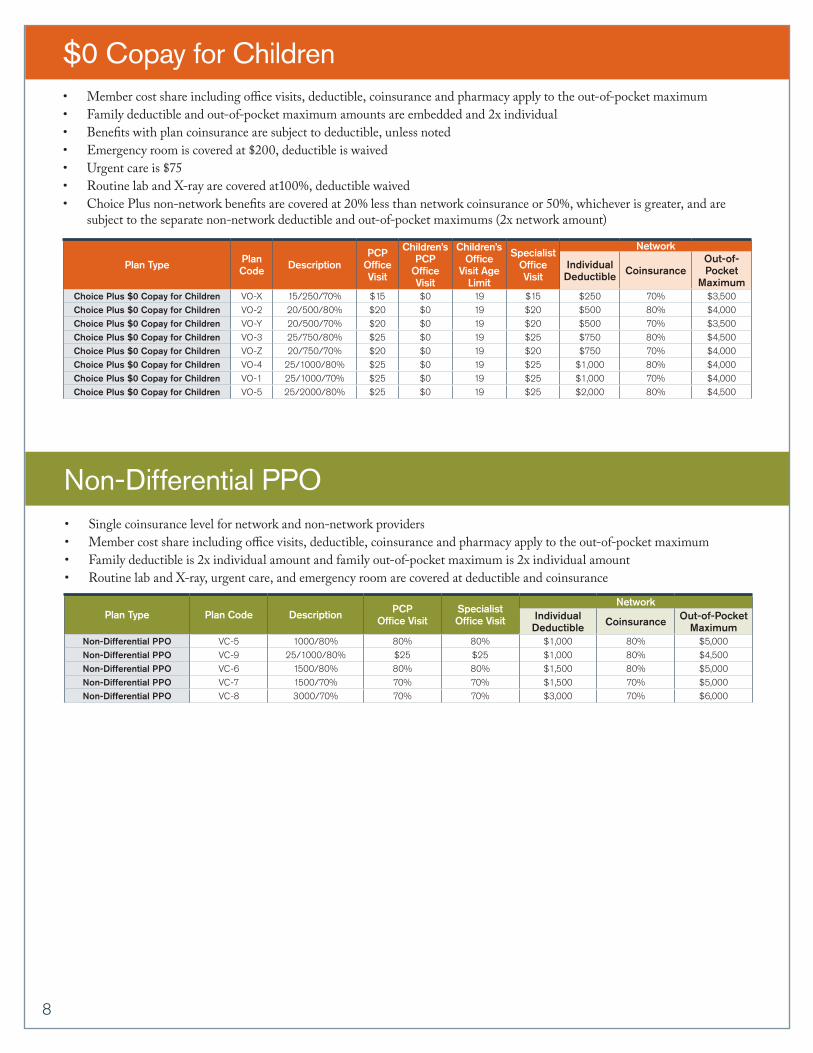
MaximumChoice Plus $0 Copay for Children VO-X 15/250/70% $15 $0 19 $15 $250 70% $3,500
Choice Plus $0 Copay for Children VO-2 20/500/80% $20 $0 19 $20 $500 80% $4,000
Choice Plus $0 Copay for Children VO-Y 20/500/70% $20 $0 19 $20 $500 70% $3,500
Choice Plus $0 Copay for Children VO-3 25/750/80% $25 $0 19 $25 $750 80% $4,500
Choice Plus $0 Copay for Children VO-Z 20/750/70% $20 $0 19 $20 $750 70% $4,000
Choice Plus $0 Copay for Children VO-4 25/1000/80% $25 $0 19 $25 $1,000 80% $4,000
Choice Plus $0 Copay for Children VO-1 25/1000/70% $25 $0 19 $25 $1,000 70% $4,000
Choice Plus $0 Copay for Children VO-5 25/2000/80% $25 $0 19 $25 $2,000 80% $4,500
$0 Copay for Children• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Family deductible and out-of-pocket maximum amounts are embedded and 2x individual• Bene�ts with plan coinsurance are subject to deductible, unless noted• Emergency room is covered at $200, deductible is waived• Urgent care is $75• Routine lab and X-ray are covered at100%, deductible waived• Choice Plus non-network bene�ts are covered at 20% less than network coinsurance or 50%, whichever is greater, and are
subject to the separate non-network deductible and out-of-pocket maximums (2x network amount)
Non-Differential PPO• Single coinsurance level for network and non-network providers• Member cost share including o ce visits, deductible, coinsurance and pharmacy apply to the out-of-pocket maximum• Family deductible is 2x individual amount and family out-of-pocket maximum is 2x individual amount• Routine lab and X-ray, urgent care, and emergency room are covered at deductible and coinsurance
Plan Type Plan Code Description PCP Office Visit
Specialist Office Visit
NetworkIndividual Deductible Coinsurance Out-of-Pocket
MaximumNon-Differential PPO VC-5 1000/80% 80% 80% $1,000 80% $5,000
Non-Differential PPO VC-9 25/1000/80% $25 $25 $1,000 80% $4,500
Non-Differential PPO VC-6 1500/80% 80% 80% $1,500 80% $5,000
Non-Differential PPO VC-7 1500/70% 70% 70% $1,500 70% $5,000
Non-Differential PPO VC-8 3000/70% 70% 70% $3,000 70% $6,000
8
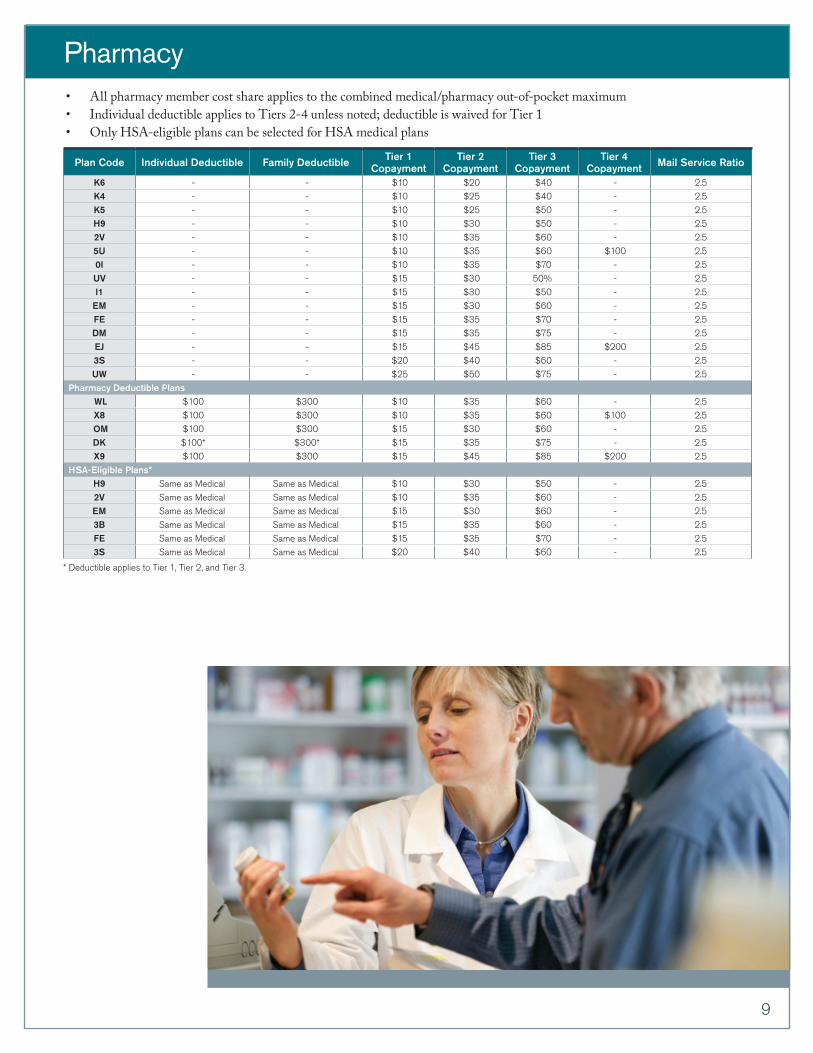
Pharmacy
Plan Code Individual Deductible Family Deductible Tier 1 Copayment
Tier 2 Copayment
Tier 3 Copayment
Tier 4 Copayment Mail Service Ratio
K6 - - $10 $20 $40 - 2.5
K4 - - $10 $25 $40 - 2.5
K5 - - $10 $25 $50 - 2.5
H9 - - $10 $30 $50 - 2.5
2V - - $10 $35 $60 - 2.5
5U - - $10 $35 $60 $100 2.5
0I - - $10 $35 $70 - 2.5
UV - - $15 $30 50% - 2.5
I1 - - $15 $30 $50 - 2.5
EM - - $15 $30 $60 - 2.5
FE - - $15 $35 $70 - 2.5
DM - - $15 $35 $75 - 2.5
EJ - - $15 $45 $85 $200 2.5
3S - - $20 $40 $60 - 2.5
UW - - $25 $50 $75 - 2.5
Pharmacy Deductible Plans WL $100 $300 $10 $35 $60 - 2.5
X8 $100 $300 $10 $35 $60 $100 2.5
OM $100 $300 $15 $30 $60 - 2.5
DK $100* $300* $15 $35 $75 - 2.5
X9 $100 $300 $15 $45 $85 $200 2.5
HSA-Eligible Plans*H9 Same as Medical Same as Medical $10 $30 $50 - 2.5
2V Same as Medical Same as Medical $10 $35 $60 - 2.5
EM Same as Medical Same as Medical $15 $30 $60 - 2.5
3B Same as Medical Same as Medical $15 $35 $60 - 2.5
FE Same as Medical Same as Medical $15 $35 $70 - 2.5
3S Same as Medical Same as Medical $20 $40 $60 - 2.5
* Deductible applies to Tier 1, Tier 2, and Tier 3.
• All pharmacy member cost share applies to the combined medical/pharmacy out-of-pocket maximum• Individual deductible applies to Tiers 2-4 unless noted; deductible is waived for Tier 1• Only HSA-eligible plans can be selected for HSA medical plans
9
The UnitedHealthcare plan with Health Savings Account (HSA) high deductible health plan (HDHP) is designed to comply with IRS requirements so eligible enrollees may open a Health Savings Account through Optum Bank, Member FDIC. The “HSA” refers generally to the UnitedHealthcare HSA product, which includes a HDHP, although at times “HSA” may refer only and specifically to the UnitedHealthcare Health Savings Account, provided in conjunction with Optum Bank and not to the associated HDHP.
For a complete description of the UnitedHealth Premium® Designation program, including details on the methodology used, geographic availability, program limitations and medical specialties participating, please see myuhc.com®.
Insurance coverage provided by or through UnitedHealthcare Insurance Company or its affiliates. Administrative services provided by United HealthCare Services, Inc. or their affiliates.
©2013 United HealthCare Services, Inc.10/13 UHCOR547577-002
Contact your UnitedHealthcare representative for more information.