From Localization to Connectivity and... Lei Sheu 1/11/2011.

lable at ScienceDirect
Tzu Chi Medical Journal 28 (2016) 121e123
brought to you by COREView metadata, citation and similar papers at core.ac.uk
provided by Elsevier - Publisher Connector
Contents lists avai
Tzu Chi Medical Journal
journal homepage: www.tzuchimedjnl .com
Case Report
Insidious malignant triton tumor of the chest wall with lateflare-up
Jeng-Yuan Wu a, b, *, Lai-Fa Sheu b, c, Chao-Yuan Yao d
a Department of Thoracic Surgery, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwanb School of Medicine, Tzu Chi University, Hualien, Taiwanc Department of Pathology, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwand Department of HematologyeOncology, Taichung Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Taichung, Taiwan
a r t i c l e i n f o
Article history:Received 27 August 2014Received in revised form22 October 2014Accepted 5 November 2014Available online 19 December 2014
Keywords:Chest wall tumorMalignant peripheral nerve sheath tumorMalignant triton tumor
Conflict of interest: none.* Corresponding author. Department of Thoracic
Hospital, Buddhist Tzu Chi Medical Foundation, 88, SecDistrict, Taichung, Taiwan. Tel.: þ886 4 36060666x30
E-mail address: [email protected] (J.-Y. Wu
http://dx.doi.org/10.1016/j.tcmj.2014.11.0011016-3190/Copyright © 2014, Buddhist Compassion Re(http://creativecommons.org/licenses/by-nc-nd/4.0/).
a b s t r a c t
Malignant triton tumor is a rare malignant peripheral nerve sheath tumor with rhabdomyoblastic dif-ferentiation. Most of these tumors are located in the head, neck, and extremities, and about half of casesare associated with neurofibromatosis type 1 featuring cafe-au-lait spots or cutaneous neurofibromas.We present a 76-year-old man with an insidious chest wall tumor with late progressive painfulenlargement and pleural and pulmonary involvement. Complete resection of the affected thoracic wall aswell as single separate lesions in the parietal pleura and left upper lung was carried out. The pathologicalexamination confirmed that it was a malignant triton tumor. The patient received adjuvant chemo-radiotherapy but eventually succumbed to disease relapse and distant metastases 6 months after thesurgery.Copyright © 2014, Buddhist Compassion Relief Tzu Chi Foundation. Published by Elsevier Taiwan LLC.
This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
1. Introduction
Malignant triton tumor (MTT) is rare and highly aggressive,and tends to develop early local recurrence and distant metasta-ses. Immunohistochemistry (IHC) showing malignant schwan-noma cells coexisting with rhabdomyoblasts confirms thediagnosis. Aggressive surgical management is of crucial impor-tance in the management of MTT, with adjuvant chemotherapyand/or radiotherapy being effective in sporadic cases. Here wereport an unusual presentation of an MTT in the chest wall of anelderly man who had no skin lesions or family history of neuro-fibromatosis. The case is unique in terms of its slow disease pro-gression and late flare-up of the tumor, leading to an initial clinicalimpression that did not favor MTT. The patient died after en blocresection followed by adjuvant chemoradiotherapy because ofongoing disease exacerbation with poor response to multi-modality treatment.
Surgery, Taichung Tzu Chition 1, Fongsing Road, Tanzih30; fax: þ886 4 36065928.).
lief Tzu Chi Foundation. Published
2. Case Report
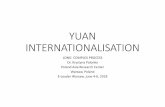
A 76-year-old otherwise healthy man presented with a large,firm mass on his left chest wall for more than 20 years. It hadenlarged progressively over the past 2 years and chest paindeveloped 1 month prior to admission. The physical examinationrevealed an ovoid 7 cm� 4.5 cm bony tumor beneath the pectoralismajor muscle. Chest computed tomography (CT) revealed a het-erogeneous tumor occupying the chest wall including the fourth rib(Fig. 1A), a single small nodular lesion over the left upper lung(Fig. 1B) and right lower lung, and focal parietal pleural thickeningin the left upper thorax. A bone scan showed Technetium-99mmethylene diphosphonate (Tc-99m MDP)-avid lesions of an unde-termined nature in the left fourth rib and right upper femur. Hereceived CT-guided fine-needle biopsy of the chest wall tumor thatpathology reported as fibromatosis. The patient underwent wideexcision of the affected chest wall with syntheticmesh replacementas well as resection of the nodules in the pleura and left upper lobe.Histopathology displayed hypercellularity, cells with spindle-shaped nuclei arrayed in a fascicular pattern, nuclear pleomor-phism, brisk mitotic activity, and areas of necrosis. There weremany rhabdomyoblasts with eosinophilic cytoplasm (Fig. 2A). IHCdemonstrated positivity of the tumor cells for anti-S100 (Fig. 2B)and antivimentin stains (Fig. 2C), but CK7, SMA, and TTF-1
by Elsevier Taiwan LLC. This is an open access article under the CC BY-NC-ND license

Fig. 1. Chest computed tomography (CT) scan demonstrating (A) a heterogeneous softtissue mass with calcification (arrow) involving the anterior segment of the left fourthrib and (B) a nodular lesion about 2 cm in diameter (arrow) in the left upper lobe.
Fig. 2. Pathology showing (A) numerous pleomorphic rhabdomyoblasts containing eosinophmalignant triton tumor (hematoxylin and eosin, �300). (B) Anti-S100 (�200) and (C) antiv
J.-Y. Wu et al. / Tzu Chi Medical Journal 28 (2016) 121e123122
immunostains were negative. Both morphological findings andimmunophenotypes were compatible with malignant peripheralnerve sheath tumor with rhabdomyoblastic differentiation, whichconfirmed the diagnosis of MTT. Postoperatively, the patientreceived three cycles of chemotherapy with cisplatin and etoposideand concurrent radiotherapy to the involved thoracic wall, at a totaldose of 7000 cGy in 35 fractions. Nevertheless, local relapse andlung-to-lung, nodal, and spinal metastases occurred subsequently,and he died of pneumonia and respiratory failure in relation toadjuvant chemoradiotherapy 6 months after the operation.
3. Discussion
MTT is a very rare but highly aggressive subtype of malignantperipheral nerve sheath tumor with rhabdomyoblastic differenti-ation. About one-third of MTTs are located in the head and neckregions [1]. The mean age of patients is about 30 years with anequal sex distribution. MTT coexists with neurofibromatosis type 1(NF-1) in 44e69% of cases, but can also occur sporadically or afterradiotherapy. When associated with NF-1, MTT tends to occur at ayoung age in males. Clinical symptoms are nonspecific and aregenerally related to a rapidly enlarging mass that invades or im-poses pressure on adjacent structures. Image studies usuallydelineate a picture of soft tissue sarcoma. Pathological examinationand IHC are essential to establish the diagnosis. The outcome ofpatients is very poor with 5-year survival rates of 11e15% and highrates of metastases (48%) and local recurrence (43%). Completesurgical resection is the most effective treatment, and adjuvanttherapymay be of value in individual patients [2e5]. The location ofthe tumor is also considered a key factor in the prognosis; those inthe extremities, head, and neck have a better prognosis than thosein the retroperitoneum, buttock, and trunk [3]. In our elderly pa-tient, who presented without NF-1, the rare location and bizarrebehavior of the chest wall MTT with its insidious course, and the
ilic cytoplasm (arrow) embedded in spindle cells with a fascicular growth pattern in aimentin (�200) immunostains of the tumor cells are positive.

J.-Y. Wu et al. / Tzu Chi Medical Journal 28 (2016) 121e123 123
late development of chest pain because of unexpectedly rapidgrowth and rib invasion, complicated by pleural and pulmonaryinvolvement, are seldom seen with this tumor. We believe that thelong-standing, asymptomatic chest wall lesion was possibly pre-cancerous and the late flare-up accelerated its malignant clinicalcourse.
The differential diagnosis of MTT consists of a large variety ofneoplasms such as rhabdomyosarcoma, leiomyosarcoma, fibrosar-coma, malignant fibrous histiocytoma, monophasic synovial sar-coma, ectomesenchymoma, neurofibroma, benign triton tumor,and hemangiopericytoma [4]. Chest CT in our patient showedmainly a chest wall soft tissue tumor containing conglomerated,amorphous calcifications of various sizes coupled with eccentriccalcification of lamellar distribution, a particular pattern not spec-ified in those MTTs reported in the literature. Comparable featuresof scattered calcifications with sunburst or lamellated periostealreactions are associated with osteosarcoma or chondrosarcoma,but infrequently with other sarcomatous lesions. Preoperativediagnostic procedures such as sonography and CT-guided fine-needle aspiration or biopsy are often used, as in this case. However,needle biopsy and incisional biopsy are not reliable enough toestablish a conclusive result in such circumstances [4]. Microscopicexamination along with IHC indicating rhabdomyoblasts amongmalignant Schwann cells in a tumor arising from a peripheral nerveverified by immunostaining with S-100 protein is essential for anaccurate diagnosis of MTT [6]. The course of illness and imagefindings in our patient indicated a likely diagnosis of chest wallosteosarcoma or chondrosarcoma; however, characteristic histo-pathological findings as well as positivity of the resected specimento anti-S100 and antivimentin stains confirmed the diagnosis.
Treatment strategies for MTT include surgical resection, neo-adjuvant and adjuvant chemotherapy, and irradiation. Completetumor resection appears to be associated with an improved chanceof survival, decreased rates of local recurrence and metastasis, anda better response to adjuvant therapies than that in patientswithout resection [2]. Although the role of adjuvant therapy is notwell defined and no treatment guidelines have been establishedbecause of the rarity of MTT, radical excision with adjuvant
radiotherapy may achieve a satisfactory outcome [1,7]. In our pa-tient, aggressive management was undertaken, including wideexcision of the chest wall tumor, and lung and pleural nodules andpostoperative chemoradiotherapy. Although ensuing distal metas-tases led to a fatal outcome, we consider the operation itself wasstill applicable to relieve symptoms primarily caused by theenlarging chest wall mass. In fact, MTT has a poor prognosis owingto its aggressive biological behavior. As in this case, most patientsdie within months even after multimodal therapy because of dis-ease progression and treatment-related events.
MTT should be regarded as a distinct clinical entity associatedwith a high incidence of local recurrence and distant metastases.IHC showing nerve sheath differentiation with rhabdomyoblasticcells confirms the diagnosis. Early diagnosis and radical excisioncoupled with adjuvant chemoradiation seem to yield a better resultthan conservative management. However, the therapeutic planshould be individualized, taking into account the location and sizeof the primary tumor, curative or palliative intent, and the patient'sperformance status. Furthermore, rapid clinical deterioration anddeath often occur despite multidisciplinary management.
References
[1] Tian L, Shang HT, Bilal S, Li YP, Feng ZH, Lei DL, et al. Treatment of malignanttriton tumor in zygomatic region. J Craniofac Surg 2012;23:e265e8.
[2] Li Z, Xiang J, Yan S, Gao F, Zheng S. Malignant triton tumor of the retro-peritoneum: a case report and review of the literature. World J Surg Oncol2012;10:96e101.
[3] Yakulis R, Manack L, Murphy Jr AI. Postradiation malignant triton tumor. A casereport and review of the literature. Arch Pathol Lab Med 1996;120:541e8.
[4] Kamperis E, Barbetakis N, Asteriou C, Kleontas A, Christoforidou V. Malignanttriton tumor of the chest wall invading the lung. A case report and literaturereview. Hippokratia 2013;17:277e80.
[5] McConnell YJ, Giacomantonio CA. Malignant triton tumorsdcomplete surgicalresection and adjuvant radiotherapy associated with improved survival. J SurgOncol 2012;106:51e6.
[6] Kiryu H, Urabe H. Malignant Triton tumor. A case with protean histopatho-logical patterns. Am J Dermatopathol 1992;14:255e62.
[7] Lang-Lazdunski L, Pons F, Jancovici R. Malignant “Triton” tumor of the posteriormediastinum: prolonged survival after staged resection. Ann Thorac Surg2003;75:1645e8.