UCLA Health Sepsis Program Health...UCLA’s Sepsis Program comprises a comprehensive infrastructure...
2
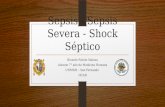
UCLA HEALTH High Reliability Organization & Sepsis Program UCLA Health Key Findings Of all patient deaths at UCLA, Septic patients account for 25.34%, and Septic Shock pa- tients have an average mortality rate of 40% Septic patients have >300% of dying com- pared to other patients Septic patients generate >1000 excess bed days per year On average 20% of septic patients readmit Septic patients stay 20% longer than other patients Bundle Compliance (CMS SEP-1) RRMC 25% SMMC 48% 27% of clinical surveillance encounters are related to Sepsis and 30% of inital deteriora- tion Greater than 75% of Sepsis patients present in the Emergency Department at SM and 64% at RR 2/5 patients who are diagnosed with severe sepsis or septic shock will die before leaving the hospital A comprehensive sepsis infastructure Santa Monica ED Bundle Compliance im- proved ~25% from 2015-2017 Repeat Lactate compliance increased from 71% at SM and 87% at RR in Jan ‘17 to 100% in March ’17 90% of nurses screen their patients upon admission to the unit UCLA Health Best Practices UCLA’s Sepsis Program comprises a comprehensive infrastructure aligned with “High Reliability” organizational principles. The program uses an interdisciplinary approach to improve overall patient outcomes through sustainable actions. The program uses current education and outreach, care connect improvements, clinical champions, and data analysis to improve overall care of the septic shock patient. The goal of the program is to recognize and treat Severe Sepsis and Septic Shock early and thereby decrease Sepsis related mortality rates and improve patient outcomes across the UCLA Health System. Research Program Integration Joint Commission Sepsis Certified Center Integration of Clincial Documentation Teams into Sepsis Improvement Complete infusion of sepsis language in clinical practice Barriers Alignment with Care Connect/ISS Dedicated resources for data analytics Systematic organizational support Consensus about treatment of septic shock/- severe sepsis treatment among Physician groups Process & Protocols Data Culture Accountability No Sepsis Guidelines Sepsis Screen- ings and Bun- dles Integrated Order Sets and Protocols Backup & Redu- dant Systems No way to measure errors Event Reports & Sepsis Dash- boards Sepsis process and outcome benchmarking Continous Re- al-Time Sepsis Sur- veillance Trial and Error Defining Roles in Sepsis Collective Drive Sepsis Day Preoccupation with Sepsis Failure Individual Au- tonomy Sepsis Safety & Quality Teams Centralized Sepsis Control Organizational Awareness 2018 GOALS 1. Standardize UCLA definition for Sepsis that integrates definitions for Sepsis 2.0, 3.0 and includes SOFA and qSOFA using ICD-10. 2. Develop unit based and service line specific dashboards (Include Time of Presentation). 3. Implement evidence based and highly reliable innovations in Care Connect to support clinical de- cision making. 4. Ensure appropriate resources to support the sepsis program, i.e. Full time sepsis coordinator 5. Improve compliance with CMS (SEP-1) core measure. Track & develop learning system from fallouts 6. Refine emergency response for sepsis, and integrate the surveillance team initatives ie. code sepsis 7. Research and complete a gap analysis on the Joint Commission certified sepsis center accreditation. Areas of Innovations and Future Opportunities: Sepsis Continuum of Care Implemented In Progress Future Opportunities EMS & Community Floor Sepsis RN (SM) & STAR (RR) Nurse Driven Protocol Nurse Driven Protocol Emergency Department SM RN BPA RRT RN Screening Tool Sepsis Audit Graph RN Screening Tool Dynamic RN tool Code Sepsis RN Screening Tool Dynamic RN tool MD BPA MD BPA ED to IP SBAR MD Orderset & Panels MD Orderset & Panels ED to IP SBAR ICU MD Ordersets Repeat Lactate MD BPA Alerts for Palliative Care RN BPA EMS Screening EMS to ED Standard 2012 Simulation Center Collaboration (MDs/RNs) Care Connect go-live Adult MD order set LIVE in Care Connect Nursing Protocol developed System level nursing champions MD order sets developed Sepsis Website Launched Adult sepsis screening tool launched Second Annual Sepsis Day QMS Manager hired for sepsis Sepsis Project Manager hired SRRMC Sepsis Coordinator hired RN mandatory education ( yearly) ED sepsis screening tool launched (CView) Adult Sepsis MD order set developed Sepsis champions model defined QMP database for sepsis cases Sepsis Lab panel created First Annual Sepsis Day Dr. Dan Uslan – named MD Champion 2013 2014 2015 2016 2017 New Definitions: Sepsis 3.0/SOFA ProCESS, ARISE, ProMISe Studies 2001 2003 2008 Early-Goal Directed Therapy Surviving Sepsis Campaign National Quality Forum Affordable Care Act Innovation: BPA pilot launched and ended Innovation: ED code sepsis page launched Innovation:MEWS - RRMC pilot 3rd Annual Sepsis Day ProCESS, ARISE, ProMISe Studies SEP-1 (CMS) Follow-up/MD fallout letter process update Clinical Triggers pilot SMH Dr. Steven Chang – interim Sepsis MD Dr. Tischa Wong – Sepsis Physician champion Sepsis module for all 1st year residents 4th Annual Sepsis Day Innovation: Parahealth Pilot RRMC Clinical Surveillance Team – pilot Dr. Russ Kerbel – Sepsis Physician Champion RRMC Clinical Surveillance Team –LIVE 24/7 RRMC Revised RRT team – LIVE 3/2017 SMH Sepsis RN hired New Website launched Innovation: Repeat lactate available Innovation: Sepsis IV fluid bolus order Innovation: Code Sepsis Inpatient (System) Value-Based Purchasing ? Hospital Compare 2018 National UCLA Long Term Goals UCLA Health Sepsis Program
Transcript of UCLA Health Sepsis Program Health...UCLA’s Sepsis Program comprises a comprehensive infrastructure...
UCLA HEALTH High Reliability Organization & Sepsis Program
UCLA Health Key FindingsOf all patient deaths at UCLA, Septic patients account for 25.34%, and Septic Shock pa-tients have an average mortality rate of 40%
Septic patients have >300% of dying com-pared to other patients
Septic patients generate >1000 excess bed days per year
On average 20% of septic patients readmit Septic patients stay 20% longer than other patients
Bundle Compliance (CMS SEP-1)RRMC 25% SMMC 48%
27% of clinical surveillance encounters are related to Sepsis and 30% of inital deteriora-tion
Greater than 75% of Sepsis patients present in the Emergency Department at SM and 64% at RR
2/5 patients who are diagnosed with severe sepsis or septic shock will die before leaving the hospital
A comprehensive sepsis infastructure
Santa Monica ED Bundle Compliance im-proved ~25% from 2015-2017
Repeat Lactate compliance increased from 71% at SM and 87% at RR in Jan ‘17 to 100% in March ’17
90% of nurses screen their patients upon admission to the unit
UCLA Health Best Practices
UCLA’s Sepsis Program comprises a comprehensive infrastructure aligned with “High Reliability” organizational principles. The program uses an interdisciplinary approach to improve overall patient outcomes through sustainable actions. The program uses current education and outreach, care connect improvements, clinical champions, and data analysis to improve overall care of the septic shock patient.
The goal of the program is to recognize and treat Severe Sepsis and Septic Shock early and thereby decrease Sepsis related mortality rates and improve patient outcomes across the UCLA Health System.
Research Program Integration
Joint Commission Sepsis Certi�ed Center
Integration of Clincial Documentation Teams into Sepsis Improvement
Complete infusion of sepsis language in clinical practice
BarriersAlignment with Care Connect/ISS
Dedicated resources for data analytics
Systematic organizational support
Consensus about treatment of septic shock/-severe sepsis treatment among Physician groups
Process & Protocols
Data
Culture
Accountability
No Sepsis Guidelines
Sepsis Screen-ings and Bun-dles
Integrated Order Sets and Protocols
Backup & Redu-dant Systems
No way to measure errors
Event Reports & Sepsis Dash-boards
Sepsis process and outcome benchmarking
Continous Re-al-Time Sepsis Sur-veillance
Trial and Error De�ning Roles in Sepsis
Collective Drive Sepsis Day
Preoccupation with Sepsis Failure
Individual Au-tonomy
Sepsis Safety & Quality Teams
Centralized Sepsis Control
Organizational Awareness
2018 GOALS 1. Standardize UCLA de�nition for Sepsis that integrates de�nitions for Sepsis 2.0, 3.0 and includes SOFA and qSOFA using ICD-10. 2. Develop unit based and service line speci�c dashboards (Include Time of Presentation). 3. Implement evidence based and highly reliable innovations in Care Connect to support clinical de-cision making.
4. Ensure appropriate resources to support the sepsis program, i.e. Full time sepsis coordinator
5. Improve compliance with CMS (SEP-1) core measure. Track & develop learning system from fallouts
6. Re�ne emergency response for sepsis, and integrate the surveillance team initatives ie. code sepsis
7. Research and complete a gap analysis on the Joint Commission certi�ed sepsis center accreditation.
Areas of Innovations and Future Opportunities: Sepsis Continuum of Care
Implemented
In Progress
Future Opportunities
EMS & Community Floor
Sepsis RN (SM) & STAR (RR)
Nurse Driven Protocol Nurse Driven Protocol
Emergency Department
SM RN BPA RRT
RN Screening Tool
Sepsis Audit Graph RN Screening ToolDynamic RN tool
Code Sepsis
RN Screening Tool Dynamic RN toolMD BPA
MD BPA
ED to IP SBAR
MD Orderset & Panels MD Orderset & Panels
ED to IP SBAR
ICU
MD Ordersets
Repeat Lactate
MD BPAAlerts for Palliative Care
RN BPA
EMS Screening
EMS to ED Standard
2012
Simulation Center Collaboration (MDs/RNs)
Care Connect go-live
Adult MD order set LIVE in Care Connect
Nursing Protocol developed
System level nursing champions
MD order sets developed
Sepsis Website Launched
Adult sepsis screening tool launched
Second Annual Sepsis Day
QMS Manager hired for sepsis
Sepsis Project Manager hired
SRRMC Sepsis Coordinator hired
RN mandatory education ( yearly)
ED sepsis screening tool launched (CView)
Adult Sepsis MD order set developed
Sepsis champions model de�ned
QMP database for sepsis cases
Sepsis Lab panel created
First Annual Sepsis Day
Dr. Dan Uslan – named MD Champion
2013
2014
2015
2016
2017
New De�nitions: Sepsis 3.0/SOFA
ProCESS, ARISE, ProMISe Studies
2001
2003
2008
Early-Goal Directed Therapy
Surviving Sepsis Campaign
National Quality Forum
A�ordable Care Act
Innovation: BPA pilot launched and ended
Innovation: ED code sepsis page launched
Innovation:MEWS - RRMC pilot
3rd Annual Sepsis Day
ProCESS, ARISE, ProMISe Studies
SEP-1 (CMS)
Follow-up/MD fallout letter process update
Clinical Triggers pilot SMH
Dr. Steven Chang – interim Sepsis MD
Dr. Tischa Wong – Sepsis Physician champion
Sepsis module for all 1st year residents
4th Annual Sepsis Day
Innovation: Parahealth Pilot
RRMC Clinical Surveillance Team – pilot
Dr. Russ Kerbel – Sepsis Physician Champion
RRMC Clinical Surveillance Team –LIVE 24/7
RRMC Revised RRT team – LIVE 3/2017
SMH Sepsis RN hired
New Website launched
Innovation: Repeat lactate available
Innovation: Sepsis IV �uid bolus order
Innovation: Code Sepsis Inpatient (System)
Value-Based Purchasing ?
Hospital Compare
2018
NationalUCLA
Long Term Goals
UCLA Health Sepsis Program
Project Coordinator
Summer Maxwell
ValU Support
Sabrina Adelaine
Business Owner
Kim Ternavan
Physician Champion
Russ Kerbel
Executive Committee
Data Development
Meng Wei
Education & Outreach
Lee Galuska
Information Technology
Carson Del Greco/Lisa Harrison
Process Improvement
Sabrina Adelaine
Physician Champions
Russ Kerbel
Nursing Champions
Yuhan Kao /Mary Lawanson-
Nichols
Abstractor Specialists
Trudy Rhodes
Pediatrics
Lynne McCullough/
Kerry Gold
Mortality Sepsis
MOVERS
Pt meets criteria for Severe Sepsis & /or Septic Shock (Time of Presentation or TOP)
Document POSITIVE severe sepsis &/or
septic shock screen in CareConnect
Initiate Severe Sepsis & /or
Septic Shock Bundle (per adult sepsis Nursing protocol & core measure requirements)
NURSES
Initial Lactate Level (per nursing protocol, no co-sign required)
Blood Cultures X 2 sets
(per nursing protocol, no co-sign required)
*NOTE: 4 bottles total; minimum of 8-10mL
per bottle
Administer IV broad spectrum antibiotic or other approved
combination of antibiotics
(RN to contact MD/NP/PA to request orders for Abx)
COMPLETE WITHIN 1 HOUR (max) Following initial time of presentation (TOP)
If hypotension persists within 1hour of
completing 30mL/kg �uid bolus, continue
interventions. If pt. no longer hypotensive
after 30ml/kg, STOP!
If initial lactate > 18mg/dl
redraw within 3 hours after
initial lactate
SEVERE SEPSIS & SEPTIC SHOCK: EARLY MANAGEMENT BUNDLE
Changes & Updates highlighted in REDREV 11/24/2015
RN RN &/or MD/NP/PA
NURSES
NURSES
MD/NP/PA
REPEAT serum Lactate level per nursing
protocol if most recent lactate level
>18mg/dL
Initiate VASOPRESSORS (contact MD/NP/PA for orders )
Vasopressors to be initiated for hypotension unresponsive to fluid
bolus of 30mL/kg
COMPLETE WITHIN 6 HOURS (max)Following initial time of presentation (TOP)
Repeat volume & tissue perfusion assessment including (ALL must be documented by MD/NP/PA): � Complete Vital Signs, AND� Cardiopulmonary exam, AND� Capillary refill evaluation, AND� Peripheral pulse evaluation, AND � Skin exam - OR -Any two of the following:� Central venous pressure (CVP) measurement � Central venous oxygen (sCVO2) measurement � Bedside cardiovascular ultrasound� Passive leg raise or fluid challenge 500mL NS/LR (min.)
ANDNURSES &/or
If INITIAL Lactate is ≥36mg/dL, MUST
perform repeat volume & tissue
perfusion assessment (regardless of repeatLactate level results )
*RN to contact MD/NP/PA to request orders for IV Abx & �uid bolus*
IF SBP <90 or >40 below baseline or MAP <65
-OR- Initial Lactate level
≥36mg/dL------------------
Total bolus minimum of 30mL/kg must complete
in < 3hrs from TOP;Administer only
0.9% NS or LR �uids
1 HOUR
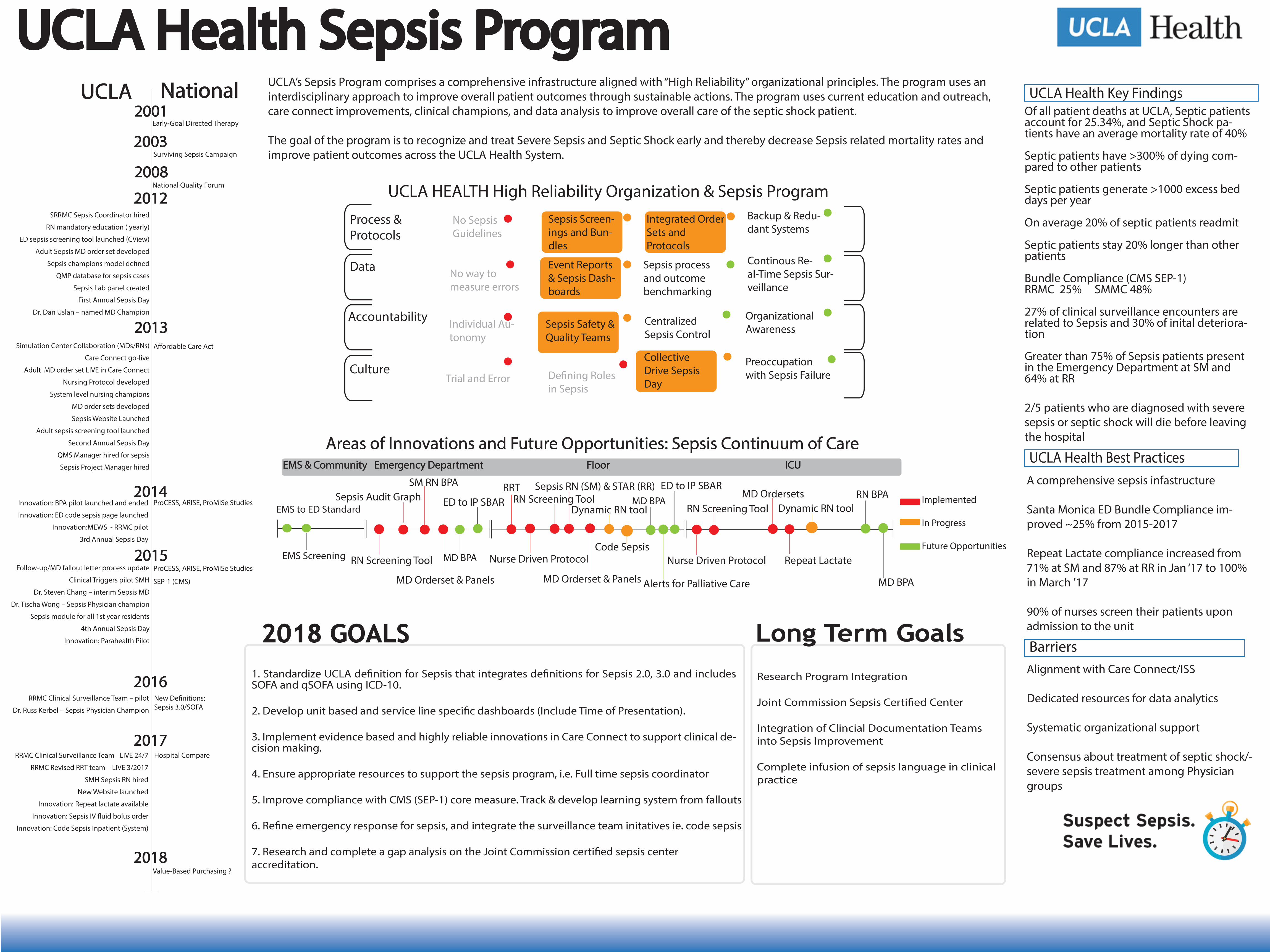
Sepsis Program Infastructure
Sepsis Bundle Timeline
Current Data for Sepsissource: Vizient & Tableau