UICC Advocacy Toolkit 4. Cancer Development
20
A GUIDE FOR ADVOCACY TO MAINSTREAM CANCER IN THE POST-2015 DEVELOPMENT AGENDA
description
A guide for advocacy to mainstream cancer in the post-2015 development agenda
Transcript of UICC Advocacy Toolkit 4. Cancer Development

A GUIDE FOR ADVOCACY TO MAINSTREAM CANCER IN THE POST-2015 DEVELOPMENT AGENDA

In September 2000, the Heads of State participating in the United Nations (UN) Millennium Summit approved a bold and wide-ranging agenda to reduce extreme poverty and meet the needs of the world’s most vulnerable. That agenda was embedded in the framework of the Millennium Development Goals (MDGs) that has guided global and national development priorities as well as the flow of bilateral and multilateral funding since that time. The eight MDGs including three health goals targeting a reduction in child mortality, combating HIV/AIDS, and improving maternal health are due to expire in 2015, with a process now underway, led by the UN to define the future global development framework that will succeed the MDGs.
Mainstreaming cancer in the post-2015 development agenda is one of UICC’s priority advocacy objectives. We have produced this guide to assist UICC member organisations to understand the case for cancer in the post-2015 development framework and provide key advocacy tools to support members and partners to actively participate in promoting the integration of post-2015 development goals that will reduce the global cancer burden. These tools include a high-level view of the decision-making processes towards the adoption of new goals in September 2015; and key actions that cancer organisations can take to make cancer and non-communicable diseases (NCDs) a top priority for governments.
A GUIDE FOR ADVOCACY TO MAINSTREAM CANCER IN THE POST-2015 DEVELOPMENT AGENDA
In 2012, there were 8.2 million cancer
deaths, of which approximately 65%
occurred in low- and middle-income
countries (LMICs). This figure is projected to
rise to 11.4 million in 2025 with 77% of the
projected increase occurring in LMICs.1
UICC Advocacy Toolkit 2014 - Cancer & Development2
FACT
Image Credit: Front cover: © Francois STRUZIK - Image of dignity Above: Creative Commons - Attribution 2.0 Generic (CC BY 2.0) by Free Grunge Textures - www.freestock.ca

For the first time, all UN Member States have agreed that NCDs constitute a major challenge to socioeconomic development, environmental sustainability and poverty alleviation. The 2011 UN Political Declaration on NCDs committed governments to strengthen and integrate NCD policies and programmes into health planning processes and national development agendas.2 Further to this Declaration, in June 2012, the Rio+20 declaration on Sustainable Development acknowledged that the global burden of NCDs constitutes one of today’s major challenges for development3; and in 2013, the World Health Organization (WHO) adopted the Global Action Plan for the Prevention and Control of NCDs 2013-2020, which declared that the prevention of NCDs including cancer is a precondition for, an outcome of and an indicator of all three dimensions of sustainable development: economic development, environmental sustainability and social inclusion.4
With the number of new cases of cancer projected to reach 19.3 million per year in 20255 and the adoption in 2013 of a mortality target of a 25% reduction in premature mortality from NCDs by 2025, it is now critical that the development agenda embrace NCDs. In close partnership with the NCD Alliance and other key stakeholders, UICC has been advocating for a health goal to be adopted in the next generation of development goals that seeks to mitigate the burden of cancer and NCDs globally through implementation of NCD policies as well as strengthening links outside of health to address the underlying social, economic, political, environmental and cultural factors, broadly known as ‘social determinants’.6
Since the UN High-level Meeting on NCDs in September 2011, some significant steps have been taken towards accelerating the prevention and control of NCDs through joining forces with development partners. In 2012, UNDP and WHO set out key activities for collective action against NCDs building on the lessons learned and precedents for best practice through addressing HIV/AIDS. Subsequently, the first meeting of the UN Interagency Taskforce on the prevention and control of NCDs (the Task Force) was convened in October 2013. The Taskforce led by WHO will coordinate activities of UN funds, programmes and agencies and other international organisations to support the realisation of commitments made in the UN Political Declaration on NCDs.
MEMBER STATES AGREE THAT CANCER IS A DEVELOPMENT ISSUE
UICC Advocacy Toolkit 2014 - Cancer & Development 3

CANCER IS AN ISSUE OF SOCIAL EQUITY
The right to health was enshrined in the Constitution of the World Health Organization (WHO) in 1946, and two years later, included in the Universal Declaration of Human Rights. Every country has now signed up to at least one treaty that acknowledges the right to health and many countries’ constitutions reflect this entitlement. Despite this, under-resourced health systems and lack of social protection in many low- and middle-income countries (LMICs) are widening gaps in access to cancer services and heightening financial risk, keeping the bottom billion locked in chronic poverty. For women, gender biases in power, resources, culture and a lack of investment in cancer interventions at the primary healthcare level negatively impact access to early diagnosis and treatment, resulting in high mortality levels for cervical and breast cancers.7
Specific actions to address inequities in access to education, challenge gender discrimination and develop social protection mechanisms must be part of the post-2015 development agenda. A global coordinated approach to tackling these inequities, as part of the next generation of development goals and targets is a matter of social justice and a pre-requisite for sustained social development and economic productivity. This approach is also critical in delivering a human rights-based approach to cancer and NCDs where proven effective cancer treatment and services are available to all people on equal terms and without suffering economic hardship as a consequence.
UNDERSTANDING THE CASE FOR CANCER IN THE POST-2015 DEVELOPMENT AGENDA
4 UICC Advocacy Toolkit 2014 - Cancer & Development

CASE STUDYA RIGHTS-BASED APPROACH TO CHILDHOOD CANCERS
Applying a rights-based approach to advocacy for childhood cancer is helpful to promoting social justice and can assist in analysing and addressing the inequalities and discriminatory practices (either due to policy or practice or at community level) that affect children’s access to appropriate and timely services for early detection, treatment and care. A rights-based approach to childhood cancer gives importance not only to survival outcomes, but also to the processes of designing policy and programmes where principles such as participation, equality and non-discrimination, and accountability are integrated into all stages of the health programming process (including conducting assessments and analysis, priority setting, programme planning and design, implementation, and monitoring and evaluation).
THE CONVENTION ON THE RIGHTS OF THE CHILD
The Convention on the Rights of the Child (CRC) is the most widely ratified international convention and is an important advocacy tool with which to work with state actors in realising the rights of children to appropriate and timely cancer treatment and care. Article 24 of the Convention stipulates that “States Parties recognise the right of the child to the enjoyment of the highest attainable standard of health and to facilities for the treatment of illness and rehabilitation of health. States Parties shall strive to ensure that no child is deprived of his or her right of access to such health care services.”
In 2013, the Committee on the Rights of the Child (the body of independent experts that monitors the implementation of the Convention) developed General Comment 15 on the right of the child to the enjoyment of the highest attainable standard of health (Article 24) and this was adopted during the Committee’s 62nd Session. The General Comment provides guidance on
the normative content of the rights of the child and adolescent to enjoyment of the highest attainable standard of health, and to facilities for the treatment of illness and rehabilitation in relation to healthcare services. In addition, it articulates the legally binding obligations of States Parties to the CRC with respect to ensuring the full realisation of the child’s right to health and provides a framework and recommendations for concrete measures and actions required by States Parties, and non-State actors. General Comment No.15 can be accessed at the following link: http://www2.ohchr.org/english/bodies/crc/comments.htm
5UICC Advocacy Toolkit 2014 - Cancer & Development
CIAN Agency © François Struzik - simply human

THE TOLL OF CANCER ON ECONOMIC DEVELOPMENT
Non-communicable Diseases (NCDs) impose enormous costs on families, households, communities and economies. It is estimated that the cost of cancer alone will reach $458 billion per year in 20308, yet the staggering financial risk that cancer poses to development is still not recognised. For individuals and families affected by cancer, there is often a large burden of out-of-pocket expenses resulting from cancer medicines and treatment as well as lost income due to absence from work for
the patient or caregivers. Studies in India also show that cancer-affected households have significantly higher rates of borrowing and asset sales for financing outpatient care.9 This is supported by findings in African countries where it is common for households to borrow and sell assets to finance healthcare and cope with out-of-pocket health payments.10 Cancer-related death and disability also have a significant impact on lowering labour supply. Overall, there is a strong relationship between economic growth and health such that the increasing burden of cancer particularly in developing economies poses a tangible threat to national productivity and development.
UNDERSTANDING THE CASE FOR CANCER IN THE POST-2015 DEVELOPMENT AGENDA (CONTINUED)
6 UICC Advocacy Toolkit 2014 - Cancer & Development
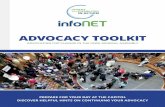
The global economic cancer burden
Cancer is costly...The economic cost* of cancer exceeds that of any other disease...
* Economic losses from disability and premature deaths. Excludes direct medical costs.Sources: American Cancer Society, Livestrong, World Health Organization.
See bit.ly/cancerburden for full data list.Information is Beautiful
$895bn cancer
$1.8bn cost of reducing exposure to key risk factors like smoking, drinking and poor diet
$753bn heart disease
$298bn stroke
$204bn diabetes
$141bn suicide
$203bn chronic obstructive pulmonary disease
$45bn tubercolosis
$25bn malaria
$193bn HIV/AIDS
$204bn traffic accidents
But cost effective solutions exist
$0.6bn smoking
$0.4bn diet and exercise
$0.8bn alcohol
and could prevent
cancer cases
1 in 3
CANCER IS COSTLY...THE ECONOMIC COST* OF CANCER EXCEEDS THAT OF ANY OTHER DISEASE...
THE GLOBAL ECONOMIC CANCER BURDEN
* Economic losses from disability and premature deaths. Excludes direct medical costs.Sources: American Cancer Society, Livestrong, World Health Organization.See bit.ly/cancerburden for full data list.

One-fourth of the Indian population does not seek out healthcare services because of the prohibitive cost of access. In India there is a heavy reliance on out-of-pocket spending in financing healthcare: government financing accounts for only about one-fourth of India’s aggregate health spending of 4.5% of GDP, and most of the residual spending is in the form of out-of-pocket spending by households.9
Cancer is on the rise in India at the same time that the burden of infectious diseases such as malaria and cholera remains unabated.11 Households across the spectrum of socioeconomic status (SES) face a large economic risk from cancer, and the risk seems particularly serious for low-SES households who rely on borrowing and asset sales to a much greater extent to finance their healthcare. The human toll can be enormous – individuals are forced to give up their life savings to care for family members, impoverishing families and causing significant financial and emotional distress to both patients and their caregivers. For countries like India, cancer represents a significant threat to economic growth as a result of lost productivity and additional stress on already overburdened heath systems.
While India faces multiple challenges to the provision of affordable and accessible healthcare for its population, the government has set out a long-term vision to achieve universal health coverage for India by 2022. At the core of this vision is the need for affordable healthcare brought about by a transformative shift in India’s healthcare sector over the next decade.
CIAN Agency © François Struzik - simply human
CASE STUDYTHE COST OF CANCER IN INDIA
7UICC Advocacy Toolkit 2014 - Cancer & Development
© Carolyn Taylor

CANCER RISK FACTORS AND CHANGING ENVIRONMENTS
Globalisation, rapid ur¬banisation, climate change and shifting agricultural and resource-use patterns that impact nutritional security are increasing exposure to common cancer risk factors namely tobacco use, harmful use of alcohol, unhealthy diet, and a lack of physical activity, as well as environmental exposures such as air pollution.
The most common risk factor, tobacco use, is responsible for five million, or 12% of all deaths of adults above the age of 30 globally each year.12 It is linked to 71% of all lung cancer deaths, and accounts for at least 22% of all cancer deaths.12 Alcohol is also a known risk factor with any level of consumption increasing the risk of cancer.13 Alcohol is strongly linked with an increased risk of cancers of the mouth, pharynx, larynx, oesophagus, bowel, liver and breast. Globally, both tobacco and alcohol use start at a young age: Nearly one in five of the world’s adolescents aged 13-15 years use tobacco; and 14% of adolescent girls and 18% of boys aged between 13-15 years in LMICs are reported to use alcohol.13,14
Much of the world is experiencing upward trends in overweight and obesity. Of particular concern are the increasing rates of obesity in children and adolescents.15 These rising rates of obesity will lead to increased cancer rates unless actions are taken to improve people’s diets and physical activity levels, with overweight and obesity strongly linked to increased risks of bowel, breast, uterine, pancreatic, oesophagus, kidney and gallbladder cancers. Across virtually all low- and middle-income regions the prevalence of overweight and obesity is approaching
levels found in higher-income countries. This is particularly true in the Middle East, North Africa, in Latin America and the Caribbean, with 65% of the world’s population now living in countries where overweight and obesity kills more people than underweight.16 The rise in obesity is largely due to a changing environment – changes in the built environment and a transition to occupations that require less physical activity, as well as a marked increase in the availability, affordability, promotion and consumption of high energy-dense, highly processed foods and drinks and a shift away from minimally processed foods such as grains, legumes, pulses, fruits and vegetables.
Sub-Saharan Africa is urbanising faster than any other region, with air pollution becoming an increasing problem.17 Air pollution is a major environmental risk factor for cancer.18 The most recent data indicates that in 2010, 223,000 deaths from lung cancer worldwide resulted from air pollution, with the predominant sources being transportation, stationary power generation, industrial and agricultural emissions, and residential heating and cooking.
UNDERSTANDING THE CASE FOR CANCER IN THE POST-2015 DEVELOPMENT AGENDA (CONTINUED)
8 UICC Advocacy Toolkit 2014 - Cancer & Development

CASE STUDYADVOCATING FOR EFFECTIVE POLICIES TO CHANGE THE FOOD ENVIRONMENT FOR GLOBAL OBESITY PREVENTION
The WHO recognises overweight and obesity as a serious challenge for low- and middle-income countries, with implications for cancer and other NCDs. Global targets on childhood and adult obesity have been adopted and the WHO has also developed a series of policy recommendations to address unhealthy diet and obesity in its Global Action Plan on NCDs (2013-2020) and the Set of Recommendations on Marketing of Food and Non-Alcoholic Beverages to children.19 While some action has been taken at the national level, many low- and middle-income countries require technical support and access to additional resources in order to initiate large-scale efforts to address obesity and overweight. Integration of NCDs within the post-2015 development agenda will make it easier for countries, UN agencies and donors to work on accelerating national implementation of policy measures.
World Cancer Research Fund International has recently released the NOURISHING Framework, which formalises a food policy package that is globally applicable and compatible with WHO global recommendations. Many of the evidence-informed actions in NOURISHING aim to create positive change in the food environment, which will enable people to adopt a healthier diet and maintain a healthy bodyweight in line with recommendations
for cancer prevention.20 In particular, the restriction of advertising and marketing of unhealthy foods and drinks to children and other forms of commercial promotion is recommended and supported by convincing evidence that television advertising influences food preferences and purchase requests. Marketing activities in low- and middle-income countries are aggressive, comprehensive and highly integrated. They aim to create demand by changing traditional drinking and eating habits. The global community has now further endorsed the development and implementation of policies that restrict marketing with Member States adopting an indicator to monitor progress in introducing such measures. Other policy actions included in NOURISHING aim to improve the quality of the food supply, through community food production, agri-food policies that are consistent with and supportive of nutrition goals, and efforts to improve nutritional composition of food products. Governments will need to set nutrition goals for policies, programmes and interventions in agriculture and across all other relevant sectors.
9UICC Advocacy Toolkit 2014 - Cancer & Development

A GLOBAL CONVERSATION
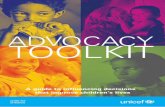
With the current MDGs set to expire in 2015, a conversation has begun on how to advance the global development agenda beyond 2015. Discussions at the UN and around the globe are underway on the successor development framework to the MDGs that will culminate at a Summit at Heads of State and Government (HoSG) level in September 2015 for the adoption of the post-2015 development agenda (Figure 1).
A number of processes have been underway in parallel, predominantly with the aim of providing content to inform the main intergovernmental negotiations that will begin at the 69th UN General Assembly (UNGA) session in September 2014.These have consisted of the following to date:
1. Intergovernmental Processes
a. Open Working Group on Sustainable Development Goals (OWG)
At the UN Conference on Sustainable Development (Rio+20), held in June 2012, Member States agreed to establish an intergovernmental, open working group to design Sustainable Development Goals (SDGs).
The OWG comprises 70 countries that share 30 seats through a balanced membership from different regions. It held regular sessions from March 2013 to February 2014 focusing on various thematic and cross-cutting issues that could be included as Sustainable Development Goals (SDGs), including health. The OWG Health Cluster meeting in June 2013 recommended that equal attention be given to existing and emerging health challenges, including NCDs, as well as setting an overarching health SDG goal that goes beyond disease silos and promotes multisectoral action. Universal health coverage was proposed as a possible goal and an important tool to foster healthy populations. The OWG is expected to submit a report by September 2014 that will contain proposed SDGs for consideration and eventual adoption by Member States in 2015. The OWG holds meetings with civil society representatives before every OWG session day.
OWG website
OWG schedule of sessions
OWG interim report (July 2013)
b. High-Level Political Forum (HLPF)
In line with the Rio+20 outcome document, the HLPF replaces the UN Commission on Sustainable Development. It will provide political leadership, guidance and recommendations for sustainable development. The first meeting took place in September 2013. The forum will meet at the level of Heads of State and Government every four years, and annually at the ministerial level. The next meeting of the HLPF will take place in July 2014.
HLPF website
THE ROADMAP TO AGREEMENT OF THE POST-2015 DEVELOPMENT AGENDA
10 UICC Advocacy Toolkit 2014 - Cancer & Development

c. Expert Committee on a Sustainable Development Financing Strategy
The Expert Committee is considering financial needs, financial resources and a related institutional framework with a view on proposing options for an effective sustainable development financing strategy. It is expected to submit its final report in September 2014.
Expert Committee website
2. Inputs into the Intergovernmental Processes
d. Secretary-General’s report on MDGs and the post-2015 agenda
To inform the discussions at the MDG Special Event held in September 2013, the UN Secretary-General (UNSG), Mr Ban Ki-moon, released his report on implementing the MDGs and further steps to advance the UN development agenda beyond 2015. The report, entitled ‘A life of dignity for all: accelerating progress towards the MDGs and advancing the UN development agenda beyond 2015,’ stresses sustainable development as the “global guiding principle” for the post-2015 era, and recognises reducing the burden of NCDs as a priority for health post-2015.
Report August 2013: A Life of Dignity for All
e. High-Level Panel of Eminent Persons on Post-2015 (HLP)
In July 2012, the UNSG appointed a high-level panel of 26 members to set out a “bold and practical” vision of the post-2015 development agenda. The HLP was co-chaired by President Yudhoyono of Indonesia, President Sirleaf of Liberia and Prime Minister Cameron of the United Kingdom. Following consultative processes (11 global thematic consultations including health and national consultations in over 60 countries), the final report of the HLP was released in May 2013. The report recognises that health outcomes can only be achieved by ensuring equity in all three dimensions of sustainable development - social, economic and environmental - and through steady progress towards achieving universal health coverage. Twelve universal goals and 54 national targets are recommended including an overarching health goal to “Ensure Healthy Lives” and a target for countries to “reduce the burden of disease from HIV/AIDS, tuberculosis, malaria, neglected tropical diseases and priority non-communicable diseases.” With this target, NCDs are placed alongside other priority health issues within the post-2015 framework. The target provides a welcome shift away from a focus on mortality to disability and morbidity.
HLP websiteReport May 2013: A New Global Partnership
THE ROADMAP TO AGREEMENT OF THE POST-2015 DEVELOPMENT AGENDA (CONTINUED)
11UICC Advocacy Toolkit 2014 - Cancer & Development

f. Sustainable Development Solutions Network (SDSN)
The SDSN was launched in 2012 to mobilise scientific and technical expertise from academia, civil society, and the private sector to identify common solutions to sustainable development challenges and to highlight best practices at local, national, and global levels. The network is structured around 12 thematic groups including health.
In June 2013, the SDSN published a report that includes 10 proposed goals for the post-2015 development agenda. This included a goal to achieve “Health and Wellbeing at all ages”. Specifically, the proposed goal calls for achieving universal health coverage at every stage of life to ensure that all people receive quality health services without suffering financial hardship. A target is proposed to reduce premature mortality (<70 years of age) from NCDs by at least 30% by 2030 compared with the level in 2015. The focus on a life-course approach to NCDs is significant as well as a strong emphasis on reducing risk factors that contribute to the increasing NCD burden.
SDSN website
Report June 2013: An Action Agenda for Sustainable Development
g. Global Compact
The UN Global Compact is a strategic policy initiative for businesses that are committed to aligning their operations and strategies with ten universally accepted principles in the areas of human rights, labour, environment and anti-corruption. It has conducted a post-2015 consultation process directed at its member companies.
In June 2013, it issued a report based on these consultations that emphasises the contribution of the private sector to the post-2015 agenda and proposes 10 goals that are broadly convergent with the goals proposed by the SDSN and the HLP reports. This included a goal for universal health coverage that supports a strong focus on affordable access to quality treatment and care.
Global Compact website
Report: Corporate Sustainability and the United Nations Post-2015 Development Agenda
THE ROADMAP TO AGREEMENT OF THE POST-2015 DEVELOPMENT AGENDA (CONTINUED)
2013SEPTEMBER: 68TH UNGA BEGINS
2014SEPTEMBER: 69TH UNGA BEGINS
2015SEPTEMBER: 70TH UNGA BEGINS
• SDS Network Report
• UN Global Compact Report
• Thematic consultations
• Country Consultations
• On-line consultations
• High-Level Panel Report (May 2013)
• SG Report (MDGs & Post-2015) Sept
2013
• SG Synthesis Report by December 2014
• SDG Open Working Group (OWG)
• High-Level Political Forum (HLPF)
1st Meeting Sept 2013
• SDG OWG Report Sept 2014
• Expert Committee on Financing Report Sept 2014
• HLPF 2nd Meeting July 2014, Report Sept 2014
• Intergovernmental Negotiations begin Sept 2014 • HoSG Summit Sept 2015 to adopt
post-2015 agenda
A VISUAL TIMELINE OF KEY MILESTONES TO AGREEMENT OF THE POST-2015 AGENDA
BLUE: INPUTS INTO THE INTERGOVERNMENTAL PROCESS
GREEN: INTERGOVERNMENTAL PROCESSES
ORANGE: UN SECRETARY-GENERAL (SG) PROCESS
RED: INTERGOVERNMENTAL NEGOTIATION
12 UICC Advocacy Toolkit 2014 - Cancer & Development

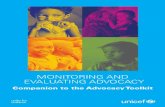
The adoption of an overarching health goal in the post-2015 agenda that recognises the central role that health and wellbeing play in development is critical. Recommended by the NCD Alliance, and endorsed by UICC, the outcome-focused goal of “maximising healthy lives at all stages of life” measures healthy life expectancy (HALE) throughout the life-course.21 Going beyond survival, this goal would seek to measure morbidity and disability at all ages and for all causes, and with the right metrics could be applied to all countries. This goal aims to move away from a vertical approach to health and instead prioritise the strengthening of health systems to tackle all global health challenges encompassing cancer and other NCDs as well as existing MDG priorities in child and maternal health, sexual and reproductive health and infectious diseases..
Maximising healthy lives at all stages of life supports a life-course approach to health to affect sustainable and inclusive development. It considers how multiple social, cultural and economic determinants such as gender equity and education interact to impact health throughout life and across generations, from pre-conception to death whatever age that may occur. A life-course perspective acknowledges that there are different entry points across the life-course for action including in childhood and adolescence through for example, delivering health promotion and health information on behavioural risk factors. Additionally, this approach provides new arenas for collaboration across education, labour, legal, agricultural, transport and other sectors that influence HALE through an approach to health that is equitable, gender-sensitive and rights-based.
WHO defines HALE as the average number of years that a person can expect to live in full health by taking into account years lived in less than full health due to disease and/or injury.
MOVING TOWARDS A HEALTH TARGET WITHIN THE POST-2015 DEVELOPMENT AGENDA
Credit: Dain, NCD Alliance
Post-2015 Health Framework
13UICC Advocacy Toolkit 2014 - Cancer & Development

An estimated 100 million people are forced into extreme poverty every year due to out-of-pocket health spending. This includes out-of-pocket expenses related to cancer services including diagnosis, treatment and palliative care that can impoverish families without access to social protection. The issue is one of social equity. Poor populations frequently live in vulnerable conditions and are disproportionately affected by the costs of cancer treatment and care and the least likely to access quality services.
The provision of universal health coverage (UHC) and other social protection measures can play an important role in closing the unacceptable gaps in access to cancer services that occur in most LMICs. Through the integration of UHC in the post-2015 framework, the international community has the opportunity to provide a country-driven strategy for ensuring that all people obtain the health services they need without suffering financial hardship.22 UHC is grounded in the right to health and aims to ensure access to quality health services based on need and not on the ability to pay or other social attributes.23
A compelling argument for the implementation of UHC is its role as an enabler for strong health systems that have the capacity to respond to cancer and other NCDs as well as facilitate progress on the existing health MDGs. This strategy avoids the vertical approach to disease management embedded in the existing development framework. At the same time it acknowledges that many LMICs are struggling with the double burden of disease which often share common underlying social determinants, exhibit co-morbidities and require joint solutions such as a skilled and supported primary health care workforce.
Universal health coverage (UHC) is defined as ensuring that all people can use the promotive, preventive, curative, rehabilitative and palliative health services they need, of sufficient quality to be effective, while also ensuring that the use of these services does not expose the user to financial hardship.
UNIVERSAL HEALTH COVERAGE AS AN ENABLER OF EQUITY IN CANCER CARE ACROSS THE LIFECOURSE
14 UICC Advocacy Toolkit 2014 - Cancer & Development

For this approach to successfully mitigate mortality, morbidity and disability from cancer, UHC must go beyond coverage and be placed within the broader context of addressing the barriers to equitable access to quality cancer services:
• Access and availability must improve across the cancer care continuum from prevention, diagnosis, multimodal treatment, supportive and palliative care services including the availability of affordable essential medicines and technologies.
• Governments must seek to adopt proven effective policies that improve access to cancer services and will contribute to making UHC attainable. For example, adopting policies to increase efficiency in procurement, supply, and use to promote affordable and equitable access to essential cancer medicines including opioids for pain relief; and policies and programmes to address the availability and accessibility of a cancer workforce with the right skills, knowledge and competencies.
• Coordinated action is required beyond the health sector with many evidence-based interventions requiring multi-sectoral approaches including the effective use of the law.
• The alleviation of other known barriers to access should be addressed such as social barriers related to culture and local beliefs.
Although no single roadmap exists for the implementation of UHC at the country level, the capacity for low-income countries to move towards UHC has been demonstrated in at least nine low-income and lower-middle-income countries in Africa and Asia. Each of these countries have implemented varied national health insurance models, with some countries (India, Kenya, the Philippines) that originally covered only inpatient services now moving to expanding benefits to cover primary and preventive services.24 Many more countries are now undergoing reforms towards UHC including South Africa, Vietnam, Ghana and Rwanda.
Importantly UHC will not be sufficient on its own to address the global cancer and NCD burden due to its focus on health. The post-2015 framework must seek to strengthen links outside of health to address the underlying social, economic, political, environmental and cultural factors that affect health outcomes.6
MOVING TOWARDS A HEALTH TARGET WITHIN THE POST-2015 DEVELOPMENT AGENDA(CONTINUED)
15UICC Advocacy Toolkit 2014 - Cancer & Development

CASE STUDYPRIORITISING AFFORDABLE, EFFECTIVE AND QUALITY CANCER SERVICES FOR UNIVERSAL COVERAGE: THAILAND AND CERVICAL CANCER PREVENTION
Thailand’s transition to universal health coverage began in 1975 with the creation of the Medical Welfare Scheme to cover the poor. Coverage has continued to expand over time, and in 2001 the Government of Thailand established the Universal Coverage Scheme, which now covers almost 100% of Thailand’s population. Beneficiaries of the scheme are entitled to pay no more than 30 baht (USD 0.84) per medical visit. Total health expenditure as a percent of GDP has remained constant, but impoverishment due to payment for health services has decreased substantially, from 18.3% before 2001 to 8% in 2004.
Decisions regarding which health technologies are eligible for funding are performed by the Health Intervention and Technology Assessment Programme (HITAP, www.hitap.net) which was set up to assess the costs, effectiveness and cost-effectiveness of health technologies – not only medications and medical procedures but also social interventions, public health measures and changes to the health system itself.26,27 One example of HITAP’s work is in devising an evidence-based screening strategy for cervical cancer.
The 2009 Report of Thailand’s Burden of Diseases, Injuries and Risk Factors shows that nine of the top ten conditions are due to NCDs, with cervical cancer one of the major causes of morbidity and mortality among Thai women. Despite the introduction of Pap screening at every hospital over 40 years ago, only 5% of women were screened. Visual inspection of the cervix with the naked eye after application with acetic acid (VIA) was introduced as an alternative in 2001 because it did not require cytologists.
The options considered by HITAP were conventional Pap screening, VIA, vaccination or a combination of Pap screening and VIA. Costs were calculated on the basis of estimated levels of participation and included costs to the healthcare provider, costs for women attending screening and costs for those who were treated for cervical cancer. Potential benefits were analysed using a model that estimated the number of women who would go on to develop cervical cancer in each scenario, and the impact on quality-adjusted life years (QALYs) was calculated by using data from a cohort of Thai patients. The study concluded that the most cost-effective strategy was to offer VIA to women every five years between the ages of 30 and 45, followed by a Pap smear every five years for women aged between 50 and 60 years. The strategy would offer an additional 0.01 QALYs and a total cost saving of 800 Baht, when compared to doing nothing. Universal introduction of vaccination for 15-year-old girls without screening would result in a gain of 0.06 QALYs at a cost of 8000 Baht, and either VIA and Pap screening alone would have costs and benefits somewhere between the two amounts.28 The approach recommended by HITAP was piloted in several provinces starting in 2009, and this has now been implemented nationally.
16 UICC Advocacy Toolkit 2014 - Cancer & Development

THE TIME TO ACT IS NOW
The most urgent priority for the cancer community is to make cancer and NCDs a top priority for governments and ensure that cancer and NCDs are embedded within the post-2015 development framework. Of equal importance is influencing aid policies to ensure the adequate flow of development assistance through human, financial and technical resources needed urgently by many LMICs to progress towards equitable access to quality cancer services.
UICC members and partners can make a difference by taking action in five ways:
• Reach out to all sectors of governments using the World Cancer Declaration together with resource-appropriate and culturally relevant examples of successful implementation of policies and programmes and send the message that there is a high cost to inaction.
› The UICC Advocacy Toolkit is designed to be a key resource to assist you in strengthening your advocacy efforts by providing Evidence Sheets that support each of the World Cancer Declaration targets as well as practical tools.
› Benchmark your country’s progress against the targets and indicators contained within the Global Monitoring Framework to assist in identifying key priorities for advocacy. Several data sources are available to assist members to benchmark country capacity and responses to cancer, including the PAHO “Cancer in the Americas: Country profiles, 2013” and the Global Opioid Policy Initiative (GOPI) project country results.
The NCD Alliance has produced a national/regional NCD civil society benchmarking tool to assess progress on NCD action. To complement this tool, UICC will soon be releasing a cancer-specific benchmarking module to assist cancer advocates in tracking progress against priority cancer targets and indicators. The NCD Alliance online Advocacy Toolkit can be found here.
17UICC Advocacy Toolkit 2014 - Cancer & Development

• • Continue pressing for cancer and NCD-related goals to be embedded within the next generation of internationally agreed development goals by contributing to consultations on the post-2015 framework at all levels both through traditional and social media outlets.
› Keep informed and provide input on global consultations through the NCD Alliance Common Interest Group.
› Follow, comment and share media reports that highlight the issues of cancer in development – for some recent examples, have a look at articles in the New York Times, and The Guardian.
• Create synergistic partnerships with non-traditional partners in other health areas (e.g. under-nutrition; communicable diseases), development, disability, education, employment and many other sectors to accelerate progress on shared goals and take advantage of existing platforms and infrastructure.
› Scope out at the local and national levels civil society organisations, relevant private sector institutions, and other stakeholders viewing cancer in the broader context including through the lens of a rights-based approach with UHC embedded in the right to health.
• Share effective strategies for advocacy with other organisations with shared goals. For example, the critical need for quality, disaggregated data to inform the planning process, monitoring, evaluation and accountability of global health and development interventions.
› Understand the key barriers to access to quality cancer services in your community and seek collaborations that will address these, remembering that many cancer-related issues require solutions outside of health including legislative and regulatory measures.
› Share information and case studies with UICC and the NCD Alliance to strengthen global advocacy.
› Contact the UICC Advocacy Team at [email protected] and NCD Alliance at http://ncdalliance.org/contact-us
• Strengthen local and regional advocacy by:
› Joining or creating national NCD coalitions
› Engaging with other organisations concerned with the post-2015 agenda
› Social mobilisation to raise the profile of NCDs and development issues among the general public.
THE TIME TO ACT IS NOW (CONTINUED)
18 UICC Advocacy Toolkit 2014 - Cancer & Development

KEY MESSAGES FOR CANCER AND DEVELOPMENT
• Cancer is not just a health issue. It has wide-reaching social, economic and human rights implications, and is a significant barrier to achieving inclusive and equitable development.
• The next generation of global development goals and targets must address equity and health as a human right with the ultimate consequence of maximising healthy lives at all stages of life.
• All people have the right to access proven effective cancer treatment and services on equal terms and without suffering economic hardship as a consequence.
• Taking a rights-based, equity and person-centred approach to health that gives equal attention to mitigating the impact of existing and emerging health challenges including cancer will accelerate progress towards the World Cancer Declaration targets and facilitate achievement of the ambitious goal of a 25% reduction in relative overall premature mortality from NCDs by 2025.
• Social protection measures, including universal health coverage (UHC), can ensure that all individuals and families have full access to quality healthcare and opportunities to prevent and control cancer. The adoption of UHC must be considered in the wider context of addressing all of the barriers to access to cancer services including the underlying social, economic, political, environmental and cultural factors, broadly known as ‘social determinants’.
• Development assistance must be aligned to country priorities so that low- and middle- income countries receive adequate human, financial and technical resources to progress towards equitable access to quality cancer services.
19UICC Advocacy Toolkit 2014 - Cancer & Development
© Francois S
TRU
ZIK - Im
age of dignity

KEY RESOURCES• Global health 2035: A world converging within a generation. – Read
the report at: http://download.thelancet.com/pdfs/journals/lancet/PIIS0140673613621054.pdf?id=8b69abadd6dadf97:4d51d508:142b742f1ef:-b3f1386057387625
• Global Thematic Consultation on Health: Final report - health in the post-2015 development agenda. Botswana 2013. Accessible at: http://www.worldwewant2015.org/file/337378/download/366802
• NCD Alliance briefing paper: Healthy Planet, Healthy People: The NCD Alliance vision for health in the post-2015 development agenda. Read the paper at: http://ncdalliance.org/visionfor2015
• NCD Alliance briefing paper: Tackling Non-communicable Diseases to Enhance Sustainable Development Read the paper at: http://ncdalliance.org/sites/default/files/NCD%20Alliance%20-%20NCDs%20and%20Sustainable%20Development%20Brief_0.pdf
• UNDP. Discussion Paper: Addressing the Social Determinants of Non-communicable Diseases, October 2013 Read the paper at: http://www.undp.org/content/undp/en/home/librarypage/hiv-aids/discussion-paper--addressing-the-social-determinants-of-noncomm
• United Nations General Assembly, The Future We Want: Outcome document of the UN Conference on Sustainable Development. A/Res/66/288. Accessible at: http://www.uncsd2012.org/thefuturewewant.html
• World Health Organization. The World Health Report 2013: Research for Universal Health Coverage. Accessible at: http://www.who.int/whr/2013/report/en/
• World Health Organization. Ten Facts on Universal Health Coverage Accessible at: http://www.who.int/features/factfiles/universal_health_coverage/facts/en/index.html
REFERENCES 1. Globocan 2012 – Prediction http://globocan.iarc.fr/Pages/burden_sel.aspx2. Political Declaration of the High-level Meeting of the General Assembly on the
Prevention and Control of Non-communicable Diseases. (2011). A/66/L.1.3. The Future We Want. (2012). Retrieved from http://www.uncsd2012.org/rio20/
thefuturewewant.html4. WHO. (2013). Global action plan for the prevention and control of non-
communicable diseases 2013 -2020. Geneva: WHO.5. Globocan 2012 http://globocan.iarc.fr/Default.aspx6. UNDP. (2013). Discussion Paper Addressing the Social Determinants of Non-
communicable Diseases. New York: UNDP.7. Knaul FM, Frenk J, Shulman L. (2011). Closing the Cancer Divide: A Blueprint
to Expand Access in Low and Middle Income Countries. Harvard Global Equity Initiative. Boston: Global Task Force on Expanded Access to Cancer Care and Control in Developing Countries.
8. Bloom DE, et al. (2011). The Global Economic Burden of Non-communicable Diseases. World Economic Forum. Geneva: World Economic Forum.
9. Mahal A, at al. (2013). The economic burden of cancers on Indian households. PLoS ONE, 8, e71853. doi:10.1371/ journal.pone.0071853.
10. Leive A, Xu K. (2008). Coping with out-of-pocket health payments: empirical evidence from 15 African countries. Bulletin of the World Health Organization, 86, 849-56.
11. Gale, J. (2013). India’s Cancer Surge. Bloomberg Markets Magazine.12. WHO. (2012). Global Report: Mortality attributable to tobacco 2012. Geneva:
World Health Organization.13. WHO. (2011). Global status report on alcohol and health. World Health
Organization.14. Warren CW, et al. (2006). Patterns of global tobacco use in young people and
implications for future chronic disease burden in adults. Lancet, 367, 749-53.15. Black RE, et al. Maternal and child undernutrition and overweight in low-
income and middle-income countries. Lancet, 382, 427-51.16. WHO. (2011). Global Status Report on noncommunicable diseases 2010.
Geneva: Wold Health Organization.17. Marquez, P. V. (2013). The Challenge of Non-Communicable Diseases and
Road Traffic Injuries in Sub-Saharan Africa. An Overview. Washington DC: The World Bank.
18. IARC. (2013). IARC Scientific Publication No. 161: Air Pollution and Cancer. (A. C. Kurt Straif, Ed.)
19. WHO. (2010). Set of recommendations on the marketing of foods and non-alcoholic beverages to children. Geneva: WHO.
20. Hawkes C, Jewell J, Allen K. (2013). A food policy package for healthy diets and the prevention of obesity and diet-related non-communicable diseases: the NOURISHING framework. Obes Rev, 14, Suppl 2, 159-168.
21. NCD Alliance. (2013). Healthy Planet, Health People: The NCD Alliance vision for health in the post-2015 development agenda. Geneva: NCD Alliance.
22. Vega, J. (2013). Universal health coverage: the post-2015 development agenda. Lancet, 381, 179-80.
23. Rockefeller Foundation, Save the Children, UNICEF, WHO. (2013). Universal Health Coverage: A commitment to close the gap. London: Save the Children.
24. Lagomarsino G, et al. (2012). Moving towards universal health coverage: health insurance reforms in nine developing countries in Africa and Asia. Lancet, 380, 933-43.
25. WHO. (2013). The world health report 2013: research for universal health coverage. Geneva: WHO.
26. Tantivess S, Teerawattananon Y, Mills A. (2009). Strengthening cost-effectiveness analysis in Thailand through the establishment of the health intervention and technology assessment program. PharmacoEconomics, 27, 931-945.
27. Hanson K, et al. (2010). Scaling up health policies and services in low- and middle-income settings. BMC Health Services Research, 10, Suppl 1, I1.
28. Praditsitthikorn N, et al. (2011). Economic evaluation of policy options for prevention and control of cervical cancer in Thailand. PharmacoEconomics, 29, 781-806.
20 UICC Advocacy Toolkit 2014 - Cancer & Development