Tumours of the posterior pharyngeal wall: the use of the platysma flap
5
Clin[ Otolaryn`ol[ 0886\ 22, 135Ð149 Tumours of the posterior pharyngeal wall: the use of the platysma flap J[C[ALVAREZ\ C[SUA lREZ\ E[SOTA\ J[P[RODRIGO\ J[A[FERNA lNDEZ\ J[L[LLORENTE + C[DIAZ Department of Otolaryn`olo`y\ Hospital Central de Asturias\ University of Oviedo\ Spain Accepted for publication 05 August 0885 ALVAREZ J [ C [\ SUA l REZ C [\ SOTA E [\ RODRIGO J [ P [\ FERNA l NDEZ J [ A [\ LLORENTE J [ L [ + DIAZ C [ "0886# Clin[ Otolaryn`ol[ 22, 135Ð149 Tumours of the posterior pharyngeal wall: the use of the platysma flap Posterior pharyngeal wall tumours are infrequent neoplasms with a very poor prognosis[ The 4 year survival rate ranges from 2) to 21)[ Most authors agree that the treatment of choice is surgery with post!operative radiotherapy[ The results of treatment of 25 patients "tumour excision plus bilateral neck dissection and post!operative radiotherapy# in which the posterior pharyngeal wall defect was closed with a platysma myocutaneous ~ap were compared with other forms of repair "02 patients#[ The 4 year survival rate was 06[1) in the whole group[ Laryngeal voice was achieved in 68) of patients having a platysma ~ap reconstruction[ The platysma myocutaneous ~ap is very satisfactory for the repair of the posterior pharyngeal wall as it is easy to perform\ it is oncologically safe and its functional results match well with other forms of reconstruction\ with the advantage of laryngeal preservation[ Keywords pharyn`eal wall squamous carcinoma platysma ~ap head and neck cancer of treatment are to cure the disease while preserving swal! Introduction lowing and\ if possible\ speech[ As these tumours are usually Tumours of the posterior pharyngeal wall are aggressive neo! large in only very few patients can the defect be closed primar! plasms not seen frequently by the head and neck surgeon[ ily[ The repair can be done with split!thickness skin grafts\ Although the AJC and UICC consider the posterior oro! and cutaneous or myocutaneous ~aps\ visceral transpositions and\ hypopharyngeal walls as distinct\ and the T!stage classi! in the last decade\ microvascular free ~aps\ most of these _cation for these tumours is di}erent\ there is no true ana! procedures involving a total laryngectomy[ The aim of this tomical separation[ When they are diagnosed\ usually they paper is to compare the oncological and functional results of involve both regions due to the tendency to submucosal reconstruction with a platysma myocutaneous ~ap and other spread[ However\ deep invasion is not frequent and generally reconstructive techniques that we have used[ it is limited by the prevertebral fascia[ Involvement of the pyriform fossa and prevertebral soft tissues are also late _nd! ings[ Patients and methods Patients with posterior pharyngeal wall tumours have a poor survival rate\ generally less than 19) after 4 years[ Sixty patients with a posterior pharyngeal wall tumour were Some authors relate this poor prognosis to the tendency of treated in our department from February 0866 to September submucosal spread\ 0 early nodal involvement\ 1Ð5 high inci! 0882[ Eleven patients were considered non!surgical candidates dence of metastases to the retropharyngeal nodes\ 6\7 distant due to poor general condition\ distant metastases or massive metastases and second primary tumours[ 1\5\8\09 loco regional involvement and they were treated palliatively Due to this bad prognosis\ an initial aggressive therapy with chemotherapy and:or radiotherapy and excluded from should be encouraged[ Nowadays\ surgery with post!oper! the study[ The patients included in the study were 36 men and ative radiotherapy is the treatment of choice[ 0\00Ð03 The aims two women[ All of them\ except one woman\ were alcohol and tobacco users "more than 19 cigarettes a day#[ Their mean Correspondence] J[C[ Alvarez\ Fuertes Acevedo 47[ 2>C\ 22995 Oviedo\ Spain[ age was 45[1 years "range 24Ð67 years# and the average time 135 Þ 0886 Blackwell Science Ltd
-
Upload
jc-alvarez -
Category
Documents
-
view
219 -
download
6
Transcript of Tumours of the posterior pharyngeal wall: the use of the platysma flap

Clin[ Otolaryn`ol[ 0886\ 22, 135Ð149
Tumours of the posterior pharyngeal wall: the use of theplatysma flap
J[C[ALVAREZ\ C[SUAłREZ\ E[SOTA\ J[P[RODRIGO\ J[A[FERNAłNDEZ\
J[L[LLORENTE + C[DIAZDepartment of Otolaryn`olo`y\ Hospital Central de Asturias\ University of Oviedo\ Spain
Accepted for publication 05 August 0885
ALVAREZ J [C [ \ SUAłREZ C [ \ SOTA E [ \ RODRIGO J [P [ \ FERNAłNDEZ J [A [ \ LLORENTE J [L [ + DIAZ C ["0886# Clin[ Otolaryn`ol[ 22, 135Ð149
Tumours of the posterior pharyngeal wall: the use of the platysma flap
Posterior pharyngeal wall tumours are infrequent neoplasms with a very poor prognosis[ The 4 yearsurvival rate ranges from 2) to 21)[ Most authors agree that the treatment of choice is surgery withpost!operative radiotherapy[ The results of treatment of 25 patients "tumour excision plus bilateral neckdissection and post!operative radiotherapy# in which the posterior pharyngeal wall defect was closed witha platysma myocutaneous ~ap were compared with other forms of repair "02 patients#[ The 4 year survivalrate was 06[1) in the whole group[ Laryngeal voice was achieved in 68) of patients having a platysma~ap reconstruction[ The platysma myocutaneous ~ap is very satisfactory for the repair of the posteriorpharyngeal wall as it is easy to perform\ it is oncologically safe and its functional results match well withother forms of reconstruction\ with the advantage of laryngeal preservation[
Keywords pharyn`eal wall squamous carcinoma platysma ~ap head and neck cancer
of treatment are to cure the disease while preserving swal!Introductionlowing and\ if possible\ speech[ As these tumours are usually
Tumours of the posterior pharyngeal wall are aggressive neo! large in only very few patients can the defect be closed primar!plasms not seen frequently by the head and neck surgeon[ ily[ The repair can be done with split!thickness skin grafts\Although the AJC and UICC consider the posterior oro! and cutaneous or myocutaneous ~aps\ visceral transpositions and\hypopharyngeal walls as distinct\ and the T!stage classi! in the last decade\ microvascular free ~aps\ most of these_cation for these tumours is di}erent\ there is no true ana! procedures involving a total laryngectomy[ The aim of thistomical separation[ When they are diagnosed\ usually they paper is to compare the oncological and functional results ofinvolve both regions due to the tendency to submucosal reconstruction with a platysma myocutaneous ~ap and otherspread[ However\ deep invasion is not frequent and generally reconstructive techniques that we have used[it is limited by the prevertebral fascia[ Involvement of thepyriform fossa and prevertebral soft tissues are also late _nd!ings[
Patients and methodsPatients with posterior pharyngeal wall tumours have apoor survival rate\ generally less than 19) after 4 years[ Sixty patients with a posterior pharyngeal wall tumour wereSome authors relate this poor prognosis to the tendency of treated in our department from February 0866 to Septembersubmucosal spread\0 early nodal involvement\1Ð5 high inci! 0882[ Eleven patients were considered non!surgical candidatesdence of metastases to the retropharyngeal nodes\6\7 distant due to poor general condition\ distant metastases or massivemetastases and second primary tumours[1\5\8\09
loco regional involvement and they were treated palliativelyDue to this bad prognosis\ an initial aggressive therapy with chemotherapy and:or radiotherapy and excluded from
should be encouraged[ Nowadays\ surgery with post!oper! the study[ The patients included in the study were 36 men andative radiotherapy is the treatment of choice[0\00Ð03 The aims two women[ All of them\ except one woman\ were alcohol
and tobacco users "more than 19 cigarettes a day#[ Their meanCorrespondence] J[C[ Alvarez\ Fuertes Acevedo 47[ 2>C\ 22995Oviedo\ Spain[ age was 45[1 years "range 24Ð67 years# and the average time
135 Þ 0886 Blackwell Science Ltd

Tumours of the posterior pharyn`eal wall 136
Table 0[ Type of closure*38 patients operated upon Table 1[ TNM stage*ÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐ*ÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐ
28 Platysma ~ap T0 T1 T2 T3
*ÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐ5 Direct closure3 Deltopectoral ~ap N9 1 1 6 1
N0 0 9 1 92 Jejunum free ~ap0 Pectoralis major ~ap N1 1 3 05 7
N2 0 9 0 0*ÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐ*ÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐNumber of patients operated\ according to their TNM stage[
from the onset of symptoms was four months[ Surgical ther!apy "Table 0# consisted of tumour reaction\ pharyngeal wall
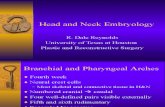
Resultsrepair and bilateral modi_ed or radical neck dissection[ Ofthe 38 patients operated upon\ in six "01[1)# the defect was The actuarial 4 year survival rate for the 38 patients operatedsmall enough for direct closure or suture to the prevertebral upon\ was 06[1) "Fig[ 1#[ Five patients "09[1)# died due tofascia and no ~ap was used for reconstruction[ For the remain! postoperative complications[ The cause of death was pneu!der\ reconstruction was achieved with a tubed pectoralis major monia "_ve platysma and one deltopectoral ~ap#\ cerebro!myocutaneous ~ap in one "1)#\ deltopectoral ~ap in four vascular accident "one platysma ~ap# and accute haemorrhage"7[1)#\ jejunum free ~ap in two "3[0)# and platysma myocu! "one direct closure# "Table 2#[taneous ~ap in 25 "62[4)#[ All patients received post!oper! Of the 25 patients reconstructed with a platysma ~ap\ par!ative radiotherapy[ tial ~ap necrosis occurred in three patients "7[2)# and two of
All patients had a tracheostomy in the postoperative period[ them developed a pharyngocutaneous _stula[ Total necrosisA total laryngectomy was done in 09 patients because of was observed in three platysma ~aps "7[2)# and none of theminvolvement of the piriform fossa by tumour "four platysma\ developed a _stula as the defect healed spontaneously on thethree deltopectoral\ one pectoral and two jejunum#[ muscle[ In the whole group of patients reconstructed with
The platysma myocutaneous ~ap was employed according a platysma ~ap\ there were nine "14)# pharyngocutaneousto the technique described by Sua�rez et al[04 To do it\ an L! _stulae that healed with conservative measures\ eight "11)#shaped incision is made on one side and is deepened to the wound infections and two "4)# cases of pneumonia "Tablelevel of super_cial cervical fascia[ The incision in the upper 2#[ In the group of 02 patients reconstructed in other ways\border of the ~ap reaches the level of the platysma muscle[ On a pharyngocutaneous _stula developed in one patient afterthe other side we usually do a stick shaped and supraclavicular deltopectoral ~ap repair\ in both jejunum free ~aps and in oneincision "Fig[ 0a#[ The skin island and the muscle pedicle are patient in whom direct closure was possible "Table 2#[elevated "Fig[ 0b#[ Skin is dissected from the platysma muscle\ The patient with a deltopectoral ~ap and preservation ofon the side where the ~ap is to be developed\ until a point the larynx was never able to swallow properly[ In patientssome 1 or 2 cm inferior to the mandible is reached "Fig[ 0c#[ who had a platysma ~ap with laryngeal preservation\ fourOn the other side\ skin and muscle are elevated at the same completion laryngectomies were performed due to intractabletime "Fig[ 0b#[ The operation proceeds as usual\ and care must aspiration and\ in another swallowing improved considerablybe taken not to divide the facial artery on the side of the after an epiglottoplasty[ In 15 patients\ after platysma ~ap~ap[ The tumour is resected through a lateral pharyngotomy reconstruction with laryngeal preservation\ only nine patientsapproach "Fig[ 0d#[ The inferior pharyngeal constrictor\ the "23)# were successfully decannulated[ The rest dependedsuperior laryngeal artery and vein\ and the superior laryngeal upon their tracheostomies due to minor problems of aspir!nerve are divided[ To improve access\ the superior cornu of ation while eating[the thyroid cartilage is resected[ The tumour is removed andthe ~ap is sutured to the mucosa surrounding the defect "Fig[ Discussion0e#\ closing the pharynx "Fig[ 0f#[
There are very few studies concerning the treatment of pos!Considering that only four patients had stage I or II disease\terior pharyngeal wall tumours due to the low frequency ofwe have not made any distinction between those tumours
arising in the oropharynx from those originating in the hypo!pharynx as most tumours a}ected both[ In a recent paper\
Table 2[ ComplicationsBarzan et al[05 state that there is no signi_cant di}erence in *ÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐ
Mortality Complication ratesurvival between tumours originated in the posterior wall of*ÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐthe hypo or oropharynx[ In Table 1\ the TNM stages areTotal "n � 38# 4:38 "09)# 07:38 "25[6)#shown[ In our series none of the patients had synchronousPlatysma "n � 25# 2:25 "7)# 03:25 "27[7)#
tumours and 29 "50[1)# had clinical evidence of neck nodes Other ~aps "n � 6# 0:6 "03)# 2:6 "31[7)#when diagnosed[ The estimation of survival was made accord! Direct closure "n � 5# 0:5 "05[5)# 0:5 "05[5)#
*ÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐÐing to the actuarial method of KaplanÐMeier[06
Þ 0886 Blackwell Science Ltd\ Clinical Otolaryn`olo`y\ 11\ 135Ð149

137 J[C[Alvarez et al[
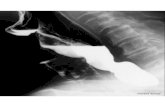
Figure 0[ "a# Skin incisions and ~ap area[ We can obtain an area of maximum dimensions 09×4 cm[ "b# Elevation of cervical skin and ~ap[Note the detachment of subcutaneous tissue from the platysma muscle on the side of the ~ap[ "c# The skin is elevated until a point 1Ð2 cm belowthe horizontal ramus of the mandible[ "d# Lateral pharyngotomy approach[ Superior laryngeal nerve\ superior thyroid artery and vein aresevered and ligated[ "e# The superior cornu of the thyroid cartilage is resected[ The tumour is removed and the skin of the ~ap is sutured to thesurrounding mucosa[ "f# The pharynx is closed suturing the lateral border of the skin island to the mucosa of the lateral pharyngeal wall[ 0\Platysma muscle[ 1\ Super_cial cervical fascia[ 2\ Superior laryngeal nerve[ 3\ Superior thyroid artery[ 4\ Superior thyroid vein[ 5\ Internaljugular vein[ 6\ Common carotid artery[ 7\ Inferior constrictor muscle[ 8[ Thyroid gland[
Þ 0886 Blackwell Science Ltd\ Clinical Otolaryn`olo`y\ 11\ 135Ð149

Tumours of the posterior pharyn`eal wall 138
100
01
Months
% S
urv
ivo
rs
50
90
80
70
60
40
30
20
10
5 9 13 17 21 25 29 33 37 41 45 49 53 57 61 65 69 73
Figure 1[ Actuarial survival rate[ e\ platysma ~ap "n � 25#^ �\ others "n � 02#^ r\ total "n � 38#[
these neoplasms if we compare them with other pharyngeal of life as it permits normal speech[ We have seen that post!operative swallowing does not depend on the area resectedsites[ However\ all authors agree on the poor prognosis of
these neoplasms[0\4\01Ð03\07 Radiotherapy alone is not an but on another yet unknown factor\ as some patients withsmall tumours are never able to swallow while others withadequate method of treatment0\08\19 due to the low cure rate if
compared with that of surgery plus radiotherapy[ On the other huge defects have no aspiration at all[ The main problem\when closing these pharyngeal defects lies in the fact that onehand\ moderate doses of radiotherapy are ine}ective07 but
high doses in this region can produce serious complications[07 must respect pharyngeal muscles and transect one superiorlaryngeal nerve[ The defect is closed with tissues that lack theMost authors prefer post!operative radiotherapy as there is
no demonstrated bene_t on survival with pre!operative radio! contractile properties of the pharynx and have no sensationat all[ As they have no mucosal lining\ many of them contracttherapy10 and there is a high risk of complications when
operating on a previously irradiated patient[ and produce strictures[ All these factors predispose to aspir!ation[When performing a total pharyngo!laryngectomy the most
common methods of reconstruction are pectoralis major Partial pharyngectomy\ bilateral neck dissection and recon!struction with a platysma ~ap is a single stage procedure[ Itmyocutaneous ~ap\ visceral transposition and jejunum free
~ap[ Most posterior pharyngeal wall tumours are suitable for is a reliable ~ap\ with a low risk of necrosis[ When necrosisoccurred\ healing was spontaneous\ with no need for sub!a partial resection\ which obviates the need for a complex
reconstruction and the loss of the larynx[ When the defect is sequent procedures[ Another advantage is that it is an easy~ap to develop\ it is hairless and there is no donor sitesmall\ it is amenable to direct closure\ partial thickness skin
graft or suture to the prevertebral fascia[ However\ if the morbidity[ We always preserve the facial artery although it isnot strictly necessary17 as the blood supply depends on thedefect is large or it a}ects the lateral pharyngeal wall\ a ~ap
should be used[ submental branch of the facial artery[ If there are massiveneck metastases and the jugular vein must be resected there isMost regional ~aps are too thick to allow reasonable post!
operative swallowing if the larynx is preserved[ Only the plat! a high risk of necrosis and the ~ap should be dissected on theother side[ Although some authors do not consider radio!ysma ~ap is thin enough to allow laryngeal preservation[ Some
authors perform a partial pharyngectomy with laryngeal pres! therapy as an absolute contraindication17\18 we never use this~ap in previously irradiated patients[ In these patients weervation and close the defect with a free jejunum {patch|
graft11\12 specially in high pharyngeal lesions[13 They report agree with Esclamado et al[29 that microvascular free ~aps area better option[good results with low complication rates[ The disadvantages
are the requirements for three surgical teams\ the need for Actuarial survival rates vary according to the series and themethod of treatment[ Our actuarial 4 year survival rate ofabdominal surgery which increases complications11 and the
duration of the surgical procedure without any functional 06[1) compares well with other series[ We must considerthat 34 "80[7)# patients were stage IIIÐIV[ We compared theadvantage over the platysma ~ap[ Another possibility is the
radial forearm free ~ap[14Ð16 All these free ~aps are complex results of treatment in stage IÐII patients with those in stageIIIÐIV with the log!rank test\ but the results were not sig!and time!consuming[ They have no better functional results
than reconstruction with a platysma ~ap\ as pharyngeal mus! ni_cant as the former group contained only four patients"7[1)#[ There is a great di}erence in _ve years survivalcles are resected and sensory innervation is partially lost[
In 22 patients in which the repair was done with a platysma between the group of patients reconstructed with a platysma~ap "19[4)# at 4 years\ and those reconstructed in other ways~ap we have preserved the larynx[ This improves the quality
Þ 0886 Blackwell Science Ltd\ Clinical Otolaryn`olo`y\ 11\ 135Ð149

149 J[C[Alvarez et al[
8 BALLANTYNE A[J[ "0856# Principles of surgical management of"9)# at 1 years[ We think that there are no real di}erencescancer of pharyngeal walls[ Cancer 19\ 552Ð556between them as survival depends on a sound oncological
09 STEFANI F[ + FELS R[W[ "0860# Carcinoma of the hypopharynx*resection\ not on the method employed for reconstruction[ a study of distant metastases\ treatment failures\ and multiple
We had three deaths "7[2)# in the group of patients recon! primary cancers in 104 male patients[ Laryn`oscope 70\ 0380Ð038600 SHAH J[P[\ SHAHA A[R[\ SPIRO R[H[ + STRONG E[W[ "0865# Car!structed with a platysma ~ap\ and two "04)# in those recon!
cinoma of the Hypopharynx[ Am[ J[ Sur`[ 021\ 328Ð332structed in other ways[ The total mortality is _ve "09)#01 MCNEILL R[ "0870# Surgical management of carcinoma of the
patients[ That could seem high\ but it is in the range of results posterior pharyngeal wall[ Head Neck Sur`ery 2\ 278Ð283reported in the literature for this kind of surgery[ 02 TEICHGRAEBER J[F[ + MCCONNELL F[M[S[ "0875# Treatment of
posterior pharyngeal wall carcinoma[ Otolaryn`ol[ Head NeckIn 29 of the 22 patients reconstructed with a platysma ~apSur`[ 83\ 176Ð189who completed the post!operative period the larynx could be
03 SPIRO R[H[\ KELLY J[\ LUNA!VEGA A[\ HARRISON L[B[ + STRONGpreserved\ but completion laryngectomy was necessary inE[ "0889# Squamous carcinoma of the Posterior Pharyngeal wall[
four[ Only nine "23)# patients of the 15 whose larynx was Am[ J[ Sur`[ 059\ 319Ð312preserved\ could be successfully decannulated[ However\ the 04 SUAłREZ C[\ LORENZO GALLEGO L[ + GALAłN CORTEłS J[C[ "0872#
Reconstruction of the posterior wall of the pharynx using aother 06 have a normal voice although they need to keep theirmyocutaneous platysma ~ap[ Br[ J[ Plast[ Sur`[ 25\ 25Ð28stoma open when they eat due to some degree of aspiration[
05 BARZAN L[\ BARRA S[\ FRANCHIN G[ et al[ "0884# Squamous cellThe remaining part of the day they can breathe and speak carcinoma of the posterior pharyngeal wall] characteristics com!normally[ After hospital discharge more needed a nasogastric pared with the lateral wall[ J[ Laryn`ol[ Otol[ 098\ 019Ð014
06 KAPLAN E[ + MEIER P[ "0847# Nonparametric estimation fortube of gastrostomy to be fed[incomplete observation[ J[ Am[ Stat[ Assoc[ 42\ 346Ð370In conclusion\ we think that reconstruction of the posterior
07 WANG C[C[ "0860# Radiotherapeutic Management of Carcinomapharyngeal wall with a platysma myocutaneous ~ap is aof the Posterior Pharyngeal Wall[ Cancer 16\ 783Ð785
reliable method both on oncological and on functional 08 MARKS J[E[\ SMITH P[G[ + SESSIONS D[G[ "0874# Pharyngeal wallgrounds[ cancer] A reappraisal after comparison of treatment methods[
Arch[ Otolaryn`ol[ 000\ 68Ð7419 KAJANTI M[ + MAÝNTYLAÝ M[ "0889# Carcinoma of the hypo!
pharynx[ A retrospective analysis of the treatment results over aAcknowledgements 14!year period[ Acta Oncolo`ica 18\ 892Ð896
10 SNOW J[B[\ GELBER R[D[\ KRAMER S[\ DAVIS L[W[\ MARICALThis work has been supported with a grant FISS 82:9399[ V[A[ + LOWRY L[D[ "0879# Randomized pre!operative and post!
operative radiation therapy for patients with carcinoma of thehead and neck] preliminary report[ Laryn`oscope 89\ 829Ð834
11 GLUCKMAN J[L[\ MCDONOUGH J[J[\ MCCAFFERTY G[J[ "0874#References Complications associated with free jejeunal graft reconstruction
of the pharyngoesophagus] a multi!institutional experience with0 PENE F[\ AVEDIAN V[\ ESCHWWEGE\ F[\ BARRETT A[\ SCHWAAB G[\
41 cases[ Head Neck Sur`[ 6\ 199Ð1994MARANDAS P[\ VAN DEN BROUCK C[ "0867# A retrospective study 12 SALASSA S[R[\ LYNCH D[\ LENIS A[ + VERHEYDEN C[ "0876# Pos!of 020 cases of carcinoma of the posterior pharyngeal wall[ Cancer terior wall pharyngectomy with preservation of laryngeal function[31\ 1389Ð1382 Otolaryn`ol[ Head Neck Sur`[ 86\ 68Ð71
1 CUNNINGHAM M[P + CATLIN D[ "0856# Cancer of the Pharyngeal 13 GULLANE P[\ HAVAS T[\ PATTERSON A[\ TODD T[ + BOYD B[ "0876#wall[ Cancer 19\ 0748Ð0755 Pharyngeal Reconstruction] Current Controversies[ J[ Otol!
2 APPAIX A[\ PECH A[\ ALMARIC R + VIDAL A[ "0857# Con! aryn`ol[ 05\ 058Ð062siderations sur les cancers pharinge�s poste�rieurs[ Ann[ Otolarin`ol[ 14 CHEN H[\ TANG Y[ + NOORDHOFF M[S[ "0878# Reconstruction of74\ 028Ð047 the entire esophagus with {{chain ~aps|| in a patient with severe
3 SILVA N + SHEDD D[P[ "0860# Pattern of lymphatic spread in corrosive injury[ Plastic[ Reconstr[ Sur`[ 73\ 879Ð873pharyngeal cancer[ J[ Sur`[ Oncol[ 2\ 304Ð308 15 JONES A[S[ + STELL P[M[ "0880# Squamous carcinoma of the
4 WILKINS S[A[ JR[ "0860# Carcinoma of the posterior pharyngeal posterior pharyngeal wall[ Clin[ Otolaryn`ol[ 05\ 351Ð354wall[ Am[ J[ Sur`[ 011\ 366Ð370 16 SHESTAK K[C[\ MYERS E[N[\ RAMASASTRY S[S[\ JONES N[F + JOHN!
5 GUILLAMONDEGUI O[M[\ MEOZ R + JESSE R[H[ "0867# Surgical SON J[T[ "0882# Vascularised free!tissue transfer in head and necktreatment of squamous cell carcinoma of pharyngeal walls[ Am[ surgery[ Am[ J[ Otolaryn`ol[ 03\ 037Ð043J[ Sur`[ 025\ 363Ð365 17 MCGUIRT W[F[\ MATTHEWS B[L[\ BRODY J[A[ + MAY J[S[ "0880#
6 HASEGAWA Y[ + MATSUURA H[ "0883# Retropharyngeal node Platysma myocutaneous ~aps] caveats reexamined[ Laryn`oscopedissection in cancer of the oropharynx and hypopharynx[ Head 090\ 0127Ð0133and Neck\ 05\ 062Ð079 18 MAGRIN J[\ KOWALSKI L[P[\ SANTO G[E[\ WALKSMANN G[ +
7 MCLAUGHLIN M[P[\ MENDENHALL W[M[\ MANCUSO A[A[\ PAR! DIPAULA R[A[ "0882# Infrahyoid myocutaneous ~ap in head andSONS J[T[\ MCCARTY P[J[\ CASSISI N[J[\ STRINGER S[P[\ TART R[P[\ neck reconstruction[ Head and Neck 04\ 411Ð414MUKHERJI S[K[ + MILLION R[R[ "0884# Retropharyngeal aden! 29 ESCLAMADO R[M[\ BURKEY B[B[\ CARROLL W[R[ + BRADFORD
opathy as a predictor of outcome in squamous cell carcinoma of C[R[ "0883# The platysma myocutaneous ~ap[ Indications andcaveats[ Arch[ Otolaryn`ol[ Head Neck Sur`[ 019\ 21Ð24the head and neck[ Head and Neck 06\ 089Ð087
Þ 0886 Blackwell Science Ltd\ Clinical Otolaryn`olo`y\ 11\ 135Ð149