Type 2 Diabetes Treatment Options - Bryan Health...TYPE 2 DIABETES MANAGEMENT ---REVIEW OF NEWER...
31
TYPE 2 DIABETES MANAGEMENT --- REVIEW OF NEWER TREATMENT OPTIONS Kara Meinke Baehr MD Nebraska Endocrinology Specialists Bryan Health Primary Care Conference; Lincoln, NE May 20, 2017
Transcript of Type 2 Diabetes Treatment Options - Bryan Health...TYPE 2 DIABETES MANAGEMENT ---REVIEW OF NEWER...

TYPE 2 DIABETES MANAGEMENT ---REVIEW OF NEWER TREATMENT OPTIONS
Kara Meinke Baehr MDNebraska Endocrinology Specialists
Bryan Health Primary Care Conference; Lincoln, NEMay 20, 2017

NO FINANCIAL DISCLOSURES


Common Principles in Type 2 DM Treatment Algorithms
■ Individualize glycemic goals based on patient characteristics
■ Promptly intensify antihyperglycemic therapy to maintain blood glucose at individual targets– Combination therapy necessary for most patients– Base choice of agent(s) on individual patient medical history, behaviors and risk
factors, ethno-cultural background, and environment
■ Insulin eventually necessary for many patients
■ Self-monitoring of blood glucose (SMBG) is vital for day-to-day management of blood sugar– All patients using insulin– Many patients not using insulin
Garber AJ, et al. Endocr Pract. 2016;22:84-113.Inzucchi SE, et al. Diabetes Care. 2015;38:140-149.
4


DPP-4 INHIBITORS(DPP-4 = Dipeptidyl peptidase 4)

DPP-4 Inhibitors
■ FDA-Approved Agents– Alogliptin (Nesina)– Linagliptin (Tradjenta) – Saxagliptin (Onglyza)– Sitagliptin (Januvia)
■ Key Features– Oral administration– Increase endogenous GLP-1 – Increase glucose-dependent
insulin secretion– Suppress glucagon production

Safety Considerationswith DPP-4 Inhibitors
GI adverse events • Minimal
Pancreatitis
• Pancreatitis has been reported with postmarketing use of some of incretin agents, although no causal relationship has been established
• Extensive review by FDA of studies involving >80,000 patients has not uncovered reliable evidence of increased pancreatic risk with incretins vs other agents
• Labeling for all incretins states these agents should be immediately discontinued if pancreatitis is suspected
Pancreatic cancer
• Extensive review by FDA of studies involving >80,000 patients has not uncovered reliable evidence of increased pancreatic risk with incretins vs other agents
• Further assessments required from long duration-controlled studies or epidemiological databases
Renal impairment
• Kidney function monitoring and dose reduction required for alogliptin, saxagliptin, and sitagliptin when used in patients with moderate-to-severe renal impairment
• Linagliptin does not require dose adjustment or periodic monitoring of drug-related kidney function
CHF • Potentially increased risk of congestive heart failure hospitalization with alogliptin and saxagliptin
Garber AJ, et al. Endocr Pract. 2016;22:84-113. White W, et al. N Engl J Med. 2013;369:1327-1335. Scirica BM, et al. Circulation. 2014;130:1579-1588.ADA/EASD/IDF statement concerning the use of incretin therapy and pancreatic disease [news release]. Alexandria, VA: American Diabetes Association, European Association for the Study of Diabetes, International Diabetes Federation; June 28, 2013. http://www.diabetes.org/newsroom/press-releases/2013/recommendations-for.html.

GLP-1 RECEPTOR AGONISTSGLP-1 = (glucagon-like peptide 1)

GLP-1 Receptor Agonists
■ FDA Approved Agents– Albiglutide (Tanzeum)– Dulaglutide (Trulicity)– Exenatide (Byetta)– Exenatide ER (Bydureon)– Liraglutide (Victoza)– Lixisenatide
■ Key Features– Injectable administration– Mimic action of native GLP-1– Increase glucose-dependent
insulin secretion– Suppress glucagon production– Slow gastric emptying

Safety Considerationswith GLP-1 Receptor Agonists
GI adverse events
• Common • Usually dose dependent and transient• Usually reduced with dose titration
Pancreatitis
• Pancreatitis has been reported with postmarketing use of some of incretin agents, although no causal relationship has been established
• Extensive review by FDA of studies involving >80,000 patients has not uncovered reliable evidence of increased pancreatic risk with incretins vs other agents
• Labeling for all incretins states these agents should be immediately discontinued if pancreatitis is suspected• Labeling for GLP-1 receptor agonists suggests consideration of other therapies for patients with a history of
pancreatitis
Pancreatic cancer
• Extensive review by FDA of studies involving >80,000 patients has not uncovered reliable evidence of increased pancreatic risk with incretins vs other agents
• Further assessments required from long duration-controlled studies or epidemiological databases
Medullary thyroid cancer
• Animal data showed an increased incidence of C-cell tumors with liraglutide and exenatide ER treatment, but confirmatory population studies are lacking
• Labeling for liraglutide and exenatide ER:• Patients should be counseled regarding medullary thyroid carcinoma and the signs/symptoms of thyroid
tumors• Contraindicated in patients with personal/family history of MTC or multiple endocrine neoplasia syndrome
type 2
Renal impairment
• Renal Impairment has been reported postmarketing, usually in association with nausea, vomiting, diarrhea, or dehydration (liraglutide found to be safe in patients with moderate renal impairment). Use caution when initiating or escalating doses in patients with renal impairment. Exenatide is contraindicated in patients with severe renal insufficiency or ESRD
ER, extended release.Garber AJ, et al. Endocr Pract. 2016;22:84-113. ADA/EASD/IDF statement concerning the use of incretin therapy and pancreatic disease [news release]. Alexandria, VA: American Diabetes Association, European Association for the Study of Diabetes, International Diabetes Federation; June 28, 2013. http://www.diabetes.org/newsroom/press-releases/2013/recommendations-for.html. Davies MJ, et al. Diabetes Care. 2016;39:222-230.

SGLT2 INHIBITORS(SGLT2 = sodium-glucose cotransporter 2)

SGLT2 Inhibitors
■ FDA- Approved Agents– Canagliflozin (Invokana)– Dapagliflozin (Farxiga) – Empagliflozin (Jardiance)
■ Key Features– Oral administration– Inhibit glucose reabsorption by
the kidneys– Result in increased urinary
excretion of glucose

Safety Considerationswith SGLT2 Inhibitors
Genitourinary infection • Increased incidence; patients should be monitored and treated if necessary
Bladder cancer• Increased incidence of bladder cancers in patients receiving dapagliflozin
• Dapagliflozin labeling recommends not using in patients with active bladder cancer and should be used with caution in patients with a history of bladder cancer
Renal impairment • Monitor kidney function during therapy, especially in patients with GFR <60 mL/min/1.73 m2
Bone fractures• Increased incidence of bone fractures in canagliflozin and dapagliflozin clinical trials
• Canagliflozin labeling includes specific warning about bone fractures
DKA • Potentially increased risk of diabetic ketoacidosis in patients with insulin deficiency and/or those undergoing acute metabolic stress
Garber AJ, et al. Endocr Pract. 2016;22:84-113. Farxiga (dapagliflozin) prescribing information. Princeton, NJ: Bristol-Meyers Squibb Company. 2015. Invokana (canagliflozin) prescribing information. Titusville, NJ: Janssen Pharmaceuticals, Inc. 2015. Jardiance (empagliflozin) prescribing
information. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals, Inc. 2015. Handelsman Y, et al. Endocr Pract. 2016;22:753-762.

NONINSULIN AGENTS:CLASS COMPARISONS

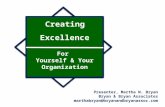
DPP-4 Inhibitors GLP-1 Receptor Agonists SGLT2 InhibitorsAlo1 Lin2 Sax3 Sit4 Alb5 Dul6 Exe7 Exe ER8 Lir9 Can10 Dap11 Emp12
Baseline A1C (%) 7.9 8.1 8.1 8.0 8.1 8.1 8.2 8.6 8.4 7.8 7.9 7.9
Glucose ReductionDPP-4 Inhibitors, GLP-1 Receptor Agonists, and SGLT2 Inhibitors Added to Metformin
(Absolute Changes from Baseline; Not Head-to-Head Trials)
1. Nauck MA, et al. Int J Clin Pract. 2009;63:46-55. 2. Taskinen MR, et al. Diabetes Obes Metab. 2011;13:65-74. 3. DeFronzo RA, et al. Diabetes Care. 2009;32:1649-1655. 4. Charbonnel B, et al. Diabetes Care. 2006;29:2638-2643. 5. Ahrén B, et al. Diabetes Care. 2014;37:2141-2148.6. Dungan KM, et al. Lancet. 2014;384:1349-1357. 7. DeFronzo RA et al. Diabetes Care. 2005;28:1092-1100. 8. Bergenstal RM, et al. Lancet. 2010;376:431-439. 9. Pratley RE, et al. Lancet. 2010;375:1447-1456. 10. Cefalu WT, et al. Lancet. 2013;382:941-950. 11. Nauck MA, et al. Diabetes Care. 2011;34:2015-2022. 12. Haring HU, et al. Diabetes Care. 2014;37:1650-1659.
∆A1
C (%
)
-0.6-0.5
-0.7 -0.7 -0.63
-1.42
-0.8
-1.5 -1.5
-0.93
-0.52
-0.77
-1.6-1.4-1.2
-1-0.8-0.6-0.4-0.2
0

Weight ReductionDPP-4 Inhibitors, GLP-1 Receptor Agonists, and SGLT2 Inhibitors Added to Metformin
(Separate Studies; Not Head-to-Head Trials)
NR, not reported.1. Nauck MA, et al. Int J Clin Pract. 2009;63:46-55. 2. Taskinen MR, et al. Diabetes Obes Metab. 2011;13:65-74. 3. DeFronzo RA, et al. Diabetes Care. 2009;32:1649-1655. 4. Charbonnel B, et al. Diabetes Care. 2006;29:2638-2643. 5. Ahrén B, et al. Diabetes Care. 2014;37:2141-2148.6. Dungan KM, et al. Lancet. 2014;384:1349-1357. 7. DeFronzo RA et al. Diabetes Care. 2005;28:1092-1100. 8. Bergenstal RM, et al. Lancet. 2010;376:431-439. 9. Pratley RE, et al. Lancet. 2010;375:1447-1456. 10. Cefalu WT, et al. Lancet. 2013;382:941-950. 11. Nauck MA, et al. Diabetes Care. 2011;34:2015-2022. 12. Haring HU, et al. Diabetes Care. 2014;37:1650-1659.
NR
DPP-4 Inhibitors GLP-1 Receptor Agonists SGLT2 InhibitorsAlo1 Lin2 Sax3 Sit4 Alb5 Dul6 Exe7 Exe ER8 Lir9 Can10 Dap11 Emp12
-0.3 -0.4-0.9
-1.2
-2.6 -2.8
-2.0
-2.8
-4.0
-3.2
-2.5
-5
-4
-3
-2
-1
0
∆W
eigh
t (kg
)

Cardiovascular Outcomes Trials (CVOT) Recent Data
Liraglutide (Victoza)■ LEADER trial showed liraglutide
significantly reduces the risk of major adverse cardiovascular events compared to placebo in large 5 year study
Empagliflozin (Jardiance)■ Large EMP-REG study showed
significant risk reduction of CV death in patients with Type 2 DM & established CV disease
■ Now has new FDA indication


INSULIN THERAPY


Pharmacokinetics of Available Insulins
22
Agent Onset (h) Peak (h) Duration (h) ConsiderationsBa
sal
NPH 2-4 4-10 10-16 Greater risk of nocturnal hypoglycemia compared to insulin analogs
GlargineDetemirDegludec
~1-4No
pronounced peak
Up to 24† Less nocturnal hypoglycemia compared to NPH
Basa
l-Pr
andi
al
Regular U-500 ≤0.5 ~2-3 12-24
• Inject 30 min before a meal• Indicated for highly insulin resistant individuals• Use caution when measuring dosage to avoid
inadvertent overdose
Pran
dial
Regular ~0.5-1 ~2-3 Up to 8• Inject 30-45 min before a meal• Injection with or after a meal could increase risk for
hypoglycemia
AspartGlulisineLisproInhaled insulin
<0.5 ~0.5-2.5 ~3-5• Can be administered 0-15 min before a meal• Less risk of postprandial hypoglycemia compared to
regular insulin
† Dose-dependent.
NPH, Neutral Protamine Hagedorn.
Moghissi E et al. Endocr Pract. 2013;19:526-535. Humulin R U-500 (concentrated) insulin prescribing information. Indianapolis: Lilly USA, LLC.

Insulin Concentrations
Drugs@FDA. http://www.accessdata.fda.gov/Scripts/cder/DrugsatFDA. Newton C, et al. AACE Annual Meeting. 2013 [abstract 271]. Segal AR, et al. Am J Health Syst Pharm. 2010;67:1526-1535.
• Insulin pens significantly reduce the risk of dosing errors and hypoglycemic events• Pens completely eliminate the need for converting doses based on the volume of insulin
injected• Dosing errors with U-500 insulin vials are common and dangerous but can be avoided with
newly available pens– 5-fold higher insulin dose relative to the same volume of a U-100 insulin
Concentration Units/mL Units/vial Units/pen
U-100 100 1000(10 units per vial)
300(3 mL/pen)
U-200 200 Not available in vials 600(3 mL/pen)
U-300 300 Not available in vials 450(1.5 mL/pen)
U-500 500 10,000(20 units/vial)
1500(1.5 mL/pen)
23

New Basal insulin/GLP-1 RA combinations
Soliqua Xultophy■ Insulin degludec (Tresiba) &
liraglutide (Victoza) combo mix
■ Coming soon
■ Insulin glargine (Lantus) & lixisenatide combo mix– For every 1 unit: get 1 unit of glargine &
0.33 of lixisenatide– Starting dose based on current dose of
basal insulin; dose ranges 15-60 units

EDUCATION TOOL

• Important to have clear insulin instructions for patients
• I have found this instruction sheet especially helpful for:
- MDI (multiple daily injections)- Elderly- Patients new to insulin

CASE STUDIES

“Sarah”■ 45 y/o female with T2DM x 2 years
– Takes Metformin 1000mg BID (normal renal function) & Januvia 100mg daily– BMI 40; desires weight loss– A1c 8.0% today
– Recommendations?

“Bob”■ 58 y/o male with T2DM x 6 years
– Did not tolerate Metformin due to significant diarrhea– Takes Glipizide 10mg BID & Farxiga 10mg daily– No hypoglycemia– A1c 9.2% today
– Recommendations?

“Joe”■ 62 y/o male with T2DM x 16 years; with DM neuropathy
– Takes Levemir 60 units BID & Humalog 35 units with meals– History of pancreatitis– CKD Stage IV– Using vials & now is interested in insulin pen options– A1c 7.4% today with fasting hypoglycemia
– Recommendations?

Conclusions■ Many options available for Type 2 diabetes management
■ Guidelines can help with therapy choices
■ Individualize treatment for what is best for the patient