
UCSF Advances in Heart Disease - UCSF Medical · PDF fileUCSF Advances in Heart Disease ......
35
1 UCSF Advances in Heart Disease UCSF Advances in Heart Disease Elliott M. Antman, MD Elliott M. Antman, MD Cardiovascular Division Cardiovascular Division Brigham and Women Brigham and Women’ s Hospital s Hospital Harvard Medical School Harvard Medical School Contemporary Management of STEMI: Contemporary Management of STEMI: Emphasis on Systems of Care Emphasis on Systems of Care December 2008
Transcript of UCSF Advances in Heart Disease - UCSF Medical · PDF fileUCSF Advances in Heart Disease ......
1
UCSF Advances in Heart DiseaseUCSF Advances in Heart Disease
Elliott M. Antman, MDElliott M. Antman, MD
Cardiovascular DivisionCardiovascular Division
Brigham and WomenBrigham and Women’’s Hospitals Hospital
Harvard Medical SchoolHarvard Medical School
Contemporary Management of STEMI:Contemporary Management of STEMI:
Emphasis on Systems of CareEmphasis on Systems of Care
December 2008

2
Disclosure
Accumetrics, Inc. Accumetrics, Inc.
Amgen, Inc. Amgen, Inc.
AstraZeneca Pharmaceuticals LPAstraZeneca Pharmaceuticals LP
BaxterBaxter
Bayer Healthcare LLCBayer Healthcare LLC
Beckman Coulter, Inc. Beckman Coulter, Inc.
Biosite IncorporatedBiosite Incorporated
BristolBristol--Myers SquibbMyers Squibb
CardioKinetixCardioKinetix
CV Therapeutics, Inc.CV Therapeutics, Inc.
DaiichiDaiichi--Sankyo Sankyo
Eli Lilly and CompanyEli Lilly and Company
FoldRxFoldRx
GlaxoSmithKlineGlaxoSmithKline
INO Therapeutics LLCINO Therapeutics LLC
Inotek Inotek Pharmaceuticals CorporationPharmaceuticals Corporation
The National Institutes of HealthThe National Institutes of Health
Integrated Therapeutics CorporationIntegrated Therapeutics Corporation
KAI PharmaceuticalsKAI Pharmaceuticals
Merck & Co., Inc.Merck & Co., Inc.
Millennium Pharmaceuticals, Inc. Millennium Pharmaceuticals, Inc.
Novartis PharmaceuticalsNovartis Pharmaceuticals
Nuvelo, Inc. Nuvelo, Inc.
OrthoOrtho--Clinical Diagnostics, Inc. Clinical Diagnostics, Inc.
Pfizer, Inc. Pfizer, Inc.
Roche Diagnostics CorporationRoche Diagnostics Corporation
Roche Diagnostics GmbHRoche Diagnostics GmbH
SanofiSanofi--AventisAventis
SanofiSanofi--SynthelaboSynthelabo RechercheRecherche
ScheringSchering--Plough Research InstitutePlough Research Institute
St Jude MedicalSt Jude Medical
The TIMI Study Group has received research / grant support in thThe TIMI Study Group has received research / grant support in the past 2 yrs e past 2 yrs
through the Brigham & Womenthrough the Brigham & Women’’s Hospital with funding froms Hospital with funding from
(in alphabetical order):(in alphabetical order):
3
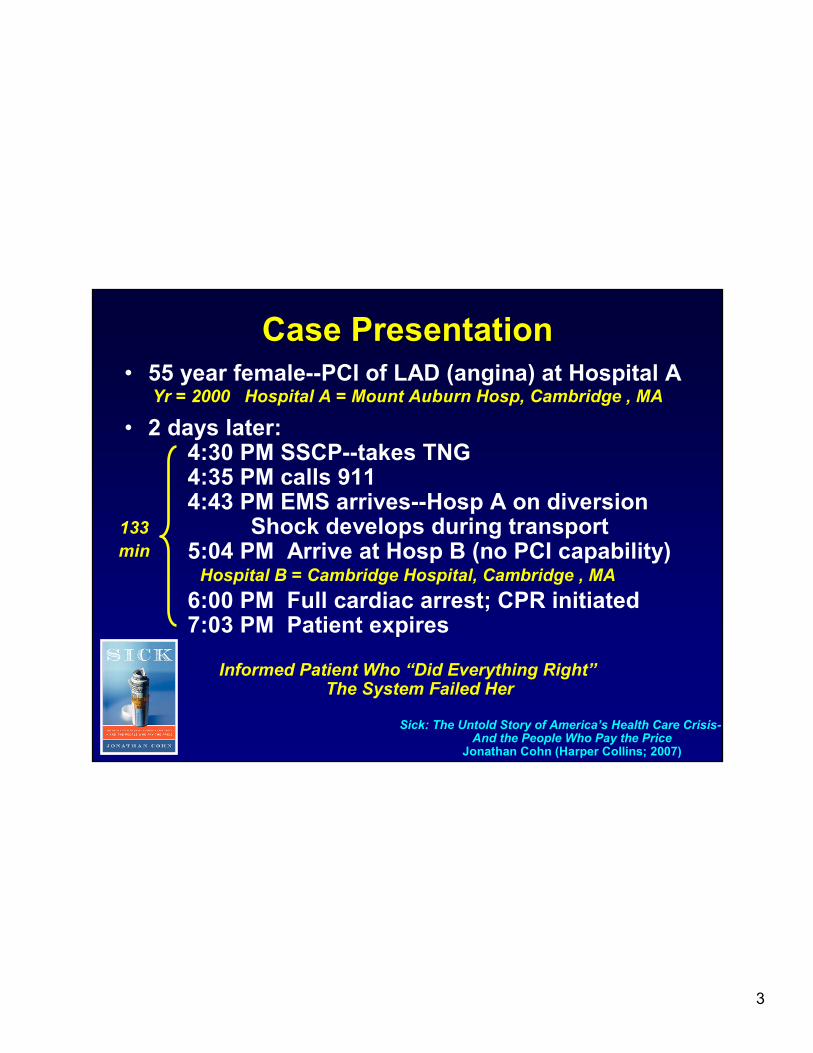
Case PresentationCase Presentation
• 55 year female--PCI of LAD (angina) at Hospital A
• 2 days later:4:30 PM SSCP--takes TNG4:35 PM calls 9114:43 PM EMS arrives--Hosp A on diversion
Shock develops during transport5:04 PM Arrive at Hosp B (no PCI capability)
6:00 PM Full cardiac arrest; CPR initiated7:03 PM Patient expires
Yr = 2000 Hospital A = Mount Auburn Hosp, Cambridge , MA
Hospital B = Cambridge Hospital, Cambridge , MA
133
min
Informed Patient Who “Did Everything Right”The System Failed Her
Sick: The Untold Story of America’s Health Care Crisis-And the People Who Pay the Price
Jonathan Cohn (Harper Collins; 2007)

4
PCI vs. Fibrinolysis:PCI vs. Fibrinolysis:ShortShort--term Clinical Outcomes (23 RCTs)term Clinical Outcomes (23 RCTs)
7
4.52.2
6
10
7 89
7 7
21
21
5
13
0
5
10
15
20
25
30
35
PCI
Fre
qu
en
cy (
%)
Keeley E, et al. Lancet. 2003;361:13.
P = 0.0002
P = 0.0003 P < 0.0001
P < 0.0001
P < 0.0001P = 0.0004
P = 0.032
P < 0.0001
Death Death, no
SHOCK
data
Re-MI Rec.
isch
Total
stroke
Hem.
stroke
Major
bleed
Death
MI
CVA
Fibrinolysis
N = 7,739N = 7,739

5
Time and Myocardial SalvageTime and Myocardial Salvage
0
20
40
60
80
100
1 3 6 12 24
HoursHours
Mo
rta
lity
Re
du
cti
on
(%
)M
ort
ali
ty R
ed
uc
tio
n (
%)
Extent of salvage (% of area at risk)
Time to treatment is criticalTime to treatment is criticalOpening the artery is the Opening the artery is the
primary goal (PCI > lysis)primary goal (PCI > lysis)
DD
EE
E – D — harm
A – B — no benefit
Potential outcomes
BA
CA – C — benefit
B – C — benefit
Gersh Gersh BJ, et al. BJ, et al. JAMAJAMA. 2005;293:979.. 2005;293:979.

6
EMS TransportEMS Transport
Onset of
symptoms of
STEMI
9-1-1
EMS
dispatch
EMS on scene• Encourage 12-lead ECGs
• Consider prehospital fibrinolytic
if capable and EMS–to–needle
within 30 min
GOALS
PCI
capable
Not PCI
capable
Hospital fibrinolysis: Hospital fibrinolysis:
DoorDoor––toto––needle needle
≤≤ 30 min30 min
EMS EMS
triage triage
planplan
InterInter--
hospitalhospital
transfertransfer
“Golden Hour” = 1st 60 min Total ischemic time: within 120 min
PatientPatient EMSEMS Prehospital fibrinolysisPrehospital fibrinolysis
EMSEMS––toto––needleneedle
≤≤ 30 min30 min
EMS transportEMS transport
EMSEMS--toto--balloon balloon ≤≤ 90 min90 min
Patient selfPatient self--transport transport
Hospital doorHospital door--toto--balloon balloon
≤≤ 90 min90 min
DispatchDispatch
1 min1 min
5
min
8
min
Options for Transport of Patients with STEMI Options for Transport of Patients with STEMI and Initial Reperfusion Treatmentand Initial Reperfusion Treatment
J Am J Am Coll CardiolColl Cardiol. 2004;44:671; . 2004;44:671; CirculationCirculation. 2004;110: 588.. 2004;110: 588.

7
Improving Access to Primary PCIImproving Access to Primary PCI
PCIPCI
capablecapable
Not PCINot PCI
capablecapablePCI w/oPCI w/o
Surg Surg BUBUCommunity Community
CenterCenter
PCIPCI
CenterCenter

8
Core StrategiesCore Strategies
1. ED physician activates the 1. ED physician activates the cath cath lab;lab;
2. One call activates the 2. One call activates the cath cath lab;lab;
3. 3. Cath Cath lab team ready in 20 lab team ready in 20 –– 30 minutes;30 minutes;
4. Prompt data feedback; 4. Prompt data feedback;
5. Senior management commitment;5. Senior management commitment;
6. Team6. Team--based approach. based approach.
A preA pre--hospital ECG to activate the hospital ECG to activate the cath cath lab is optional.lab is optional.
While other strategies exist, including having a cardiologist inWhile other strategies exist, including having a cardiologist in the the
hospital 24/7, they are not required for participation in the D2hospital 24/7, they are not required for participation in the D2B campaign.B campaign.
http://www.d2balliance.org/http://www.d2balliance.org/

9
Medical Simulation Training and Research to
Improve D2B Time Among Healthcare Teams
• Pt is 55 yr old male(wheelchair)
• Brought to ED by grandson• SSCP• Intermittent unresponsiveness• DM, Prior MI• Triage RN
Pages Resusc. TeamSends Grandson to Regist.
• BP 70/30• Pages Card x2• Call for CXR• Transport by main
elevator to cath lab
• BP 49/29• 9 persons in lab• ED RN unsure of
communication role• Room loud• Repeated briefings
on pt as morepersons arrive
Advances in Simulation-Based Team Training
HammanWR et al
10
Will issue reports on D2B time

11
AHA 08 AHA 08 Abst Abst 3173 3173 Nallomothu Nallomothu et alet al
0
20
40
60
80
100
06Q3 06Q4 07Q1 07Q2 07Q3 07Q4 08Q1
D2B
Non D2B% Rx
% RxWithin 90 min
Within 90 min
Prim PCI (non transfer) in GWTG hospitalsPrim PCI (non transfer) in GWTG hospitals
in D2B in D2B vs vs Not in D2BNot in D2B
5555
7575
7272
5353

12
Zone1 Protocol
Aspirin 325 mgAspirin 325 mg
Clopidogrel 600mgClopidogrel 600mg
UFHUFH
BetaBeta--blockerblocker
PCIPCI
Zone 2 Protocol
Aspirin 325 mgAspirin 325 mg
Clopidogrel 600mgClopidogrel 600mg
UFHUFH
TNK TNK ½½ dosedose
BetaBeta--blockerblocker
PCIPCI
Regional STEMI
System for PCI
Minneapolis
< 60 miles
< 60-210
miles
Henry et al Circ 2007

13
• ASA tablets in package
• Clopidogrel tables in package
• Metoprolol bolus x3
• Heparin bolus
• Heparin drip and tubing
• Alcohol swabs
• Calculator
• Standing orders with fibrinolytic calculations
• Blood vials
• PCS forms (Physician Certification Statement for Transfer)
• Transfer datasheet
• Standing orders
Level 1 MI Emergency Department Kit

14
Hot Load Transport of
STEMI Patients

15
Level 1 Page
Patient
PlacementPt Placement
SupervisorTelecommunications
Director
Chaplaincy
Security/Dispatch
ER Charge RN
CV Holding Room
CV/OR Manager
Answering Service
MCA Coordinator
CV Operations
CCU Charge RN
STEMI Program
ManagerHouse Supervisor
ED Com Physician
Admitting Director
Minneapolis Heart Institute

16
Minneapolis Heart Institute

17
Regional STEMI System for PCIMinneapolis Mar 2003 - Nov 2006; N= 1345
65
95
120
171
203214
4.4 4.6 5.7
0
50
100
150
200
PPCI Ctr Zone1 Zone2
Door 1-Balloon (min)
Sx-Balloon (min)
30 Day Mortality (%)
Henry et al Circ 2007
N=297 N=620 N=396

18
Regional STEMI
System for PCI
Mayo Clinic
PPCI Ctr
(St Mary’s)
28 Regional Hosp
Sx < 3h: lytic
Sx > 3 h: transfer
for PCI
Ting et al Circ 2007

19
Regional STEMI System for PCIMayo Clinic May 2004 - Dec 2006; N= 597
71
116
25
188
278
103
7.2 7.1 3.70
50
100
150
200
250
PPCI Ctr Transfer PCI Regional Lytic
Door 1-Rx (min)
Sx-Rx (min)
30 Day Mortality (%)
Ting et al Circ 2007
N=258 N=105 N=131

20
RACE Centers (N=65) and Regions
10 PCI centers
16 Transfer for PCI
28 Lytics
11 Mixed
Asheville
Winston-Salem Durham-Chapel Hill-
Greensboro
Charlotte
East Carolina
Each non-PCI center was assessed for
reperfusion designation based on resources,
transfer ability, and transfer time to PCI center
Jollis. JAMA 2007;298:2371-2380.

21
STEMI Treatment Time in RACE Hospitals
85
165
120
35
90
74
128
71
29
108
0
20
40
60
80
100
120
140
160
180
200
All Direct Transfer Door in to
Door out
D2N
Preintervention
Postintervention
Me
dia
n, M
inu
tes
P<0.001
P<0.001
P<0.001
Jollis. JAMA 2007;298:2371-2380.
P<0.001
P<0.002
First Door-to-Device at PCI Hosp Mx at non PCI Hosp

22
Improving the System of Care for STEMI Patients
STEMI Chain of Survival

23
Road Map for Transformation of Road Map for Transformation of
Reperfusion Therapy for STEMIReperfusion Therapy for STEMI
ACC D2B Alliance
AHA Mission:Lifeline
How Should Care Be Delivered ?
Measurement + accountability
System redesign
Spread of interventions
Research in above domains
3
ACTION Registry®-GWTG™
Who benefits ?
Outcomes Research
Effectiveness Research
Health Services Research
2
RCTs of Lysis vs PCI
What care works ?
Clinical Efficacy Research1
Reperfusion for STEMIKey AspectsStep
Dougherty D, Conway PH. JAMA 2008;299:2319-21 Antman EM JACC 2008

24
• National initiative
• Improve quality of care + outcomes in STEMI
• Improve health care system readiness and
response to STEMI.
Jacobs et al Circ. 116: 217, 2007

25
Improving Access to Improving Access to TimelyTimely Care for STEMICare for STEMI
Jacobs et al Circ. 116: 217, 2007
THE IDEAL SYSTEMTHE IDEAL SYSTEM

26
PCI
capable
Not PCI
capable
Patient
EMS
ED
STEMI
Referral
Payers
Policy
Makers STEMI
Receiving
NHAAP
CDC NAEMT
NAEMSP
NASEMSO
NEMSIS
ACEP
American Ambulance Assn
AACCN
ENA
ACTION/GWTG
NRHA
SCAI
Society of
Chest Pain
Centers
ACP
STS
AACCN
ENA
CMSAetna
UnitedHealth Networks
CMS
Center of
Care
Adapted from Jacobs et al. Circulation. 2007;116:217-230.
Evaluation
& Outcomes
AHRQ
FDA
JCAHO
Mission: Lifeline:Mission: Lifeline: Collaborating OrganizationsCollaborating Organizations

27
ECC
Task Force
Model Evaluation
Task Force
Advisory
Working Group
EMSEMS Point ofPoint of
EntryEntry
• Survey of Existing Systems
Administration
Locale (Urban, Rural)
Processes of Care
Financial Considerations
• Construct Templates for
System Development to Be
Used by Other Providers
Circ 116: e64, 2007Circ 116: e64, 2007
28
Circ 116: e64, 2007Circ 116: e64, 2007
Evaluation of Systems for STEMI Care
Structural Measures
EMS: staff, equipment, protocols
ED: staff, protocols, one-contact hotline
PPCI Ctr: 24/7, volume/experience, ?SOS
QA: feedback system, oversight comm.

29
Improving the System of Care for STEMI Patients
System Assessment & Improvement---on line surveys
29

30
Patient Flow Through STEMI System and Data CollectionPatient Flow Through STEMI System and Data Collection
STEMI
PT
Hosp A
Non PCI
Hosp B
PCI
1
2 3
4
5 6
911-EMSHybrid
NEMSIS
M:L EMS
M:L Bridging Form ACTION-GWTG
NCDR-PCI
Long Term Follow up--? sources
Pt self-
transport to
non PCI hosp
Pt self-
transport to PCI
hosp
Interhospital
transfer
Hosp C
Non PCI
CMS Data Only
7
Hosp D
PCI
Not participating in
ACTION/GWTG
CMS or NCDR Cath
PCI only
8

31
Dept of HHS Response to IOM Reports on Emergency Care:Dept of HHS Response to IOM Reports on Emergency Care:
1.1. Creation of lead agency within HHS to coordinate Creation of lead agency within HHS to coordinate
Emergency CareEmergency Care
2.2. Coordinate with AHRQ,Coordinate with AHRQ, FDA, CDC, NIH to promote FDA, CDC, NIH to promote
systems based Emergency Care researchsystems based Emergency Care research
3.3. Promote regionalization of Emergency CarePromote regionalization of Emergency Care
www.www.hhshhs..govgov

32

33
Potential Geometry ofPotential Geometry of
STEMI NetworksSTEMI Networks
Single Hub (PCI) w
Multiple Spokes
Multiple Hubs (PCI) w
Multiple Spokes
Intregrated Hubs (PCI)
and Spokes
Adapted from:
Exploring The Geometry
of Treatment Networks
Salanti Ann Int Med 148: 544, 2008
34
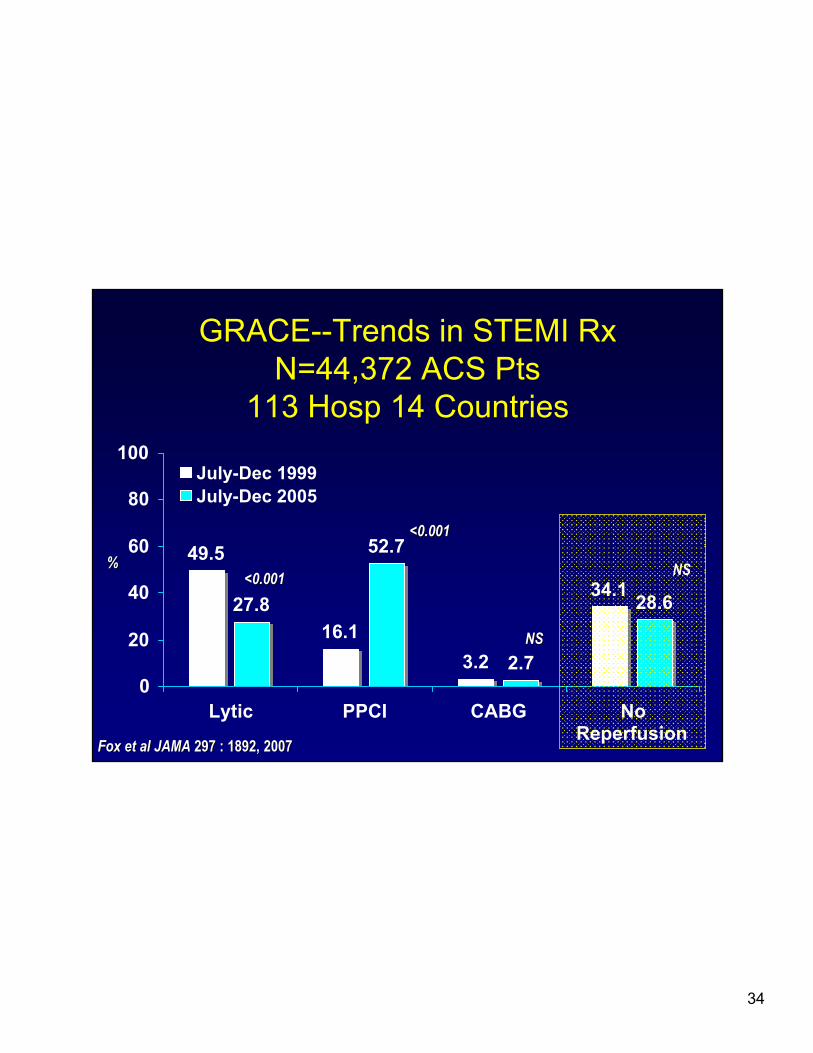
GRACE--Trends in STEMI Rx
N=44,372 ACS Pts
113 Hosp 14 Countries
49.5
16.1
3.2
34.127.8
52.7
2.7
28.6
0
20
40
60
80
100
Lytic PPCI CABG NoReperfusion
July-Dec 1999
July-Dec 2005
%%<0.001<0.001
<0.001<0.001
NSNS
NSNS
Fox et al JAMAFox et al JAMA 297 : 1892, 2007297 : 1892, 2007
35
Reperfusion Strategies for STEMI Reperfusion Strategies for STEMI
Widely availableWidely available
Quickly administeredQuickly administered
Less effectiveLess effective
Bleeding riskBleeding risk
Limited availabilityLimited availability
Treatment delay Treatment delay
More effectiveMore effective
Bleeding risk lowerBleeding risk lower
PharmacologicPharmacologic PCIPCI


















