UFH & LMWH & fondaparinux
37
1
-
Upload
mohammed-adel -
Category
Documents
-
view
587 -
download
3
Transcript of UFH & LMWH & fondaparinux

1

2
Non-Warfarin AnticoagulantsFrom comparison into
clinical practiceBy:
Mohammed Adel B.Sc., PharmDClinical Pharmacy Department
Al-Ahrar General Hospital

3
Content•Blood hemostasis•UFH vs LMWH vs Fondaparinux •Practice guidelines recommendations about:•UFH•LMWH•Fondaparinux

4
Blood hemostasis

5
UFH vs LMWH vs Fondaparinux •Mechanism of action •Timing of treatment before surgery•Pharmacokinetic Parameters•Dosing frequencies

6
UFH vs LMWH vs Fondaparinux •Pregnancy •Ability to cause HIT•Use in HIT treatment•Use in Pt with Hx of HIT

7
UFH vs LMWH vs Fondaparinux •Mechanism of action:
UFH:Binds to and potentiates the actions of antithrombin (AT) to inactivate factor Xa
Prevent the conversion of prothrombin to thrombin

8
UFH vs LMWH vs Fondaparinux •Mechanism of action:
UFH:Prevent the conversion of fibrinogen to fibrin
Binds nonspecifically to various plasma proteins and endothelial cells resulting in an unpredictable dose-response relationship and low bioavailability after subcutaneous (SC) administration

9
UFH vs LMWH vs Fondaparinux •Mechanism of action:
LMWH:Same as UFH but with longer and more preferential binding with factor Xa
Less able to inhibit the production of thrombin and bind to plasma proteins and endothelial cells less due to their decreased size

10
UFH vs LMWH vs Fondaparinux •Mechanism of action:
LMWH:More predictable anticoagulant responseLess inter-patient variabilityLonger duration of action than heparin.

11
UFH vs LMWH vs Fondaparinux •Mechanism of action:
Fondaparinux:Enhances the anti-Xa activity of AT by 300-fold
AT specificity does not allow binding to other plasma proteins

12
UFH vs LMWH vs Fondaparinux •Mechanism of action:
Fondaparinux:It has no direct effect on thrombinIt has excellent bioavailability after SC administration and longer half-life

13
UFH vs LMWH vs Fondaparinux •Timing before surgery:
Agent of treatment
Half life Last dose before procedure
UFH 45 mins 4 HrsLMWH 4-7 Hrs 24 HrsFondaparinux
17-21 Hrs 2-4 days

14
UFH vs LMWH vs Fondaparinux

15
Practice guidelines recommendations
Primary and secondary prevention of cardiovascular diseases
Management of anticoagulantsPrevention of VTE in non-surgical Pts
Treatment of VTE
ACCF/AHA joint
Guidelines
9th ACCP
Guidelines

16
ACCF/AHA RECOMMENDATIONS
3.5. Adjunctive Antithrombotic Therapy to Support Reperfusion With Primary PCI
STEMI
17
ACCF/AHA RECOMMENDATIONS
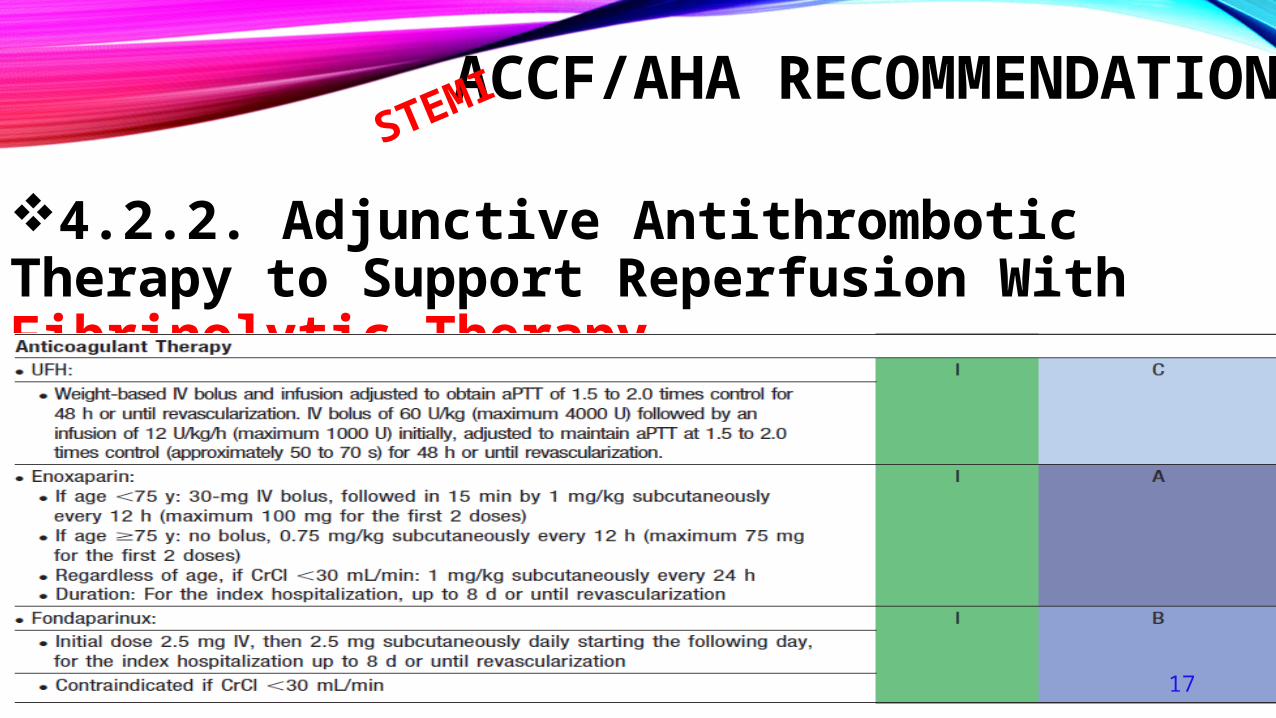
4.2.2. Adjunctive Antithrombotic Therapy to Support Reperfusion With Fibrinolytic Therapy
STEMI

18
ACCF/AHA RECOMMENDATIONS
5.4.1. Anticoagulant Therapy to Support PCI After Fibrinolytic Therapy
STEMI

19
ACCF/AHA RECOMMENDATIONSNSTEMI
Early initiation

20
ACCF/AHA RECOMMENDATIONSNSTEMI

21
ACCP RECOMMENDATIONS
The 8th edition of the ACCP guidelines included 600 recommendations in 968 pages
Very lengthyPractice non-friendly
In 2012 the 9th edition provided highly focused and brief recommendations in addition to the detailed edition

22
ACCP RECOMMENDATIONS
Management of anticoagulants6.1 UFH Dose Adjustment by Weight
For VTE IV UFH, bolus 80 units/kg followed by 18 units/kg per h
For cardiac or stroke patients bolus 70 units/kg followed by 15 units/kg per h
Use of a fixed dose (bolus 5,000 units followed by 1,000 units/h).

23
ACCP RECOMMENDATIONS
Management of anticoagulants6.2 Dose Management of (SC) UFH:
For outpatients with VTE treated with SC UFH, we suggest weight-adjusted dosing (first dose 333 units/kg, then 250 units/kg) without monitoring rather than fixed or weight adjusted dosing with monitoring (Grade 2C) .

24
ACCP RECOMMENDATIONS
Management of anticoagulants7.1 Therapeutic Dose of LMWH in Patients With Decreased Renal FunctionFor patients receiving therapeutic LMWH who have severe renal insufficiency (CrCL, 30 mL/min), we suggest a reduction of the dose rather than using standard doses (Grade 2C) .

25
ACCP RECOMMENDATIONS
Management of anticoagulants8.1 Fondaparinux Dose Management by Weight:
For patients with VTE and body weight over 100 kg, we suggest that the treatment dose of Fondaparinux be increased from the usual 7.5 mg to 10 mg daily SC (Grade 2C).

26
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts2.3. Hospitalized Acutely ill Medical Patients
For acutely ill hospitalized medical patients at increased risk of thrombosis, we recommend anticoagulant thromboprophylaxis with:
Low molecular weight heparin LMWHLow-dose unfractionated heparin (LDUH) bid or tid
Fondaparinux

27
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts2.4. For acutely ill hospitalized medical patients at low risk of thrombosis:We recommend against The use of:
Pharmacologic prophylaxisMechanical prophylaxis

28
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts2.7.1. For acutely ill hospitalized medical patients who are bleeding or at high risk for bleeding:we recommend against anticoagulant thromboprophylaxis (Grade 1B) .

29
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts2.7.2. For acutely ill hospitalized medical patients at increased risk of thrombosis who are bleeding or at high risk for major bleeding:we suggest the optimal use of mechanical thromboprophylaxis with graduated compression stockings (GCS)(Grade 2C) intermittent pneumatic compression (IPC) (Grade 2C) , rather than no mechanical thromboprophylaxis.

30
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts2.7.2. For acutely ill hospitalized medical patients at increased risk of thrombosis who are bleeding or at high risk for major bleeding:When bleeding risk decreases, and if VTE risk persists, we suggest that pharmacologic thromboprophylaxis be substituted for mechanical thromboprophylaxis (Grade 2B).

31
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts2.8. In acutely ill hospitalized medical patients who receive an initial course of thromboprophylaxis:We suggest against extending the duration of thromboprophylaxis beyond the period of patient immobilization or acute hospital stay (Grade 2B) .

32
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts3.2. In critically ill patients:
We suggest against routine ultrasound screening for DVT (Grade 2C) .
We suggest using LMWH or LDUH thromboprophylaxis over no prophylaxis (Grade 2C).

33
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts3.4.4. For critically ill patients who are bleeding, or are at high risk for major bleeding:We suggest mechanical thromboprophylaxis with GCS (Grade 2C) or IPC (Grade 2C) until the bleeding risk decreases, rather than no mechanical thromboprophylaxis.
When bleeding risk decreases, we suggest that pharmacologic thromboprophylaxis be substituted for mechanical thromboprophylaxis (Grade 2C) .

34
ACCP RECOMMENDATIONS
Prevention of VTE in non-surgical Pts4.2.2. In outpatients with solid tumors who have additional risk factors for VTE and who are at low risk of bleeding:We suggest prophylactic dose LMWH or LDUH over no prophylaxis (Grade 2B) .

35
ACCP RECOMMENDATIONS
Treatment of VTE 2.1 Initial Anticoagulation for Patients With Acute DVT of the LegIn patients with acute DVT of the leg treated with VKA
therapy, we recommend initial treatment with parenteral anticoagulation (LMWH, Fondaparinux, IV UFH, or SC UFH) over no such initial treatment (Grade 1B).

36
ACCP RECOMMENDATIONS
Treatment of VTE 2.5 Choice of Initial Anticoagulant Regimen in Patients With Proximal DVTIn patients with acute DVT of the leg, we suggest LMWH or Fondaparinux over IV UFH (Grade 2C) and over SC UFH (Grade 2B for LMWH; Grade 2C for Fondaparinux) .
In patients with acute DVT of the leg treated with LMWH, we suggest once- over twice-daily administration(Grade 2C).
Talking
about
Dalteparin

37
Thank
youBest Regards








![UFH [Compatibility Mode]](https://static.fdocuments.net/doc/165x107/577cdf961a28ab9e78b18bcf/ufh-compatibility-mode.jpg)