
UNITED STATES PATENT AND TRADEMARK OFFICE … · A. Scope and Content of the Prior Art ... I...
97
1 UNITED STATES PATENT AND TRADEMARK OFFICE BEFORE THE PATENT TRIAL AND APPEAL BOARD Petitioner, v. Genentech, Inc. Patent Owner Patent No. 7,892,549 Title: TREATMENT WITH ANTI-ERbB2 ANTIBODIES Inter Partes Review No. IPR2017-01122 DECLARATION OF ROBERT EARHART, M.D., Ph.D. IN SUPPORT OF CELLTRION’S PETITION FOR INTER PARTES REVIEW OF U.S. PATENT NO. 7,892,549 1 of 97 Celltrion, Inc., Exhibit 1002
Transcript of UNITED STATES PATENT AND TRADEMARK OFFICE … · A. Scope and Content of the Prior Art ... I...

1
UNITED STATES PATENT AND TRADEMARK OFFICE
BEFORE THE PATENT TRIAL AND APPEAL BOARD
Petitioner, v.
Genentech, Inc. Patent Owner
Patent No. 7,892,549
Title: TREATMENT WITH ANTI-ERbB2 ANTIBODIES
Inter Partes Review No. IPR2017-01122
DECLARATION OF ROBERT EARHART, M.D., Ph.D. IN SUPPORT OF CELLTRION’S PETITION FOR INTER PARTES REVIEW OF
U.S. PATENT NO. 7,892,549
1 of 97 Celltrion, Inc., Exhibit 1002

2
Table of Contents
Page
I. INTRODUCTION ........................................................................................... 4
II. SUMMARY OF OPINIONS ........................................................................... 4
III. QUALIFICATIONS AND EXPERIENCE ..................................................... 5
IV. LEGAL PRINCIPLES ................................................................................... 11
V. LEVEL OF ORDINARY SKILL IN THE ART ........................................... 13
VI. SCIENTIFIC BACKGROUND .................................................................... 13
A. Breast Cancer and its Treatment as of December 1996 ...................... 13
B. Development of Cancer Therapies ...................................................... 20
C. HER2+ Breast Cancer and Its Treatments .......................................... 22
1. Baselga 1996 (Ex. 1020) ........................................................... 24
2. Seidman 1996 (Ex. 1011) ......................................................... 26
3. Pegram 1995 (Ex. 1022) ........................................................... 28
4. Preclinical Studies ..................................................................... 30
D. Combination Therapy for Breast Cancer ............................................ 36
E. Measurements of Efficacy for Cancer Treatments ............................. 41
VII. U.S. PATENT NO. 7,892,549 ....................................................................... 44
A. The Specification of the ’549 Patent ................................................... 44
B. The Claims of the ’549 Patent ............................................................. 46
C. Prosecution History of the ’549 Patent ............................................... 49
VIII. CLAIM CONSTRUCTION .......................................................................... 54
IX. OBVIOUSNESS ANALYSIS ....................................................................... 58
A. Scope and Content of the Prior Art ..................................................... 58
B. Level of Ordinary Skill in the Art ....................................................... 58
C. Differences Between the Claims and the Prior Art and Conclusion of Obviousness ......................................................................................... 59
D. Response To The Sliwkowski Declaration ......................................... 72
2 of 97 Celltrion, Inc., Exhibit 1002

3
1. A Person of Ordinary Skill in the Art Would Not Have Expected an Antagonistic Interaction Between Paclitaxel and Trastuzumab .............................................................................. 72
2. Xenograft Data is a Helpful Tool for Developing Combination Therapies ................................................................................... 79
E. Claim-by-Claim Analysis of Obviousness .......................................... 83
F. Secondary Considerations ................................................................... 90
1. Dr. Hellmann Did Not Point to Data that Established that the Combination of Paclitaxel and Trastuzumab Results in Synergy ................................................................................................... 91
2. The Combination of Trastuzumab and Doxorubicin Did Not Result in Unexpected Toxicity and is Not Relevant to the Claimed Combination ............................................................... 95
X. CONCLUSION .............................................................................................. 97
3 of 97 Celltrion, Inc., Exhibit 1002

4
1. I, Robert Earhart, M.D., Ph.D., declare as follows:
I. INTRODUCTION
2. I have been retained by Celltrion, Inc. (“Celltrion”) in this matter.
3. I understand that Celltrion is seeking to challenge the patentability of
the claims of U.S. Patent No. 7,892,549 (“the ’549 patent”) in inter partes review
proceedings before the before the Patent Trial and Appeal Board (“PTAB”) of the
United States Patent and Trademark Office.
4. Celltrion has asked me analyze the state of the art and the scope and
content of the prior art as of December 12, 1996, and to provide my expert opinion
about whether claims 1-11 and 14-17 of the ’549 patent would have been obvious
to a person of ordinary skill in the art at that time.
5. I am being compensated at my standard rate for my time spent
preparing this Declaration, and my compensation is not contingent on the opinions
I provide or on the outcome of this matter. I have no financial interest in the
outcome of this matter.
II. SUMMARY OF OPINIONS
6. The statements, analysis and opinions that I provide in this
Declaration are my own and are based on my own personal knowledge, my many
years of experience in the field of cancer research, and the materials I reviewed in
connection with preparing this Declaration.
4 of 97 Celltrion, Inc., Exhibit 1002

5
7. Based on my analysis, knowledge and experience, it is my opinion
that claims 1-11 and 14-17 of the ’549 patent would have been obvious to a person
of ordinary skill in the art at the relevant time in light of the prior art references
Baselga 1996, Pegram 1995, Seidman 1996, and the 1995 Physicians’ Desk
Reference (“PDR”) entry for Taxol® (paclitaxel), in view of the knowledge of the
person of ordinary skill in the art. Each of these references is defined and analyzed
in more detail below.
8. More specifically, as of December 6, 1996, the person of ordinary
skill in the art would have been motivated by the prior art to administer a
combination of trastuzumab, cisplatin and paclitaxel to treat a human patient with
metastatic HER2+ breast cancer in amounts that would be effective to extend the
patient’s time to disease progression, and would have had a reasonable expectation
of success in so doing. As discussed in more detail below, claims 1-11 and 14-17
of the ’549 patent would have been obvious to a person of ordinary skill in the art.
III. QUALIFICATIONS AND EXPERIENCE
9. I graduated from Northwestern University in Chicago, Illinois with a
B.S. in Medicine in 1966. I subsequently earned an M.D. in 1972 and a Ph.D. in
pharmacology in 1975, both from Northwestern University.
10. I have worked in academia and in industry as a physician and clinical
pharmacologist since 1976. I also conducted research in pharmacokinetics and
5 of 97 Celltrion, Inc., Exhibit 1002

6
radioimmunoassay development at the University of Michigan with Prof. John
Wagner from summer 1976 through spring 1978.
11. From 1978 through 1982, I worked at the Wisconsin Clinical Cancer
Center (WCCC), where I was involved in research, clinical care and teaching.
While at WCCC, I established an Analytical Instrumentation Laboratory and
directed Phase I clinical and pharmacokinetic trials under a National Cancer
Institute (NCI) Phase I contract. My laboratory provided analytical chemistry
(HPLC, GC, GC-mass spectrometry, atomic absorption) and pharmacokinetic
support as well as protocol development and execution of NCI contract Phase I
trials of PCNU, DON, ICRF-187, carboplatin, acivicin, and combinations of
cyclophosphamide + misonidazole and cisplatin + amifostine, all of which are
chemotherapeutic agents.
12. I was a member of the New Agents and Pilot Studies Committee, and
chaired the Pharmacology Subcommittee of Eastern Cooperative Oncology Group,
an NCI-sponsored national consortium of US cancer centers. I designed and
supervised the conduct of multiple group-wide Phase II studies of the most
promising of these agents and regimens.
13. As a WCCC faculty medical oncologist, I conducted an outpatient
clinic year-round, and served as an Attending Faculty physician for several month-
long assignments in the University Hospital and the associated VA Hospital. I also
6 of 97 Celltrion, Inc., Exhibit 1002

7
taught cancer pharmacology course segments in the School of Pharmacy, and
developed and taught a graduate-level course in Pharmacology of Anticancer
Agents for the Department of Human Oncology.
14. In 1982, I joined The Upjohn Company as a Physician-Scientist, and
established a new in-house program of Phase I trials in cancer patients, resulting in
(1) the first induction of interferon in man by oral bropirimine, (2) optimization of
administration schedule for acivicin, (3) investigation of a suspension formulation
of bropirimine, and (4) development of a method to prevent dose-limiting CNS
toxicity of acivicin while potentiating peripheral antitumor activity of the drug,
resulting in doubling of the clinically tolerated dose.
15. While at Upjohn, I monitored Phase I and II extramural evaluation of
the oral anthracycline menogaril, which resulted in the identification of the Phase
II working dose and showed clinical activity in breast cancer. I also designed
strategy for clinical development through registration with the FDA.
Simultaneously, I designed clinical strategy for the new anticancer drugs
ormaplatin and adozelesin, which entered clinical trials in 1990, as well as
bizelesin and carzelesin. I also chaired the Drug Development Team which
organized the preclinical and clinical evaluation of acivicin.
16. I passed the first offered subspecialty examination of the American
Board of Clinical Pharmacology in 1991, and was thereby board-certified in the
7 of 97 Celltrion, Inc., Exhibit 1002

8
newly-emerging discipline of Clinical Pharmacology (#91406). Briefly, clinical
pharmacologists conduct research to optimize the use of therapeutic agents in
patients, both to understand and predict the results of clinical treatment and to
investigate the effects of human pathophysiology, concomitant treatments and
other factors on the use of drugs in the clinical setting.
17. In 1995, I joined Rhône-Poulenc Rorer as Associate Director of
Oncology Medical Affairs. While at the company, I was responsible for Phase
I/II/III/IV clinical trials of docetaxel (Taxotere®) which led to broadened use of this
drug after market introduction in 1996. In medical affairs, clinical trials known as
investigator-sponsored trials are routinely conducted after a cancer drug has been
approved for marketing. Every drug company with an FDA-approved product has
a medical affairs unit whose role, among others, is to consider whether to approve
or disapprove investigator-sponsored trials. These units review many such
proposals, although the exact number will vary depending on the size of the
company. By way of example, in the month of September 1996, while at Rhone
Poulenc Rorer, I personally reviewed 27 proposals for such studies. The purpose
of these activities is to fulfil the company’s ethical responsibility to develop valid
medical evidence that can inform clinical decisions involving the product, and to
guide its use to minimize patient risk, maximize patient benefit, and answer
important questions in clinical studies. Not all of the proposals were approved but
8 of 97 Celltrion, Inc., Exhibit 1002

9
many were, and some resulted in improvement in the clinical treatment of cancer
patients, and developed the basic information that led to FDA approval for
Taxotere® in additional oncology indications. I therefore have had substantial
experience in evaluating the information that is required to conduct clinical studies
in oncology with due regard to scientific, safety, efficacy and ethical concerns.
18. In late 1999, I worked as Senior Director of U.S. Bioscience. In
2000, U.S. Bioscience became MedImmune Oncology, where I was Vice President
of Clinical Oncology. There, I was responsible for Phase I clinical and
pharmacokinetic trials of Vitaxin® (a humanized monoclonal antibody against
human α-V β-3 integrin, an antiangiogenesis agent) in America and Europe, and a
Phase III product line extension trial of amifostine (Ethyol®) for prevention of
acute esophagitis in patients with stage III non-small-cell lung carcinoma
undergoing chemoradiotherapy. I formed and chaired Project Teams for both
Vitaxin® and Ethyol® to conduct these programs.
19. In 2003, I joined Cell Therapeutics in Seattle as Vice President of
Global Medical Affairs. I became responsible for planning, staffing, budgeting
and execution of Medical Affairs activities that supported Cell Therapeutics’
marketed product Trisenox® (arsenic trioxide), and late-phase development
products Xyotax® (paclitaxel polyglumex) and pixantrone.
9 of 97 Celltrion, Inc., Exhibit 1002

10
20. In 2005, I founded Arrowsmith Oncology LLC. This company
provides consultative services to the pharmaceutical industry in the areas of
strategic planning, process development, medical writing, staff training, medical
affairs support, clinical meeting organization and business development.
21. In March 2008, I joined Poniard Pharmaceuticals as Senior Director
of Clinical Development. Poniard needed a full-time physician/monitor to
supervise their Phase II combination (colorectal and prostate cancer), oral
bioavailability and QTc trials of their drug candidate, picoplatin. During my time
at Poniard, I continued some consultancy activity for Arrowsmith Oncology,
primarily teaching activities. In 2010, I returned to full-time consultative activities
at Arrowsmith Oncology, which I have being doing ever since. As a voting
member of the Institutional Review Board for the Cancer Research and
Biostatistics (CRAB®) nonprofit Contract Research Organization, I continue to
review scientific, clinical and ethical aspects of studies involving patients with
cancer.
22. I am a member of the American Society for Clinical Oncology
(“ASCO”), which I joined in 1998. I am also a member of the American
Association for Cancer Research (“AACR”), which I joined in 1982, and a
member of the American Society for Clinical Pharmacology and Therapeutics,
10 of 97 Celltrion, Inc., Exhibit 1002

11
which I joined in 1991. I have published over 40 peer reviewed research and
review articles and 60 abstracts in the field of oncology and drug development.
23. A copy of my curriculum vitae is provided as Exhibit 1003.
IV. LEGAL PRINCIPLES
24. Counsel has advised me of the following legal standards regarding
obviousness to assist me in preparing this declaration.
25. I am advised that the following four elements should be considered in
conducting an obviousness analysis: (1) the scope and content of the prior art;
(2) the differences between the prior art and the claim; (3) the level of ordinary
skill in the art; and (4) secondary considerations/objective indicators of
nonobviousness. I am advised that a patent claim is unpatentable for obviousness
if the differences between the subject matter sought to be patented and the prior art
are such that the subject matter as a whole would have been obvious at the time the
invention was made to a person of ordinary skill in the art to which the subject
matter pertains. I am further advised that a patent claim is obvious if a person of
ordinary skill in the art would have been motivated to combine the elements of the
claim, in view of the prior art and the state of the art, and would have had a
reasonable expectation of success in doing so. I am advised that the law requires
only a reasonable expectation of success, and does not require absolute certainty of
success.
11 of 97 Celltrion, Inc., Exhibit 1002

12
26. I am advised that the combination of known elements according to
known methods is likely to be obvious when it does no more than yield predictable
results, and that any need or problem known in the art at the time of the alleged
invention can provide a reason for combining elements. I am further advised that
obviousness is assessed via a common sense approach that is flexible, rather than
adherent to rigid application of legal standards or tests.
27. It is my understanding that obviousness is viewed through the eyes of
a person of ordinary skill in the art as of the time of the invention in question. I am
advised that, for purposes of this proceeding, I should consider only “prior art” in
the form of patents and printed publications which were publicly available and
were published more than a year before the filing date of the earliest application
for the patent. Here, the ’549 patent was filed on February 3, 2003, but is a
continuation of U.S. Patent No. 7,846,441 (“the ’441 patent”), which was filed on
December 10, 1998, and claims priority to Provisional Application No.
60/069,349, which was filed on December 12, 1997. For purposes of this
declaration, I have been asked to assume that patents and printed publications that
were published before December 12, 1996 constitute prior art to the ’549 patent
and may be considered as part of an obviousness analysis in this proceeding.
12 of 97 Celltrion, Inc., Exhibit 1002
13
V. LEVEL OF ORDINARY SKILL IN THE ART
28. I am advised that in defining a POSA the following factors may be
considered: (1) the educational level of the inventor; (2) the type of problems
encountered in the art; (3) prior art solutions to those problems; (4) rapidity with
which innovations are made; (5) sophistication of the technology; and (6)
educational level of active workers in the field.
29. In my opinion, a person of ordinary skill in the art as of December
1996 would have been an M.D. with subspecialty training in oncology and
substantial experience treating breast cancer patients and/or a Ph.D. with
substantial experience in researching and developing oncologic therapies. Such an
individual would also have had substantial experience in the design and/or
implementation of clinical trials for breast cancer treatments, and/or an active
research role relating to breast cancer treatments.
VI. SCIENTIFIC BACKGROUND
A. Breast Cancer and its Treatment as of December 1996
30. Cancers, including breast cancers, are characterized by the
uncontrolled and often rapid division of cells, caused by mutations in various genes
that are responsible for coordinating cellular processes, including cell division,
13 of 97 Celltrion, Inc., Exhibit 1002
14
cellular metabolism, and cell death. (Ex. 1005,1 at 1256.) The dividing cells form
a tumor, or a solid mass. The original tumor is called the primary tumor. (Id. at
1258.) Benign tumors are confined to the primary site; malignant tumors have the
ability to “metastasize,” in which some of the tumor cells leave the primary site
and form secondary tumors in other parts of the body. (Id. at 1256.) Cancers that
have metastasized are called “metastatic” or “advanced” cancers.
31. Most breast cancers are carcinomas, which are cancers derived from
epithelial cells.
32. As of December 1996, breast cancer was treated with a
multidisciplinary approach involving pharmaceuticals, radiation and/or surgery.
(Ex. 1016 (Abellof’s)2 at 201-206.) These approaches were often used in
combination. (Id. at 204.) The pharmaceutical treatments used in treating breast
cancer primarily included chemotherapy and hormone therapy. Note that the
treatment of advanced (metastatic) breast cancer is in some ways different from
neoadjuvant treatment (given prior to surgery with the intent of improving the
surgical outcome) or adjuvant treatment (given after surgical resection with the
1 ALBERTS, BRUCE et al., MOLECULAR BIOLOGY OF THE CELL 1255-1294 (3rd. ed.
New York: Garland Publishing, Inc., 1994) (“Albert’s”).
2 Excerpts from CLINICAL ONCOLOGY (Martin D. Abeloff et al., eds., New
York: Churchhill Livingstone, 1995) (“Abeloff’s”).
14 of 97 Celltrion, Inc., Exhibit 1002

15
intent of eliminating or delaying recurrence of disease). The end points (criteria
for success) will be different in each of these settings.
33. The goal in using most chemotherapeutic agents is to slow the growth
rate or decrease the size of the tumor, either by killing cancer cells by forcing the
cells to undergo a process called “apoptosis,” or by stopping cellular processes,
such as cell division. Apoptosis is the process of programmed cell death that
eliminates damaged or unwanted cells from multicellular organisms. (Ex. 1005 at
1268-1269.) It is also a common mechanism by which cancer drugs kill cancer
cells. Cellular pathways caused by genetic mutations often block apoptosis in
cancer cells, thereby increasing their survival even in the face of abnormalities that
would normally be recognized as cell damage and would therefore normally spur a
cell to undergo apoptosis.
34. Biochemical events of apoptosis lead to characteristic changes in cell
appearance and death. These include loss of cell membrane asymmetry and
attachment, cell shrinkage, nuclear fragmentation, chromatin condensation and
chromosomal DNA fragmentation. Although chemotherapeutics as a class are
designed to attack cells, different chemotherapy drugs achieve this goal in different
ways. Clinical experience has shown that some cancer histotypes respond to some
types of chemotherapies and other histotypes respond to other types of
15 of 97 Celltrion, Inc., Exhibit 1002
16
chemotherapies. Often, it is the type of cellular mutation that determines which
chemotherapy will work on a given cell.
35. As of December 1996, the following classes of chemotherapeutic
agents were commonly used to treat breast cancer: alkylating agents, including
cyclophosphamide, cisplatin and carboplatin3; antimetabolites, including 5-
fluorouracil and methotrexate; antibiotics, including doxorubicin and epirubicin;
and plant alkaloids, including the taxoids paclitaxel and docetaxel. (Ex. 1016 at
210.) Common use does not necessarily mean that the drug was FDA approved for
treating the specific histotype. Due to medical need, publication of trial results
sometimes outstrips formal drug development and approval processes, and
oncologists sometimes use promising regimens based on robust published data.
36. Each of the above chemotherapy classes has a different mechanism of
action and induces cell death in a different way. Doxorubicin, epirubicin, cisplatin,
paclitaxel and docetaxel were all FDA approved prior to December 1996.
Approval implies that the agent is commercially available for clinical use at the
discretion of the practitioner.
37. The taxoids paclitaxel (Taxol®) and docetaxel (Taxotere®) were FDA-
approved in December 1992 and May 1996, respectively, and were considered
3 Note that in terms of mechanism of antitumor activity, cisplatin and carboplatin
are highly similar; they differ somewhat in clinical toxicity, however.
16 of 97 Celltrion, Inc., Exhibit 1002
17
among the most promising chemotherapies in the mid-1990s. Taxoids were shown
to successfully treat some cancers that were refractory (non-responsive) to
anthracyclines. (See, e.g., Ex. 1010 (Seidman 1995)4 at 108.) Paclitaxel had anti-
cancer activity in many metastatic breast cancer patients. (Ex. 1010 at 108-111.)
Paclitaxel was used as monotherapy and as part of a combination of active agents
(such as cisplatin) in the treatment of metastatic breast cancer. (Ex. 1013
(Tolcher)5 at 37; Ex. 1007 (Abrams)6 at 1164.)
38. The 1995 Physician’s Desk Reference (“PDR”) entry for TAXOL®
(Ex. 1012 (1995 PDR)7) bears a copyright date of 1995. (Ex. 1012 at 2.) In my
experience, the PDR is a periodical distributed to physicians, which contains
4 A. Seidman et al., Memorial Sloan-Kettering Cancer Center Experience with
Paclitaxel in the Treatment of Breast Cancer, 22(5) SEMINARS ONCOLOGY
(SUPPLEMENT), 108-116 (Oct. 1995). (“Seidman 1995”).
5 Anthony W. Tolcher, Paclitaxel Couplets with Cyclophosphamide or Cisplatin in
Metastatic Breast Cancer, 23(1) Suppl. 1 SEMINARS ONCOLOGY 37-43 (Feb. 1996).
6 J. Abrams et al., New Chemotherapeutic Agents for Breast Cancer, 74(3)
INTERDISCIPLINARY INT. J. AM. CANCER SOC. (SUPPLEMENT), 1164-1176 (Aug.
1994). (“Abrams”).
7 Taxol® (Paclitaxel) for Injection Concentrate, in PHYSICIANS’ DESK REFERENCE,
682-685 (49th ed. 1995). (“1995 PDR”).
17 of 97 Celltrion, Inc., Exhibit 1002

18
safety, efficacy, and dosing information for drugs approved by the FDA. The
information contained in the PDR is the exact text of the most recent “package
insert” or “label” that has been exhaustively reviewed and approved by the FDA; it
is the most authoritative drug prescribing information available. The PDR is
published annually, and in my experience becomes publicly available to physicians
as of its publication date. In other words, a PDR that bears a copyright date of
1995—like the Taxol excerpt marked as Exhibit 1012—becomes available in 1995.
39. The 1995 PDR entry for Taxol® (paclitaxel) stated that the drug was
“indicated for the treatment of breast cancer after failure of combination
chemotherapy for metastatic disease or relapse within 6 months of adjuvant
chemotherapy. Prior therapy should have included an anthracycline unless
clinically contraindicated.” (Ex. 1012 at 683.) The recommended dosage of
paclitaxel to treat breast cancer was 175 mg/m2, administered intravenously over
the course of three hours, every three weeks. (Id. at 685.) “Mg/m2” and “mg/kg”
are two commonly used measurements of drugs that are dosed based on the surface
area and weight of the patient. Chemotherapeutic and other anti-cancer drugs are
often dosed by mg/m2 or mg/kg.
40. Chemotherapies are designed to kill cells or inhibit cellular functions.
Accordingly, chemotherapeutic agents, by their very nature, are toxic and can
cause a variety of side effects, ranging from minor to severe. Most of these are
18 of 97 Celltrion, Inc., Exhibit 1002
19
dose-related (more common or severe at higher doses of the drug) and among
these, some toxic effects are cumulative (more common or severe with repeated
treatments with the agent).
41. On the more severe side, the anthracycline class was known to cause
dose-related cumulative toxicity to the heart muscle, or cardiomyopathy. (Ex.
1016 at 810.) The risk of cardiomyopathy caused by anthracyclines was known to
increase with total lifetime dose. (Id.) Clinical evidence of cardiomyopathy
caused by anthracyclines may present immediately upon treatment with the
anthracycline or even years after treatment has stopped. Based on this knowledge,
treating physicians knew to limit the total amount of anthracycline that a patient
receives over a lifetime. (Id. at 813.) Careful monitoring for changes in cardiac
function (LVEF, or left ventricular ejection fraction) by ultrasound was used as a
means of identifying the rare patient whose cardiac function was compromised
earlier in the treatment program at low cumulative doses, or the patient with pre-
existing cardiac dysfunction who would not be a good candidate for anthracycline
treatment. (Id. at 812.)
42. Chemotherapies are most often administered to patients as part of a
regimen of therapies, given over a time period called a treatment cycle. A regimen
of a single agent may consist of infusions or oral doses of that drug on a set
schedule, such as at daily, weekly or monthly intervals. For example, for treating
19 of 97 Celltrion, Inc., Exhibit 1002

20
metastatic breast cancer, the Taxol® prescribing information recommended a
paclitaxel dose of 175 mg/m2 based on the calculated body surface area of the
patient (a function of height and weight), administered intravenously over the
course of three hours, every three weeks. (Ex. 1012 at 685.) For some regimens,
each infusion may use a different amount of a drug, adjusted depending on how the
patient tolerates the treatment. Regimens of combinations of drugs may consist of
infusions of each of the drugs, each with its own schedule and dosage, but with the
schedules overlapping with each other.
B. Development of Cancer Therapies
43. Before being administered to humans, anticancer drugs are developed
in the laboratory to evaluate their potential safety, efficacy and other properties.
Typically, drug candidates are first assessed in vitro, such as in cell lines and tissue
samples, for potential activity against a target or for potential toxicity. If in vitro
data are promising, the drug may be tested in living animals (e.g., mice, rats, dogs,
etc.) to determine potential toxicity in a live model.
44. “Xenografts” are an in vivo preclinical study method conducted in
living, immunocompromised mice, designed to model a human cancer patient as
closely as possible. (Ex. 1026 (Fiebig)8 at 343-346.) The immunocompromised
8 H.H. Fiebig et al., Comparison of Tumor Response in Nude Mice and in the
Patients, 74 BEHRING INST. MITTEILUNGEN, 343-352 (1984). (“Fiebig”).
20 of 97 Celltrion, Inc., Exhibit 1002

21
mice are injected with human cancer cells, which are able to grow unabated
because the mice’s immune systems are partially deficient. (Id.) This process
results in mice with “human” tumors, which maintain many features of the human
histotype from which they arose. (Id.) The tumor cells in the mouse undergo the
same cellular processes as the human tumor cells and exhibit the same genetic
mutations that caused the cells to be cancerous in humans. (Id.) Moreover, the
host animal will experience many of the dose-limiting toxic effects of the drug and
will eliminate the drug by processes that are similar to those of the human “species
of interest.” (Id.) Thus, xenografts provide a relatively reliable platform on which
to experiment with new therapies. (Id.)
45. By administering experimental anticancer drugs or drug combinations
to a xenograft animal model, researchers can evaluate activity and toxicity against
the target “human” tumor in a living organism. Thus, xenograft results provide a
“high[ly] correct prediction for resistance and sensitivity of a tumor” to a particular
agent. (Ex. 1026 at 349.) Because this predictive power is reproducible, the
mouse xenograft system validates “human tumor xenografts as tumor models to
test new drugs and combinations.” (Id. at 343; see also, Ex. 1028 (Mattern)9 at
9 Mattern, et al., Human Tumor Xenografts as Model for Drug Testing, 7 CANCER
AND METASTASIS REVIEWS, 263-284 (1988). (“Mattern”).
21 of 97 Celltrion, Inc., Exhibit 1002

22
279-80 (concluding that xenografts have strong predictive value for testing new
anticancer agents).)
46. Although xenografts are not conclusive evidence of efficacy or
toxicity in humans, they serve as a helpful tool that can provide further evidence of
efficacy or safety that researchers may find informative in developing new
treatments or designing clinical studies. This was true as of December 1996 and
still is today.
C. HER2+ Breast Cancer and Its Treatments
47. By December 1996, it was understood that some breast cancers have a
mutation in the “HER2” gene (also known as the “erbB2” gene). (Ex. 1020
(Baselga 1996)10 at 737.) This mutation causes the cancer cells to “overexpress” a
protein called the “HER2 receptor” (or “ErbB2” receptor). Healthy cells have
many protein receptors on the cell surface, including a limited number of the
HER2 receptor, whereas a cancer cell that “overexpresses” the HER2 receptor has
more copies of the HER2 receptor on the cell surface than a normal cell does.
10 J. Baselga et al., Phase II Study of Weekly Intravenous Recombinant Humanized
Anti-p185HER2 Monoclonal Antibody in Patients with HER2/neu-Overexpressing
Metastatic Breast Cancer, 14(3) J. CLINICAL ONCOLOGY 737-744 (Mar. 1996).
(“Baselga 1996”).
22 of 97 Celltrion, Inc., Exhibit 1002

23
Breast cancers in which the cancerous cells overexpress the HER2 receptor are
commonly called “HER2+ breast cancer.”
48. As of December 1996, HER2+ breast cancer was understood to
account for 25% to 30% of human breast cancers and known to be aggressive,
associated with a worse prognosis, and particularly difficult to treat with traditional
anti-cancer agents. (Ex. 1020 (Baselga 1996) at 737.)
49. In the 1980s and 1990s, researchers began to focus on antibody
therapy for cancer. (Ex. 1015 (Pietras 1994)11 at 1829-1830.) Other chemotherapy
drugs kill cells by interrupting normal cellular processes, and are therefore not
specifically targeted to cancer cells. In contrast, antibody therapy is targeted to
specific proteins that may be abnormally overexpressed in a given histotype of
cancerous cells.
50. First developed in late 1980s, trastuzumab is an antibody that targets
the HER2 receptor. Trastuzumab is a humanized version of 4D5, a murine
(mouse) antibody against the HER2 receptor that had been found, in vitro and in
xenograft models, to be a potent inhibitor of growth of HER2+ human breast
cancer cells. (Ex. 1020 (Baselga 1996) at 737.) Because murine antibodies are
11 R. J. Pietras et al., Antibody to HER-2/neu Receptor Blocks DNA Repair After
Cisplatin in Human Breast and Ovarian Cancer Cells, 9 ONCOGENE, 1829-1838
(1994). (“Pietras).
23 of 97 Celltrion, Inc., Exhibit 1002

24
immunogenic in humans and therefore of limited clinical use, 4D5 was
“humanized” to facilitate clinical investigations and use. (Id.) Trastuzumab,
which was at the time was commonly known as “rhuMAb HER2” or “humanized
4D5,” was found to be safe in two phase I clinical trials before 1996. (Id.)
51. As discussed below, as of December 1996, the prior art had reported
that both trastuzumab and paclitaxel were clinically effective against metastatic
HER2+ breast cancer, preclinical studies of this combination against this type of
cancer were very promising, and clinical trials of this combination were already
underway.
52. Trastuzumab was ultimately approved by the FDA in 1998 as
Herceptin® for the treatment of metastatic HER2+ breast cancer, either as a single
agent or in combination with chemotherapeutic drugs.
1. Baselga 1996 (Ex. 1020)
53. In March 1996, researchers at Memorial Sloan Kettering Cancer
Center (“MSKCC”) and Genentech published an article, Baselga 1996, in the
Journal of Clinical Oncology that reported the results of a phase II clinical trial of
trastuzumab. (Id. at 737.) In 1996, I was personally familiar with the Journal of
Clinical Oncology. It was directed to cancer researchers. It published monthly,
with issues becoming available during the month of their publication. For
example, the March 1996 issue became available to readers in March 1996. In
24 of 97 Celltrion, Inc., Exhibit 1002

25
1996, this journal was widely available to and consulted by POSAs around the
world, including in the United States.
54. The clinical trial in Baselga 1996 included 46 patients who had
extensive metastatic breast carcinoma, “one of the most dire prognostic
characteristics regarding response to therapy.” (Id. at 741.) All of the patients’
cancers were HER2+ breast cancer. (Id. at 738.) The patients were treated with an
initial dose of 250 mg of trastuzumab on day 0, and beginning on day 7, 100 mg of
trastuzumab weekly for a total of 10 doses. (Id. at 738.)
55. The study reports that 43 of the 46 patients were “assessable” (one
had died, one had developed a bacterial infection that precluded treatment, and one
declined treatment). Of these, five patients had tumor responses, including one
complete remission and four partial remissions. “Two patients had minor
responses and 14 patients had stable disease at day 77… The median time to
progression for the patients with either minor or stable disease was 5.1 months.”
(Id. at 740.)
56. Baselga 1996 reports that “[t]reatment with rhuMAb HER2 [i.e.,
trastuzumab] was remarkably well tolerated.” (Id. at 739.) The study reported
adverse events of fever and chills, pain at tumor site, diarrhea, nausea and emesis.
Of these, most were “moderate,” with a rating of “Grade 2,” and one was “severe,”
with a rating of “Grade 3.” (Id. at 740.)
25 of 97 Celltrion, Inc., Exhibit 1002

26
57. Baselga 1996 states that “[t]hese data are specially interesting in light
of the absence of significant toxicity observed here, for in a setting in which
palliation is a main objective, quality of life while on treatment should be a main
end point.” (Id. at 741.)
58. Baselga 1996 concludes: “In preclinical studies, both in vitro and in
xenografts, rhuMAb HER2 [i.e., trastuzumab] markedly potentiated the antitumor
effects of several chemotherapeutic agents, including cisplatin, doxorubicin, and
paclitaxel, without increasing their toxicity. Laboratory studies of the mechanism
of this effect and clinical trials of such combination therapy are currently in
progress.” (Id. at 743.) Baselga 1996 cites Baselga Abstract 53, discussed further
below, in support of this statement about the preclinical results for the
trastuzumab/paclitaxel and trastuzumab/doxorubicin combinations. (Id.)
2. Seidman 1996 (Ex. 1011)
59. Some of the same researchers from MSKCC published data on
paclitaxel’s clinical activity against HER2+ breast cancer in an abstract, Seidman
199612 (Ex. 1011), that was submitted for the 32nd Annual Meeting of the
American Society of Clinical Oncology (“ASCO”) in May 1996 and published in
12 A. Seidman et al., Over-Expression and Clinical Taxane Sensitivity: A
Multivariate Analysis in Patients with Metastatic Breast Cancer (MBC), 15 PROC.
AM. SOC. CLINICAL ONCOLOGY 104, abs. 80 (Mar. 1996). (“Seidman 1996”).
26 of 97 Celltrion, Inc., Exhibit 1002

27
the Programs/Proceedings book for the meeting in May 1996. I am very familiar
with the annual ASCO meetings, which thousands of oncology specialists and
cancer researchers attend each year. I typically attend the ASCO annual meeting,
and know that copies of the Programs/Proceedings book are distributed to
attendees during or before the meetings. I submitted an abstract for the May 1996
ASCO meeting, and attended the meeting. I, along with other persons of ordinary
skill in the art, received a copy of Programs/Proceedings book during or prior to
that meeting, which is before the December 1996 date that is important to this
proceeding.
60. Seidman 1996 reports on treatment of metastatic breast cancer
patients with paclitaxel. Fifty-one of the 126 (40.5%) patients studied had HER2+
breast cancer, while the others had cancer that did not overexpress the HER2
protein. (Id.) Thirty of the 51 (58.8%) patients with HER2+ breast cancer
responded to treatment with paclitaxel. (Id.) Twenty-nine of the 75 (38.7%)
patients with non-HER2+ breast cancer responded to treatment. (Id.) That is, a
higher percentage of patients were found to respond to treatment with paclitaxel
for HER2+ breast cancer than for non-HER2+ breast cancer. Seidman 1996
concludes: “Thus, HER2 over-expression in MBC [metastatic breast cancer] seems
to confer sensitivity rather than resistance to taxanes, in spite of a positive
27 of 97 Celltrion, Inc., Exhibit 1002

28
correlation of HER2 positivity with poor prognostic features. Cellular mechanisms
for this effect are under investigation.” (Id.)
3. Pegram 1995 (Ex. 1022)
61. In 1995, some of the same researchers from MSKCC and Genentech,
together with researchers from other institutions including UCLA, published data
on the clinical activity of the combination of trastuzumab and cisplatin against
HER2+ breast cancer. This data was submitted in an abstract, Pegram 199513 (Ex.
1022), for the 31st Annual Meeting of ASCO in May 1995 that was published in
the Programs/Proceedings book for the meeting in March 1995. I submitted an
abstract for the May 1995 ASCO meeting, and attended the meeting. I, along with
other persons of ordinary skill in the art received a copy of Programs/Proceedings
book during or prior to that meeting, which is before the December 1996 date that
is important to this proceeding.
62. Pegram 1995 begins by explaining that “[p]hase I studies conducted at
UCLA show that rhuMAb HER-2 [i.e., trastuzumab] has no substantial toxicity at
any dose level and localizes to malignant cells overexpressing the HER-2 receptor
13 M. Pegram et al., Phase II Study of Intravenous Recombinant Humanized Anti-
p185 HER-2 Monoclonal Antibody (rhuMAb HER-2) Plus Cisplatin in Patients
with HER-2/NEU Overexpressing Metastatic Breast Cancer, 14 PROC. AM. SOC.
CLINICAL ONCOLOGY 106, abs. 124 (Mar. 1995). (“Pegram 1995”).
28 of 97 Celltrion, Inc., Exhibit 1002

29
protein.” (Ex. 1022 (Pegram 1995).) The abstract then states that “[i]n preclinical
studies, therapy with this antibody plus cisplatin (CDDP) elicits a synergistic and
cytocidal effect on tumor cells which overexpress p185HER-2/neu.” (Id.)
63. Pegram 1995 reports a phase II, open-label, multicenter clinical trial
of the combination of trastuzumab and cisplatin in patients with metastatic HER2+
breast cancer. (Ex. 1022.) The patients received 75 mg/m2 of cisplatin on days 1,
29, and 57, and received a 250-mg loading dose of trastuzumab followed by
weekly doses of 100 mg for 8 weeks. (Id.) This trastuzumab regimen in this trial
was the same as that used in the Baselga 1996 trastuzumab-only trial (except that
the patients were treated for 10 weeks total in Baselga 1996, but 9 weeks total in
Pegram 1995). (Id.; Ex. 1020 (Baselga 1996) at 738.)
64. Of 36 patients treated in the study, one had a complete response and
seven had partial responses. (Ex. 1022 (Pegram 1995).) Pegram 1995 further
reports: “The toxicity profile was that expected from [cisplatin], and there were no
acute serious adverse events recorded following treatment with rhuMAb HER-2
[i.e., trastuzumab].” (Id.)
65. Pegram 1995 concludes that the “use of rhuMAb HER-2 [i.e.,
trastuzumab] plus CDDP [i.e., cisplatin] in patients with HER2/neu overexpressing
MBC [metastatic breast cancer] resulted in response rates above that expected from
CDDP alone, and the combination showed no apparent increase in toxicity.” (Id.)
29 of 97 Celltrion, Inc., Exhibit 1002

30
4. Preclinical Studies
66. In addition to the clinical evidence of efficacy for treating metastatic
HER2+ breast cancer of (1) trastuzumab alone, (2) paclitaxel alone, and (3) the
trastuzumab/cisplatin combination, preclinical data in mouse xenograft models also
supported the combined use of trastuzumab and paclitaxel for metastatic HER2+
breast cancer.
a. Baselga Abstract 53 (Ex. 1019)
67. In 1994, some of the same researchers from MSKCC and Genentech,
submitted an abstract, Baselga Abstract 5314 (Ex. 1019), for the 30th Annual
Meeting of ASCO in May 1994 that was published in the Programs/Proceedings
book for the meeting in May 1994. I submitted an abstract for the May 1994
ASCO meeting and attended that meeting. I, along with other persons of ordinary
skill in the art received a copy of Programs/Proceedings book during or prior to
that meeting, which is before the December 1996 date that is important to this
proceeding.
68. Baselga Abstract 53 reports a study of “humanized anti-HER2 4D5
against HER2” (i.e., trastuzumab) and other chemotherapeutic agents, alone and in
14 J. Baselga et al., Anti HER2 Humanized Monoclonal Antibody (MAb) Alone and
in Combination with Chemotherapy Against Human Breast Xenografts, 13 PROC.
AM. SOC. CLINICAL ONCOLOGY 63, abs 53 (Mar. 1994). (“Baselga Abstract 53”).
30 of 97 Celltrion, Inc., Exhibit 1002

31
various combinations, against HER2+ breast carcinoma xenografts. (Ex. 1019
(Abstract 53).) Baselga Abstract 53 reports the following results:
Treatment Result As Compared to Placebo Trastuzumab 35% growth inhibition at 5 weeks
Paclitaxel 35% growth inhibition at 5 weeks Doxorubicin 27% growth inhibition at 5 weeks
Trastuzumab and paclitaxel 93% growth inhibition at 5 weeks Trastuzumab and doxorubicin 70% growth inhibition at 5 weeks
69. As indicated above, each of trastuzumab and paclitaxel, when used
alone, inhibited tumor growth by 35%. The combination of
trastuzumab/paclitaxel, however, “resulted in a major antitumor activity with 93%
inhibition of growth” inhibited tumor growth by 93%. (Id.) The
trastuzumab/paclitaxel results were more promising than for the
trastuzumab/doxorubicin combination, which resulted in 70% tumor inhibition,
though “[c]omplete tumor eradication was seen in both groups.” (Id.) As a
possible explanation for the better results seen with the combinations, the authors
postulate that “[t]hese observations suggest that dual insults to cell cycle
transversal through checkpoints (MAb-mediated growth factor deprivation, and
drug mediated damage to DNA or tubulin) may activate cell death in tumor cells
which can survive either treatment given singly.” (Id.)
70. Baselga Abstract 53 further states that “MAb 4D5 [i.e., trastuzumab]
did not increase the toxicity of paclitaxel or doxorubicin in animals as determined
by animal survival and weight loss.” (Id.)
31 of 97 Celltrion, Inc., Exhibit 1002

32
71. Baselga Abstract 53 concludes: “In summary, anti HER2 MAbs can
eradicate well established tumors and enhance the activity of paclitaxel and
doxorubicin against human breast cancer xenografts. Clinical trials are underway.”
(Id.)
b. Baselga Abstract 2262 (Ex. 1021)
72. The MSKCC and Genentech researchers also published this same
xenograft study in an abstract, Baselga Abstract 226215 (Ex. 1021), for the 85th
Annual Meeting of the American Association for Cancer Research in April 1994
that was published in the Proceedings book for the meeting in March 1994. I am
very familiar with the annual AACR meetings and I often attend those meetings,
including prior to 1994. In 1994 and today, this meeting is well-attended by
oncology specialists and cancer researchers. I know that copies of the
Programs/Proceedings book are distributed to attendees during or before the
meetings. I also know that copies of the Programs/Proceedings book are available
once published by contacting the AACR. In the case of Baselga Abstract 2262, the
Programs/Proceedings book was also available for purchase as of April 1994,
15 J. Baselga et al., Antitumor Activity of Paclitaxel in Combination with Anti-
growth Factor Receptor Monoclonal Antibodies in Breast Cancer Xenografts, 35
PROC. AM. ASSOC. CLINICAL CANCER RES. 380, abs. 2262 (Mar. 1994). (“Baselga
Abstract 2262”).
32 of 97 Celltrion, Inc., Exhibit 1002
33
which is before the December 1996 date that is important to this proceeding. (See
Ex. 1021 at 2, copyright notice.) Based on my experience attending AACR
meetings, I believe that all registered attendees at that March 1994 meeting, many
of whom were persons of ordinary skill in the art, received copies of the
Programs/Proceedings book at or prior to that meeting.
73. Baselga Abstract 2262 reports the same xenograft data that were
published in Baselga Abstract 53.16 With regard to the combinations in the study,
Baselga Abstract 2262 states: “The combined treatment with paclitaxel plus 4D5
[i.e., trastuzumab] resulted in a major antitumor activity with 93% inhibition of
growth. This result was markedly better than doxorubicin plus 4D5 (70%
inhibition).” (Exhibit 1021.)
74. Baselga Abstract 2262 additionally states: “Thus, equipotent doses of
paclitaxel and doxorubicin differed in their combined effect with ARMAs [anti-
16 Baselga Abstract 2262 does not specify that the antibody was the humanized
version of 4D5. However, in my opinion, a POSA would have known that Baselga
Abstract 2262 was reporting results of a study using humanized 4D5. The study
reported in Baselga Abstract 2262 is the same study reported in Baselga Abstract
53, which does specify the use of the humanized antibody. The results reported in
the two abstracts are identical.
33 of 97 Celltrion, Inc., Exhibit 1002

34
growth factor receptor monoclonal antibodies, which includes 4D5], which
suggests synergy between paclitaxel and 4D5.” (Id.)
75. Like Baselga Abstract 53, Baselga Abstract 2262 also reports:
“ARMAs did not increase the toxicity of paclitaxel in animals as determined by
animal survival and weight loss.” (Id.)
76. Baselga Abstract 2262 concludes: “The antitumor effects of
paclitaxel can be markedly enhanced by the addition of ARMAs. Mechanisms are
being explored.” (Id. (emphases added).)
c. Seidman 1995 (Ex. 1010)
77. The MSKCC researchers also published an article, Seidman 1995 (Ex.
1010), in Seminars in Oncology in October 1995. The Seminars in Oncology
journal, published every two months, is well respected in the field of oncology and
has been since before December 1996.
78. Seidman 1995 primarily concerns the development of paclitaxel,
including the development via routine trial and error of the optimal dosing
schedule for paclitaxel given as a single agent. (Ex. 1010 (Seidman 1995) at 110-
111.)
79. Seidman 1995 also discusses the development of paclitaxel-based
combination therapies, including combinations of paclitaxel with doxorubicin,
cisplatin, and trastuzumab. (Id. at 111-112.) Citing references including Baselga
34 of 97 Celltrion, Inc., Exhibit 1002

35
Abstract 2262 (ref. 21), Seidman 1995 states: “Since 1992, we and others have
developed strong experimental data suggesting that combining maximally tolerated
doses of chemotherapeutic agents with MoAb-mediated blockade of either EGFR
or HER-2/neu receptors [e.g., trastuzumab] can eradicate well-established human
tumor xenografts that were resistant to either treatment given singly.” (Id. at 112.)
Seidman 1995 further states: “Striking antitumor effects are observed when
paclitaxel is given in human breast cancer xenografts in combination with either
anti-EGFR or anti-HER-2 MoAbs [e.g., trastuzumab]. This strong synergy is
achieved with no increased toxicity in the animal model.” (Id.)
80. That section of Seidman 1995 concludes: “While mechanisms for the
apparent synergy are being explored, these data provide a lead for translation into
the clinic. Indeed, future clinical trials combining paclitaxel with anti-growth
factor receptor MoAbs [(e.g., trastuzumab)] are being planned.” (Id.)
81. In summary , Seidman 1995 states that the “striking antitumor”
effects, “strong synergy” and “no increased toxicity” of paclitaxel and trastuzumab
in xenograft models “provide a lead for translation into the clinic” and that such
“future clinical trials” of the trastuzumab/paclitaxel combination “are being
planned.” (Id.)
35 of 97 Celltrion, Inc., Exhibit 1002

36
D. Combination Therapy for Breast Cancer
82. Treating cancer with a combination of therapeutic agent has been
established and common practice since the 1960s. (Ex. 1006 (DeVita) at 278-279;
Ex. 1016 at 208.)
83. A person of ordinary skill in the art understood that different cancers
respond to different types of therapies. A person of ordinary skill in the art also
understood that tumors can exhibit “intra-tumor heterogeneity,” in which, within a
single tumor, different cells may have different mutations that support the cancer
phenotype. (See, e.g., Ex. 1005 at 1271; Ex. 1020 at 738 (“Tumors were
considered to overexpress HER2 if at least 25% of tumor cells” were shown to
overexpress that receptor.).) Therefore, the different cells within a single tumor
may respond to different types of therapy.
84. Further, a person of ordinary skill in the art understood that tumors
that may initially respond to one type of therapy may develop “resistance” to that
therapy and no longer respond, simply due to the selection and preferential survival
of resistant cells. (Ex. 1005 at 1267, 1271-1273.) These resistant cells may
become sensitized to respond to different therapies in a process called “collateral
36 of 97 Celltrion, Inc., Exhibit 1002
37
sensitivity.” (Ex. 102517 at 246.) Another resistance-related phenomenon is
“cross-resistance,” whereby prolonged treatment with one anticancer drug can also
cause the cancer to develop resistance, not just to the drug being administered, but
also to other drugs within the same class. (Id.)
85. The following is a hypothetical for illustration purposes: A single
tumor includes cancerous cells, 90% of which are responsive to “type A”
chemotherapy, but 10% of which are resistant. In the best case scenario, therefore,
only 90% of the cells in the tumor will be killed by treatment with “type A”
chemotherapy, and 10% will survive. In a more realistic scenario, even some of
the 90% of cells that should respond to “type A” chemotherapy do not respond.
These cells, via a “resistance mechanism,” adapt to treatment with “type A,” and
mutate such that they are no longer of the type that would respond to “type A”
chemotherapy. These cells may also develop sensitivity to “type B”
chemotherapy. The 10% of cells that do not respond to “type A” and the small
fraction of the 90% that mutated continue to replicate, and the tumor grows with
cells that are resistant to “type A” chemotherapy. Therefore, treatment with just
17 Dorris J. Hutchison, Cross Resistance and Collateral Sensitivity Studies in
Cancer Chemotherapy, in 7 ADVANCES IN CANCER RESEARCH 235-348 (Alexander
Haddow and Sidney Wienhouse eds., Academic Press 1963). (“Hutchinson”).
37 of 97 Celltrion, Inc., Exhibit 1002

38
one type of chemotherapy is often not sufficient to kill all of the cells in a given
tumor and to stop the tumor from growing.
86. Because of the various mutations that may occur in a tumor and that
may arise in a tumor as a result of treatment, it is very uncommon for a single
treatment to be effective in killing all of the cells of the tumor. (Ex. 1006 at 279-
281.)
87. This complicated web of mutations and resistance mechanisms arises
in cells in a dynamic process that is interactive with treatment. A person of
ordinary skill in the art would have understood that combination therapy gave
patients their best chance of surviving cancer because a combination of drugs
allows the therapy to attacks cells in different ways at the same time. (Ex. 1016 at
204 (“The optimal exploitation of the chemotherapy strategies discussed earlier
requires the use of combination chemotherapy, because with rare exceptions single
agents do not cure cancer…The superior results achieved by combination
chemotherapy can be explained in several ways. Resistance to any given single
agent is almost always present, even in clinically responsive tumors, at
diagnosis. Tumors that are initially ‘sensitive’ rapidly acquire resistance to single
agents either as a result of selection of a pre-existing clone of resistant tumor cells
or due to an increased rate of mutation leading to drug resistance. Combination
chemotherapy theoretically addresses both important phenomena by providing a
38 of 97 Celltrion, Inc., Exhibit 1002

39
broader range of coverage of initially resistant clones of cells and preventing or
slowing the development of resistant clones.”).)
88. Thus, physicians and researchers use combinations of drugs to treat
cancer, based on the understanding that within a single tumor, the different cells
will respond to different drugs, and total efficacy of the combination will be
greater than the efficacy of single agents used alone. (Ex. 1006 at 208.) This was
true as of December 1996, and remains true today.
89. In developing new combinations of drugs, a person of ordinary skill in
the art relied on a set of four reasoned principles. (Ex. 1016 at 204-205.) First,
each drug in the combination should have exhibited efficacy in the target
population (histotype) when used alone. This principle ensures that only drugs that
are expected to work are used in combinations. (Id.) Second, the drugs in the
combinations should have non-overlapping toxicities. This principle ensures, as
much as possible, that any particular type of toxicity is not unduly severe or
frequent; ideally, this allows full doses of each of the drugs to be combined in the
regimen. (Id.) Third, the drugs in the combination should have different
mechanisms of action (addressing different oncogenic abnormalities), and fourth,
the drugs in the combination should have different resistance mechanisms. The
third and fourth principles ensure that the combination treatment is effective
against cells with as many types of cellular mutations as possible, whether those
39 of 97 Celltrion, Inc., Exhibit 1002

40
mutations were within original tumor cells, or arose via a resistance mechanism.
(Id.) I have lectured extensively on the development of combination therapies and
these principles, before December 1996 and continuing through today.
90. These principles of combination therapy are generally applicable to
anti-cancer drugs. The principles apply to all types of anti-cancer therapy
(including antibody therapy) in the same way that they apply to chemotherapy.
Some scientific literature in the early to mid-1990s focused on developing
combination therapies with paclitaxel, and illustrates the use of these principles.
For example, Arbuck 1994, a review article, succinctly describes the principles
behind combination therapy: “The best therapeutic results in cancer chemotherapy
are usually achieved with combinations of two or more drugs. When possible,
efforts are made to combine full doses of non-cross resistant drugs with single-
agent activity, differing mechanisms of action, and nonoverlapping toxicity.” (Ex.
102418 at 130-131 (emphasis added to point out the four principles of combination
therapy); see also, Ex. 1013 at 37 (“[p]aclitaxel combined with either
cyclophosphamide or cisplatin has several potential advantages: cisplatin and
cyclophosphamide are active single agents against previously untreated metastatic
breast cancer, colony-stimulating factors can modulate overlapping toxicities like
18 S. Arbuck et al., Paclitaxel (Taxol) in Breast Cancer, 8(1) HEMATOLOGY
ONCOLOGY CLINICS NORTH AM., 121-140 (Feb. 1994). (“Arbuck 1994”).
40 of 97 Celltrion, Inc., Exhibit 1002

41
myelosuppression, and no mechanisms of cross-resistance between paclitaxel and
these agents are yet known.”) (emphasis added).) Once paclitaxel had been shown
to be effective in treating metastatic breast cancer, “the logical progression for the
clinical development of this agent includes combination studies of paclitaxel and
other drugs that possess proven activity against breast cancer.” (Id.) The
development of combination therapies with paclitaxel was “logical” because
persons of skill in the art understood that cancer is most effectively treated with
combinations of more than one drug.
91. Consistent with the development of combination therapies for
paclitaxel in the years following the initial positive results with that drug,
combination therapies for trastuzumab were also under development as of
December 1996, following the initial positive clinical results for the individual
agent and positive preclinical results for the combinations, including the
trastuzumab/paclitaxel combination. For example, Baselga 1996, Abstract 2262
and Seidman 1995 report that clinical trials with the combination of trastuzumab
and chemotherapeutic agents, including paclitaxel, were underway or being
planned.
E. Measurements of Efficacy for Cancer Treatments
92. Cancer treatments are typically evaluated for efficacy using one or
more of the following clinical endpoints in clinical trials: (1) Overall Survival
41 of 97 Celltrion, Inc., Exhibit 1002

42
(“OS”), which measures the median survival time of the treated population, and is
the “gold standard” of efficacy; this is not to be confused with point estimates of
survival rate, the percentage of patients alive at a defined time after initiation of the
treatment (for example, one-year or five-year survival rate). (2) Progression Free
Survival (“PFS”), which measures the median time from initiation of treatment
until progression , death or loss to follow-up; PFS incorporates all deaths
regardless of cause and is a preferred surrogate end-point for OS. (3) Time to
Tumor Progression (“TTP”), which measures the median time from diagnosis or
start of treatment until tumor progression, but censors deaths that are not related to
cancer, and also censors loss to follow-up or withdrawal of the patient from the
study. (4) Disease-Free Survival (“DFS”), which measures the median time from a
potentially curative intervention (such as surgery) until recurrent cancer is seen or
until death or loss to follow-up. (5) Response Rate (“RR”), which measures the
percentage of patients whose tumor is reduced in size by a specified amount
following treatment. (Ex. 1023 (ASCO Guidelines)19 at 671-677.) OS, PFS, TTP
and DFS parameters are collectively called “time-to-event” end points, and are
thus more or less dependent on the determination of the specific event involved.
19 Outcomes of Cancer Treatment for Technology Assessment and Cancer
Treatment Guidelines, 14(2) J. CLINICAL ONCOLOGY, 671-679 (Feb. 1996). (“ASCO
Guidelines”).
42 of 97 Celltrion, Inc., Exhibit 1002

43
93. The World Health Organization (“WHO”) system that was in use
prior to 2000 classifies responses of solid tumors as either (1) Complete Response
(“CR”), characterized by the disappearance of all clinical evidence of disease and
normalization of disease symptoms and clinical markers, shown on two
measurements taken at least 4 weeks apart; (2) Partial Response (“PR”), defined as
a reduction of ≥50% in the sum of the cross products (the products of the longest
dimension times the longest perpendicular dimension) of all measurable tumor
masses, and no new lesions appearing; (3) Progressive Disease (“PD”), defined as
an increase of 25% or more in the sum of the cross products of all measurable
tumor masses, or new lesions; and (4) Stable Disease (“SD,” also called Minor
Response or “MR”), characterized by tumor size which over a pre-defined period
(usually two cycles) does not change enough to be classified as PR or PD. (Ex.
102920 at 211-212.) It was common to report clinical trial results in terms of
Objective Response Rate (“ORR”), which is the sum of the CR rate and the PR
rate. Reporting “clinical benefit,” the sum of CR, PR and MR, is sometimes done.
Special considerations are applied to lesions in bone or to lesions that are not
bidimensionally measurable.
20 Miller, A. B. et al., Reporting Results of Cancer Treatment, 47 CANCER, 207-
214 (Jan. 1981). (“Miller”)
43 of 97 Celltrion, Inc., Exhibit 1002

44
94. Overall survival is an ideal endpoint for showing efficacy, but it can
be difficult to establish due to the short duration of a clinical trial. For Phase 2
studies, which have the purpose of detecting useful clinical activity that can be
confirmed by definitive Phase 3 trials, response rate is normally employed.
Progression-free survival and time to disease progression are often used as
surrogates for overall survival, depending on the setting. Historical data has shown
that an increase in progression free survival or time to disease progression often
(but not always) correlates with an increase in overall survival. (Id. at 212.)
VII. U.S. PATENT NO. 7,892,549
A. The Specification of the ’549 Patent
95. The abstract of the ’549 patent states: “The present invention
concerns the treatment of disorders characterized by the overexpression of ErbB2.
More specifically, the invention concerns the treatment of human patients
susceptible to or diagnosed with cancer overexpressing ErbB2 with a combination
of an anti-ErbB2 antibody and a chemotherapeutic agent other than an
anthracycline, e.g., doxorubicin or epirubicin.” (Ex. 1001,21 Abstract.)
96. The specification states that Baselga 1996 showed that trastuzumab
“has been clinically active in patients with ErbB2-overepressing metastatic breast
cancers.” (Id., 3:36-42.) Further, overexpression of ErbB2 “is commonly regarded
21 U.S. Patent No. 7,892,549.
44 of 97 Celltrion, Inc., Exhibit 1002

45
as a predictor of a poor prognosis…and has been linked to sensitivity and/or
resistance to hormone therapy and chemotherapeutic regimens.” (Id., 3:43-52.)
However, according to the specification, HER2+ patients were three times as more
likely to respond to treatment with taxanes than patients whose tumors did not
overexpress HER2. (Id., 3:52-56.) Preclinical studies had shown that trastuzumab
enhanced the activity of each of paclitaxel and doxorubicin in mouse xenografts,
an in vivo test that closely models human cancers. (Id., 3:56-61.)
97. The specification includes an Example that describes a study in which
patients with HER2+ breast cancer were treated with one of four treatment
regimens: (1) anthracycline + cyclophosphamide (“AC”); (2) anthracycline +
cyclophosphamide + trastuzumab (“AC + H”); (3) paclitaxel (“T”); (4) paclitaxel +
trastuzumab (“T + H”). (Id., 26:34-30:25.) The patent reports the following
results for TTP in months, RR in percent, and AE (adverse events) in percent:22
Treatment Number of patients
TTP (months) RR (%) AE(%)
AC 145 6.5 42.1. 71 AC + H 146 9.0 64.9 68
T 89 4.2 25.0 59 T + H 89 7.1 57.3 70
22 The patent also reports results for “CRx” (chemotherapy) and “CRx + H.”
“CRx” is the combined data for “AC” and “T,” and “CRx + H” is the combined
data for “AC + H” and “T + H.”
45 of 97 Celltrion, Inc., Exhibit 1002

46
(Id., 29:11-30:12.) The specification states that “[a] syndrome of myocardial
dysfunction similar to that observed with anthracyclines was reported more
commonly with a combined treatment of AC+H (18% Grade 3/4) than with AC
alone (3%), T (0%), or T+H (2%).” (Id. at 30:13-25.) The specification states that
the results favor the combination of trastuzumab and paclitaxel:
These data indicate that the combination of anti-ErbB2 antibody
treatment with chemotherapy markedly increases the clinical benefit,
as assessed by response rates and the evaluation of disease
progression. However, due to the increased cardiac side-effects of
doxorubicin or epirubicin, the combined use of anthracyclines with
anti-ErbB2 antibody therapy is contraindicated. The results, taking
into account risk and benefit, favor the combined treatment with
HERCEPTIN® and paclitaxel (TAXOL).
(Id.)
B. The Claims of the ’549 Patent
98. The ’549 patent has 17 claims. Claims 1, 5, and 16 are independent
claims. Claims 2-4 depend from claim 1, claims 6-15 depend from claim 5, and
claim 17 depends from claim 16. I understand that Celltrion’s Petition for inter
partes review challenges all of the claims other than claims 12 and 13. Claims 1-
11 and 14-17 are reproduced below.
46 of 97 Celltrion, Inc., Exhibit 1002

47
1. A method for the treatment of a human patient with breast cancer
that overexpresses ErbB2 receptor, comprising administering a
combination of an antibody that binds ErbB2, a taxoid, and a further
growth inhibitory agent to the human patient in an amount effective to
extend the time to disease progression in the human patient, wherein
the antibody binds to epitope 4D5 within the ErbB2 extracellular
domain sequence.
2. The method of claim 1 wherein the antibody is a humanized 4D5
anti-ErbB2 antibody.
3. The method of claim 1 wherein the antibody cross-blocks binding
of 4D5 to the ErbB2 extracellular domain sequence.
4. The method of claim 1 wherein the antibody binds to amino acid
residues in the region from about residue 529 to about residue 625 of
the ErbB2 extracellular domain sequence.
5. A method for the treatment of a human patient with breast cancer
characterized by overexpression of ErbB2 receptor, comprising
administering an effective amount of a combination of an anti-ErbB2
antibody which binds epitope 4D5 within the ErbB2 extracellular
domain sequence, a taxoid, and a further therapeutic agent, to the
human patient.
6. The method of claim 5 wherein the breast cancer is metastatic
breast carcinoma.
47 of 97 Celltrion, Inc., Exhibit 1002

48
7. The method of claim 5 wherein the antibody is a humanized 4D5
anti-ErbB2 antibody.
8. The method of claim 7 wherein the antibody is administered as a 4
mg/kg dose and then weekly administration of 2 mg/kg.
9. The method of claim 5 wherein the taxoid is paclitaxel.
10. The method of claim 5 wherein efficacy is measured by
determining the time to disease progression or the response rate.
11. The method of claim 5, wherein the further therapeutic agent is
selected from the group consisting of: another ErbB2 antibody, EGFR
antibody, ErbB3 antibody, ErbB4 antibody, vascular endothelial
growth factor (VEGF) antibody, cytokine, and growth inhibitory
agent.
14. The method of claim 5 wherein the further therapeutic agent is a
growth inhibitory agent.
15. The method of claim 14 wherein the growth inhibitory agent is a
DNA alkylating agent.
16. A method for the treatment of a human patient with ErbB2
overexpressing breast cancer, comprising administering a combination
of an antibody that binds epitope 4D5 within the ErbB2 extracellular
48 of 97 Celltrion, Inc., Exhibit 1002
49
domain sequence, a taxoid and a further growth inhibitory agent, in
the absence of an anthracycline derivative, to the human patient in an
amount effective to extend the time to disease progression in the
human patient.
17. The method of claim 16 wherein the breast cancer is metastatic
breast carcinoma.
C. Prosecution History of the ’549 Patent
99. Below, I describe the obviousness arguments presented by the
Examiner, as well as the pertinent details of (1) a declaration by one of the ’549
patent’s named inventors, Susan D. Hellmann, M.D., M.P.H. (“Hellmann
Declaration” (Ex. 1008)), that Patent Owner submitted in the parent application
(for the ’441 patent) on August 25, 2000, and again relied on in the prosecution of
the ’549 patent on September 12, 2006 in response to the Examiner’s first
obviousness rejection of the application’s claims, and (2) a declaration from a
Genentech employee, Mark X. Sliwkowski, Ph.D.23 (“Sliwkowski Declaration”
(Ex. 1009)), that Patent Owner submitted on October 15, 2009 to respond to the
Examiner’s fourth (and last) obviousness rejection of the application’s claims.
23 Declaration of Mark X. Sliwkowski, Ph. D. (Dec. 10, 1998). (“Sliwkowski
Declaration”).
49 of 97 Celltrion, Inc., Exhibit 1002

50
100. Based on my reading of the prosecution history of the ’549 patent (Ex.
1004),24 I understand that (1) the Examiner did not ultimately find the arguments in
the Hellmann Declaration persuasive, and that the ’549 patent did not issue as a
result of the Hellmann Declaration (Ex. 1008; see also Ex. 1004 at 1550), and (2)
that the Examiner withdrew the obviousness rejections and ultimately issued the
’549 patent as a result of the statements made in the Sliwkowski Declaration (Ex.
1009; see also Ex. 1004 at 2351).
101. The claims of the ’549 patent are similar to the claims that were
pending for most of the prosecution of the patent application. In general, those
claims were drawn to a method of treating a human patient who has HER2+ breast
cancer with a combination of trastuzumab, paclitaxel, and a third anti-cancer agent.
I understand that during prosecution, the Patent Owner elected to treat carboplatin
as the third anti-cancer agent for examination purposes (Ex. 1004 at 1396
(02/16/2006 Office Action at 2); 1406 (03/16/2006 Response at 5)), and so the
Examiner concentrated on the combination of trastuzumab, paclitaxel, and
carboplatin for many of the rejections (id. at 1419, 1788, 1839 (Office Actions
dated 06/02/2006, at 2; 06/26/2008, at 2; 03/20/2009, at 2)).
102. In a series of rejections, the Examiner rejected the claims on a number
of grounds, including as obvious over the prior art. Although the exact
24 Ex. 1004 is the Prosecution History of the ’441 patent.
50 of 97 Celltrion, Inc., Exhibit 1002

51
combination of prior art references that the Examiner relied on as the basis of the
obviousness rejections sometimes differed from one rejection to the next, the
obviousness rejections were all very similar. First, the Examiner found that it was
known in the prior art that trastuzumab had shown anti-tumor efficacy in clinical
studies with patients who were suffering from HER2+ breast cancer. Second, it
was known in the prior art that the combination of trastuzumab and paclitaxel had
resulted in a synergistic antitumor response in preclinical mouse xenograft studies.
Third, the examiner found that it was known that the combination of paclitaxel and
carboplatin may be used to treat patients with advanced breast cancer. Therefore,
according to the Examiner, it would have been obvious to a person of ordinary skill
in the art to combine the therapies of trastuzumab, paclitaxel, and carboplatin and
to use that combination to treat human patients who had HER2+ breast cancer.
103. In response to these obviousness rejections, the Patent Owner relied
upon and resubmitted the Hellmann Declaration from the parent application. (Ex.
1008; see also Ex. 1004 at 1456, 1522-25, 1550-615.) In that declaration, Dr.
Hellmann opined that the claimed combination of drugs produced a synergistic
clinical response in human patients and that this response was unexpected. (Ex.
1008 at ¶¶ 3-6.) She also opined that the combination of trastuzumab and
doxorubicin resulted in unacceptable increased cardiac toxicity, and that the
absence of such increased toxicity with the trastuzumab/paclitaxel combination
51 of 97 Celltrion, Inc., Exhibit 1002
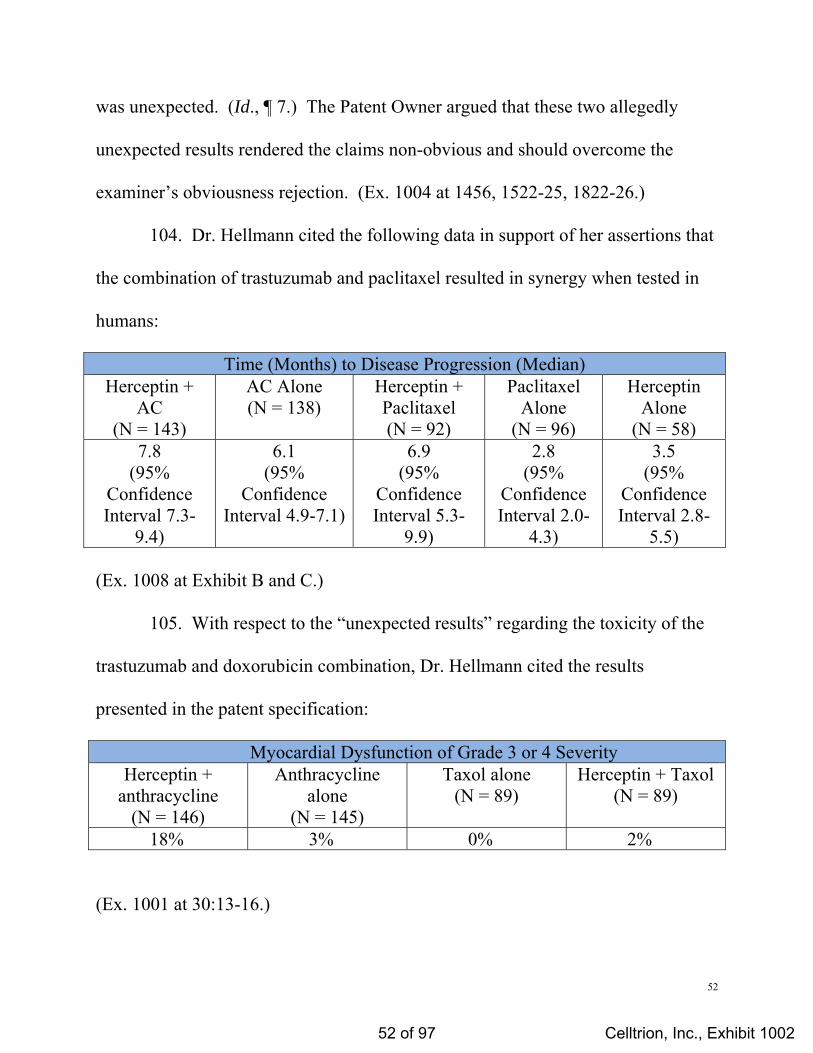
52
was unexpected. (Id., ¶ 7.) The Patent Owner argued that these two allegedly
unexpected results rendered the claims non-obvious and should overcome the
examiner’s obviousness rejection. (Ex. 1004 at 1456, 1522-25, 1822-26.)
104. Dr. Hellmann cited the following data in support of her assertions that
the combination of trastuzumab and paclitaxel resulted in synergy when tested in
humans:
Time (Months) to Disease Progression (Median) Herceptin +
AC (N = 143)
AC Alone (N = 138)
Herceptin + Paclitaxel (N = 92)
Paclitaxel Alone
(N = 96)
Herceptin Alone
(N = 58) 7.8
(95% Confidence Interval 7.3-
9.4)
6.1 (95%
Confidence Interval 4.9-7.1)
6.9 (95%
Confidence Interval 5.3-
9.9)
2.8 (95%
Confidence Interval 2.0-
4.3)
3.5 (95%
Confidence Interval 2.8-
5.5)
(Ex. 1008 at Exhibit B and C.)
105. With respect to the “unexpected results” regarding the toxicity of the
trastuzumab and doxorubicin combination, Dr. Hellmann cited the results
presented in the patent specification:
Myocardial Dysfunction of Grade 3 or 4 Severity Herceptin +
anthracycline (N = 146)
Anthracycline alone
(N = 145)
Taxol alone (N = 89)
Herceptin + Taxol (N = 89)
18% 3% 0% 2%
(Ex. 1001 at 30:13-16.)
52 of 97 Celltrion, Inc., Exhibit 1002
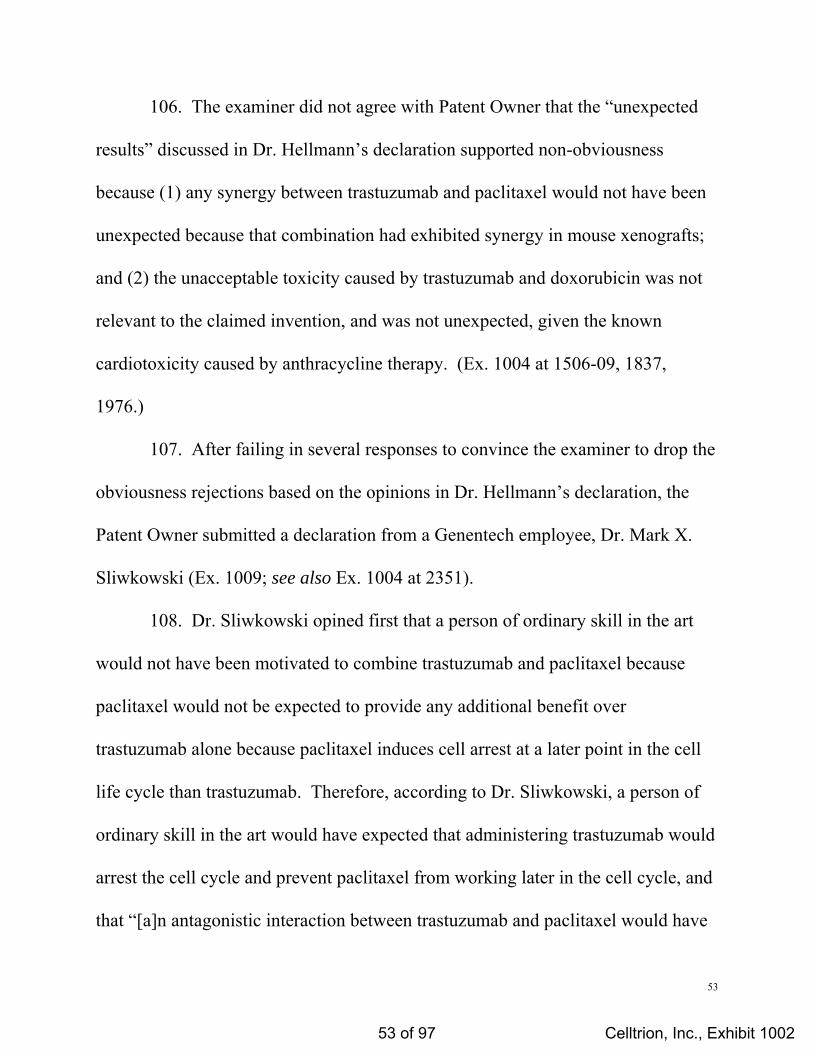
53
106. The examiner did not agree with Patent Owner that the “unexpected
results” discussed in Dr. Hellmann’s declaration supported non-obviousness
because (1) any synergy between trastuzumab and paclitaxel would not have been
unexpected because that combination had exhibited synergy in mouse xenografts;
and (2) the unacceptable toxicity caused by trastuzumab and doxorubicin was not
relevant to the claimed invention, and was not unexpected, given the known
cardiotoxicity caused by anthracycline therapy. (Ex. 1004 at 1506-09, 1837,
1976.)
107. After failing in several responses to convince the examiner to drop the
obviousness rejections based on the opinions in Dr. Hellmann’s declaration, the
Patent Owner submitted a declaration from a Genentech employee, Dr. Mark X.
Sliwkowski (Ex. 1009; see also Ex. 1004 at 2351).
108. Dr. Sliwkowski opined first that a person of ordinary skill in the art
would not have been motivated to combine trastuzumab and paclitaxel because
paclitaxel would not be expected to provide any additional benefit over
trastuzumab alone because paclitaxel induces cell arrest at a later point in the cell
life cycle than trastuzumab. Therefore, according to Dr. Sliwkowski, a person of
ordinary skill in the art would have expected that administering trastuzumab would
arrest the cell cycle and prevent paclitaxel from working later in the cell cycle, and
that “[a]n antagonistic interaction between trastuzumab and paclitaxel would have
53 of 97 Celltrion, Inc., Exhibit 1002

54
been viewed as a reasonable possibility.” (Ex. 1009 at ¶¶ 7-8.) Dr. Sliwkowski
based this theory on purported antagonism reported in the prior art for a different
combination (tamoxifen and anthracyclines). (Id.) Second, Dr. Sliwkowski opined
that the synergistic response to the combination of trastuzumab and paclitaxel in
mouse xenografts would not have motivated a person of ordinary skill in the art to
use that combination in humans, or have led a person of ordinary skill in the art to
a reasonable expectation of success, because mouse xenografts are not predictive
of results in humans. (Id. at ¶ 9.) The only reference that Dr. Sliwkowski cited to
support this argument was published in 2001, more than four years after the
application for the parent application (for the ’441 patent) was filed.
109. In response to the Sliwkowski Declaration and Patent Owner’s related
arguments, the Examiner withdrew the obviousness rejections, but without
substantively responding to the Sliwkowski Declaration. (Ex. 1004 at 1978-79
(12/28/2009 Office Action at 2-3).) After resolution of a remaining rejection for
double patenting, the Examiner allowed the claims. (Id. at 2016-20 (10/08/2010
Notice of Allowance).)
VIII. CLAIM CONSTRUCTION
110. I have been informed by counsel that the challenged claims should
be given their broadest reasonable construction in light of the specification of the
patent. The following terms in the claims of the ’549 patent are explicitly defined
54 of 97 Celltrion, Inc., Exhibit 1002

55
in the specification and should therefore be construed in accordance with those
explicit definitions:
a. The term “humanized” (claims 2 and 7) means “contains
minimal sequence derived from non-human immunoglobulin.” (Ex. 1001, 9:17-
22.)
b. The term “epitope 4D5” (claims 1, 5 and 16) means “the region
in the extracellular domain of ErbB2 to which the antibody 4D5 binds.” (Id., 5:26-
28.)
c. The terms “overexpresses ErbB2 receptor” (claim 1) /
“overexpression of ErbB2 receptor” (claim 5) / “ErbB2 overexpressing” (claim
16) mean having significantly higher than normal ErbB2 receptor/ErbB2 levels
compared to a noncancerous cell of the same tissue type. Cancers with these
characteristics are termed HER2+ cancers., i.e., these terms refer to HER2+ breast
cancer. (Id., 5:59-61.)
d. The term “growth inhibitory agent” (claims 1, 11, 14, 15 and
16) means “a compound or composition which inhibits growth of a cell, especially
an ErbB2-overexpressing cancer cell either in vitro or in vivo.” (Id. at 11:20-40.)
“Growth inhibitory agent” includes, for example, cisplatin, a DNA alkylating
agent. (Id.)
55 of 97 Celltrion, Inc., Exhibit 1002

56
111. The following terms, while not explicitly defined in the specification,
have meanings derived from the specification based on the knowledge of one of
ordinary skill in the art:
a. The term “therapeutic agent” (claims 5, 11 and 14) means “an
agent with efficacy in the treatment of cancer.” (See Ex. 1001 at 11:4-19, 10:41-
50.) The specification expressly defines “chemotherapeutic agent” as “a chemical
compound useful in the treatment of cancer.” (Id. at 11:4-19.) Based on claim 5,
which requires administering “an effective amount of a combination of an anti-
ErbB2 antibody …, a taxoid, and a further therapeutic agent,” the “further
therapeutic agent” must have efficacy in treating cancer, as opposed to simply
general efficacy in treating any condition. This conclusion is supported by the
specification, which defines “therapeutically effective amount” as “an amount
having antiproliferative effect.” (Id. at 10:41-50.) “Therapeutic agent” includes,
for example, cisplatin, a DNA alkylating agent. (Id. at 11:4-19.)
b. The term “time to disease progression” (claims 1, 10 and 16)
means the “time period calculated from the beginning of therapy until the disease
worsens.” (Id.. at 29:3-9; see also Ex. 1004 at 2304 (’441 patent prosecution
history, Response to Office Action dated Sep. 22, 2008 at 7 (citing National
Cancer Institute Definition “measure of time after a disease is diagnosed (or
treated) until the disease starts to get worse.”)).)
56 of 97 Celltrion, Inc., Exhibit 1002
57
c. The term “response rate” (claim 10) means the percentage of
patients whose disease responds to treatment. (See, e.g., Ex. 1001, col. 28, lines
46-67; col. 29, lines 11-30:20.)
d. The term “extend the time to disease progression in the
human patient” (claims 1 and 16) is a relative term. Based on the specification,
the appropriate comparison is to compare the claimed combination treatment
versus treatment with a taxoid alone. This is supported by the Example in the
specification, which begins at Col. 26, line 34. The Example reports a clinical
study in which patients received either paclitaxel alone, or paclitaxel together with
humanized anti-ErbB2 antibody (Herceptin®). (Id. at col. 28, lines 3-6 and 15-23.)
The specification shows that the comparisons of time to disease progression and
evaluations of adverse events for the taxoid/antibody combination were made
based on the combination of the taxoid (Taxol®) with the anti-ErbB2 antibody
(Herceptin®) versus treatment with the taxoid (Taxol®) alone. (Id. at col. 29, line 9
– col. 30, line 25.)
I note that, during prosecution of the ’549 patent’s parent application,
Application No. 09/208,649 (now the ’441 patent), Patent Owner asserted that the
appropriate comparison for the term “extend the time to disease progression” is to
compare the claimed combination treatment to no treatment at all. For example, in
response to an indefiniteness rejection based on the ambiguity of this claim term,
57 of 97 Celltrion, Inc., Exhibit 1002

58
Patent Owner stated: “Clearly, the combination of anti-ErbB2 antibody and taxoid
is administered in an amount effective to extend the time to disease progression
relative to an untreated patient.” (Ex. 1004 at 416 (Response dated Jan. 17, 2002 at
3).) In my opinions in this declaration, I have considered this alternate claim
construction as well, but it does not impact my analysis.
IX. OBVIOUSNESS ANALYSIS
112. It is my opinion that claims 1-11 and 14-17 of the ’549 patent would
have been obvious to a person of ordinary skill in the art in view of the following
combination of prior art references: Baselga 1996 (Ex. 1020), Seidman 1996 (Ex.
1011), Pegram 1996 (Ex. 1022), and the 1995 PDR entry for Taxol® (Ex. 1012).
113. As indicated above in Section IV above (Legal Principles), I
understand that there are four factual inquiries that go into an obviousness analysis.
A. Scope and Content of the Prior Art
114. I described the scope and content of the prior art above, including the
disclosures of Baselga 1996, Seidman 1996, Pegram 1995, and the 1995 PDR entry
for Taxol®. The scope and content of the prior art also includes the discussion in
this section on obviousness.
B. Level of Ordinary Skill in the Art
115. I described the level of ordinary skill in the art in Section V above.
58 of 97 Celltrion, Inc., Exhibit 1002
59
C. Differences Between the Claims and the Prior Art and Conclusion of Obviousness
116. Claims 1-11 and 14-17 of the ’549 patent are generally directed to the
administration of an effective amount of a combination of an anti-ErbB2 antibody
(which can be trastuzumab), a taxoid (which can be paclitaxel), and a third agent
(which can be cisplatin) to treat a human patient with metastatic HER2+ breast
cancer. Claims 1-4 and 16-17 require the effective amount of the combination to
be “an amount effective to extend the time to disease progression in the human
patient,” whereas claims 5-11 and 14-15 require simply an “effective amount.”
117. The prior art teaches that each of trastuzumab alone (Baselga 1996),
the combination of trastuzumab and cisplatin (Pegram 1995), and paclitaxel alone
(Seidman 1996) is clinically effective for the treatment of humans with metastatic
HER2+ breast cancer. The prior art (Baselga 1996) also taught that, following
promising preclinical data that showed major antitumor activity and synergy of the
trastuzumab/paclitaxel combination for this type of cancer without increasing
toxicity relative to paclitaxel alone, clinical trials of the trastuzumab/paclitaxel
combination were already underway. The prior art also disclosed regimens of
trastuzumab-alone (Baselga 1996), the trastuzumab/cisplatin combination (Pegram
1995), and paclitaxel alone (1995 PDR) that were known to be clinically effective
against metastatic breast cancer.
59 of 97 Celltrion, Inc., Exhibit 1002

60
118. Based on these teachings, Baselga 1996, Pegram 1995, and Seidman
1996 would have provided a person of ordinary skill in the art with a motivation to
combine trastuzumab, cisplatin and paclitaxel to treat human patients with
metastatic HER2+ breast cancer with a reasonable expectation that the
combination would be effective. A person of ordinary skill in the art would have
been motivated by Pegram 1995 and the 1995 PDR to use the doses of
trastuzumab, cisplatin, and paclitaxel that were known in the prior art to be
effective against metastatic breast cancer. Based on the teaching in Baselga 1996
that trastuzumab was “remarkably well tolerated,” lacked “significant toxicities,”
and did not increase the toxicity of either cisplatin (when combined in clinical
trials) or paclitaxel (when combined in preclinical studies), a person of ordinary
skill in the art would have reasonably expected the prior art amounts of
trastuzumab, cisplatin, and paclitaxel to extend the time to disease progression.
119. As I explained above, as of December 1996, combination therapy
was a well-established approach for treating cancer. In the natural progression of
cancer research, a new agent is typically tested in combination with others after the
new agent has proven clinical efficacy in a target population. Particularly for the
population of metastatic HER2+ breast cancer patients, which typically had a
worse prognosis than other cancer patients and had been underserved in the past
because this cancer often did not respond to traditional anti-cancer therapies, a
60 of 97 Celltrion, Inc., Exhibit 1002
61
person of ordinary skill in the art would have been interested in testing
combinations with any drug that had proven efficacy for metastatic HER2+ breast
cancer. Baselga 1996, Pegram 1995, and Seidman 1996 respectively report the
clinical efficacy of trastuzumab, trastuzumab/cisplatin, and paclitaxel in the
metastatic HER2+ breast cancer population, and therefore provided a strong
motivation to test those drugs in combination in human metastatic HER2+ breast
cancer patients.
120. The clinical data in Baselga 1996, which demonstrated that
trastuzumab had clinical efficacy in treating patients with metastatic HER2+ breast
cancer, would have motivated a person of ordinary skill in the art to combine
trastuzumab with other anti-cancer drugs to treat patients with this disease with a
reasonable expectation of success. As explained, it was well-known that cancers
are not homogeneous with respect to the cellular mutations that are responsible for
the cancer. Therefore, if a particular cancer overexpresses the HER2 receptor, that
cancer likely also has other mutations that would make some cells of that cancer
susceptible to other treatments. (See, e.g., Baselga 1996 (Ex. 1020) at 738
(“Tumors were considered to overexpress HER2 if at least 25% of tumor cells
exhibited characteristic membrane staining for p185HER2.”).) The established
efficacy of trastuzumab in treating patients with metastatic HER2+ breast cancer
would have motivated a person of skill in the art to use trastuzumab in combination
61 of 97 Celltrion, Inc., Exhibit 1002

62
with other therapies that had proven efficacy in all types of metastatic breast
cancer, and cisplatin and paclitaxel were particularly attractive options.
121. Pegram 1995 discloses that the trastuzumab/cisplatin combination is
clinically effective against metastatic HER2+ breast cancer, and reports that adding
trastuzumab to cisplatin resulted in elevated response rates, with no apparent
increase in toxicity, relative to what was expected for cisplatin-alone. (Ex. 1022.)
Based on this knowledge, a person of ordinary skill in the art would have been
motivated to develop combination therapies for metastatic HER2+ breast cancer
that included trastuzumab and cisplatin.
122. Seidman 1996 reports that paclitaxel is clinically effective against
metastatic HER2+ breast cancer. (Ex. 1011.) Based on this disclosure, combined
with the knowledge of a person of ordinary skill in the art that paclitaxel had
efficacy in patients with metastatic breast cancer regardless of whether or not the
cancer overexpress HER2, a person of ordinary skill in the art would have been
motivated to develop combination therapies for metastatic HER2+ breast cancer
that included paclitaxel. This made paclitaxel an ideal candidate for combination
with trastuzumab/cisplatin for this patient population. Accordingly, a person of
ordinary skill in the art would have been motivated to add paclitaxel to the
established trastuzumab/cisplatin combination and would have reasonably
62 of 97 Celltrion, Inc., Exhibit 1002

63
expected this three-drug combination to effectively treat metastatic HER2+ breast
cancer.
123. The motivation and reasonable expectation of success for the
trastuzumab/cisplatin/paclitaxel combination would have been reinforced by the
knowledge of a person of ordinary skill in the art that the underlying two-drug
combinations (trastuzumab/cisplatin, trastuzumab/paclitaxel, and
paclitaxel/cisplatin) were already being administered by persons of ordinary skill
in the art to treat metastatic breast cancer patients. Indeed, a person of ordinary
skill in the art knew from the prior art that:
the trastuzumab/cisplatin combination was clinically effective
against metastatic HER2+ breast cancer and reasonably safe (Pegram
1995 (Ex. 1022));
the trastuzumab/paclitaxel combination was already undergoing
clinical trials to treat metastatic HER2+ breast cancer as stated in
Baselga 1996: (Baselga 1996 (Ex. 1020) at 743); and
the paclitaxel/cisplatin combination was already being used
successfully, including to treat patients with metastatic breast cancer
(1995 TAXOL PDR (Ex. 1012) at 683; Ex. 1013 (Tolcher) at 37; Ex.
1014 (Gelmon 1996) at 1185).
63 of 97 Celltrion, Inc., Exhibit 1002
64
This knowledge would have confirmed that persons of skill in the art were already
motivated to combine these drugs for the treatment of metastatic breast cancer,
including metastatic HER2+ breast cancer, and based on their willingness to
administer the combination to humans and their ethical responsibilities to use only
treatments that are likely to succeed, reasonably expected success with the
combination.
124. Further, the ongoing clinical studies of the trastuzumab/paclitaxel
combination were supported by promising preclinical data. Baselga 1996 reported
that in preclinical xenografts studies of HER2+ breast cancer, trastuzumab
“markedly potentiated the antitumor effects of several chemotherapeutic agents,
including … paclitaxel, without increasing their toxicity.” (Ex. 1020 at 743.)
Baselga 1996 cites Baselga Abstract 53, from which a person of ordinary skill in
the art would have already known that the trastuzumab/paclitaxel combination
exhibited “major antitumor activity” with 93% inhibition of growth, demonstrating
better results than the trastuzumab/doxorubicin combination, and that trastuzumab
did not increase the toxicity of paclitaxel when combined. (Id.) The xenograft
data would have further reinforced the motivation to combine trastuzumab and
paclitaxel for the treatment of metastatic HER2+ breast cancer and the reasonable
expectation that the combination would work.
64 of 97 Celltrion, Inc., Exhibit 1002
65
125. The combination of trastuzumab, cisplatin, and paclitaxel also made
logical sense based on the four guiding principles of combination therapy.
126. First, trastuzumab, cisplatin, and paclitaxel each had proven clinical
efficacy in the target population, metastatic HER2+ breast cancer patients.
(Baselga 1996 (Ex. 1020); Pegram 1995 (Ex. 1022); Seidman 1996 (Ex. 1011).)
Indeed, as reported in Seidman 1996, paclitaxel was clinically effective in both the
sub-population of metastatic HER2+ breast cancer patients and the larger
population of metastatic breast cancer patients, which made it a strong choice to
combine with trastuzumab/cisplatin to treat metastatic HER2+ breast cancer,
particularly based on the known concept of intra-tumor heterogeneity. Therefore,
the trastuzumab/cisplatin/paclitaxel combination satisfied the first principle of
combination therapy.
127. Second, trastuzumab, cisplatin, and paclitaxel were not known to have
any significant overlapping toxicities. Trastuzumab was reported to have
“remarkably [good] tolerability” with an “absence of significant toxicities.”
(Baselga 1996 (Ex. 1020).) When trastuzumab was combined with cisplatin in
clinical trials, the combination showed no increase in toxicity compared with
cisplatin alone (Pegram 1995 (Ex. 1022)), which would have suggested to a person
of ordinary skill in the art that trastuzumab and cisplatin do not have any
significant overlapping toxicities.
65 of 97 Celltrion, Inc., Exhibit 1002

66
128. A person of ordinary skill in the art also would have known that the
dose-limiting toxicity (i.e., the toxicity that determines the maximum dose of a
drug that may be administered to a patient) of paclitaxel was myelosuppression.
(Ex. 1018 (Gelmon 1994)25 at 24.) The prior art did not associate trastuzumab with
myelosuppression. (Baselga 1996 (Ex. 1020) at 739, 741.) Based on the lack of
toxicity observed in the xenografts with the combination of trastuzumab and
paclitaxel, a person of ordinary skill in the art, going into clinical trials, would have
reasonably expected to be able to administer the two agents at full effective doses
in combination without creating serious safety or tolerability concerns. A person
of ordinary skill in the art would also have known from clinical studies reported in
the prior art that myelosuppression associated with the paclitaxel/cisplatin
combination could be minimized by adjusting the sequencing of administration,
and other adverse events were tolerable. (Ex. 1012 at 683; Ex. 1013 at 38.)
129. Based on their toxicity profiles, a person of ordinary skill in the art
would have reasonably expected trastuzumab, cisplatin, and paclitaxel to work
well together in combination. Therefore, the trastuzumab/cisplatin/paclitaxel
combination satisfied the second principle of combination therapy.
25 Karen A. Gelmon, Biweekly Paclitaxel (Taxel) and Cisplatin in Breast and
Ovarian Breast Cancer, 21(5) SEMINARS ONCOLOGY (SUPPLEMENT), 24-28 (Oct.
1994). (“Gelmon 1994”).
66 of 97 Celltrion, Inc., Exhibit 1002
67
130. Third, trastuzumab, cisplatin, and paclitaxel were known to have
different mechanisms of action. Trastuzumab is a growth factor receptor targeted
antibody, and paclitaxel is a cytotoxic chemotherapeutic agent. Cisplatin and
paclitaxel are non-specific chemotherapeutic agents that treat cancer in different
ways. Cisplatin is a DNA alkylating agent that acts by modifying cellular DNA.
Paclitaxel is plant alkaloid that acts on the cell’s microtubules. (Ex. 1018 at 24.)
Because these agents have different mechanisms of action, a person of ordinary
skill in the art would have reasonably expected them to work well together.
Therefore, the trastuzumab/cisplatin/paclitaxel combination satisfied the third
principle of combination therapy.
131. Fourth, a person of ordinary skill in the art would have reasonably
expected that trastuzumab, cisplatin, and paclitaxel would not exhibit any cross-
resistance with one another because they have very different mechanisms of action.
Indeed, paclitaxel and cisplatin were already known not to exhibit cross-resistance
with one another. Ex. 1013 at 37 (“[C]isplatin … [has no] known mechanisms of
cross-resistance with paclitaxel.”); Ex. 1014 at 1185 (“We were also interested in
combining the new agent [paclitaxel] with a non-cross-resistant drug with a
different spectrum of toxicity. Cisplatin seemed to be an appropriate choice.”).
Because there are virtually no common mechanisms through which targeted
antibodies like trastuzumab and chemotherapies like paclitaxel and cisplatin induce
67 of 97 Celltrion, Inc., Exhibit 1002
68
apoptosis or otherwise kill cells, a person of ordinary skill in the art would not
believe that these agents have the potential to exhibit cross-resistance with one
another. (Ex. 1016 at 113.) Therefore, the trastuzumab/cisplatin/paclitaxel
combination satisfied the fourth principle of combination therapy.
132. With respect to the effective amount of the combination, a person of
ordinary skill in the art would have been motivated to target the known effective
regimens of trastuzumab/cisplatin and paclitaxel when used as single agents. A
bedrock principle of combination therapy is that, when possible, the drugs in a
combination should be administered at their full doses at which they are known to
be effective individually, to maximize the anticancer effects. Therefore, a person
of ordinary skill in the art would have been motivated to use the
trastuzumab/cisplatin dosing regimen that Pegram 1995 reported to be effective in
treating metastatic HER2+ breast cancer (Ex. 1022.), and the dosing regimen for
paclitaxel that was recommended in the 1995 PDR entry for Taxol® as being
effective for treating metastatic breast cancer. (Ex. 1012 at 685.) A person of
ordinary skill in the art would have been motivated to use these regimens and
would have reasonably expected these combined regimens to extend the time to
disease progression, without increasing overall severe adverse events, relative to
paclitaxel alone, based on many factors, including (a) the promising clinical results
reported for these drugs in Baselga 1996, Pegram 1995 and Seidman 1996, (b) the
68 of 97 Celltrion, Inc., Exhibit 1002
69
good tolerability and absence of significant toxicities associated with trastuzumab
reported in Baselga 1996, (c) the report in Baselga 1996 that trastuzumab did not
increase the toxicity of paclitaxel, (d) the report in Pegram 1995 that adding
trastuzumab to cisplatin increased the response rates in metastatic HER2+ breast
cancer patients with no apparent increase in toxicity relative to that expected from
cisplatin alone, and (e) the lack of known significant overlapping toxicities
between trastuzumab and paclitaxel.
133. If a person of ordinary skill in the art discovered, upon administering
the combination to a patient, that the amounts of trastuzumab, cisplatin, or
paclitaxel needed adjustment, it would have been a routine matter for a person of
ordinary skill in the art to optimize the combined regimen for maximal tolerability
and efficacy to arrive at amounts that extend the time to disease progression.
134. A person of ordinary skill in the art would have known how to
optimize that combined dose, via routine and conventional techniques, for both a
standard “recommended” dosage amount, and for individual patients’ needs, if
necessary. Routine dose finding studies normally follow one of two possible
patterns: either the dose of one or more agents is held constant while the dose of
the other agent is increased, or the dosages of all agents are increased by the same
multiplicative factor. In both cases, the increase is stopped when the adverse
effects of the treatment become unacceptable.
69 of 97 Celltrion, Inc., Exhibit 1002

70
135. Indeed, the conclusion that a person of ordinary skill in the art would
have known how to optimize the dosage amount is admitted by the ’549 patent
specification, which describes the amount of paclitaxel, cisplatin. or other
chemotherapeutic agent to use in combination with trastuzumab as follows:
“Preparation and dosing schedules for such chemotherapeutic agents may be used
according to manufacturers’ instructions or as determined empirically by the
skilled practitioner.” (Ex. 1001, col. 25, lines 1-19.) In discussing the amount of
trastuzumab to administer in the combination, the specification provides a broad
range (15,000-fold) of possible dosages—“about 1 μg/kg to 15 mg/kg (e.g. 0.1-20
mg/kg)”—“[d]epending on the type and severity of the disease.” (Id. at col. 25,
lines 43-54.) The specification acknowledges that there are many possible
regimens by which trastuzumab may be administered and that physicians routinely
optimize the dose, based on many well-known factors, stating that “progress of this
therapy is easily monitored by conventional techniques and assays.” (Id.)
136. In summary, by using the known effective amounts of each
component of the combination, a person of skill in the art would have reasonably
expected that the trastuzumab/cisplatin/paclitaxel combination would be effective
in extending the time to disease progression. As explained, it is rare for a single
drug to kill all of the cancerous cells in a patient’s tumors. With a combination of
different agents, the expectation is that more of the cells will be killed and
70 of 97 Celltrion, Inc., Exhibit 1002

71
therefore, the time to disease progression and other measures of efficacy, including
the response rate, would improve.
137. These measures of efficacy would also improve relative to no
treatment, in accordance with the alternate claim construction presented in Section
VIII. A person of ordinary skill in the art would have known that treatment with
paclitaxel alone resulted in extension of time to disease progression and a higher
response rate than no treatment. Therefore, an extension of time to disease
progression and increase in response rate relative to treatment with paclitaxel,
logically also results in an extension of time to disease progression and increase in
response rate relative to no treatment. A person of ordinary skill in the art would
have also expected that the treatment of trastuzumab, cisplatin, and paclitaxel in
combination would not have resulted in any unacceptable toxicities, based on the
known toxicity profiles of each of those drugs when given alone or in two-drug
combinations.
138. A person of skill in the art would have been motivated to use the triple
combination of trastuzumab/paclitaxel/cisplatin because that combination was
obvious based on the principles of combination therapy, as explained above.
Further, a person of ordinary skill in the art would have excluded an anthracycline
derivative from the combination in order to avoid the cardiotoxicity that is
associated with that class of drugs. Anthracyclines were known to cause
71 of 97 Celltrion, Inc., Exhibit 1002

72
irreversible cardiotoxicity, a phenomenon associated with the total lifetime dose a
patient receives. (Ex. 1016 at 813.) While treating patients with anthracyclines is
often unavoidable in the course of a patient’s cancer treatment, limiting the total
dose of an anthracycline is a goal. (Id. at 810, 813; see also Ex. 1020 at 740
(stating that a patient died of congestive heart failure due to doxorubicin treatment
during treatment with trastuzumab.) A person of ordinary skill in the art would
have expected that many patients had previous anthracycline treatment, given that
anthracyclines were a first-line therapy for breast cancer. (Ex. 1016 at 1693.)
Therefore, particularly for patients who had already been treated with an
anthracycline, it would have been obvious not to include the drug in the
combination of trastuzumab and paclitaxel.
139. For these reasons, a person of ordinary skill in the art would have
been motivated to avoid administering further anthracycline derivatives to the
many patients who had already been treated with this class of drug. (Id.)
D. Response To The Sliwkowski Declaration
1. A Person of Ordinary Skill in the Art Would Not Have Expected an Antagonistic Interaction Between Paclitaxel and Trastuzumab
140. In his declaration, Dr. Sliwkowski argues that “a skilled scientist
would have anticipated that paclitaxel would provide little or no additional benefit
to treatment with trastuzumab alone” because trastuzumab arrests the cell cycle at
72 of 97 Celltrion, Inc., Exhibit 1002

73
the G1 phase, which precedes the G2/M phase at which paclitaxel purportedly
arrests the cell cycle. (Ex. 1009 at ¶ 7.) Based on this theory, Dr. Sliwkowski
argues that combining trastuzumab with paclitaxel “would provide little or no
additional benefit,” because trastuzumab would “arrest cell cycle before it reaches
the G2/M phase, where taxoids exert their apoptotic antitumor activity.” (Ex. 1009
(Sliwkowski Dec.), ¶ 7.)
141. I disagree with Dr. Sliwkowski’s theory and reasoning because they
are based on several false assumptions about how these agents work to treat
cancer, and are contradicted by the data available in the prior art, which predicted a
favorable interaction between trastuzumab and paclitaxel, rather than antagonism.
142. First, Dr. Sliwkowski’s theory wrongly assumes that because
paclitaxel causes cell death by attacking microtubules, it only acts when a cell is in
the phase of its cell cycle in which microtubules are active. A person of ordinary
skill in the art would have known, however, that paclitaxel exerts its anticancer
effects during all phases of the cell cycle, and not only while the microtubules were
active in the G2/M phase. (Ex. 1007 at 1165; Ex. 1006 (De Vita) at 415.) A
person of ordinary skill in the art would have known that the cellular component
on which paclitaxel exerts its effect is tubulin, a component of microtubules, as Dr.
Sliwkowski acknowledges. (Ex. 1009 at ¶ 7.) However, a person of ordinary skill
in the art would have known that an injury to the microtubules causes a cell to
73 of 97 Celltrion, Inc., Exhibit 1002
74
undergo apoptosis (i.e., cell death) regardless of whether the microtubules are
active at the time of the injury. In other words, paclitaxel does not work only
during one phase of the cell cycle, and therefore, cycle arrest caused by
trastuzumab would not preempt the activity of paclitaxel. (See, e.g., Ex. 1007 at
1165.)
143. As support for his assertion that paclitaxel lead to “an arrest of the
cells in the G2/M phase” of the cell cycle, Dr. Sliwkowski cites to C.M. Woods et
al., Taxol-Induced Mitotic Block Triggers Rapid Onset of a p53-Independent
Apoptotic Pathway, 1(5) MOLECULAR MEDICINE 506-526 (1995) (“Woods”). (Ex.
1009, ¶ 7, Exhibit B.) Woods, however, does not support Dr. Sliwkowski’s
statement that paclitaxel works only during the G2/M phase of the cell cycle (i.e.,
at the end of interphase and the beginning of prophase). Woods clearly states that
paclitaxel induces two types of apoptosis, one in prophase (i.e., the G2/M phase),
and another in the earlier G1 phase of the cell cycle. (Ex. 1009, Exhibit B at 21;
see also Ex. 1006 (De Vita) at 60-66.) Dr. Sliwkowski’s declaration does not
mention or otherwise account for the knowledge in the prior art that he cited that
paclitaxel induces apoptosis in this earlier G1 phase of the cell cycle. Dr.
Sliwkowski’s failure to mention paclitaxel’s anticancer effects at the G1 phase is
an important omission, given that Dr. Sliwkowski asserts in his declaration that
trastuzumab exerts its anti-tumor effects at the G1 phase. (Ex. 1009, ¶ 8.) A
74 of 97 Celltrion, Inc., Exhibit 1002

75
person of ordinary skill in the art would have known that trastuzumab and
paclitaxel work at the same phase of the cell cycle. This information is a
significant flaw in Dr. Sliwkowski’s theory.
144. Second, Dr. Sliwkowski’s theory wrongly assumes that tumors are
homogenous—that all cells in a tumor have the same mutations, behave in the
same way, and exist at precisely the same phase in the cell cycle as one another.
(Id., ¶ 109.) A person of ordinary skill in the art, however, would have known that
tumors are typically heterogeneous and contain of cancer cells having a variety of
mutations and growing at different stages. Therefore, even if it were true that
trastuzumab and paclitaxel only exert their effects at different phases of the cell
cycle, a person of ordinary skill in the art would have known that the cells in the
tumor would exist at different cell cycle phases and could be attacked by both
trastuzumab and paclitaxel. (Id., ¶ 109.)
145. Third, and relatedly, Dr. Sliwkowski’s theory wrongly assumes that
trastuzumab will kill all of the cells in the tumor when they are in the G1 phase.
However, a person of ordinary skill in the art would understand that drugs are
typically not 100% effective. That is, trastuzumab would not be expected to kill
every single cancer cell in the tumor, and paclitaxel would still be able to attack the
remaining cells in the phase of G2/M. Indeed, because trastuzumab targets HER2+
cancer cells, it would not be expected to kill every cell in a HER2+ tumor. In the
75 of 97 Celltrion, Inc., Exhibit 1002

76
prior art, a breast carcinoma was considered to be HER2+ if at least 25% of tumor
cells exhibited the HER2 receptor. (See, e.g., Ex. 1020 at 738 (“Tumors were
considered to overexpress HER2 if at least 25% of tumor cells exhibited
characteristic membrane staining for p185HER2.”).) That means that a HER2+
breast cancer tumor will very likely contain a significant proportion of cells that
are not individually HER2+. As explained, a person of ordinary skill in the art
would want to combine trastuzumab with one or more drugs with proven efficacy
in all types of metastatic breast cancer (such as paclitaxel and cisplatin) that could
target cells that are not HER2+. Dr. Sliwkowski’s theory simply does not work in
the context of HER2+ breast cancer.
146. Dr. Sliwkowski’s theory that “an antagonistic interaction between
trastuzumab and paclitaxel would have been viewed as a reasonable possibility”
was based on the purported observation in the prior art that tamoxifen, a hormone
that causes antitumor effects at the G0-G1 cell cycle phase, exhibited an
antagonistic interaction when combined with anthracyclines, which act later in the
cell cycle. (Ex. 1009, ¶ 8.)
147. Based on the prior art, a person of ordinary skill in the art would have
had no basis to believe that Dr. Sliwkowski’s theory based on the
tamoxifen/doxorubicin combination would be applicable to the unrelated
combination of trastuzumab/paclitaxel.
76 of 97 Celltrion, Inc., Exhibit 1002

77
148. First, in my opinion, the activity of the tamoxifen/anthracycline
combination provides information only about that particular combination and
cannot be reasonably extrapolated to other combinations of drugs. Indeed,
according to the articles cited by Dr. Sliwkowski in support of his analogy to the
tamoxifen/doxorubicin combination, the antagonism that is seen with tamoxifen
and doxorubicin may not be extrapolated even to combinations of tamoxifen with
other chemotherapeutic drugs. (See, e.g., Ex. 1009, Exhibit F (Osborne) at 715)
(“The antagonism is drug specific and even alkylating agent specific.”).) The
articles cited by Dr. Sliwkowski also note that antagonism between tamoxifen and
doxorubicin is not always seen (Ex. 1009, Exhibit F (Osborne) at 715; Exhibit G
(Woods) at 1449), and that any antagonism may be due to many factors, not only
to the particular combination of tamoxifen and doxorubicin. (Exhibit G (Woods)
at 1450-1451.) These articles therefore do not provide any information to a person
of ordinary skill in the art regarding why or even if an antagonistic relationship
exists between tamoxifen and doxorubicin; and they certainly do not provide
information regarding other combinations. Further, a person of ordinary skill in
the art would have known that tamoxifen is an anti-estrogen hormone therapy and
that trastuzumab is an antibody against a growth factor receptor. These agents
work in very different ways, and analogies between them should not be drawn
without reference to specific similarities between those drugs.
77 of 97 Celltrion, Inc., Exhibit 1002

78
149. Second, the prior art discloses combinations that are more analogous
to trastuzumab/paclitaxel than tamoxifen/doxorubicin that contradict Dr.
Sliwkowski’s theory. For example, the prior art disclosed the combination of
trastuzumab and cisplatin. (Pegram 1995 (Ex. 1022).) Like paclitaxel, cisplatin
was known to arrest the cell cycle at the G2/M phase. (Ex. 1027 (Sorenson).)26 If
Dr. Sliwkowski’s theory were correct that trastuzumab would arrest the cell cycle
of every cancer cell at the G1 phase, and prevent a chemotherapy that acts later in
the cell cycle from exerting its anticancer effects, then one would expect that
trastuzumab would have antagonized cisplatin and caused cisplatin to “provide
little or no additional benefit to treatment with trastuzumab alone.” (Ex. 1009, ¶
7.) But Pegram 1995 reports that (a) the trastuzumab/cisplatin combination
exhibited synergistic effects against HER2+ cancer cells in vitro, (b) that the
combination was clinically effective in humans with metastatic HER2+ breast
cancer, and (c) the response rates for the combination were above those that were
expected from cisplatin alone. (Ex. 1022 (Pegram 1995).) This prior experience
using a more analogous combination in the very system of interest (metastatic
HER2+ breast cancer) would have dispelled for a person of ordinary skill in the art
26 Christine M. Sorenson et al., Analysis of Events Associated with Cell Cycle
Arrest at G2 Phase and Cell Death Induced by Cisplatin, 82 JOURNAL OF THE
NATIONAL CANCER INSTITUTE 9, 749-755 (1990) (“Sorenson”)
78 of 97 Celltrion, Inc., Exhibit 1002

79
any concerns based on Dr. Sliwkowski’s theory. Dr. Sliwkowski’s declaration
does not mention Pegram 1995 or the trastuzumab/cisplatin combination.
150. Third, with regard to the specific combination of
trastuzumab/paclitaxel, prior experience in preclinical xenograft studies informed a
person of ordinary skill in the art that trastuzumab was not preventing paclitaxel
from working. (See, e.g., Ex. 1021.) That is, in live human cancer cells in live
animals, trastuzumab did not antagonize paclitaxel and, indeed, did just the
opposite and exhibited synergistic antitumor effects. (Id.) The favorable results
and synergy reported for the combination of trastuzumab/paclitaxel in the prior art
would have dispelled any theoretical concern about potential antagonism with this
particular combination. Furthermore, a person of ordinary skill in the art would
have known that, following these favorable preclinical studies, the
trastuzumab/paclitaxel combination was undergoing clinical trials, which would
have confirmed that other persons of skill in the art were motivated to combine
these drugs with a reasonable expectation of success. In summary, a person of
ordinary skill in the art had no basis to anticipate that the trastuzumab-paclitaxel
combination would behave antagonistically.
2. Xenograft Data is a Helpful Tool for Developing Combination Therapies
151. Dr. Sliwkowski asserted in his declaration that xenograft models are
not predictive of clinical efficacy for breast cancer and therefore a person of
79 of 97 Celltrion, Inc., Exhibit 1002

80
ordinary skill in the art would not have reasonably expected success for the
trastuzumab-paclitaxel combination based on the xenograft data reported in the
prior art. (Ex. 1004 at ¶ 9.) While it is true that xenografts are not predictive in the
sense that results seen in xenografts are not identical to results that are seen in
patients, it is my experience that positive xenograft data can forecast positive
results in humans, and were considered valuable in developing cancer drugs for the
clinic as of December 1996, and remain valuable today. (Ex. 1028 at 279
(“Xenografts of a particular tumor type are often able to identify agents of known
clinical activity against that disease.”).) If not, there would be no reason to burden
preclinical drug development programs with the cost and effort involved in such
activities. In no case would such results be disregarded by persons of ordinary
skill in the art.
152. In vivo animal studies such as xenografts, when available, can be
valuable tools in developing an experimental therapy or designing a clinical trial.
Such studies can be designed to test specific hypotheses related to a proposed
human study. For example, if during the development of new combination
therapies, a concern is raised that a particular combination might be antagonistic,
xenograft studies may be used to test that hypothesis. Favorable results with the
combination, such as those reported for trastuzumab and paclitaxel in Baselga
Abstract 53 and Abstract 2262, would have supported a reasonable level of
80 of 97 Celltrion, Inc., Exhibit 1002

81
confidence in the ethical validity and potential success of proceeding with
developing the combination in clinical trials.
153. Based on the finding in Abstract 2262 and Baselga Abstract 53 of a
93% growth inhibition for the trastuzumab-paclitaxel combination, compared to a
70% growth inhibition for the trastuzumab-doxorubicin combination, a person of
ordinary skill in the art would reasonably have given a higher priority to the former
regimen, if a choice needed to be made. Such a higher priority is expressly
suggested in the prior art: “The combined treatment with paclitaxel plus 4D5
resulted in a major antitumor activity with 93% inhibition of growth. This result
was markedly better than doxorubicin plus 4D5 (70% inhibition). Thus, equipotent
doses of paclitaxel and doxorubicin differed in their combined effect with ARMAs,
which suggests synergy between paclitaxel and 4D5.” (Ex. 1021.) The favorable
xenograft results of the trastuzumab-paclitaxel combination against HER2+ breast
cancer pointed the way to an obvious next step in the drug development process:
clinical trial of the trastuzumab-paclitaxel combination for patients with HER2+
breast cancer. Indeed, the prior art stated that those clinical trials were already
underway. (Ex. 1020 at 743.)
154. I also note that Dr. Sliwkowski submitted his declaration in 2009,
which is more than ten years after the date that the application for the ’441 patent
was filed. As support for his assertions, he relied on an article published in 2001,
81 of 97 Celltrion, Inc., Exhibit 1002

82
which is also later than the date that the application was filed. However, in 1999
(which is later than the filing date of the patent but earlier than Dr. Sliwkowski’s
2009 declaration and earlier than the 2001 article upon which Dr. Sliwkowski
relied), Dr. Sliwkowski co-authored an article that explicitly relied upon xenograft
data “to determine how best to use this antibody both as a single agent and in
combination with established cancer therapeutics.” (Ex. 101727 at 2242.) Dr.
Sliwkowski’s research in xenografts was aimed at demonstrating that some
combinations are “rational” to test in “human clinical trials.” (Id. at Abstract.) In
that article, Dr. Sliwkowski reports that in order to test a hypothesis that
trastuzumab is synergistic with chemotherapeutic agents, he tested the drugs
together in vitro and then, as a confirmatory tool, he tested the drugs in mouse
tumor xenografts. (Id.)
155. Dr. Sliwkowski’s assertions that a person of ordinary skill in the art
would not have predicted synergistic results between trastuzumab and paclitaxel
based on xenografts rings hollow in the face of his reliance on xenografts to test for
synergy. Dr. Sliwkowski’s published xenograft testing and reliance in 1999 is
aligned with the understanding of a person of ordinary skill in the art as of
27 M. Pegram et al., Inhibitory Effects of Combinations of HER-2.neu Antibody and
Chemotherapeutic Agents Used for Treatment of Human Breast Cancers, 18
ONCOGENE, 2241-2251 (1999). (“Pegram 1999”).
82 of 97 Celltrion, Inc., Exhibit 1002

83
December 1996. His declaration, submitted in 2009, and relying on art from 2001,
is not.
E. Claim-by-Claim Analysis of Obviousness
156. Independent claim 1 claims a method for the treatment of a human
patient with a breast cancer that overexpresses ErbB2 receptor with the
combination of an antibody which binds to epitope 4D5 within the ErbB2
extracellular domain sequence, a taxoid, and a further growth inhibitory agent in an
amount that is effective to extend the time to disease progression.
157. The patient described in claim 1 has a HER2+ breast cancer. The
antibody described in claim 1 is directed to epitope 4D5 within the ErbB2
extracellular domain, and therefore, may be trastuzumab. Paclitaxel is a taxoid.
As I explained above, cisplatin is a growth inhibitory agent within the meaning of
the patent claims. Baselga 1996, Seidman 1996, Pegram 1995, and the 1995 PDR
entry for Taxol® would have motivated to a person of ordinary skill in the art to
administer trastuzumab, paclitaxel and cisplatin to treat metastatic HER2+ breast
cancer patients with a reasonable expectation of success that the combination
would extend the time to disease progression, as discussed in Section IX.C
above.28 With regard to the amount of each drug in the combination to use, a
28 To the extent the phrase “extend the time to disease progression” is construed to
mean relative to an untreated patient, as opposed to meaning relative to treatment
83 of 97 Celltrion, Inc., Exhibit 1002

84
person of ordinary skill in the art would have used the reported effective amounts
of each agent (i.e., for trastuzumab, a loading dose of 250 mg, followed by 100 mg
per week, see Ex. 1020 at 738-39, Ex. 1022; for paclitaxel, 135 mg/m2 or 175
mg/m2, see Ex. 1012 at 685; and for cisplatin, 75 mg/m2 , see Ex. 1022) as a
starting point. To the extent that the amount of any drug needed to be adjusted for
a “generic” recommendation or for a specific patient, a person of ordinary skill in
the art would have known how to adjust and optimize the dosage amounts using
routine and conventional techniques. Therefore, claim 1 is obvious over Baselga
1996, Seidman 1996, Pegram 1995, and the 1995 PDR entry for Taxol®.
158. Independent claim 5 claims a method for the treatment of a human
patient with breast cancer characterized by overexpression of ErbB2 receptor with
an anti-ErbB2 antibody which binds epitope 4D5 within the ErbB2 extracellular
domain sequence, a taxoid, and a further therapeutic agent, in an effective amount.
159. The patient population defined in claim 5 is the HER2+ breast cancer
population, and the antibody, directed against the HER2 receptor, may be
with a taxoid alone, my opinion is still the same because a person of ordinary skill
in the art would have known that treatment with paclitaxel extends the time to
disease progression relative to no treatment. By extension, a treatment that extends
the time to disease progression relative to paclitaxel also must extend the time to
disease progression relative to no treatment.
84 of 97 Celltrion, Inc., Exhibit 1002

85
trastuzumab. Paclitaxel is a taxoid. Cisplatin, a chemotherapeutic agent, is within
the definition of the term “further therapeutic agent” as defined above. As I
explained above, Baselga 1996, Seidman 1996, Pegram 1996, and the 1995 PDR
entry for Taxol® would have motivated person of ordinary skill in the art to use the
claimed combination to treat patients in the claimed population, in amounts that
would provide a reasonable expectation of success in treating the cancer. With
regard to the amount of each drug in the combination to use, a person of ordinary
skill in the art would have used the reported effective amounts of each agent as a
starting point, as discussed above for claim 1. To the extent that the amount of any
drug needed to be adjusted for a “generic” recommendation or for a specific
patient, a person of skill in the art would have known how to adjust and optimize
the dosage amounts using routine and conventional techniques. Therefore, claim 5
is obvious over Baselga 1996, Seidman 1996, Pegram 1995, and the 1995 PDR
entry for Taxol®.
160. Independent claim 16 claims a method for the treatment of a human
patient with ErbB2 overexpressing breast cancer with an antibody that binds
epitope 4D5 within the ErbB2 extracellular domain sequence, a taxoid, and a
further growth inhibitory agent, in the absence of an anthracycline derivative, in an
amount that is effective to extend the time to disease progression. The patient
population described in this claim has HER2+ cancer that has the potential to
85 of 97 Celltrion, Inc., Exhibit 1002

86
metastasize, and the antibody, directed against the HER2 receptor, may be
trastuzumab. Paclitaxel is a taxoid. Cisplatin is a further growth inhibitory agent
within the meaning of the ’549 patent claims as defined above. Baselga 1996,
Seidman 1996, Pegram 1995, and the 1995 PDR entry for Taxol®, would have
motivated a person of ordinary skill in the art to use the claimed combination, in
amounts that would provide a reasonable expectation of success in meeting the
efficacy limitation of the claim. With regard to the amount of each drug in the
combination to use, a person of ordinary skill in the art would have used the
reported effective amounts of each agent as a starting point, as discussed above
with respect to claim 1. To the extent that the amount of any drug needed to be
adjusted for a “generic” recommendation or for a specific patient, a person of skill
in the art would have known how to adjust and optimize the dosage amounts using
routine and conventional techniques.
161. With respect to the limitation in claim 16 requiring “the absence of an
anthracycline derivative,” a person of skill in the art would have been motivated to
exclude an anthracycline derivative from the combination in order to avoid the
cardiotoxicity that is associated with that class of drugs. While treating patients
with anthracyclines is often unavoidable in the course of a patient’s cancer
treatment, limiting the total dose of an anthracycline is a goal. Therefore,
particularly for patients who had already been treated with an anthracycline or
86 of 97 Celltrion, Inc., Exhibit 1002

87
those with pre-existing cardiomyopathy regardless of cause, it would have been
obvious to not include the drug in the combination of trastuzumab and paclitaxel.
A person of ordinary skill in the art would have expected that many patients had
previous anthracycline treatment, given that anthracyclines were a first line therapy
for breast cancer. (Ex. 1016 at 1693.) Indeed, paclitaxel was indicated for use
only after first-line therapy that included anthracycline. (1995 TAXOL PDR (Ex.
1012) at 683.) Therefore, claim 16 is obvious over Baselga 1996, Seidman 1996,
Pegram 1995, and the 1995 PDR entry for Taxol®.
162. Claims 2-4 depend from claim 1and therefore incorporate all of the
limitations in claim 1. Claim 7 depends from independent claim 5 and therefore
incorporates all of the limitations of claim 5. Claim 2 further requires that the
antibody is a humanized 4D5 anti-ErbB2 antibody; claim 3 further requires that the
antibody crossblocks binding of 4D5 to the ErbB2 extracellular domain sequence;
claim 4 further requires that the antibody binds to amino acid residues in the region
from about residue 529 to about residue 625 of the ErbB2 extracellular domain
sequence; and claim 7 requires that the antibody is a humanized 4D5 anti-ErbB2.
These requirements are all properties of trastuzumab. Therefore, it is my opinion
that claims 2-4 and 7 would have been obvious over Baselga 1996, Seidman 1996,
Pegram 1995, and the 1995 PDR entry for Taxol® for the same reasons that
independent claims 1 and 5 would have been obvious.
87 of 97 Celltrion, Inc., Exhibit 1002

88
163. Claim 6 depends from independent claim 5 and therefore incorporates
all of the limitations from claim 5. Claim 17 depends from independent claim 16
and therefore incorporates all of the limitations of claim 16. Claims 6 and 17 each
further require that the breast cancer is metastatic breast carcinoma (another word
for tumor). Therefore, it is my opinion that claims 6 and 17 would have been
obvious over Baselga 1996, Seidman 1996, Pegram 1995, and the 1995 PDR entry
for Taxol® for the same reasons that independent claims 5 and 16 would have been
obvious.
164. Claim 8 depends from claim 7, which depends from claim 5. Claim 8
further requires that the antibody is administered as a 4 mg/kg dose and then
weekly administration of 2 mg/kg. The dose of the trastuzumab that was shown to
be clinically effective when used alone and when used in combination with
cisplatin was a 250 mg loading dose followed by weekly 100-mg doses. (Baselga
1996 (Ex. 1020); Pegram 1995 (Ex. 1022).) For an average patient of about 62.5
kg (approximately 143 pounds), the dose described in Baselga 1996 and Pegram
1995 is the same as a 4 mg/kg loading dose, followed by 1.6 mg/kg weekly doses.
The dose in Baselga 1996 and Pegram 1995 would have been the starting point for
a POSA designing a combination therapy with trastuzumab, cisplatin, and
paclitaxel. A POSA would have been motivated to optimize this regimen for
efficacy using routine and conventional techniques and would have arrived at the
88 of 97 Celltrion, Inc., Exhibit 1002

89
claimed dosage amounts. Therefore, it is my opinion that claim 8 would have been
obvious over Baselga 1996, Seidman 1996, Pegram 1995, and the 1995 PDR entry
for Taxol® for the same reasons that independent claim 5 would have been
obvious.
165. Claim 9 depends from independent claim 5 and therefore incorporates
all of the limitations in claim 5. Claim 9 further requires that the taxoid is
paclitaxel. As explained, the combination of trastuzumab/paclitaxel/cisplatin
would have been obvious. Therefore, it is my opinion that claim 9 would have
been obvious over Baselga 1996, Seidman 1996, Pegram 1995, and the 1995 PDR
entry for Taxol® for the same reasons that independent claim 5 would have been
obvious.
166. Claim 10 depends from independent claim 5 and therefore
incorporates all of the limitations from claim 5. Claim 10 further requires that
“efficacy is measured by determining the time to disease progression or the
response rate.” As discussed above in Section VI.E, person of ordinary skill in the
art would have been well aware of both time to disease progression and response
rate as part of a clinical trial and would have measured efficacy with both of those
metrics as a matter of course. Therefore, it is my opinion that claim 10 would have
been obvious over Baselga 1996, Seidman 1996, Pegram 1995, and the 1995 PDR
89 of 97 Celltrion, Inc., Exhibit 1002

90
entry for Taxol® for the same reasons that independent claim 5 would have been
obvious.
167. Claims 11, 14, and 15 depend directly or indirectly from independent
claim 5 and therefore incorporate all of the limitations from claim 5. Claim 11
further specifies types of agents that may be the “further therapeutic agent.” One
of the listed types of agents is a “growth inhibitory agent.” Claim 14 further
requires that the further therapeutic agent is a growth inhibitory agent. Claim 15
further requires that the growth inhibitory agent is a DNA alkylating agent.
Cisplatin is a growth inhibitory agent within the express definition given in the
patent, and is a DNA alkylating agent. Therefore, it is my opinion that claims 11,
14, and 15 would have been obvious over Baselga 1996, Seidman 1996, Pegram
1995, and the 1995 PDR entry for Taxol® for the same reasons that independent
claim 5 would have been obvious.
F. Secondary Considerations
168. As I noted above, I understand that objective indications of non-
obviousness, such as purported unexpected results or the fulfillment of a long-felt
need, must be considered in an obviousness analysis. Patent Owner submitted the
Hellmann Declaration during prosecution of the application for the ’549 patent.
This declaration alleged two unexpected results: (1) that the combination of
paclitaxel and trastuzumab resulted in unexpected synergy, and (2) that the
90 of 97 Celltrion, Inc., Exhibit 1002

91
combination of trastuzumab and doxorubicin resulted in unexpected toxicity. I
disagree with both of these assertions.
1. Dr. Hellmann Did Not Point to Data that Established that the Combination of Paclitaxel and Trastuzumab Results in Synergy
169. Dr. Hellmann opined in her declaration that the combination of
trastuzumab and paclitaxel is “surprisingly synergistic with respect to extending
TTP” because it achieves a therapeutic effect in terms of TTP which is greater than
that expected by the simple addition of the effects of the component drugs.” (Ex
1008, ¶ 6.) I do not agree that this result is surprising in view of the prior art, nor
do I agree that the data she cited demonstrated clinical synergy of the claimed
combination.
170. As an initial matter, Dr. Hellmann’s alleged synergy is limited to the
two-drug combination of trastuzumab/paclitaxel and she did not allege any
evidence of synergy of the claimed combination of an anti-ErbB2 antibody, a
taxoid and a third agent. Therefore, regardless of whether Dr. Hellmann
demonstrated synergy and regardless of whether synergy would have been
expected, Dr. Hellmann offered no evidence about the combinations that are
claimed in the ’549 patent. Still, below I address the evidence of synergy that Dr.
Hellmann alleged in her declaration.
91 of 97 Celltrion, Inc., Exhibit 1002

92
171. Practically speaking, the outcome of interest to a person of ordinary
skill in the art in a clinical trial of a two-drug combination is whether the results
show that patients are more likely to benefit from the combination (in terms of
either the duration or quality of response) than they are from treatment with the
single agents, either individually or sequentially. With respect to the combination
of trastuzumab and paclitaxel, while a person of ordinary skill in the art would not
have been able to predict with complete accuracy the clinical efficacy results based
on the available single agent clinical data, single agent preclinical data, and
combination preclinical data, a person of ordinary skill in the art would not have
found the clinical efficacy results Dr. Hellmann reported to be surprising in light of
the data that were available in the prior art.
172. The efficacy results Dr. Hellmann reported were reasonably expected
based on the known clinical efficacy of each of trastuzumab and paclitaxel as
single agents in patients with metastatic HER2+ breast cancer, and based on the
known activity of the combination in mouse xenografts. (Ex. 1020; Ex. 1011; Ex.
1019.) Xenograft studies were performed using live cancer cells in live organisms,
and were considered a reasonably accurate model for predicting clinical activity, as
I explained above in Section VI.C.4. The xenografts studies for the trastuzumab-
paclitaxel combination provided a meaningful level of assurance that significant
and synergistic anti-cancer activity could be achieved in human patients.
92 of 97 Celltrion, Inc., Exhibit 1002
93
173. The efficacy results Dr. Hellmann reported were also reasonably
expected based on the general principles supporting the use of combination therapy
against cancer: that multiple drugs will kill more cancer cells than a single drug
alone, provided the combination therapy can be tolerated. This understanding of
combination therapy includes an expectation of improved outcome with
concomitant administration of two active agents because of the collateral
sensitivity and resistance mechanisms that are inherent in a cancer/treatment
system. As explained, treatment with some agents prime cells to be particularly
sensitive to treatment with other agents; if two agents are given at the same time, it
is expected that the second agent will then be able to kill more cells than it would
have, had it been given alone.
174. Moreover, reliance on the data presented in the Exhibits to the
Hellmann Declaration is flawed, and a conclusion of synergy from those data is not
possible. Dr. Hellmann asserted that Exhibit B attached to her declaration
provided the results of the H0648 trial in which patients were treated with
HERCEPTIN® and paclitaxel. (Id.) She further asserted that Exhibit C attached
to her declaration provided the results of the H0650 study, in which patients were
treated with HERCEPTIN® as a single agent at the same dose as in the H0648
trial. (Id.) According to Dr. Hellmann, these data show that paclitaxel alone
extended TTP by 2.8 months and HERCEPTIN® alone extended TTP by 3.5
93 of 97 Celltrion, Inc., Exhibit 1002

94
months (for a combined TTP of 2.8 + 3.5, or 6.3 months), whereas the combination
of HERCEPTIN® and paclitaxel extended TTP by 6.9 months. (Id.) Dr.
Hellmann concludes that “the combination is surprisingly synergistic with respect
to extending TTP.” (Id.)
175. The data presented in the Hellmann declaration are insufficient to
draw a conclusion of synergy. For example, the trastuzumab only and
trastuzumab/paclitaxel combination studies were different. (See Ex. 1008
(Hellmann Dec. at 13-14 (Exhibits A- C).) Dr. Hellmann did not provide any
information to conclude that a comparison of values across these separate studies,
which presumably used different protocols and included different patient
populations, would be proper.
176. Further, Dr. Hellmann cited only the median TTP, but ignored the
95% confidence interval data reported for TTP. (Id.) When factoring in the 95%
confidence intervals—as is proper—the TTP values for monotherapy groups
overlap with the values for the trastuzumab-plus-paclitaxel group. Specifically, in
the H0650 study, the patients who received only Herceptin® had a median TTP of
3.5 months, with a 95% confidence interval of 2.8 – 5.5 months. (Hellmann Dec.
at 13 (Exhibit B).) In the H0648 study, the patients who received only paclitaxel
had a median TTP of 2.8 months, with a 95% confidence interval of 1.6 – 5.4
months. (Hellmann Dec. at 14 (Exhibit C).) In that same study, the patients who
94 of 97 Celltrion, Inc., Exhibit 1002

95
received Herceptin® plus paclitaxel had a median TTP of 6.9 months, with a 95%
confidence interval of 5.3 – 9.9 months. (Hellmann Dec. at 14 (Exhibit C).)
177. Even assuming that TTP is properly additive (i.e., assuming that it is
meaningful to add the Herceptin®-only and paclitaxel-only TTPs together), and
properly compared across studies, given the overlap in the confidence intervals, no
conclusion can be drawn about relative TTPs. The data show that the TTP for the
Herceptin®-only group was somewhere in the range of 2.8 – 5.5 months; the TTP
for the paclitaxel-only group was 1.6 – 5.4 months, and the TTP for the
Herceptin/paclitaxel group was 5.3 – 9.9. months. Given these data, the TTP for
each group could be the same, e.g., 5.3, or 5.4, or even 5.5 months. This means
that based on the data presented by Dr. Hellmann, one is unable to discern whether
there is actually any meaningful difference between TTP for trastuzumab alone
versus the trastuzumab/paclitaxel combination.
178. For at least these reasons, the Hellmann Declaration does not show a
synergistic relationship between trastuzumab and paclitaxel in humans.
2. The Combination of Trastuzumab and Doxorubicin Did Not Result in Unexpected Toxicity and is Not Relevant to the Claimed Combination
179. Dr. Hellmann also opined that combining trastuzumab with
anthracycline/cyclophosphamide (AC) chemotherapy unexpectedly “resulted in a
syndrome of myocardial dysfunction (similar to that observed with anthracyclines)
95 of 97 Celltrion, Inc., Exhibit 1002

96
substantially more commonly than with AC alone.” (Ex. 1008 at ¶ 4.) Regardless
of this observed result, unexpected or not, as discussed above, a person of ordinary
skill in the art would have been motivated to pursue a combination treatment that
excluded doxorubicin in order to treat the many patients who had already been
treated with first-line-agent doxorubicin.
180. Further, I fail to see the connection between an adverse event that is
observed with a combination of trastuzumab and doxorubicin on the one hand, and
the claimed combination of an anti-ErbB2 antibody, a taxoid and a third agent on
the other. It is my opinion that Dr. Hellmann’s assertions are not relevant to the
claims of the ’549 patent.
181. Further, whether the increased myocardial dysfunction was expected
or not, it does not affect whether a person of ordinary skill of the art would have
been motivated to combine trastuzumab and paclitaxel or reasonably expected
success with that combination for the target population.
182. I am not aware of any other objective indicators of non-obviousness
that could be connected to the claims of the ’549 patent. The prior art indicates
that the combination of paclitaxel and trastuzumab had already been contemplated
before the application was filed, and therefore, any indicators would be a result of
those earlier disclosures in the prior art, and not a result of the disclosure in the
96 of 97 Celltrion, Inc., Exhibit 1002

'549 patent. I reserve the right to respond to any assertions of secondary
considerations that Patent Owner alleges during this proceeding.
X. CONCLUSION
183. For all of the reasons discussed above, it is my opinion that claims 1-
11 and 14-17 of the '549 patent are obvious in view of the prior art.
184. I hereby declare that all statements made herein of my own
knowledge are true and that all statements made on information and belief are
believed to be true; and further that these statements were made with the
knowledge that willful false statements and the like so made are punishable by fine
or imprisonment, or both, under Section 1001 of Title 18 of the United States
Code.
Dated: 2 J N fl(lCH 2 0 J 7 By: Robert Earhart, M.D., Ph.D.
99
97 of 97 Celltrion, Inc., Exhibit 1002


















