UMEÅ UNIVERSITY MEDICAL DISSERTATION 2007 ISSN 0345...
48
UMEÅ UNIVERSITY MEDICAL DISSERTATION 2007 ISSN 0345-7532 ISBN 978-91-7264-383-3 _________________________________________ Studies of p63 and p63 related proteins in patients diagnosed with oral lichen planus Majid Ebrahimi
Transcript of UMEÅ UNIVERSITY MEDICAL DISSERTATION 2007 ISSN 0345...
UMEÅ UNIVERSITY MEDICAL DISSERTATION 2007 ISSN 0345-7532
ISBN 978-91-7264-383-3 _________________________________________
Studies of p63 and p63 related proteins in patients
diagnosed with oral lichen planus
Majid Ebrahimi

Studies of p63 and p63 related proteins in patients
diagnosed with oral lichen planus
Majid Ebrahimi
Department of Medical Biosciences/Pathology and Department of Odontology
Umeå University, Umeå, Sweden Umeå 2007
•

Copyright© 2007 by Majid Ebrahimi All previously published papers were reproduced with permission from the publishers. Coverpicture "Lichenes" from Ernst Haeckel's Artforms of Nature, 1904 UMEÅ UNIVERSITY MEDICAL DISSERTATIONS Series Nr. 100 ISSN 0345-7532 ISBN 978-91-7264-383-3
Printed by Print & Media, UMEÅ, 2007,2003794

In memory of my parents
•

ABSTRACT Oral lichen planus (OLP) is a chronic inflammatory disease of the oral mucosa and also one of the more common mucosal conditions mostly affecting middle aged individuals. Even though OLP is well investigated the etiology of this disease is still unknown, even if autoimmunity as a possible etiologic factor has been suggested. WHO classifies OLP as a pre malignant condition but malignant transformation of OLP is a matter of great controversy. The p53 protein is a tumour suppressor with the potential to induce apoptosis or cell cycle arrest of DNA damaged cells. Another member of the p53 family, p63, comprises six different isoforms, and plays a crucial role in the formation of oral mucosa, salivary glands, teeth and skin. p63 has also been suggested to be involved in development of squamous cell carcinoma of the head and neck (SCCHN). β-catenin, E-cadherin and epidermal growth factor receptor (EGFR) are p63 related proteins and abnormalities in their expression are suggested to be involved in development of SCCHN. Methods. Using immunohistochemistry and antibodies directed against p53 and those distinguishing between the p63 isoforms we analysed biopsies of OLP, SCCHN and normal oral tissue. We also mapped levels of p63 and p53 isoforms using RT-PCR technique. Furthermore expression of the p63 related proteins β-catenin, E-cadherin and EGFR was studied using immunoblot analysis. In an attempt to investigate autoimmunity as a causative factor of OLP we analysed sera from patients diagnosed with OLP and matched control individuals in order to see if there were autoantibodies directed against the p53 family. Results. When mapping p53 and p63 protein status decreased expression of p63 and increased expression of p53 was seen in OLP compared to normal tissue. In accordance with these results, levels of p63 RNA were also lower in OLP lesions compared with normal tissue. Concerning p53 isoforms, the “original” p53 isoform was expressed in all OLP lesions and normal control tissue. Of the other isoforms, p53β and Δ133p53 were expressed in the majority of samples. Our results regarding p63 related proteins showed a generally lower expression of these proteins in OLP lesions compared to normal control tissue. When studying sera from patients with OLP we found circulating autoantibodies against all six p63 and four p73 isoforms in two patients. Conclusions. The potential for malignant transformation of OLP is still a subject of discussion and rather controversial. While some of our results regarding status of p53 and p63 both at protein and RNA levels support this theory, other results concerning for example p63 related proteins point in the opposite direction. Based on our studies it is thus not possible to either support nor contradict the statement that OLP is a clear-cut premalignant condition. In our effort to understand the etiology of OLP we were the first to demonstrate autoantibodies against p63 and p73 in what could be a subgroup of OLP patients. OLP could thus be suggested to be not one distinct disease, but based on our data a disease comprising different subgroups.
5
Original Articles I) Ebrahimi M, Wahlin YB, Coates PJ, Sjöström B and Nylander K.
(2006). Decreased expression of p63 in oral lichen planus and graft- vs.-host-disease associated with oral inflammation. J Oral Pathol Med 35(1):46-50
II) Ebrahimi M, Boldrup L, Wahlin YB, Coates PJ, Bourdon JC and
Nylander K. (2007). Expression of novel p53 isoforms in oral lichen planus. Oral Oncology Apr 4; [Epub ahead of print] doi:10.1016/j.oraloncology.2007.01.014
III) Ebrahimi M, Boldrup L, Wahlin YB, Coates PJ and Nylander K.
(2007). Decreased expression of p63 related proteins β-catenin, E-cadherin and EGFR in oral lichen planus. [Epub ahead of print] doi:10.1016/j.oraloncology.2007.08.001
IV) Ebrahimi M, Wahlin YB, Coates PJ, Wiik A, Roos G and NylanderK.
(2007). Detection of antibodies against p63 and p73 isoforms in sera from patients diagnosed with oral lichen planus. J Oral Pathol Med. Feb;36(2):93-8.
6
•

Abbreviations AEC ankyloblepharon and ectodermal dysplasia-clefting ADULT acro-dermato-ungual-lacrimal-tooth malformation cDNA complementary DNA DLE discoid lupus erythematosus EEC ectrodactyly ectodermal dysplasia-clefting syndrome EGFR epidermal growth factor receptor GvHD graft versus host disease HCV hepatitis C virus HSCT haematopoietic stem cell transplantation LE lupus erythematosus LMS limb mammary syndrome LP lichen planus OLCL oral lichenoid contact lesion OLDR oral lichenoid drug lesion OLP oral lichen planus PCR polymerase chain reaction RT-PCR reverse transcriptase polymerase chain reaction SCCHN squamous cell carcinoma of the head and neck SHFM split-hand/foot malformation WHO World Health Organisation
7

Table of Contents Pages 1 Lichen Planus 9 2 Oral Lichen Planus 9 2.1 Clinical manifestation 9 2.2 Histopathologic features 11 2.3 Etiology 11 2.3.1 Autoimmunity 11 2.3.2 Infection 12 2.3.3 Psychological factors 12 2.4 Differential diagnoses to OLP 13 2.4.1 Lichenoid reaction 13 2.4.2 Graft versus host disease 13 2.4.3 Lupus erythematosus 14 2.4.4 Candidiasis 14 2.5 Chronic inflammation and cancer 14 2.5.1 Malignant transformation of OLP 15 3 The p53 family comprising p53, p63 and p73 15 3.1 p53 15 3.2 p73 16 3.3 p63 16 3.3.1 Function of p63 proteins 18 3.3.2 Expression pattern of p63 proteins 18 4 p63 related proteins 19 4.1 β-catenin 19 4.2 E-cadherin 20 4.3 EGFR 20 5 Aims of the studies 22 6 Materials and methods 23 6.1 Paper I 23 6.2 Paper II 24 6.3 Paper III 26 6.4 Paper IV 27 7 Results & Discussion 32 7.1 Paper I 32 7.2 Paper II 33 7.3 Paper III 34 7.4 Paper IV 35 8 General discussion 36 9 Conclusion 39 10 Acknowledgements 40 11 References 42 12 Paper I-IV 49
8
•

Introduction 1. Lichen Planus The word” lichen ” originates from botany and refers to a group of flowerless plants named moss and planus comes from the Latin word planum which means surface. It is a disease of mucosa and skin with a broad range of clinical manifestations (Jungell P, 1991). Lichen planus affects not only the oral cavity but also the skin, the male and female genital mucosa (Eisen D, 1999). In a study by Eisen vulvar and vaginal involvement was demonstrated in about 25% and skin lesions in 15% of female patients with OLP (Eisen D, 1999). Considering both females and males 5-45% of patients with oral lichen planus show skin involvement (Reichart PA & Phlipson HP, 2000). The typical skin lesions of lichen planus can be described as purplish, polygonal, planar, pruritic papules and plaques (Katta R, 2000). These skin lesions usually involve the bending muscle (flexor) surfaces of the legs and arms, especially the wrists. The nail beds can also be affected, with resultant ridging, thinning and subungual hyperkeratosis (Katta R, 2000). Involvement of the scalp can lead to scarring and permanent hair loss if untreated. 2. Oral Lichen Planus (OLP) Oral lichen first described in 1869 (Wilson E, 1869) is a chronic inflammatory disease which in contrast to lichen of the skin has a low tendency to spontaneous regression (Dissemond J, 2004). Depending on population size and demographics the prevalence of OLP differs between 0.1-4%. Bouquot et al., reported a prevalence of 1.1/1,000 in 23,616 white Americans, (Bouquot JE & Gorlin RJ, 1986) and Axell et al., when investigating 20,333 Swedish adults found oral lichen planus in 1.9%; 1.6% among males and 2.2% among females. The highest prevalence for men was found in the age group 65-74 and for women in the age group 55-64 years (Axell T & Rundquist L, 1987). In another study by Axell et al., 234 individuals from Thailand and 233 from Malaysia were investigated showing a prevalence of OLP of 3.8% and 2.1% respectively (Axell T et al., 1990). Children are only rarely affected (Jungell P, 1991).
2.1 Clinical Manifestations Oral lichen planus can appear anywhere in the oral cavity but the main sites are buccal mucosa, lateral side of the tongue and gingiva, whereas palatal lesions are uncommon (Jungell P, 1991; de Moura Castro Jacques C et al., 2003). Oral lesions are usually multiple and almost always have a bilateral, “symmetrical” distribution (Silverman S, Jr., 1991). In a study by Andreasen 115 cases of OLP were clinically evaluated and divided into six different subtypes described as either “white” or “red” forms. White forms of OLP comprise reticular, papular and plaque-like lesions which are usually asymptomatic and painless and
9
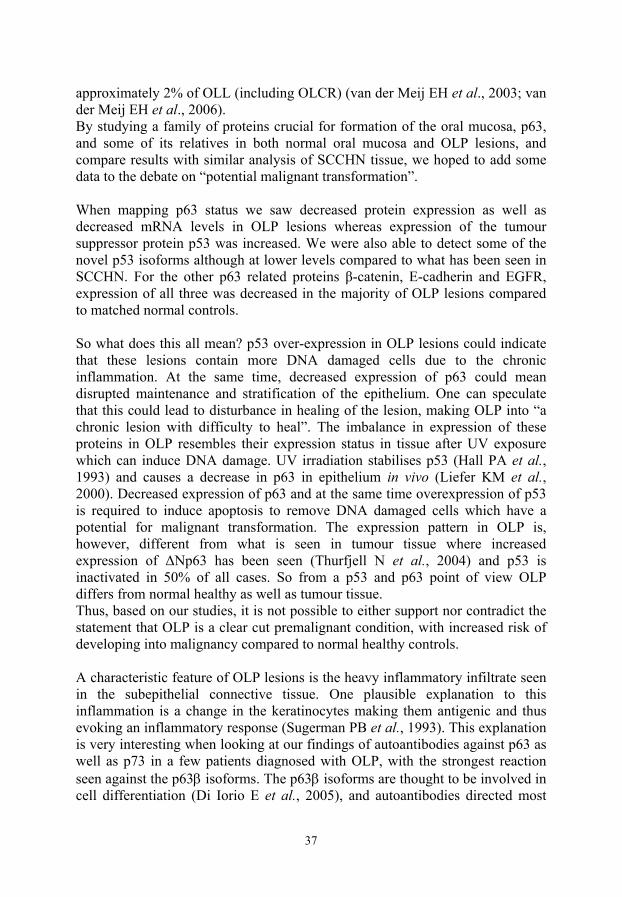
clinically appear as white keratotic lesions. Red forms include erosive (ulcerative), atrophic and bullous lesions. Different forms can co-exist in the same patient. In contrast to white lesions, red lesions are often associated with discomfort, burning sensation and in many cases also cause severe pain (Andreasen JO, 1968). (Figure 1) The reticular form of OLP is considered to be the most common type. It is characterized by a network of white striae, so called Wickham`s striae. The most commonly affected sites are the buccal mucosa and the lateral side of the tongue, whereas lesions on the lips and the palate are uncommon. The floor of the mouth is almost never involved. The reticular lesions are comparatively easy to diagnose clinically due to their characteristic features (Mollaoglu N, 2000). The papular type of oral lichen planus is sometimes called “acute” type (Pindborg JJ, 1992). It is characterized by small whitish papules 0,5mm in diameter. Due to their limited size these lesions are very difficult to observe (de Moura Castro Jacques C et al., 2003). Lesions are small flat, polygonal and of a reddish color. On the surface of these papules a white/grey covering can be seen (Wickham´s striae). This “papular type” may be seen mainly in the initial phase and is of transitory nature (Thorn JJ & Holmstrup P, 1988). Plaque-like lichen planus may present as a single lesion but multiple lesions may also be observed. The surface varies from flat to irregular shape with a whitish colour. The main location sites are the dorsal surface of the tongue and the buccal mucosa (Bricker SL, 1994) and these lesions are more common in smokers (Thorn JJ et al., 1988). Ulcerative/erosive is the second commonest type of oral lichen planus. The clinical features vary from a few to multiple lesions which usually are covered by a pseudomembrane. They are usually seen in combination with reticular lesions. The ulcerative/erosive lesions are often symptomatic and patients complain about pain, burning sensation and sometimes metal taste (de Moura Castro Jacques C et al., 2003). Atrophic type. The dominant clinical feature of these lesions is a red, erythematous mucosa due to atrophy which is poorly delineated by Wickham’s striae in the periphery. These lesions can be seen on the dorsum of the tongue (de Moura Castro Jacques C et al., 2003). The bullous type of oral lichen plans is uncommon. The bullae vary in size from a few millimetres up to several centimetres. The bullae burst soon after formation, leaving ulceration. Bullae formation may be due to edema in the connective tissue as well as basal cell degeneration (Pindborg JJ, 1992).
10
•

Figure 1. 54 year old patient suffering from bilateral OLP and skin LP since 2000. The picture is taken at the time of diagnosis before biopsy, and shows the characteristic Wickham`s striae, atrophic area and small ulceration in the left buccal mucosa. 2.2 Histopathologic features Histologically the white forms of oral lichen planus are characterized by hyperkeratosis either ortho- or parakeratinization, epithelial atrophy, basal cell liquefaction degeneration and a distinct bandlike infiltrate of lymphocytes in the superficial lamina propria (Pindborg JJ et al., 1997). The histopathological features of OLP are characteristic, however, they can also be seen in other conditions such as oral lichenoid reactions to drugs and dental material and Graft versus Host Disease (GvHD). Thus the patient´s history and clinical information is of great value for setting the correct diagnosis. 2.3 Etiology 2.3.1 Autoimmunity The etiology of oral lichen planus is so far unknown but an autoimmune cause has been suggested. OLP has been associated with some autoimmune diseases such as alopecia areata, myasthenia gravis, ulcerative colitis and vitiligo
11
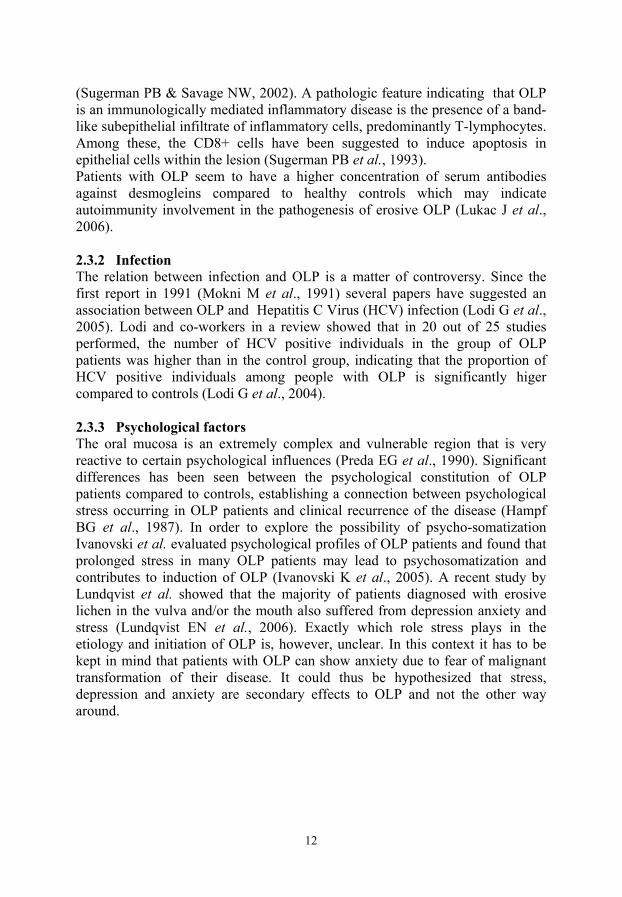
(Sugerman PB & Savage NW, 2002). A pathologic feature indicating that OLP is an immunologically mediated inflammatory disease is the presence of a band-like subepithelial infiltrate of inflammatory cells, predominantly T-lymphocytes. Among these, the CD8+ cells have been suggested to induce apoptosis in epithelial cells within the lesion (Sugerman PB et al., 1993). Patients with OLP seem to have a higher concentration of serum antibodies against desmogleins compared to healthy controls which may indicate autoimmunity involvement in the pathogenesis of erosive OLP (Lukac J et al., 2006). 2.3.2 Infection The relation between infection and OLP is a matter of controversy. Since the first report in 1991 (Mokni M et al., 1991) several papers have suggested an association between OLP and Hepatitis C Virus (HCV) infection (Lodi G et al., 2005). Lodi and co-workers in a review showed that in 20 out of 25 studies performed, the number of HCV positive individuals in the group of OLP patients was higher than in the control group, indicating that the proportion of HCV positive individuals among people with OLP is significantly higer compared to controls (Lodi G et al., 2004). 2.3.3 Psychological factors The oral mucosa is an extremely complex and vulnerable region that is very reactive to certain psychological influences (Preda EG et al., 1990). Significant differences has been seen between the psychological constitution of OLP patients compared to controls, establishing a connection between psychological stress occurring in OLP patients and clinical recurrence of the disease (Hampf BG et al., 1987). In order to explore the possibility of psycho-somatization Ivanovski et al. evaluated psychological profiles of OLP patients and found that prolonged stress in many OLP patients may lead to psychosomatization and contributes to induction of OLP (Ivanovski K et al., 2005). A recent study by Lundqvist et al. showed that the majority of patients diagnosed with erosive lichen in the vulva and/or the mouth also suffered from depression anxiety and stress (Lundqvist EN et al., 2006). Exactly which role stress plays in the etiology and initiation of OLP is, however, unclear. In this context it has to be kept in mind that patients with OLP can show anxiety due to fear of malignant transformation of their disease. It could thus be hypothesized that stress, depression and anxiety are secondary effects to OLP and not the other way around.
12
•

2.4 Differential diagnoses to OLP 2.4.1 Lichenoid reactions Oral lichenoid (lichen like) reaction is a common term comprising a variety of lesions resembling OLP both clinically and histopathologically. Oral lichenoid contact lesions (OLCL) appear as an allergic reaction in mucosa in direct contact with dental materials. A tissue reaction in mucosa in contact with dental restorative amalgam is most common but other dental materials can also cause OLCL (van der Meij EH & van der Waal I, 2003). When the material in question is removed or replaced, the majority of these lesions should regress within months. Hypersensitivity to certain medications and drugs can cause oral lichenoid drug reactions (OLDR) which, however, are rather uncommon compared to cutaneous reactions. Data regarding drugs which can cause OLDR are few, however, a limited number of studies of oral lichenoid drug reaction in connection with angiotension-converting enzyme inhibitors and nonsteroidal anti-inflammatory drugs (NSAIDs) have been published (Al-Hashimi I et al.,2007). Other agents such as penicillamine and gold have also been mentioned in the literature as causes of lichenoid reactions (Al-Hashimi I et al., 2007). 2.4.2 Graft-Versus-Host Disease (GvHD) Graft-Versus-Host Disease (GvHD) is a common complication after allogeneic haematopoietic stem cell transplantation (HSCT) and characterized by chronic inflammation affecting the skin, liver, oral mucosa and the gastrointestinal tract. The clinical and histological features of oral GvHD are similar to OLP. Despite completely different etiology, oral GvHD and OLP present similar clinical appearances (Fujii H et al., 1988; Mattsson T et al., 1992; Hasseus B et al., 2001). There are two subtypes of GvHD: acute GvHD (aGvHD) which appears within 100 days after HSCT and chronic GvHD (cGvHD) which develops 100 days after HSCT (Woo SB et al., 1997). It is likely that both GvHD and OLP share similar immunological mechanisms leading to apoptosis of basal keratinocytes and disruption of epithelial basal cell membrane, giving medical history an important role in distinguishing between the two (Hasseus B et al., 2001). Patients undergoing HSCT and concomitant therapy are at risk of developing secondary cancer, in particular leukemia and lymphoma. Development of solid tumours is not so common, however, the incidence seems higher if patients develop GvHD and the most common type being squamous cell carcinoma. Long-term monitoring of patients with GvHD is therefore recommended (Demarosi F et al., 2005).
13
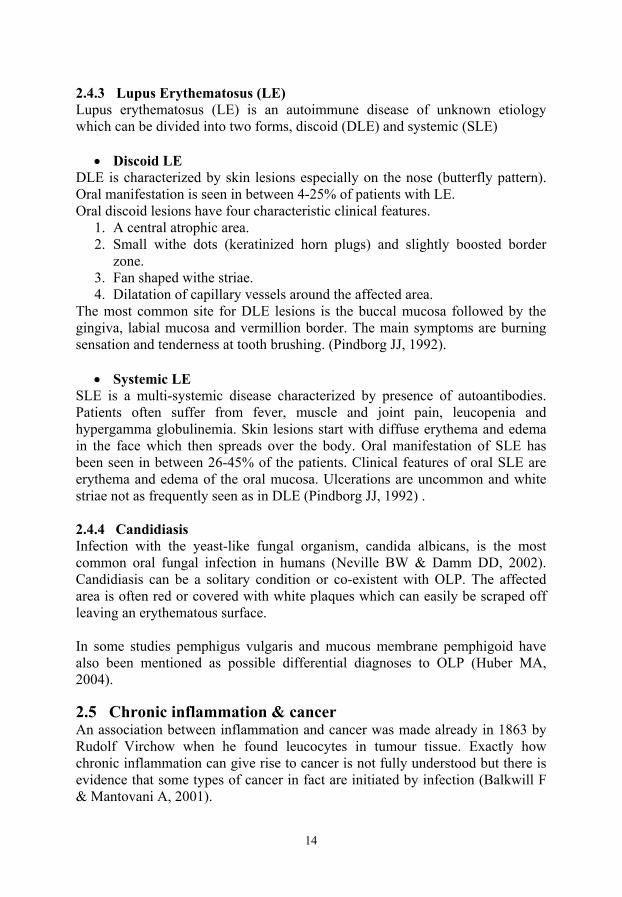
2.4.3 Lupus Erythematosus (LE) Lupus erythematosus (LE) is an autoimmune disease of unknown etiology which can be divided into two forms, discoid (DLE) and systemic (SLE)
• Discoid LE DLE is characterized by skin lesions especially on the nose (butterfly pattern). Oral manifestation is seen in between 4-25% of patients with LE. Oral discoid lesions have four characteristic clinical features.
1. A central atrophic area. 2. Small withe dots (keratinized horn plugs) and slightly boosted border
zone. 3. Fan shaped withe striae. 4. Dilatation of capillary vessels around the affected area.
The most common site for DLE lesions is the buccal mucosa followed by the gingiva, labial mucosa and vermillion border. The main symptoms are burning sensation and tenderness at tooth brushing. (Pindborg JJ, 1992).
• Systemic LE SLE is a multi-systemic disease characterized by presence of autoantibodies. Patients often suffer from fever, muscle and joint pain, leucopenia and hypergamma globulinemia. Skin lesions start with diffuse erythema and edema in the face which then spreads over the body. Oral manifestation of SLE has been seen in between 26-45% of the patients. Clinical features of oral SLE are erythema and edema of the oral mucosa. Ulcerations are uncommon and white striae not as frequently seen as in DLE (Pindborg JJ, 1992) . 2.4.4 Candidiasis Infection with the yeast-like fungal organism, candida albicans, is the most common oral fungal infection in humans (Neville BW & Damm DD, 2002). Candidiasis can be a solitary condition or co-existent with OLP. The affected area is often red or covered with white plaques which can easily be scraped off leaving an erythematous surface. In some studies pemphigus vulgaris and mucous membrane pemphigoid have also been mentioned as possible differential diagnoses to OLP (Huber MA, 2004). 2.5 Chronic inflammation & cancer An association between inflammation and cancer was made already in 1863 by Rudolf Virchow when he found leucocytes in tumour tissue. Exactly how chronic inflammation can give rise to cancer is not fully understood but there is evidence that some types of cancer in fact are initiated by infection (Balkwill F & Mantovani A, 2001).
14
•

A long-term infection induces chronic inflammation. Leucocytes, phagocytic cells and other inflammatory cells produce reactive oxygen species (ROS) and reactive nitrogen species (RNS) which normally fight infection but also can induce DNA damage in proliferating cells (Maeda H & Akaike T, 1998). Repeated tissue damage and regeneration in an environment with highly reactive oxygen and nitrogen species interacting with DNA in proliferating epithelium can thus result in permanent genomic changes such as mutation, deletion and rearrangements (Coussens LM & Werb Z ,2002). 2.5.1 Malignant transformation of OLP OLP lesions have been suggested to have a higher cell turnover than normal tissue (Epstein JB et al., 2003). The World Health Organisation, WHO, classifies OLP as a premalignant condition making ”oral mucosa more sensitive to exogenous carcinogens and thus to develop oral carcinoma” (Pindborg JJ et al., 1997). A review of 98 reports in the literature regarding malignant transformation of OLP found that the transformation rate varies between 0.4% to
5.6%, however, the majority of reports showed inadequate documentation (van der Meij EH et al., 1999). Pindborg and coworkers reported malignant transformation into squamous cell carcinoma in 2-3% of OLP patients (Pindborg JJ et al., 1997). The underlying mechanisms initiating development into SCCHN have not been clarified, however, an association between chronic inflammation and a variety of cancers is known as mentioned above (Coussens LM & Werb Z, 2002; Clevers H, 2004; Philip M et al., 2004). 3. The p53 family comprising p53, p63, and p73 3.1 P53 The TP53 gene located on chromosome 17p13.1 gives rise to the p53 protein (Lane DP & Crawford LV, 1979; Linzer DI & Levine AJ, 1979). P53 is a tumor suppressor protein initially thought to be an oncogene that was directly involved in various types of tumours. p53 functions as a transcription factor involved in induction of cell-cycle arrest or apoptosis allowing DNA repair to occur or apoptotic cell death if DNA damage can not be repaired (Romer L et al., 2006). Cellular stress such as for example DNA damage or exposure to oncogenes leads to activation of p53. Mutation which causes inactivation of the protein has been seen in approximately half of all human tumours studied. The p53 protein consists of four different domains, an amino-terminal transactivation domain (NTD), a central DNA binding domain (DBD) directly involved in specific DNA-binding and also the site for the majority of mutations, a tetramerization domain (TD) and a regulatory domain (RD) located in the C-terminus. The p53 protein has very short half-life (< 20min) and therefore only small amounts of protein can be detected in cells. There are several mechanisms controlling and maintaining levels of p53. Until 2005 it was believed that p53 comprised only
15

one isoform but then Bourdon et al .discovered at least nine different p53 isoforms in human (Bourdon JC et al., 2005) (Figure 2). In 1997 two new genes with homology to p53 were also discovered. These genes, p63 (Yang A et al., 1998) and p73 (Kaghad M et al., 1997), like p53 encode proteins which can function as transcription factors. The full-length isoforms TAp63 and TAp73 can, like p53, bind to DNA and transactivate at least some p53 targets and induce programmed cell-death, apoptosis, and cell-cycle arrest (Yang A et al., 1998). Both the p63 and the p73 genes have an alternative promoter, leading to expression of N-terminal truncated isoforms (∆Np63 and ∆Np73). 3.2 p73 The p73 gene located on chromosome 1p36.3 was first described by Kaghad et al. in 1997 located in a region repeatedly deleted in for example neuroblastoma (Kaghad M et al., 1997). The human p73 gene is composed of 15 exons and expresses at least seven alternative C-terminal isoforms and four alternative N-terminal isoforms. Altogether p73 expresses at least 35 mRNA variants which theoretically can encode at least 29 different p73 protein isoforms (Bourdon JC, 2007). The total number of p73 isoforms is most likely not definitive as alternative splicing has not been analysed (Murray-Zmijewski F et al., 2006). 3.3 P63 The p63 gene is located on chromosome 3q27-29, and encodes six proteins with homology to p53 (Yang A et al., 1998; Yang A & McKeon F, 2000). The structure of the different p63 proteins is similar to p53 with an N-terminal transactivation domain, a DNA binding domain in the central part and an oligomerization domain close to the C-terminus (Yang A et al., 1998). The three full-length proteins (TAp63α, TAp63β and TAp63γ) contain a transactivation domain in the N-terminus whereas the other three proteins lack the N-terminus transactivational domain (∆Np63α, ∆Np63β and ∆Np63γ). It was long thought that ∆Np63 proteins due to their lack of the N-terminus transactivation domain functioned as inhibitors of p53 as well as the TAp63 isoforms, which have similar functions to p53 (Yang A & McKeon F, 2000). In 2002, however, a second transactivational domain was found in the C-terminus explaining the transcriptional activity of the ΔNp63 isoforms (Ghioni P et al., 2002).
16
•

Figure 2. Schematic and simplified illustration of the p53 family proteins (Ebrahimi M et al., 2006; Murray-Zmijewski F et al., 2006). Through alternative splicing at the C-terminus, and the presence of two promoters, six different p63 isoforms are formed. The p53 and p73 families consist of more proteins, but only these isoforms were included in the present studies.(Illustration kindly provided by Stefan Pekkari, 2007)
17

3.3.1 Function of p63 p63 is required for development of normal oral mucosa, skin and other ectodermally-derived structures (Yang A et al., 1999). p63 knockout mice lacking all p63 proteins accordingly lack normal epidermal structures such as skin, hair follicles, oral mucosa, teeth, salivary glands etc. These mice die soon after birth due to dehydration (Yang A et al., 1998; Mills AA et al., 1999). During embryogenesis, TAp63 is suggested to be the molecular switch required for initiation of epithelial stratification (Koster MI & Roop DR, 2004), whereas in mature epithelium these isoforms seem to have a more differentiation related role (Thurfjell N et al., 2004). Mutations in the p63 gene in humans cause several dominantly inherited diseases including:
1. Ectrodactyly Ectodermal dysplasia Clefting syndrome (EEC). Patients with EEC syndrome show 3 clinically appearances: Ectrodactyly with anomaly of the hands and feet also known as lobster-claw, Ectodermal dysplasia with defects of ectodermally derived structures such as hair, teeth, nails and sweat glands and Clefting, cleft lip with or without cleft palate.
2. Acro-Dermato-Ungual-Lacrimal-Tooth malformations (ADULT). The ADULT syndrome differs from EEC syndrome by the absence of facial clefting.
3. Limb–Mammary Syndrome (LMS). These patients suffer from split-hand and/or foot malformation, mammary gland and nipple hypoplasia and isolated cleft palate. They do, however, not suffer from ectodermal dysplasia.
4. Hay–Wells syndrome, also named AEC syndrome for Ankyloblepharon (partial or complete fusion of eyelids) and Ectodermal dysplasia-Clefting. AEC patients have minimal or no limb anomaly in contrast to the EEC patients.
5. Split-Hand/Foot Malformations (SHFM). Patients have median clefts of the hands and feet but no other features of EEC syndrome. Approximately 10% of these patients have p63 germ line mutations.
6. Rapp–Hodgkin Syndrome. Patients suffer from ectodermal dysplasia, cleft lip and palate, malformed ears and genitourinary abnormalities (van Bokhoven H & McKeon F, 2002)
3.3.2 Expression pattern of the p63 proteins Normal oral mucosa In 2002 isoform-specific antibodies against p63 isoforms were developed (Nylander K et al., 2002). Using these antibodies, it was demonstrated that in
18
•

contrast to the p53 protein, which is expressed in all tissues, expression of p63 is limited to certain types of tissue. Data from this study also indicated that the N-terminal-truncated ΔNp63 proteins are restricted to epithelium, whereas full length TAp63 proteins are expressed also in other tissues such as endothelium and lymphoid cells (Nylander K et al., 2002; Thurfjell N et al., 2004). Cancer and p63 The p63 protein was discovered as a homolog to the tumour suppressor p53 and therefore the initial studies were designed to map similarities between these proteins. The role of p63 in tumour development seems complex and it has been suggested that p63 may have a dual function, either as a tumour suppressor (Osada M et al., 1998; Ikawa S et al., 1999; Nishi H et al., 1999) or as an oncogene (Hall PA et al., 2000; Nylander K et al., 2002) . Tumour suppressor genes are defined as genes that frequently are lost or inactivated in human tumours. With regard to this definition p63 differs markedly from p53 as it is rarely mutated in human cancer (Moll UM & Slade N, 2004). The majority of tumours keep their expression of p63 and in some cases such as SCCHN some p63 protein isoforms are over-expressed (Thurfjell N et al., 2004) indicating a more oncogenic role for p63. Results from investigations are, however, contradictory. 4. P63 related proteins 4.1 β-catenin Catenins (from catena the Latin word for chain) are proteins associated with the intercellular adhesion molecule E-cadherin (Ozawa M et al., 1989). They comprise α-catenin (102 kDa, chromosome 5q21-22) (Herrenknecht K et al., 1991), β-catenin (88 kDa, chromosome 3p21) (McCrea PD et al., 1991) and γ-catenin (placoglobin, 82 kDa, chromosome 11q11) (Knudsen KA & Wheelock MJ, 1992). ß-catenin is a part of the adherens junctions that mediate Ca²+-dependent cell-cell adhesion in epithelial cells. ß-catenin binds to E-Cadherin, a process essential for the formation and maintenance of epithelial tissue (Potter E et al., 1999). Free ß-catenin is constantly targeted for degradation through phosphorylation by a multi component complex involving axin, the tumor suppressor adenomatous polyposis coli (APC), and the serine/threonine kinase glycogen synthase kinase 3ß (GSK3ß) (Nakamura T et al., 1998). Levels of free ß-catenin in the cell cytoplasm remains low and no accumulation of ß-catenin in the cell nucleus is seen. Regulation of ß-catenin is handled in part by the Wnt signaling cascade which controls cell proliferation during development. Activation of wnt leads to inhibition of phosphorylation and thus ubiquitin-mediated destruction of free ß-catenin, leading to intranuclear accumulation of β-catenin and transactivation of target genes that induce for example proliferation (He TC et al., 1998; Barker N
19

& Clevers H, 2000; Savage NW et al., 2002). It has been suggested that ∆Np63 isoforms are involved in the activation of β-catenin signalling, an important event in many cancers (Patturajan M et al., 2002). 4.2 E-cadherin Cadherins belong to a group of four cell adhesion molecules (CAM) involved in cell to cell and cell to matrix adhesion. The other 3 molecules in the CAM group are the integrins, the immunoglobulin superfamily and the selectins (Pignatelli M & Vessey CJ, 1994; Huber O et al., 1996). Cadherins represent a distinct family of single-transmembrane domain glycoproteins which serve as specific cell adhesion molecules acting in a Ca²+dependent manner, largely by homophilic protein-protein interaction (Takeichi M, 1995). Apart from this transmembrane domain, cadherins comprise an extracellular part responsible for cadherin-cadherin interaction and an intracellular part with connection to ß-catenin and γ-catenin regulating the cadherin function (Wheelock MJ et al., 1996). There are different types of cadherins depending on tissue type. E-cadherin (E-CD) is expressed in epithelial cells and participates in the formation and maintenance of differentiated epithelial tissues, whereas N-cadherin (N-CD) mainly is expressed in neural tissue, muscle cells, and a variety of mesenchymal cells (Ramburan A et al., 2002). P-cadherin (P-CD) expression is restricted to the basal or lower layers of stratified epithelia, suggesting that P-CD may have other functions in differentiation and cell growth in addition to maintaining cellular adhesion (Hajra KM & Fearon ER, 2002; Ramburan A et al., 2002). E-cadherin maintains normal epithelial polarity, anchoring the cytoskeleton of adjacent cells via cytoplasmic proteins into the catenin family (Imai T et al., 2004). There are many reports suggesting an importance of cadherin adhesion during cell growth and differentiation. 4.3 EGFR The epidermal growth factor receptor (EGFR) was recognized as a critical protein in development and survival of epithelial tissue ever since the discovery of the epidermal growth factor in 1962 (Cohen S,1962). Expression of EGFR has been seen in a number of human epithelial carcinomas including SCCHN tumours (Matheny KE et al., 2003). Rubin and co-workers studied expression of EGFR using immunohistochemical staining and found that overexpression of EGFR can function as an early marker in SCCHN carcinogenesis and overexpression increases in parallel to observed histological abnormalities, from hyperplasia to invasive carcinoma, through dysplasia and in situ carcinoma (Rubin Grandis J et al., 1996). Stimulation of human EGFR can lead to several different phenomena important for formation and progression of SCCHN including cell proliferation, invasion, adhesion, survival and angiogenesis (Matheny KE et al., 2003). Overexpression of EGFR has been correlated to
20
•

disease progression, poor survival, poor response and resistance to cytotoxic agents (Baselga J, 2002).
21

5 Aims of the studies • Map similarities/dissimilarities between OLP, GvHD lesions, normal oral
mucosa and SCCHN concerning expression of p63 and p53. • Map presence of the novel p53 isoforms in OLP lesions, and further see if
there was any correlation between RNA and protein levels of the different p63 isoforms.
• Study expression of the p63 related proteins β-catenin, E-cadherin and
EGFR in OLP lesions and compare to expression in SCCHN.
• Study presence of autoantibodies directed against p53, p63 and p73 in sera from patients diagnosed with OLP.
22
•

6. Materials & Methods 6.1 Paper I Decreased expression of p63 in oral lichen planus and graft versus host disease associated with oral inflammation. Material Biopsies from 46 patients clinically diagnosed with oral lichen planus and from 8 patients with clinical signs of oral manifestation of GvHD were retrieved from the archive at Clinical Pathology, Umeå University. The diagnosis of oral lichen planus was histologically verified on hematoxylin eosin stained slides, and all cases of OLP were in an active state of inflammation, showing a well defined inflammatory infiltrate. None of the OLP/GvHD lesions had histologically dysplastic features (Table 1). Biopsies from clinically normal buccal mucosa from 16 smokers, 8 women and 8 men, and 16 age and sex matched non smokers as well as tumour tissue from 12 patients with SCCHN had previously been collected. None of the SCCHN tumours had, to our knowledge, developed in OLP or GvHD lesions. Antibodies Antibodies directed against TAp63, ΔNp63, p63α, p53, Ki-67 and CD8 were used for staining of consecutive sections (Table 2). As negative controls for the p63 antibodies, the corresponding preimmune serum was used at the same concentration as the antibody. As controls for staining with monoclonal antibodies an antibody with irrelevant specificity but with the same isotype as the specific antibody was used. Sections were dewaxed, rehydrated by standard procedures and subjected to boiling in 10mM citrate buffer (pH 6.0) for 15 minutes using a microwave oven for antigen retrieval. Staining was performed using a Ventana staining machine and reagents according to the supplier’s recommendation. Evaluation of staining All slides were evaluated independently by ME and KN and results compared between the two. The amount of positive cells within the whole lesion was estimated without specific calculation of percentage positive cells. Ethical permission Permission for the study was granted by the Ethical Committee (dnr 03-201; dnr 01-057; dnr 01-210).
23
6.2 Paper II Expression of novel p53 isoforms in oral lichen planus. Material Two 4 mm punch biopsies were, after informed consent, taken from the buccal mucosa on twenty consecutive patients with OLP referred to the department of Odontology, Oral Diagnostics, Umeå University. All patients were clinically and histologically diagnosed with oral lichen planus (Table 1). Fourteen were females with a mean age of 63,5 (range 42-78) and six were males with a mean age of 59,5 (range 48-75). Biopsies were also collected from twenty sex and age matched healthy controls. All samples were immediately frozen and stored at -80°C. RNA extraction One of the frozen biopsies was cut into pieces in a Petri dish placed on dry ice and transferred into a 1,5ml tube containing 250µl TRIzol reagent (Invitrogen Co, CA, USA). Samples were homogenized using a pellet mixer (MARCK Eurolab), a further 750 µl of TRIzol added and samples incubated at room temperature for 5 minutes. Mixtures were then centrifuged for 15 minutes at 13000rpm at 4°C. The upper liquid phase was moved to a new tube, diluted with an equal amount of isopropyl alcohol, incubated for 10 minutes and again centrifuged for 10 minutes at 4°C. The upper layer was carefully removed and pellets washed in 70% ethanol before drying and dissolved in DePc-H2O by pipetting 10-20 times, heated to 60° C for 10 minutes and pipetted another 10-20 times. Extracted RNA was kept at -80° C until use. cDNA synthesis and RT-PCR for analysis of p53 isoforms cDNA was synthesized using a Cloned AMV First-Stand cDNA Synthesis kit (Invitrogen) according to the manufacturers instructions. One μg of RNA was added into a total reaction volume of 20 μl. The cDNA was amplified in two rounds of PCR (nested PCR) in order to detect the different isoforms of p53. For primer sequences and combination of primers used, see Table 3. The PCR programme comprised 35 cycles with 94°C for 30s, 60°C for 45s and 72°C for 90s. PCR products were loaded on 1% agarose gels (Bourdon J C et al.,2005) All samples were analysed in duplicate and most of them in triplicate, and considered positive when positive in all replicates, or positive/variable when isoforms were detected in at least one PCR run. Quantitative PCR for analysis of p63 isoforms Quantitative RT-PCR for analysis of p63 isoforms was performed using a human p63/β-actin multi-parametric kit (Search LC, Heidelberg, Germany) and analyzed on a LightcyclerTM from Roche. In brief, cDNA was diluted 12 times and then mixed with the different primer sets to amplify each of the p63 splice
24
•

variant mRNAs individually and, simultaneously amplify β-actin to serve as an internal control for cDNA integrity and relative cDNA quantity in the different tissue samples. Primers were selected to bridge intronic sequences in order to discriminate between amplification of cDNA and contaminating genomic DNA. Reactions were analyzed on the LightcyclerTM with one denaturation cycle, 50 amplification cycles, one melting curve analysis cycle, and, finally, one cooling cycle. Reactions were run in duplicate, and a mean value of the two samples was calculated. Statistical analysis For analysis of p63 mRNA levels in OLP lesions and corresponding clinically normal oral mucosa an independent samples T-test was performed using Computer software SPSS version 12.0. Protein extraction From one frozen biopsy protein was extracted using a Micro-dismembrator (B. Braun Biotech International) for pulverizing the sample. One hundred μl of lysis buffer containing 0.5% NP-40, 0.5 % Na-deoxycholate, 0.1% SDS, 150 mM NaCl, 50 mM Tris pH 7.5, 1 mM EDTA, 1mM NaF and protease inhibitor cocktail (Sigma-Aldrich Chemie, Steinheim, Germany) was added and the pulverized samples homogenized. Protein concentrations were determined using BCA Protein Assay Kit (Pierce, Rockford, IL, USA). Immunoblot Analysis and Quantification Bio-Rad PROTEAN II xi | XL Vertical Electrophoresis system or vertical mini-gels were used according to the user manual. Thirty μg of protein was mixed with 2X loading buffer, boiled for 10 minutes and electrophoresed on 10% SDS-polyacrylamide gels. Proteins were transferred to nitrocellulose membranes (Hybond ECL, Amersham Biosciences, Little Chalton, NA, USA) and stained with ponceau red for evaluation of transfer efficiency and loading. Membranes were blocked in 5% milk with 0.4% Tween in 1X PBS, and antibodies diluted in the same blocking solution. Primary antibodies used in this study were DO-1 and DO-12 (Table 2). Ethical permission Permission for the study was granted by the Ethical Committee (dnr 05-010 M).
25

6.3 Paper III: Decreased expression of the p63 related proteins β-catenin, E-cadherin and EGFR in Oral Lichen Planus. Material Same patients as in paper II were analyzed (Table 1). Protein extraction Same method as in paper II was used. Immunoblot analysis and quantification. Same method as in paper II. Primary antibodies used were directed against ß-catenin, E-Cadherin, EGFR and β-actin. (Table 2) Secondary antibodies were goat anti-mouse (Pierce, Rockford, IL, USA), rabbit anti-mouse (Dako Cytometric, Glostrup, Denmark) and rabbit anti-sheep (Dako Cytometric). For chemiluminescence detection, Chemidoc XRS (Bio-Rad Lab, CA, USA) and Quantity one (Bio-Rad) was used in combination with ECL advance (Amersham Biosciences) for development and quantification. All samples were analysed as matched pairs, meaning that one OLP lesion and corresponding matched control were analysed in parallel, though coded, as to hide which sample was lesion and which was control. Samples were run in duplicate and evaluated and quantified in matched pairs by two independent researchers (ME and LB), showing concordant results. After quantification the amount of protein in the control was divided with corresponding volume in the matched OLP sample (Ctrl/OLP). A value higher than one thus meaning higher amount of protein in controls. The mean value for each protein was also calculated for the whole group of controls and OLPs respectively and compared using statistical analysis. Statistical analysis Mann-Whitney U test was used for comparing mean levels for the different proteins between the group of controls and the group of OLP samples. The level of significance was set at 0.05. Statistical analysis was performed using SPSS statistical software version 12.0.1. Ethical permission Permission for the study was granted by the Ethical Committee (dnr 05-010 M).
26
•

6.4 Paper IV
Detection of antibodies against p63 and p73 isoforms in sera from patients diagnosed with oral lichen planus. Material Sera from twenty consecutive OLP patients referred to the department of Odontology, Oral Diagnostics, Umeå University were collected after informed consent. All patients were clinically and histologically diagnosed with oral lichen planus (Table 1). Sixteen patients were women with a mean age of 64 years (range 48-84) and four were men, with a mean age of 62 (range 54-75). None of them smoked nor used snuff. The majority used alcohol. Three women had immunosuppressive treatment, one after lung transplantation and the other two suffering from cranial arteritis (polymyalgia rheumatica). One patient suffered from Mb Crohn and was treated with olsalazine (a sulfasalazine homologue), and one had Sjögren´s syndrome and primary biliary cirrhosis, but had never received any treatment for her diseases. At the time of referral, all patients clinically had white striations and atrophy. Ten patients had additional clinical symptoms: five desquamative gingivitis and ulcerations of the tongue and/or buccal mucosa, three desquamative gingivitis only and two ulcerations of the buccal mucosa. These 10 could thus based on the clinical appearance be diagnosed as having CUS. Sera were also collected from twenty controls, 14 women with a mean age of 57 (range 24-78) and 6 men with a mean age of 62 (range 42-77). Controls were healthy without known autoimmune disease and immunosuppressive treatment. As there were problems finding healthy elderly female volunteers, the control group comprised more men. Tissue culture FaDu cells (ATCC), a human cell line originating from a squamous cell carcinoma of oropharynx were cultured in D-MEM (Gibco, Invitrogen) containing 10% fetal calf serum (Gibco, Invitrogen) at 10% CO2. For protein extraction cells were lysed in 0.5% NP-40, 0.5% Na-deoxycholate, 0.1% SDS, 150mM NaCl, 50mM Tris, pH 7.5, 1mM EDTA, 1mM NaF and protease inhibitor mix (7µl/3ml) (Sigma-Aldrich Chemie, Steinheim, Germany). Cells were shaken for 30 minutes on ice, sonicated for 15 seconds, shaken on ice for another 30 minutes, centrifuged for 30 minutes at 14000 rpm and the supernatant collected and protein concentration measured. In vitro transcription/translation Vectors with cDNA for all p63 isoforms in pcDNA3, myc-tagged, were kindly provided by Dr L Guerrini (Italy) and Dr F McKeon (USA). cDNA for p73α, p73β, p73γ, p73δ, HA-tagged, and p53 in pcDNA3 vector, was kindly provided
27

28
by Dr B Vojtesek, Czech Republic and Dr S Bray, Scotland. For in vitro transcription/translation (IVTT) the TNT® Quick Coupled System was used according to the manufacturer’s recommendations (Promega Corporation, Madison, WI, USA). One µl of the vector was mixed with 40µl TNT Quick Master Mix, 1µl methionine and 8µl pH20. The reaction was incubated at 30°C for 30-60 minutes. Western blotting Same method as in paper II, with the exception that eighty µg of protein was loaded into each lane. Membranes were incubated with sera from OLP patients and controls, diluted 1:200, 1:500 or 1:1000 in 5% sheep serum (NeoMarkers Fremont CA, USA). The secondary antibody was HRP conjugated sheep anti-human Ig antibodies diluted 1:20000 and binding was identified with chemiluminescence (Amersham Biosciences). After development, membranes were stripped and stained with mouse monoclonal antibodies for detection of myc, HA and DO1 (Table 2). Secondary antibody was peroxidase conjugated rabbit anti-mouse Ig diluted 1:50000 (Dako Cytomation, Denmark). Ethical permission Permission for the study was granted by the Ethical Committee (dnr 05-010 M). •
Stud
y G
ende
r M
/F
Mea
n ag
e R
ange
ye
ars
Mea
n O
LP
dura
tion
Ran
ge y
ears
Bila
tera
l le
sion
%
Skin
L
P %
Gen
ital
LP %
Tob
acco
/Snu
sus
er
%
Alc
ohol
co
nsum
ptio
n%
His
tolo
gic
conf
irm
atio
n %
I
23/2
6 63
25
-93
78
10
0
II a
nd
III
6/14
63
.5
43-7
9 5.
9 0-
23
100
50
70
10 /
5 85
10
0
IV
4/16
56
50
-86
9.6
2-20
10
0 25
60
10
/ 5
75
100
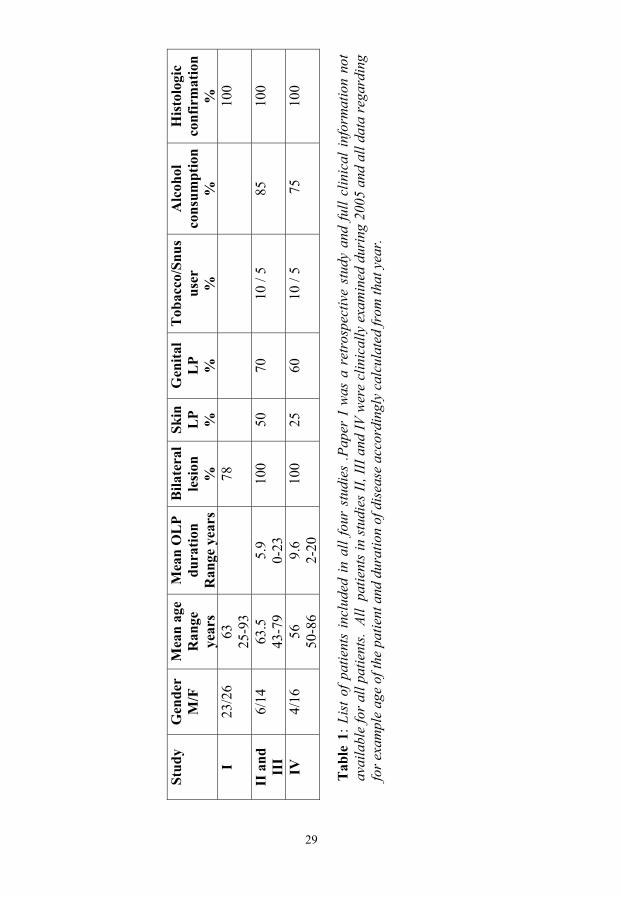
Tab
le 1
: Lis
t of p
atie
nts
incl
uded
in a
ll fo
ur s
tudi
es .P
aper
I w
as a
ret
rosp
ectiv
e st
udy
and
full
clin
ical
info
rmat
ion
not
avai
labl
e fo
r al
l pat
ient
s. A
ll p
atie
nts
in s
tudi
es II
, III
and
IV w
ere
clin
ical
ly e
xam
ined
dur
ing
2005
and
all
data
reg
ardi
ng
for e
xam
ple
age
of th
e pa
tient
and
dur
atio
n of
dis
ease
acc
ordi
ngly
cal
cula
ted
from
that
yea
r.
29

Antibody Recognition Company Dilution Paper KN-TA
TAp63
Nylander et al. 2002
1:750
I
KN-∆
∆Np63
Nylander et al. 2002
1:2000
I
KN-α
p63α
Nylander et al. 2002
1:450
I
DO7
p53, p53β, p53γ aa 20-25
Novocastra, Immunkemi F&D, Sweden
1:25
I
DO1
p53, p53β, p53γ aa 20-25
Kindly provided by Dr.B Vojtesek
1:5000
II and IV
DO12
p53, p53β, p53γ Δ40p53, Δ40p53β, Δ40p53γ Δ133p53, Δ1330p53β, Δ133p53γ aa 256-270
Kindly provided by Dr.J-C Bourdon
1:500
II
MIB-1
Ki-67 Cycling cells
DAKO Glostrup Danmark
1:50
I
CD8
Cytotoxic T-cells
DAKO
1:100
I
β –catenin
β –catenin
BD Biosciences San Jose, CA USA
1:2000
III
E-cadherin
E-cadherin
BD Transduction San Jose, CA USA
1:250
III
EGFR
EGFR
AbCam, Cambridge, UK
1:2000
III
Actin
β-actin
Chemicon, Millipore Co, MA, USA
1:20 000
III
HA
HA-tagged protein
AbCam, Cambridge, UK
1:1000
IV
Myc
Myc-tagged protein
NeoMarkers Fremont, CA, USA
1:500
IV
Table 2: List of antibodies and their target proteins used in all four papers.
30
•

1:
st
PCR
Pr
otei
n Pr
imer
and
sequ
ence
s:
p5
3 p5
3β
p53γ
e2.1
R
T1
(5´-
GTC
AC
TGC
CA
TGG
AG
GA
GC
CG
CA
-3´)
(5
´-G
AC
GC
AC
AC
CTA
TTG
CA
AG
CA
AG
GG
TTC
-3´)
∆1
33p5
3 ∆1
33p5
3β
∆133
p53γ
i4f1
R
T2
(5´-
CTG
AG
GTG
TAG
AC
GC
CA
AC
TCTC
TCTA
G-3
´)
(5´A
ATG
TCA
GTC
TGA
GTC
AG
GC
CC
TTC
TGTC
-3´)
2:nd
PC
R
p53
e2
RT2
(5
´- A
TGG
AG
GA
GC
CG
CA
GTC
AG
AT-
3´)
(5´-
AA
TGTC
AG
TCTG
AG
TCA
GG
CC
CTT
CTG
TC-3
´)
p5
3β
e2
p53b
(5
´- A
TGG
AG
GA
GC
CG
CA
GTC
AG
AT-
3´)
(5´-
TTT
GA
AA
GC
TGG
TCTG
GTC
CTG
A-3
´)
p5
3γ
e2
p53g
(5
´- A
TGG
AG
GA
GC
CG
CA
GTC
AG
AT-
3´)
(5´-
TC
GTA
AG
TCA
AG
TAG
CA
TCTG
AA
GG
-3´)
∆133
p53
i4f2
R
DN
p53
(5´-
GC
TAG
TGG
GTT
GC
AG
GA
GG
TGC
TTA
CA
C-3
´)
(5´-
CTC
AC
GC
CC
AC
GG
ATC
TGA
-3´)
∆133
p53β
i4f2
p5
3b
(5´-
GC
TAG
TGG
GTT
GC
AG
GA
GG
TGC
TTA
CA
C-3
´)
(5´-
TTT
GA
AA
GC
TGG
TCTG
GTC
CTG
A-3
´)
∆1
33p5
3γ
i4f2
p5
3g
(5´-
GC
TAG
TGG
GTT
GC
AG
GA
GG
TGC
TTA
CA
C-3
´)
(5´-
TC
GTA
AG
TCA
AG
TAG
CA
TCTG
AA
GG
-3´)
T
able
3. P
rim
er se
quen
ces a
nd p
rim
er c
ombi
natio
ns u
sed
for P
CR
ampl
ifica
tion
of d
iffer
ent p
53 is
ofor
ms.
31

7. Results & Discussion 7.1 Paper I p53 expression. In normal oral mucosa only a few cells in the basal cell layer expressed p53, whereas OLP lesions showed more p53 expressing cells. Tissue from GvHD patients showed the same pattern as OLP lesions. SCCHN tumours either completely lacked detectable p53 protein or were positive for p53 at varying degrees.
ΔNp63 expression. In normal oral epithelium, ΔNp63 expressing cells were detected in the basal and parabasal cell layers, up to approximately half to 2/3 of the epithelial thickness. In all but a few cases of OLP lesions, fewer cells expressed this subgroup of p63 and cells expressing these proteins seemed to have a lesser intensity compared to normal tissue. The difference was most obvious in areas with very atrophic epithelium. GvHD lesions showed the same pattern as OLP. In SCCHN, ΔNp63 protein was detected at a similar or higher level compared to normal mucosa.
TAp63 expression. In normal oral mucosa, expression of TAp63 protein was seen all through the epithelium. OLP and GvHD lesions showed the same pattern of TAp63 expression as normal oral mucosa but with lower levels of protein in individual cells. In SCCHN, TAp63 was detected, though seemingly at slightly lower levels compared to normal mucosa.
p63α expression. As with the other p63 isoforms, expression of p63α was weaker in OLP and GvHD lesions compared to normal oral tissue. In SCCHN expression was seen within the tumour cells.
No obvious difference in Ki-67 expression was seen in OLP and GvHD lesions, indicating no difference in the amount of cycling cells compared to normal. Looking at CD8+ cytotoxic T-cells these were mainly seen in the subepithelial inflammatory infiltrate in OLP lesions. However, a few could also be detected within the epithelium, mainly in the basal half. Also GvHD lesions expressed cytotoxic T-cells at the same location as in OLP but generally at lower frequency.
All p63 isoforms studied, TAp63, ΔNp63 and p63α, showed decreased expression in OLP and GvHD lesions compared to normal oral epithelium. In concordance with SCCHN, OLP and GvHD lesions showed decreased expression of TAp63 proteins. Expression of ΔNp63 isoforms on the other hand was decreased in OLP and GvHD lesions, in contrast to the increased expression seen in tumour tissue (Thurfjell N et al., 2004). The staining pattern of p53 and p63 seen in OLP and GvHD lesions are similar to the expression of these
32
•

proteins seen in epithelia with DNA damage due to ultraviolet light exposure, which is known to cause stabilization of p53 (Hall PA et al., 1993) as well as decreased expression of ΔNp63, which is crucial for UV-induced apoptosis (Liefer KM et al., 2000). Our findings of decreased expression of p63 and increased expression of p53 in OLP and GvHD lesions could thus indicate a coordinated action between these two related proteins in order to protect the oral mucosa from the DNA damaging effects of the underlying inflammation. 7.2 Paper II Expression of p53 isoforms using RT-PCR. In order to amplify six p53 isoforms (p53, p53β, p53γ, ∆133p53, ∆133p53β, and ∆133p53γ) in both OLP and matched normal control tissue nested RT-PCR was used. All samples were analysed as matched pairs. p53 mRNA could be detected in replicate analyses of all but 1 of the 20 OLP samples as well as all but 1 of the 20 controls. The majority of OLP (75%) and control samples (85%) also expressed the p53β and 50% of OLP and 70% of control samples expressed the ∆133p53 isoform. Expression of p53γ, ∆133p53β and ∆133p53γ was, however, limited to only a few samples. Immunoblot analysis. In order to detect different p53 isoforms also at protein levels, two antibodies DO-1 and DO-12 were used (Table 2), however, only one OLP sample showed detectable levels of p53 protein. We have thus been able to detect mRNA for 3 p53 isoforms, the “original” and two novel isoforms, in the majority of OLP lesions and normal controls analysed. The function of the novel isoforms is, so far, not known but the same isoforms have also been amplified in samples of SCCHN, at seemingly higher levels, which could indicate a more tumour related role for these isoforms. The need for nested RT/PCR in detection of these novel isoforms is taken as evidence of their low level of expression. Expression of p63 isoforms. Concerning mRNA levels of the different p63 isoforms, p63α had the highest and ∆Np63 the second highest levels of all p63 isoforms. TAp63 had the lowest levels in both OLP and corresponding normal tissue. Results showed a general decrease in levels of p63 isoforms in OLP compared to normal tissue. The most pronounced decrease seen for p63γ, p63α and ∆Np63. Thus the down regulation of p63 RNA seen in OLP lesions compared to normal controls and SCCHN is in concordance with results from paper I showing decreased expression of p63 proteins in OLP lesions.
33

7.3 Paper III Expression of β-catenin. Quantification of the 17 matched pairs that were successfully analysed in duplicate for expression of β-catenin showed lower expression of β-catenin in all but one of the OLP tissues compared to normal samples. When comparing the whole group of control samples to the group of OLP lesions analysed, the amount of β-catenin was also significantly lower in the group of OLP samples (p=0.008) (Table 4). Expression of E-cadherin. Out of the nineteen successfully analysed matched pairs lower levels of E-cadherin was seen in 16 of the OLP compared to matched normal sample. As a group, OLP also showed significantly lower levels of E-cadherin compared to the normal control group (p<0.001) (Table 4). Expression of EGFR. Quantification of 19 matched pairs analysed for EGFR expression showed lower levels of EGFR in all OLP lesions compared to normal tissus. Levels of EGFR were also lower in the whole group of OLP samples compared to the group of normal controls (p<0.001) (Table 4). Results showed that in accordance with p63, expression of β-catenin, E-cadherin as well as EGFR was decreased in the majority of OLP lesions compared to the matched normal controls. With our previous results showing decreased expression of ΔNp63, a decrease in β-catenin could be expected, as ΔNp63 can save β-catenin from degradation. Increased expression of EGFR could also be expected, once expression of its inhibitor, one of the TAp63 isoforms was decreased in OLP (Nishi H et al., 2001). These EGFR data were, however, based on in vitro analysis of cell lines, and previous studies of oral premalignant lesions and oral cancers have shown over-expression of EGFR in the majority of cases (Grandis JR& Tweardy DJ, 1993; Ke LD et al., 1998; Rubin Grandis J et al., 1998). Cancer cells, however, exclusively express a mutated form of EGFR, EGFRvIII, which is not detected by the antibody used in our study, which recognises wt EGFR only, phosphorylated as well as unphosphorylated, (Boldrup L et al., 2005). Taken together this shows the complexity when analysing human tissue samples compared to cell lines, and also the importance of using the same reagents and conditions when comparing results. In our study OLP lesions, in accordance with SCCHN tissue, showed a decreased expression of EGFR, but whether they also express the mutated EGFRvIII could not be concluded from the present analysis. E-cadherin has been suggested to inhibit apoptosis (Peluso JJ et al., 2001; Galaz S et al., 2005), thus the decreased expression of E-cadherin seen in OLP lesions could serve as an inducer of apoptosis in order to remove DNA damaged cells caused by the chronic inflammation. Our analysis of OLP lesions thus showed an expression pattern similar to SCCHN tumours with decreased expression of β-catenin and E-cadherin whereas expression of EGFR was more similar to conditions seen in normal oral
34
•

mucosa. This analysis of p63-related proteins in OLP lesions does thus not shed any light on the problematic question whether OLP is more similar to normal or malignant oral mucosa.
Ctrl/OLP
Β-catenin
E-cadherin
EGFR
> 1
16
16
19
< 1
1
3
0
Comparison of mean values
Ctrl/OLP p-value
0.008
< 0.001
< 0.001
Number of
matched pairs analysed
17
19
19
Table 4. Reproduced from paper III. Quantification data comparing matched pairs of healthy controls and patients with OLP, where a value >1 means higher protein expression in control tissue. For comparing mean values for the different proteins within the whole groups of OLP-patients and healthy controls respectively Mann-Whitney U test was used, showing significantly higher mean levels in the control group for all proteins compared to the OLP group.
7.4 Paper IV Western blot on FaDu extracts. In order to test sera on squamous cells originating from the head and neck area in Western blot, protein extract was made from FaDu cells. When incubating filters containing this protein extract with sera from patients with OLP and control persons, a distinct band of approximately 70 kDa was detected in 4 out of 18 OLP patients analysed. Western blot on p63, p73 and p53 proteins. As the size of the protein detected by OLP sera in FaDu cells was of the approximate size of some of the p63 isoforms, all 6 p63 proteins were produced using so called in vitro transcription translation technique. Sera from 2 OLP patients reacted with these p63 IVTT proteins. Both patients reacted with all six p63 isoforms with varying intensity. The strongest reaction was seen against the TAp63β protein, even though levels of this protein were hard to detect on the same gel using a myc-antibody for
35

detection of the myc-tag. One of the two OLP patients also reacted with the four p73 isoforms but none of the sera from OLP patients reacted with the p53 protein .
The p63 proteins are crucial for formation of the oral mucosa and autoantibodies against one of these six proteins, ΔNp63α, has previously been seen in patients with chronic oral ulcerations. By analysing all six p63 isoforms, four p73 isoforms and p53 with sera from patients with OLP, we could detect antibodies directed against p63 and p73 in two out of twenty patients diagnosed with OLP. Both patients reacted strongly especially with the p63β isoforms. The reason for this is not clear, although it is known that TAp63β is one of the most potent transactivators of the p63 proteins (Ghioni P et al., 2002). The TAp63β and ΔNp63β isoforms are also thought to be involved in cell differentiation (Di Iorio E et al., 2005), suggesting that the reaction against these isoforms could be a reaction against the differentiation process. The strong reaction seen against p63β in these OLP patients could thus be an indication that the epithelial cells in these lesions, due to blockage of these differentiation connected isoforms, could not differentiate normally, and thus are considered “foreign” to the body and evoke an immune response. The reason why only a part, 10%, of the OLP patients studied had antibodies is not clear but it can be speculated that the severity and duration of the disease plays a role, and both patients with antibodies directed against p63 had had their disease for more than 20 years, affecting oral as well as genital mucosa and skin.
8. General discussion One of the major problems when comparing results from different studies of OLP is the lack of universally accepted criteria (Ismail SB et al., 2007) and the fact that different authors use different criteria for inclusion of patients. In three of our four studies (II, III and IV) only patients diagnosed according to the WHO criteria were included. In study I, which was retrospective, complete clinical information was not available for all patients, and the diagnosis of OLP thus not based on both histology and clinical picture in all cases. In eleven out of totally 49 OLP patients we were not able to verify whether lesions were bilateral or not, but based on positive histology these lesions were still included in the study. One must also keep in mind that clinical diagnosis of OLP demands an experienced clinician to discover lesions which can vary in type, shape and size and sometimes even be difficult to discover. Concerning malignant transformation of OLP some authors have reported a relatively high frequency (>5%) (Lo Muzio L et al., 1998; Yaacob HB et al., 2002) whereas others have reported 0% transformation of OLP but
36
•
approximately 2% of OLL (including OLCR) (van der Meij EH et al., 2003; van der Meij EH et al., 2006). By studying a family of proteins crucial for formation of the oral mucosa, p63, and some of its relatives in both normal oral mucosa and OLP lesions, and compare results with similar analysis of SCCHN tissue, we hoped to add some data to the debate on “potential malignant transformation”. When mapping p63 status we saw decreased protein expression as well as decreased mRNA levels in OLP lesions whereas expression of the tumour suppressor protein p53 was increased. We were also able to detect some of the novel p53 isoforms although at lower levels compared to what has been seen in SCCHN. For the other p63 related proteins β-catenin, E-cadherin and EGFR, expression of all three was decreased in the majority of OLP lesions compared to matched normal controls. So what does this all mean? p53 over-expression in OLP lesions could indicate that these lesions contain more DNA damaged cells due to the chronic inflammation. At the same time, decreased expression of p63 could mean disrupted maintenance and stratification of the epithelium. One can speculate that this could lead to disturbance in healing of the lesion, making OLP into “a chronic lesion with difficulty to heal”. The imbalance in expression of these proteins in OLP resembles their expression status in tissue after UV exposure which can induce DNA damage. UV irradiation stabilises p53 (Hall PA et al., 1993) and causes a decrease in p63 in epithelium in vivo (Liefer KM et al., 2000). Decreased expression of p63 and at the same time overexpression of p53 is required to induce apoptosis to remove DNA damaged cells which have a potential for malignant transformation. The expression pattern in OLP is, however, different from what is seen in tumour tissue where increased expression of ΔNp63 has been seen (Thurfjell N et al., 2004) and p53 is inactivated in 50% of all cases. So from a p53 and p63 point of view OLP differs from normal healthy as well as tumour tissue. Thus, based on our studies, it is not possible to either support nor contradict the statement that OLP is a clear cut premalignant condition, with increased risk of developing into malignancy compared to normal healthy controls. A characteristic feature of OLP lesions is the heavy inflammatory infiltrate seen in the subepithelial connective tissue. One plausible explanation to this inflammation is a change in the keratinocytes making them antigenic and thus evoking an inflammatory response (Sugerman PB et al., 1993). This explanation is very interesting when looking at our findings of autoantibodies against p63 as well as p73 in a few patients diagnosed with OLP, with the strongest reaction seen against the p63β isoforms. The p63β isoforms are thought to be involved in cell differentiation (Di Iorio E et al., 2005), and autoantibodies directed most
37

strongly against these specific isoforms could thus result in disturbed differentiation of the keratinocytes. This could in turn start off an antigenic reaction against these epithelial cells and cause an inflammatory reaction supporting the hypothesis that OLP is in fact an autoimmune disease. In conclusion, the present project adds much novel data to the mapping of the OLP disease. In our effort to understand the etiology of OLP we were the first to demonstrate autoantibodies directed against p63 and p73 in, what could be a possible aetiology of, a subgroup of OLP patients. OLP could thus be suggested to be not one distinct disease, but based on our data a disease comprising different subgroups.
38
•

9. Conclusions • Decreased expression of p63 and increased expression of p53 was seen in
OLP and GvHD lesions compared to normal oral mucosa and SCCHN. Results indicate a coordinated action of these two related proteins in order to protect the oral mucosa from the damaging effects of the underlying inflammation.
• Three out of six p53 isoforms analysed were detected at RNA level in the
majority of OLP lesions and normal controls analysed. Two of these isoforms belong to the group of recently detected novel p53 isoforms. Levels of the novel isoforms were in general lower compared to levels in SCCHN, indicating a more tumour related role for these isoforms. All p63 isoforms showed decreased RNA levels in OLP lesions in accordance with the previously shown decreased expression of the p63 proteins.
• In accordance with previous analysis of SCCHN tumours, results showed
an expression pattern similar to SCCHN tumours with decreased expression of β-catenin and E-cadherin whereas expression of EGFR was more similar to conditions in normal oral mucosa.
• Autoantibodies directed against all p63 and four p73 isoforms were
detected in sera from two patients diagnosed with OLP.
39

10. Acknowledgements The fulfilment of this thesis and project had not been possible without plentiful support of many people and in particular I am indebted to: Karin Nylander my main supervisor who introduced me to the field of pathology. Thank you for giving me this golden opportunity to work with you. You have always supported me and our project 100% and provided me with the best possible working conditions. Words can not possibly describe my gratitude for what you have done for me. I will miss our “Sunday school”. Ylva Britt Wahlin my co-supervisor who with great patience taught me the clinical aspect and provided me with patients. You always with your own special way challenged me to learn more. I consider myself lucky to have such a prominent colleague and friend. Philip J Coates my other co-supervisor, thank you for all the valuable discussion and fruitful collaboration. You have always been easy to reach even though you were in Dundee. Linda Boldrup my co-author who did a wonderful job helping me with lab work and sharing her experience with me. Good luck with your dissertation. Many thanks to the rest of my co-authors Göran Roos, Björn Sjöström, Jean-Christophe Bourdon and Allan Wiik. It has been a pleasure knowing and working with you. My special thanks to the lab staff who guided me through this project, especially Bodil Bäcklund. I appreciate all you have done. You were and will always be irreplaceable. Britta Lindgren who did a wonderful job with immunhistological staining and Inger Cullman for helping me with RNA. Xiaolian Gu my room mate and friend who patiently helped me with the computer problems. My best wishes for your newborn child. Niklas Thurfjell for teaching me the basis of light cycler. Thanks to administrative staff of Department of Medical Biosciences Åsa Lundstén, Karin Bodén and Terry Persson. Elisabet Nylander for giving me the opportunity to participate in clinical examination of your patients.
40
•
Many thanks to Ingegerd Johansson, Ulf Sjögren, Bodil Wallin, Ulrika Funegård and Gunilla Berglund for their goodwill and support of this project. Special thanks to my colleagues Malin Brundin and Hans Ingridsson for covering for me at the student clinic when I could not be there. Christin Rampling and Agneta Kågström for helping me to administrate patients even though you were very busy. My group mates Matilda Rentoft and Monica Brage. My special thanks to all patients and volunteers who made an enormous contribution. Without you this project could not have been preformed. And last but absolutely not least many, many thanks to my friend, companion and beloved wife Karin Danielsson, my beautiful children Sarah and Sam for everything. You have always been patient with me and stood by my side even though it was not always easy. I promise to make it up to you. This project was supported by grants from The County Council of Västerbotten, the Swedish Dental Society, Department of Odontology Umeå University, The Swedish Cancer Society Grant number 4569-B05-05XAC and Lion´s Cancer Research Foundation, Umeå University.
41

11. References Al-Hashimi I, Schifter M, Lockhart PB et al., (2007). "Oral lichen planus and
oral lichenoid lesions: diagnostic and therapeutic considerations." Oral Surg Oral Med Oral Pathol Oral Radiol Endod 103 Suppl: S25 e1-12.
Andreasen JO (1968). "Oral lichen planus. 1. A clinical evaluation of 115 cases." Oral Surg Oral Med Oral Pathol 25(1): 31-42.
Axell T and Rundquist L (1987). "Oral lichen planus--a demographic study." Community Dent Oral Epidemiol 15(1): 52-6.
Axell T, Zain RB, Siwamogstham P et al., (1990). "Prevalence of oral soft tissue lesions in out-patients at two Malaysian and Thai dental schools." Community Dent Oral Epidemiol 18(2): 95-9.
Balkwill F and Mantovani A (2001). "Inflammation and cancer: back to Virchow?" Lancet 357(9255): 539-45.
Barker N and Clevers H (2000). "Catenins, Wnt signaling and cancer." Bioessays 22(11): 961-5.
Baselga J (2002). "Why the epidermal growth factor receptor? The rationale for cancer therapy." Oncologist 7 Suppl 4: 2-8.
Boldrup L, Coates PJ, Hedberg Y et al., (2005). "Expression of p63, COX-2, EGFR and beta-catenin in smokers and patients with squamous cell carcinoma of the head and neck reveal variations in non-neoplastic tissue and no obvious changes in smokers." Int J Oncol 27(6): 1661-7.
Bouquot JE and Gorlin RJ (1986). "Leukoplakia, lichen planus, and other oral keratoses in 23,616 white Americans over the age of 35 years." Oral Surg Oral Med Oral Pathol 61(4): 373-81.
Bourdon JC (2007). "p53 and its isoforms in cancer." Br J Cancer 97(3): 277-82.
Bourdon JC, Fernandes K, Murray-Zmijewski F et al., (2005). "p53 isoforms can regulate p53 transcriptional activity." Genes Dev 19(18): 2122-37.
Bricker SL (1994). "Oral lichen planus: a review." Semin Dermatol 13(2): 87-90.
Clevers H (2004). "At the crossroads of inflammation and cancer." Cell 118(6): 671-4.
Cohen S (1962). "Isolation of a mouse submaxillary gland protein accelerating incisor eruption and eyelid opening in the new-born animal." J Biol Chem 237: 1555-62.
Coussens LM and Werb Z (2002). "Inflammation and cancer." Nature 420(6917): 860-7.
de Moura Castro Jacques C, Cardozo Pereira AL, Cabral MG et al., (2003). "Oral lichen planus part I: epidemiology, clinics, etiology, immunopathogeny, and diagnosis." Skinmed 2(6): 342-7; quiz 348-9.
Demarosi F, Soligo D, Lodi G et al., (2005). "Squamous cell carcinoma of the oral cavity associated with graft versus host disease: report of a case and
42
•

review of the literature." Oral Surg Oral Med Oral Pathol Oral Radiol Endod 100(1): 63-9.
Di Iorio E, Barbaro V, Ruzza A et al., (2005). "Isoforms of DeltaNp63 and the migration of ocular limbal cells in human corneal regeneration." Proc Natl Acad Sci U S A 102(27): 9523-8.
Dissemond J (2004). "Oral lichen planus: an overview." J Dermatolog Treat 15(3): 136-40.
Eisen D (1999). "The evaluation of cutaneous, genital, scalp, nail, esophageal, and ocular involvement in patients with oral lichen planus." Oral Surg Oral Med Oral Pathol Oral Radiol Endod 88(4): 431-6.
Epstein JB, Wan LS, Gorsky M et al., (2003). "Oral lichen planus: progress in understanding its malignant potential and the implications for clinical management." Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96(1): 32-7.
Fujii H, Ohashi M and Nagura H (1988). "Immunohistochemical analysis of oral lichen-planus-like eruption in graft-versus-host disease after allogeneic bone marrow transplantation." Am J Clin Pathol 89(2): 177-86.
Galaz S, Espada J, Stockert JC et al., (2005). "Loss of E-cadherin mediated cell-cell adhesion as an early trigger of apoptosis induced by photodynamic treatment." J Cell Physiol 205(1): 86-96.
Ghioni P, Bolognese F, Duijf PH et al., (2002). "Complex transcriptional effects of p63 isoforms: identification of novel activation and repression domains." Mol Cell Biol 22(24): 8659-68.
Grandis JR and Tweardy DJ (1993). "Elevated levels of transforming growth factor alpha and epidermal growth factor receptor messenger RNA are early markers of carcinogenesis in head and neck cancer." Cancer Res 53(15): 3579-84.
Hajra KM and Fearon ER (2002). "Cadherin and catenin alterations in human cancer." Genes Chromosomes Cancer 34(3): 255-68.
Hall PA, Campbell SJ, O'Neill M et al., (2000). "Expression of the p53 homologue p63alpha and deltaNp63alpha in normal and neoplastic cells." Carcinogenesis 21(2): 153-60.
Hall PA, McKee PH, Menage HD et al., (1993). "High levels of p53 protein in UV-irradiated normal human skin." Oncogene 8(1): 203-7.
Hampf BG, Malmstrom MJ, Aalberg VA et al., (1987). "Psychiatric disturbance in patients with oral lichen planus." Oral Surg Oral Med Oral Pathol 63(4): 429-32.
Hasseus B, Jontell M, Brune M et al., (2001). "Langerhans cells and T cells in oral graft versus host disease and oral lichen planus." Scand J Immunol 54(5): 516-24.
He TC, Sparks AB, Rago C et al., (1998). "Identification of c-MYC as a target of the APC pathway." Science 281(5382): 1509-12.
43

Herrenknecht K, Ozawa M, Eckerskorn C et al., (1991). "The uvomorulin-anchorage protein alpha catenin is a vinculin homologue." Proc Natl Acad Sci U S A 88(20): 9156-60.
Huber MA (2004). "Oral lichen planus." Quintessence Int 35(9): 731-52. Huber O, Bierkamp C and Kemler R (1996). "Cadherins and catenins in
development." Curr Opin Cell Biol 8(5): 685-91. Ikawa S, Nakagawara A and Ikawa Y (1999). "p53 family genes: structural
comparison, expression and mutation." Cell Death Differ 6(12): 1154-61. Imai T, Horiuchi A, Shiozawa T et al., (2004). "Elevated expression of E-
cadherin and alpha-, beta-, and gamma-catenins in metastatic lesions compared with primary epithelial ovarian carcinomas." Hum Pathol 35(12): 1469-76.
Ismail SB, Kumar SK and Zain RB (2007). "Oral lichen planus and lichenoid reactions: etiopathogenesis, diagnosis, management and malignant transformation." J Oral Sci 49(2): 89-106.
Ivanovski K, Nakova M, Warburton G et al., (2005). "Psychological profile in oral lichen planus." J Clin Periodontol 32(10): 1034-40.
Jungell P (1991). "Oral lichen planus. A review." Int J Oral Maxillofac Surg 20(3): 129-35.
Kaghad M, Bonnet H, Yang A et al., (1997). "Monoallelically expressed gene related to p53 at 1p36, a region frequently deleted in neuroblastoma and other human cancers." Cell 90(4): 809-19.
Katta R (2000). "Lichen planus." Am Fam Physician 61(11): 3319-24, 3327-8. Ke LD, Adler-Storthz K, Clayman GL et al., (1998). "Differential expression of
epidermal growth factor receptor in human head and neck cancers." Head Neck 20(4): 320-7.
Knudsen KA and Wheelock MJ (1992). "Plakoglobin, or an 83-kD homologue distinct from beta-catenin, interacts with E-cadherin and N-cadherin." J Cell Biol 118(3): 671-9.
Koster MI and Roop DR (2004). "The role of p63 in development and differentiation of the epidermis." J Dermatol Sci 34(1): 3-9.
Lane DP and Crawford LV (1979). "T antigen is bound to a host protein in SV40-transformed cells." Nature 278(5701): 261-3.
Liefer KM, Koster MI, Wang XJ et al., (2000). "Down-regulation of p63 is required for epidermal UV-B-induced apoptosis." Cancer Res 60(15): 4016-20.
Linzer DI and Levine AJ (1979). "Characterization of a 54K dalton cellular SV40 tumor antigen present in SV40-transformed cells and uninfected embryonal carcinoma cells." Cell 17(1): 43-52.
Lo Muzio L, Mignogna MD, Favia G et al., (1998). "The possible association between oral lichen planus and oral squamous cell carcinoma: a clinical evaluation on 14 cases and a review of the literature." Oral Oncol 34(4): 239-46.
44
•

Lodi G, Giuliani M, Majorana A et al., (2004). "Lichen planus and hepatitis C virus: a multicentre study of patients with oral lesions and a systematic review." Br J Dermatol 151(6): 1172-81.
Lodi G, Scully C, Carrozzo M et al., (2005). "Current controversies in oral lichen planus: report of an international consensus meeting. Part 2. Clinical management and malignant transformation." Oral Surg Oral Med Oral Pathol Oral Radiol Endod 100(2): 164-78.
Lukac J, Brozovic S, Vucicevic-Boras V et al., (2006). "Serum autoantibodies to desmogleins 1 and 3 in patients with oral lichen planus." Croat Med J 47(1): 53-8.
Lundqvist EN, Wahlin YB, Bergdahl M et al., (2006). "Psychological health in patients with genital and oral erosive lichen planus." J Eur Acad Dermatol Venereol 20(6): 661-6.
Maeda H and Akaike T (1998). "Nitric oxide and oxygen radicals in infection, inflammation, and cancer." Biochemistry (Mosc) 63(7): 854-65.
Matheny KE, Barbieri CE, Sniezek JC et al., (2003). "Inhibition of epidermal growth factor receptor signaling decreases p63 expression in head and neck squamous carcinoma cells." Laryngoscope 113(6): 936-9.
Mattsson T, Sundqvist KG, Heimdahl A et al., (1992). "A comparative immunological analysis of the oral mucosa in chronic graft-versus-host disease and oral lichen planus." Arch Oral Biol 37(7): 539-47.
McCrea PD, Turck CW and Gumbiner B (1991). "A homolog of the armadillo protein in Drosophila (plakoglobin) associated with E-cadherin." Science 254(5036): 1359-61.
Mills AA, Zheng B, Wang XJ et al., (1999). "p63 is a p53 homologue required for limb and epidermal morphogenesis." Nature 398(6729): 708-13.
Mokni M, Rybojad M, Puppin D, Jr. et al., (1991). "Lichen planus and hepatitis C virus." J Am Acad Dermatol 24(5 Pt 1): 792.
Moll UM and Slade N (2004). "p63 and p73: roles in development and tumor formation." Mol Cancer Res 2(7): 371-86.
Mollaoglu N (2000). "Oral lichen planus: a review." Br J Oral Maxillofac Surg 38(4): 370-7.
Murray-Zmijewski F, Lane DP and Bourdon JC (2006). "p53/p63/p73 isoforms: an orchestra of isoforms to harmonise cell differentiation and response to stress." Cell Death Differ 13(6): 962-72.
Nakamura T, Hamada F, Ishidate T et al., (1998). "Axin, an inhibitor of the Wnt signalling pathway, interacts with beta-catenin, GSK-3beta and APC and reduces the beta-catenin level." Genes Cells 3(6): 395-403.
Neville B.W, Damm D.D, Allen C.M et al., (2002). Oral and Maxillofacial Pathology, W.B. Saunders company.
Nishi H, Isaka K, Sagawa Y et al., (1999). "Mutation and transcription analyses of the p63 gene in cervical carcinoma." Int J Oncol 15(6): 1149-53.
45

Nishi H, Senoo M, Nishi KH et al., (2001). "p53 Homologue p63 represses epidermal growth factor receptor expression." J Biol Chem 276(45): 41717-24.
Nylander K, Vojtesek B, Nenutil R et al., (2002). "Differential expression of p63 isoforms in normal tissues and neoplastic cells." J Pathol 198(4): 417-27.
Osada M, Ohba M, Kawahara C et al., (1998). "Cloning and functional analysis of human p51, which structurally and functionally resembles p53." Nat Med 4(7): 839-43.
Ozawa M, Baribault H and Kemler R (1989). "The cytoplasmic domain of the cell adhesion molecule uvomorulin associates with three independent proteins structurally related in different species." Embo J 8(6): 1711-7.
Patturajan M, Nomoto S, Sommer M et al., (2002). "DeltaNp63 induces beta-catenin nuclear accumulation and signaling." Cancer Cell 1(4): 369-79.
Peluso JJ, Pappalardo A and Fernandez G (2001). "E-cadherin-mediated cell contact prevents apoptosis of spontaneously immortalized granulosa cells by regulating Akt kinase activity." Biol Reprod 64(4): 1183-90.
Philip M, Rowley DA and Schreiber H (2004). "Inflammation as a tumor promoter in cancer induction." Semin Cancer Biol 14(6): 433-9.
Pignatelli M and Vessey CJ (1994). "Adhesion molecules: novel molecular tools in tumor pathology." Hum Pathol 25(9): 849-56.
Pindborg JJ, Reichart PA, Smith CJ et al., (1997). Histological typing of cancer and precancer of the oral mucosa. In: World Health Organization international histological classification of tumours. Berlin, Springer.
Pindborg JJ (1992). Atlas of diesases of the Oral mucosa. Copenhagen, Denmark, Munksgaard.
Potter E, Bergwitz C and Brabant G (1999). "The cadherin-catenin system: implications for growth and differentiation of endocrine tissues." Endocr Rev 20(2): 207-39.
Preda EG, Pasetti P, Caggiula S et al., (1990). "[Oral pathology of pscyhosomatic origin. Review of the literature]." Dent Cadmos 58(1): 66-72.
Ramburan A, Govender D and (2002). "Cadherins and catenins in pathology." Curr Diag Pathol 8(5): 305-317.
Reichart PA and Philipsen HP (2000). Color Atlas of Dental Medicine Oral Pathology. Stuttgart, Germany and New York, USA, Thieme.
Romer L, Klein C, Dehner A et al., (2006). "p53--a natural cancer killer: structural insights and therapeutic concepts." Angew Chem Int Ed Engl 45(39): 6440-60.
Rubin Grandis J, Melhem MF, Barnes EL et al., (1996). "Quantitative immunohistochemical analysis of transforming growth factor-alpha and epidermal growth factor receptor in patients with squamous cell carcinoma of the head and neck." Cancer 78(6): 1284-92.
46
•

Rubin Grandis J, Tweardy DJ and Melhem MF (1998). "Asynchronous modulation of transforming growth factor alpha and epidermal growth factor receptor protein expression in progression of premalignant lesions to head and neck squamous cell carcinoma." Clin Cancer Res 4(1): 13-20.
Savage NW, Walsh LJ, Zhao ZZ et al., (2002). "The pathogenesis of oral lichen planus." Crit Rev Oral Biol Med 13(4): 350-65.
Silverman S, Jr. (1991). "Lichen planus." Curr Opin Dent 1(6): 769-72. Sugerman PB and Savage NW (2002). "Oral lichen planus: causes, diagnosis
and management." Aust Dent J 47(4): 290-7. Sugerman PB, Savage NW, Walsh LJ et al., (1993). "Disease mechanisms in
oral lichen planus. A possible role for autoimmunity." Australas J Dermatol 34(2): 63-9.
Takeichi M (1995). "Morphogenetic roles of classic cadherins." Curr Opin Cell Biol 7(5): 619-27.
Thorn JJ, Holmstrup P, Rindum J et al., (1988). "Course of various clinical forms of oral lichen planus. A prospective follow-up study of 611 patients." J Oral Pathol 17(5): 213-8.
Thurfjell N, Coates PJ, Uusitalo T et al., (2004). "Complex p63 mRNA isoform expression patterns in squamous cell carcinoma of the head and neck." Int J Oncol 25(1): 27-35.
van Bokhoven H and McKeon F (2002). "Mutations in the p53 homolog p63: allele-specific developmental syndromes in humans." Trends Mol Med 8(3): 133-9.
van der Meij EH, Mast H and van der Waal I (2006). "The possible premalignant character of oral lichen planus and oral lichenoid lesions: A prospective five-year follow-up study of 192 patients." Oral Oncol.
van der Meij EH, Schepman KP, Smeele LE et al., (1999). "A review of the recent literature regarding malignant transformation of oral lichen planus." Oral Surg Oral Med Oral Pathol Oral Radiol Endod 88(3): 307-10.
van der Meij EH, Schepman KP and van der Waal I (2003). "The possible premalignant character of oral lichen planus and oral lichenoid lesions: a prospective study." Oral Surg Oral Med Oral Pathol Oral Radiol Endod 96(2): 164-71.
van der Meij EH and van der Waal I (2003). "Lack of clinicopathologic correlation in the diagnosis of oral lichen planus based on the presently available diagnostic criteria and suggestions for modifications." J Oral Pathol Med 32(9): 507-12.
Wheelock MJ, Knudsen KA and KR: J (1996). "Membrane–cytoskeleton interaction with cadherin cell adhesion proteins: role of catenins as linker protein." Curr Top Membr 43: 169-185.
Wilson E (1869). "On lichen planus." J Cutan Med Dis Skin 3: 117-132.
47

Woo SB, Lee SJ and Schubert MM (1997). "Graft-vs.-host disease." Crit Rev Oral Biol Med 8(2): 201-16.
Yaacob HB, Tan PL and Ngeow WC (2002). "Malignancy in oral lichen planus: a review of a group from the Malaysian population." J Oral Sci 44(2): 65-71.
Yang A, Kaghad M, Wang Y et al., (1998). "p63, a p53 homolog at 3q27-29, encodes multiple products with transactivating, death-inducing, and dominant-negative activities." Mol Cell 2(3): 305-16.
Yang A and McKeon F (2000). "P63 and P73: P53 mimics, menaces and more." Nat Rev Mol Cell Biol 1(3): 199-207.
Yang A, Schweitzer R, Sun D et al., (1999). "p63 is essential for regenerative proliferation in limb, craniofacial and epithelial development." Nature 398(6729): 714-8.
48
•