Type A Accident Investigation of the June 21, 2001 Drilling Rig ...
62
August 2001 Type A Accident Investigation of the June 21, 2001 Office of Environment, Safety and Health Oversight Environment, Safety and Health Drilling Rig Operator Injury at the Fermi National Accelerator Laboratory
Transcript of Type A Accident Investigation of the June 21, 2001 Drilling Rig ...
August 2001
Type A Accident Investigationof the June 21, 2001
Office of Environment, Safety and Health OversightEnvironment, Safety and Health
Drilling Rig Operator Injury at the Fermi National Accelerator Laboratory

OV
ER
SIG
HT
Table of Contents
EXECUTIVE SUMMARY .................................................................. 1
1.0 INTRODUCTION ...................................................................... 71.1 Background ....................................................................... 71.2 Facility Description............................................................ 71.3 Scope, Purpose, and Methodology.................................... 8
2.0 THE ACCIDENT ..................................................................... 102.1 Background and Accident Description ........................... 10
2.1.1 Accident Overview................................................ 102.1.2 Background ........................................................... 102.1.3 Accident Description ............................................. 122.1.4 Engineering Evaluation of the Failed Components13
2.2 Emergency Response and Medical Treatment ............... 132.3 Investigative Readiness and Accident
Scene Preservation.......................................................... 153.0 ACCIDENT FACTS AND ANALYSIS .................................... 16
3.1 Physical Hazards, Controls, and Related Factors ........... 163.1.1 Define the Scope of Work ...................................... 163.1.2 Hazard Analysis ..................................................... 183.1.3 Develop and Implement Controls ......................... 203.1.4 Perform Work Within Controls ............................. 243.1.5 Feedback and Improvement ................................. 243.1.6 Management Systems ........................................... 31
3.2 Barrier Analysis ............................................................... 363.3 Change Analysis .............................................................. 363.4 Causal Factors Analysis .................................................. 36
4.0 JUDGMENTS OF NEED ......................................................... 415.0 BOARD SIGNATURES ........................................................... 446.0 BOARD MEMBERS, ADVISORS, AND STAFF ................... 45
APPENDIX A – BOARD APPOINTMENT MEMORANDUM ..... 46APPENDIX B – DRILL RIG ACCIDENT EVENT
CHRONOLOGY .................................................... 47APPENDIX C – EVENTS AND CAUSAL FACTORS CHART ...... 49APPENDIX D – BARRIER ANALYSIS ........................................... 53
List of Tables, Figures, and Exhibits ................................................ 58
Abbreviations Used in This Report ....................... Inside Back Cover


1
The Accident
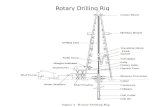
On June 21, 2001, at approximately 9:40 A.M.,a construction sub-tier contractor employee (the“Operator”) at the Fermi National AcceleratorLaboratory (Fermilab) received serious head injuriesrequiring hospitalization when he was struck by partof the drilling rig (a “tong”) that he was operating.The equipment involved in the accident, known asa tong, was a 32-inch steel bar with a handleessentially used as a pipe wrench to connect anddisconnect drill pipe. The accident occurred whena welded connection in the hydraulic system usedto apply force to the tong failed, as the two-mancrew was removing lower sections of the drillassembly. The drill rig Helper indicated that, at thetime of weld failure, the Operator was standing withhis head near the tong and operating the hydrauliccylinder to disconnect a drill section joint. Basedon an analysis of the evidence, the Board concludedthat the weld failure released tension on a wire ropesling attached to the tong; the tong recoiled towardthe Operator and struck him in the head. Failureof the weld was determined to be the direct causeof the accident. The Operator remained hospitalizeduntil July 9, 2001.
On June 25, 2001, the Acting Assistant Secre-tary for Environment, Safety and Health, U.S.Department of Energy (DOE), upon the recom-mendation of the DOE Chicago Operations Office,appointed a Type A Accident Investigation Boardto analyze causal factors, identify root causes, anddetermine judgments of need to preclude similaraccidents in the future. The Board arrived on sitetwo days later and completed the investigation inJuly 2001.
Background
Fermilab is the nation’s largest particleaccelerator laboratory and lies 30 miles west ofChicago, Illinois. Fermilab operates under theprogrammatic direction of the DOE Headquarters’Office of Science. The DOE Fermi Area Office,under the DOE Chicago Operations Office,
oversees site contractor activities. UniversityResearch Associates, Inc., a consortium ofuniversities, manages and operates the site for DOE.
The injured Operator was an employee of theLayne-Western Company of Aurora, Illinois. Theinjury occurred at the Neutrinos at the Main InjectorProject, whose construction includes tunnel boringand shaft drilling activities. Fermilab employedthe S. A. Healy Company of Lombard, Illinois, toperform this underground construction work. S. A.Healy subcontracted with Layne-Western to drillsix holes for air ventilation and survey risers. TheLayne-Western crew was working on the fifth shaftat the time of the accident using a drilling rig thatwas manufactured in 1969.
On March 2, 1999, the drilling crew performedan “in-field” welding activity to repair a failure ofthe eyebolt-to-piston rod connection. The weldattached the eyebolt to the hydraulic cylinder pistonrod that was used to apply force to the tong. Beforethe repair, the eyebolt apparently threaded directlyinto the end of the piston rod, and this threadedconnection had evidently failed. At the time of theaccident, one end of the wire rope sling wasattached to the eyebolt by a shackle, and the otherend was connected to the tong. The Boardrequested the record of this equipment modification,but Layne-Western could not produce it. The onlydocumentation consisted of a brief entry in a dailydrilling log, and the injured Operator, who hadperformed the weld repair in 1999, was the onlyperson with first-hand knowledge of this work. Theinjured Operator declined to be interviewed by theBoard.
Results and Analysis
The accident resulted from a number ofdeficiencies in the execution of specific activitiesand in the implementation of a series of managementsystems and related processes. These weaknessesinvolved all elements of the line organization,including the Office of Science, Chicago OperationsOffice, the Fermi Area Office, Fermilab, S.A. Healy,and Layne-Western.
Executive Summary

2
In terms of weaknesses in executing specificactivities, the injured Operator, who was not formallytrained or qualified to make structural welds, performeda “field” weld repair to the eyebolt and piston rodconnection in 1999. An independent engineeringevaluation by an outside laboratory, performed at therequest of the Board, indicated that the weld was ofuncertain quality and likely failed due to either metalfatigue from repeated loading during equipment use orfrom unusually high stress at the time of failure.Evaluation also showed that three cracks in the end ofthe piston rod existed before the accident, and thatmakeshift weld repairs of these cracks had beenattempted. These equipment modifications were notsubject to an engineering review to determine whetherthe weld was equivalent in strength to the threadedconnection it apparently replaced. In addition, theOperator stood with his head in close proximity to thetong while it was under tension from the hydraulicsystem. Widely available drilling industry guidanceidentifies this practice as unsafe. If a hazard analysiswhich addressed all job tasks and identified all controlshad been performed, this unsafe work practice wouldhave been recognized and the injury would have beenprevented.
In terms of weaknesses in management systemsand processes, the DOE Chicago Operations Office,the Fermi Area Office, and Fermilab did not effectivelyimplement and ensure flowdown of the integrated safetymanagement system framework to constructionsubcontractors and sub-tier contractors. Theseorganizations did not use contracting, procurement, andproject management mechanisms to consistently conveyand enforce safety and health expectations to theconstruction subcontractor and sub-tier contractor.These weaknesses enabled key individuals to performfunctions for which they were not qualified and allowedthe construction workforce to perform activities withoutbeing held accountable for strict compliance withrequirements.
Fermilab did not establish and implement processesto translate safety and health requirements intosubcontractor procedures and did not tailor the existingsystems for managing subcontractor construction safetyto address sub-tier contractors. Controls were notestablished to assure that sub-tier contractors wereadequately prepared to work safely before authorizingthe start of work. These weaknesses enabled drillingto commence in September 2000 without formalauthorization and resulted in neither Fermilab norS.A. Healy enforcing contract requirements mandatingdevelopment of a hazard analysis for drilling work.
The Fermi Area Office and Fermilab did noteffectively communicate roles, responsibilities, and clearlines of authority to ensure the adequate protection ofall workers, including construction subcontractors andsub-tier contractors. The Fermi Area Office conductedonly two inspections at the drill site prior to the accident,focusing narrowly on environmental issues. Fermilabincorrectly believed that only S.A. Healy was requiredto review sub-tier contractor safety programs, andFermilab neither conducted such reviews nor assuredthat S.A. Healy did. S.A. Healy did not require Layne-Western drilling personnel to conduct a hazard analysisand none was performed until June 2001.
The Fermi Area Office and Fermilab did not ensurethat the construction subcontractor and sub-tiercontractors had systems in place to train employees inhazard recognition and mitigation. Fermilab and S.A.Healy did not ensure that the Layne-Western personnelwere adequately trained and qualified to perform work.Layne-Western personnel were not trained in theFermilab hazard analysis process before starting work;did not participate in the June 9, 2001, safety stand-down training (which included hazards analysistraining); and did not receive sitewide safety orientation.
The Fermilab hazard analysis system could not beeffectively applied to task-specific hazards forconstruction subcontractors and sub-tier contractors.The Fermilab hazard analysis process did not provideclear guidance for evaluating task-specific hazards. TheS.A. Healy hazards analysis process was not used; evenif used, this process would not have resulted in anadequate hazards analysis because of its lack ofspecificity and rigor. Layne-Western did not provide ahazard analysis plan before commencing drillingoperations, and the only hazards analysis that wasconducted (June 2001) did not comprehensivelyaddress drilling hazards to which personnel wereexposed. The Board identified this weakness (absenceof task-specific hazards analysis) as the root cause ofthe accident and considered that an effective hazardanalysis system would have identified and correctedthe unsafe work practice concerning the Operator’slocation and could have drawn attention to the overallsubstandard condition of the drill rig and the relatedequipment.
During the investigation, the site providedconstruction injury rate data to the Board indicatingthat, for a 750-day period between August 1998 andSeptember 2000, Fermilab experienced no lost-workdaycases. However, the Board identified that asubcontractor pipe fitter dislocated his shoulder onNovember 11, 1998, which resulted in six lost workdays.

3
In addition, for six months during 1999, no fixed-priceconstruction work was performed by subcontractorsor sub-tier contractors, thus significantly lowering thepossibility that lost workday cases would have beenexperienced.
Finally, the Fermi Area Office and Fermilaboversight programs did not identify fundamentalweaknesses in construction subcontractor and sub-tiercontractor safety and health programs. The Fermi AreaOffice and Fermilab did not adequately analyze priorconstruction occurrences to identify and correct rootcauses and systemic weaknesses underlying these events.Causal factors present in the two personnel injury eventsthat led to project safety stand-downs in June 2001were also contributors to the drilling rig accident, aswere causal factors identified by two Type B accidentinvestigations in 1997 and 1998. Recurring deficienciesfrom prior occurrence reports involving worker injuriesat the construction site indicated that weaknessespersisted in work planning, hazard analysis, and workcontrols. Fermilab had not conducted a safety inspectionof the Layne-Western equipment upon arrival at theFermilab site. Work site safety inspections were notrigorous, formal, or documented. After the accident,the Board identified numerous safety deficiencies atthe job site, including some potential imminent-dangersituations, none of which had been identified by linemanagement or oversight personnel.
Conclusions
The Accident Investigation Board concluded thatthis accident was preventable. The Board identifiedsignificant weaknesses in the site’s implementation of
integrated safety management policy as it related tothe sub-tier contractor performing drilling activities.Weaknesses in translating safety and health requirementsinto operating procedures, implementing hazard analysisprocesses and associated controls, authorizing work,personnel training, and performing line oversightimpacted the effectiveness of construction worker safetyand health protection.
Fermilab did not ensure that the drilling sub-tiercontractor met basic requirements imposed by theDepartment, the site, and the U.S. Occupational Safetyand Health Administration. Although Fermilabexperienced a series of construction safety events withsimilar systemic causes prior to the accident andinstituted two safety stand-downs in the weeks beforethe event, a lack of rigorous causal analysis preventedidentification of lessons learned and systemicweaknesses, and implementation of effective correctiveactions. The hazard analysis program in place at thetime of the accident had not evaluated specific hazardsassociated with the drilling operation, Fermilab had notenforced the requirement for preparing such a task-specific hazard analysis, and line oversight of the drillingoperation had not identified the absence of such a hazardanalysis.
The DOE Chicago Operations Office, the FermiArea Office, and Fermilab need to intensify their effortsand commitment to ensure that all the elementsassociated with integrated safety management arepromptly and effectively addressed for all constructionsubcontractors and sub-tier contractors to preventadditional accidents at the Neutrinos at the Main InjectorProject and at other Fermilab construction sites.

4
Table ES-1. Causal Factors and Judgments of Need
Judgments of Need
Fermilab needs to improve the existing hazards analysisprocess in Fermilab Environment, Safety and Health Manual7010 by developing instructions and guidance to ensurethat it applies to sub-tier construction contractors at thework activity level.
Fermilab needs to implement a revised hazards analysisprocess such that:• Detailed procedures are established to formalize the
process for conducting task-level job-specific hazardanalyses (job hazard analyses).
• Personnel are trained on the task-level hazard analysisprocesses to ensure implementation by all assignedpersons.
• The process is revised to ensure that all workoperations at Fermilab are subjected to formal andeffective hazard analyses. This would include allpotentially hazardous operations planned forsubcontractors and sub-tier contractors.
• The process is revised to ensure that hazard analysesinvolve both the appropriate technical expertise andworkers, and receive appropriate review and approvalbefore work begins.
Fermilab needs to ensure that root and contributing cause(s)from incidents and occurrences are thoroughly evaluatedagainst integrated safety management core functions andguiding principles, and that resulting lessons learned aredisseminated and communicated to all appropriatepersonnel. Additionally, Fermilab needs to conduct follow-up reviews to ensure that the information is used to improvethe level of safety at the site.
Fermilab needs to ensure that incidents and occurrences atFermilab are reported through the appropriate DOEreporting systems (i.e., the Computerized Accident/IncidentReporting System and the Occurrence Reporting andProcessing System), evaluated, analyzed, and trended toensure that systemic weaknesses are identified andcorrected in a timely manner.
The Fermi Area Office needs to revise its process forvalidating closure and effectiveness of corrective actions.Additionally, FAO needs to conduct follow-up reviews toensure that corrective actions are effectively implemented.
Causal Factors
Fermilab failed to implement a hazard analysis process thatwas effectively applied to task-specific hazards forconstruction subcontractors and sub-tier contractors.
The Fermi Area Office and Fermilab failed to adequatelyanalyze prior occurrences to identify and correct rootcauses and systemic weaknesses underlying these events.

5
Table ES-1. Causal Factors and Judgments of Need (Continued)
Causal Factors Judgments of Need
Fermilab failed to establish and implement processes totranslate safety and health requirements into subcontractorprocedures. Fermilab did not establish controls to assurethat sub-tier contractors were adequately prepared to worksafely before authorizing the start of work.
Fermilab failed to tailor the system for managingsubcontractor construction safety to address sub-tiercontractors.
DOE and Fermilab oversight programs failed to identifyfundamental weaknesses in construction subcontractor andsub-tier contractor safety and health programs.
The Chicago Operations Office Manager needs to developand implement a process to provide assurance that effectivecorrective actions are implemented, and establish a methodto obtain feedback on corrective actions taken.
Fermilab needs to establish and implement a process toensure that all safety and health requirements flow down tosubcontractors and sub-tier contractors such that:• Procedures are adopted by subcontractors and sub-tier
contractors that are tailored for the specific roles andresponsibilities for each contracting organization.
• Specific procedures are validated to ensure that safetyand health requirements are properly implemented.
• Improved controls are established to assure thatsubcontractors and sub-tier contractors are adequatelyprepared to work safely before authorization to startwork is issued.
The FAO needs to ensure that Fermilab establishes andimplements processes to verify and validate that safety andhealth requirements are translated into subcontractor andsub-tier contractor procedures.
The Chicago Operations Office Manager needs to validatethe processes and procedures used by FAO and Fermilabto verify that work controls are established andimplemented before the start of work.
Fermilab needs to ensure that a program is established andimplemented for comprehensive environment, safety, andhealth oversight of all construction subcontractor and sub-tier contractor work operations.
The FAO needs to ensure that oversight of Fermilab iseffectively performed as specified in DOE Policy 450.5,Line Environment, Safety and Health Oversight.
The Chicago Operations Office Manager needs to ensurethat line management and independent oversight are beingperformed and are effective as specified by DOE Policy450.5, Line Environment, Safety and Health Oversight,and DOE Order 414.1A, Quality Assurance.
The Office of Science needs to ensure that formalcorrective actions are developed and implemented forES&H issues resulting from programmatic and technicalreviews of the NuMI Project.

6
Table ES-1. Causal Factors and Judgments of Need (Continued)
Causal Factors Judgments of Need
Fermilab failed to effectively communicate roles,responsibilities, and clear lines of authority to ensureadequate protection of all workers, including constructionsubcontractors and sub-tier contractors.
Fermilab failed to ensure that the constructionsubcontractor and sub-tier contractors had systems in placeto train employees in recognition and mitigation ofoperational hazards.
Chicago Operations Office and Fermilab failed toeffectively utilize contracting, procurement, and projectmanagement mechanisms to consistently convey, oversee,and enforce safety and health expectations to thesubcontractor and sub-tier contractors.
Chicago Operations Office and Fermilab failed to properlyimplement and ensure the flowdown of the integrated safetymanagement framework to subcontractors and sub-tiercontractors.
The Office of Science needs to implement the requirementsestablished in the Office of Science Functions,Responsibilities, and Authorities Manual for measuring lineES&H oversight effectiveness of the Chicago OperationsOffice.
Fermilab needs to establish and implement a formalizedsafety management system with clearly defined roles,responsibilities, and authorities when multipleorganizations, subcontractors, and/or sub-tier contractorsare involved in a construction project.
Fermilab needs to strengthen the training and competenceof all workers, managers, engineers, and safetyprofessionals responsible for construction safety.
Fermilab needs to establish processes to assure that hazardrecognition and training are in compliance with applicablerequirements (Occupational Safety and Health, DOE, andindustry standards).
The Chicago Operations Office and Fermilab need to revisecontracting, procurement, and project managementprocesses to ensure that safety and health requirementsassociated with construction operations (by subcontractorand sub-tier contractors) are clearly conveyed.
Fermilab needs to strengthen implementation of theintegrated safety management core functions to assure thatall potentially hazardous work and operations are subjectedto effective, formal, and documented hazard analysis.
Fermilab needs to establish and implement a process toensure that the framework of ISM flows down to allsubcontractor and sub-tier contractors.
The Chicago Operations Office Manager needs to ensurethat the Fermilab process for flowdown of the ISMframework to subcontractors and sub-tier contractors iseffective.

7
1.1 Background
On June 21, 2001, at approximately 9:40 A.M.,a construction subcontractor employee (referred toas the Operator) operating a drilling rig at the FermiNational Accelerator Laboratory (Fermilab) receivedserious head injuries that required hospitalizationwhen he was struck by part of the drilling rig.
On June 25, 2001, the Acting AssistantSecretary for Environment, Safety and Health, U.S.Department of Energy (DOE), upon therecommendation of the DOE Chicago OperationsOffice, appointed a Type A Accident InvestigationBoard to investigate this accident in accordance withDOE Order 225.1A, Accident Investigations. Acopy of the appointment memorandum appears inAppendix A.
1.2 Facility Description
Fermilab occupies approximately 6,800 acresof DOE property 30 miles west of Chicago, Illinois.Fermilab was established in 1968 by the U. S.Atomic Energy Commission. The site includes over300 buildings, such as laboratories, shops, andassembly bays, along with particle accelerators anddetector enclosures.
As the largest particle physics laboratory in theUnited States, Fermilab operates particleaccelerators used in investigating the fundamentalproperties of matter, space, and time. Fermilab’sother operations include superconducting magnetresearch, design, and development; detectordevelopment and operation; and high performancecomputing and networking. Some 2,500 physicistsfrom around the world utilize Fermilab facilities fortheir research. Fermilab is open to the public and atypical day will find university students visiting thesite.
Fermilab operates under the programmaticdirection of the DOE Office of Science. The DOEFermi Area Office (FAO) of the DOE ChicagoOperations Office manages the site contractoroperations. Universities Research Association, Inc.,a consortium of universities, is the site contractorthat manages and operates Fermilab for DOE. A
Board of Trustees maintains fiduciary responsibilityfor the corporation.
Figure 1-1 displays the organizationalrelationships between Fermilab and the Neutrinosat the Main Injector (NuMI) construction project,where the accident occurred. (This organizationalchart was provided to the Board by Fermilab duringthe in-briefing meeting on June 27, 2001.) TheNuMI Project included excavating a series oftunnels and experimental halls beneath the Fermilabsite, operations known as the NuMI Tunnels andHalls Project. The NuMI Project will supportadvanced physics experiments utilizing a neutrinobeam that would enter a detector at Fermilab andpass through the earth to another detector locatedin northern Minnesota.
The lead subcontractor for the NuMI Tunnelsand Halls Project was the S. A. Healy Company ofLombard, Illinois, a tunneling and heavyconstruction contractor. Layne-Western, a divisionof the Layne Christensen Company of MissionWoods, Kansas, a well drilling company and aS. A. Healy subcontractor, provided services fordrilling exhaust air ventilation (EAV) and surveyriser shafts from the surface to the undergroundtunnel. The injured Operator was a Layne-Westernemployee.
Early in the NuMI Project, Fermilab identifiedthe need to augment its staff with persons havingunderground construction experience. In October1999, Fermilab contracted with Harza Engineeringto provide three individuals with undergroundconstruction experience to serve as constructioncoordinators. Under this contract, Harza employeeswould be supervised by Fermilab and wouldmonitor, but not manage, S. A. Healy; nonetheless,they were assigned to direct certain aspects of thework. Fermilab subsequently increased the numberof Harza construction coordinators to four. Harzaalso provided a safety consultant to conduct safetyaudits.
The NuMI Project Management Plan specifiedthat construction work would be performed incompliance with standards contained in the FermilabEnvironment, Safety, and Health (ES&H) Manual(FESHM) and all applicable ES&H standards in
Introduction1.0

8
the laboratory’s work smart standards. In addition, allrelated work was to be performed in compliance withapplicable Federal, state, and local regulations. InOctober 1999, the DOE Chicago Operations Officeverified that Fermilab had implemented the DOEintegrated safety management (ISM) system, and thatISM policies were reflected in the site ES&H Manual.
1.3 Scope, Purpose, andMethodology
The Type A Accident Investigation Board beganits onsite investigation on June 27, 2001; completed theonsite phase of its investigation on July 20, 2001; andsubmitted its report to the Assistant Secretary forEnvironment, Safety and Health. The scope of theBoard’s investigation was to review and analyze thecircumstances of the accident to determine its causes inaccordance with DOE Order 225.1A. The purposes ofthis investigation were to analyze causal factors, identifyroot causes and determine judgments of need to preventrecurrence of similar accidents at Fermilab and acrossthe DOE complex.
The Board conducted its investigation using thefollowing methodology:
• Inspecting and photographing the accident scene andindividual items of evidence related to the accident
• Performing a limited engineering evaluation of thefailed components
• Gathering facts through interviews, document andevidence reviews, and walk-downs of the area
• Reviewing emergency and medical responseoperations
• Analyzing facts and identifying causal factors throughevents and causal factors charting and analysis, barrieranalysis, and change analysis
• Developing judgments of need for corrective actionsto prevent recurrence based on analysis of theinformation gathered.
Figure 1-1. Organizational Chart Related to the NuMI Project

9
Accident Investigation Terminology
A causal factor is an event or condition in the accident sequence that produces or contributes to the occurrence ofthe accident. There are three types of causal factors:
(1) Direct cause, the immediate event(s) or condition(s) that caused the accident(2) Root cause(s), the causal factor(s) that, if corrected, would prevent recurrence of the same accident or
similar accidents(3) Contributing causes, factors that collectively with other causes increase the likelihood of an accident, but
that individually did not cause the accident.
Events and causal factors analysis includes charting, which depicts the logical sequence of events and conditions(causal factors) that allowed the event to occur, and the use of deductive reasoning to determine events orconditions that contributed to the accident.
Barrier analysis reviews hazards, the targets (people or objects) of the hazards, and the controls or barriers thatmanagement systems put in place to separate the hazards from the targets. Barriers may be physical, such asequipment design or protective clothing, or elements of management, such as training and supervision.
Change analysis is a systematic approach that examines planned or unplanned changes in a system that causedundesirable results related to the accident.

10
2.1 Background andAccident Description
2.1.1 Accident Overview
On the morning of June 21, 2001, twoLayne-Western employees, the drill rigOperator and a Helper, were conductingdrilling operations at Fermilab. The accidentoccurred at approximately 9:40 A.M., asthe drill crew was attempting to disconnectdrill pipe sections. An equipment failureoccurred during disconnecting (breaking)drill pipe sections as they were beingremoved from the shaft. A hydraulicsystem (hydraulic ram, piston rod, wire rope sling,shackle, and eyebolt) was being used to apply forceto a tong, effectively a large pipe wrench, whenthe equipment failed. The threaded eyebolt, whichserved as the point of connection to the piston rod,disengaged, releasing the hydraulic force andresulting in an instantaneous release of energystored within the drill pipe. The unrestrained tongand tong handle rotated, striking the Operator onthe right side of his head, just below his hard hat.It was the Board’s assessment that the tong, ratherthan the eyebolt and shackle assembly, struck theOperator; this conclusion differs form the Helper’sverbal report immediately following the accidentand is based upon the Board’s engineering analysis,interview statements, and a subsequent job sitewalkdown.
Exhibit 2-1 shows the location of the drillingsite. Exhibit 2-2 shows the drill rig operating stationwhere the Operator was standing when the injuryoccurred. Figure 2-1 shows the eyebolt connectionto the piston rod.
2.1.2 Background
Fermilab pre-qualified construction contractorsto bid on the NuMI Tunnels and Halls Project inJuly 1999. The pre-qualification process used thefollowing “Safety and Health Program Criteria” toscreen construction contractors to bid on the NuMIProject:
• The construction contractor’s corporate safetyphilosophy
• Experience modification rates for the previousthree years
• Occupational Safety and Health Administration(OSHA) 200 logs for the previous three years
The Accident2.0
Drilling rig mast
Tool trailer
Upper tong thatstruck Operator
Normal path ofwire rope sling
RollerRotary table
Wire rope sling
Eyebolt and shackle
Exhibit 2-2. Drill Rig Where the Injury Occurred
Exhibit 2-1. Drilling Site Where the Accident Occurred

1 1
PISTON ROD
WELD WHICH FAILED
ANCHOR SHACKLE
EYEBOLT SHOWN REMOVEDFROM PISTON ROD
EYEBOLT
Note that after weld failure, the threads of theeyebolt would fit into the end of the rod, which wasdistorted with three visible longitudinal cracks,without thread engagement. Each crack showedevidence of previous weld repair on the outsidesurface of the piston rod..
Eyebolt: thread length = 1*, diameter = 0.825,damaged threadsPiston rod: internal thread depth of rod = 2.5,Inside diameter = 0.833, threads did not appeardamaged
* Measurements are in inches
• Total number of hours worked by employees foreach of the last three years
• Resumes of two to four safety professionals whoare current employees of the company.
Fermilab evaluated the “Safety and Health ProgramCriteria” to ensure that each construction contractorhad developed and implemented a corporate safety planand that the contractor had achieved the following:
• Experience modification rate less than 1.0
• Recordable injury case rate less than or equal to9.5
• Lost workday case rate less than or equal to 4.4.
Fermilab evaluated 13 construction contractors andqualified 10 to receive a Request For Proposalsolicitation package. Criteria for evaluating eachconstruction contractor’s proposal were based on aweighted average considering 70 percent cost,15 percent project schedule, 10 percent onsite personnelresources, and five percent onsite equipment resources.After this point, contractor safety and health programsand safety records were no longer considerations in theselection of the construction contractor for the NuMIProject.
Fermilab awarded the NuMI Tunnels and Hallscontract to S. A. Healy, which had the lowest cost and
the highest technical rating. When S. A. Healy beganoperations, a single full-time safety professional wason staff at the site. S. A. Healy supplemented thesafety professional with a part-time consultant and lateradded two additional full-time safety personnel to theirstaff.
Fermilab issued a Notice to Proceed on March 6,2000, and construction started shortly thereafter. OnSeptember 13, 2000, S. A. Healy subcontracted withLayne-Western to drill EAV and survey riser shafts forthe NuMI Tunnels and Halls Project. A pre-qualifyingprocess was not followed when S.A. Healy awardedthe subcontract to Layne-Western. In addition, Fermilabdid not review the past safety performance of Layne-Western before awarding the drilling contract.
On September 25, 2000, Layne-Western begandrilling the first of four EAV shafts and two survey risershafts. These shafts ranged from 18 inches to 25 inchesin rough diameter, with depths varying fromapproximately 100 feet to approximately 350 feet basedon the tunnel’s location. The accident occurred duringdrilling of EAV-2. This job site lies on the north side ofGiese Road and west of, and adjacent to, Indian Creek,as shown in Exhibit 2-1.
The drilling rig involved in the accident was builtby Gardner-Denver in 1969 and was mounted on aheavy truck bed for Layne-Western. Layne-Westernhad used the rig on various drilling projects since 1969.
The Board determined that at least two equipmentmodifications were made after the drill rig was builtthat are relevant to the accident. In the early 1970s,the hydraulic breaking mechanism was installed toreplace a manual breakout wrench used to loosen andtighten the drill pipe section joints. In 1999, the eyebolt-piston rod connection involved in the accident failed.An entry in a Layne-Western Daily Drilling report datedMarch 2, 1999, stated “Broke eyebolt on end ofhyd[raulic] ram for breaking but we [were] able to weldit up.” The Daily Drilling report indicated that the drillingcrew performed this repair in the field.
On April 20, 2001, representatives of the U. S.Department of Agriculture inspected the EAV-2/EAV-3job site, acting on behalf of the U. S. Army Corps ofEngineers in connection with the Fermilab wetlandspermit, and requested that drilling operations besuspended until environmental improvements relatedto the work could be made. Layne-Western resumedwork at the site on April 30, 2001, after S. A. Healymade necessary improvements, and after receivingverbal restart authorization from the U. S. Departmentof Agriculture. The Layne-Western crew began drillingEAV-2 on May 4, 2001.
Figure 2-1. Piston Rod End Fixture

12
On May 25, 2001, the Operator performed a safetyinspection of the drilling rig, related equipment, and theEAV-2/EAV-3 job site. Although the inspection recordcompleted by the Operator was incomplete, completedportions of the record did not identify safety deficienciesrequiring corrective action. Between May 4, 2001, andJune 21, 2001, a number of cognizant FAO, Fermilab,and S. A. Healy safety personnel visited the job site,but did not document any safety deficiencies.
On June 9, 2001, S. A. Healy instituted a safetystand-down on the NuMI Tunnels and Halls Projectconstruction work following a rigging/material handlingaccident in which an S. A. Healy employee was struckby a suspended load. S. A. Healy used the stand-downto conduct pre-planned safety training. Work resumedon June 10, 2001.
On June 13, Fermilab and S. A. Healy jointlyinstituted another safety stand-down on the NuMITunnels and Halls Project construction work, followingthe injury of two S. A. Healy employees in anothermaterials handling accident. This second accidentoccurred when rigging for a suspended load failed,causing the load to strike a man-lift in which the twoemployees were positioned. Work resumed on June 15.Although these safety stand-downs included training
and orientation of the NuMI Tunnels and HallsProject workforce on safety policies andprocedures, along with techniques of hazardanalysis, the Layne-Western drilling crew wasnot asked to participate in the stand-downs, nordid they receive the related hazard analysistraining.
On June 15, 2001, the Fermilab Directorordered an investigation into S. A. Healy�ssafety performance and safety management.The Fermilab investigation was under way whenthe drilling rig injury involving the Layne-Westernemployee occurred, and was completed onJuly 2, 2001.
On the morning of June 21, 2001, twoNuMI construction coordinators visited theEAV-2/EAV-3 job site, but did not documentany safety deficiencies.
When the accident occurred, the two-person crew, composed of the Operator and theHelper, was removing the second of six 20-footdrill collars from the EAV-2 shaft. A drill collaris a length of heavy pipe placed immediatelyabove the drill bit to provide concentrated weightto enable the bit to drill properly, and to producea vertical hole. Each collar was approximatelysix inches in diameter, and the entire drillassembly at maximum depth weighed
approximately 15,000 pounds. A chronology of eventsrelated to the accident appears in Appendix B.
2.1.3 Accident Description
The accident occurred when the welded connectionbetween the eyebolt and the hydraulic cylinder pistonrod failed during operation. This event released tensionon the wire rope sling connecting the eyebolt to theupper tong. The sling, with the shackle and eyeboltattached, sprang back toward the end of the drilling rigwhere the Operator and his Helper were standing.
The release of tension on the sling, coupled withthe torsion on the drill collars, caused the tong to recoiltoward the Operator. The tong, which was 32 incheslong, made of forged steel, and weighed approximately150 pounds, struck the Operator on the right side of hishead, just below the rim of his hard hat.
After the accident, the Helper demonstrated theOperator�s position to the Board, indicating that theOperator was leaning in towards the tong whileoperating the lever controlling pressure to the hydrauliccylinder with his left hand. This body position wouldhave placed the Operator�s head at the approximateelevation of the tong handle.
The accident resulted from the failure of the weldconnecting the wire rope to the hydraulic cylinder used in makingand breaking threaded drill pipe section joints. Torsion isapplied to the joints by mechanical tongs (in effect, pipewrenches) that grip the outer diameter of the drill pipe section.One of the tongs is braced against a drill rig stop pin, while theother tong is operated (i.e., pulled) by a mechanical forcesupplied by the hydraulic cylinder. This force is transmittedthrough a wire rope sling connected with miscellaneoushardware.
� � � � � � � � �
� � � � � � � � � ��
� � � � � � �� �� � � � � � � � � � � � �� � � � � � � � � � � � � �

13
The Helper stated that he thought the shackle andeyebolt struck the Operator. However, the Board�sengineering evaluation indicated that the tong mostlikely struck the Operator. The Operator declined tobe interviewed by the Board. The Board concludedthat a blow to the Operator�s head by the recoilingtong handle was the most credible injury scenario.
On June 21, 2001, shortly following the accident,Fermilab issued a stop-work order for the NuMITunnels and Halls construction project, halting all drillingoperations by Layne-Western and all S. A. Healy work.On June 28, 2001, Fermilab authorized a phased restartof work on the project.
2.1.4 Engineering Evaluation of theFailed Components
The Board conducted a limited engineeringevaluation on the failed components using anindependent offsite laboratory. Attorneys representingLayne-Western would not allow destructive tests to beperformed.
The evaluation considered the condition of theeyebolt after the accident, and the condition of the endof the piston rod, as shown in Exhibit 2-3. It includeddetailed visual inspection, measurements, hardnesstesting, and engineering analyses. Visual inspectiondisclosed three longitudinal cracks in the threaded endof the piston rod, one of which is visible in Exhibit 2-3.The threaded portion of the eyebolt was considerablydeformed, as can be seen in Exhibit 2-3.
Examination of the eyebolt and piston rod followingthe accident revealed that these components separatedwhen a weld that held them together failed. Thethreaded portion of the eyebolt had been inserted intothe threaded socket in the end of the piston rod, butthere was apparently little or no thread engagement dueto expansion of the socket diameter. This expansionwas attributed to through-wall cracks in the socket andto possible distortion due to weld repairs of previouscracks. The load on the connection was apparentlysupported entirely by a circumferential weld that joinedthe shoulder of the eyebolt to the end of the piston rod.The weld failed either because of cracks that developeddue to fatigue related to repetitive loading or because ofunusually high stress at the time of failure.
2.2 Emergency Response andMedical Treatment
Emergency response to the accident consisted of(1) the initial emergency medical response operationsat the scene, (2) the transport of the injured Operatorto the hospital, and (3) the medical care provided at thehospital.
When the Operator was struck on the right side ofhis head, he fell onto the wooden platform that servedas the operating deck. The Helper, who was alsostanding on the platform but to the right of and behindthe Operator, provided immediate aid by laying himdown on the wooden pallets to the left of and adjacentto the drill rig and then went to call for emergencyassistance.
As the Helper was en route to obtain a cellulartelephone available at the job site to call for assistance,he saw a Fermilab employee driving by the job site.The Helper flagged down the Fermilab employee, who
Exhibit 2-3. Eyebolt That Was Connected to the Piston Rod (Left) and the End of the Piston Rod After the Accident (Right)

14
Engineering Evaluation Supporting the ConclusionThat the Operator Was Most Likely Struck by the Tong
Hydrauliccylinder
Pistonrod
Truck bed
Upper Tong &Handle
Wire ropeTruckcab
“Line ofFlight Zone”
Roller Shackle and eyebolt
Helper
Operator
Drill Platform
“Line of Flight”
Although the Helper stated that he thought the Operator was struck by the shackle and eyebolt, it does notappear that there is a high probability that this happened. The motion of the wire rope would have been veryrapid and ultimately could have resulted in the attached shackle and eyebolt being located near the injuredOperator. However, the structural configuration of the rig and the fact that the Helper was not injured areprincipal reasons for not supporting this assertion.
• The assumed path of the broken shackle and eyebolt through the mast structure to the injured Operatorwas not a straight line. To reach the Operator, the shackle and eyebolt would need to “turn the corner”at the roller and somehow miss the Helper, who was reported to be standing on the corner of the drillplatform. If the Operator had been hit by the shackle and eyebolt, the shackle, eyebolt and wire ropewould also have struck, or wrapped around, the Helper. As shown in the accompanying sketch, theHelper would have had to be out of the “line of flight” of the wire rope.
• Instantaneous release of tension by the weld failure would have caused the shackle, eyebolt and wirerope to fly toward the roller – much like a rubber band. Its straight-line motion could have helped theshackle, eyebolt and 8 feet of wire rope pass through the mast structure and confining passages, so thatthe rope extended behind the drill platform. However, this initial rope movement should have resultedin injury to the Helper if he was standing in the “line of flight zone.”
• Combined with the clockwise rotation of the tong handle, this tension release would have jerked thewire rope end (attached to the tong handle) toward the Operator’s location while he was operating thehydraulic controls. This jerk (approximately 2 or 3 feet of tong handle movement) could have pro-pelled the other rope end and shackle and eyebolt within the “line of flight zone” and toward the tonghandle. Again, it is unclear how these assumed wire rope motions could have occurred without injuringthe Helper.
In summary, based on the Helper’s report of both his and the Operator’s position, and the fact that the Helperwas not injured, the wire rope and shackle/eyebolt end did not fly through the “line of flight zone” to strike theOperator. Therefore, the tong handle must have struck the Operator.

15
then called the site emergency telephone number usinghis cellular telephone. This call was placed at 9:44 A.M.,approximately four minutes after the accident, and resultedin Fermilab emergency personnel arriving at the scene at9:45 A.M. and the Fermilab ambulance arriving at9:48 A.M.
Based on their initial assessment of the Operator’shead injuries, the first Fermilab firefighters/emergencymedical technicians (EMTs) arriving at the scenerequested the aid of Tri-City Ambulance Service. (Thelaboratory had contracted with Tri-City AmbulanceService for advanced life support ambulance service.)Paramedics from the town of Geneva responded. TheFermilab fire department established incident commandat 9:48 A.M., immediately outside the job site on GieseRoad. The Geneva advanced life support ambulancearrived at the accident scene at 9:57 A.M. Initial reportsindicated that the Operator’s breathing was irregular, thathe was not responsive, and that four EMTs were requiredto restrain and immobilize him as he regainedconsciousness.
At 10:15 A.M., the Geneva ambulance left the sceneand transported the Operator to the Delnor CommunityHospital for emergency care. A Fermilab firefighter/EMT drove the ambulance, enabling the two Genevaparamedics to continue rendering assistance to theOperator. He was transported to Delnor CommunityHospital, where he was admitted and evaluated.
At the hospital, medical diagnosis determined thatthe Operator had sustained a frontal skull fracture with amild to moderate brain injury consisting of a contusion ofthe right frontal lobe, with swelling. He also sustained afracture of the right jawbone and dysfunction of the rightthird cranial nerve, which controls certain eye movements.These injuries are consistent with a blunt force type oftrauma, such as being hit by the tong handle. After heregained consciousness, he exhibited some unsteadinesson his feet and mild difficulties with thinking and reasoningas a result of his injuries. He also had blurred vision anddecreased vision in the right eye. The Operator did notrequire surgery, and improved sufficiently such that onJuly 2, 2001, he was transferred to a rehabilitation facility,where he received occupational, physical, and speechtherapy.
The Board concluded that the initial emergencyresponse and medical response were timely and wellcoordinated.
2.3 Investigative Readiness andAccident Scene Preservation
Shortly after the Geneva ambulance left the accidentscene with the Operator, the Incident Commander turned
custody of the scene over to a representative of theFermilab Facility Engineering Services Section. Controlof the accident scene was subsequently transferred toFermilab ES&H Section. Arrangements were then madeto clearly establish the accident scene perimeter withyellow tape, photograph the scene, and formally institutean access control point by posting a security guard at theentrance to the scene. The guard was given instructionsto limit access to only authorized individuals. The guardmaintained a record of those who entered the area, theirduration at the scene, and the purpose of their visit.
On June 27, 2001, the Board assumed custody of theaccident scene, relinquishing control back to the FAO onJuly 17, 2001. During this period, a security guardmaintained continuous access control to the accidentscene.
While the actions Fermilab took to preserve theaccident scene were commendable, three areas ofconcern were noted by the Board:
(1) Potential exposure to bloodborne pathogens.Prior to establishing an access control point, Fermilab,S. A. Healy, and Layne-Western personnel werepresent at the accident scene for various purposes.In a typical accident involving contact between ahuman and equipment or machinery, it is notuncommon to have blood at the accident scene.Personnel visiting the accident scene could have comein contact with bloodborne pathogens, creating anunnecessary health risk to themselves and others theymay come in contact with.
(2) Alteration of evidence. To obtain high-qualityphotographs of the failed components involved in theaccident, personnel repositioned the components.Moreover, they degreased and cleaned the equipmentin preparation for the photographer, thereby removingany other evidence, such as metal shavings, that mighthave been of use to the Board.
(3) Removal of material. The Operator’s personalpossessions were removed from the accident scene.Later, the Board was unable to validate certainspecific testimonial information relative to hisbelongings (e.g., possession of the Operator’s personalcopy of his company’s safety manual) becausepersonnel from his organization removed themprematurely from the accident scene.
The Board concluded that an effective accesscontrol system was not instituted in a timely fashion toproperly preserve the accident scene.

16
This section addresses the facts related to theaccident, along with the results of the Board’sanalysis. The Board presents this information interms of the ISM core functions and guidingprinciples, which comprise the fundamental DOEsafety and health policies that should have beenincorporated into the work planning and execution.
3.1 Physical Hazards,Controls, and RelatedFactors
3.1.1 Define the Scope of Work
Effective work execution begins with thepreparation of a well-defined scope of work thattranslates the mission and requirements into termsthat those who are to accomplish the work canclearly understand. The definition of work scopemust provide sufficient detail to support hazardanalysis and development and implementation ofcontrols at the task level. To fulfill its responsibilities,line management must determine the work to beperformed and be accountable for understandingit as completely as possible through every phaseof the work cycle. This process applied to theNuMI Tunnels and Halls construction project andthe associated Layne-Western shaft drillingoperations. The scope of the construction project,including shaft drilling operations, was defined in aseries of tiered documents. These documents,summarized below, included the Project ExecutionPlan, the NuMI Project Management Plan, theFermilab-S. A. Healy contract, the S. A. Healywork plan, and Layne-Western “job letters.”
The Project Execution Plan dated February1999 described the mission needs and justificationfor the NuMI Project, its objectives and scope, theDOE project management structure, and theresource plan. DOE prepared the ProjectExecution Plan and the Director, Office of EnergyResearch, the predecessor organization to theOffice of Science, approved the plan, whichconstituted Critical Decision number one inaccordance with DOE Order 430.1A, Life Cycle
Asset Management, and the Joint Program OfficeDirection on Project Management. Discussion ofES&H requirements in this plan was limited toreferences to the NuMI EnvironmentalAssessment, excerpts from the subsequent Findingof No Significant Impact related to theEnvironmental Assessment, and a reference to theNuMI Preliminary Safety Assessment Document.
The Project Management Plan dated March 8,1999, set forth the plans, organizations, andmanagement systems to be used by Fermilab andDOE to manage the NuMI Project. The FermilabNuMI Project Manager prepared the NuMIProject Management Plan, which complementedthe Project Execution Plan and indicated thatproject management would be conducted inconformance with DOE Order 430.1A and theJoint Program Office Direction on ProjectManagement. The Project Management Plan wasprepared by Fermilab for approval by DOE. Whileit was approved by the FAO, the DOE Office ofScience indicated “approved provisionally –pending peer review.” At the time of the accident,this document remained provisionally approved bythe Office of Science, and did not reflect thecurrent site organizational structure or operations.
The Project Management Plan indicated thatdesign, construction, operation, anddecommissioning operations would be performedin compliance with the FESHM standards and allapplicable ES&H standards in the work smartstandards set. However, the document mademinimal reference to construction safety.
The S. A. Healy contract with Fermilab forthe NuMI Tunnels and Halls Project, datedFebruary 11, 2000, described the scope of workassociated with shaft excavation. The scope ofwork provided the general technical requirementsand established the applicable American Societyfor Testing and Materials, the American WeldingSociety, the American Water Works Association,and OSHA standards—specifically the U. S. Codeof Federal Regulations 29 CFR 1926, Subpart S(Underground Construction, Caissons, Cofferdam,and Compressed Air) and Subpart U (Blasting andUse of Explosives).
Accident Facts and Analysis3.0

17
In August 2000, S. A. Healy submitted a “Work Planfor the Drilling of the Vent Shafts and Survey Risers(Submittal No. 42)” in accordance with its contract withFermilab. The submittal identified Layne-Western as thesubcontractor for the ventilation shafts and survey risers,and established the work progression for the task. Itincluded a basic outline of the drilling methods and outlinedthe environmental precautions that would be taken at theEAV-2 and EAV-3 job site. The work plan referencedthe need to de-energize overhead power lines at the EAV-1and SR-2 job sites, and that the work would be completedin compliance with OSHA requirements. The work plandid not address the management of S. A. Healysubcontractors, nor was this required by the Fermilab-S. A. Healy contract.
On September 9, 2000, Fermilab reviewed the workplan and returned it with the notation “Approved as Noted:Resubmit,” with comments concerning extending thegravel base at the EAV-2/EAV-3 job site due toenvironmental concerns. Fermilab approved the workplan on November 8, 2000.
Layne-Western signed a contract with S. A. Healyon September 13, 2000, to drill four EAV and two surveyriser shafts for the NuMI Tunnels and Halls Project.However, the construction schedule called for drilling tocommence on August 14, 2000, and finish on November1, 2001. The contract required Layne-Western to providea work plan to S. A. Healy 30 days before commencingwork. Among the other Layne-Western contractrequirements were:
• “Take all precautionary measures in protection of theenvironment and surrounding areas from impact dueto their work.”
• “Attend all required Safety Orientations (conductedby Fermilab and by the contractor) prior tocommencement of work.”
• “Provide a hazard analysis plan for work that they willbe performing and all of their employees shall sign theplan to acknowledge that they have read andunderstand the plan.”
• “State the name of the person that will be designatedas their ‘Competent Person’ prior to commencementof the work. The Competent Person shall be at thework site whenever there is work in progress by theSubcontractor.”
A Layne-Western job letter dated September 15,2000, provided work instructions to the Operator andidentified the Operator as the “Competent Person.” The
Fermilab-S. A. Healy contract, as referenced by theS. A. Healy-Layne-Western contract, defined aCompetent Person as the onsite safety official, who musthave completed the 30-hour OSHA construction safetycourse, or equivalent. The Layne-Western Operator hadnot met the Competent Person requirements. However,the Board noted that this determination applied only to theOperator’s qualifications regarding safety, and not hiscompetence in the drilling trade.
Layne-Western began mobilizing on September 18,2000, and drilling the first of six shafts commenced onSeptember 25, 2001. Layne-Western did not provideS. A. Healy with a formal work plan.
On March 12, 2001, Layne-Western began drillingthe EAV-2 shaft. This work was also initiated withoutsubmitting a work plan to S. A. Healy, although the Layne-Western General Manager had issued a job letter onDecember 7, 2000, addressing the work at EAV-2,EAV-3, and EAV-4. The job letter had not specifiedworker safety and health requirements, had not referencedother documents that contained such requirements, andhad not invoked OSHA requirements. The job letter alsohad not included a detailed breakdown of drilling tasksnecessary to complete a comprehensive hazard analysisof every task.
Significant attention was paid to environmental aspectsof the Layne-Western drilling operation. For example,the EAV-2/EAV-3 job site was requested to be shut downon April 20, 2001, after a U.S. Department of Agricultureinspection revealed non-compliance with the Fermilabwetlands permit. Layne-Western had penetrated themembrane placed under the gravel fill when it installed asettling basin. S. A. Healy took immediate action to correctthe environmental non-compliances. However, minimalattention was focused on the safety and health aspectsof the work.
The safety and health expectations associated withconstruction and shaft drilling operations were not fullyconveyed as part of the array of “scope of work”documents, and project planning did not include provisionsfor managing S. A. Healy subcontractors. NeitherFermilab nor S. A. Healy enforced the contractualrequirements for Layne-Western to provide a work plan30 days before commencement of work. Layne-Western“job letters” had not provided sufficient breakdown ofthe work scope to support adequate task-specific hazardanalysis.
The Board concluded that line management failedto adequately address safety as part of planning forLayne-Western drilling operations and failed toenforce compliance with existing safety requirements.

18
3.1.2 Hazard Analysis
The objective of hazard analysis is to develop anunderstanding of task-specific hazards that may affectthe worker, the public, and the environment. Each levelof hazard analysis is the foundation for a more detailedanalysis; that is, a construction project hazard analysisis, in turn, used as the basis for an activity-level ortask-level hazard analysis. Hazard identification andanalysis must occur at any phase of the work cycle towhich it applies, including construction. The proceduresused to carry out hazard assessments at the projectlevel are contained in the FESHM.
The FESHM established mandatory ES&Hpolicies. FESHM 7010, Subcontractor SafetyProgram, described Fermilab’s program, procedures,and safety requirements for construction work.According to FESHM 7010, “Work will not proceedon that activity until the hazard analysis has beenaccepted by the construction coordinator.” Constructioncoordinators were defined as individuals specificallyassigned to oversee the work of a fixed-pricedsubcontractor for conformance to the subcontractdocuments. Construction coordinators were primarilyfurnished by the Fermilab Engineering Services SectionEngineering Group, which, at times, was supported byan outside Architectural Engineering Group.
The hazard analysis section in FESHM 7010 didnot provide sufficient detail to communicaterequirements to subcontractors specifying when and howa hazard analysis was to be completed for each taskassociated with the scope of work, nor did it indicate aneed for worker involvement in the process. FESHM7010 included ES&H Administrative Form #17, HazardAnalysis Form, but had not referenced or requiredcompletion of this form. Additionally, page one of theform stated: “This form is to be completed by theconstruction coordinator for acceptance prior to theNotice to Proceed,” indicating that this was a one-timecontract submittal before receiving authorization toinitiate work.
The Fermilab contract with S. A. Healy did notdirectly invoke FESHM 7010; however, S. A. Healyessentially adopted the FESHM by referencing thisdocument in the S. A. Healy Safety and Health Manual.The contract included various clauses for safe workoperations. Two clauses important to this event werethe “Project Specific Safety and Health” and the “ES&HWork Procedures” Exhibit A clauses. The hazardanalysis requirement was contained in the ProjectSpecific Safety and Health clause. Some of the more
important requirements that affected hazard analysiswere:
• Exhibit A, paragraph 13.6, of the S. A. Healy contractwith Fermilab required hazard analyses for Healyoperations and operations of its sub-tier contractors.
• Initial hazard analyses were required to be submittedand accepted by Fermilab before the Notice toProceed.
• Sub-tier contractor operations were required to beincluded in the hazard analysis.
• An acceptable hazard analysis was required for allwork.
• Fermilab would review all hazard analyses forcompleteness and conformance with OSHA andindustry standards.
• The name of the Competent Person would beincluded on the hazard analysis and communicatedto all workers.
• Job-specific safety orientation would be providedbased on the hazard analysis.
• All contractual submissions would have to be metfor Fermilab to issue a Notice to Proceed.
Section 16 of the S. A. Healy Safety and HealthManual outlined the hazard analysis process. Thissection included the Project Hazard Analysis Form fromthe June 1999 version of FESHM 7010. The generalinstructions in the S. A. Healy Safety and Health Manual,under Hazard Analysis and Site Inspections, requiredhazard analyses to be prepared as follows:
“Before the start of each major work phase, a job safetyanalysis will be prepared. This will determine thesafety and health hazards involved during this workphase. The name of Competent Persons shall beincluded on the Hazard Analysis [HA].
“This is to isolate any anticipated hazard and to outlinemitigating actions (including PPE [personal protectiveequipment]) in advance in order to control the hazards.
“Prior to the start of actual work, a meeting will be heldwith the Contractor(s) representative and any affected

19
subcontractor to review the “Job Hazard Analysis” andbe prepared for this work phase. A job-specific safetyorientation to all Sub-contractor and Sub-Sub-contractoremployees based upon each HA. Each employee willsign the HA to indicate having received the orientation.The signature list shall be available for review by theConstruction Coordinator. As the HA is updated, theemployees must be advised of the new information.”
Section 16 of the S. A. Healy Safety and HealthManual did not reference FESHM 7010. It providedbrief instructions for completing a hazard analysis, butthey were not sufficient to prepare a proper hazardanalysis at the task level.
The Layne-Western contract with S. A. Healyrequired development of a hazard analysis plan. It alsorequired Layne-Western personnel to followS. A. Healy contract requirements. However, theserequirements were not met or enforced by Fermilab orS. A. Healy before drilling operations began.
Although Section 4 of the Layne Christensen Healthand Safety Program was entitled “Hazard Analysis,”it presented only some of the generic hazards thatemployees could encounter. An attached table, also
entitled “Hazard Analysis,” identified some of thehazards associated with drilling and very genericcontrols for the hazards. The table did not identifyhazards specific to the drilling activity, nor did it identifyspecific controls to be implemented by the drilling crew.Additionally, Layne-Western did not have a documentedprocedure or process that provided instructions foremployees to conduct a hazard analysis.
The S. A. Healy General Superintendent stated thathe had asked the Layne-Western Operator to begin fillingout the S. A. Healy hazard analysis forms approximatelytwo weeks before the accident. After the accident, heasked the Layne-Western Helper for a copy of thehazard analysis for the job. The hazard analysisconsisted of two pages dated June 21, 2001 (the dateof the accident). The first page was similar to thoseprovided by S. A. Healy for their work. A copy of theLayne-Western EAV-2/EAV-3 hazard analysisworksheet appears in Figure 3-1. No signaturesappeared on the form. An approved hazard analysiscould not be located for the Layne-Western work relatedto drilling the EAV-2 and EAV-3 shafts, nor were anyhazard analyses performed for the work related to boringthe previous shafts, which began in September 2000.
Figure 3-1. Layne-Western Job Hazard Analysis Worksheet
20
Well drilling is a hazardous activity. It involveshigh-energy mechanical systems, hoisting and riggingcapabilities, rotating machinery, highly-tensioned ropes,cables and chains, noise, chemicals, and structural issues.A hazard analysis addressing this activity would requirethe expertise of engineering personnel as well as craftworkers. However, the inadequate hazard analysisprepared by the Operator focused solely on commonoccupational safety issues, such as slips and falls fromwalking and working surfaces, and contained noengineering or supervisory input.
The hazard analysis processes that were availableto the Operator and the Helper for the drilling operationwere the Layne Christensen Health and Safety Program,the S. A. Healy Safety and Health Manual, and FESHM7010. The Layne Christensen Health and SafetyProgram (used by Layne-Western) did not specify aprocess that would allow the Operator and the Helperto identify and address task-specific hazards of thedrilling operation (i.e., breaking down the operation intosubtasks and associated hazards). The hazard analysisprocess identified in the S. A. Healy Safety and HealthManual also did not provide specific guidance for thedevelopment of task-specific hazard analyses. FESHM7010 indicated that hazard analyses were required forall construction work, and ES&H Administrative Form#17 provided guidance that would be applicable to thedrilling operation. However, FESHM 7010 did notrequire that the guidance in Form #17 be used in thedevelopment of a hazard analysis. Although the Layne-Western drill crew attempted to complete a form titled“Job Hazard Analysis Worksheet,” neither the Fermilab,S. A. Healy, nor Layne-Western ES&H programsprovided complete instructions for developing a hazardanalysis at this level.
Regarding job site reviews, the FAO personnel,Fermilab personnel, NuMI Project constructioncoordinators, and S. A. Healy line managers visited theEAV-2/EAV-3 job site frequently to verify environmentalcompliance and to check on drilling progress. None ofthese personnel identified that the work was beingperformed without an approved hazard analysis, nordid they identify construction safety deficiencies at thejob site.
The S. A. Healy General Superintendent, who wasappointed three weeks before the accident, recognizedthat there was no hazard analysis for the work andinitiated action to have one prepared; however, he tookno action to curtail drilling operations until a hazardanalysis was completed. The previous S. A. HealyGeneral Superintendent took no action to assure that ahazard analysis was prepared. Various ES&H
personnel who visited the Layne-Western job sites overa nine-month period did not identify the absence of ahazard analysis for the work.
The drilling operations were allowed to continuewith numerous hazard analysis program deficiencies.As previously noted, a hazard analysis did not existwhen drilling began and neither the GeneralSuperintendent nor the construction coordinator requiredcompletion of the hazard analysis. Consequently, noCompetent Person was named on the hazard analysisas required. Documentation was unable to be producedwhich demonstrated that tool or equipment inspectionswere conducted by the construction coordinator.
The Board concluded the following:
• The hazard analysis process outlined in the LayneChristensen Health and Safety Program wasincomplete and did not adequately address thisdrilling operation.
• Fermilab and S. A. Healy procedures for requiringand performing hazard analyses of subcontractorsand sub-tier contractors were ineffective.
• The hazard analysis program in place at the time ofthe accident did not evaluate task-specific hazardsassociated with the Layne-Western drillingoperations for the NuMI Project.
• Fermilab and S. A. Healy did not enforce therequirement for preparing a hazard analysis, nordid Layne-Western implement the hazard analysisrequirements for the drilling work.
• Safety and health oversight of the Layne-Westernoperations failed to identify the absence of a hazardanalysis.
3.1.3 Develop and Implement Controls
The objective of developing and implementingcontrols is to identify and provide the full range ofcontrols (i.e., engineering, administrative, and personalprotective equipment) consistent with the level andnature of the hazards to be encountered during taskperformance. The development and implementationof work controls assumes that the contractor hasadequately and completely identified the hazardsassociated with the defined scope of work. The Boardevaluated several aspects of this process, including

21
(1) requirements management and proceduredevelopment, (2) maintenance operations, and (3)general worker safety.
Throughout the Department, contractualrequirements are used to establish the terms andconditions that define DOE safety expectations for itscontractors. DOE Acquisition Regulation (DEAR)970.5204-2 requires contractors to comply with therequirements of applicable Federal, state, and local lawsand regulations in developing and implementing controls,unless the appropriate regulatory agency has granted awaiver in writing. DOE has identified safetyrequirements in rules and DOE orders and hasdeveloped a wide variety of associated technicalstandards, guides, and manuals, and encourages theuse of national consensus technical standards. Inaddition to complying with applicable Federal, state,and local laws and regulations in developing andimplementing controls, as required by DEAR 970.5204-2(a) (List A), the contractor must also comply with therequirements of applicable DOE directives appendedto the contract (List B in DEAR 970.5204-2(b)).
Nonetheless, a number of weaknesses in the pro-cess of communicating safety and health requirementsfrom Fermilab to S. A. Healy and from S. A. Healy toLayne-Western were identified. The weaknesses listedbelow contributed to a work environment where equip-ment use and equipment modifications were performedwithout a comprehensive set of formal procedures toguide these operations:
• Neither Fermilab nor S. A. Healy reviewed andaccepted the Layne-Western ES&H Manual.
• The Fermilab contract with S. A. Healy required allsubcontractors, including sub-tier contractors, to bemanaged in accordance with the S. A. Healy ES&HManual, which invoked FESHM 7010. FESHM7010 was not tailored to address S. A. Healyconstruction sub-tier contractors. Additionally,S. A. Healy had not established a method toimplement the requirements of FESHM 7010.
• The S. A. Healy contract with Layne-Western forconstruction of vent and survey risers invokedrequirements from the FESHM. Specifically,Appendix A of the Layne-Western contract statedthat “All work shall be performed in full accordancewith the Contract Documents for Fermi NationalAccelerator Laboratory’s Project No. 6-7-4.” This
contract did not refer to specific requirements withwhich Layne-Western was expected to comply.
• Although no formalized work controls wereestablished for the EAV-2/EAV-3 job site, personnelwere expected to comply with requirements stipulatedin the Layne Christensen Health and Safety Program.This document was not reviewed and accepted byS. A. Healy, nor was it located at the job site.Observations at the scene and personnel interviewsindicated that full compliance with electrical safety,fall protection, and hoisting and rigging requirementswas not ensured. As stated by Layne-Westernpersonnel, many of the safe work proceduresreferenced in the hazard analysis section of the LayneChristensen ES&H Manual do not exist.
The Board evaluated maintenance operations andworker safety associated with the drilling work. Anequipment maintenance program was not specificallyidentified as a contractual requirement between S. A.Healy and Layne-Western. Nonetheless, the nature ofthe work, the inherent hazards, and the type ofequipment used would indicate the need for a rigorous,formalized maintenance program.
Layne-Western has a limited equipmentmaintenance program. Records indicated that thecompany expected the drilling rig crew to performrepairs in the field, including structural welding, for whichthey were not formally trained or qualified. When thecrew welded the eyebolt to the hydraulic cylinder pistonrod in 1999, no engineering evaluation was performedto determine whether the strength of the weld wasequivalent to the threaded connection it apparentlyreplaced.
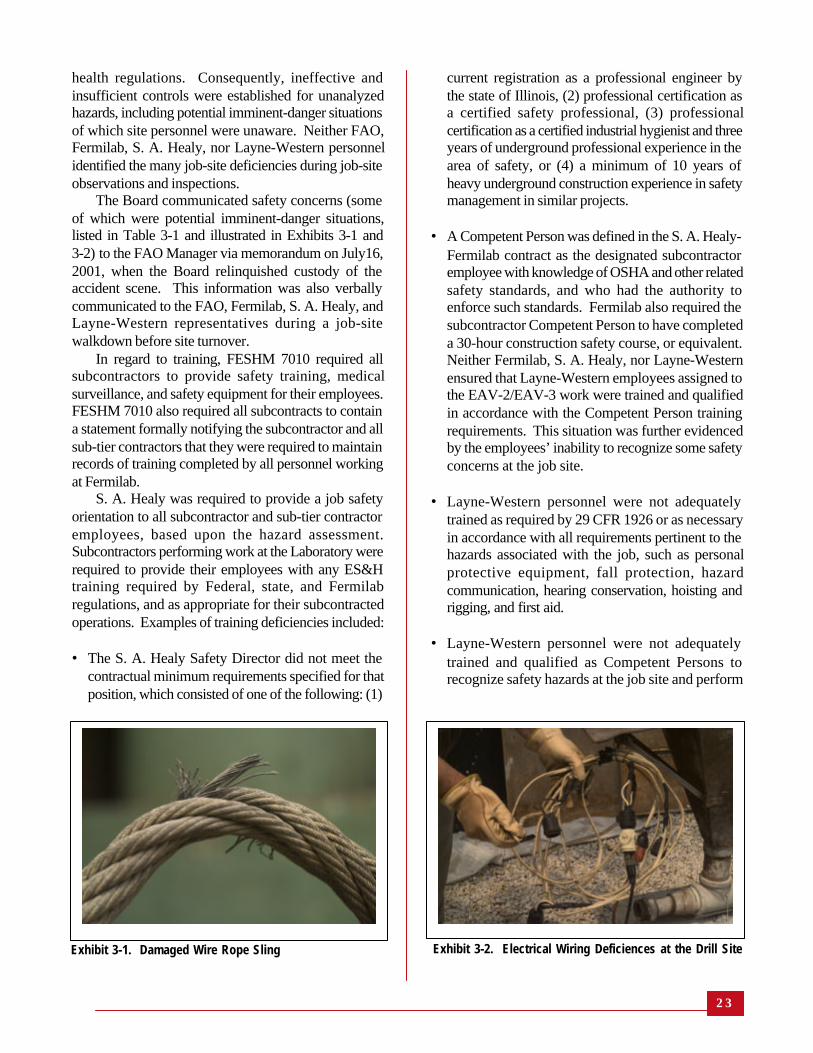
A Layne-Western Field Superintendent and theOperator conducted a drill rig safety inspection at theEAV2/EAV-3 job site in September 2000, and theOperator conducted a similar inspection in May 2001,approximately one month before the incident. TheOperator’s safety inspection was incomplete; forexample, it failed to cover all required inspection itemsor identify safety deficiencies and potential imminent-danger situations at the job site. The safety inspectiondeficiencies and safety conditions at the job site wereindicative of a work environment that was not attentiveto proper health and safety practices. Examples of safetydeficiencies the Board discovered at the job site arelisted in Table 3-1.
Management processes were not implemented toassure program compliance with applicable safety and

22
Equipment
Compressor Trailer
Mist PumpPortable Generator
Wire Rope Slings
Synthetic Web Slings
Welded Alloy Steel Chains
Inadequate Eelectrical Installations
Inadequate Fall Protection
Inadequate Walking/workingSurfaces
Deficiency
• Bald tires• Gouged tires• Bent wheel rim• No barricades/fall protection on work platforms• Leaking fuel/oil• Inadequate guarding on rotating equipment• Rotating equipment not guarded• Leaking oil• Makeshift lifting attachment – no load rating• Inadequate Storage• Compressed eyes• Birdcaging• Kinks• Crushing• Abrasions• Broken cores• Shortened/attached to hook by knotting• No regular inspections• No rated capacity – damaged slings not removed from service• Markings and codings illegible• Discoloration• Distortion• Cuts• Abrasions• Damaged slings not removed from service• No regular inspections• Missing permanently affixed, durable identification of size, grade,
rated capacity and sling manufacturer• Deformed links• Electrical extension cords not designed for construction applica-
tions (hard or extra hard usage)• Electrical extension cords not protected from damage (damaged
extension cords on the ground)• Ground fault circuit interrupters not used• Makeshift light string – leads inadequately terminated• Insulation worn off power cord for submersible sump pump• Extension cord not protected from damage when run through
trailer door pinch point• Fall protection not used when climbing or working at or above six
feet• Fall protection equipment (harness) not fit for use• Work surfaces at or above six feet not guarded• Wooden pallets used for walking surfaces present tripping hazard• Slipping hazards due to oil or other fluids on rig/equipment deck
Table 3-1. Examples of Safety Deficiencies at the Drilling Site
2 3
health regulations. Consequently, ineffective andinsufficient controls were established for unanalyzedhazards, including potential imminent-danger situationsof which site personnel were unaware. Neither FAO,Fermilab, S. A. Healy, nor Layne-Western personnelidentified the many job-site deficiencies during job-siteobservations and inspections.
The Board communicated safety concerns (someof which were potential imminent-danger situations,listed in Table 3-1 and illustrated in Exhibits 3-1 and3-2) to the FAO Manager via memorandum on July16,2001, when the Board relinquished custody of theaccident scene. This information was also verballycommunicated to the FAO, Fermilab, S. A. Healy, andLayne-Western representatives during a job-sitewalkdown before site turnover.
In regard to training, FESHM 7010 required allsubcontractors to provide safety training, medicalsurveillance, and safety equipment for their employees.FESHM 7010 also required all subcontracts to containa statement formally notifying the subcontractor and allsub-tier contractors that they were required to maintainrecords of training completed by all personnel workingat Fermilab.
S. A. Healy was required to provide a job safetyorientation to all subcontractor and sub-tier contractoremployees, based upon the hazard assessment.Subcontractors performing work at the Laboratory wererequired to provide their employees with any ES&Htraining required by Federal, state, and Fermilabregulations, and as appropriate for their subcontractedoperations. Examples of training deficiencies included:
• The S. A. Healy Safety Director did not meet thecontractual minimum requirements specified for thatposition, which consisted of one of the following: (1)
current registration as a professional engineer bythe state of Illinois, (2) professional certification asa certified safety professional, (3) professionalcertification as a certified industrial hygienist and threeyears of underground professional experience in thearea of safety, or (4) a minimum of 10 years ofheavy underground construction experience in safetymanagement in similar projects.
• A Competent Person was defined in the S. A. Healy-Fermilab contract as the designated subcontractoremployee with knowledge of OSHA and other relatedsafety standards, and who had the authority toenforce such standards. Fermilab also required thesubcontractor Competent Person to have completeda 30-hour construction safety course, or equivalent.Neither Fermilab, S. A. Healy, nor Layne-Westernensured that Layne-Western employees assigned tothe EAV-2/EAV-3 work were trained and qualifiedin accordance with the Competent Person trainingrequirements. This situation was further evidencedby the employees’ inability to recognize some safetyconcerns at the job site.
• Layne-Western personnel were not adequatelytrained as required by 29 CFR 1926 or as necessaryin accordance with all requirements pertinent to thehazards associated with the job, such as personalprotective equipment, fall protection, hazardcommunication, hearing conservation, hoisting andrigging, and first aid.
• Layne-Western personnel were not adequatelytrained and qualified as Competent Persons torecognize safety hazards at the job site and perform
Exhibit 3-1. Damaged Wire Rope Sling Exhibit 3-2. Electrical Wiring Deficiences at the Drill Site

24
hazard analyses, or to abate the several potentialimminent-danger situations identified by the Boardfollowing the accident. Although recent efforts weremade by Fermilab and S. A. Healy to increasesubcontractor knowledge of hazard analysis, theinformation was not shared with Layne-Westernemployees since they were not included in the twosafety stand-downs and the related training.
The Board concluded that the occupational safetyand health policies, programs, and procedures forworker safety and health were not routinelyimplemented or enforced.
3.1.4 Perform Work Within Controls
Controls must be identified and implemented beforestarting work. Examples where necessary controls werenot implemented on the Layne-Western EAV-2/EAV-3drilling activity being performed at the time of theaccident included:
• S. A. Healy did not impose controls equivalent tothose specified by FESHM 7010 to assure thatLayne-Western would operate safely. S. A. Healydid not require Layne-Western to perform a numberof expected operations equivalent to Fermilab ES&Hcontract submittal requirements specified in FESHM7010, before initiation of work.
• S. A. Healy did not require Layne-Western tosummarize its past safety performance as requiredunder “Qualification of Subcontractors.” Layne-Western did not submit a copy of its ES&H Plan asrequired under FESHM 7010, “Safety Plan Review.”Layne-Western did not complete a pre-constructionchecklist equivalent to ES&H Administrative Form#19.
• The hazard analyses included in the Layne-WesternSafety and Health Manual were generic and nottailored to the specific drilling activity for EAV-2/EAV-3.
• The hazard analysis generated the day of the accidentdid not address either the hazards of the drillingoperations or the appropriate controls, nor was itreviewed or approved.
• Layne-Western performed work from September 25,2000, until the day of the accident without a hazardanalysis.
• Fermilab procedures required current excavationpermits and burn permits to be attached to the hazardanalysis. These permits were not attached to theLayne-Western job hazard analysis. Although anexcavation permit was issued for the EAV-2/EAV-3drilling activity on October 6, 2000, the permitexpired seven days after it was issued, and the permitwas not extended or updated.
• Fermilab and S. A. Healy did not compare the workoperations being conducted to the hazard analysisgenerated on the day of the accident to verify thatsafety hazards were adequately identified andappropriate controls established. Evidence indicatedthat neither the FAO, Fermilab, S. A. Healy, norLayne-Western line and safety management hadreviewed the work activity to evaluate occupationalsafety hazards, hazard control and abatement, orperformance of work since Layne-Western begandrilling operations on September 25, 2000.
• Pre-job briefings were informal, not documented,and not effective in conveying the extent of hazards.A work package with a step-by-step review processwas not used.
• Work was not performed using appropriate controls,and actions that would be expected as a condition offormally authorizing initiation of work were notimplemented.
The Board concluded that because the scope ofwork was not adequately defined, task-specific hazardscould not be analyzed and work could not be performedwithin controls.
3.1.5 Feedback and Improvement
Feedback and improvement processes for Fermilabsubcontractor construction projects consisted of thefollowing mechanisms: assessment processes, analysisof performance information, reporting DOE accident/incident information, corrective action processes, andlessons-learned processes. These mechanisms formedthe core of a continuing improvement process forFermilab subcontractor construction projects.
The Office of the Deputy Assistant Secretary forES&H Oversight had responsibility for performingindependent ES&H oversight of DOE sites. This officehad not performed oversight of Fermilab or the NuMIProject.

25
The Office of High Energy and Nuclear Physicsin the Office of Science had the responsibility for theprogrammatic and technical overview of the NuMIProject. Since November 1998, the Office ofConstruction Management Support within the Officeof Science had conducted six reviews of the NuMIProject, including ES&H. These reviews includedES&H recommendations to the Fermilab Director,although they were not communicated in ISM terms.
Subsequent reviews by the Office of ConstructionManagement Support evaluated the effectiveness of theactions to address the recommendations of the previousreview. However, corrective actions addressingrecommendations made by the Office of ConstructionManagement Support were not tracked in the FermilabEnvironment Safety Health Tracking (ESHTRK)database, or in any other database.
No corrective action plans were developed, althoughsome corrective actions were undertaken. For example,the draft May 22-24, 2001, review report indicated thatthe Fermilab organizational structure for the NuMITunnel and Halls Project was “complex and unwieldy,”and that responsibilities and authorities were “confused,and a number of people involved do not have relevantunderground construction experience.” The reviewreport also noted that the current management structure“is not effective for managing this critical stage of theS. A. Healy tunnels and halls construction contract.” Areorganization was under way at the time of the accident.
The Chicago Operations Office Safety andTechnical Services organization provided ES&H supportto the FAO, as requested. The Chicago OperationsOffice Manager did not perform independent ES&Hoversight of Chicago Operations Office lineorganizations. Since participating in the October 1999combined Phase I and II ISM verification of Fermilab,Safety and Technical Services had not been asked toprovide technical support to the FAO, or independentoversight on behalf of the Chicago Operations OfficeManager. In particular, Safety and Technical Serviceshad not been asked to provide support of safetyoversight of NuMI Project construction operations orreview of subcontractor safety management at Fermilab.
The Office of Science Functions, Responsibilities,and Authorities Manual, dated June 30, 2000, identifiedthe Office of Science as primarily involved in providingdirection and defining scope of work, while OperationsOffice managers oversee their contractors’ performancein analyzing hazards, developing and implementingcontrols, providing feedback, and pursuingimprovement. The document noted that the Chicago
Operations Office Manager had responsibility for “day-to-day” oversight of contractor operations, but thatorganizational elements of the Office of Science hadresponsibility for appraising the performance of theChicago Operations Office Manager and maintaining“executive-level” awareness of contractor operationalperformance.
In describing how the Office of Science exercisedthe functions, responsibilities, and authorities formeasuring the adequacy of line management oversight,the document noted that monitoring of the ChicagoOperations Office Manager and associated contractorswould be accomplished by (1) reviewing informationprovided by the Chicago Operations Office; (2) whenappropriate, participating in Chicago Operations Officeappraisals; and (3) conducting onsite reviews of ChicagoOperations Office performance, including verificationof appraisal of the contractors.
FAO had line management oversight responsibilityfor programs, projects, and facilities at Fermilab. Forthe NuMI Project, the FAO Manager assigned, withthe approval of the Director of High Energy Physics, aproject manager who was responsible for day-to-dayexecution of the project. The DOE NuMI ProjectManager’s responsibilities included monthly projectperformance reviews and assurance that the NuMIProject complied with ES&H and contractingregulations. He performed bi-weekly inspections ofthe project using a standard form to document ES&Hconcerns. The concerns identified during each inspectionwere reviewed during subsequent inspections to ensurethat corrective actions were implemented. Inspectionsconducted by the DOE NuMI Project Manageraddressed general project safety, but lacked in-depthinformation on the status of compliance with 29 CFR1926 and Fermilab requirements. Inspection forms werecontained in project files but were not used as input tothe ESHTRK system or any other project database.An FAO staff member performed two inspections ofthe EAV-2/EAV-3 job site, but these inspectionsconcentrated on environmental protection issues andwere not documented. FAO operational awarenessreviews did not cover the NuMI Project. Figure 3-2displays the DOE organizational relationships formanagement of the NuMI Tunnels and Halls Project.
Feedback and improvement processes at Fermilabwere described in the Fermilab Integrated SafetyManagement Plan, Revision 3, August 2000. Forsubcontractor construction projects, performanceevaluations and self-inspections were used as feedbackmechanisms. The FESHM required that all
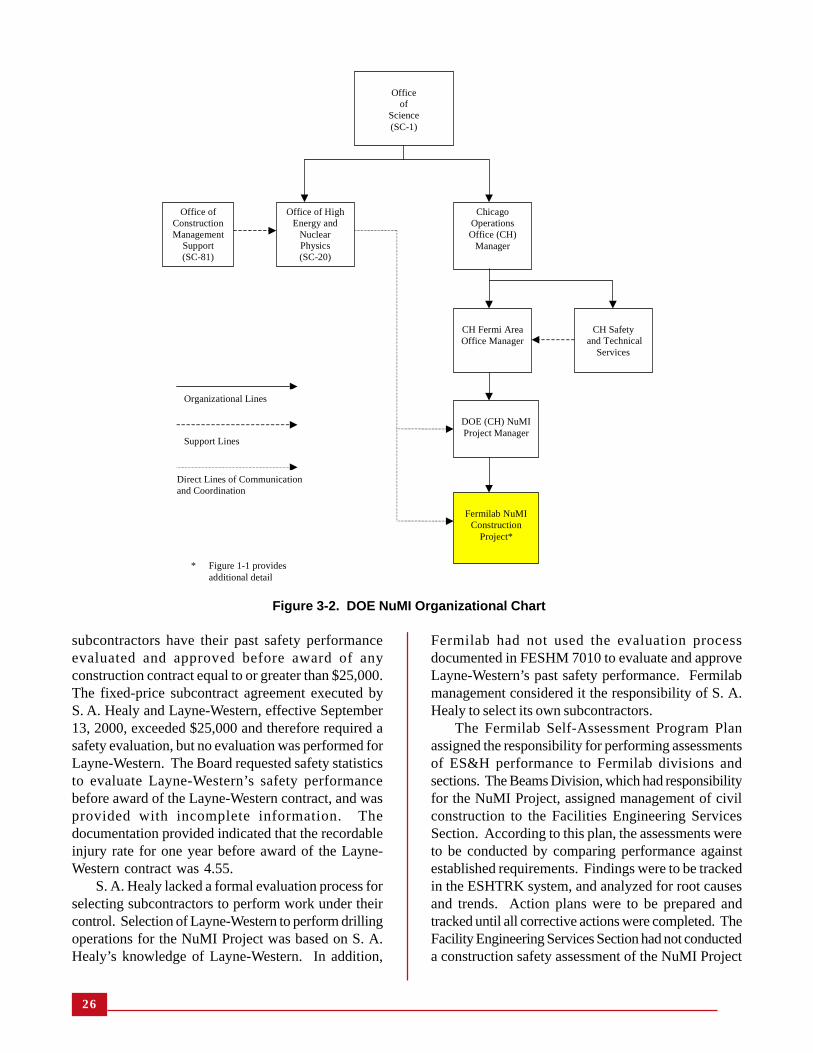
26
subcontractors have their past safety performanceevaluated and approved before award of anyconstruction contract equal to or greater than $25,000.The fixed-price subcontract agreement executed byS. A. Healy and Layne-Western, effective September13, 2000, exceeded $25,000 and therefore required asafety evaluation, but no evaluation was performed forLayne-Western. The Board requested safety statisticsto evaluate Layne-Western’s safety performancebefore award of the Layne-Western contract, and wasprovided with incomplete information. Thedocumentation provided indicated that the recordableinjury rate for one year before award of the Layne-Western contract was 4.55.
S. A. Healy lacked a formal evaluation process forselecting subcontractors to perform work under theircontrol. Selection of Layne-Western to perform drillingoperations for the NuMI Project was based on S. A.Healy’s knowledge of Layne-Western. In addition,
Fermilab had not used the evaluation processdocumented in FESHM 7010 to evaluate and approveLayne-Western’s past safety performance. Fermilabmanagement considered it the responsibility of S. A.Healy to select its own subcontractors.
The Fermilab Self-Assessment Program Planassigned the responsibility for performing assessmentsof ES&H performance to Fermilab divisions andsections. The Beams Division, which had responsibilityfor the NuMI Project, assigned management of civilconstruction to the Facilities Engineering ServicesSection. According to this plan, the assessments wereto be conducted by comparing performance againstestablished requirements. Findings were to be trackedin the ESHTRK system, and analyzed for root causesand trends. Action plans were to be prepared andtracked until all corrective actions were completed. TheFacility Engineering Services Section had not conducteda construction safety assessment of the NuMI Project
Figure 3-2. DOE NuMI Organizational Chart
Officeof
Science(SC-1)
Office of HighEnergy and
NuclearPhysics(SC-20)
Office ofConstructionManagement
Support(SC-81)
ChicagoOperationsOffice (CH)
Manager
CH Fermi AreaOffice Manager
DOE (CH) NuMIProject Manager
Fermilab NuMIConstruction
Project*
CH Safety and Technical
Services
Organizational Lines
Support Lines
Direct Lines of Communicationand Coordination
* Figure 1-1 providesadditional detail

27
to evaluate the performance of S. A. Healy and Layne-Western against requirements contained in the Fermilab-S. A. Healy contract, FESHM, or 29 CFR 1926.
FESHM 7010 required construction subcontractorsafety performance to be monitored using inspectionsperformed by the construction coordinators inaccordance with the Fermilab SubcontractorConstruction Safety Program. The SubcontractorConstruction Safety Program in FESHM 7010 requiredthe ES&H Section and/or the Senior Safety Officer ofthe landlord division—in this case, the FacilityEngineering Services Section—to perform oversightinspections of construction sites.
Program requirements stipulated that non-conformance with safety standards must bedocumented, along with the corrective actionsdetermined by line managers. Inspections andsurveillances of work performed by S. A. Healy andLayne-Western were conducted by both the NuMIProject construction coordinators and a safety engineerfrom the ES&H Section. The inspections of Layne-Western focused on environmental issues and notoccupational safety. FESHM 7010 also required thatrandom inspections of subcontractor owned tools maybe performed by the construction coordinators andES&H Section construction safety personnel. Noinspections of contractor-owned tools associated withthe Layne-Western drill rig were performed either bythe construction coordinators or by Fermilab ES&H.
In accordance with their company safety manuals,both S.A Healy and Layne-Western assignedresponsibilities to safety personnel to conduct job sitesafety inspections. The S. A. Healy Safety Officer hadnot recorded observations resulting from daily safetyinspections. The Operator, who was the designatedCompetent Person and safety supervisor, documentedtwo semi-annual inspections of the drilling rig. Layne-Western was unable to provide documentation of therequired daily inspections, nor was there evidence thatany inspections identified the existing safety deficienciesat the job site. Prior to the accident, Fermilab personnelhad not documented any job site safety inspections ofdrilling operations by Layne-Western.
The Board analysis of feedback and improvementprocesses indicated that:
• The requirements for ES&H line managementoversight by the Office of Science Functions,Responsibilities, and Authorities Manual were notbeing fully implemented.
• Since participating in the October 1999 combinedPhase I and II ISM verification of Fermilab, Safetyand Technical Services Support was not requestedto provide technical support to the FAO, or to performindependent oversight on behalf of the ChicagoOperations Office Manager.
• The Facility Engineering Services Section had notconducted any requirements-based assessments ofthe NuMI Project.
• The DOE NuMI Project Manager performed ES&Hinspections and documented the results of theinspections of the NuMI Project, but the inspectionresults were not incorporated into the ESHTRKdatabase or another system to show trends in theresults of the inspections.
• Layne-Western’s past safety performance was notevaluated before awarding their contract.
• FAO, Fermilab, S. A. Healy, and Layne-Westerninspections of work site safety at the EAV-2/EAV-3job site were not rigorous, formal, or documented.Consequently, important safety information thatwould have provided indications of the degradedcondition of the drill rig, safety and healthnoncompliance, and adverse trends was not collected,compiled, and provided to management.
The Board concluded that Department of Energyand Fermilab oversight programs had not been effectivein identifying fundamental weakness in Fermilabsubcontractor construction safety and health programs.
In evaluating how the site had analyzed performanceinformation, the Board reviewed recent occurrences atFermilab to determine whether precursor events existedbefore the accident. Fermilab had more than 20occurrence reports between January 1, 1998, and theday of the accident, 6 of them related to constructionoperations (in one report there are two separateoccurrences yielding seven construction safetyoccurrences). The Board identified similar underlyingcauses for all six construction occurrences, which aresummarized in Table 3-2:
• Work planning and control processes wereinadequate to perform work within controls.
• Inadequate hazard analyses were performed.

28
Accident
Date
HazardAnalysis and
Control
Proceduresand Procedure
Adherence
“Skill of theCraft”
Training andCompetencies
Pre-job Briefing
Use of MSDS*
Provision anduse of PPE*
LessonsLearned
CorrectiveActions
Institutionaliza-tion and
communicationof hazard and
controls
Management/SupervisoryInvolvement/
ControlOversight
Type B AccidentElectrical Arc
Blast at BuildingF-Zero
October 22,1997
Informal – expertbased No JHA*
“RoutineMaintenance”
Inadequate, noprocedure used
Over reliance
Inadequate forhazard
Inadequate toidentify and
control hazardand response
NA*
Inadequate PPE& staging
Inadequateresponse to
previous events
Not adequatelydefined
institutionalized orcommunicated
ISM notimplementedinadequateoversight/
accountability
Type B AccidentFlammable Liquid
Fire/Explosion
September 4,1998
Informal – expertbased No JHA
“RoutineMaintenance”
Inadequate, noprocedure used
Over reliance
Not trained onhazard
No safety briefing
MSDS not usedfor hazardsanalysis or
control
Inadequate PPE
Inadequateresponse to
previous events
Not adequatelydefined
institutionalized orcommunicated
ISM notimplementedInadequateoversight/
accountability
Constructionsubcontractor
saw cutelectricalconduits
August 28,1999
Informal –expert based
No JHA“Routine
Maintenance”
Inadequate, noprocedures
used
Over reliance
Inadequate onuse of scanning
equipment
No safetybriefing
NA
NA
Inadequateresponse to
previousevents
Not adequatelydefined
institutionalizedor communi-
cated
Inadequatemanagement ofwork planning
and control
Falling Rockinjured worker inNuMi Target Hall
January 31,2001
Informal – expertbased
No JHA“Routine
Maintenance”
Not followed
Over reliance
Inadequate onhazard and
controls
No safety briefing
NA
NA
Inadequateresponse to
previous events
Hazards ignoredand controls not
followed
Inadequatemanagement
oversight controlof work and
hazard controlsand processes
NuMI constructionworkers received
2nd degreechemical burns to
legs
March 14,2001
Informal –expert based
No JHA“Routine
Maintenance”
Inadequate, notfollowed
Over emphasis
Inadequatetraining on
hazard
No safety briefing
MSDS not usedfor hazardanalysis or
control
InadequatePPE
Inadequateresponse to
previous events
Requirements notinstitutionalized or
communicated
Inadequatemanagement ofwork planning
and control
NuMIconstruction
worker receivedcontusion to face,
riggingdeficiencymoving
transformer
June 2,2001
Informal – expertbased No JHA
“RoutineMaintenance”
Inadequate, noprocedure used
Over emphasis
Inadequateimproper rigging
No safetybriefing
NA
NA
Inadequateresponse to
previous events
Not adequatelydefined or
communicated
Inadequatemanagement ofwork planning
and control (Notreported)
NuMIconstruction
rigging deficiency,worker received
broken ribs
June 13,2001
Informal –expert based
No JHA“Routine
Maintenance”
Inadequate, noprocedure used
Over emphasis
Inadequateimproper rigging
No safety briefing
NA
NA
Inadequateresponse to
previous events
Not adequatelydefined or
communicated
Inadequatemanagement ofwork planning
and control(Safety stand-
down directed byFermi)
Equipmentfailure causingPersonal Injury
and worksuspension
June 21,2001
Informal – expertbased
No JHA“Routine
Maintenance”
Inadequate, noprocedure used
Over reliance
Inadequatetraining on
hazard analysis
No safetybriefing
NA
NA
Inadequateresponse to
previous events
Not adequatelydefined or
communicated
Inadequatemanagement
of work planningand control
* JHA = Job Hazard AnalysisMSDS = Material Safety Data SheetNA = Not ApplicablePPE = Personal Protective Equipment
Table 3-2. Analysis of Previous Fermilab Construction Occurrences

29
• Procedures were inadequate or not used to performwork.
• Corrective actions developed in response to previouslyidentified events did not effectively preventrecurrence of similar problems.
The Board concluded that Fermilab had a seriesof construction safety events with similar systemiccauses before the accident. Fermilab did not analyzeavailable construction occurrences to identify trendsand root causes. As a result, the systemicweaknesses underlying these events were neitheridentified nor addressed.
The Board evaluated how the site reported accidentinformation. A majority of the Fermilab constructionoccurrences involved personnel injuries that requiredmedical treatment and, in some cases, hospitalization.Even though most of these occurrences met thesignificance threshold for reporting in the DOEComputerized Accident/Incident Reporting System(CAIRS), none of these occurrences were found inthe system.
In addition, the Board evaluated FermilabConstruction Subcontractor Lost Workday Case ratesto identify reporting and construction trends associatedwith this data. The Board used CAIRS Lost WorkdayCase rates from March 1993 to June 2001. This timeperiod includes construction of Fermilab’s two majortunneling projects, the Main Injector Tunnel and NuMITunnels and Halls. The Board compared the LostWorkday Case rate information for FermilabConstruction Subcontractors provided to the Boardduring the inbriefing to Lost Workday Case rateinformation in CAIRS for the period August 27, 1998,to September 15, 2000. Although Fermilab data shows750 days without a lost workday case during this timeperiod, the Board identified that a subcontractor pipefitter dislocated his shoulder on November 11, 1998,resulting in 6 lost workdays. Additionally, for six monthsduring the same period of time, Fermilab did not performany fixed price construction work, thus minimizing thepossibility that a lost workday case would have beenexperienced by subcontractors. Finally, a review ofLost Workday Case rates for the first six months ofconstruction activities on each tunneling project indicatedthe Lost Workday Case rate approached 20 during theinitial phases of construction as shown in Figure 3-3.
Fermilab Construction Subcontractors Lost Workday Case Rate
Mar-93
Jun-93
Mar-94
Jun-94Sep-94
Mar-95
Sep-95
Mar-00
Sep-00
Dec-00
Mar-01
Jun-01
Dec
-97
Dec-95
Jun-95
Mar
-98
Dec
-98Sep
-98
Jun-
98
Jun-
99
Mar
-99
Sep
-99
Dec-99
Jun-96
Mar-97
Dec
-96
Sep
-96
Sep
-97
Jun-
97
Sep-93Dec-93
Mar-96
Dec-94
Jun-000
10
20
30
40
50
60
Date by Quarter
LWC
Rat
e
Series1
Main Injector Tunnel - $16 Million NuMI Tunnelsand Halls
- $38 Million
NTP
Figure 3-3. Fermilab Construction Subcontractors Lost Workday Case Rate

30
The Board concluded that Fermilab had notconsistently and effectively reported accident andinjury information pertaining to constructionsubcontractors into CAIRS.
To determine whether corrective actions wereeffective in preventing recurrence of similar problems,the Board reviewed a sample of Fermilab correctiveaction plans. The plans included two Type B accidentinvestigations conducted by the Chicago OperationsOffice for accidents involving subcontractors thatoccurred on October 22, 1997, and September 4, 1998,and the Fermilab investigation report for the NuMIaccident of March 12, 2001. Both Type B accidentinvestigations identified causal factors that recurred inthis accident as shown in Table 3-2. The site developedand implemented corrective actions for the causal factorsfor both Type B accidents, and by December 22, 2000,the FAO had verified that all were closed.
Fermilab had performed investigations of othersafety events that occurred on the NuMI Project. TheBoard reviewed the report of the March 12, 2001,concrete placement-burn accident, and the January 31,2001, accident where a subcontractor was struck by afalling rock in the NuMI Tunnel, to understand theprocess for identifying and implementing correctiveactions for these investigations. The Fermilab accidentinvestigation team’s report indicated that the safety plan:(1) was not being fully implemented or enforced,(2) lacked an effective written fall protection and scalingprogram, (3) did not address corrective actions andlessons learned, and (4) did not assign responsibility fora corporate safety auditing function.
In a memorandum to the Fermilab Director datedApril 30, 2001, the Fermilab investigation teamrecommended that S. A. Healy implement correctiveactions to address these deficiencies. Fermilabincorporated the corrective actions into the ESHTRKsystem. However, according to an ESHTRK reportdated June 29, 2001, every action item related to thisinvestigation still remained open.
A Harza consultant performed independent safetyreviews and audits of underground construction workand aboveground work related to the tunnel construction,except for the Layne-Western drilling operations. Fouraudits of S. A. Healy during 2001 identified deficienciesin the company’s hazard analysis program. Reviewsand audit reports documented general comments,deficiencies, and suggestions for improvement. Onereport dated March 19, 2001, to March 21, 2001,included a trend analysis evaluating project-relatedinjuries. The consultant recommended that S. A. Healy
develop a proactive program to address areas thatcontributed increased recordable injuries on the NuMIProject. Results of these reviews and audits were notinput to the ESHTRK system, and no corrective actionplan was developed to address the recommendationsresulting from the trend analysis.
The causal factors identified in two previousaccident investigations contributed to the June 21, 2001,accident. Recurrence of the causal factors in thisaccident indicated that Fermilab corrective actionprocesses were ineffective and did not assure necessaryimprovement of construction subcontractor safetymanagement systems.
The Board concluded the following:
• Corrective actions implemented by line managementin response to identified deficiencies, adverse trends,occurrence reports, and recurring events—including improvements in subcontractor safetymanagement systems and processes—were noteffective in preventing recurrence of thesedeficiencies.
• NuMI Project line management had neitherestablished an effective formalized process to captureand track ES&H-related deficiencies and associatedcorrective actions from investigations, inspections,and audits, nor implemented mechanisms, such asindependent verification and performance-basedevaluations, to ensure that corrective actions weretimely, complete, and effective.
The Board reviewed Fermilab mechanisms forcommunication, dissemination, and use of lessonslearned involving construction subcontractors and sub-tier contractors. The Subcontractor SafetySubcommittee (S-3) and processes of FESHM 7010and FESHM 7020, Subcontractor Safety – Other ThanConstruction (Interim), were used to provide aninterface between Fermilab and the subcontractor forsharing lessons learned from both onsite and offsiteincidents. The Board reviewed the minutes of the S-3committee meetings from March 2000 to April 2001.The minutes indicated that the meetings were usefulfor facilitating communication between Fermilabdivisions, but no subcontractors or sub-tier contractorsattended the meetings. Additionally, the minutesindicated that there were no discussions of lessonslearned from either onsite or offsite incidents, althoughnumerous construction-related OSHA-recordableinjuries occurred on the NuMI Project during this time

31
period. The focus of these meetings indicates missedopportunities to discuss lessons learned.
The processes of FESHM 7010 and FESHM 7020afforded subcontractors many opportunities to interfacewith Fermilab safety personnel while planning andexecuting work. However, these chapters lackedguidance and direction regarding the use of lessonslearned for subcontractors.
Section 4.5 of the Fermilab ISM Plan addressedthe core function “Feedback and ContinuousImprovement.” One of the mechanisms that Fermilabused to implement this core function was the Fermilablessons- learned program. Central to this program wasthe use of the Fermilab ES&H website. The Boardsearched the website and found many construction-related lessons learned applicable to NuMI Projectsubcontractor construction safety management systems.Of particular note are February 23, 1998, lessons learnedfrom the Idaho National Engineering and EnvironmentalLaboratory discussing the use of formal jointcollaborating safety surveillances to prevent accidents,increase communications between general and sub-tiercontractors, and promote compliance with OSHArequirements. Use of this lesson learned by NuMITunnels and Halls line management would have assistedin identifying OSHA deficiencies, improvingcommunications between organizations, and formalizingthe process of obtaining safety information for trackingand trending.
Similarly, other safety lessons-learned informationreadily available to Fermilab from internal and externalsources was never communicated to either Layne-Western or S. A. Healy.
The International Association of DrillingContractors website contained public information thatdiscussed safety measures to be employed for operatingdrilling equipment. The information addressed theproper positioning of a drilling crew when making orbreaking pipe string. Use of this lesson learned mighthave mitigated or prevented the Operator injury.
The Board concluded that Fermilab processes wereineffective in ensuring that lessons learned wereunderstood and applied by construction subcontractorsand sub-tier contractors.
During the investigation, Layne-Western was unableto provide a variety of records and documents requestedby the Board, indicating a lack of rigor and formality inmanaging safety documents. The following documentsrequired by OSHA, DOE, and/or Fermilab were notgenerated or maintained:
• Hazard analyses
• Inspection records/equipment maintenance records
• Training records for training associated withCompetent Persons, site orientation, hazardcommunications, personal protective equipment, fallprotection, hazard assessment, and ladder safety
• Welding, cutting, and brazing permit requirements
• Fire watch training records
• Inspection requirements for slings
• Hazardous energy isolation records
• Work and excavation permits
• Welder qualification records
• Rigger qualification records.
The Board concluded that management had notenforced requirements for maintenance of recordsdocumenting the conduct of hazards analyses, inspec-tions, training, and permitting.
3.1.6 Management Systems
Integrated safety management was first introducedat Fermilab in 1997, and the system has evolved sincethat time to incorporate improvements. The programwas most recently changed in August 2000 toincorporate changes suggested by a combined Phase Iand Phase II ISM verification review that wascompleted in October 1999. The verification team notedtwo key opportunities for improvement among thoselisted in the verification report, the hazard analysisprocess and feedback and improvement, andrecommended that they be given high priority.
The Office of Science conducted a review of theNuMI Project in May 2001. That review characterizedthe management structure for the NuMI Project as noteffective and concluded that responsibilities andauthorities were “confused.” The organizationalstructure for controlling the NuMI constructionsubcontractor provided several parallel lines of authority.The report provided a number of examplesdemonstrating that contract requirements were not

32
followed and that ISM was not embodied in the safetyculture. Moreover, the impact of not instituting aneffective ISM program was highlighted by the series ofinjuries that occurred at the NuMI Project since January2001. Those injuries, taken collectively, amounted toa breakdown in all of the ISM core functions and guidingprinciples.
The Board also noted deficiencies in all componentsof ISM as applied to the NuMI Tunnels and HallsProject. For example, responsibilities were not clearlyassigned, safety training was insufficient, safetyprograms and procedures were deficient, and, oversightwas inadequate to validate implementation of the fivecore functions of ISM.
Fermilab demonstrated a lack of clarity in contractrequirements and their subsequent flowdown toconstruction subcontractors and sub-tier contractors.The absence of clarity was exemplified by theinconsistent responsibilities of construction coordinators.Under FESHM 7010, NuMI construction coordinatorswere assigned responsibilities for ensuring thatconstruction operations were completed in accordancewith the safety plan and the hazard analysis. Thisassignment of responsibility was inconsistent withCondition 4.2 of the Harza contract with Fermilab,which stated, in part, that Harza “shall not have controlof and shall not be responsible for safety.” However,Sections 2.4 and 2.5 and Exhibit A of the contractrequired Harza construction coordinators to accomplishsafety audits. This dichotomy contributed to NuMIconstruction coordinators not having a clearunderstanding of their safety oversight responsibilities.The ability of management to effectively manage theNuMI Project, including the ability to enforcecompliance with contracts, was compromised byunclear lines of authority in the project organization.Fermilab and S. A. Healy management had not clearlyand properly communicated safety responsibilities totheir staffs.
Fermilab and S. A. Healy management also failedto ensure that individuals involved with hazard analysisfor the NuMI Project had the necessary knowledgeand skills to perform their jobs safely. They failed toadminister controls to ensure that effective hazardanalysis would be performed on the NuMI constructionoperations. The S. A. Healy contract with Fermilabrequired hazard analyses for the operations of S. A.Healy and its subcontractors. Fermilab managersexpected S. A. Healy and its subcontractors toadminister hazard analysis programs in accordance withthe requirements in FESHM 7010, but the Fermilabcontract with S. A. Healy did not invoke this manual or
make it clear that responsibilities and procedures inFESHM 7010 applied to subcontractors of S. A. Healy.The term subcontractor, as used in this document,was applicable to the construction contractors ofFermilab, but was not tailored to apply to contractorsof S. A. Healy, such as Layne-Western.
The Chicago Operations Office Managerdelegated line oversight responsibility as described inDOE Policy 450.5, Line Environment, Safety andHealth Oversight, to the FAO Manager, but did notprovide independent evaluations consistent with DOEoversight policy as described in DOE Order 414.1A,Change 1, Quality Assurance.
FAO and the NuMI Project management’s failureto correct previously identified deficiencies inmanagement systems contributed to continuingperformance deficiencies. Neither organization madesure that corrective actions were effective in preventingadditional accidents, or that common causal factorsrelated to the ISM core functions and guiding principleswere effectively addressed. Specifically, neitherorganization identified that Layne-Western performeddrilling operations from September 2000 until June 21,2001, without a hazard analysis, or that responsibilitiesfor preparation and approval of hazard analyses werenot clearly assigned. The FAO did not assign a staffmember to monitor the safety of Layne-Western drillingoperations until June 2001, even though drilling had beenin progress since the previous fall, and the review ofLayne-Western operations by this staff member didnot focus on safety. The S. A. Healy Safety Directorand NuMI construction coordinator who had visitedthis site also failed to identify safety deficiencies.
Causal factors identified in the 1998 Type Baccident investigation appear to be recurring. Thissituation was noted in the May 2001 semiannual safetyperformance reviews of the construction project bythe Office of Science. Additionally, the same causalfactors have been identified as weaknesses in morethan 20 injury reports over the last 12 months, 2 ofwhich prompted safety stand-downs.
The effectiveness of feedback and improvementprocesses applied to construction operations wasreduced by documentation deficiencies. Results ofsafety inspections were not consistently documentedand reported, and workplace injuries were notdocumented in CAIRS. Without such documentation,feedback to management was inaccurate andmanagement decisions were based on incompletesafety information. Performance feedback processeswere not adequate to support needed improvements insafety for the NuMI Project. The FAO did not perform

33
Implementation Deficiencies
Guiding Principle 1: Line Management Is Directly Responsible for the Protection of the Public, Workers,and the Environment.
• The FAO did not provide effective line management for the NuMI Project.• Neither S. A. Healy nor Layne-Western prepared an ISM plan, and the Fermilab ISM system was not
effective in assuring that Layne-Western met the FAO safety expectations.• S. A. Healy line management did not assure that the condition of Layne-Western equipment met contractual
requirements, did not assure that Layne-Western was providing safety oversight of its drilling operations,and did not clearly convey expectations to Layne-Western for preparation of job hazard analyses.
• Layne-Western line management did not set standards for the material condition of the drill rig that weresufficient to prevent equipment failure, did not assure that operators performed required safety inspectionsor appropriate maintenance of the rig, and did not provide oversight of drilling operations by a safetyprofessional.
Guiding Principle 2: Clear and Unambiguous Lines of Authority and Responsibility for Ensuring SafetyShall Be Established and Maintained at All Organizational Levels Within the Department and ItsContractors.
• Fermilab did not establish clear lines of responsibility or authority for management of S. A. Healy and itssubcontractors, and did not enforce compliance with safety requirements.
• Fermilab assigned Harza employees responsibilities for ES&H oversight and control, even though theHarza contract with Fermilab stated that Harza employees were not responsible for safety.
• S. A. Healy assigned administrative and non-ES&H responsibilities to their Safety Director, limiting histime to monitor the safety operations in the field.
Guiding Principle 3: Personnel Shall Possess the Experience, Knowledge, Skills, and Abilities That AreNecessary to Discharge Their Responsibilities.
• Fermilab and S. A. Healy personnel assigned to provide oversight of Layne-Western drilling operationswere not fully trained and/or qualified for this assignment.
Guiding Principles of Integrated Safety Management
sufficient oversight of safety practices at the job site,or of the safety program applied to Layne-Western byS. A. Healy, to identify significant deficiencies.Fermilab line management did not effectively monitoror control the operations of its subcontractor, S. A.Healy, to assure that S. A. Healy met the terms andconditions of its contract with Fermilab or the provisionsof the Fermilab ISM Plan. Line management oversightwas not adequate to identify significant safetydeficiencies at the Layne-Western job site or to identifythe poor condition of the drill rig.
Continuing weaknesses existed in the Fermilab ISMprogram, as it was applied to constructionsubcontractors on the NuMI Project. Specifically,Fermilab management had not established sufficientlyformalized management systems or work control
processes or procedures, but instead relied primarilyon expert-based knowledge, skills, and abilities to assurethat work was done safely. For example: (1) roles andresponsibilities were not well understood,(2) qualifications were not commensurate with assignedduties, (3) the workforce was not held accountable forstrict compliance with requirements, and(4) performance feedback systems were not adequateto support needed improvements.
The Board concluded that deficiencies in theconstruction safety management systems atFermilab indicated a need for increased commitmentby line management to ensure effectiveimplementation of the ISM framework for allsubcontractors and sub-tier contractors.
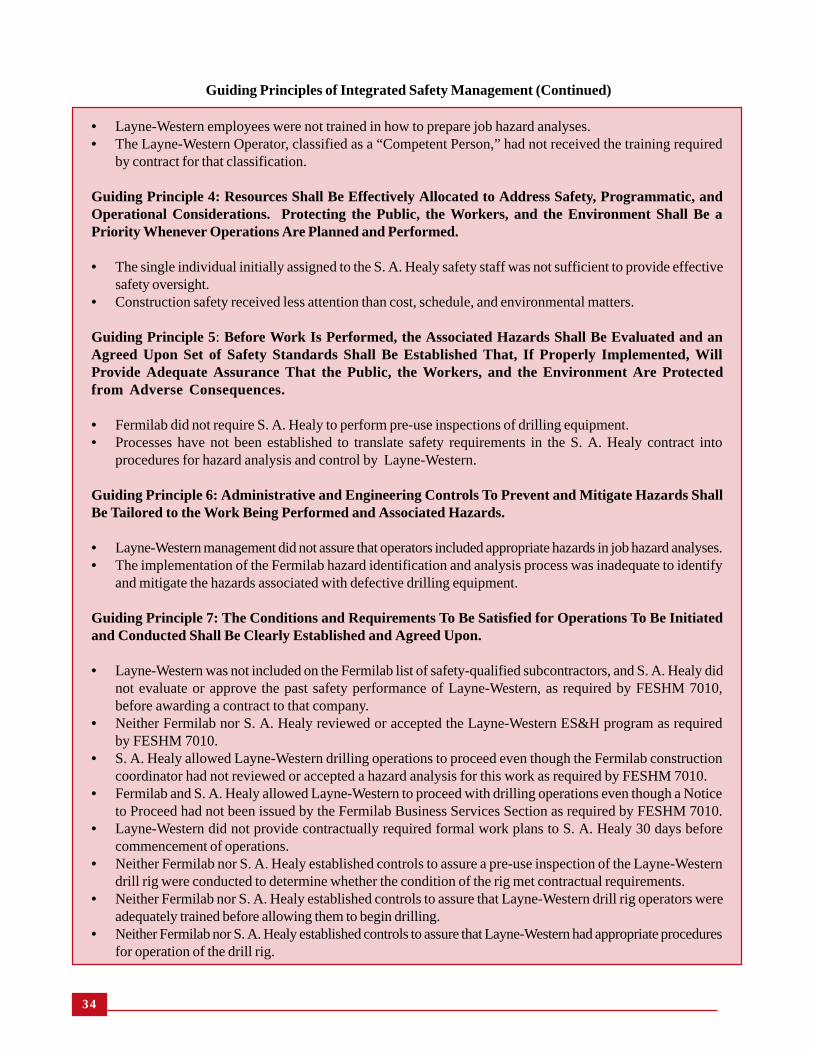
34
• Layne-Western employees were not trained in how to prepare job hazard analyses.• The Layne-Western Operator, classified as a “Competent Person,” had not received the training required
by contract for that classification.
Guiding Principle 4: Resources Shall Be Effectively Allocated to Address Safety, Programmatic, andOperational Considerations. Protecting the Public, the Workers, and the Environment Shall Be aPriority Whenever Operations Are Planned and Performed.
• The single individual initially assigned to the S. A. Healy safety staff was not sufficient to provide effectivesafety oversight.
• Construction safety received less attention than cost, schedule, and environmental matters.
Guiding Principle 5: Before Work Is Performed, the Associated Hazards Shall Be Evaluated and anAgreed Upon Set of Safety Standards Shall Be Established That, If Properly Implemented, WillProvide Adequate Assurance That the Public, the Workers, and the Environment Are Protectedfrom Adverse Consequences.
• Fermilab did not require S. A. Healy to perform pre-use inspections of drilling equipment.• Processes have not been established to translate safety requirements in the S. A. Healy contract into
procedures for hazard analysis and control by Layne-Western.
Guiding Principle 6: Administrative and Engineering Controls To Prevent and Mitigate Hazards ShallBe Tailored to the Work Being Performed and Associated Hazards.
• Layne-Western management did not assure that operators included appropriate hazards in job hazard analyses.• The implementation of the Fermilab hazard identification and analysis process was inadequate to identify
and mitigate the hazards associated with defective drilling equipment.
Guiding Principle 7: The Conditions and Requirements To Be Satisfied for Operations To Be Initiatedand Conducted Shall Be Clearly Established and Agreed Upon.
• Layne-Western was not included on the Fermilab list of safety-qualified subcontractors, and S. A. Healy didnot evaluate or approve the past safety performance of Layne-Western, as required by FESHM 7010,before awarding a contract to that company.
• Neither Fermilab nor S. A. Healy reviewed or accepted the Layne-Western ES&H program as requiredby FESHM 7010.
• S. A. Healy allowed Layne-Western drilling operations to proceed even though the Fermilab constructioncoordinator had not reviewed or accepted a hazard analysis for this work as required by FESHM 7010.
• Fermilab and S. A. Healy allowed Layne-Western to proceed with drilling operations even though a Noticeto Proceed had not been issued by the Fermilab Business Services Section as required by FESHM 7010.
• Layne-Western did not provide contractually required formal work plans to S. A. Healy 30 days beforecommencement of operations.
• Neither Fermilab nor S. A. Healy established controls to assure a pre-use inspection of the Layne-Westerndrill rig were conducted to determine whether the condition of the rig met contractual requirements.
• Neither Fermilab nor S. A. Healy established controls to assure that Layne-Western drill rig operators wereadequately trained before allowing them to begin drilling.
• Neither Fermilab nor S. A. Healy established controls to assure that Layne-Western had appropriate proceduresfor operation of the drill rig.
Guiding Principles of Integrated Safety Management (Continued)

35
Implementation Deficiencies
Core Function 1: Define the Scope of Work
• DOE project execution, Fermilab project management, and S. A. Healy work plans lacked detailed provisionsfor occupational safety.
• Layne-Western did not define specific work steps to be accomplished in planning documents, job letters,or work procedures.
• Responsibilities were not clearly assigned by Fermilab or S. A. Healy for management of constructionoperations performed by Layne-Western. FESHM 7010 was not fully implemented.
• Safety management systems did not convey DOE safety expectations to Layne-Western.
Core Function 2: Analyze the Hazards
• The hazard analysis prepared for drilling on June 21, 2001, was inadequate.• Requirements for preparation, review, approval, and use of job hazard analyses were not clearly conveyed
to operators, and the job hazard analysis generated on the day of the accident was not reviewed orapproved before starting work.
• Layne-Western operators were not trained in the preparation of job hazard analyses.• No project job hazard analysis was submitted to Fermilab or S. A. Healy for approval before initial drilling
by Layne-Western.• The condition of Layne-Western drilling equipment was not determined before use as specified by the
Fermilab Subcontractor Training Manual.• Layne-Western operators did not perform or document daily checks of safety or equipment condition as
required by the S. A. Healy/Layne-Western contract.
Core Function 3: Develop and Implement Controls
• Hazard controls were not established in job letters, work procedures, or job hazard analyses.• Layne-Western drilling equipment was not inspected or maintained in accordance with the Layne Christensen
Health and Safety Program, vendor recommendations, or OSHA requirements.• Rigging equipment associated with the drill rig was not tested in accordance with OSHA requirements for
hoisting and rigging equipment.• Electrical equipment at the drill site did not meet OSHA requirements.• Layne-Western had no process to assure engineering review and control over design changes to the drill
rig.• No training or qualification requirements were established for the operator making rig weld repairs.• Neither the FESHM, nor the S. A. Healy Safety Manual, nor the Layne Christensen Safety Manual was
provided at the drill site.• Layne-Western provided little line supervision over drilling operations.• The Operator designated as a “Competent Person” did not meet contract requirements for that designation.
Core Function 4: Perform Work Safely
• The wire rope, which extended from the tong handle to the hydraulic ram, was apparently routed aroundstructural interferences on the drill rig, increasing tension on the cable and stress on the connection thatfailed.
• The injured Operator did not stand clear of the tongs, as recommended in industry guidance, while usingthe hydraulic cylinder to apply torque to the drill stem.
Core Functions of Integrated Safety Management

36
3.2 Barrier Analysis
Barrier analysis is based on the premise thathazards are associated with all tasks. A barrier is anymanagement or physical means used to control, prevent,or impede the hazard from reaching the target (i.e.,persons or objects that a hazard may damage, injure,or harm). The results of the barrier analysis areintegrated into the events and causal factors chart tosupport the development of causal factors. Table 3-3contains the Board’s summary of physical andmanagement barriers that did not perform as intendedand thereby contributed to the accident. Appendix Dcontains the complete barrier analysis.
3.3 Change Analysis
Change analysis examines planned or unplannedchanges that caused undesirable results related to theaccident. This process analyzes the difference betweenwhat is normal, or expected, and what actually occurredbefore the accident. The results of the change analysisconducted by the Board are integrated into the eventsand causal factors chart to support the development ofcausal factors. The results reinforced the barrieranalysis results presented above.
• Operators were exposed to several OSHA non-compliances at the drilling site.• Operators did not routinely inspect drilling equipment as specified by the Layne Christensen Health and
Safety Program.
Core Function 5: Feedback and Improvement
• DOE, Fermilab, S. A. Healy, and Layne-Western provided ineffective safety oversight.• Previously-identified deficiencies in Fermilab and S. A. Healy safety programs were not fully addressed.• Information from previous accidents at the NuMI Project (23 incidents involving worker injuries) was not
used to identify and trend safety issues.• Layne-Western did not take action to prevent recurrence of a previous failure of the eyebolt-cable/piston rod
connection.• Safety deficiencies have not been consistently documented in inspection reports, and workplace injuries
have not been documented in CAIRS.• Corrective actions for previous Type B accidents did not adequately address causal factors.
Core Functions of Integrated Safety Management (Continued)
3.4 Causal Factors Analysis
A causal factors analysis was performed inaccordance with the DOE Workbook, ConductingAccident Investigations, Revision 2.
Causal factors are the events or conditions thatproduced or contributed to the occurrence of theaccident and consist of direct, root, and contributingcauses.
The direct cause is the immediate event orcondition that caused the accident. The Boarddetermined that the direct cause of the accident wasthe failure of the welded connection between the pistonrod and the wire rope, releasing the stored energy ofthe breaking mechanism.
Root causes are events or conditions that, ifcorrected, would prevent recurrence of this and similaraccidents.
The Board also identified contributing causes.Contributing causes are events or conditions thatcollectively with other causes increase the likelihoodof the accident, but that individually did not cause theaccident.
The root and contributing causes summarizing theBoard’s causal factors analysis appears in Table 3-4.
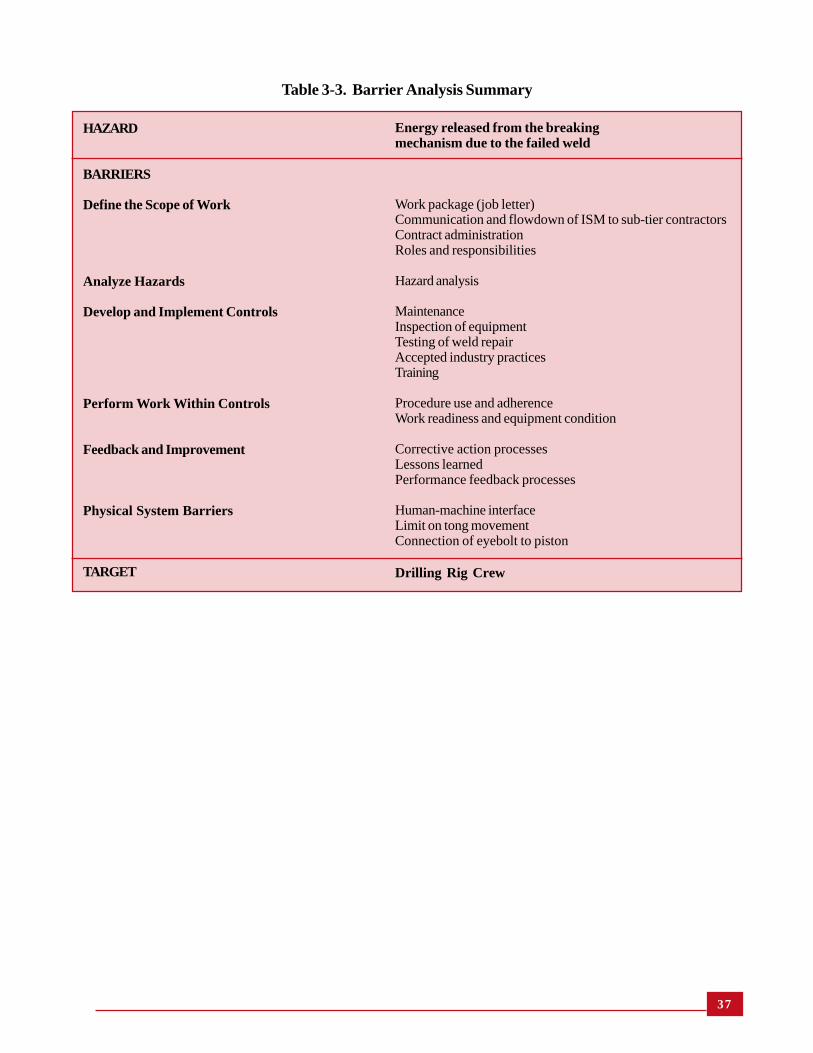
37
Table 3-3. Barrier Analysis Summary
HAZARD
BARRIERS
Define the Scope of Work
Analyze Hazards
Develop and Implement Controls
Perform Work Within Controls
Feedback and Improvement
Physical System Barriers
TARGET
Energy released from the breakingmechanism due to the failed weld
Work package (job letter)Communication and flowdown of ISM to sub-tier contractorsContract administrationRoles and responsibilities
Hazard analysis
MaintenanceInspection of equipmentTesting of weld repairAccepted industry practicesTraining
Procedure use and adherenceWork readiness and equipment condition
Corrective action processesLessons learnedPerformance feedback processes
Human-machine interfaceLimit on tong movementConnection of eyebolt to piston
Drilling Rig Crew

38
Root Cause
Fermilab failed to implement a hazardanalysis process that was effectively appliedto task-specific hazards for constructionsubcontractors and sub-tier contractors.
Contributing Causes
FAO and Fermilab failed to adequatelyanalyze prior occurrences to identify andcorrect root causes and systemicweaknesses underlying these events.
Fermilab failed to establish and implementprocesses to translate safety and healthrequirements into subcontractorprocedures. Fermilab did not establishcontrols to assure that sub-tier contractorswere adequately prepared to work safelybefore authorizing the start of work.
Discussion
• Layne-Western did not provide a hazard analysis plan before commencingdrilling operations.
• Drilling began in September 2000 without development of a hazardanalysis.
• Drill personnel were not requested to develop a hazard analysis for theirwork until June 2001.
• The hazard analysis dated June 21, 2001, did not comprehensively addressdrilling hazards to which personnel were exposed.
• Forms used for the June 21, 2001, hazard analysis did not match S. A.Healy or Fermilab hazard analysis documents.
• The Layne-Western hazard analysis process was too generic to identifytask specific drilling hazards and was not used.
• The S. A. Healy hazard analysis process was not used; if used, it wouldnot have resulted in an adequate task specific hazard analysis.
• FESHM 7010 was not used. Instructions in the attachment to ES&HAdministrative Form #17 were not required to be used for developmentof a hazard analysis.
• The Fermilab hazard analysis process did not provide clear proceduralguidance for evaluating task-specific hazards.
Discussion
• Causal factors from two previous Type B accidents contributed to theJune 21, 2001, accident. (e.g., inadequate work planning, hazard analysis,work controls).
• Recurring deficiencies from prior occurrence reports involving workerinjuries indicated that inadequate work planning, hazard analysis, and workcontrols were allowed to continue to exist at the NuMI Project.
• Corrective actions taken by line management in response to identifieddeficiencies, adverse trends, and recurring events, includingimprovements to subcontractor safety management, were not effective.
• NuMI line management neither established a formalized process tocapture and track ES&H-related deficiencies and associated correctiveactions from investigations, inspections, and audits, nor implementedmechanisms, such as independent verification and performance-basedevaluations, to ensure that corrective actions were timely, complete, andeffective.
• Processes were ineffective in disseminating lessons learned toconstruction subcontractors and sub-tier contractors, and to ensure thatlessons learned were understood and applied.
• Work site safety inspections were not rigorous, formal or documented,so important safety information was not collected or entered into theESHTRK database or another system to show systemic trends.
• Reportable accidents and injury reports from construction accidents onthe NuMI Project were not entered into CAIRS.
• Drilling personnel began work in September 2000 without formal workauthorization.
• The Layne-Western job letter did not address occupational safetyrequirements.
• S. A. Healy did not enforce contract requirements for hazard analysis ondrilling work.
• Fermilab did not enforce contract requirements for hazard analysis.
Table 3-4. Causal Factors Analysis Summary

39
Table 3-4. Causal Factors Analysis Summary (Continued)
• S. A. Healy did not enforce safety and health requirements for Layne-Western work.
• S. A Healy adopted the FESHM by reference but did not tailor it forsub-tier contractors.
• NuMI construction coordinators’ responsibility for acceptance ofhazard analysis was not clear.
• FESHM 7010 requirements did not translate to sub-tier contractors.• Fermilab did not ensure implementation of the FESHM 7010 hazard
analysis process by sub-tier contractors.
• Layne-Western inspections did not identify safety deficiencies.• Layne-Western equipment inspections did not identify existing safety
concerns.• NuMI construction coordinators were confused on roles and
responsibilities related to safety oversight.• Health and safety professionals focused on environmental issues
because of the April 26, 2001, wetlands issue.• Fermilab oversight was limited to S. A Healy operations and did not
include Layne-Western drilling operations.• FAO, Fermilab, and S. A. Healy safety personnel failed to identify job
site safety hazards during numerous visits to the drill site.• Fermilab did not conduct a safety inspection of the Layne-Western
equipment (drill rig) upon arrival at the site.
• S. A Healy did not require Layne-Western drilling personnel to conducta hazard analysis until June 20, 2001.
• NuMI construction coordinators were not aware of their responsibilityfor safety at Layne-Western drilling site.
• Fermilab safety and health professionals focused on environmentalissues because of the wetlands issue.
• There is no evidence that Fermilab safety professionals conducted safetyand health walkthroughs of the Layne-Western site.
• Fermilab believed that review of sub-tier contractor safety programswas the responsibility of only S. A. Healy.
• FAO conducted only two inspections of Layne-Western operationsbefore the accident, both with a focus on wetlands environmental issues.
• Layne-Western drilling personnel were not trained in the Fermilab hazardanalysis process before starting work.
• Layne-Western drilling personnel were not adequately trained as requiredby 29 CFR1926, or as necessary in accordance with the hazards associatedwith the job.
• Layne-Western personnel were not asked to participate in the June 9,2001, safety stand-down training.
• Layne-Western personnel did not participate in the June 13, 2001, safetystand-down that included hazard analysis training.
• Records did not indicate that Layne-Western personnel attended Fermilabsite training.
• The S. A. Healy Safety Director was not trained in preparing hazardanalyses.
• Fermilab and S. A. Healy failed to ensure that Layne-Western personnelwere adequately trained and qualified to perform work.
Fermilab failed to tailor the system formanaging subcontractor constructionsafety to address sub-tier contractors.
DOE and Fermilab oversight programsfailed to identify fundamental weaknessesin construction subcontractor and sub-tiercontractor safety and health programs.
Fermilab failed to effectively communicateroles, responsibilities, and clear lines ofauthority to ensure the adequate protectionof all workers, including constructionsubcontractors and sub-tier contractors.
Fermilab failed to ensure that theconstruction subcontractor and sub-tiercontractors had systems in place to trainemployees in recognizing and mitigatingoperational hazards.
Contributing Causes Discussion

40
Table 3-4. Causal Factors Analysis Summary (Continued)
• The Layne-Western Operator, who was designated as the “CompetentPerson,” did not meet contract requirements.
• Layne-Western did not provide a hazard analysis plan before start ofdrilling, as required.
• The S. A. Healy Safety Director did not meet minimum qualificationrequirements specified in the contract.
• Roles and responsibilities were not well understood.• Qualifications were not commensurate with assigned duties.• The workforce was not held accountable for strict compliance with
requirements.• Performance feedback systems were not adequate to support needed
improvements.
Contributing Causes Discussion
Chicago Operations Office and Fermilabfailed to effectively utilize contracting,procurement, and project managementmechanisms to consistently convey,oversee, and enforce safety and healthexpectations to the subcontractor and sub-tier contractors.
Chicago Operations Office and Fermilabfailed to properly implement and ensurethe flowdown of the ISM framework tosubcontractors and sub-tier contractors.
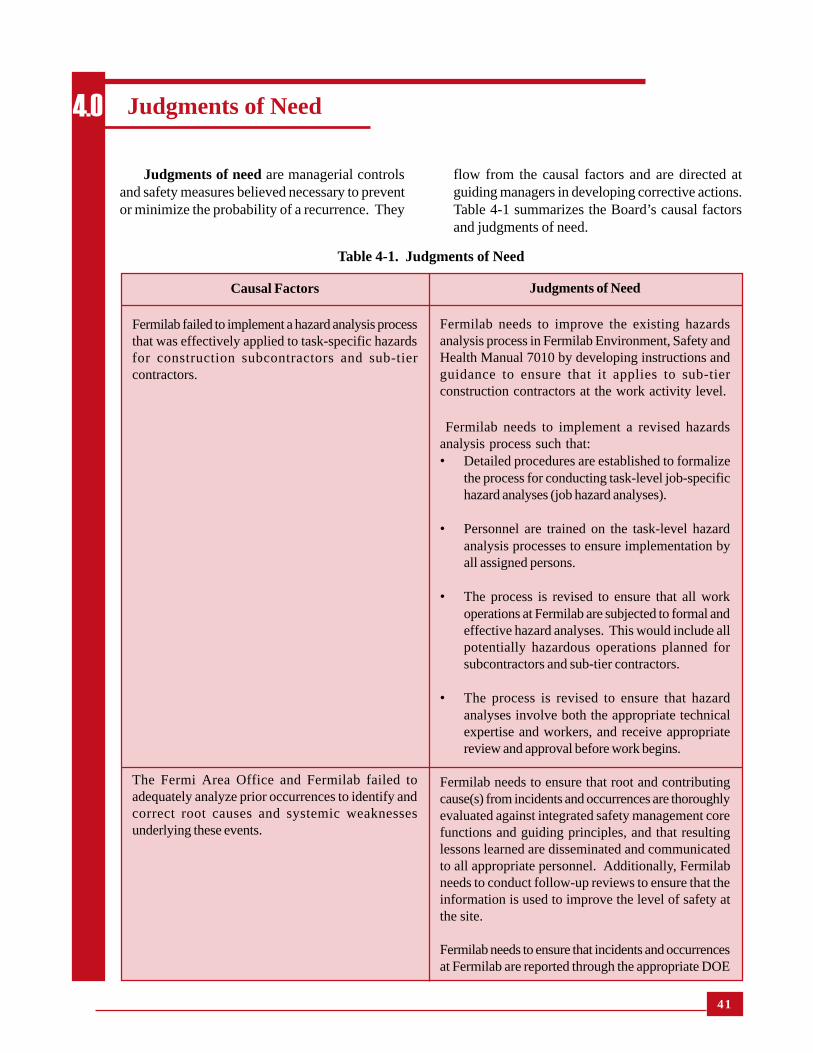
41
Judgments of Need
Fermilab needs to improve the existing hazardsanalysis process in Fermilab Environment, Safety andHealth Manual 7010 by developing instructions andguidance to ensure that it applies to sub-tierconstruction contractors at the work activity level.
Fermilab needs to implement a revised hazardsanalysis process such that:• Detailed procedures are established to formalize
the process for conducting task-level job-specifichazard analyses (job hazard analyses).
• Personnel are trained on the task-level hazardanalysis processes to ensure implementation byall assigned persons.
• The process is revised to ensure that all workoperations at Fermilab are subjected to formal andeffective hazard analyses. This would include allpotentially hazardous operations planned forsubcontractors and sub-tier contractors.
• The process is revised to ensure that hazardanalyses involve both the appropriate technicalexpertise and workers, and receive appropriatereview and approval before work begins.
Fermilab needs to ensure that root and contributingcause(s) from incidents and occurrences are thoroughlyevaluated against integrated safety management corefunctions and guiding principles, and that resultinglessons learned are disseminated and communicatedto all appropriate personnel. Additionally, Fermilabneeds to conduct follow-up reviews to ensure that theinformation is used to improve the level of safety atthe site.
Fermilab needs to ensure that incidents and occurrencesat Fermilab are reported through the appropriate DOE
Judgments of need are managerial controlsand safety measures believed necessary to preventor minimize the probability of a recurrence. They
Judgments of Need4.0
flow from the causal factors and are directed atguiding managers in developing corrective actions.Table 4-1 summarizes the Board’s causal factorsand judgments of need.
Causal Factors
Fermilab failed to implement a hazard analysis processthat was effectively applied to task-specific hazardsfor construction subcontractors and sub-tiercontractors.
The Fermi Area Office and Fermilab failed toadequately analyze prior occurrences to identify andcorrect root causes and systemic weaknessesunderlying these events.
Table 4-1. Judgments of Need

42
Table 4-1. Judgments of Need (Continued)
Causal Factors Judgments of Need
reporting systems (i.e., the Computerized Accident/Incident Reporting System and the Occurrence Reportingand Processing System), evaluated, analyzed, and trendedto ensure that systemic weaknesses are identified andcorrected in a timely manner.
The Fermi Area Office needs to revise its process forvalidating closure and effectiveness of corrective actions.Additionally, FAO needs to conduct follow-up reviews toensure that corrective actions are effectively implemented.
The Chicago Operations Office Manager needs to developand implement a process to provide assurance that effectivecorrective actions are implemented, and establish a methodto obtain feedback on corrective actions taken.
Fermilab needs to establish and implement a process toensure that all safety and health requirements flow down tosubcontractors and sub-tier contractors such that:� Procedures are adopted by subcontractors and sub-tier
contractors that are tailored for the specific roles andresponsibilities for each contracting organization.
� Specific procedures are validated to ensure that safetyand health requirements are properly implemented.
� Improved controls are established to assure thatsubcontractors and sub-tier contractors are adequatelyprepared to work safely before authorization to startwork is issued.
The FAO needs to ensure that Fermilab establishes andimplements processes to verify and validate that safety andhealth requirements are translated into subcontractor andsub-tier contractor procedures.
The Chicago Operations Office Manager needs to validatethe processes and procedures used by FAO and Fermilab toverify that work controls are established and implementedbefore the start of work.
Fermilab needs to ensure that a program is established andimplemented for comprehensive environment, safety, andhealth oversight of all construction subcontractor and sub-tier contractor work operations.
The FAO needs to ensure that oversight of Fermilab iseffectively performed as specified in DOE Policy 450.5,Line Environment, Safety and Health Oversight.
Fermilab failed to establish and implement processes totranslate safety and health requirements into subcontractorprocedures. Fermilab did not establish controls to assurethat sub-tier contractors were adequately prepared to worksafely before authorizing the start of work.
Fermilab failed to tailor the system for managingsubcontractor construction safety to address sub-tiercontractors.
DOE and Fermilab oversight programs failed to identifyfundamental weaknesses in construction subcontractor andsub-tier contractor safety and health programs.

43
Causal Factors Judgments of Need
The Chicago Operations Office Manager needs to ensurethat line management and independent oversight are beingperformed and are effective as specified by DOE Policy450.5, Line Environment, Safety and Health Oversight,and DOE Order 414.1A, Quality Assurance.
The Office of Science needs to ensure that formal correctiveactions are developed and implemented for ES&H issuesresulting from programmatic and technical reviews of theNuMI Project.
The Office of Science needs to implement the requirementsestablished in the Office of Science Functions,Responsibilities, and Authorities Manual for measuring lineES&H oversight effectiveness of the Chicago OperationsOffice.
Fermilab needs to establish and implement a formalizedsafety management system with clearly defined roles,responsibilities, and authorities when multipleorganizations, subcontractors, and/or sub-tier contractorsare involved in a construction project.
Fermilab needs to strengthen the training and competenceof all workers, managers, engineers, and safetyprofessionals responsible for construction safety.
Fermilab needs to establish processes to assure that hazardrecognition and training are in compliance with applicablerequirements (Occupational Safety and Health, DOE, andindustry standards).
The Chicago Operations Office and Fermilab need to revisecontracting, procurement, and project managementprocesses to ensure that safety and health requirementsassociated with construction operations (by subcontractorand sub-tier contractors) are clearly conveyed.
Fermilab needs to strengthen implementation of theintegrated safety management core functions to assure thatall potentially hazardous work and operations are subjectedto effective, formal, and documented hazard analysis.
Fermilab needs to establish and implement a process toensure that the framework of ISM flows down to allsubcontractor and sub-tier contractors.
The Chicago Operations Office Manager needs to ensurethat the Fermilab process for flowdown of the ISMframework to subcontractors and sub-tier contractors iseffective.
Fermilab failed to effectively communicate roles,responsibilities, and clear lines of authority to ensureadequate protection of all workers, including constructionsubcontractors and sub-tier contractors.
Fermilab failed to ensure that the constructionsubcontractor and sub-tier contractors had systems in placeto train employees in recognition and mitigation ofoperational hazards.
Chicago Operations Office and Fermilab failed toeffectively utilize contracting, procurement, and projectmanagement mechanisms to consistently convey, oversee,and enforce safety and health expectations to thesubcontractor and sub-tier contractors.
Chicago Operations Office and Fermilab failed to properlyimplement and ensure the flowdown of the integrated safetymanagement framework to subcontractors and sub-tiercontractors.
Table 4-1. Judgments of Need (Continued)

44
Board Signatures5.0

45
Chairperson Patricia Worthington, Ph.D., DOE-HQ, EH-22
Member Bruce Breslau, DOE-HQ, EH-21
Member William Cooper, DOE-HQ, EH-22
Member Robert Crowley, DOE-HQ, EH-24
Member Don Galbraith, DOE-Carlsbad Field Office
Member Justin Zamirowski, DOE-Chicago
Advisor Matt Cole, DOE HQ, Office of Science
Advisor Al Gibson, Eagle Research Group
Advisor Steve Kirchhoff, Battelle Columbus
Advisor Mike Lambert, Eagle Research Group
Advisor Karl Moro, DOE-Chicago
Advisor Dennis Vernon, DOE-HQ, EH-21
Consultant Thomas Groeneveld, Battelle Columbus
Consultant Norm Malcosky, Battelle Columbus
Medical Advisor Joseph Falco, M.D., M.P.H.
Legal Advisor Vicki Prouty, DOE-Chicago
Technical Writer Bob McCallum, Battelle Columbus
Technical Writer Jim McNeil, Eagle Research Group
Administrative Support Vikki Hanks, Battelle Columbus
Administrative Support Barbie Harshman, DOE-HQ, EH-21
Administrative Support Marcia Taylor, Battelle Columbus
Board Members, Advisors, and Staff6.0

46
APPENDIX ABOARD APPOINTMENT MEMORANDUM
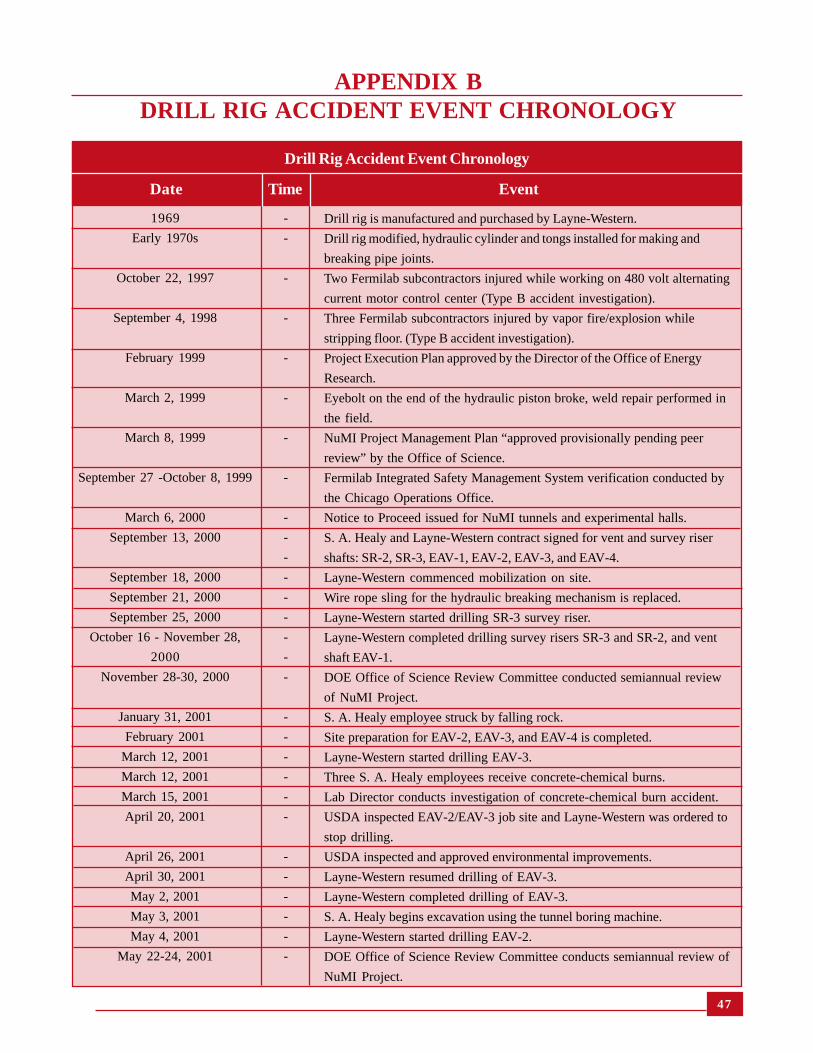
47
1969
Early 1970s
October 22, 1997
September 4, 1998
February 1999
March 2, 1999
March 8, 1999
September 27 -October 8, 1999
March 6, 2000
September 13, 2000
September 18, 2000
September 21, 2000
September 25, 2000
October 16 - November 28,
2000
November 28-30, 2000
January 31, 2001
February 2001
March 12, 2001
March 12, 2001
March 15, 2001
April 20, 2001
April 26, 2001
April 30, 2001
May 2, 2001
May 3, 2001
May 4, 2001
May 22-24, 2001
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
-
Drill rig is manufactured and purchased by Layne-Western.
Drill rig modified, hydraulic cylinder and tongs installed for making and
breaking pipe joints.
Two Fermilab subcontractors injured while working on 480 volt alternating
current motor control center (Type B accident investigation).
Three Fermilab subcontractors injured by vapor fire/explosion while
stripping floor. (Type B accident investigation).
Project Execution Plan approved by the Director of the Office of Energy
Research.
Eyebolt on the end of the hydraulic piston broke, weld repair performed in
the field.
NuMI Project Management Plan “approved provisionally pending peer
review” by the Office of Science.
Fermilab Integrated Safety Management System verification conducted by
the Chicago Operations Office.
Notice to Proceed issued for NuMI tunnels and experimental halls.
S. A. Healy and Layne-Western contract signed for vent and survey riser
shafts: SR-2, SR-3, EAV-1, EAV-2, EAV-3, and EAV-4.
Layne-Western commenced mobilization on site.
Wire rope sling for the hydraulic breaking mechanism is replaced.
Layne-Western started drilling SR-3 survey riser.
Layne-Western completed drilling survey risers SR-3 and SR-2, and vent
shaft EAV-1.
DOE Office of Science Review Committee conducted semiannual review
of NuMI Project.
S. A. Healy employee struck by falling rock.
Site preparation for EAV-2, EAV-3, and EAV-4 is completed.
Layne-Western started drilling EAV-3.
Three S. A. Healy employees receive concrete-chemical burns.
Lab Director conducts investigation of concrete-chemical burn accident.
USDA inspected EAV-2/EAV-3 job site and Layne-Western was ordered to
stop drilling.
USDA inspected and approved environmental improvements.
Layne-Western resumed drilling of EAV-3.
Layne-Western completed drilling of EAV-3.
S. A. Healy begins excavation using the tunnel boring machine.
Layne-Western started drilling EAV-2.
DOE Office of Science Review Committee conducts semiannual review of
NuMI Project.
Drill Rig Accident Event Chronology
APPENDIX BDRILL RIG ACCIDENT EVENT CHRONOLOGY
Date Time Event

48
June 2, 2001
June 9, 2001
June 13, 2001
June 13, 2001
June 15, 2001
June 15, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
June 21, 2001
-
-
-
2:15 PM
8:00 AM
-
~7:00 AM
-
~9:40 AM
~9:40 AM
-
-
9:44 AM
9:48 AM
9:48 AM
~9:50 AM
9:57 AM
~10:00 AM
10:02 AM
10:15 AM
10:00 AM-
12:00 PM
~12:00 PM
1:30 PM
S. A. Healy employee injured due to improper rigging.
S. A. Healy conducted full safety stand-down but did not include Layne-
Western.
Two S. A. Healy employees injured due to improper rigging.
Safety stand-down for S. A. Healy work instituted by Fermilab and S. A.
Healy.
Work resumed by S. A. Healy.
Fermilab Director assigned team to investigate S. A. Healy safety perfor-
mance and safety management.
Layne-Western drilling crew started the day continuing to drill EAV-2.
Fermilab construction coordinators visited EAV2/3 drill site.
Weld connection between eyebolt and piston rod failed, releasing tension on
tong handle.
Layne-Western drill rig Operator injured when struck by tong handle.
Layne-Western drill rig Helper attends to the injured Operator, and then seeks
emergency response.
Fermilab employee is driving on Giese Road past EAV-2/EAV-3 job site.
Fermilab employee called 3131, site emergency number for assistance. Two
Fermilab Fire Department EMTs arrived at scene. Two additional Fermilab
firefighters arrived with basic life support ambulance.
Fermilab Fire Department Captain arrived and established incident command
center on Giese Road.
Fermilab ES&H personnel responded to emergency call.
Fermilab fire fighters secured injured Operator on backboard and carried
Operator to the road. Simultaneously, advanced life support (Geneva Fire
Department) ambulance arrives at scene.
Fermilab ES&H Section personnel restrict access into job site by requesting
site security subcontractor on scene to tape off job site entrance and control
crowd.
Incident Command Center declares emergency secured and turns scene over
to Fermilab Facility Engineering Services Section.
Geneva Fire Department ambulance leaves scene and transports injured
Operator to Delnor Community Hospital in Geneva, Illinois.
Fermilab ES&H Section Safety Coordinator and others inspect the accident
scene and take photographs.
Fermilab security posted at job site to restrict access.
Formal Stop-Work Order issued to S. A. Healy by Fermilab.
Drill Rig Accident Event Chronology
Date Time Event
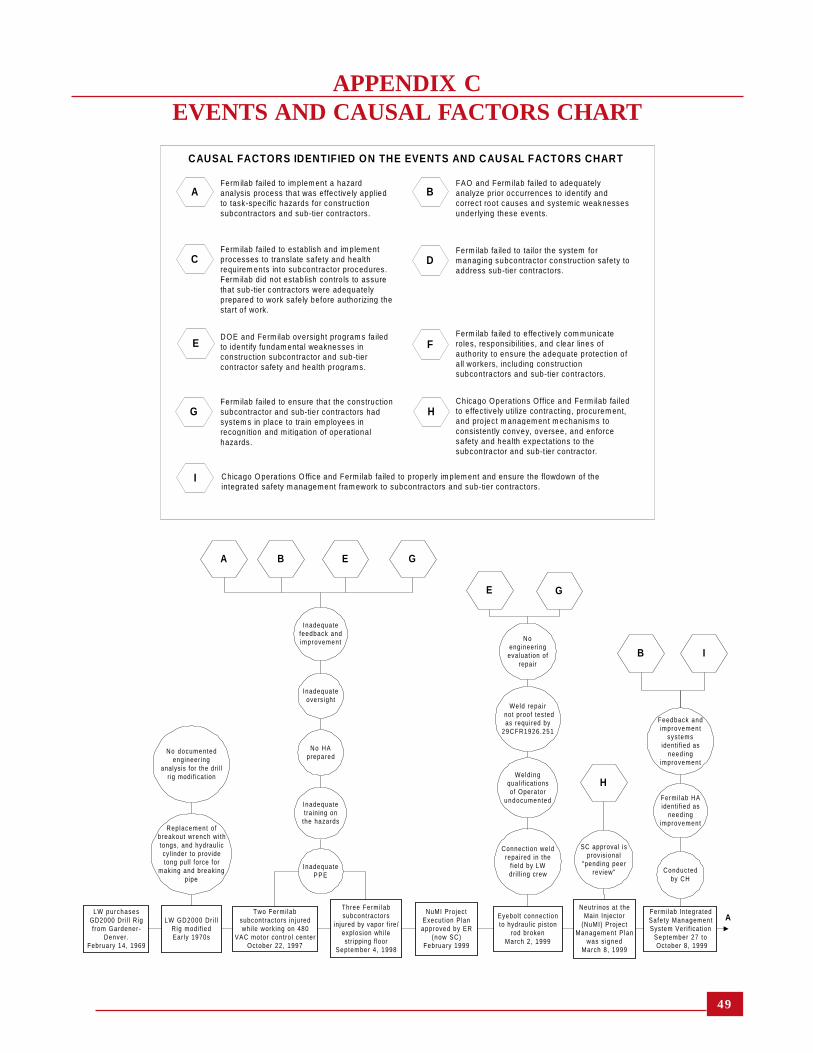
49
APPENDIX CEVENTS AND CAUSAL FACTORS CHART
AFerm ilab fa iled to im plem ent a hazardanalys is process that was effective ly appliedto task-specific hazards for constructionsubcontractors and sub-tier contractors.
FAO and Ferm ilab failed to adequatelyanalyze prior occurrences to identify andcorrect root causes and system ic weaknessesunderlying these events.
Ferm ilab fa iled to estab lish and im plementprocesses to translate safety and healthrequirem ents in to subcontractor procedures.Ferm ilab did not estab lish contro ls to assurethat sub-tier c ontractors were adequate lyprepared to work safely before authorizing thestart o f work.
CAUSAL FACTORS IDENTIFIED ON THE EVENTS AND CAUSAL FACTORS CHART
Ferm ilab fa iled to tailor the system form anaging subcontractor construction safety toaddress sub-tier contractors.
DOE and Ferm ilab oversight program s fa iledto identify fundam ental weaknesses inconstruction subcontractor and sub-tiercontractor safety and health program s.
Ferm ilab fa iled to e ffective ly com m unicateroles, responsibilities, and clear lines ofauthority to ensure the adequate protection ofa ll workers, inc luding constructionsubcontractors and sub-tier contractors.
Ferm ilab fa iled to ensure that the constructionsubcontractor and sub-tier contractors hadsystem s in p lace to train em ployees inrecognition and m itigation of operationalhazards.
Chicago Operations Office and Ferm ilab fa iledto effec tively u tilize contracting, procurem ent,and pro jec t m anagem ent m echanism s toconsistently convey, oversee, and enforcesafety and health expectations to thesubcontractor and sub-tier contractor.
Chicago O perations O ffice and Ferm ilab failed to properly im plem ent and ensure the flowdown of theintegrated safety m anagement fram ework to subcontractors and sub-tier contractors.
B
C D
E F
G H
I
Two Fermi labsubcontractors in juredwhi le working on 480
VAC motor contro l centerOctober 22, 1997
LW GD2000 Dr i l lRig modi f iedEar ly 1970s
LW purchasesGD2000 Dri l l Rigf rom Gardener-
Denver .February 14, 1969
Replacement o fbreakout wrench wi thtongs, and hydraul iccyl inder to providetong pul l force for
making and breakingpipe
No documentedengineer ing
analysis for the dri l lr ig modif icat ion
Three Fermi labsubcontractors
injured by vapor f i re/explosion whi lestr ipping f loor
September 4 , 1998
Eyebol t connect ionto hydraul ic piston
rod brokenMarch 2, 1999
Connect ion weldrepaired in the
f ie ld by LWdri l l ing crew
Weld ingqual i f icat ionsof Operator
undocumented
ANeutr inos at the
Main Injector(NuMI) Project
Management P lanwas s igned
March 8, 1999
SC approval isprovisional
"pending peerreview"
Weld repair not proof tested
as required by29CFR1926.251
Noengineer ing
evaluat ion ofrepair
NuMI ProjectExecut ion Planapproved by ER
(now SC)February 1999
InadequateP P E
No HAprepared
Inadequatetraining on
the hazards
Inadequateoversight
Fermi lab IntegratedSafety ManagementSystem Veri f icat ion
September 27 to October 8, 1999
Feedback andimprovement
sys temsidenti f ied as
needingimprovement
Fermi lab HAidenti f ied as
needingimprovement
Conductedby CH
Inadequatefeedback andimprovement
A B E G
H
GE
IB

50
SAH and LW con t rac ts igned for dr i l l ing
act iv i t iesSep tember 13 , 2000
S A Hrequ i rementsimposed on
L W
F E S H M 7 0 1 0not ta i lored for
S A Hsubcont rac tors
Fermi labassumes no
E S & Hresponsibi l i t ies
for sub-t iercont ractors
R & R o fconst ruc t ioncoord inators
no tunders tood
Not ice to Proceed issued forNuMI tunne ls andexper imenta l ha l ls
March 6 , 2000
SAH Sa fe t yDi rec tor does
no t havespec i f ic HA
tra in ing
SAH accep tsF E S H M 7 0 1 0by re fe rence
F E S H M 7 0 1 0not ta i lored for
S A Hsubcont rac tors
DOE sa fe t yand hea l th
expec ta t ionsno t unders tood
b y S A H
A B
SAH Sa fe t yDirector
exper iencedoesn ' t meet
specs
Use of sub- t iercont ractors not
or iginal lyp lanned fo r
dri l l ing
LW beg ins mob i l i za t ionon s i te
Sep tember 18 , 2000
SAH d id no trequ i re work
p lan
N o H Adeve loped
Job le t ter doesnot
commun ica teE S & H
expecta t ions
No workp lan
prepared
No s i tetra in ing for
L Wemp loyees
Cont rac tua lexpec ta t ionsnot en fo rced
R & R o fconst ruc t ioncoord inators
no t unders tood
No s i teinspect ion by
Fermi labpr ior to work
on s i te
L W p u r c h a s e s n e wwire rope for break ing
m e c h a n i s m Sep tember 21 , 2000
Rep lacemen tcab le
repor ted ly hash igher s t rength
N ospeci f icat ion
for propercab le
No hazardassessmen t
fo r newconf igura t ion
Prev iouscab les
cont inued tob reak
LW star ted dr i l l ingS R - 3
Sep tember 25 ,2 0 0 0
Safe tyexpec ta t ions
were no tcommun ica tedt o L W b y S A H
N o H Adeve loped
before workstar ts
SAH d id no tunders tand
D O Eexpecta t ions
Fermi labE S & H
prior i t ies areno t focusedon sub- t iers
Fermi lab notmoni to r ing
SAH sa fe ty &hea l th
pe r fo rmance
FAO, Fermi lab ,SAH d id no t
rev iew LW jobs i te for S&H
concerns
L W c o m p l e t e ddr i l l ing SR-3
October 16 , 2000
W o r kconduc tedwi thou t HA
Const ruc t ioncoord inatorsvisit si te to
moni to rp rogress
Coord ina torsd id not
recogn ize works tar ted w/o HA
G
H
I
F
D
I
F
H
A
E
D
F
GC
F GA DC E
LW star teddr i l l ing SR-2October 17,
2000
B LW comple tesdr i l l ing of SR-2November 7 ,
2000
C
Safetyexpectat ions
were notcommun ica tedto LW by SAH
No HAdeve loped
before workstarts
SAH d id notunders tand
D O Eexpectat ions
Fermi labE S & H
priori t ies arenot focusedon sub-t iers
Fermi lab notmoni tor ing
SAH safety &heal th
per fo rmance
FAO, Fermi lab,SAH d id not
rev iew LW jobsi te for S&H
concerns
W o r kconduc tedwi thout HA
Construct ioncoord inatorsvisit site to
moni torprogress
Coord inatorsdid not
recognizework star ted
w/o HA
LW star teddr i l l ing EAV-1November 8 ,
2000
LW comp le teddr i l l ing EAV-1November 28 ,
2000
Safetyexpectat ions
were notcommun ica tedto LW by SAH
No HAdeve loped
before workstarts
SAH d id notunders tand
D O Eexpectat ions
Fermi labE S & H
priori t ies arenot focusedon sub-t iers
Fermi lab notmoni tor ing
SAH safety &heal th
per fo rmance
FAO, Fermi lab,SAH d id not
rev iew LW jobsi te for S&H
concerns
W o r kconduc tedwi thout HA
Construct ioncoord inatorsvisit site to
moni torprogress
Coord inatorsdid not
recognizework star ted
w/o HA
SC Rev iew Commi t teeconducts semiannual
rev iew of NuMI Pro jectNovember 28-30, 2000
Recommenda t i onfor str ict oversight
o f ES&H
SAH emp loyeestruck by fal l ing
rockJanuary 31, 2001
Eventcaused byinadequate
superv is ion andprocedures not
used
Fif th eventin January
N oformal ized system
for t rackingrecommendat ions
Si te preparat ionfor EAV-2, 3, and
4 comple tedFebruary 2001
First work byLW s inceNovember28, 2000
LW started dr i l l ingEAV-3
March 12, 2001
Safetyexpectat ions
were notcommun ica tedto LW by SAH
No HAdeve loped
before workstarts
SAH d id notunders tand
D O Eexpectat ions
Fermi labE S & H
priori t ies arenot focusedon sub-t iers
Fermi lab notmoni tor ing
SAH safety &heal th
per fo rmance
FAO, Fermi lab,SAH d id not
rev iew LW jobsi te for S&H
concerns
W o r kconduc tedwi thout HA
Construct ioncoord inatorsvisit site to
moni torprogress
Coord inatorsdid not
recognize workstar ted w/o HA
A D E FC G
E
B
F

51
C DThree SAHemployees in juredby concrete burns
March 12, 2001
InadequateH A
Lack o fp roper PPE
S A HManagement /
superv is ion wasless thanadequate
Fermi lab invest igat ionof concrete chemica l
burn inc identMarch 15, 2001
Verbal s topwork order to
stop dr i l l ing dueto breech at
set t l ing basin
NuMIconstruct ioncoord inatorsinspect s i te
No Fermi labor SAH
considerat iong iven to S&H
aspects of the dr i l ls i te
USDA re- inspects andapproves env i ronmenta l
improvementsApr i l 26, 2001
USDA inspec tsEAV-2/3 job s i te
Apr i l 20, 2001
Inspect ionfai led to
ident i fy S&Hdef ic ienc ies
LW restar tauthor ized
Repor tident i f ied work
p lanningdef ic ienc ies and
inadequatesuperv is ion
SAH Safe tyPlan is not ful lyimplemented or
enforced
LW comp le teddr i l l ing of EAV-3
May 2, 2001
LW resumedr i l l ing of EAV-3
Apr i l 30, 2001
SAH beg instunnel excavat ion
us ing the TBMMay 3, 2001
Safetyexpectat ions
were notcommun ica tedto LW by SAH
No HAdeve loped
before workstarts
SAH d id notunders tand
D O Eexpectat ions
Fermi labE S & H
prior i t ies arenot focused on
sub-t iers
Fermi lab notmoni tor ing
SAH safe ty &heal th
per fo rmance
FAO, Fermi lab,SAH d id not
rev iew LW jobs i te for S&H
concerns
W o r kconduc tedwi thout HA
Construct ioncoord inatorsvisi t si te to
moni torprogress
Coord inatorsdid not
recognize workstar ted w/o HA
A D E FC G
E FG
F
E
A
LW star tsdr i l l ing EAV-2May 4, 2001
D ESC Rev iew Commi t teeconducts semiannual
review of NuMI ProjectMay 22-24, 2001
Contractorconstruct ion
safetyprob lemsidenti f ied
Fermi labinit iates
reorganizat ionbased on
rev iew
SAH employee st ruck inhead by a suspended
loadJune 2, 2001
SAH not heldaccountable
for recordkeeping
Fermi lab didnot adequatelycommunica te
record keepingrequi rements
O S H Areportable
however notreported to
CAIRs
FAO is notrev iewing CAIRsto val idate injury
and i l lnessper formance
No HAdevelopedbefore start
of work
Inadequateprocedure
used
No pre- jobbr ief ing wasconducted
Inadequatework
planning
SAH conducted fu l lsafety s tand-downfor al l employees
June 9, 2001
Stand-downdid not
inc lude LW
Safety s tand-downordered by Fermi lab
to SAH2:15 PM
June 13, 2001
Two SAHemployees in jured
due to improperr igging
June 13, 2001
Hazards ofLW work not
recognizedS A H
HA processrequired by7010 didn' tf low wel l to
sub-t iers
Work resumedby S. A. Healy
8 :00 AMJune 15, 2001
LW nevers topped
work
LW did notbenef i t f romHA training
SAH andFermi lab
general safetyawareness and
HA training
LW did notpart icipate ins tand-down
training
No CAIRsreport
Inconsistenciesin OSHA
report ing byS A H
SAH d idnot require
LW todevelop
H A
No HAdeveloped
Inadequateprocedure for
doing work
G
B
A
D
F
A
B
E
F
F
GI
Director assigns teamto invest igate SAH
safety per formance andsafe ty management
June 15, 2001
Safety wasnot
integratedinto SAH
work
SAH did notful ly understand
safetyresponsibi l i t ies
Report resul tsin 27 f indings
B
E

52
F
Estab l ishedincident
c o m m a n dcenter
FireDepar tment
Inc identCommander kep tcrowd back f rom
injured LW Dr i l l RigOperator
Fermi lab Fi reDepar tment
Captain arr ived atthe scene9:48 AM
June 21, 2001
ES&H Sec t ionpersonnelrespond to
emergency ca l l~9 :50
June 21, 2001
Geneva F i reDepar tmentambu lance
arr ives at scene9:57 AM
June 21, 2001
Geneva F i reDepar tmentambu lancetransportsOperator
10:15 AMJune 21, 2001
IncidentC o m m a n d e r
dec laresemergency
secured10:02 AM
June 21, 2001
Fermi lab ES&Hpersonnel restr ic t
access in to jobsi te crowd~10:00 AM
June 21, 2001
E M T stransport
Operator toambu lance ~9:58 AM
June 21, 2001
Numerouspeople at the
scene inaddit ion to Fire
Depar tment
Scene is tapedof f by SAHand FES
Sect ion to l imitaccess
Contro l ofscene turnedover Fermi labFES Sect ion
Transpor tOperator to
DelnorCommun i t yHospi ta l in
Geneva, I l l ino is
Fermi labsecur i ty posted
at job si te~12:00
June 21, 2001
Fermi lab ES&HSect ion Safety
Coord inator10:00 - 12:00
June 21, 2001
Numeroussafety people
from al lorganizat ionsat the scene
Mult ip le Fermi labemployees
handle wire ropeand shack lear rangement
Fermi lab ES&HSect ion personnel
"c lean" eyebol t andpiston ram with
degreaser toimprove vis ib i l i ty of
weld fai lure
FES Sect iontransferred
control of thescene to ES&H
Sect ionrepresentat ive
Instruct ionsgiven that the
scene is not beturned over to
S A H
EMTs ass is tGeneva inprepar ing
Operator fortransport to
hospi ta l
Secur i tyescor ts
ambulance tothe acc ident
scene
Formal Stop-Work Order
issued to SAHby Fermi lab
1 :30 PMJune 21, 2001
Fermi labissued
phrasedrestart onJune 28
Fermi labbus inessserv ices
sect ion issuesorder
Advanced l i fesuppor t
ambu lance
Ambulance isdr iven by
Fermi lab Fi reFighter
Bo th GenevaFi re Depar tment
Paramed icsattend to pat ient
Restr ic tsaccess toauthor izedindiv iduals
Acc identscene
inspected andphotographs
taken
Potent ia l loss ofev idence due to
handl ing andcleaning of r igcomponen ts
EFLW Operator work ing
on hazard analysisevening
June 20, 2001
LW Dri l l RigCrew starts
work~ 7:00 AM
June 21, 2001
Crewconducted dai lyoi l checks and
basicmaintenance
Dri l l crewinitiated
removal ofdri l l pipe from
EAV-2
Result inghazard
analysis didnot identify all
hazards
Crew notformally trained
on hazardanalysisprocess
Hazardanalysis
"f inished"that
morn ing
Hazardanalysis wasnot complete
and notapproved
NuMIconstruct ioncoordinatorsvisit drill site
twice
No review ofHA and
existing safetyconcerns not
recorded
Hazardanalysiswas not
approved
Dri l l Rig Helperattends to the
injured Dri l l RigOperator
Fermi lab employeeis driving on GieseRoad past EAV-2/3
job siteJune 21, 2001
Helper laysinjured
Operator onpallets on eastside of dril l rig
Helper f lagsdown employee
to assist incall ing for
emergencyassistance
Helper goes totool trailer to get
cel l phone tocall for
ambu lance
Weld connect ionbetween eyebolt
and piston rod fai led ~9:40 AM
June 21, 2001
Energyin tong handle
released ascrew was
breaking dri l lcol lar
Operator wasstanding on theeast side of the
dri l l platform
Helper wasstanding onthe westsideof the dril l rig
p lat form
Dril l RigOperator injured
when struck by tonghandle ~9:40 AM
June 21, 2001
Operatorposit ion wasin the pathof the tong
Operator 'swork locat ionwas not IAW
IADC
IADC was notincorporated
into LWsafety manual
A
A
G
FD EC
Fermi labemployee cal lssi te number for
emergencyresponse9:44 AM
June 21, 2001
Maintainedphone contact withthe Comm Center
Dispatcher unti lFermi lab Fire
Depar tment EMTsarrived
Fermilab FireDepar tment EMTs
arrive at scene9:48 AM
June 21, 2001
Twoinitial Fire
Depar tmentresponders cal ldispatcher for
ALS f romTri-City
Five FireDepar tmentpersonnelrespond to
attend to injuredOperator
phased

53
APPENDIX DBARRIER ANALYSIS
ManagementBarriers
Core Function 1Work package (jobletter)
Core Function 1Communication andflowdown of ISM tosub-tier contractors
Core Function 1Contractadministration
Core Function 1Roles andResponsibilities:
EH-2SCCHFAOFermilabS. A. HealyLayne-Western
Failed
Failed
Failed
Failed
“Job letter” was the extent of the work package.No task-specific breakdown of the work wasperformed to identify hazards and associated controlsto satisfy safety and health expectations.
Systems and processes were inadequate to implementmanagement safety expectations or to influence changefor subcontracted construction projects.
Line management did not ensure that the ISMframework was clearly communicated to the sub-tiercontractor.
Line management did not verify that subcontractorsand sub-tier contractors were utilizing the ISMframework in day-to-day work operations.
There were multiple levels of contracts from DOE toFermilab to subcontractor and sub-tier contractor. Theset of requirements was adequate, but administrationof the various tier contracts from the Office of Science(SC), to the Chicago Operations Office (CH), to theFAO, to Fermilab, and to S. A. Healy to Layne-Western was not adequate.
DOE roles and responsibilities are established by therespective Functions, Responsibilities, AuthoritiesManuals for the Office of ES&H Oversight (EH-2),the Office of Science (SC), the Chicago OperationsOffice (CH), and FAO. Many of these responsibilitiesfor both line and independent oversight were notimplemented at Fermilab.
CH delegated oversight role to the FAO through theCH Functions, Responsibilities, Authorities Manual.
FAO documentation identifies oversight responsibilitiesfor the NuMI construction project.
NuMI Project Management Plan identified roles andresponsibilities for the NuMI Project but was only“provisionally approved pending peer review” by theOffice of Science on March 8, 1999.
FESHM 7010 defined Fermilab ES&H roles andresponsibilities for subcontractor construction safety.
Job letter did not provide specificprocedural controls to identify thehazards associated with the job or providecontrols for the work hazards.
Fermilab has not demonstrated thecommitment to implement ES&Hrequirements for operations involvingcontractors, as illustrated by the severityand frequency of past accidents,incidents, and near misses over the pastyear at the NuMI Project.
The flowdown of ISM processes to S. A.Healy and Layne-Western, the sub-tiercontractor, could have prevented thisaccident.
Administration of all aspects of allcontracts would have resulted inapplication of safety and healthrequirements specified in thosecontracts, thus preventing the use ofsubstandard equipment and therebypreventing the accident.
Lack of independent oversight andeffective line management oversight byall organizations and management levelspermitted hazards to go unrecognized andunmitigated.
Lack of line management oversightallowed inconsistent imple-mentation ofFESHM 7010. Its application to sub-tiercontractors remained unclear, so safetyoversight responsibility for sub-tiercontractors was not clear.
The construction coordinators for theNuMI Project did not understand andtherefore did not implement their safetyand health roles and responsibilities.
S. A. Healy and Layne-Western linemanagement did not actively engage insafety oversight.
Hazard: Energy released from the breakingmechanism due to the failed weld
Target: Drill Rig Crew
What were thebarriers?
How dideach barrier
perform?
Why did the barrier fail? How did the barrier affectthe accident?

54
The Layne-Western work package (“jobletter”) for the drilling operation did notidentify the job-specific tasks or analyzethe hazards. The hazard analysisdeveloped just before the accident didnot identify the specific job tasks or thehazards associated with those tasks. Adetailed, task-level hazard analysiswould have identified the potentialhazard of the tong handle and would haveprescribed appropriate controls. Thiswould have prevented the accident.
Implementation of an effectiveequipment maintenance program wouldhave identified the substandard conditionof the drill rig before use. Thisidentification could have led to propermaintenance of the drill rig andassociated tools, thus preventing theaccident.
Implementation of the equipmentinspection program requirements wouldhave identified the substandard conditionof the drill rig and associated toolsbefore use.
Testing and inspection of the weldbefore use would have identified thesubstandard weld and resulted in a more
Failed
Failed
Failed
Not Used
Hazard: Energy released from the breakingmechanism due to the failed weld
Target: Drill Rig Crew
What were thebarriers?
How dideach barrier
perform?
Why did the barrier fail? How did the barrier affectthe accident?
However, the manual was not based on the projectmanagement organization at the time of the accident,nor did it address the roles and responsibilities whensub-tier contractors were involved.
S. A. Healy and Layne-Western roles andresponsibilities were clearly defined, but they werenot executed as specified in the respective safety andhealth manuals.
FESHM 7010 established a hazard analysis processfor construction subcontractor work. However, thisprocess was not implemented for the Layne-Westernjob. The project was drilling its fifth hole beforeS. A. Healy requested a hazard analysis, even thoughone was required before the start of work.
Drill rig equipment maintenance and inspection werenot performed in accordance with Fermilab andLayne-Western corporate requirements, resulting inthe drilling rig arriving at Fermilab in a degradedcondition.
Documents were not being maintained and thereforedid not accurately inform management of equipmentmaintenance status.
Neither Fermilab nor S. A. Healy conducted a pre-use inspection of Layne-Western equipment when itwas brought on site. Fermilab subcontractor trainingrequired equipment inspection before use. Thistraining was not provided to the Layne-Westernemployees.
ES&H manuals established equipment inspection andmaintenance safety requirements. Vendor manualsestablished equipment specification andrecommendations.
Hoisting and rigging equipment was not tested;electrical installations were not to code; operationsand maintenance guides were not with the drill rig orvehicle; and drill rig equipment modification and repairwere not controlled.
An incomplete weld repair was made to the eyeboltand piston rod connection in 1999. There was nodocumentation to verify the adequacy of the weld.
Core Function 2Hazard Analysis
Core Function 3Maintenance
Core Function 3Inspection ofequipment
Core Function 3Testing following repair

55
Hazard: Energy released from the breakingmechanism due to the failed weld
Target: Drill Rig Crew
What were thebarriers?
How dideach barrier
perform?
Why did the barrier fail? How did the barrier affectthe accident?
Public documents from the International Associationof Drilling Contractors discussed the proper positioningof the drilling crew to safely make or break a pipe string.These public documents were available on theorganization’s website. The drill rig crew did notimplement recommended industry practice at the timeof the accident.
The S. A. Healy Safety Director position requiredcertain qualifications and/or experience that were notmet by the individual filling this position.
Two stand-downs on June 9 and June 13 did not includeLayne-Western personnel. Layne-Western did notparticipate in site-specific training (i.e., FEHSM siteorientation).
Layne-Western management appointed the drill rigOperator as the Competent Person. The Operator alsoserved as the safety supervisor for the drilling operation.This person did not meet the S. A. Healy contractualdefinition of a Competent Person. Training recordsfor the designated Competent Person did not includeany training on hazard analysis or recognition, nor didhe receive the 30-hour OSHA construction safetycourse or equivalent, as required by the contract.
Layne-Western personnel did not receive training onhazard analysis before the start of work.
There is an appropriate set of ES&H requirements inthe contracts between Fermilab, S. A. Healy, andLayne-Western (FESHM 7010, S. A. Healy safetymanual, Layne-Western safety manual).
The associated documents were not provided to Layne-Western (FESHM 7010 and the S. A. Healy safetymanual), nor was the manual found at the job site. S. A.Healy did not receive a copy of the Layne-Westernsafety manual so S. A. Healy could determine whetherthe company met contract safety requirements.
Layne-Western was unaware of the safe workpractices specified in the contract and the S. A. Healysafety manual before the start of work for the NuMIProject.
Layne-Western, S. A. Healy, and Fermilab did notimplement inspection procedures for OSHAcompliance.
controlled repair process, thus eliminatingthe direct cause of the accident.
The Operator’s position at the time ofthe accident resulted in the breakingmechanism (tong handle) striking theOperator.
The Competent Person designated byLayne-Western was not provided withtraining to ensure that he wasknowledgeable of Fermilab-specificrequirements, OSHA, or other relatedsafety standards; therefore, Fermilabmanagement systems (FESHM 7010) didnot flow down to the sub-tier contractor.
No formal training was provided to thedesignated Competent Person beforestarting work to ensure that the hazardanalysis process at Fermilab wasunderstood.
Fermilab, S. A. Healy, and Layne-Western did not implement the proceduralrequirements of FESHM 7010 or theirrespective safety manuals to ensure safeoperation.
Not Used
Failed
Failed
Core Function 3Accepted industrypractice
Core Function 3Training
Core Function 4Procedure use andadherence

56
Hazard: Energy released from the breakingmechanism due to the failed weld
Target: Drill Rig Crew
What were thebarriers?
How dideach barrier
perform?
Why did the barrier fail? How did the barrier affectthe accident?
Core Function 4Work readiness andequipment condition
Core Function 5Corrective Actionprocesses
Core Function 5Lessons learned
Failed
Failed
Not used
The notice to proceed for the Layne-Western workwas not approved by contract administration as requiredby FESHM 7010. The notice to proceed requiredhazard analysis and appropriate permits (excavation,burn permit, etc.).
Fermilab did not ensure that all work was beingperformed consistent with Fermilab safety and healthrequirements.
Two Type B accident investigations of subcontractorsat Fermilab identified hazard analysis and identificationof safety requirements as causal factors.
Implementation of corrective action processes atFermilab was ineffective to ensure that:• Effective hazards analysis processes were
developed and implemented for work involvingsubcontractors and sub-tier contractors.
• Safety requirements were effectivelycommunicated, understood, and implemented bysubcontractors and sub-tier contractors.
The Fermilab investigation of the cement burn incident(March 2001) and the Fermilab-initiated review ofS. A. Healy safety performance and safetymanagement (completed on April 30) identified findingssimilar to the two Type B investigations and thecombined Phase I and II ISM verification conductedin October 1999. All findings related to theinvestigation that are tracked in ESHTRK remain open.
Corrective action plans for the March 2001independent safety audits were not developed andtherefore not tracked in ESHTRK.
Fermilab lacked requirements, direction, or guidanceon the use of lessons learned for constructionsubcontractor operations.
Layne-Western, a sub-tier contractor, did notparticipate in the June 2001 S. A. Healy safety stand-downs. Neither S. A. Healy nor Fermilab ensuredtheir participation in the hazard analysis trainingsession.
Feedback and improvement processes documented inFermilab ISM Plan were ineffective for subcontractorand sub-tier contractor operations.
Fermilab did not ensure that a hazardanalysis was developed, reviewed, andapproved before work.
Fermilab did not verify that the drill rigequipment met safety expectations beforedrilling work.
Corrective action implementation fromprevious Type B accident investigationsand the ISM verification was notadequate to prevent recurrence.
Previous accidents identified that hazardanalysis processes were not effectivelyimplemented for work operationsconducted by sub-tier contractors. Forthe Layne-Western drilling operations, ahazard analysis was not requested ordeveloped before the start of work.
Preparation of the hazard analysis, at thejob and task level, might have identifiedtong handle rotation as a hazard andproper controls could have beenestablished, thus avoiding the accident.
The lessons-learned program failed todisseminate information to theappropriate subcontractor levels.
The mechanism for communicatinglessons learned to constructionsubcontractors was inadequate to assurecontinuous feedback and improvement.
Layne-Western was not given anopportunity to improve its hazard analysisprocess based on Fermilab lessonslearned. The drill crew was not properlyprepared to identify and mitigate alloperational hazards associated with thedrill rig.

57
Hazard: Energy released from the breakingmechanism due to the failed weld
Target: Drill Rig Crew
What were thebarriers?
How dideach barrier
perform?
Why did the barrier fail? How did the barrier affectthe accident?
Core Function 5Performance feedbackprocesses
Physical Barriers
Physicalh u m a n - m a c h i n einterface
Physicallimit on tongmovement
Physical connection ofeyebolt to piston
Failed
Failed
Not Effective
Failed
Review Committee semi-annual reviews providedoversight on behalf of the Office of Science.
The DOE NuMI Program Manager was getting onlylimited information on ES&H status from the DOENuMI Project Manager, who collected only limitedsafety and health information.
The Chicago Operations Office’s delegation of theoversight role to FAO was not effectivelyimplemented for safety oversight.
Fermi ES&H did only environmental reviews forcompliance with the wetlands permit.
Construction coordinators did not focus on safetyduring their daily reviews of the job site, and therewere no documented safety audits. Therefore, trendanalysis for safety was not possible.
S. A. Healy and Layne-Western observations ofsafety were informal and not documented.
The NuMI Project had experienced at least 23incidents involving worker injuries, at least 15 of whichwere recordable incidents that had not been reportedthrough CAIRS. As a result, management was notprovided with an accurate assessment of injury trends.
The location of the operating station used to controlhydraulic pressure to the piston rod placed theOperator near the danger zone of tong handle rotation.No safety bulletin or operating procedure wasavailable at the job site to alert the Operator of thepotential hazard.
The reported physical location of the Operator justbefore the accident placed him within the range ofmotion of the tong handle, inside the physical stop onthe drill rig.
Weld repair of the eyebolt connection to the pistonrod was conducted with no evidence of engineeringreview of the existing design (threaded connection).No engineering analysis of the adequacy of the weldrepair.
Line Management did not use feedbackand assessment processes to maintainaccurate information on the status ofworker health and safety.
The lack of assessment and feedback,through documenting safety observationsof the drill sites and the Layne-Westerntools and equipment, removed a methodof assuring that Layne Western drillingoperations conformed to safetyrequirements.
The Operator was physically locatedinside the danger zone of tong handlerotation while he was attempting to breakpipe when the weld failure occurred.
The Operator was inside the danger zoneof the range of motion of the tong handle.When the weld failed and the tension wasreleased on the tong, the tong was rapidlyrotated by the torsional energy stored inthe pipe string, striking the Operator.
Failure of the welded connection releasedthe tension on the wire rope and tonghandle. Stored energy in the pipe thencaused the tong handle to rotate and strikethe Operator.

58
Tables, Figures, and Exhibits
Tables
ES-1 Causal Factors and Judgments of Need ............................................................................... 43-1 Examples of Safety Deficiencies at the Drilling Site .......................................................... 223-2 Analysis of Previous Fermilab Construction Occurrences ................................................. 283-3 Barrier Analysis Summary ................................................................................................ 373-4 Causal Factors Analysis Summary .................................................................................... 384-1 Judgments of Need ............................................................................................................ 41
Figures
1-1 Organizational Chart Related to the NuMI Project .............................................................. 82-1 Piston Rod End Fixture ......................................................................................................113-1 Layne-Western Job Hazard Analysis Worksheet ............................................................... 193-2 DOE NuMI Organizational Chart ...................................................................................... 263-3 Fermilab Construction Subcontractors Lost Workday Case Rate ...................................... 29
Exhibits
2-1 Drilling Site Where the Accident Occurred ........................................................................ 102-2 Drill Rig Where the Injury Occurred .................................................................................102-3 Eyebolt That Was Connected to the Piston Rod and the End of the Piston Rod
After the Accident .............................................................................................................133-1 Damaged Wire Rope Sling ................................................................................................ 233-2 Electrical Wiring Deficiencies at the Drill Site................................................................... 23

Abbreviations Used in This Report
CAIRS Computerized Accident Information Reporting System
CFR Code of Federal Regulations
DEAR Department of Energy Acquisition Regulation
DOE U. S. Department of Energy
EAV Exhaust Air Vent
EMT Emergency Medical Technician
ES&H Environment, Safety, and Health
ESHTRK Environment, Safety and Health Tracking (system)
FAO DOE Fermi Area Office
Fermilab Fermi National Accelerator Laboratory
FESHM Fermilab Environment, Safety, and Health Manual
HA Hazard Analysis
ISM Integrated Safety Management
JHA Job Hazard Analysis
MSDS Material Safety Data Sheet
NuMI Neutrinos at the Main Injector
OSHA Occupational Safety and Health Administration
PPE Personal Protective Equipment
SC DOE Headquarters Office of Science