Understanding Care
53
Duchenne Muscular Dystrophy : Understanding Care 101 Brenda Wong, MD Cincinna< Children’s Hospital Medical Center 24 June 2010
-
Upload
parent-project-muscular-dystrophy -
Category
Documents
-
view
215 -
download
1
description
Understanding Care presented by Brenda Wong at PPMD's 2010 Annual Connect Conference
Transcript of Understanding Care

Duchenne Muscular Dystrophy :
Understanding Care 101
Brenda Wong, MD Cincinna< Children’s Hospital Medical Center
24 June 2010
CINCINNATI CHILDREN’S HOSPITAL MEDICAL CENTER MAIN CAMPUS

Acknowledgements
• PPMD/Pat
• Pa<ents and families
• NM community – esp Prof Victor Dubowitz
• Non NM Colleagues – Dr Nelson WaUs (UC Osteoporosis Center); Dr James Heubi ( DEXA lab)
Overview
• Introduc<on • Fundamentals of care: The whole pa<ent • The pa<ent with DMD: -‐ Motor func<on/dysfunc<on -‐ Growth, development, nutri<on and bone health -‐ Common GI and GU problems
• Conclusion
Understanding Care: Introduc<on
The whole pa<ent vs the disease Generic care vs specific care aspects Proac<ve care vs reac<ve care approaches
Players: -‐ Health care providers -‐ Families and care givers -‐ Pa<ents
Understanding Care: Pa<ent vs disease
Sir William Osler, M.D., C.M.
“The good physician treats the disease;
The great physician treats the pa<ent who has the disease”

INTERDISCIPLINARY MANAGEMENT OF DMD
Lancet Neurology online 30 Nov 2009

Understanding Care: Generic and specific care aspects
• Generic care: -‐ Healthy diet (Healthy Diet in Young Children Promotes Bone Mass and Lower Body Fat Over Time -‐ Am J Clin Nutr 2010 Jun 2 epub; Wosje KS et al) -‐ Hydra<on -‐ Exercise – passive range of mo<on stretches -‐ Sleep -‐ Surveillance of health problems
• Specific DMD care program: -‐ Steroids and endocrine care -‐ Cardio-‐pulmonary, PT/rehab/ortho -‐ Psychosocial, etc
Duchenne Muscular Dystrophy
• The disease -‐ DMD
and • The pa<ent with DMD

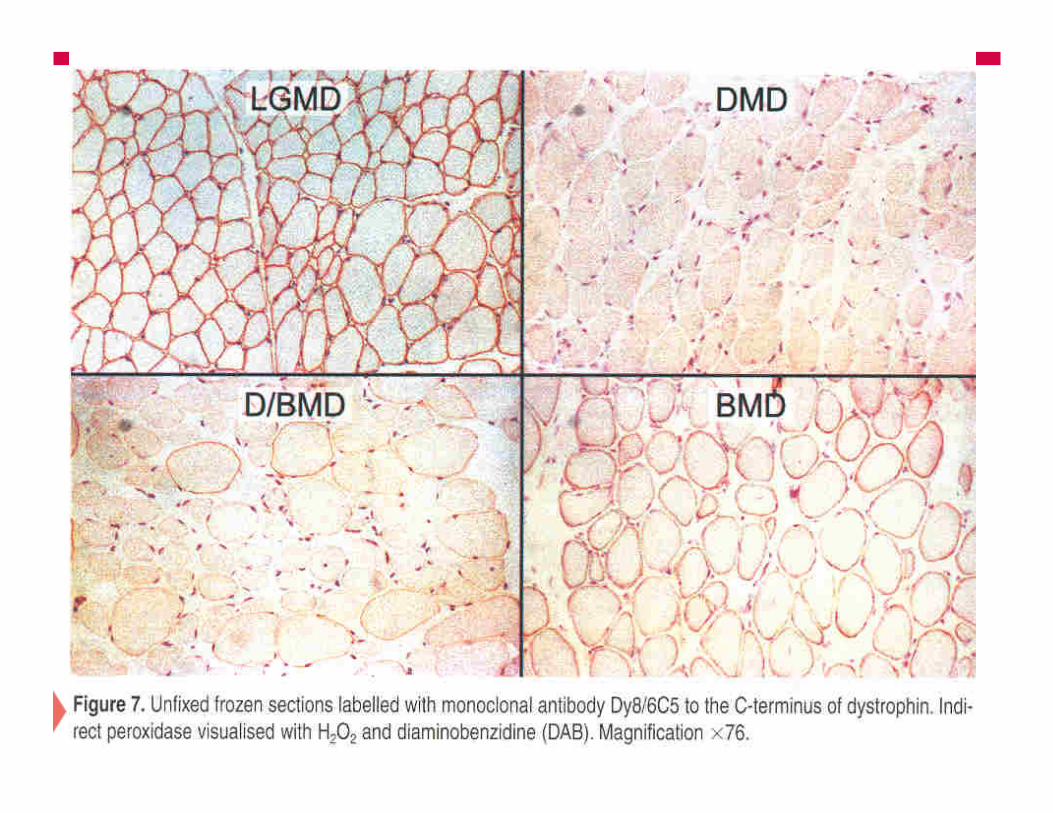
+ DYSTROPHIN


Dystrophin isoforms

Duchenne vs Becker muscular dystrophy



DMD – the disease
• Skeletal muscles -‐ Neuromuscular/PT/Rehab/Ortho
• Respiratory muscles -‐ Pulmonary
• Cardiac muscles -‐ Cardiac
• Smooth muscles -‐ GI/GU
• Brain dystrophin -‐ Neurocogni<ve
The pa<ent with DMD
• Motor func<on/dysfunc<on: -‐ strength -‐ load ( weight/BMI) -‐ alignment
• Growth, development and nutri<on -‐ Height, weight, BMI -‐ Bone health -‐ Puberty
• Cardio-‐pulmonary func<on

The pa<ent with DMD
• GI/GU func<on -‐ cons<pa<on -‐ urinary problems -‐ kidney stones
• DMD and psycho-‐social func<on -‐ home, school, work
• DMD and family : gene<c counseling -‐ Moms and extended family

Motor func<on
• Strength -‐ steroids, emerging targeted therapies
• Load -‐ Weight, BMI
• Alignment -‐ range of joint mo<on/contractures -‐ symmetry -‐ scoliosis

Steroids vs. No Steroids
• 37/54 (69%) boys exceeded the natural history of 12 years with 27 s<ll ambula<ng in 1/08.
• 17 (31%) boys on steroids lost ambula<on before the age of 12 • 26/26 (100%) boys who never used steroids lost ambula<on before age 12,
the youngest was 6.5 years old.

Load : Normal weight growth on 5 years of daily deflazacort
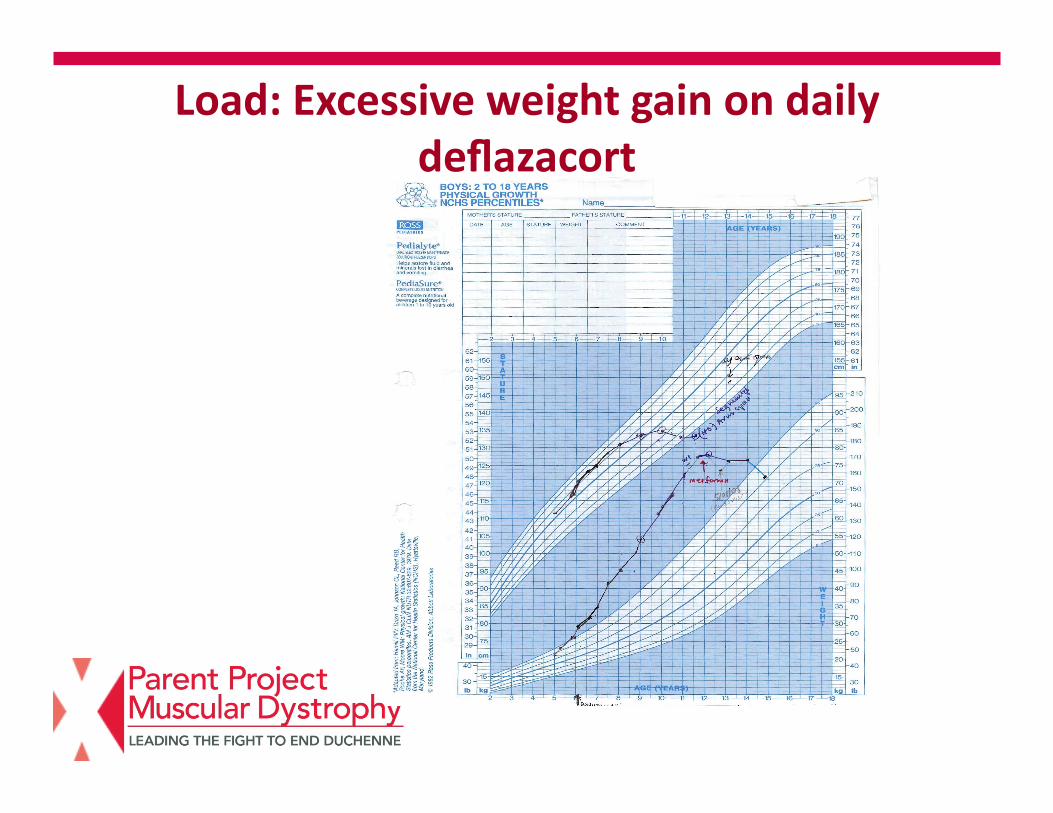
Load: Excessive weight gain on daily deflazacort
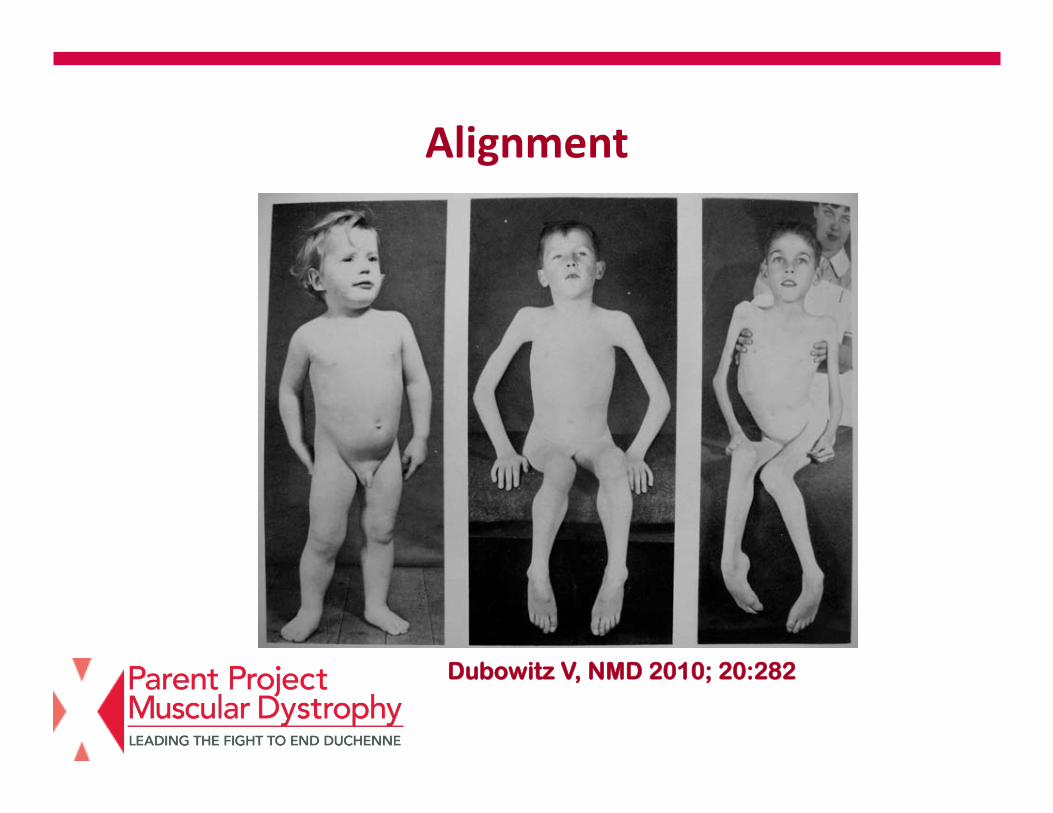
Alignment
Dubowitz V, NMD 2010; 20:282

Alignment – PT/stretch program

Alignment – PT/stretch program

Dubowitz V, NMD 2010; 20:282
Alignment, posture and mobility

Maintaining Ambulatory Status in DMD with percutaneous myofascial lengthenings, ischial weight-‐bearing KAFOs and Intensive Therapy (US Pediatrics, Touch Briefings 2008)

Combined steroids and suppor<ve physical therapy – 20.5 years old

Symmetry and spine


Growth, development and nutri<on
• Excessive weight gain with and without steroids
• Poor weight gain for older pa<ents • Delayed puberty and testosterone insufficiency with steroids
• Osteoporosis with and without steroids

Excessive weight gain with steroids
• Family history of diabetes • Diet – por<on control, low glycemic index diet
• Insulin resistance with steroids – low glycemic index diet; meoormin

Insulin resistance – diet and meoormin Jan 2008
Jan 2009 March 2010

Growth hormone may improve growth, neuromuscular and pulmonary func<on in Duchenne muscular dystrophy
RuUer, Rose, Wong, PAS 2008; WMS 2008

2-22-06 2-22-07
2-21-08 2-19-09

Growth Hormone improves growth in DMD boys with steroid induced growth failure
GH treatment of DMD boys with steroid induced growth failure resulted in:
• Improved height growth
• Improved BMI • No detrimental effects on neuromuscular/ pulmonary func<on
RuPer M et al, The Endocrine Society Annual ScienSfic MeeSng June 2010

GH and DMD Best Evidence Statement (BESt) Date published/posted: July 20, 2009 Growth Hormone Therapy in Duchenne Muscular Dystrophy Clinical Ques<on P (popula*on/problem) In children with Duchenne Muscular Dystrophy I (interven*on) do growth hormone injec*ons C (comparison) compared to placebo O (outcome) improve muscle func*on and strength?
Target Popula<on Children with Duchenne Muscular Dystrophy (DMD)
Recommenda<ons (See Table of Recommenda<on Strength following references) – It is recommended, because of insufficient evidence on the benefits and risks
of growth hormone (GH) therapy in children with Duchenne Muscular Dystrophy, that GH not be prescribed for the primary purpose of improving muscle func<on and strength
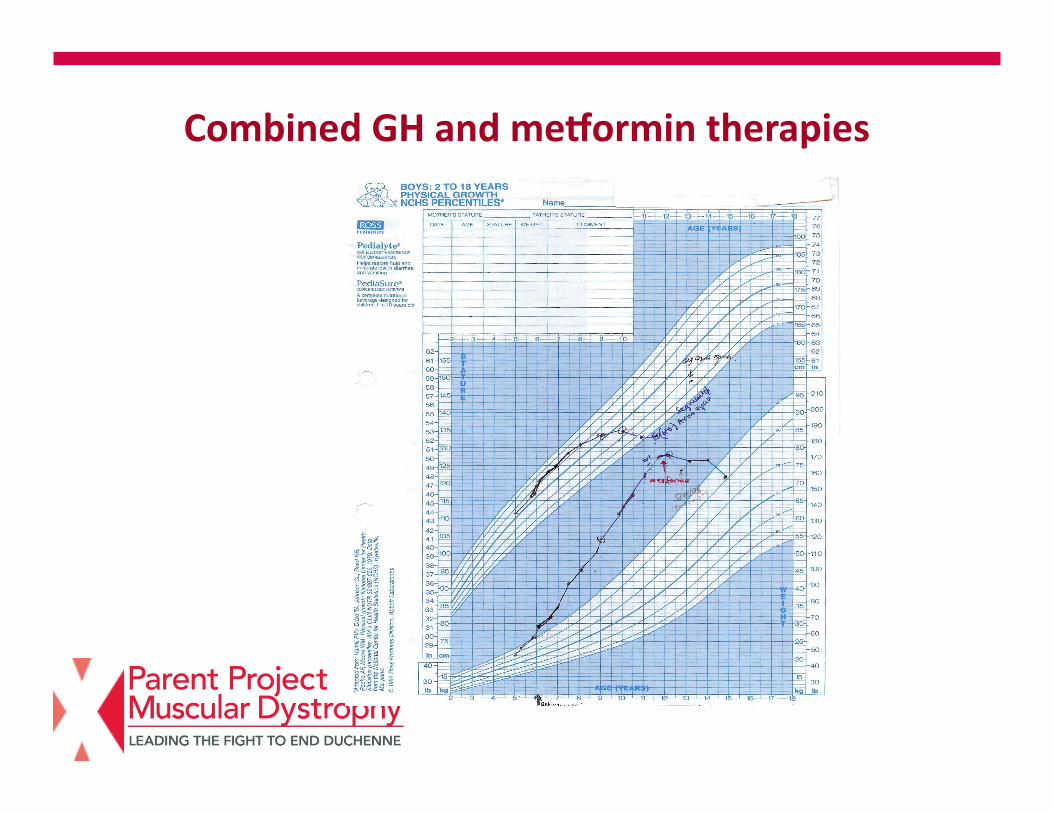
Combined GH and meoormin therapies

Oct 07
May 2010

Pubertal delays and testosterone deficiency with chronic steroids
• Secondary sexual characteris<cs and psycho-‐social health, emo<onal well being
• Effect of testosterone deficiency on bone health (osteoporosis)

Pubertal delays, osteoporosis and testosterone deficiency -‐ deflazacort since age 9.7 years old
19 years old 23 years old
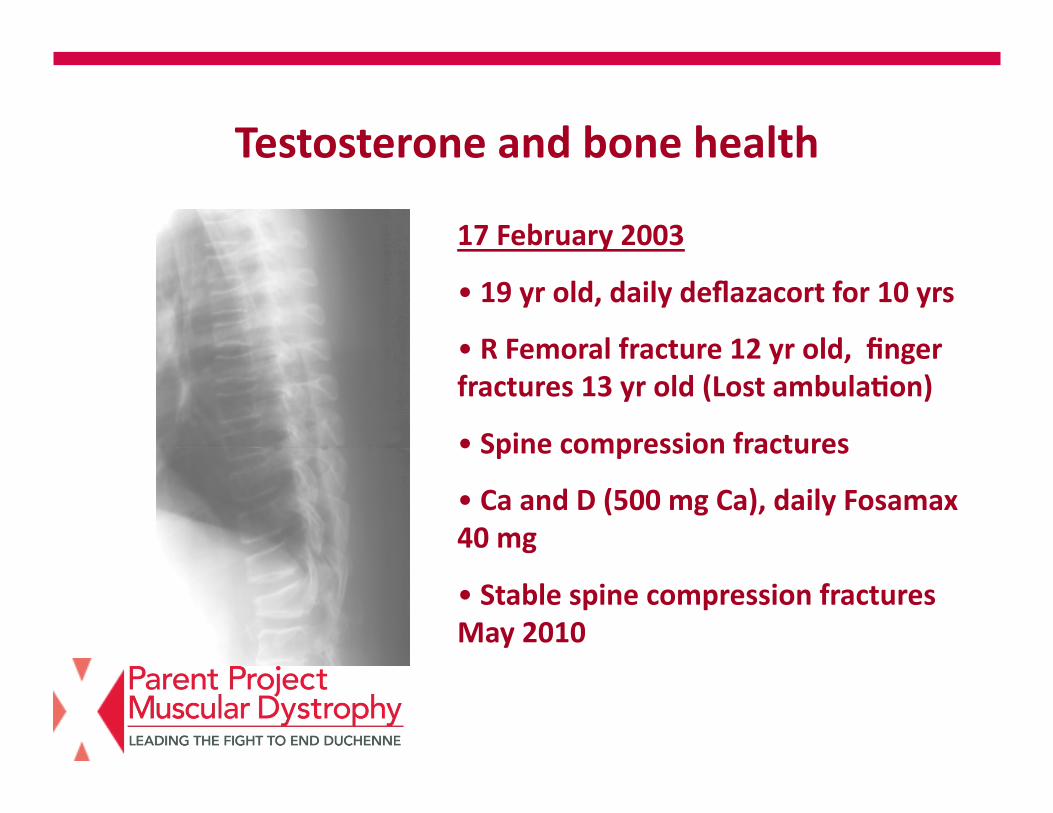
Testosterone and bone health
17 February 2003
• 19 yr old, daily deflazacort for 10 yrs • R Femoral fracture 12 yr old, finger fractures 13 yr old (Lost ambula<on)
• Spine compression fractures
• Ca and D (500 mg Ca), daily Fosamax 40 mg
• Stable spine compression fractures May 2010

Synthesis and metabolism of vitamin D in the regula<on of calcium, phosphorus and bone metabolism (Holick, 2007)

Metabolism of 25-‐Hydroxyvitamin D to 1,25-‐Dihydroxyvitamin D for non-‐skeletal func<ons. (Holick, 2007)
Muscle strength and falls – improved with increase in 25 OH D levels .
Ref: EsSmaSon of opSmal serum concentraSons of 25 OH D for mulSple health outcomes. Am J Clin Nutr 2006; 84:18-‐28

Vitamin D health
• Vitamin D deficiency: -‐ < 20 ng/ml (50 nmol/L)
• Vitamin D insufficiency:
-‐ 21 to 29 ng/ml (52 – 72 nmol/L)
• Vitamin D sufficiency:
-‐ > 30 ng/ml (75 nmol/L)
• Intoxica<on: > 150 ng/ml
• Preferred range: 30-‐60 ng/ml
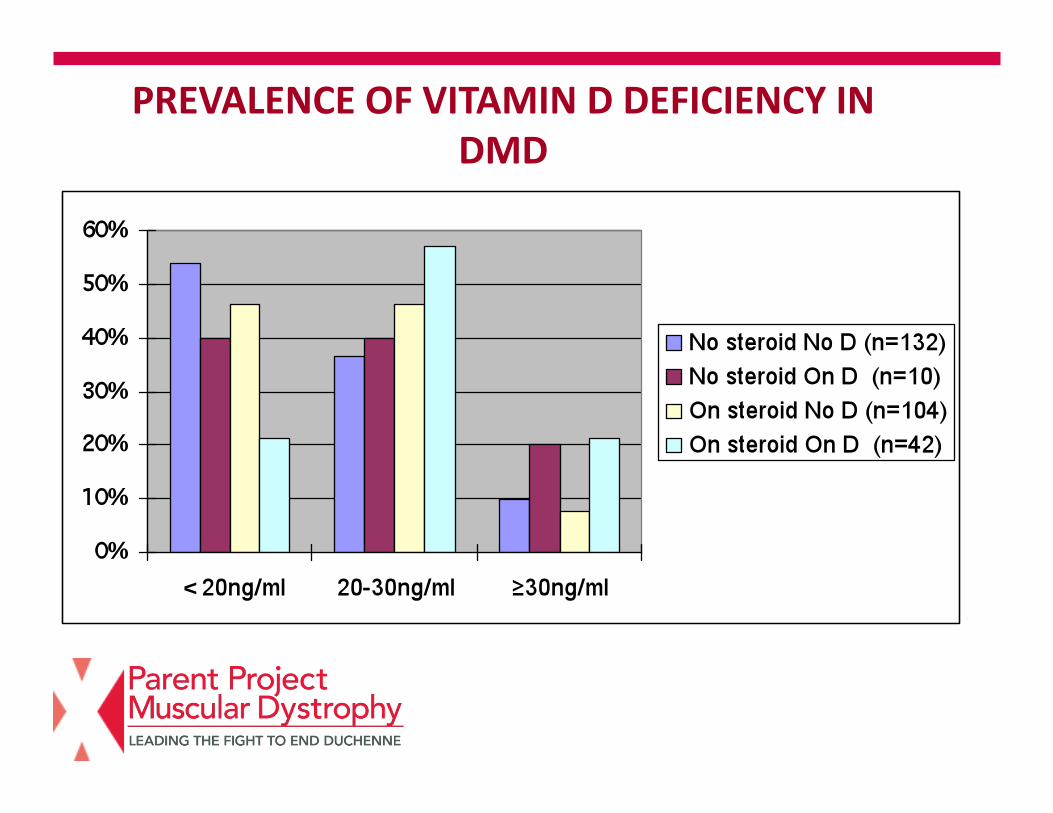
PREVALENCE OF VITAMIN D DEFICIENCY IN DMD

MANAGEMENT OF BONE HEALTH IN DMD: CCHMC D3 supplementa<on
Vitamin D supplementation for ALL neuromuscular patients based on serum 25 OH D levels (ng/ml) (with calcium as per age and steroid requirements) :
• D2 load 50,000 IU q wk for 8 weeks for < 5 ng/ml
• D3 2000 IU a day for 20-30 ng/ml
• D3 4000 IU a day for <20 ng/ml

9 yr old DMD, on daily deflazacort 15 months, inadequate Ca intake, no D supplements, 25 OHD 17.5 ng/ml. Asymptomatic
10 yr old DMD, daily deflazacort for 4 years, calcium intake 2000 mg /day, D3 2000 IU qd, 25 OH D 35.7 ng/ml, LS BMD z score -1.4, DF R1 -1.6
DMD : common GI and GU symptoms
• Abdominal pains -‐ cons<pa<on -‐ renal stones (Family history)
• Urinary frequency and bedweung -‐ cons<pa<on
• Management for renal stones : -‐ fluids ( 1 oz /lb body wt) -‐ low sodium, high potassium diet

Others….
• Gene<c counseling • Dental health • Eye evalua<ons for ocular complica<ons of chronic steroid and / GH therapies
• Neurocogni<ve and behavioral needs • Emo<onal well being of pa<ent and family

Conclusion
• Treat the pa<ent with DMD • Proac<ve an<cipatory approach • Journey with HOPE
Sir William Osler: “The future is today”

Our boys, our young men with DMD – our inspira<on
27 year old DMD pa<ent: “Yesterday is history, tomorrow is a mystery, today is a giv – that is why it is called a present. I am happy to be alive!”
“If you cannot stand up, stand out!”