Tumours of the Lung - iarc.fr · CHAPTER 1 Tumours of the Lung With more than 1.1 million deaths...
116
CHAPTER 1 Tumours of the Lung With more than 1.1 million deaths annually worldwide, lung cancer is the most frequent and one of the most deadly cancer types. In men, 85-90% of cases can be attributed to tobacco smoking. Some Western countries in which the smoking habit took off about 100 years ago, tobacco control programmes have led to a significant decline in mortality. Unfortunately, the habit has now spread to many newly industrialized countries, particularly in Asia, and in Europe, there is a worrying trend of increasing smoking prevalence in young women. The progno- sis of lung cancer is still poor, with 5-years survival rates of approximately 10% in most countries. Thus, primary prevention by not starting or by stopping smoking remains the most prom- ising approach. The association between smoking and lung cancer is not sole- ly based on epidemiological studies. Lung tumours of smokers frequently contain a typical, though not specific, molecular fin- gerprint in the form of G:C > T:A mutations in the TP53 gene which are probably caused by benzo[a]pyrene, one of the many carcinogens in tobacco smoke.
-
Upload
hoangquynh -
Category
Documents
-
view
216 -
download
0
Transcript of Tumours of the Lung - iarc.fr · CHAPTER 1 Tumours of the Lung With more than 1.1 million deaths...

CHAPTER 1
Tumours of the Lung
With more than 1.1 million deaths annually worldwide, lungcancer is the most frequent and one of the most deadly cancertypes. In men, 85-90% of cases can be attributed to tobaccosmoking. Some Western countries in which the smoking habittook off about 100 years ago, tobacco control programmeshave led to a significant decline in mortality. Unfortunately, thehabit has now spread to many newly industrialized countries,particularly in Asia, and in Europe, there is a worrying trend ofincreasing smoking prevalence in young women. The progno-sis of lung cancer is still poor, with 5-years survival rates ofapproximately 10% in most countries. Thus, primary preventionby not starting or by stopping smoking remains the most prom-ising approach.The association between smoking and lung cancer is not sole-ly based on epidemiological studies. Lung tumours of smokersfrequently contain a typical, though not specific, molecular fin-gerprint in the form of G:C > T:A mutations in the TP53 genewhich are probably caused by benzo[a]pyrene, one of themany carcinogens in tobacco smoke.

10 Tumours of the lung - WHO Classification
WHO histological classification of tumours of the lung
__________1 Morphology code of the International Classification of Diseases for Oncology (ICD-O) {6} and the Systematized Nomenclature of Medicine (http://snomed.org).
Behaviour is coded /0 for benign tumours, /3 for malignant tumours, and /1 for borderline or uncertain behaviour.
Malignant epithelial tumoursSquamous cell carcinoma 8070/3
Papillary 8052/3Clear cell 8084/3Small cell 8073/3Basaloid 8083/3
Small cell carcinoma 8041/3Combined small cell carcinoma 8045/3
Adenocarcinoma 8140/3Adenocarcinoma, mixed subtype 8255/3Acinar adenocarcinoma 8550/3Papillary adenocarcinoma 8260/3Bronchioloalveolar carcinoma 8250/3
Nonmucinous 8252/3Mucinous 8253/3Mixed nonmucinous and mucinous or indeterminate 8254/3
Solid adenocarcinoma with mucin production 8230/3Fetal adenocarcinoma 8333/3Mucinous (“colloid”) carcinoma 8480/3Mucinous cystadenocarcinoma 8470/3Signet ring adenocarcinoma 8490/3Clear cell adenocarcinoma 8310/3
Large cell carcinoma 8012/3Large cell neuroendocrine carcinoma 8013/3
Combined large cell neuroendocrine carcinoma 8013/3Basaloid carcinoma 8123/3Lymphoepithelioma-like carcinoma 8082/3Clear cell carcinoma 8310/3Large cell carcinoma with rhabdoid phenotype 8014/3
Adenosquamous carcinoma 8560/3
Sarcomatoid carcinoma 8033/3Pleomorphic carcinoma 8022/3Spindle cell carcinoma 8032/3Giant cell carcinoma 8031/3Carcinosarcoma 8980/3Pulmonary blastoma 8972/3
Carcinoid tumour 8240/3Typical carcinoid 8240/3Atypical carcinoid 8249/3
Salivary gland tumoursMucoepidermoid carcinoma 8430/3Adenoid cystic carcinoma 8200/3Epithelial-myoepithelial carcinoma 8562/3
Preinvasive lesionsSquamous carcinoma in situ 8070/2Atypical adenomatous hyperplasiaDiffuse idiopathic pulmonary neuroendocrine cell hyperplasia
Mesenchymal tumoursEpithelioid haemangioendothelioma 9133/1Angiosarcoma 9120/3Pleuropulmonary blastoma 8973/3Chondroma 9220/0Congenial peribronchial myofibroblastic tumour 8827/1Diffuse pulmonary lymphangiomatosisInflammatory myofibroblastic tumour 8825/1Lymphangioleiomyomatosis 9174/1Synovial sarcoma 9040/3
Monophasic 9041/3Biphasic 9043/3
Pulmonary artery sarcoma 8800/3Pulmonary vein sarcoma 8800/3
Benign epithelial tumoursPapillomas
Squamous cell papilloma 8052/0Exophytic 8052/0Inverted 8053/0
Glandular papilloma 8260/0Mixed squamous cell and glandular papilloma 8560/0
AdenomasAlveolar adenoma 8251/0Papillary adenoma 8260/0Adenomas of the salivary gland type
Mucous gland adenoma 8140/0Pleomorphic adenoma 8940/0Others
Mucinous cystadenoma 8470/0
Lymphoproliferative tumoursMarginal zone B-cell lymphoma of the MALT type 9699/3Diffuse large B-cell lymphoma 9680/3Lymphomatoid granulomatosis 9766/1Langerhans cell histiocytosis 9751/1
Miscellaneous tumoursHarmatomaSclerosing hemangioma 8832/0Clear cell tumour 8005/0Germ cell tumours
Teratoma, mature 9080/0Immature 9080/3Other germ cell tumours
Intrapulmonary thymoma 8580/1Melanoma 8720/3
Metastatic tumours

__________
A help desk for specific questions about the TNM classification is available at http://www.uicc.org/tnm/##The regional lymph nodes are the intrathoracic, scalene, and supraclavicular nodes.
TNM classification of carcinomas of the lung {738,2045}
T – Primary TumourTX Primary tumour cannot be assessed, or tumour proven by the pres
ence of malignant cells in sputum or bronchial washings but not visualized by imaging or bronchoscopy
T0 No evidence of primary tumourTis Carcinoma in situ
T1 Tumour 3 cm or less in greatest dimension, surrounded by lung or visceral pleura, without bronchoscopic evidence of invasionmore proximal than the lobar bronchus, i.e., not in the main bronchus (1)
T2 Tumour with any of the following features of size or extent:• More than 3 cm in greatest dimension• Involves main bronchus, 2 cm or more distal to the carina• Invades visceral pleura• Associated with atelectasis or obstructive pneumonitis that
extends to the hilar region but does not involve the entire lungT3 Tumour of any size that directly invades any of the following:
chest wall (including superior sulcus tumours), diaphragm, mediastinal pleura, parietal pericardium; or tumour in the mainbronchus less than 2 cm distal to the carina1 but without involvement of the carina; or associated atelectasis or obstructive pneumonitis of the entire lung
T4 Tumour of any size that invades any of the following: mediastinum, heart, great vessels, trachea, oesophagus, vertebral body, carina; separate tumour nodule(s) in the samelobe; tumour with malignant pleural effusion (2)
Notes: 1. The uncommon superficial spreading tumour of any size with itsinvasive component limited to the bronchial wall, which mayextend proximal to the main bronchus, is also classified as T1.2. Most pleural effusions with lung cancer are due to tumour. In a few patients, however, multiple cytopathological examinationsof pleural fluid are negative for tumour, and the fluid is non-bloodyand is not an exudate. Where these elements and clinical judgmentdictate that the effusion is not related to the tumour, the effusion should be excluded as a staging element and the patient should beclassified as T1, T2, or T3.
N – Regional Lymph Nodes##
NX Regional lymph nodes cannot be assessedN0 No regional lymph node metastasisN1 Metastasis in ipsilateral peribronchial and/or ipsilateral hilar lymph
nodes and intrapulmonary nodes, including involvement by direct extension
N2 Metastasis in ipsilateral mediastinal and/or subcarinal lymph node(s)
N3 Metastasis in contralateral mediastinal, contralateral hilar,ipsilateral or contralateral scalene, or supraclavicular lymph node(s)
M – Distant Metastasis MX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis, includes separate tumour nodule(s) in a
different lobe (ipsilateral or contralateral)
Stage Grouping Occult carcinoma TX N0 M0Stage 0 Tis N0 M0Stage IA T1 N0 M0Stage IB T2 N0 M0Stage IIA T1 N1 M0Stage IIB T2 N1 M0
T3 N0 M0Stage IIIA T1, T2 N2 M0
T3 N1, N2 M0Stage IIIB Any T N3 M0
T4 Any N M0Stage IV Any T Any N M1
TNM classification of the lung
11TNM classification

Geographical differences
Lung cancer is the most common cancerin the world today (12.6% of all new can-cers, 17.8% of cancer deaths). Therewere an estimated 1.2 million new casesand 1.1 million deaths in 2000; the sexratio (M:F) is 2.7. Lung cancer is relative-ly more important in the developed thandeveloping countries as it accounts for22% versus 14.6% of cancer deaths,respectively. In developed countries,geographic patterns are very much areflection of past exposure to tobaccosmoking {505}.In men, the areas with the highest inci-dence and mortality are Europe (espe-cially Eastern Europe), North America,Australia/New Zealand, and SouthAmerica. The rates in China, Japan andSouth East Asia are moderately high,while the lowest rates are found in south-ern Asia (India, Pakistan), and sub-Saharan Africa. In certain population sub-groups (e.g. US blacks, New ZealandMaoris), incidence is even higher, andwith current incidence rates, men in thesetwo groups have about a 13% chance ofdeveloping a lung cancer before the ageof 75.
In women, the geographic pattern issomewhat different, chiefly reflecting dif-ferent historical patterns of tobaccosmoking. Thus, the highest incidencerates are observed in North America andNorth West Europe (U.K., Iceland,Denmark) with moderate incidence ratesin Australia, New Zealand and China.
Differences by histology
Almost all lung cancers are carcinomas(other histologies comprise well under1%). In the combined data from theseries published in Cancer Incidence inFive Continents {1554}, small cell carci-nomas comprise about 20% of casesand large cell /undifferentiated carcino-mas about 9%. But for the other histolog-ical types, the proportions differ by sex:squamous cell carcinomas comprise44% of lung cancers in men, and 25% inwomen, while adenocarcinomas com-prise 28% cases in men and 42% inwomen. Incidence rates, and the esti-mated rates by histological subtype havebeen reported for 30 populations forwhich a relatively high proportion ofcases had a clear morphological diagno-sis {1554}. Figure 2 shows overall inci-
dence rates, and the estimated rates byhistological subtype for 30 populationsfor which a relatively high proportion ofcases had a clear morphological diagno-sis {1554}. Among men, only in certainAsian populations (Chinese, Japanese)and in North America (USA, Canada)does the incidence of adenocarcinomaexceed that of squamous cell carcinoma.In women, however, adenocarcinoma isthe dominant histological type almosteverywhere, except for Poland andEngland where squamous cell carcino-mas predominate, and Scotland wheresmall cell carcinoma is the most frequentsubtype {1554}. Adenocarcinomas areparticularly predominant in Asianfemales (72% cancers in Japan, 65% inKorea, 61% in Singapore Chinese). Thedifferences in histological profiles arestrongly influenced by the evolution ofthe epidemic of smoking-related lungcancer over time (see below).
Time trends
Because tobacco smoking is such apowerful determinant of risk, trends inlung cancer incidence and mortality are areflection of population-level changes insmoking behaviour, including dose, dura-tion, and type of tobacco used {685,1206}. Study of time trends in lung cancerincidence or mortality by age groupshows that the level of risk is closely relat-ed to birth cohort; in the U.K. and U.S.cohort-specific incidence is related to thesmoking habits of the same generation{228,1152}. Thus, in men, the countrieswhere smoking was first established werefirst to see a diminution in smoking preva-lence, followed, in the same generationsof men, by a decline in risk. Changes arefirst seen among younger age groups{1396}, and as these generations of menreach the older age groups, where lungcancer is most common, a decline inoverall incidence and mortality is seen.The U.K. was the first to show this inci-dence/mortality falling since 1970-74, fol-lowed by Finland, Australia, TheNetherlands, New Zealand, the U.S.A.,Singapore and, more recently, Denmark,Germany, Italy and Sweden {221}. In
12 Tumours of the lung - Introduction
Lung cancer epidemiology
and etiology
M. ParkinJ.E. TyczynskiP. Boffetta
J. SametP. Shields
N. Caporaso
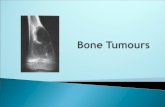
Fig. 1.01 Estimates of the male incidence rates of lung cancer in different world regions, adjusted to theworld standard age distribution (ASR). From Globocan 2000 {572A}.

most other countries there is a continuingrise in rates, and this is most dramatic insome countries of Eastern and SouthernEurope (i.e. Hungary, Spain) {223,2042}.In women, the tobacco habit has usuallybeen acquired recently, or not at all. Thus,the most common picture in western pop-ulations is of rising rates, while in manydeveloping countries (where femalesmoking generally remains rare), lungcancer rates remain very low. A few coun-tries, where prevalence of smoking inwomen is declining, already showdecreasing rates in younger women; inthe U.K., where this trend is longestestablished, there is already a decline in
overall incidence and mortality sinceabout 1990 {221,2042}.There are, however, clear differences intime trends by histological type. In the U.S.{487,2027} squamous cell carcinomareached maximum incidence in men in1981, but the incidence of adenocarcino-ma continued to rise (until about 1987 inblack males, around 1991 in whites). As aresult, adenocarcinoma is now the mostfrequent form of lung cancer in men inUSA, while it had only constituted a smallminority of cases (around 5%) in the 1950s{2027,2029}. In contrast, the incidence ofboth histological types has continued toincrease in females, though there is a sug-
gestion that the incidence of squamouscell carcinomas had reached its maximumby 1990. These changes were related tospecific birth cohorts, with maximum inci-dence in men in the 1925-29 cohort forsquamous cell carcinomas and 1935-39for adenocarcinomas, and in women some10-20 years later {487,2241}. Somewhatsimilar observations (increasing adenocar-cinoma and decreasing squamous cellcarcinoma) have been reported from theNetherlands {923}, Japan {1843} and theU.K. {779}. While part of this differentialtrend may be due to artefact (changes inclassification and coding, improved diag-nostic methods for peripheral tumours), the
13Epidemiology and etiology
Fig. 1.03 A Although cigarette smoking carries the greatest risk of lung cancer, the differences among tobacco products are small when adjusted to similar amountsof tobacco consumption. Adapted from Boffetta et al. {191}. B All lung carcinomas are strongly associated with tobacco smoking, the risk being highest for squa-mous cell carcinoma, followed by small cell carcinoma and adenocarcinoma. Adapted from J.H. Lubin and W.J. Blot {1211} and {2250}.
BA
Fig. 1.02 Trends in male lung cancer mortality. A In some countries with early, high rates, a substantial reduction in mortality began in the 1970s (UK) or 1980s(Belgium, Netherlands, Australia). B In other countries (Italy, USA, Canada), the decline started in the 1990s. C Failure to achieve a significant reduction in tobac-co consumption until recently has in some countries caused rising lung cancer mortality without apparent levelling off in males at ages 55-74. From R. Peto et al.{1589A}.
BA C
creo

14
incidence of adenocarcinomas is truly ris-ing. In part, it may be due to an ever-increasing proportion of ex-smokers in thepopulation, since the decline in risk of lungcancer on smoking cessation is faster forsquamous cell tumours than for small cellcarcinomas and adenocarcinomas {927,1211}. It seems probable, too, thatchanges in cigarette composition, to lowtar, low nicotine, filtered cigarettes, are alsoresponsible, as switching to these “safer”brands results (in addicted smokers) tomore intense smoking (more puffs, deeperinhalation), and hence greater exposure tothese carcinogens in the peripheral lungwhere adenocarcinomas are more com-mon {336,2177}.
Tobacco smoking
There is overwhelming evidence thattobacco smoking is the major cause oflung cancer in most human populations{884}. The smoke inhaled by smokers ofcigarettes and other tobacco productscontains numerous carcinogens, as wellas agents that cause inflammation.An increased risk of lung cancer in smok-ers has been demonstrated in epidemio-logical studies conducted during the1950s in the United States {2176} andUnited Kingdom {504}, and the causalrole of smoking has been recognized bypublic health and regulatory authoritiessince the mid-1960s. The geographicaland temporal patterns of lung cancertoday largely reflect tobacco consump-tion dating from two or three decadesback. Because of the strong carcino-genic potency of tobacco smoke, amajor reduction in tobacco consumptionwould result in the prevention of a largefraction of human cancers, includinglung cancer {2155}.
Relative risk (RR)The risk among smokers relative to therisk among never-smokers is in the orderof 8-15 in men and 3-10 in women. Forthose who smoke without quitting, recentrelative risk estimates are as high as 20to 30. The overall relative risk reflects thecontribution of the different aspects oftobacco smoking: average consumption,duration of smoking, time since quitting,age at start, type of tobacco product andinhalation pattern {192}.
Risk attributed to tobacco smokingThe proportion of lung cancer cases dueto tobacco smoking has been estimated
by comparing incidence (or mortality)rates in different areas, with the rates innon-smokers observed in large cohortstudies {1553,1589}. Based on the world-wide incidence rates estimated for 2000.Worldwide, 85% of lung cancer in menand 47% of lung cancer in women is esti-mated as being the consequence oftobacco smoking.
Dose and durationSeveral large cohort and case-controlstudies have provided detailed informa-tion on the relative contribution of dura-tion and amount of cigarette smoking inexcess lung cancer risk. Duration ofsmoking is the strongest determinant ofrisk, but this also increases in proportionto the number of cigarettes smoked{884}. The strong role of duration ofsmoking explains the observation thatearly age of starting is associated with amorbid lung cancer risk later in life.
Effect of cessation of smokingAn important aspect of tobacco-relatedlung carcinogenesis is the effect of ces-sation of smoking. The excess risksharply decreases in ex-smokers afterapproximately 5 years since quitting; insome studies the risk after 20 or moreyears since cessation approaches that ofnever-smokers. However an excess riskthroughout life likely persists even in
long-term quitters {884}. Thus, smokingcessation is beneficial at all ages.
Type of cigarettes and inhalationSome studies show a lower lung cancerrisk among smokers of low-tar and low-nicotine cigarettes than among othersmokers {192}, but recent evidence sug-gests that low tar cigarettes are not lessharmfull, and may be worse. A similareffect has been observed among long-term smokers of filtered cigarettes, orcompared to smokers of unfiltered ciga-rettes. Smokers of black (air-cured)tobacco cigarettes are at two- to three-fold higher relative risk of lung cancerthan smokers of blond (flue-cured)tobacco cigarettes. Tar content, pres-ence of filter and type of tobacco areinterdependent; high-tar cigarettes tendto be unfiltered and, in regions whereblack and blond tobacco are used, morefrequently made of black tobacco.A 1.5- to 3-fold difference in relative riskof lung cancer has been observed inseveral studies between smokers whodeeply inhale cigarette smoke and smok-ers of comparable amounts who do notinhale or inhale slightly.
Type of tobacco productsAlthough cigarettes are the main tobaccoproduct smoked in western countries, adose-response relationship with lungcancer risk has been shown also forcigars, cigarillos and pipe, with a similarcarcinogenic effect of these products{191}. A stronger carcinogenic effect ofcigarettes than of cigars and pipe insome studies might arise due to differentinhalation patterns or composition ofcigars {902}. An increased risk of lung cancer has alsobeen shown with the bidis widelysmoked in India and water pipes in China{884}. Adequate epidemiological dataare not available on lung cancer risk fol-lowing consumption of other tobaccoproducts, such as narghile in westernAsia and northern Africa, and hooka inIndia.
Lung cancer typeTobacco smoking increases the risk of allmajor histological types of lung cancer,but appears to be strongest for squa-mous cell carcinoma, followed by smallcell carcinoma and adenocarcinomama.The association between adenocarcino-ma and smoking has become stronger
Tumours of the lung - Introduction
Fig. 1.04 The effects of stopping smoking at differ-ent ages on the cumulative risk (%) of death fromlung cancer up to age 75. From R. Peto et al.{1588A}.

15Epidemiology and etiology
over time, and adenocarcinoma hasbecome the most common type in manyWestern countries.
Impact of sex and ethnicityWhilst earlier studies have suggested adifference in risk of lung cancer betweenmen and women who have smoked acomparable amount of tobacco, morerecent evidence does not support thisnotion: the carcinogenic effect of smok-ing on the lung appears to be similar inmen and women.The higher rate of lung cancer amongBlacks in the United States as comparedto other ethnic groups is likely explainedby higher tobacco consumption {486}.Indeed, there is no clear evidence of eth-nic differences in susceptibility to lungcarcinogenesis from tobacco.
Involuntary smoking
The collective epidemiologic evidenceand biologic plausibility lead to the con-clusion of a causal association betweeninvoluntary tobacco smoking and lungcancer risk in non-smokers {884}. Thisevidence has been challenged on thebasis of possible confounding by activesmoking, diet or other factors, and ofpossible reporting bias. However, whenthese factors were taken into account,the association was confirmed {884}.Several large-scale studies and meta-analyses consistently reported an increa -sed risk of lung cancer in the order of20–25% {190,603,754}.Additional evidence of a carcinogeniceffect of involuntary smoking comes fromthe identification in people exposed toinvoluntary smoking of nicotine-derivedcarcinogenic nitrosamines such as NNK,of haemoglobin adducts of 4-amino -byphenyl, a carcinogen in tobaccosmoke and of albumin adducts of poly-cyclic aromatic hydrocarbons {884}. Thecomparison of levels of cotinine, the mainmetabolite of nicotine, suggests thatexposure to involuntary smoking entails
an exposure equivalent of 0.1-1.0 ciga-rettes per day: the extrapolation of therelative risk found in light smokers is con-sistent with the relative risk detected inpeople exposed to involuntary tobaccosmoking.
Occupational exposure
The important role of specific occupa-tional exposures in lung cancer etiologyis well established in reports dating backto the 1950s {192}. The table lists theoccupational agents recognized as lungcarcinogens by the International Agencyfor Research on Cancer (IARC). Themost important occupational lung car-cinogens include asbestos, crystalline
silica, radon, mixtures of polycyclic aro-matic hydrocarbons and heavy metals.Welding and painting were consistentlyassociated with increased risk of lungcancer. However, the exact agent(s) inthese jobs have not yet been identified.Although their contribution to the globalburden of lung cancer is relatively small,occupational carcinogens are responsi-ble for an important proportion oftumours among exposed workers. Formost known occupational carcinogens,some synergism has been shown withtobacco smoking.
Table 1.01Occupational agents and exposure circumstances classified by the IARC Monographs Programme(http://monographs.iarc.fr), as carcinogenic to humans, with the lung as target organ.
Agents, mixture, circumstance Main industry, use
Arsenic and arsenic compounds Glass, metals, pesticides Asbestos Insulation, filters, textiles Beryllium and beryllium compounds Aerospace Bis(chloromethyl)ether and Chloromethyl methyl ether Chemical intermediate Cadmium and cadmium compounds Dye/pigment Chromium[VI] compounds Metal plating, dye/pigment Dioxin (TCDD) Chemical industry Nickel compounds Metallurgy, alloy, catalyst Plutonium-239 Nuclear Radon-222 and its decay products Mining Silica, crystalline Stone cutting, mining, glass, paper Talc containing asbestiform fibers Paper, paintsX- and gamma-radiation Medical, nuclear Coal-tar pitches Construction, electrodes Coal-tars Fuel Soots Pigments
Exposure circumstances Aluminum production Coal gasification Coke production Haematite mining (underground)
with exposure to radon Iron and steel founding Painter (occupational exposure)
creo

16
Signs and symptoms
Patients with lung cancer present withprogressive shortness of breath, cough,chest pain/oppression, hoarseness orloss of voice, haemoptysis (mostly withsquamous cell carcinoma). Pneumonia(often recidivant) is the presenting fea-ture in many patients. Relative to otherforms of non small cell lung cancer, ade-nocarcinoma is more often asympto-matic, being more frequently identified inscreening studies or as an incidentalradiologic finding {5,391}. Patients withsmall cell lung cancer (SCLC) differ inmany ways from those with non-small celllung cancer (NSCLC), in that they oftenpresent with symptoms referable to dis-tant metastases (see below). About 10%of patients with SCLC present with supe-
rior vena cava syndrome. Stridor andhaemoptysis are rare symptoms inpatients with SCLC. Symptoms related todisseminated disease include weightloss, abdominal pain due to involvementof the liver, adrenals and pancreas, andpain due to bone (marrow) metastases.At presentation brain metastases areidentified in 5-10% of patients with SCLCand neurological symptoms occur, butCNS involvement develops during thecourse of the disease in many patientsand multiple lesions are usually found inautopsy in patients with CNS involvement{848,1048,1493}.
Paraneoplastic symptoms
Paraneoplastic symptoms are commonin lung cancer. Endocrine and paraneo-
plastic syndromes are less common inadenocarcinoma than in other histologictypes of lung cancer. SCLC is character-ized by neuroendocrine activity andsome of the peptides secreted by thetumour mimic the activity of pituitary hor-mones. About 10% have abnormal ACTHlike activity. Latent diabetes may becomesymptomatic but a Cushing syndrome israre, probably because of short latency.Some SCLCs (15%) produce antidiuretichormone (ADH) (Inappropriate ADH syn-drome, Schwartz-Bartter syndrome)leading to water retention with oedema.The patients feel clumsy, tired and weak,and the plasma sodium is low. This isassociated with an inferior prognosis{1523,1849}. Cerebrospinal metastasesor meningeal seeding may cause neuro-logical symptoms. Neurological symp-toms may also be a paraneoplastic phe-nomenon, which might include sensory,sensorimotor, and autoimmune neu-ropathies and encephalomyelitis. The
Tumours of the lung - Introduction
Table 1.02Signs and symptoms of lung carcinoma. Approximately 5-20% of cases are clinically occult. Modified, from T.V. Colby et al. {391}
Systemic symptomsWeight loss, loss of appetite, malaise, fever
Local /direct effectsFrom endobronchial growth and/or invasion of adjacent structures
including chest wall and vertebral columnCough, dyspnoea, wheeze, stridor, haemoptysisChest pain/back painObstructive pneumonia (+/- cavitation)Pleural effusion
Extension to mediastinal structuresNerve entrapment : recurrent laryngeal nerve (hoarseness), phrenic
nerve (diaphragmatic paralysis), sympathetic system (Horner syn-drome), brachial plexopathy from “superior sulcus” tumours
Vena cava obstruction: superior vena cava syndromePericardium: effusion, tamponadeMyocardium: arrythmia, heart failureOesophagus: dysphagia, bronchoesophageal fistulaMediastinal lymph nodes: pleural effusion
Metastatic diseaseDirect effects related to the organ(s) involved
Paraneoplastic syndromesDermatomyositis/polymyositisClubbingHypertrophic pulmonary osteoarthropathEncephalopathyPeripheral neuropathiesMyasthenic syndromes (including Lambert-Eaton)Transverse myelitisProgressive multifocal leukoencephalopathy
Endocrine syndromesParathormone-like substance: hypercalcemiaInappropriate antidiuretic hormone: hyponatremiaACTH: Cushing syndrome, hyperpigmentationSerotonin: carcinoid syndromeGonadotropins: gynecomastiaMelanocyte-stimulating hormone: increased pigmentationHypoglycemia, hyperglycemiaHypercalcitonemiaElevated growth hormoneProlactinemiaHypersecretion of vasoactive intestinal polypeptide (VIP): diarrhea
Hematologic/coagulation defectsDisseminated intravascular coagulationRecurrent venous thrombosesNonbacterial thrombotic (marantic) endocarditisAnemiaDysproteinemiaGranulocytosisEosinophiliaHypoalbuminemiaLeukoerythroblastosisMarrow plasmacytosisThrombocytopenia
Miscellaneous (very rare)Henoch-Schönlein purpuraGlomerulonephritis, Nephrotic syndrome Hypouricemia, HyperamylasemiaAmyloidosisLactic acidosisSystemic lupus erythematosus
Clinical features and staging F.R. HirschB. Corrin
T.V. Colby

17Clinical features and staging
symptoms may precede the primarydiagnosis by many months, and might insome cases be the presenting com-plaint. They may also be the initial sign ofrelapse from remission. A specific exam-ple is the Lambert-Eaton myasthenicsyndrome resulting in proximal muscularweakness that improves with continueduse and hypoflexia and dysautonomy.Characteristic electromyographic find-ings confirm the diagnosis. This syn-drome may also occur months before thetumour is disclosed {1497}. The weak-ness will often improve when the tumourrespond on therapy. Hypercalcemia israre in SCLC, and almost pathognomicfor squamous cell carcinoma.
Relevant diagnostic procedures
Fiberoptic bronchoscopy allows macro-scopic examination of the respiratorytree up to most of the subsegmentalbronchi and biopsies associated tobronchial aspiration and brushing.Biopsies of bone, liver, lymph node(mediastinoscopy), skin and adrenalgland may also be used for diagnosis ifthey are metastatically involved. Pulmo-
nary function tests are performed if sur-gery seems possible. Serum tumourmarkers are not routinely recommended.Because of its central location squamouscell carcinoma is readily diagnosed bybronchoscopic biopsy and/or brushand/or sputum cytology {532}. Fluores-cence bronchoscopy may be useful forassessing the extent of associatedintraepithelial neoplasia. For peripherallesions transthoracic CT guided fine nee-dle aspiration biopsy is now generallypreferred.Due to common central location, smallcell carcinoma is often diagnosed viabronchoscopically retrieved histologicand cytologic samples and to a lesserextent sputum cytology.Small peripheral lesions are often sub-jected to fine needle aspiration biopsy,transbronchial biopsy, or sometimeswedge resection for initial diagnosis.
Staging of NSCLC
The internationally accepted TNM stag-ing system is recommended. The stageof the disease is important for prognosisand treatment planning. Pathologic stag-
ing is based on the pathologic evalua-tion of sampled tissues according to theTNM system. For patients in whom surgi-cal resection is attempted, there are sur-gical protocols for sampling the lymphnode stations, including superior medi-astinal nodes (numbered 1-4), aorticnodes (numbered 5 and 6), inferiormediastinal nodes (numbered 7-9) andnodes associated with the lobectomyspecimen labeled “N1” nodes (num-bered 10-14).
Staging of SCLC
The TNM staging classification is gener-ally not utilized in SCLC, as it does notpredict well for survival. SCLC is usuallystaged as either limited or extensive dis-ease. The consensus report of theInternational Association for the Study ofLung Cancer (IASLC) modified the olderVALG classification in accordance withthe revised TNM system:
Limited diseaseDisease restricted to one hemithorax withregional lymph node metastases includ-ing:
HormonesAdrenocorticotropic hormone (ACTH)Melanocyte-stimulating hormone (MSH)Human chorionic gonadotropin (hCG)Human placental lactogen (HPL)Human growth hormone (HGH)Parathyroid hormone (PTH)CalcitoninAntidiuretic hormone (ADH)ProlactinBombesin (gastrin-releasing peptide)5-Hydroxytryptophan (serotonin)OestradiolHypoglycemic factorRenin, ErythropoietinGlucagon, InsulinNeuron-specific enolase (NSE)ß-Endorphin, Gastrin, Secretin
Serum proteinsAlpha fetoprotein (AFP)Carcinoembryonic antigen (CEA)Placental alkaline phosphatase (PAP)HistaminaseL-dopa decarboxylaseAnti-Purkinje cell antibodiesAntineuronal nuclear antibodies (ANNA)Ferritin
Table 1.03Tumour markers found in the serum of patientswith lung carcinoma. From refs {5,13,391}.
Table 1.04Imaging techniques in lung cancer staging.From T.V. Colby et al. {391}.
Conventional Primary detection/characterization of parenchymal tumourradiographs Assessment of main bronchi/tracheal involvement
Detection of chest wall invasionAssessment of hilar and mediastinal invasion/adenopathyDetection of obstructive atelectasis/pneumonitisDetection of pleural effusion
CT Assessment of main bronchi/tracheal involvementDetection of chest wall invasionAssessment of hilar and mediastinal invasion/adenopathyDetection of liver, adrenal, brain metastases
MRI Detection of chest wall invasion (particularly superiorsulcus [tumours])Detection of mediastinal or spinal canal invasionAssessment of hilar and mediastinal adenopathy in patientswith equivocal CT examinations or contraindications tointravenous contrast mediaCharacterization of isolated adrenal masses
Ultrasound Detection of pleural effusion/guidance for thoracentesisGuidance for biopsy of peripheral lung or mediastinal mass
Gallium-67 Detection of hilar and mediastinal adenopathyscan Detection of distal metastases
Pulmonary Evaluation of central pulmonary artery invasionangiography
creo

18
> Hiliar ipsilateral and contralateral > Mediastinal ipsilateral and contralateral> Supraclavicular ipsilateral and con-
tralateral> Ipsilateral pleural effusion (indepen-
dent of cytology)Limited disease is equivalent to stage I-III of the TNM system.
Extensive diseaseAll patients with sites of disease beyondthe definition of limited disease, equiva-lent to stage IV in the TNM system.
Staging Procedures
The staging procedures have the pri-mary goal to distuingish patients who arecandidate for surgery, those with loco-regional disease, and those withmetastatic disease. Standard procedures include chest X-ray, general physical examination, bron-choscopy and blood samples. If findingsat these procedures do not preclude sur-gery or radiotherapy, staging proceeds
with a CT-scan of chest and upperabdomen. Staging stops here if the CTscan shows definitive signs of inoperabledisease such as tumour invasion of themediastinum or distant metastases to theliver or the adrenals. If, however, surgeryseems possible, lymph nodes in themediastinum must be examined formetastatic deposits. If none of the lymphnodes are enlarged (greatest diameter>1.5 cm) and the tumour is proven to beof the squamous cell type, lymph nodebiopsies can be omitted; otherwise apreoperative mediastinoscopy with biop-sies is recommended. In recent yearsthis invasive procedure has beenenhanced by PET scan, although theaccuracy (diagnostic sensitivity andspecificity) of this imaging procedure hasnot yet been fully validated in lung can-cer. If PET is not available, ultrasonogra-phy is still a very helpful procedure andallows fine needle biopsies from suspectlesions in abdominal sites plus otherdeeply located structures such as axil-
lary lymph nodes and the thyroid gland.SCLC is characterized by a rapid dis-semination to extrathoracic organs.Autopsy studies performed 1 month aftersurgical resection showed that 63% (12of 19 patients) with SCLC had distantmetastases compared to 14-40% ofpatients with NSCLC {848}.Staging of SCLC includes bronchoscopy,chest X-ray, chest CT scan, upperabdominal CT scan or ultrasonographyplus a bone marrow examination and/ora bone scintigram. Bone scintigrams arestill used but this procedure will probablybe left with the increasing availability ofPET scanners. Finally, magnetic reso-nance imaging (MRI) scans are useful ifbone metastases or central nervous sys-tem metastases are suspected. Patientswith neurological symptoms should havea cranial CT or MR scan.Staging of SCLC will prove extensivestage disease in about 65% of thepatients due to metastases to one ormore of the following sites: the contralat-eral lung (10%), skin or distant lymphnodes (10%), brain (10%), liver (25%),adrenals (15%), bone marrow (20%),retroperitoneal lymph nodes (5%), orpancreas (5%). Osteolytic bone metas-tases and hypercalcaemia are rarelyseen, but are almost pathognomonic forsquamous cell carcinoma. Enlargedadrenals might represent metastases butcan also be a glandular hypertrophy dueto ectopic ACTH secretion from thetumour, which is observed in about 10%of patients with SCLC {780,847,887,1849}.
Tumours of the lung - Introduction
Table 1.05Chest radiographic findings at presentation according to histologic type of lung carcinoma. From ref {391}.
Radiographic Squamous Cell Adeno- Small Cell Large CellFeature Carcinoma carcinoma Carcinoma Carcinoma
Nodule <or= 4 cm 14% 46% 21% 18%
Peripheral location 29% 65% 26% 61%
Central location 64% 5% 74% 42%
Hilar/perihilar mass 40% 17% 78% 32%
Cavitation 5% 3% 0% 4%
Pleural/chest wall 3% 14% 5% 2%involvement
Hilar adenopathy 38% 19% 61% 32%
Mediastinal adenopathy 5% 9% 14% 10%
Table 1.07Stage and survival in NSCLC*. Modified, from {232}.
Stage Survival (%)3 yr 5 yr
Clinical stagecIA (n = 687) 71 61cIB (n = 1189) 46 38cIIA (n = 29) 38 34cIIB (n = 357) 33 24cIIIA (n = 511) 18 13cIIIB (n = 1,030) 7 5cIV (n = 1,427) 2 1
Pathologic stagepIA (n = 511) 80 67pIB (n = 549) 67 57pIIA (n = 76) 66 55pIIB (n = 375) 46 39pIIIA (n = 399) 32 23
Table 1.06Stage of lung carcinoma at presentation by histologic subtype. SEER data 1983-1987. Modified, from reference {192}.
Stage Squamous Adenocarcinoma Small cell Large cell
Localized 21.5% 22.2% 8.2% 15.2%
Regional 38.5% 33.1% 26.1% 31.5%
Distant 25.2% 35.9% 52.8% 40.3%
Unstaged 14.8% 8.8% 12.8% 12.9%
creo

19Concept of neuroendocrine tumours
Tissue collection and interpretation
Optimal tissue collection is important fora precise classification of lung tumours.Several diagnostic approaches are avail-able, including sputum cytology, bron-choalveolar lavage, bronchoscopic biop-sy, brushing and washing, thoracoscopicbiopsy, resected surgical material andneedle biopsies as well as pleural cytol-ogy.Rapid fixation and minimal trauma areimportant. Small specimens may notshow differentiation when the tumour isexcised; it is, therefore, advisable to limitcategorization to SCLC and NSCLC. Thecurrent classification is largely based onstandard H&E sections. Some lung carci-nomas remain unclassified. They usuallyfall into the “non-small cell carcinoma”category or are cases where small biop-sy or cytology specimens precludedefinitive histologic typing.
Histologic heterogeneity
Lung cancers frequently show histologicheterogeneity, with variation in appear-ance and differentiation from microscop-ic field to field and from one histologicsection to the next {1676}. Almost 50% oflung carcinomas exhibit more than one ofthe major histologic types. This fact hasimportant implications for lung tumourclassification and must be kept in mind,especially when interpreting small biop-sies.The designation of a minimum require-ment such as 10% for the adenocarcino-ma and squamous cell carcinoma com-ponents of adenosquamous carcinomaor the spindle and/or giant cell carcino-ma component of pleomorphic carcino-mas set in the 1999 WHO classificationare maintained in this classification, rec-ognizing that they are an arbitrary criteri-on since the extent of histologic sampling
will influence classification of suchtumours {584,2024}. Although thesetumours may be suspected on smallspecimens such as bronchoscopic orneedle biopsies, a definitive diagnosisrequires a resected specimen. If thisproblem arises in a resected tumour,additional histologic sections may behelpful. Nevertheless, defining a specificpercentage for a histologic componentcan be a useful criterion for entities suchas adenosquamous carcinoma and pleo-morphic carcinoma.
The concept of pulmonary
neuroendocrine tumours
W.D. Travis
Tumours with neuroendocrine mor-
phology
Neuroendocrine tumours of the lung area distinct subset of tumours, which sharemorphologic, ultrastructural, immunohis-tochemical and molecular characteris-tics and although these tumours areclassified into different morphologic cat-egories within the WHO classification,certain concepts relating specifically toneuroendocrine tumours merit discus-sion. The major categories of morpho-logically identifiable neuroendocrinetumours are small cell carcinoma(SCLC), large cell neuroendocrine carci-noma (LCNEC), typical carcinoid (TC),and atypical carcinoid (AC). Historicalterms such as well-differentiated neu-roendocrine carcinoma, neuroendocrinecarcinoma (grade 1-3), intermediate cellneuroendocrine carcinoma, malignantcarcinoid and peripheral small cell car-cinoma resembling carcinoid, should beavoided {1999}.
With regard to nomenclature, the termstypical and atypical carcinoid are pre-ferred for a number of reasons.Clinicians are familiar with these diag-nostic terms and the tumours share a
distinctive basic microscopic appear-ance, resembling carcinoids found atother body sites. Spindle cell, oncocyticand melanocytic patterns and stromalossification occur in both typical andatypical carcinoids. Patients with typicaland atypical carcinoids are also signifi-cantly younger than those with SCLCand LCNEC. Within the high-grade neu-roendocrine tumours, LCNEC and SCLCare morphologically distinct and it hasnot been proven that chemotherapyused for SCLC is effective for patientswith LCNEC.
With regard to distinguishing the fourmain types of neuroendocrine tumours,all show varying degrees of neuroen-docrine morphologic features by lightmicroscopy including organoid nesting,palisading, a trabecular pattern, androsette-like structures, with the cardinaldistinguishing features being mitoticactivity and the presence or absence ofnecrosis. For mitotic activity, Arrigoni, etal. {75} originally proposed that atypicalcarcinoids had between 5-10 mitosesper 10 high power fields. However, themitotic range for atypical carcinoid wasrecently modified to 2-10 mitoses per
2 mm2 (10 high power fields – see belowfor mitosis counting method) {2028}. Thepresence of necrosis also distinguishesatypical from typical carcinoid. Cytologicatypia is unreliable as a diagnostic fea-ture.
A mitotic count of 11 or more mitoses per2 mm2 (10 high power fields) is the maincriterion for separating LCNEC andSCLC from atypical carcinoid {2028}.LCNEC and SCLC usually have veryhigh mitotic rates, with an average of 70-80 per 2 mm2 (10 high power fields insome microscope models). LCNEC andSCLC also generally have more exten-sive necrosis than atypical carcinoid.LCNEC are separated from SCLC usinga constellation of criteria, which includelarger cell size, abundant cytoplasm,prominent nucleoli, vesicular or coarsechromatin, polygonal rather thanfusiform shape, less prominent nuclearmolding and less conspicuous deposi-tion of hematoxylin-stained material(DNA) in blood vessel walls. LCNECcells more closely resemble those of alarge cell carcinoma than a carcinoidtumour. Mitoses should be counted inthe areas of highest mitotic activity andthe fields counted should be filled withas many viable tumour cells as possible.Since the area viewed in a high powerfield varies considerably depending onthe microscope model, we define themitotic range based on the area of viable

20
tumour examined. These criteria wereestablished on a microscope with a 40Xobjective, an eyepiece field of view num-ber of 20 and with no magnificationchanging devices. With this approachthe area viewed in one high power field is0.2 mm2 and 10 high power fields = 2mm2. If microscopes with other objectiveand eyepiece field of view numbers areused, the area in a high power fieldshould be measured to allow calibrationto cover a 2 mm2 area.There is substantial reproducibility(kappa statistic of .70) for this subclassi-fication scheme. The greatest repro-ducibility is seen with SCLC and typicalcarcinoid. The most common disagree-ments involve LCNEC vs SCLC, followedby typical carcinoid vs atypical carci-noid, and atypical carcinoid vs LCNEC.Additional research on atypical carcinoidand LCNEC is needed to better definetheir clinical characteristics and optimaltherapy.Interestingly, despite separation into fourmain groups, there is increasing evi-dence that TC and AC are more closelyassociated to each other than to LCNECand SCLC. Clinically, approximately 20-40% of patients with both typical andatypical carcinoids are non-smokers
while virtually all patients with SCLC andLCNEC are cigarette smokers. In con-trast to SCLC and LCNEC, both typicaland atypical carcinoids can occur inpatients with Multiple EndocrineNeoplasia (MEN) type I {464}. In addi-tion, neuroendocrine cell hyperplasiawith or without tumourlets is relatively fre-quent in both typical and atypical carci-noids but not in LCNEC or SCLC.Histologic heterogeneity with other majorhistologic types of lung carcinoma(squamous cell carcinoma, adenocarci-noma, etc.) occurs with both SCLC andLCNEC but not with typical or atypicalcarcinoids {2024}. In contrast to largecell neuroendocrine carcinoma, mosttypical and atypical carcinoids are readi-ly diagnosed by light microscopy withoutthe need for immunohistochemistry orelectron microscopy. There are alsogenetic data indicating that SCLC iscloser to LCNEC than to the TC and AC,in that abnormalities in many geneticmarkers such as p53 {1516,1622},bcl2/bax {217}, cyclin D1 {746}, RB lossand LOH at 3p {726} are seen in a highpercentage of both SCLC and LCNECwith minimal and intermediate percent-ages of TC and AC showing abnormali-ties, respectively (see below).
Non-small cell carcinomas with neu-
roendocrine differentiation
Some lung carcinomas, which do notshow neuroendocrine morphology bylight microscopy, demonstrate immuno-histochemical and/or ultrastructural evi-dence of neuroendocrine differentiation.Neuroendocrine differentiation can beshown by immunohistochemistry in 10-20% of squamous cell carcinomas, ade-nocarcinomas, and large cell carcino-mas. It is seen most often in adenocarci-nomas. These tumours are collectivelyreferred to as NSCLC with neuroen-docrine differentiation (NSCLC-ND).While this issue has drawn much interest,there is controversy over whether thesetumours have worse or better survivaland whether they are more or lessresponsive to chemotherapy thanNSCLC lacking neuroendocrine differen-tiation. Therefore these tumours requirefurther study before they are included asa separate category in a histologic clas-sification. They should be classifiedaccording to the conventional typingherein, with neuroendocrine differentia-tion noted {2024}.
Tumours of the lung - Introduction
Table 1.09The spectrum of neuroendocrine (NE) prolifera-tions and neoplasms. From W.D. Travis et al. {2024}
Neuroendocrine cell hyperplasiaand tumourlets
NE cell hyperplasiaNE cell hyperplasia with fibrosis
and/or inflammationNE cell hyperplasia adjacent to
carcinoid tumoursDiffuse idiopathic NE cell hyperplasia
with or without airway fibrosis Tumourlets
Tumours with NE morphology Typical carcinoidAtypical carcinoid Large cell neuroendocrine carcinomaSmall cell carcinoma
Non-small cell carcinomas with NE differentiation
Other tumours with NE propertiesPulmonary blastomaPrimitive neuroectodermal tumourDesmoplastic round cell tumourCarcinomas with rhabdoid phenotypeParaganglioma
Table 1.08Criteria for diagnosis of neuroendocrine tumours.From W.D. Travis et al. {2024}
Typical carcinoidA tumour with carcinoid morphology and less than 2 mitoses per 2 mm2 (10 HPF), lacking necrosis and0.5 cm or larger
Atypical carcinoidA tumour with carcinoid morphology with 2-10 mitoses per 2 mm2 (10 HPF) OR necrosis (often punctate)
Large cell neuroendocrine carcinoma1. A tumour with a neuroendocrine morphology (organoid nesting, palisading, rosettes, trabeculae) 2. High mitotic rate: 11 or greater per 2 mm2 (10 HPF), median of 70 per 2 mm2 (10 HPF) 3. Necrosis (often large zones) 4. Cytologic features of a non-small cell carcinoma (NSCLC): large cell size, low nuclear to
cytoplasmic ratio, vesicular, coarse or fine chromatin, and/or frequent nucleoli. Some tumours have fine nuclear chromatin and lack nucleoli, but qualify as NSCLC because of large cell size and abundant cytoplasm.
5. Positive immunohistochemical staining for one or more NE markers (other than neuron specific enolase) and/or NE granules by electron microscopy.
Small cell carcinomaSmall size (generally less than the diameter of 3 small resting lymphocytes)1. Scant cytoplasm2. Nuclei: finely granular nuclear chromatin, absent or faint nucleoli3. High mitotic rate (11 or greater per 2 mm2 (10 HPF), median of 80 per 2 mm2 (10 HPF)4. Frequent necrosis often in large zones

21Genetic and molecular alterations
Molecular and pathological diversity
of lung cancers
Lung cancers result from complex,genetic and epigenetic changes charac-terized by stepwise malignant progres-sion of cancer cells in association withaccumulation of genetic alterations. Thisprocess, referrred to as multistep car-cinogenesis, develops through the clonalevolution of initiated lung cells. Initiationconsists in the acquisition of definedgenetic alterations in a small number ofgenes that confer a proliferative advan-tage that facilitates progression towardsinvasive carcinoma. Many environmentalcarcinogens present in tobacco smokeor in industrial pollutants can act as ini-tiators for bronchial or bronchiolar-alveo-lar epithelial cells {807,2145}. These car-cinogens often have a global effect onthe entire bronchial tree, resulting in thefrequent occurrence of several primarylesions within the same, exposed organ.This observation has led to the conceptof field carcinogenesis.Over the past 25 years, evidence hasaccumulated for stepwise accumulationof genetic changes in all major histologi-cal types of lung cancers. Thesechanges include allelelic losses (LOH),chromosomal instability and imbalance,mutations in oncogenes and tumor sup-pressor genes, epigenetic gene silenc-ing through promoter hypermethylationand aberrant of expression of genesinvolved in the control of cell proliferation{564,687,1235,1323,2209}. Althoughmany of these genetic changes occurindependently of histological type, theirfrequency and timing of occurrence withrespect to cancer progression is differentin small cell lung carcinomas (SCLC),that may originate from epithelial cellswith neuro-endocrine features, and non-small cell lung carcinomas (NSCLC), thatoriginate from bronchial or alveolarepithelial cells. Furthermore, a number ofgenetic and epigenetic differences havebeen identified between squamous cellcarcinoma (SCC), that arises frombronchial epithelial cells through a squa-mous metaplasia/dysplasia process),
and adenocarcinoma (ADC), that derivesfrom alveolar or bronchiolar epithelialcells {2017,2209}.
Genetic changes frequent in all major
histological types
Invasive lung carcinoma display multiplegenetic alterations, such as LOH at manydifferent loci including 3p14-23 {220,1210,1446}, 8q21-23 {2159}, 9p21{670,1299}, 13q, 17q, 18q and 22p {687,1268,1996,2209}. However, three fre-quent aberrations emerge as commonchanges in all histological types of lungcancers.
TP53 mutationsThe most frequent one is mutation in thetumor suppressor gene TP53, encodingthe p53 protein that plays multiple, anti-proliferative roles, in particular inresponse to genotoxic stress {881,1947}.Inactivating TP53 mutations (mostly mis-sense mutations) are detected in up 50%of NSCLC and in over 70% of SCLC{1591}. In both SCC and ADC, there isevidence that mutation can occur veryearly in cancer progression and that theirprevalence increases from primary, insitu lesions to advanced, metastatic car-cinomas.
Retinoblastoma pathwayThe second most common alteration isinactivation of the pathway controllingRB1 (retinoblastoma gene, 13q11), asuppressor gene encoding the Rb pro-tein that acts as a “gatekeeper” for theG1 to S transition of cell cycle {215,2209}. The most common mechanismsfor inactivation of this pathway are loss ofRB1 expression, silencing of INK4 (alsotermed CDKN2a, encoding p16) throughLOH (9p21) and promoter hypermethyla-tion, and overexpression of CCND1(encoding cyclin D1), sometimes con-secutive to gene amplification (11q13){189,215}. These three genes act in asequential manner within the signallingcascade that controls Rb inactivation byphosphorylation. There is a constantinverse correlation between loss of Rb
protein, inactivation of p16 and overex-pression of cyclin D1, consistent with thenotion that these events have essentiallysimilar functional consequences {215}.Interestingly, the mechanism by whichthis pathway is altered differs betweenNSCLC and SCLC. Loss of Rb proteinexpression is detectable in over 80-100% of high grade neurorendocrinetumors, most of them retaining normalp16 and cyclin D1 expression {189,670}.In contrast, loss of Rb protein is lesscommon in NSCLC (15%) but inactiva-tion of INK4 is present in up to 70% of thecases, whereas amplification of CCDN1is detectable in a significant proportion ofSCC (10%) {215,2209}. It should also benoted that the INK4 gene locus containsa reading frame encoding another pro-tein, p14arf, which is different from p16but also plays roles in growth suppres-sion. Initial studies suggested that theexpression of p14arf is often lost inSCLC, suggesting that alterations of theINK4 locus may have functional conse-quences other than deregulation of thecascade controlling RB1 {669}. Recentreports indicate that p14arf methylationdoes not play a role of in the develop-ment of SCLC and NSCLC {1550,1746}.
LOH 3pThe third common genetic event thatoccurs in all lung cancers irrespective oftheir histological type is LOH on chromo-some 3p, detectable in up to 80% ofNSCLC as well as SCLC {220,1210,1446}. This region encompasses severalpotential tumor suppressor genes,including FHIT, RASSF1 and SEMA3B{1167,1183,2209}. The FHIT gene(Fragile Histidine Triad) is located in ahighly fragile chromosomal site where it isparticularly prone to partial deletion as aresult of direct DNA damage by carcino-gens present in tobacco smoke {895}.FHIT encodes a protein with ADP hydro-sylase activity that has been proposed tohave various intracellular functions,including regulation of DNA replicationand signalling stress responses {112}.RASSF1 encodes a protein involved inthe control of the activity of members ofthe RAS family of oncogenes. SEMA3Bencodes semaphorin 3B, a member of afamily of genes encoding secreted pro-teins with critical roles in development ofneuronal and epithelial tissues. The con-tributions of these genes to the develop-ment of lung cancers is still poorly under-
Genetic and molecular
alterations
A. GazdarW.A. FranklinE. Brambilla
P. HainautJ. Yokota
C.C. Harris

22 Tumours of the lung - Introduction
stood. Their expression is frequently lostin tumors, despite the presence of resid-ual, apparently intact alleles. This obser-vation has led to the hypothesis that sev-eral genes in chromosome 3p are com-mon targets for epigenetic abnormalitiesthrough mechanisms that are not yet fullyelucidated {560}.
Genetic changes in histological types
of lung cancer
Among the less common changesobserved in lung cancers, some appearto be more frequent in specific histologi-cal types. For example, mutations atcodon 12 in KRAS are found in 30 to 40%of ADC but are extremely rare in otherforms of NSCLC or in SCLC {402,1669}.KRAS mutation is detected in a signifi-cant proportion of atypical alveolarhyperplasias, indicating that this lesion isa potential pre-invasive lesion for ADC{2126}. In contrast, mutational activationof the beta-catenin gene is rare {1502}but has been identified in different histo-logical types of lung cancer {1801,1904}.Mutations of the APC gene, another com-ponent of the Wnt pathway, have beenidentified in up to 5% of squamous celland small cell lung cancer {1502}.Amplifications of MYC (8q21-23) arefound only in a minority of advancedNSCLC (less than 10%) but are commonin pre-invasive stages SCLC (30%).Similarly, LOH on chromosome 5q are
frequent at early stages of SCLC but areinfrequent in non-metastatic NSCLC{2209}. The target gene on chromosome5q is still not identified.The gradual increase of molecularabnormalities along the spectrum of neu-roendocrine lung tumours strongly sup-ports the grading concept of typical car-cinoid as low grade, atypical carcinoidas intermediate grade and large cellneuroendocrine carcinoma and smallcell lung carcinoma as high-grade neu-roendocrine lung tumours. MEN1 genemutation and LOH at the MEN1 genelocus 11q13 was recently demonstratedin 65% of sporadic atypical carcinoids{463} and was not found in high gradeneuroendocrine tumours {464}.Although epigenetic silencing of genes,mainly through promoter hypermethyla-tion, is widespread in all forms of lungcancers, the methylation profile of tumorsvaries with histological type. SCLC, car-cinoids, SCC and ADC have unique pro-files of aberrantly methylated genes. Inparticular, the methylation rates of APC,CDH13 and RARb are significantly high-er in ADC than in SCC {2017}.Several striking differences also exist atthe level of gene expression. The p63protein, encoded by TP63, a member ofthe TP53 gene family located on chromo-some 3q, is highly expressed and some-times amplified in SCC but not in otherhistological types {826}. This protein
plays a role in squamous differentiationand its presence may be required for thedevelopment of SCC. As there is nosquamous epithelium in the normal lung,deregulation of p63 expression may be afundamental event in the pathogenesis ofthe metaplasia that precedes SCC.
DNA adducts and mutagen finger-
prints
About 90% of lung cancers in Westerncountries, and a rapidly growing numberof cancers in non-western countries, arecaused by smoking. Tobacco smoke is amixture of over 4800 chemicals, includ-ing over 60 that were classified as car-cinogens by the International Agency forResearch on Cancer. They belong to var-ious classes of chemicals, includingpolycyclic aromatic hydrocarbons (PAH),aza-arenes, N-nitrosamines, aromaticamines, heterocyclic aromatic amines,aldehydes, volatile hydrocarbons, nitrocompounds, miscellaneous organiccompounds, and metals and other inor-ganic compounds {807,1591}. Althoughthe dose of each carcinogen per ciga-rette is quite small, the cumulative dosein a lifetime of smoking can be consider-able. In target cells, most of these car-cinogens are converted to intermediatescompounds by Cytochrome P450enzymes, which catalyze the addition ofan oxygen to the carcinogen, increasingits water solubility. The resulting metabo-lites are readily converted to excretablesoluble forms by glutathione S-trans-ferase, providing an efficient detoxifica-tion mechanism. However, during thisprocess, electrophilic (electron-deficient)intermediates are formed, that are highlyreactive with DNA, resulting in the forma-tion of DNA adducts {2145}. Cells are equipped with elaborate sys-tems to eliminate DNA adducts from thegenome, including the nucleotide exci-sion repair pathway (NER, that preferen-tially eliminates so-called bulky DNAadducts consisting of large chemicalgroups covalently attached to DNA), thebase excision repair systems (BER), thatremoves DNA bases altered by attach-ment of small chemical groups or frag-mented by ionizing radiation or oxidation,as well as a specialized, direct repairsystem that acts through the enzyme O6-methylguanine DNA methyltransferase(O6MGMT), which repairs the miscodingmethylated base O6-methylguanine.Many of these enzymes are polymorphic
Fig. 1.05 Genetic models for the development non-small cell lung carcinomas (NSCLC) and of small cell lungcarcinoma (SCLC). From J. Yokota and T. Kohno {2209}.

23Genetic and molecular alterations
in the human population. Thus, the bal-ance between metabolic activation,detoxification and repair varies amongindividuals and is likely to affect cancerrisk {1570,1970}. Carcinogens can damage DNA in specif-ic ways depending upon their chemicalnature {881}. TP53 mutations are morefrequent in lung cancers of smokers thanin non-smokers {1591,2058}. Studies ofdata compiled in the IARC TP53 mutationdatabase (see www.iarc.fr) have shownthat the pattern of TP53 mutations in lungcancers of smokers is unique, with anexcess of transversions at G bases (G toT, 30%) that are uncommon in non-tobac-co-related cancers (9%). In lung cancersof non-smokers, the overall prevalence ofG to T transversions is 13%. In subjectswith the highest reported exposure totobacco, G to T transversions representalmost 50% of all mutations. These trans-versions preferentially occur at a limitednumber of codons (157, 158, 245, 248,273) that have been experimentally iden-tified as sites of adduction for metabo-lites of benzo(a)pyrene, one of the majorPAH in tobacco smoke {477,1591}.Mutations at these codons can be foundin histologically normal lung tissues adja-cent to cancers in smokers, as well as inlung tissues of smokers without lung can-cers {880}. This observation providesdirect evidence that some tobacco com-pounds can act as carcinogens in lungcells. Comparisons between histologicaltypes reveal an excess of G to T trans-versions for all histological types insmokers, implying a general, causaleffect of tobacco carcinogens {1591}.However, there are considerable differ-ences in TP53 mutation patterns accord-ing to histological type and, significantly,gender. Interestingly, the vast majority oflung cancers with TP53 mutations in non-smokers are adenocarcinomas occurringin women {1588,2020}. Thus, the differ-ence in G to T transversions betweensmokers and non-smokers is mainly dueto female non-smokers having a low fre-quency of these transversions comparedto female smokers. Several other genes also show differentrates of alterations in smokers and non-smokers. These genes include muta-tions in KRAS, that are more frequent insmokers (30%) than in non-smokers(5%), as well as hypermethylation ofINK4 and FHIT genes {1236, 2017,2058,2162}.
Impact of genetic studies on lung
cancer therapy
Despite accumulating knowledge on thespecificity of the genetic pathways lead-ing to different histological types of lungcancers, there is still little understandingof how these events cooperate with eachother in cancer progression. One of themain challenges remains the identifica-tion of events that are predictive of therate of progression towards metastaticcancer. However, the identification of alimited number of genes that are oftenaltered at early stages of lung cancers(such as methylation of INK4 or of geneson 3p, mutations in TP53 and in KRAS)represent an interesting opportunity fordeveloping approaches for early detec-
tion, for example using material frombronchial lavages and expectorations{1322}. In the future, many of these alter-ations may provide interesting targets fordesigning new, alternative therapeuticstrategies.
Fig. 1.06 Mutational hotspots for G to T transversions in lung cancers of smokers: concordance with posi-tions of DNA adducts in the TP53 gene in primary bronchial cells exposed to benzo(a)pyrene in vitro. Codonnumbers are indicated. Adapted from G.P. Pfeifer et al. {1591}.
Fig. 1.07 Pattern of TP53 mutations in lung carcinomas. Note the high frequency of G:C>T:A mutations intumours of smokers, probably due to benzo(a)pyrene or related tobacco carcinogens. Adapted from G.P.Pfeifer et al {1591}.

The risk of lung cancer in subjects with afamily history of this tumour is about 2.5{1781}. Given the strong link betweenexposure to carcinogens (mostly tobac-co smoke) and lung cancer, the study ofgenetic polymorphisms as possible riskmodifiers has focused on enzymesinvolved in Phase I/II-xenobiotic metabo-lism, DNA-repair and the effects on nico-tine addiction.
Phase I
CYP1A1 bioactivates polycyclic aromatichydrocarbons (PAH). Several variant alle-les are known (http://www.imm.ki.se/CYPalleles/cyp1a1.htm). Two closelylinked polymorphisms, MspI at 6235 ntand I462V, have been extensively stud-ied in relation to lung cancer, yieldinginconsistent results. In a pooled analysisan OR of 2.36 (95% confidence interval(CI) 1.16 - 4.81) for the MspI homozy-gous variant genotype in Caucasianswas found {2086}. The OR was not sig-nificant for this variant in a meta-analysisincluding both Caucasians and Asians{870}. The frequencies of CYP1A1 allelicvariants are substantially lower inCaucasians than in Asians and the func-tional significance has not been convinc-ingly shown. PAH-exposed individualswith variant CYP1A1 alleles had higherlevels of PAH-DNA adducts in WBC andlung tissue {37}, particularly in conjunc-tion with GSTM1 null.CYP1B1 present in lung, bioactivatesmany exogenous procarcinogens includ-ing PAH and also estrogens. There ispolymorphic inducibility in lymphocytes{2004}. Five SNPs result in amino acidsubstitutions, of which 2 are located inthe heme binding domain {1998}. Ser119has been shown to be associated withSCC in Japanese {2111}. Ethnic variationin allelic frequency has been demon-strated.CYP2D6 metabolizes clinically importantdrugs and also the tobacco specificnitrosamine, NNK (poor substrate).Among at least 40 SNPs and differentallelic variants, many lead to alteredCYP2D6 activity. The much-studied
association between lung cancer andpolymorphic expression of CYP2D6 hasremained inconsistent: A meta-analysisreported a small decrease in lung cancerrisk for the poor metaboliser phenotype,which the genotype analysis could notconfirm {1696}.CYP2A13, a highly polymorphic gene, isexpressed in the human lung and effi-ciently bioactivates NNK. Among severalvariant alleles, only one SNP is located inthe coding region, leading to an A257Camino acid change; the 257C variantwas less active than the wild-type pro-tein. Inter-ethnic differences in allelicvariant frequencies have been found{2239A}. CYP2A6 is also important forthe bioactivation of NNK. There are sev-eral polymorphisms for this gene, withsome positive studies in Japanese {73}and Chinese {1968}, but overall the dataare conflicting {1208,1642}.The microsomal epoxide hydrolase(MEH3) may affect lung cancer riskbased on pooled analysis of 8 studies(His/His OR = 0.70, CI = 0.51-0.96),which was not observed in a meta-analy-sis of the same studies {1154}. There aresome positive studies for MEH4 {1303,2175,2240}.
Phase II
Glutathione-S-transferases (GST) detoxi-fy tobacco carcinogens such as PAH byconjugation. Individuals lacking GSTM1(null polymorphism e.g. in 50% ofCaucasians) appear to have a slightlyelevated risk of lung cancer: A meta-analysis of 43 studies found an OR of1.17 (CI 1.07 - 1.27) for the null geno-type. When the original data from 21case-control studies (9500 subjects)were analysed no evidence of increasedlung cancer risk among null carriers, noran interaction between GSTM1 genotypeand smoking was found {144}. A base-substitution polymorphism in GSTM1seems to affect squamous cell cancerrisk in non-smokers {1228}. GSTM1genotype affects internal carcinogendose levels: DNA adduct levels werehigher in lung tissue and white blood
cells from GSTM1 null individualsexposed to PAH {37}. Because adductlevels are affected by a range of geneticpolymorphisms {697} results from allGSTM1 studies were not consistent.Among two GST-Pi polymorphisms stud-ied, one in exon 6 has been associatedwith lung cancer risk {1891,2106},although other studies did not {944,1447}. Studies of environmental tobaccosmoke further support a role of this poly-morphism in lung cancer {1312}. Studieson a deletion polymorphism in GST-T1are mostly negative {944,1447,1891} orcontradictory for the “at-risk” allele {869}.A role for younger persons with lung can-cer has been suggested {1943}.N-Acetyltransferases (NAT) 1 and 2 withdistinct but overlapping substrate speci-ficities activate and/or detoxify aromaticamines. From 11 studies on lung cancerORs, fast acetylation vs. slow NAT2ranged from 0.5 – 3.0; most studiesfound no significant association, but insome, fast NAT2 acetylators were atincreased risk {2243}. The NAT1*10allele, (a putative fast allele) has incon-sistently been associated with anincreased risk for lung cancer.Myeloperoxidase (MPO): 11 Lung cancercase-control studies have reported ORsfrom 0.54 - 1.39 for the G/A genotype,0.20 - 1.34 for the A/A genotype and 0.58- 1.27 for the (G/A + A/A) genotypes. Alarge study did not find the A-allele to beprotective for lung cancer, while a meta-analysis (excluding this study) showedmarginally significant inverse correla-tions of the A/A and/or G/A genotypeprevalence and lung cancer risk {576}.Carriers of the A-allele had a significant-ly reduced capacity to bioactivate B(a)Pinto its epoxide in coal tar treated skin{1678}.
DNA repair genes
DNA repair genes are increasingly stud-ied, for example PADPRP (193bp dele-tion), XPD (Codons 751, 312), AGT(Codons 143, 160), XRCC3 (Codon 241),and XRCC1 (codons 194, 280 or 399).As most study sizes were small, only a
24 Tumours of the lung - Introduction
Genetic susceptibility H. BartschA. Haugen
A. RischP. Shields
P. Vineis

few were statistically significant, includ-ing an OR of 1.86 (CI 1.02 - 3.4) for XPDcodon 312 (genotype AA) {260}, an ORof 1.8 (1.0 - 3.4) for XRCC1 codon 280(AA+AG) {1641}, and an OR of 2.5 (1.1 -5.8) for XRCC1 Codon 399 (AA) {500A}.In the latter study there was inconsisten-cy among ethnic groups (CaucasiansOR 3.3, 1.2 - 10.7; Hispanics OR 1.4, 0.3- 5.9). In one study {744} a strong effectof PADPRP (193bp deletion) wasobserved only in African-Americans (OR30.3, 1.7 - 547) and in Hispanics (OR 2.3,1.22 - 4.4), but not in Caucasians (OR0.5, 0.1 - 1.9); the biological plausibility ishard to assess {160, 161}.hOGG1, which repairs oxidative DNAdamage (8-oxo-dG) {1045} has beenstudied. Functional effects of the variantsand a few positive lung cancer associa-tions have been reported {914,1145,1899}.In the p53 gene there is a genetic poly-morphism in codon 72, and several hap-lotypes are known. A functional effect bythese variants has not been described,but an association with lung cancer riskwas found {169,554,978,1193}. The riskwas more elevated in persons, whencombined with GSTM1 null {1193,2003}and GST Pi {1313} variants. Also, aninteraction with CYP1A1 has been report-ed {978}.Phenotypic DNA repair studies foundconsistently an increased risk of lung
cancer associated with putative impairedrepair functions {160,161}.
Smoking behaviour and addiction
Evidence for a genetic component fornicotine addiction (an obvious risk factorfor lung cancer) comes from twin studies{291,805,806}. Most polymorphism stud-ies have focused on dopamine neuronalpathways in the brain, including genescoding for dopamine receptors,dopamine transporter reuptake (SL6A3)and dopamine synthesis. Many of thesepolymorphic genes result in altered pro-tein function, but the data for any specif-ic candidate polymorphism are not con-sistent {396,1163-1166,1482,1715,1800,1864}.
Combinations
The risk modifying effect of any one SNPmay be more pronounced when it occursin combination with other ‘at risk’ geno-types of biotransformation and repairenzymes implicated in pathways of agiven carcinogen. The combined geno-types for CYPs and GSTs have shown anenhanced effect on lung cancer risk andan impact on intermediate end-points (e.g.DNA adduct level and mutations){117,260}. Gene-gene interactions for acombination of GST polymorphisms{944,1006,1024,1891} are known andprospective studies confirmed theincreased risk {1570}. An interaction for
p53 and GST genotypes {978,1193,2003}, might be more important in youngerpersons {1313}.
Conclusions
Studies on genetic polymorphisms andlung cancer risk have identified a num-ber of candidate genes involved in xeno-biotic metabolism, DNA repair and possi-bly nicotine addiction. Certain variants ofthese genes and combinations thereofwere shown to modify the risk of tobaccorelated lung cancer. Their influence var-ied by ethnicity, by histological lungtumour types, by exposure and by otherhost-/life-style factors. Due to this com-plexity, to date lung cancer risk cannotbe predicted at an individual level.
25Genetic susceptibility

26 Tumours of the lung - Malignant epithelial tumours
Definition
Squamous cell carcinoma (SCC) is amalignant epithelial tumour showing ker-atinization and/or intercellular bridgesthat arises from bronchial epithelium.
ICD-O code
Squamous cell carcinoma 8070/3Papillary carcinoma 8052/3Clear cell carcinoma 8084/3Small cell carcinoma 8073/3Basaloid carcinoma 8083/3
Synonym
Epidermoid carcinoma
Epidemiology - Etiology
Over 90% of squamous cell lung carci-nomas occur in cigarette smokers{1860}. Arsenic is also strongly associat-ed with squamous cell carcinoma andother causes are summarized in Table 1.
Sites of involvement
The majority of squamous cell lung carci-nomas arise centrally in the mainstem,lobar or segmental bronchi {2007}.
Imaging
Radiography. In central SCC, lobar orentire lung collapse may occur, with shiftof the mediastinum to the ipsilateral side{263,264,614,1676}. Central, segmentalor subsegmental tumours can extendinto regional lymph nodes and appear ashilar, perihilar or mediastinal masses with
or without lobar collapse {264}.Peripheral tumours present as solitarypulmonary nodules (< 3 cm) or masses(> 3 cm). Squamous cell carcinoma isthe most frequent cell type to cavitategiving rise to thick walled, irregular cavi-ties with areas of central lucency on thechest film. When located in the superiorsulcus of the lung, they are calledPancoast tumours and are frequentlyassociated with destruction of posteriorribs and can cause Horner’s syndrome.The chest radiograph may be normal insmall tracheal or endobronchial tumours{1820}. Hilar opacities, atelectasis orperipheral masses may be associatedwith pleural effusions, mediastinalenlargement or hemidiaphragmatic ele-vation. CT and spiral CT. The primary tumourand its central extent of disease is usual-ly best demonstrated by CT scan {614}.Spiral CT may assess better the thoracicextension of the lesion, reveal small pri-mary or secondary nodules invisible onchest radiograph, and exhibit lymphaticspread. PET scan. This is now the method ofchoice to identify metastases (excludingbrain metastases which may requireMRI) {195,614,2061}. Bone metastasesare typically osteolytic.
Cytology
The cytologic manifestations of squa-mous cell carcinoma depend on the
degree of histologic differentiation andthe type of sampling {673,936}. In abackground of necrosis and cellulardebris, large tumour cells display cen-tral, irregular hyperchromatic nucleiexhibiting one or more small nucleoli withan abundant cytoplasm. Tumour cells areusually isolated and may show bizarreshapes such as spindle-shaped and tad-pole-shaped cells. They may appear incohesive aggregates, usually in flatsheets with elongated or spindle nuclei.In well-differentiated squamous cell car-cinoma keratinized cytoplasm appearsrobin’s egg blue with the Romanowskystains, whereas with the Papanicolaoustain, it is orange or yellow. In exfoliativesamples, surface tumour cells predomi-nate and present as individually dis-persed cell with prominent cytoplasmickeratinization and dark pyknotic nuclei.In contrast, in brushings, cells fromdeeper layers are sampled, showing amuch greater proportion of cohesiveaggregates.
Macroscopy and localization
The tumours are usually white or greyand, depending on the severity of fibro-sis, firm with focal carbon pigmentdeposits in the centre and star-like retrac-tions on the periphery. The tumour maygrow to a large size and may cavitate.Central tumours form intraluminal poly-poid masses and / or infiltrate through thebronchial wall into the surrounding tis-
Squamous cell carcinoma L. CarvalhoI. PetersenA. Gazdar
M. MeyersonS.M. Hanash
J. JenC.C. Harris
N. PetrovitchevY. MatsunoS. AisnerR. Rami-PortaV.L. CapelozziR. Schmidt
S.P. HammarC. BrambillaB. PugatchK. GeisingerE.A. FernandezP. Vogt
B CAFig. 1.08 Squamous cell carcinoma (SCC) cytology. A SCC with keratinization. Sheets of dysplastic and malignant cells. Isolated pleomorphic malignant cells withseveral squamous ghosts. Bronchial brushing. Papanicolaou stain. B SCC without keratinization. Clusters of malignant cells with variation in nuclear shape, dis-tinct nuclear chromatin and high nuclear:cytoplasmic ratio. Bronchial brushing. Papanicolaou stain. C SCC without keratinization, fine needle aspiration cytology.Gaps between cells and distinct cell borders in this sheet of tumor cells identify the tumor as a squamous cell carcinoma. Papanicolaou stain.

27Squamous cell carcinoma
sues and may occlude the bronchiallumen resulting in stasis of bronchialsecretions, atelectasis, bronchial dilata-tion, obstructive lipoid pneumonia andinfective bronchopneumonia. A minorityof cases may arise in small peripheral air-ways. This may be changing since arecent study reported 53% of squamouscell carcinomas were found in the periph-eral lung {640}.
Tumour spread and staging
Central squamous cell carcinoma ischaracterized by two major patterns ofspread: intraepithelial (in situ) spreadwith or without subepithelial invasion,and endobronchial polypoid growth{391,1220}. Extensive intraepithelialspreading is common in major bronchi,and the epithelia of bronchial glands orducts may often be involved. Two pat-terns of early invasive squamous cellcarcinoma have been described: Onegrows laterally along the bronchialmucosa replacing surface epithelium,with submucosal microinvasion andinvolvement of the glandular ducts(“creeping type”); the other appears assmall polypoid mucosal lesions withdownward invasion (“penetrating type”){1424}. Direct involvement of hilar medi-astinal tissue including lymph nodes maybe encountered in advanced cases.Peripheral squamous cell carcinomacharacteristically forms a solid nodule,commonly with intrabronchiolar nodulargrowth, intraepithelial extension, or both{640}. In advanced cases, peripheralsquamous cell carcinoma may involvethe chest wall or diaphragm directlythrough the pleura.Staging is usually performed according tothe TNM system {738,2045}. In general,squamous cell carcinoma tends to belocally aggressive involving adjacentstructures by direct contiguity. Meta-stases to distant organs is much less fre-quent than in adenocarcinoma or otherhistologic types of primary lung cancer{1629}. For peripheral tumours less than 2cm in diameter, regional lymph nodemetastases are exceptional {77}. Tumourswith poorly differentiated histology maymetastasize early in their clinical course toorgans such as the brain, liver, adrenals,lower gastrointestinal tract, and lymphnodes. Locoregional recurrence after sur-gical resection is more common in squa-mous cell carcinoma than in other celltypes {276}.
Histopathology
Squamous cell carcinoma shows kera-tinization, pearl formation and/or intercel-lular bridges. These features vary with
degree of differentiation, being promi-nent in well-differentiated tumours andfocal in poorly differentiated tumours.
DCFig. 1.09 Squamous cell carcinoma (SCC). A Peripheral SCC showing expansile growth, central necrosisand pleural puckering. B Marked cavitation of an SCC arising in an 18 year-old male with HPV11 infectionand papillomatosis. C Central SCC arising in a lobar bronchus with bronchial and parenchymal invasion andcentral necrosis. D Cenral bronchogenic squamous carcinoma with extensive distal obstructive changes,including bronchiectasis.
A
Fig. 1.10 Squamous carcinoma (SCC). A The endobronchial component of this SCC shows a papillary sur-face while the tumour has invaded through the bronchial wall superficially into the surrounding lung. Notethe postobstructive bronchiectasis. B Central bronchogenic SCC arising in the proximal left lower lobebronchus. Contiguous intralobar lymph node invasion, obstructive lipoid pneumonia and mucopurulentbronchiectasis in the basal segments.
BA
B

28 Tumours of the lung - Malignant epithelial tumours
Papillary variant of SCC. This may showexophytic and endobronchial growth insome proximal tumors. Sometimes theremay be a very limited amount of intraep-ithelial spread without invasion; but inva-sion is seen in most cases {218,519}.
Clear cell variant of SCC is composedpredominantly or almost entirely of cellswith clear cytoplasm {634,971}. This vari-ant requires separation from large cellcarcinoma, adenocarcinoma of the lungwith extensive clear cell change andmetastatic clear cell carcinoma from kid-ney.Small cell variant is a poorly differentiat-ed squamous cell carcinoma with smalltumour cells that retain morphologiccharacteristics of a non-small cell carci-noma and show focal squamous differ-entiation. This variant must be distin-guished from combined small cell carci-noma in which there is a mixture of squa-mous cell carcinoma and true small cellcarcinoma. The small cell variant lacksthe characteristic nuclear features ofsmall cell carcinoma having coarse orvesicular chromatin, more prominentnucleoli, more cytoplasm and more dis-tinct cell borders. Focal intercellularbridges or keratinization may be seen{214,372,767,2024}.Basaloid variant shows prominentperipheral palisading of nuclei. Poorlydifferentiated lung carcinomas with anextensive basaloid pattern but lackingsquamous differentiation are regarded asthe basaloid variant of large cell carcino-ma {604,1892,2024}.Alveolar space-filling type of peripheralSCC was recently described in which thetumor cells fill alveolar spaces withoutcausing destruction of the alveolarframework; this contrasts with an
expanding type which causes destruc-tion of the alveolar framework and thelung architecture {640}. This typeappears to comprised only approximate-ly 5% of peripheral SCCs {640}. Rarenon-keratinizing squamous cell carcino-mas resemble a transitional cell carcino-ma.
Electron microscopySquamous cell carcinomas show cyto-plasmic intermediate keratin filaments,which frequently aggregate to formtonofilaments. The less well-differentiat-ed carcinomas show few desmosomesand lesser amounts of cytoplasmic fila-ments.
ImmunohistochemistryThe majority of squamous cell carcino-mas express predominantly high molec-ular weight keratin (34ßE12), cytokeratins5/6, and carcinoembryonic antigen(CEA). Many express low molecularweight keratin (35ßH11) and very fewexpress thyroid transcription factor-1(TTF-1) or cytokeratin 7 (CK7) {352,367,634,1757}.
Differential diagnosis
Separation from large cell carcinoma isbased on the presence of squamous dif-ferentiation. Focal intracellular mucin canbe present. Even though invasive growth isnot identified, papillary SCC can be diag-nosed if there is sufficient cytologic atypia.Small biopsy specimens that show verywell differentiated papillary squamousepithelium should be interpreted with cau-tion since separation of a papillary squa-mous carcinoma from a papilloma can bedifficult. The pattern of verrucous carcino-ma is very rare in the lung and is includedunder papillary squamous carcinoma.
Massive involvement of the anteriormediastinal tissue can make differentialdiagnosis from thymic squamous cellcarcinoma difficult and requires carefulcorrelation with operative and radiologicfindings. In the lung parenchyma, squa-mous cell carcinoma may entrap alveolarpneumocytes, which sometimes resultsin histological misinterpretation asadenosquamous carcinoma {391}.Squamous metaplasia with cytologicatypia in diffuse alveolar damage (DAD)may also raise concern for squamouscarcinoma. The presence of overall fea-tures of DAD such as hyaline mem-branes, diffuse alveolar septal connec-tive tissue proliferation with pneumocytehyperplasia and bronchiolocentricity ofthe squamous changes would favor ametaplastic process.
Somatic genetics
Cytogenetics and CGH Several differences have been foundbetween lung squamous cell carcinomasand adenocarcinomas. Squamous cellcarcinoma of the lung is either a neardiploid or hyperdiploid-aneuploid neo-plasm with mean chromosome numbersin the triploid range {104,1582}.Detection of aneuploidy by DNA meas-urement has been shown to be predic-tive for bad prognosis {1581}. Cyto-genetics and CGH indicated a multitudeof alterations with amplifications of thetelomeric 3q region being most charac-teristic for the squamous carcinoma phe-notype {1582}. Gain of 3q24-qter is pres-ent in the majority of squamopus cell car-cinomas and in a minority of adenocarci-nomas {104,176}. While the gene in theamplicon has not been identified withcertainty, one candidate is the PIK3CAgene, which encodes the catalytic sub-
B CAFig. 1.11 Squamous cell carcinoma (SCC). A Invasion of fibrous stroma. Squamous cell differentiation is evident by the keratin pearls and prominent keratinization.Cytologic atypia with hyperchromatic nuclei indicates cytologic malignancy. B Squamous differentiation in these cytologically malignant cells, is manifest by thesquamous pearl and distinct intercellular bridges. C The squamous differentiation reflected by layers of keratin. From Travis et al. {2024}.

unit of phosphatidylinositol-3 kinase, anessential component of many cell signal-ing pathways {104}. Deletions on theshort arm of chromosome 3 are also fre-quent. Additional recurrent alterationsare deletions on chromosomes 4q, 5q,8p, 9p, 10q, 11p, 13q, 17p, 18q and 21qalong with overrepresentations of chro-mosomes 5p, 8q, 11q13 and 12p {104,125,898,1301,1330,1582}. The numberof chromosomal imbalances accumu-lates during progression {370,1584}.Small interstitial deletions have a tenden-cy to increase in size resulting into adeletion pattern similar to small cell car-cinoma. In contrast, overrepresentationsof entire chromosome arms may con-dense into smaller amplicons. Specificalterations, in particular deletions of3p12-p14, 4p15-p16, 8p22-p23, 10q,21q and overrepresentation of 1q21-q25,8q11-q25 have been associated with themetastatic phenotype {1584}.
Molecular genetics Squamous cell carcinoma commonlyshows distinct molecular genetic charac-teristics. ErbB (EGFR, HER2/neu, KRAS)pathway abnormalities are common innon-small cell carcinoma but absent inSCLC. An average of 84% of squamouscell carcinomas are EGFR positive {608}.Lung cancers with detectable levels ofepidermal growth factor receptor proteinare significantly more frequent amongsquamous cell carcinomas than amongother types of lung tumour {152}.HER2/neu expression, while relativelyfrequent in adenocarcinoma, is relativelyrare in squamous cell carcinoma {845}.While activating mutations of the KRASgene are frequent (~30%) in adenocarci-noma, they are rare in squamous cellcarcinoma.Disruption of normal p53 gene function,usually by point mutations, is frequent inall types of lung cancers. Mutations,
while more frequent in SCLC, occur inthe majority of NSCLC tumours includingsquamous cell carcinomas.Disruption of the RB gene pathway is uni-versal in lung cancers {981}. While muta-tions of the RB gene are the usual methodof disruption in SCLC, they are rare inNSCLC. In NSCLC the mechanism of dis-ruption is via the upstream pathway. Inparticular, inactivation of p16Ink4 asdemonstrated by immunohistochemistry,occurs via epigenetic or genetic mecha-nisms (homozygous deletions, mutations,methylation), while cyclin D1 and E areoverexpressed {215}.Most squamous cell carcinomas demon-strate large 3p segments of allelic loss,whereas most adenocarcinomas and pre-neoplastic/preinvasive lesions have small-er chromosome areas of 3p allele loss{2158} One well studied gene is FHIT(fragile histidine triad) at chromosome3p14.2, by deletions or by a combination
Fig. 1.12 A Exophytic, endobronchial SCC with papillary growth pattern. B Squamous cell carcinoma, papillary variant. The well-differentiated squamous carcino-ma is growing in a papillary pattern. From Travis et al. {2024}.
BA
Fig. 1.13 A Squamous cell carcinoma. Difference histogram between metastatic and non-metastatic squamous cell carcinoma determined by CGH. Each tumorgroup consist of 25 cases. The chromosomal imbalances determined by CGH are shown as incidence curves along each ideogram. Left side loss, right side gains{1584}. B Squamous cell carcinoma, basaloid variant. The nests of tumour cells have prominent peripheral palisading of cells with less cytoplasm and more hyper-chromatic nuclei than the tumour cells situated more centrally that have more abundant cytoplasm and prominent keratinization. From Travis et al. {2024}.
BA
29Squamous cell carcinoma

30 Tumours of the lung - Malignant epithelial tumours
of deletion and promoter region methyla-tion {1855}. The status of another genelocated at 3p21.3, the RASSF1A gene,while more frequently inactivated inSCLC, does not demonstrate differencesin the methylation frequencies betweenNSCLC types {238}.
Epigenetic gene silencingThe major mechanism is methylation,although histone deacetylation plays animportant co-operative role. Mostsilenced genes are known or suspectedtumour suppressor genes. The methyla-tion profile varies with the tumour typeand the methylation rates of APC, CDH13and RAR-beta are significantly higher inadenocarcinomas than in squamous cellcarcinomas {2017}.
Gene expression profiles
Squamous cell lung carcinoma is charac-terized by high-level expression of keratingenes and histologic evidence of kera-tinization. Markers of squamous cell lungcarcinoma have been analyzed usingoligonucleotide and cDNA microarrayhybridisation {163,661} and serial analy-sis of gene expression or SAGE{623,1420}. When results are comparedacross experimental platforms, signifi-cant overlap can be seen. Genes for ker-atin 5, 6, 13, 14, 16, 17, and 19 are promi-nent among the gene expression markersfor squamous cell lung carcinoma. Othergenes found as squamous cell lung car-cinoma markers in more than one dataset include collagen VII alpha 1, galectin7, the ataxia-telangiectasia group D-associated protein, the s100 calciumbinding protein A2, and bullous pem-phigoid antigen 1. In addition, squamouscell lung carcinomas are characterizedby over-expression of the p53-relatedgene p63. Using gene expression profilegenerated by SAGE, a transcriptomemap integrating the gene expression pro-file along each arm of the human chro-mosomes has been generated {623}.This transcriptome map revealed knownchromosome regions and a novel locuswith significantly altered gene expressionpatterns in squamous cell carcinoma.The identification of these molecularchanges may provide potential markersfor lung cancer.
Prognosis and predictive factors
Stage for stage, survival rate for squa-mous cell carcinoma is significantly bet-
ter than for adenocarcinoma. Approxima-tely 80% of patients with resected stage1 (T1 N0 M0) squamous cell carcinomaare alive at five years after diagnosiscompared to approximately 70% of simi-larly staged adenocarcinomas. Similardifferences are seen in the rate of sur-vival between stage 2 squamous cellcarcinoma and stage 2 adenocarcinoma.Histologic factors important in prognosisare difficult to determine, although neo-plasms that exhibit a great deal of necro-sis are thought to be associated with aworse prognosis than those neoplasmthat do not show necrosis.
Clinical criteria Although clinical staging generallyunderestimates the extent of the lesions,the cTNM classification represents themain prognostic factor with clear-cut sur-vival difference between the surgicalcases and the rest (70% of the patients).In non-surgical cases weight loss, poorperformance status and metastasis-relat-ed symptoms convey an adverse prog-nosis. In resectable tumours, advancedage is a cause of increased post opera-tive morbidity. The female gender is afavourable factor in overall lung cancersurvival, but it is mainly clinically signifi-cant in adenocarcinoma and less insquamous cancer. Race is not a progno-sis factor when it can be separated fromsocio-economic factors which affect theoutcome. Many biological tests havebeen published, such as elevation ofLactate Dehydrogenase (LDH) or serumtumour markers, but they are not inde-pendent prognostic factors of cTNMand/or weight loss in most cases.
Histopathological criteria Currently, the stage of disease and theperformance status at diagnosis remainthe most powerful prognostic indicatorsfor survival for primary squamous cellcarcinoma. Nevertheless, histologicsubtyping carries independent prog-nostic information. For example, well-differentiated squamous cell carcinomatends to spread locally within the chestdirectly involving adjacent mediastinalstructures. Poorly differentiated squa-mous cell carcinoma tends to metasta-size early and to distant sites. The alve-olar space-filling pattern of peripheralsquamous cell carcinoma appears tocarry a more favourable prognosis{641}
Genetic predictive factors Prognostic biomarkers of nonsmall celllung carcinoma (NSCLC) have beenidentified, but not ultimately confirmed,including the diminished expression ofcyclin-dependent kinase inhibitors, e.g.,p16INK4A, p21WAF1, and p27KIP1, theoverexpression of cyclins, e.g., cyclin E,members of growth factor signal trans-duction pathways, e.g., HER2 andinsulin-like growth factor-binding protein-3, and the inactivation of tumour suppres-sor genes, e.g., Rb, and FHIT, and p53{146,251,279,332,348,836,875,1007,1327,1406,1432,1817,1856,2012}. P53inactivation is not of prognostic signifi-cance in squamous cell carcinoma{1331}. Epigenetic mechanisms such asDNA methylation transcriptional silencingof p16INK4A and genetic mutations ofp53 are examples of the different molec-ular mechanisms responsible for theirinactivation. p53 and FHIT mutations andepigenetic transcriptional silencing ofp16INK4A are more frequent in squa-mous cell carcinomas compared to ade-nocarcinomas and in smokers comparedto never smokers {1007,1856,2012}.Because most studies have examined arelatively small number of NSCLC, theyhave limited statistical power to comparesquamous cell carcinoma with the otherhistological types. One strategy has beento perform a meta-analysis of multiplereports. For example, a meta-analysis of43 articles revealed that p53 mutationsand/or accumulation predicted poorprognosis of patients with adenocarcino-ma, but not squamous cell carcinoma{1331}. Loss of Rb predicts poor survivalof patients with squamous cell carcinomaor adenocarcinoma {279}, whereas thenuclear localization of the transcriptionfactor YB-1 is a prognostic factor only forsquamous cell carcinoma {1799}.

31Small cell carcinoma
Definitions Small cell carcinoma of the lung (SCLC)A malignant epithelial tumour consistingof small cells with scant cytoplasm, ill-defined cell borders, finely granularnuclear chromatin, and absent or incon-spicuous nucleoli. The cells are round,oval and spindle-shaped. Nuclear mold-ing is prominent. Necrosis is typicallyextensive and the mitotic count is high.
Combined small cell carcinomaSmall cell carcinoma combined with anadditional component that consists ofany of the histologic types of non-smallcell carcinoma, usually adenocarcinoma,squamous cell carcinoma or large cellcarcinoma but less commonly spindlecell or giant cell carcinoma.
ICD-O code
Small cell carcinoma 8041/3Combined small cellcarcinoma 8045/3
Synonyms
Previous classifications used terms suchas oat cell carcinoma, small cell anaplas-tic carcinoma, undifferentiated small cell
carcinoma, intermediate cell type, andmixed small cell/large cell carcinoma butthese are no longer recognised.
Clinical features
Signs and symptoms Symptoms reflect central location andlocoregional spread, although stridorand haemoptysis are comparatively rarewhile hoarsness and vocal cord paralysisare more common, when compared tolocoregional spread of squamous cellcarcinoma. However, clinical symptomsmore often reflect disseminated disease(e.g bone marrow and liver metastases).At the time of primary diagnosis, brainmetastases are diagnosed in a minorityof patients, but tend to develop duringthe course of disease {568,933,1797}.Paraneoplastic syndromes are also com-mon in association with small cell carci-noma.
Imaging Small cell carcinomas appear as hilar orperihilar masses often with mediastinallymphadenopathy and lobar collapse{263,614}. Often, the primary tumour is
not detected on radiographic studies. CTdepicts mediastinal nodal involvementand superior vena caval obstruction withgreater detail than the chest radiograph.Peripheral small cell carcinomas areradiographically indistinguishable fromother pulmonary neoplasms.
Cytology Cytologic specimens show loose andirregular or syncytial clusters, as well asindividual tumour cells frequentlyarranged in a linear pattern {673,936,2231}. Within cohesive aggregates,nuclear moulding is well developed.Mitoses are easily seen. Each neoplasticcell has a high nuclear/cytoplasmic ratiowith an ovoid to irregular nuclear contour.Well-preserved cells feature finely granu-lar and uniformly distributed chromatin,yielding the classic “salt and pepper”quality, while poorly preserved cells havea very dark blue structureless chromatin.Conspicuous nucleoli are absent or rare{1410,2099,2231}. Due to the fragility ofthe malignant nuclei, chromatin streaksare commonly seen in smears of alltypes, but especially in aspiration biop-sies and brushings. In addition, thesmear background often contains apop-totic bodies and granular necroticdebris.
Macroscopy and localization
Tumours are typically white-tan, soft, fri-able perihilar masses that show exten-sive necrosis and frequent nodal involve-
Small cell carcinoma W. TravisS. NicholsonF.R. HirschB. PugatchK. GeisingerE. BrambillaA. Gazdar
I. PetersenM. MeyersonS.M. Hanash
J. JenT. Takahashi
E.A. FernandezF. Capron
Fig. 1.14 Small cell carcinoma. A Central tumor extending toward the lung periphery in a sheath-like fash-ion around bronchovascular bundles. B Small cell carcinoma spreading along peribronchial lymphatics andinterlobular septa.
BA
Fig. 1.15 Cluster of cells with scant cytoplasm,nuclear molding and finely granular chromatin.Absence of nucleoli.Incipient rosette formation.

32 Tumours of the lung - Malignant epithelial tumours
ment. Within the lung the tumour typical-ly spreads along bronchi in a submucos-al and circumferential fashion, ofteninvolving lymphatics. Approximately 5%of SCLC present as peripheral coinlesions {427}.
Tumour spread and staging
The tendency for widespread dissemina-tion at presentation has led to small cellcarcinoma being staged as limited ver-sus extensive disease rather than usingthe TNM system {1871}.
Histopathology (including variants)
Architectural patterns include nesting,trabeculae, peripheral palisading, androsette formation as shared by other neu-roendocrine tumours. Sheet-like growthwithout these neuroendocrine morpho-logic patterns is common. Tumour cellsare usually less than the size of threesmall resting lymphocytes and haveround, ovoid or spindled nuclei andscant cytoplasm. Nuclear chromatin isfinely granular and nucleoli are absent orinconspicuous. Cell borders are rarelyseen and nuclear moulding is common.There is a high mitotic rate, averagingover 60 mitoses per 2mm2. The tumour isby definition high grade, thus grading isinappropriate. No in-situ phase is recog-nized. In larger specimens, the cell sizemay be larger and scattered pleomor-phic, giant tumour cells, dispersement ofnuclear chromatin prominent nucleoli,extensive necrosis, brisk apoptotic activ-ity, and crush artifact with encrustation ofbasophilic nuclear DNA around bloodvessels (Azzopardi effect) may all beseen {1470,2024}.The combined small cell carcinoma vari-ant refers to the admixture of non-smallcell carcinoma elements including squa-mous cell, adeno- and large cell carcino-ma and less commonly spindle cell orgiant cell carcinoma. For combined smallcell and large cell carcinoma thereshould be at least 10% large cells pres-ent {1470}.
ImmunohistochemistryWhile small cell carcinoma is a lightmicroscopic diagnosis, electronmicroscopy shows neuroendocrine gran-ules approximately 100 nm in diameter inat least two-thirds of cases and immuno-histochemistry is positive for CD56, chro-mogranin and synaptophysin in mostcases {1470}. Less than 10% of SCLCare negative for all neuroendocrimemarkers {750}. Small cell carcinoma isalso positive for TTF-1 in up to 90% ofcases {600,975}.
Differential diagnosis 10314The differential diagnosis includes lym-phoid infiltrates, other neuroendocrinetumours, other “small round blue celltumours” (SRBCT), and primary ormetastatic non-small cell carcinomas.Crush artifact can occur not only withsmall cell carcinomas, but also carci-noids, lymphocytes of inflammation or
Fig. 1.16 Small cell carcinoma. A Tumour cells are densely packed, small, with scant cytoplasm, finely gran-ular nuclear chromatin and absence of nucleoli. Mitoses are frequent. B The fusiform (spindle cell) shapeis a prominent feature. The nuclear chromatin is finely granular and nucleoli are absent. C In this example,cells are somewhat larger and show some cytoplasm as well as a few inconspicuous nucleoli. D Small cellcarcinoma with extensive necrosis. E Combined small cell carcinoma and adenocarcinoma. A malignantgland is present within the small cell carcinoma. F Combined small cell and large cell carcinoma. The largecell component has more cytoplasm and prominent nucleoli.
FE
DC
A B
BAFig. 1.17 Small cell carcinoma. A Many tumour cells show a cytoplasm staining with antibody to chromo-granin. B CD56 immunoreactivity with a membranous staining pattern.

33Small cell carcinoma
lymphomas and poorly differentiatednon-small cell carcinomas. In crushedspecimens some preserved tumour cellsmust be seen for a SCLC diagnosis.Immunohistochemical staining for cytok-eratin vs leukocyte common antigen aswell as neuroendocrine markers andTTF-1 may be helpful. Carcinoidtumours, typical and atypical, do notshow the degree of necrosis, mitotic andapoptotic activity of small cell carcino-mas {1470,2024}. Other SRBCTs includ-ing primitive neuroectodermal tumours(PNET) are less mitotically active thanSCLC but also mark for MIC-2 (CD99)and not for cytokeratin or TTF-1 {765,1214}. Positive staining for Cytokeratin20, but not for Cytokeratin 7 or TTF-1 dis-tinguishes Merkel cell carcinoma fromSCLC {326,351}.Morphologic separation of SCLC fromNSCLC can be difficult {846,1240,1470,2024,2089}. Examination of a good qual-ity H&E stained section of well-fixed tis-sue is essential. The distinction does notrest on a single feature but incorporatescell size, nuclear: cytoplasmic ratio,nuclear chromatin, nucleoli, and nuclearmolding. Corresponding cytology speci-mens may show much better-preservedtumour cell morphology.
Histogenesis
While the precise cell of origin is notknown for SCLC, there is likely to be apluripotent bronchial precursor cell thatcan differentiate into each of the majorhistologic types of lung cancer. However,within the spectrum of neuroendocrinetumours, there is closer morphologic andgenetic similarity between large cell neu-roendocrine carcinoma and small cellcarcinoma than either typical or atypicalcarcinoid.
Somatic genetics
Cytogenetics and CGH SCLCs are invariably aneuploid neo-plasms although DNA cytometry fre-quently suggests a near diploid chromo-some content. Cytogenetics and CGHrevealed a characteristic pattern of chro-mosomal imbalances with a high inci-dence of deletions on chromosomes 3p,4, 5q, 10q, 13q and 17p along with DNAgains on 3q, 5p, 6p, 8q, 17q, 19 and 20q{104}. Chromosome 3p deletions arepresent in nearly 100% of cases and areoften associated with a 3q isochromo-some formation. Amplification of chromo-
somal subregions occurs particularlyduring tumour progression and in pre-treated patients. DNA gain of chromo-some 17q24-q25 is a potential marker forbrain metastasis formation {1583}.
Molecular genetic alterationsSCLC and pulmonary carcinoids areclassic neuroendocrine (NE) tumoursand they reflect all of the characteristicfeatures of NE cells. However whileSCLC is highly associated with smoking,carcinoids are not. While these two NEtumours share certain molecular abnor-malities {269,727,1516}, there are alsodifferences. SCLC tumours have a high-er rate of p53 mutations {1516} while car-
cinoids are characterized by mutations inthe menin gene {463}. There are similari-ties and differences in the genetic pro-files of SCLC and NSCLC {269,727,2244}. Most of these differences are rela-tive. The absolute differences betweenthese two major divisions of lung cancerare relatively few and include the pres-ence of Ras gene mutations {1668} andCox-2 {827,1248} over expression inNSCLC, while amplification of MYC {931}and methylation of caspase-8 {1814}, akey antiapoptotic gene, are characteris-tic of SCLC. While loss of cell cycle con-trols is a hallmark of cancers, the mech-anism by which the two major types oflung cancer achieve this aim are very dif-
Fig. 1.18 Small cell carcinoma. Comparative genomic hybridization (CGH). A Chromosomal imbalances areshown as incidence curves along each chromosome. Areas on the left side of the chromosome ideogramcorrespond to loss of genetic material, those on the right side to DNA gains. B CGH analysis of the primarytumour (C) and the metastasis (D) reveals a clonal relationship as evidenced by the high number of commonchanges. Red, DNA losses. Green, DNA gains.
B
A

34 Tumours of the lung - Malignant epithelial tumours
ferent. Inactivation of the retinoblastoma(RB) gene and overexpression of E2F1are almost universal in SCLC {549,981}.SCLC but rarely NSCLC, show more fre-quent inactivation of the 14-3-3 sigmaand p14arf, two important G2 checkpointgenes {551,1471,1520}.Most small cell lung carcinomas andsquamous cell carcinomas demonstratelarge 3p segments of allele loss, where-as most of the adenocarcinomas andpreneoplastic/preinvasive lesions havesmaller chromosome areas of 3p alleleloss {2158}. Because these regions aregene rich, and the genes seldom demon-strate mutations, identification of theTSGs took nearly two decades. PutativeTSGs have been identified at four widelyseparated regions, 3p12-13(ROBO1/DUTT1), 3p14.2 (FHIT), 3p21.3(multiple genes including RASSF1A,FUS1, HYAL2, BAP1, Sema3B, Sema3F,and beta-catenin at 3p21.3), and 3p24-6(VHL and RAR-beta) {2228}. Of these,the FHIT, RASSF1A and RAR-beta genesare the best studied.Mutations of the p53 gene are the mostfrequent genetic abnormality identified in
human cancers, and are more commonin SCLC than in NSCLC. Mutations arethe most common mechanism of deregu-lation of gene activity. The frequency,type, and pattern of mutations in lungcancer are strongly related to cigarettesmoking, with G to T transversions beingmore common in smokers (especiallywomen) than in never smokers {1666}.Multiple other changes occur frequentlyin SCLC, including upregulation of theproapoptotic molecule Bcl-2, activationof autocrine loops (bombesin like pep-tides, c-kit/stem cell factor), upregulationof telomerase, loss of laminin 5 chainsand inhibitors of matrix matalloproteinas-es, and expression of vascular growthfactors. In contrast to inactivation ofTSGs (most often by epigenetic phenom-ena, especially methylation), the genesinvolved at sites of chromosomal gainshave seldom been identified (with theexception of the MYC family). SCLC spe-cific preneoplastic changes have notbeen identified and little is known aboutthe molecular changes preceeding thistumour, although frequent allelic losseshave been identified in histologically nor-
mal or hyperplastic bronchial epitheliumadjacent to invasive tumours {2160}.
Gene expression profilesGene expression analysis can readilyidentify markers for small cell lung carci-noma. Given the histological andimmunohistochemical features of neu-roendocrine differentiation, it is not sur-prising that many of the gene expressionmarkers are neuroendocrine genesincluding chromogranin B, chromograninC, and l-aromatic amino acid decarboxy-lase. Experimental studies of geneexpression in SCLC include analysis ofprimary tumours by oligonucleotidearrays {163}, analysis of primary tumourswith cDNA arrays {661}, and analysis ofcell lines with oligonucleotide arrays{1901}. Strikingly, the three studies iden-tify sets of overlapping genes. All threestudies identified insulinoma-associatedgene 1 (IA-1) and the human achaete-scute homolog 1 (hASH1) as SCLCmarkers. Two of the three studies identi-fied forkhead box g1b (FOXG1B), theIsl1 transcription factor, thymosin beta,and tripartite motif-containing 9.
Prognosis and predictive factors
Adverse clinical prognostic factorsinclude ‘extensive’ stage of disease,poor performance status, elevatedserum LDH or alkaline phosphatase, lowplasma albumin and low plasma sodiumlevels {1523,1849}. No histologic orgenetic factors are predictive of progno-sis {1470}. A small percentage of lowstage tumours may be successfullyresected.
Table 1.10Limited versus extensive staging system for small cell lung cancer (SCLC) {1796}.
Limited stage SCLC
> Patients with disease restricted to one hemithorax with regional lymph node metastases, including hilar, ipsi-, and contralateral mediastinal, or supraclavicular nodes.
> Patients with contralateral mediastinal lymph nodes and supraclavicular lymph nodes since the prognosis is somewhat better than that of distant metastatic sites.
> Patients with ipsilateral pleural effusion (benign or malignant)
Extensive stage disease
> All patients with disease who cannot be included in the limited stage.
creo

35Adenocarcinoma
Definition
A malignant epithelial tumour with glan-dular differentiation or mucin production,showing acinar, papillary, bronchiolo-alveolar or solid with mucin growth pat-terns or a mixture of these patterns.
ICD-O codes
Adenocarcinoma 8140/3Adenocarcinoma mixed subtype 8255/3Acinar adenocarcinoma 8550/3Papillary adenocarcinoma 8260/3Bronchioloalveolar carcinoma 8250/3Nonmucinous 8252/3Mucinous 8253/3Mixed nonmucinous andmucinous or indeterminate 8254/3Solid adenocarcinoma with mucin production 8230/3
Variants
Fetal adenocarcinoma 8333/3Mucinous (“colloid”) carcinoma
8480/3Mucinous cystadenocarcinoma
8470/3Signet ring adenocarcinoma
8490/3Clear cell adenocarcinoma
8310/3
Epidemiology
Adenocarcinoma has surpassed squa-mous carcinoma as the most common
histologic subtype of lung cancer inmany countries {391}. Although mostcases are seen in smokers, it developsmore frequently than any other histologictype of lung cancer in individuals (partic-ularly women) who have never smoked{391,1002}.
Imaging
Compared to other lung cancers, adeno-carcinomas are most frequently periph-eral nodules under 4.0 cm in size {391,614}. They infrequently present in a cen-tral location as a hilar or perihilar massand only rarely show cavitation. Pleuraand chest wall involvement is seen inapproximately 15% of cases and this ismore frequent than with other forms oflung cancer. Hilar adenopathy is less fre-quent with adenocarcinoma than withother forms of lung cancer.Adenocarcinomas account for the major-ity of small peripheral cancers identifiedradiologically. By CT screening, adeno-carcinoma is often distinct from the otherhistologic subtypes of lung cancer. Solidnodules (solid-density), ground glassopacities (non-solid, air-containing) andmixed solid/ground glass (part solid,subsolid) opacities are all recognizedpatterns of adenocarcinoma {817,1050,1425,1952}.Increased use of CT has lead toincreased identification of small periph-eral nodules, many of which prove to beadenocarcinomas. The larger the propor-
tion of solid compared to ground glasscomponent in a lung adenocarcinoma,the greater the likelihood of invasivegrowth and a less favorable outcome.
Cytology
Diagnosis of adenocarcinoma by cytol-ogy is based on a combination of indi-vidual cell cytomorphology and architec-tural features of cell clusters {673,936,1826}. Adenocarcinoma cells maybe single or arranged in three-dimen-sional morulae, acini, pseudopapillae,true papillae with fibrovascular coresand/or sheets of cells. Borders of cellclusters are typically sharply delineated.Cytoplasm varies in volume but is usual-ly relatively abundant. It is typicallycyanophilic and more translucent incomparison with squamous cell carcino-ma. In most cells the cytoplasm is dis-tinctly homogeneous or granular and inothers is foamy due to abundant smallindistinct vacuoles. A single large mucin-filled vacuole may be prominent and, insome cases, distends the cytoplasm andcompresses the nucleus to one margin,forming a so-called signet-ring cell.Nuclei are usually single, eccentric andround to oval with relatively smooth con-tours and minimal nuclear irregularity.Chromatin tends to be finely granularand evenly dispersed in better-differenti-ated tumours and coarse and irregularlydistributed or hyperchromatic in poorlydifferentiated tumours. In most tumours,
Adenocarcinoma P. OhoriR. Rami-PortaT. FranksY. ShimosatoY. MatsunoA. KhoorW.H. Westra
N.A. JambhekarI. Petersen
T. TakahashiT. Kawai
M. MeyersonS.M. Hanash
J. Jen
T.V. ColbyM. NoguchiC. HenschkeM.F. VazquezK. GeisingerT. Yokose
B CAFig. 1.19 A. Bronchioloalveolar carcinoma. High-resolution CT of a part-solid nodule in the right upper lobe in a 71 year-old women. Solid components are central-ly located, surrounded by non-solid component. B Adenocarcinoma. This peripheral tumor consists of a lobulated white mass with central anthracosis and scar-ring. At the periphery there is a yellow area of bronchioloalveolar carcinoma with preservation of airspaces. C Adenocarcinoma. A predominantly bronchioloalve-olar pattern prevailed histologically (alveolar spaces can just be seen on the tumour cut surface); the white and solid foci showed invasive disease.

36 Tumours of the lung - Malignant epithelial tumours
nucleoli are prominent and characteristi-cally they are single, macronucleoli,varying from smooth and round to irregu-lar.Cytologic pleomorphism reflects histo-logic grade and has recently beenreported to be related, in part, to tumoursize. Morishita et al {1388} concludedthat cells from BAC less than 2 cm indiameter are relatively small and round toovoid when compared with other small-sized adenocarcinomas (invasive adeno-carcinoma).Although certain cytologic features havebeen proposed to favor a diagnosis ofBAC over other adenocarcinoma pat-terns {1218,1607}, the diagnosis of BACrequires thorough histologic evaluation toexclude the presence of invasive growth.Mucinous BAC may be suggested basedon the cytologic features in the appropri-ate radiologic setting. BAC cells in wash-ings and bronchoalveolar lavage tend tobe homogeneous with uniform, round,smooth, pale nuclei and inconspicuousnucleoli. BAC often shows clusters of uni-form cells that display a three-dimension-al “depth of focus”, especially with the
mucinous type, presumably due to theirabundant cytoplasm. Tissue fragmentsin aspiration specimens may show histo-logic features such as growth alongintact alveolar septal surfaces {1218},but this does not exclude an unsampledinvasive component. On occasion, indi-vidual BAC cells resembling alveolarmacrophages are dispersed in a smearbut can be recognized because nucleiare rounder and larger than macrophagenuclei and a few cohesive clusters areusually present.Currently, there are no established crite-ria for diagnosing AAH on cytology andto distinguish it from nonmucinous BAC.Anecdotally there is apparent overlap ofthe cytologic features. The Early LungCancer Action Project (ELCAP) has acytology protocol, which includes a cate-gory of lesions designated “atypicalbronchioloalveolar cell proliferation”when the findings are suspicious for, butnot diagnostic of BAC {817,818}. Thedesignation applies to lesions, which,when resected, may prove to be eitheratypical adenomatous hyperplasia (AAH)or BAC.
Macroscopy and localization
Pulmonary adenocarcinomas may besingle or multiple and have a wide rangein size. The vast majority of pulmonaryadenocarcinomas present with one of sixmacroscopic patterns and these all havecorresponding radiologic correlates.Combinations of these patterns may alsooccur.The most common pattern is a peripher-al tumour {1809}. Gray-white centralfibrosis with pleural puckering may beapparent. The central area underlyingpleural puckering is often a V-shapedarea of desmoplastic fibrosis associatedwith anthracotic pigmentation. Invasion,when present histologically, is identifiedin areas of fibrosis and may be accom-panied by necrosis, cavitation, and hem-orrhage. The edges of the tumour maybe lobulated or ill defined with stellateborders. In small tumours with a contigu-ous nonmucinous BAC pattern somealveolar structure may be grossly appar-ent at the edge of the solid portion of thenodule corresponding to the groundglass opacity noted radiologically inthese lesions. Some peripheral adeno-
B CAFig. 1.21 Adenocarcinoma cytology. A Three-dimensional, large cluster of uniform malignant cells with distinct nuclear structure, nucleoli and finely vacuolatedcytoplasm. Bronchial brushing. Liquid Based Cytology. Papanicolaou stain. B Cohesive three-dimensional cluster with papillary pattern. Fine needle aspiration, con-ventional cytology. Papanicolaou stain. C This cluster of malignant cells lacks definite cytoplasmic borders but shows vacuolization. Pale nuclei have small but dis-tinct nucleoli. Fine needle aspiration, conventional cytology. Papanicolaou stain.
B CAFig. 1.20 Adenocarcinoma of mixed subtypes in a nonsolid nodule which developed a solid component. A High-resolution CT of a nonsolid nodule in the right mid-dle lobe in a 76 year-old woman. B High resolution CT four years later shows the development of a solid component without any increase in the overall size of thenodule. C One year later the solid component has increased.

37Adenocarcinoma
carcinomas may have a gelatinous qual-ity due to abundant mucin production.A second pattern of adenocarcinoma is acentral or endobronchial tumour {1042}.The neoplasm may grow as a plaque orin polypoid fashion with preservation ofthe overlying mucosa. With increasingdegrees of bronchial luminal obstruction,the distal parenchyma may showobstructive “golden” (lipoid) pneumonia.The third pattern is a diffuse pneumonia-like, lobar consolidation with preservationof underlying architecture, typical ofmucinous BAC.A fourth pattern consists of diffuse bilat-eral lung disease. In some cases thismanifests as widespread nodules (vary-ing from tiny to large) involving all lobes;in other cases the appearance suggestsan interstitial pneumonia due to wide-spread lymphangitic spread of carcino-ma.In the fifth pattern, the tumour preferen-tially invades and extensively dissemi-nates along the visceral pleura, resultingin a rind-like thickening mimicking malig-nant mesothelioma (pseudomesothe-liomatous carcinoma) {1060}.Finally adenocarcinoma may develop inthe background of underlying fibrosis,either a localized scar or diffuse intersti-tial fibrosis {391} Adenocarcinoma aris-ing in association with a focal scar isquite rare, in contrast to the relativelycommon central secondary scarring thatdevelops in localized peripheral adeno-carcinomas.
Tumour spread and staging
Adenocarcinoma spreads primarily bylymphatic and hematogenous routes.
Aerogenous dissemination commonlyoccurs in bronchioloalveolar carcinomaand is characterized by spread of tumourcells through the airways forming lesionsseparate from the main mass.Aerogenous dissemination can includeinvolvement of the same lobe or differentlobes in the ipsilateral and/or contralater-al lung resulting in the multicentricityseen in bronchioloalveolar cell carcino-ma. Peripheral adenocarcinomas occa-sionally spread over the pleural surfacesmimicking mesothelioma.Approximately one fifth of newly diag-nosed adenocarcinomas present withdistant metastases. Brain, bone, adrenalglands and liver are the most commonmetastatic sites {1629}. Isolated localrecurrence after resection is less com-mon in adenocarcinoma than in othernon-small cell types {276}.Adenocarcinomas are staged accordingto the international TNM system {738,2045}.
Histopathology
Adenocarcinomas mixed subtype. Theseare the most frequent subtype, repre-senting approximately 80% of resectedadenocarcinomas {1993}. In addition tothe mixture of histologic subtypes, differ-ent degrees of differentiation (well, mod-erate, poor) and cytologic atypia (mild,moderate, marked) are typically encoun-tered, varying from field to field andblock to block. Any of the histologic sub-types may have a component with a lossof cellular cohesion with individualtumour cells filling alveolar spaces.The major individual histologic pat-terns/subtypes are acinar, papillary,
bronchioloalveolar, and solid adenocar-cinoma with mucin production {2024}.Adenocarcinomas consisting purely ofone of these histologic subtypes areuncommon compared to the mixed histo-logic subtype, especially in largertumours. Well, moderate, and poorly dif-ferentiated histologies are recognizedamong the acinar and papillary tumours.The bronchioloalveolar pattern is virtuallyalways moderately or well differentiated.The acinar pattern is characterized byacini and tubules composed of cuboidalor columnar cells which may be mucin
B CAFig. 1.22 Adenocarcinoma. A The malignant nuclei are ovoid with delicate smooth membranes and finely reticulated, evenly dispersed chromatin with small nucle-oli and a single large nuclear pseudoinclusion. Cytoplasm is delicate and contains secretory vacuoles some of which contain mucin. Diff-Quik. B A cluster of tumorcells is present in this sputum sample from a patient with a bronchioloalveolar carcinoma cells, mucinous type. The cells have relatively small bland nuclei withsmooth outlines, fine even chromatin, and inconspicuous nucleoli. The nuclear-to-cytoplasmic ratios are low as cytoplasmic mucin vacuoles occupy most of thecellular volume. Papanicolaou stain. C This bronchial washing demonstrates the alveolar macrophage pattern of bronchiolalveolar carcinoma. Neoplastic cells areindividually dispersed. They have relatively low nuclear-to-cytoplasmic ratios and delicate, vacuolated cytoplasm. However, compared to the adjacentmacrophages, the nuclei are larger and hyperchromatic. Papanicolaou stain.
Fig. 1.23 Adenocarcinoma, summary of macro-scopic growth patterns. Pattern 1 is the most com-mon type: peripheral adenocarcinoma with desmo-plastic fibrosis retracting the overlying pleura.Pattern 2 is the central or endobronchial adeno-carcinoma. Pattern 3 is the diffuse pneumonia-likeconsolidation often associated with bronchi-oloalveolar or papillary growth. Pattern 4 repre-sents the diffuse pleural thickening seen in‘pseudomesotheliomatous carcinoma’ (see redline). Pattern 5 is the adenocarcinoma arising in thebackground of underlying fibrosis.

38 Tumours of the lung - Malignant epithelial tumours
producing and resemble bronchial glandor bronchial lining epithelial cells, includ-ing Clara cells {2024}.The papillary pattern is characterized bypapillae with secondary and tertiary pap-illary structures that replace the underly-ing lung architecture {2024}. Necrosisand lung invasion may be present.Bronchioloalveolar carcinomas that havesimple papillary structures within intactalveolar spaces are excluded from thisdefinition. The lining cells in papillaryadenocarcinoma may be cuboidal tocolumnar, mucinous or non-mucinousand some cases may mimic papillarycarcinoma of the thyroid. Some evidencesuggests a micropapillary pattern of ade-nocarcinoma, in which papillary tufts lacka central fibrovascular core, may beprognostically unfavourable {1335}.A bronchioloalveolar carcinoma (BAC)pattern shows growth of neoplastic cellsalong pre-existing alveolar structures(lepidic growth) without evidence of stro-mal, vascular, or pleural invasion {2024}.Septal widening with sclerosis is com-
mon in bronchioloalveolar carcinomas,particularly the non-mucinous variant.When there is marked alveolar collapsewith increase in elastic tissue in the thick-ened alveolar septa, distinction betweensclerosing BAC and early invasive ade-nocarcinoma may be difficult. Invasion isgenerally characterized by significantincrease in cytologic atypia, a fibroblas-tic stromal reaction, and usually an aci-nar pattern of growth.The non-mucinous variant of BAC typi-cally shows Clara cell and/or type II celldifferentiation {2024}. Clara cells are rec-ognized as columnar with cytoplasmicsnouts and pale eosinophilic cytoplasm.Nuclei may be apical in location. Type IIcells are cuboidal or dome-shaped withfine cytoplasmic vacuoles or clear tofoamy cytoplasm. Intranuclear eosino-philic inclusions may be present. In non-mucinous BAC there is no known clinicalsignificance in distinguishing Clara fromtype II cells.Mucinous BAC is by definition low grade,composed of tall columnar cells with
basal nuclei and pale cytoplasm, some-times resembling goblet cells, with vary-ing amounts of cytoplasmic mucin andtypically showing mucin production withmucus pooling in the surrounding alveo-lar spaces {2024}. Cytologic atypia isgenerally minimal. Aerogenous spread ischaracteristic and satellite tumours sur-rounding the main mass are typical.Extensive consolidation is common,sometimes with a lobar and/or pneumon-ic pattern. By convention small lesions,even those a few millimeters in size,showing this histology are consideredmucinous BAC.Rarely BACs are composed of a mixtureof mucinous and non-mucinouscells.Mucinous and nonmucinous BACmay be solitary lesions, multifocal or con-solidative (eg lobar) and the latter twoare interpreted as aerogenous spread.Most solitary BACs encountered are ofthe nonmucinous subtype.Solid adenocarcinoma with mucin iscomposed of sheets polygonal cellslacking acini, tubules, and papillae but
BAFig. 1.24 Acinar adenocarcinoma. A This tumour forms irregular-shaped glands with cytologically malignantcells exhibiting hyperchromatic nuclei in a fibroblastic stroma. B Positive immunohistochemical staining forTTF-1 in an acinar adenocarcinoma. The nuclear staining varies.
Fig. 1.25 Papillary adenocarcinoma. Tumour cellsshow a complex papillary glandular proliferationalong fibrovascular cores. From Travis et al. {2024}.
Fig. 1.26 A,B Invasive adenocarcinoma. Central area of invasion in an adenocarcinoma that at the periphery consisted of a non-mucinous bronchioloalveolar car-cinoma. Invasion is associated with a significant increase in cytologic atypia and myofibroblastic stroma.
BA

39Adenocarcinoma
with mucin present in at least 5 tumourcells in each of two high power fieldsconfirmed with histochemical stains formucin {2024}. Squamous carcinomasand large cell carcinomas of the lungmay show rare cells with intracellularmucin production, but this does not indi-cate classification as adenocarcinoma.Adenocarcinoma with mixed histologicpatterns is an invasive tumour in whichthere is a mixture of histologic subtypes.The pathologic diagnosis of adenocarci-noma with mixed histologic patternsshould include the histologic subtypewith a comment about the pattern(s)identified: for example “adenocarcinomawith acinar, papillary and brochioloalveo-lar patterns”. The extent of the stromalinflammation and fibrosis varies {391}.Small tumours (<2 cm.) with a BAC com-ponent should be histologically sec-
tioned entirely to search for foci of inva-sion and to measure the size of fibroticscars. Complete sampling is required fora diagnosis of localized nonmucinousBAC. In tumours that exhibit a compo-nent of nonmucinous BAC, the size andextent of invasion and scarring should benoted, as these may have prognosticimportance. Tumours with localized fibro-sis less than 5 mm. in diameter (regard-less of the presence or absence of inva-sion) appear to have a 100% 5-year sur-vival similar to localized BAC {1484,1929,1993,2208} This localized fibrosisdiffers from the mild alveolar septal scle-rosis and elastosis that is common innonmucinous BAC. Central scars typical-ly present as alveolar collapse withdense elastosis or active fibroblastic pro-liferation; when invasive carcinoma ispresent it is usually identified in regions
of active fibroblastic proliferation andassociated with increased atypia of theneoplastic cells. In some cases the dis-tinction between elastotic sclerosis withtrapping of airspaces lined by atypicalcells from foci of fibroblastic proliferationwith invasion may be difficult. In the set-ting of underlying diffuse interstitial fibro-sis (from a variety of causes) there is sig-nificant fibrosis with honeycombchanges. However, all histologic types oflung cancer, not just adenocarcinoma,may arise in this setting {91}.Multifocal invasive adenocarcinomasmay be encountered. If a component ofnonmucinous BAC can be confirmedcontiguous with the invasive carcinoma,a presumptive diagnosis of a primarycarcinoma can be made. Separate pri-mary adenocarcinomas should be distin-guished from satellite lesions that may be
Fig. 1.27 Chest x-ray from an 18-year-old nonsmok-ing woman who presented with bilateral non-muci-nous bronchioloalveolar carcinoma.
Fig. 1.28 Bronchioloalveolar carcinoma, non-muci-nous subtype. Fine needle aspiration cytologyshows a cohesive cell group with variable nuclearsize, prominent nucleoli and perinucleolar clearing.
Fig. 1.30 Bronchioloalveolar carcinoma, non-mucinous, subtype. A Cuboidal to columnar tumor cells growalong alveolar walls. The monotony and crowding of the cells exclude a metaplastic process. From Traviset al. {2024}. B Immunohistochemistry for surfactant apoprotein A.
BAFig. 1.31 Bronchioloalveolar carcinoma, mucinoussubtype. There is a monotonous proliferation ofwell-differentiated mucinous epithelium growingalong alveolar walls in a lepidic fashion with anabrupt transition from tumor to normal alveolarwalls.
Fig. 1.29 Bronchioloalveolar carcinoma, non-muci-nous. Cuboidal to columnar shaped cells growalong alveolar walls in a lepidic fashion.

40 Tumours of the lung - Malignant epithelial tumours
encountered adjacent to the maintumour. Histologic disimilarity betweenthe tumours also favors separate primar-ies. A definitive diagnosis of multifocalityrequires proof of molecular/genetic dif-ferences between the tumours, but suchstudies are often not feasible. Whether atumour is classified as a separate pri-mary or an intrapulmonary metastasishas implications regarding staging.
Fetal adenocarcinoma Synonyms: well differentiated fetal ade-nocarcinoma, pulmonary adenocarcino-ma of fetal type, pulmonary endodermaltumour resembling fetal lung.This is a distinctive adenocarcinomavariant consisting of glandular elementscomposed of tubules of glycogen-rich,non-ciliated cells that resemble fetal lungtubules. Subnuclear and supranuclearglycogen vacuoles give the tumour anendometrioid appearance. Roundedmorules of polygonal cells with abundanteosinophilic and finely granular cyto-plasm are common {2024} (and resem-ble squamous morules in endometrioidadenocarcinomas). Some cases show a
clear cell pattern. Rarely, fetal adenocar-cinomas are associated with other histo-logic types of lung cancer includingother subtypes of adenocarcinoma. Mostfetal adenocarcinomas are well differenti-ated; Nakatani, et al {1436} has recentlydescribed a variant designated poorlydifferentiated fetal adenocarcinoma.When fetal adenocarcinoma is associat-ed with a sarcomatous primitive blaste-mal stroma the tumour is classified aspulmonary blastoma.
Mucinous (“colloid”) adenocarcinomaA lesion identical to their counterparts inthe gastrointestinal tract, with dissectingpools of mucin containing islands of neo-plastic epithelium {2024}. The epitheliumin such cases may be extremely well dif-ferentiated and sometimes tumour cellsfloat within the pools of mucin.
Mucinous cystadenocarcinomasA circumscribed tumour that may have apartial fibrous tissue capsule. Centrallythere is cystic change with mucin poolingand the neoplastic mucinous epitheliumgrows along alveolar walls.
Signet ring adenocarcinomaSignet ring adenocarcinoma in the lungis usuallly a focal pattern associated withother histologic subtypes of adenocarci-noma. Exclusion of a metastasis, particu-larly from the gastrointestinal tract isimportant.
Clear cell adenocarcinoma.This morphological feature is most oftenfocal, but rarely it may be the major com-ponent of the tumour (clear cell adeno-carcinoma) and it may occur in any of themajor patterns of adenocarcinoma {391,2024}. Metastatic renal cell carcinoma isan important consideration in suchcases.
ImmunohistochemistryThe immunohistochemical features ofadenocarcinomas vary somewhat withthe subtype and the degree of differentia-tion. Expression of epithelial markers(AE1/AE3, CAM 5.2, epithelial membraneantigen, and carcinoembryonic antigen)is typical {391}. CK7 is more frequentlyexpressed than CK20 {1702}. TTF-1staining is usually present, especially inbetter-differentiated tumours {1137,2201}. In TTF-1 positive cases, a negativethyroglobulin helps to exclude metastaticthyroid carcinoma. Staining for surfactantapoprotein is seen less frequently thanTTF-1 but is more problematic due topotential absorption of surfactant bymetastatic tumour cells from the sur-rounding lung {14}. Mucinous tumours,especially mucinous BAC may representexceptions, being TTF-1 negative andpositive for CK7 and frequently CK20{1136,1790}.
Differential diagnosis
The differential diagnosis includesmetastatic adenocarcinoma, mesothe-
B CAFig. 1.32 Bronchioloalveolar carcinoma, mucinous subtype. A Computed tomography of a mucinous bronchioloalveolar carcinoma that presented as diffuse bilat-eral lung disease. B Macroscopy of mucinous bronchioloalveolar carcinoma, producing consolidation of a lobe without discrete mass formation. C Closer view ofthe macroscopy of another mucinous bronchioloalveolar carcinoma shows multiple tiny nodules.
BAFig. 1.33 A Solid adenocarcinoma with mucin formation. This poorly differentiated subtype of adenocarci-noma shows a substantial number of intracytoplasmic mucin droplets as seen on this periodic acid Schiffstain after diastase digestion. B Well-differentiated fetal adenocarcinoma, growing in glands withendometrioid morphology, including squamoid morules. Tumour cells are columnar, with clear cytoplasmthat often has subnuclear vacuoles similar to endometrial glands. From Travis et al. {2024}.

41Adenocarcinoma
lioma, AAH, and reactive pneumocyteatypia associated with scars or organiz-ing alveolar injury.Patients with metastatic adenocarcinomausually have a history of primary carcino-ma and present with multiple lesions inthe lung. Obtaining the histologic slidesfrom the primary carcinoma for compari-son with the histology of the lung lesioncan be very informative. If the lesion inthe lung is solitary, differentiationbetween primary and metastatic carcino-ma may be more difficult. The presenceof heterogeneity of histologic subtypes ischaracteristic of lung adenocarcinomaand this feature may be helpful in sepa-rating pulmonary primary from metastat-ic adenocarcinomas, since the lattertend to be more homogeneous. Thepresence of a bronchioloalveolar carci-noma (BAC) component favours primaryadenocarcinoma of the lung over a
metastasis. However, some metastaticadenocarcinomas may rarely spreadalong the alveolar septa and mimic bron-chioalveolar carcinoma.Adenocarcinomas of the lung often showdifferentiation toward Type II cells orClara cells and express markers foundnormally in these cell types. Up to 60% ofpulmonary adenocarcinomas expresssurfactant proteins (SP-A, pro-SP-B, pro-SP-C) {138}. Thyroid transcription factor1 (TTF-1), a transcription factor that playsan important role in the lung specificexpression of surfactant proteins, isexpressed in up to 75% of pulmonaryadenocarcinomas {2232}. Metastaticadenocarcinomas with the exception ofcarcinomas of thyroid origin are negativefor TTF-1. Negative mucin stains andpositive staining for thyroglobulin helpseparate metastatic thyroid carcinomafrom an adenocarcinoma of the lung.
This topic is discussed in more detailbelow in the section on metastases.Cytokeratin (CK) 7 and CK20 may alsobe useful in differentiating primary versusmetastatic adenocarcinoma {1702}. Mostpulmonary adenocarcinomas have aCK7 positive, CK20 negativeimmunophenotype. One exception ismucinous BAC, which is usually positivefor CK20 and negative with TTF-1. Thedifferentiation of mucinous BAC frommetastatic colonic adenocarcinoma,which is also typically CK20 positive, isaided with positive staining for the CDX2homeobox gene {110,2124}. Prostatespecific antigen, prostatic acid phos-phatase and gross cystic disease fluidprotein 15 may identify metastatic ade-nocarcinomas of prostate and breast ori-gin, respectively {403,1780}.Differentiation between pulmonary ade-nocarcinoma and epithelioid malignant
DC
BA
Fig. 1.34 A Mucinous (“colloid”) adenocarcinoma.This subpleural tumor has a lobulated gelatinous tan-white surface. B Mucinous (“colloid”) adenocarcinoma.The tumour consists of pools of mucin flooding airspaces and spreading in a permeative fashion into adjacent alveolar tissue. At low power microscopy the neo-plastic cells are difficult to discern. C Mucinous (“colloid”) adenocarcinoma. There is abundant mucin within alveolar spaces. Scattered clusters of tumour cellsare present within the pools of mucin. Columnar mucinous epithelial cells line fibrotically thickened alveolar walls. D Signet ring adenocarcinoma. Tumour cellscontain abundant cytoplasmic mucin that pushes the nucleus to the periphery. Stromal invasion adjacent to bronchial cartilage (left). From Travis et al. {2024}.

42 Tumours of the lung - Malignant epithelial tumours
mesothelioma should include clinical,macroscopic and microscopic, as wellas immunohistochemical and/or electronmicroscopic analysis. This is addressedin detail in the pleural chapter. A typicalworkup should include a mucin stain,pan cytokeratin, and at least 2 generaladenocarcinoma markers (e.g. CEA,CD15, or MOC 31), a marker specific forpulmonary adenocarcinoma (TTF-1) and2 mesothelioma markers (e.g. calretinin,cytokeratin 5/6) {286,395}. When exam-ined under the electron microscope,microvilli of malignant mesothelioma aremore slender than those of pulmonaryadenocarcinoma. In malignant mesothe-lioma, the ratio of length to diameter oftenexceeds 10 {2107}.The separation of a small peripheral non-mucinous BAC from AAH may be diffi-cult. No single criterion suffices and thisdistinction must be based on a constella-tion of features. Nonmucinous bron-chioalveolar carcinoma is typically >5mm. size with marked cellular stratifica-tion, high cell density and marked over-lapping of nuclei, coarse nuclear chro-matin and the presence of nucleoli,columnar cell change with cellularcrowding, and micropapillary tufting.AAH usually shows no more than one ofthese features. Marked pneumocyteatypia may be encountered adjacent tolung scars and associated with organiz-ing alveolar injury. In the latter situation ahistory of pneumonia or prior chemother-apy or radiation is very helpful. In bothsituations the presence of a heteroge-neous population of metaplastic cells,including ciliated cells, and a relativelack of cellular crowding and cytologicmonotony (which favor adenocarcinoma)are important.Prominent bronchiolar metaplasia infibrotic lesions such as usual interstitialpneumonia may be confused with ade-nocarcinoma. The presence of papillaryor invasive growth and abundant intracy-toplasmic mucin favors adenocarcino-ma.
Grading
Histological grading is a qualitativeassessment of tumour differentiation andis an important component of the pathol-ogy report. Grading of pulmonary adeno-carcinomas is based on conventionalhistological criteria, including the extentto which the architectural pattern of thetumour resembles normal lung tissue,
and cytologic atypia. The amount of eachcomponent should be considered.Typically, three grades are used. Well(grade 1), moderate (grade 2), and poor-ly differentiated (grade 3) tumours arerecognized among acinar and papillaryadenocarcinomas. The bronchioloalveo-lar pattern is virtually always well or mod-erately differentiated, whereas solid ade-nocarcinomas are poorly differentiated. Ifthere is evidence of more than one gradeof differentiation in a tumour, the least dif-ferentiated component should be record-ed as the histological grade.
Histogenesis
Attempts to identify the cell of origin forlung adenocarcinomas has been frustrat-ed by the diversity of epithelial cell typeslining the airways, the propensity of lungadenocarcinomas to undergo phenotyp-ic shifts during tumour progression, andthe consequent morphologic hetero-geneity among different lung adenocar-cinomas and even within individualtumours. The phenotypic expression isinfluenced by anatomic location.Centrally located tumours arising fromthe large bronchi typically consist of acombination of columnar cells and muci-nous cells. These central adenocarcino-mas likely arise from the bronchialepithelium or bronchial glands. The
absence of a recognized preinvasivelesion for these central adenocarcinomashas handicapped efforts to trace theirorigin to a specific progenitor cell.Most adenocarcinomas develop in thelung periphery. By light microscopy,electron microscopy, immunohistochem-istry and gene expression analysis, theseperipheral adenocarcinomas are com-posed of cells that closely resemble typeII pneumocytes and Clara cells {163,481,661,800} and these cells are identified asthe likely cells of origin {1021,1377,1521}. AAH is recognized as a preinva-sive lesion for peripheral lung adenocar-cinomas (particularly non-mucinousbronchioloalveolar carcinomas) {2125}.In AAH, the epithelial cells consist most-ly of type II pneumocytes; Clara cells aremore likely to be seen in bronchioloalve-olar carcinomas than in AAH {481,800,1022}.
Somatic genetics
Cytogenetics and CGHLung adenocarcinoma may be neardiploid with only simple numerical chro-mosome changes, in particular loss ofthe Y chromosome and gains of auto-somes 1 and 7. Alternatively, they maybe hyperdiploid but also, even less com-monly, hypodiploid, particularly the latterstate being associated with extensive
Fig. 1.35 Adenocarcinoma. Chromosomal imbalances of 30 primary lung adenocarcinomas. The chromoso-mal imbalances are shown as incidence curves along each chromosome. Areas on the left side of the chro-mosome ideogram correspond to loss of genetic material, those on the right side to DNA gains. The fre-quency of the alterations can be determined from the 50% and 100% incidence lines depicted parallel to thechromosome ideograms. DNA changes with 99% significance are coloured in blue, additional changes with95% significance are depicted in green. The proportion of pronounced DNA imbalances are visualised inred. They are most likely to represent high copy amplifications or multi copy deletions.

43Adenocarcinoma
numerical and structural aberrations. Themean chromosome number is near thetriploid range {104,1330}. The most fre-quent chromosomal imbalance is 1qoverrepresentation {1582}. It is probablyresponsible for the inherent highercapacity of adenocarcinoma for hemato-genous dissemination compared tosquamous cell cancer because gain ofthe centromeric 1q region is also associ-ated with metastasis formation {698}.Other frequently observed imbalancesare deletions on chromosomes 3p, 4q,5q, 6q, 8p, 9, 13q and gains on 5p, 8q,20q {104,125,698,898,1301,1330,1582}.The CGH pattern can be helpful in thedifferentiation from squamous cell carci-noma {1582} and in particular mesothe-lioma {178,1075}.
Molecular genetics The genetic alterations in adenocarcino-ma include point mutations of dominantoncogenes, such as the K-ras gene, andtumour suppressor genes such as p53and p16Ink4. K-ras mutations occur inapproximately 30% of adenocarcinomas{1837} but are rare in other lung cancers.Most mutations are in codon 12, withsmaller numbers in codon 13 and rarelyin codon 61. They are more common incancers arising in smokers. Mutationsresult in constant downstream signalingresulting in proliferative stimuli. Mutationshave also been described in the putativeprecursor lesion, atypical adenomatoushyperplasia. p53 mutations are also anegative prognostic factor for limitedstage adenocarcinoma {432,1331}.Increased expression of p27, one of thecell cycle regulators, correlates with bet-ter tumour differentiation and morefavourable prognosis {2200}. p16Ink4inactivation by multiple mechanismsoccurs frequently in adenocarcinomasand may be smoking related {1300}.LKB1/STK11, the gene responsible forPeutz-Jeghers syndrome, is reported tobe frequently inactivated in adenocarci-noma of the lung {1733}. Other importantchanges frequent in adenocarcinomas,but also present in smaller numbers ofother non-small cell carcinomas, areover-expression of the HER2/Neu andCOX-2 genes.
Expression profiles Recently, using the microarray tech-nique, several genome-wide analyseshave been reported. For example, using
gene expression profiling, lung carcino-mas have been subdivided into severalgroups and it has been possible to dis-criminate primary cancers from metas-tases of extrapulmonary origin {163,661,1332,1638,2147}. The abnormal expres-sion of genes involved in maintaining themitotic spindle checkpoint and genomicstability contributes to the molecularpathogenesis and tumour progression oftobacco smoke-induced adenocarcino-ma of the lung {1332}. Alterations in cellcycle genes have also been identified inlung adenocarcinoma using geneexpression profiling {1830}.Gene expression profiles revealed bymicroarray analyses have been found tobe of prognostic significance in adeno-carcinomas. Two studies have focusedon classifying lung adenocarcinomas{163,661} using hierarchical clustering{535} to identify sub-classes in an unbi-ased fashion. Two of these subclassesare highlighted below. One adenocarci-noma subgroup is comprised of tumoursthat express neuroendocrine markers,such as l-aromatic amino acid decar-boxylase, the human achaete-scutehomolog 1 (hASH1), and insulinoma-associated 1. This expression patternwas associated with a significantdecrease in patient survival when com-pared to other adenocarcinomas {163}.Adenocarcinoma group 1 of the cDNAmicroarray expression study {661}shared significant patterns of relativelyhigh-level gene expression with adeno-carcinoma group C4 in the oligonu-cleotide array study {163}. These studiesidentified a subset of adenocarcinomathat appeared to express markers ofalveolar type II pneumocytes {661}. Highrelative expression levels of surfactantprotein genes and several other sharedgenes, including BENE, cytochrome b5,and selenium-binding protein 1, charac-terize these two groups. These sampleswere often diagnosed as bronchioloalve-olar carcinomas {163} and appear toform a clear and distinct branch withinthe adenocarcinomas. More recently, arisk index compiling the relative expres-sion of 50 genes was developed to iden-tify high or low risk groups of Stage I ade-nocarcinomas that correlated inverselywith patient survival {133} Using an inde-pendent, non-selective gene expressionanalysis method, serial analysis of geneexpression or SAGE {623,1420} demon-strated that lung adenocarcinoma
exhibits distinct molecular characteris-tics as observed by the oligonucleotidemicroarray {163}. Furthermore, SAGEanalyses also identified the down regula-tion of several p53 regulated genes andthe over expression of immuno-relatedgenes in lung adenocarcinoma {1420}.Matrix-assisted laser desorption/ionisa-tion mass spectrometry has been utilizedto classify lung tumors based on theirproteomic profile. In one study, proteom-ic spectra were obtained for 79 lungtumors and 14 normal lung tissues{2194}. More than 1600 protein peakswere detected from histologically select-ed 1 mm diameter regions of singlefrozen sections from each tissue. Class-prediction models based on differentiallyexpressed peaks enabled the classifica-tion of lung cancer histologies, distinc-tion between primary tumors and metas-tases to the lung from other sites, andclassification of nodal involvement with85% accuracy {2194}.
Prognostic and predictive factors
Radiologic featuresLesions with a component of groundglass opacity found in the context of CTscreening, when resected, were found tobe 1) atypical adenomatous hyperplasia,if very small, and when larger either 2)bronchioloalveolar carcinoma or 3)mixed adenocarcinoma with BAC andother patterns {819,1324,1425}. Kodamaet al. {1039} showed that the ground-glass component correlates with thebronchioloalveolar carcinoma compo-nent in the histologic specimen.CT screening which started in 1993 inJapan, showed long-term survival ofpatients with nodules to be associatedwith ground glass opacity {1038,1039,2112,2192}. All of these studies show amore favourable prognosis for patientswith tumours having a larger ground-glass component than a solid compo-nent, with long-term survival rates of upto 100%. Suzuki {1926} showed thatnone of the 69 cases of lung cancerfound in sub-solid nodules had lymphnode metastases and all were alive witha median follow-up time of 35 months.Takashima et al found that the presenceof air bronchograms was an independentpredictor of prognosis {1951}.
Histopathological criteria Histological grading has prognosticimplications. In general, patients with

44 Tumours of the lung - Malignant epithelial tumours
poorly differentiated adenocarcinomashave more local recurrences and lymphnode metastases than patients with wellor moderately differentiated tumours{371}. However, histological grade maynot be of prognostic importance inperipheral T1 adenocarcinoma {408}.The papillary pattern, including caseswith a micropapillary pattern, appears torepresent an unfavorable prognosticfinding {1335,1484,1825}.Histologic parameters that correlate withunfavourable prognosis include high his-tologic grade and vascular invasion{391}. Also considered promising, asunfavourable prognostic indicators areincreased mitotic activity, relatively fewtumour infiltrating lymphoid cells, andextensive tumour necrosis {391,1934}.Histologic assessment that relates tostage (pleural invasion, evaluation ofresection margins, assessment of sam-pled lymph nodes, search for intrapul-monary metastases) are all importantand should be carefully evaluated ineach case. The diagnosis of bronchioloalveolar ade-nocarcinoma (BAC) is restricted to casesshowing no pleural, vascular, or stromalinvasion. In some series this applies toup to 20% of resected adenocarcinomas{1993}. The 5-year survival for localizedresected BAC is 100% {1484,1929,1993,2208} Recent studies {1929,1993,2208}suggest that adenocarcinomas with apredominant BAC pattern and centralscarring less than 0.5 cm in tumours of 3cm or less in diameter or p-T1 tumors,(regardless of the issue of invasion) havea similar, very favourable prognosis. Upto 30% of resected adenocarcinomasmay be in this category {1993}.In a study by Maeshima et al small ade-nocarcinomas (less than 2.0 cm) show-ing a bronchioloalveolar pattern without acentral desmoplastic reaction showed100% survival at ten years. The prognos-tic effect of the stromal reaction in smalladenocarcinomas is important. Caseswith central scars less than 0.5 cm indiameter (even if stromal invasion is
present in this focus) have a veryfavourable prognosis {1222,1929,1993,2208}.These data, the radiologic studies above{1038,1039,1952,2112,2192}, and otherrecent studies {912} suggest that limitedresection (eg. wedge resection) may bereasonable for small (< 2 cm., with goodCT correlation, and entirely sectionedhistologically) noninvasive peripheraltumours lacking active central fibrosis.Additional prospective confirmatorystudies are necessary. This approachwould render the distinction betweenAAH and BAC less critical for smalllesions that have been entirely removed.Ishiwa et al. {912} showed that 13 of 54patients (24%) with adenocarcinomas <2cm. lacking fibroblastic proliferation andinvasion (BAC) had no lymph nodemetastases on routine sectioning andwith cytokeratin staining looking formicrometastases.Bronchioloalveolar differentiation andnever-smoking history predicts sensitivityto IRESSA in advanced non-small celllung carcinoma {1321}.
Genetic predictive factors There are no universally accepted genet-ic factors predictive of prognosis thathave become part of routine clinicalpractice at the present time. Some prom-
ising preliminary studies have appeared.K-ras oncogene activation by point muta-tion correlates with poor survival and isalso associated with the effect ofchemotherapy at advanced stage{1670}. Another important prognosticfactor is p53 gene mutation. The nega-tive prognostic effect of p53 alteration ishighly significant especially in adenocar-cinoma both at the protein and DNA level{1331}. Also predictive of poor survival isthe overexpression of p185neu (c-erbB2oncogene-encoded protein) {1451}.Mutations in the EGFR gene have beenfound in patients who respond to the inhi-bor of the EGFR signaling pathway IRES-SA (gefinitib) {1217,1530}. Testing 3 molecular markers — c-Ki-ras,p53, and c-erbB2 – appears to improvethe estimation of prognosis {1767}. Inaddition to these gene alterations, prog-nostic significance has been reported inmany genes, although this is still contro-versial. For example, while expression ofp21WAF1 is associated with favourableprognosis, expressions of cyclin D andbcl-2, and inactivation of retinoblastomaand p16 genes are associated with poorprognosis {589,1012,1479,2092}Several studies using gene expressionprofiling have begun to identify prognos-tically significant subsets of lung adeno-carcinoma {163,661,715}.Loss of heterozygosity at chromosomes2q, 9p, 18q, and 22q occurs frequently inadvanced non-small cell lung carcinoma(NSCLC) plays an important role in theprogression of NSCLC and predicts poorsurvival {1813}. Although reports of func-tional losses of the repair genes in ade-nocarcinoma have been infrequent, therehave been reports that allelic imbalancesat 9p and 22q with p53 alteration correlates with shortened survival {2011}.
Fig. 1.36 Kaplan-Meier curves of lung adenocarci-noma subgroups based on cDNA microarray geneexpression profiling. Group 3 carcinomas with theworst prognosis shared with large cell carcinomasthe expression of genes involved in tissue remod-eling. Reproduced from Garber et al. 2001 {661}.

45Large cell carcinoma
Definition
Large cell carcinoma is an undifferentiat-ed non-small cell carcinoma that lacksthe cytologic and architectural featuresof small cell carcinoma and glandular orsquamous differentiation.
ICD-O codes
Large cell carcinoma 8012/3
Large cell neuro-endocrine carcinoma 8013/3Combined large cell neuro-endocrine carcinoma 8013/3Basaloid carcinoma 8123/3Lymphoepithelioma-like carcinoma 8082/3Clear cell carcinoma 8310/3Large cell carcinoma with rhabdoid phenotype 8014/3
Synonyms
Large cell carcinoma has previouslybeen called large cell anaplastic carci-noma and large cell undifferentiated car-cinoma. Before the description of largecell neuroendocrine carcinoma termssuch as large cell neuroendocrinetumour {769}, neuroendocrine carcinomawith intermediate differentiation {2109},atypical endocrine tumour of the lung{1283}, and large cell carcinoma of thelung with neuroendocrine differentiation{2135} were used for tumours that wenow call large cell carcinoma with neu-roendocrine differentiation. LCNEC wasdescribed in 1991 {2026}; basaloid car-
cinoma was described in 1992 {216} andboth tumours were recognized as distinctclinicopathological entities by the WHOin the 1999 classification {2024}.
Epidemiology
Large cell carcinoma accounts forapproximately 9% of all lung cancers{2029} in most studies {916,1957}. Largecell neureoendocrine carcinomaaccounts for about 3% of lung cancer{916}. All types predominate in smokers,except lymphoepithelioma-like carcino-ma. Average age at diagnosis is about60 and most patients are male {216,916,1390,2026}. Lymphoepithelioma-like car-cinoma (LELC) is a very rare tumour, butrepresents 1% of lung tumours in China,affects younger, mostly female patients(mean age 57) and only 40% are smok-ers {324,331,340,770,771,2168}.
Clinical features
Signs and symptoms Symptoms are common with those ofother NSCLC. Most tumours are periph-eral except basaloid carcinoma. Ectopichormone production is uncommon inLCNEC {475}.
Relevant diagnostic procedures Large cell carcinomas have no particulardistinguishing radiological features. Theappearance depends on the site of thetumour {614}. Large cell carcinomas,except basaloid carcinoma, occur pref-
erentially in the lung periphery, so thattumours may be accessible by transtho-racic fine needle aspiration biopsy aswell at bronchoscopy. Specific diagnosisof LCC and variants can only be reliablyachieved on surgical material.
Cytology
Most cases of LCC do not have specificdiscriminating cytologic features. Mostcytologic samples show cellular aggre-gates; less often cells are dispersed.Cellular borders are indistinct so syncytiaform haphazardly {673,936,1826}. Nucleivary from round to extremely irregular{255} with irregular chromatin distribu-tion. Nucleoli are generally very promi-nent. Cytoplasm is basophilic, usuallyscant with a high nuclear-to-cytoplasmic(N/C) ratio. LCNEC shows neuroendocrine features(nuclear palisading and molding), butare distinguished from SCLC by the presence of prominent nucleoli and
Large cell carcinoma E. BrambillaB. PugatchK. GeisingerA. GalM.N. SheppardD.G. GuineeS.X. Jiang
S. LantuejoulY.L. ChangI. Petersen
M. MeyersonS.M. HanashM. Noguchi
BAFig. 1.37 A Peripheral LCC with cream-white foci of necrosis, central scar and anthracotic pigmentation.The periphery shows a homogeneous grey cut surface. B Large tumour cells have abundant cytoplasm withlarge nuclei, vesicular nuclear chromatin and prominent nucleoli. No glandular or squamous differencia-tion. From Travis et al. {2024}.
Fig. 1.38 Large cell carcinoma. In this bronchialbrushing specimen, a loose syncytial aggregate ofobviously malignant cells is present. The nucleihave thick very irregular membranes, coarselygranular and dark chromatin, and prominent andirregular nucleoli. No evidence of specific differen-tiation is apparent. Papanicolaou stain.

46 Tumours of the lung - Malignant epithelial tumours
nuclei larger than 3 times the diameter ofa small resting lymphocyte. {2132,2197}.Basaloid carcinoma in smears consistsof both individual tumour cells and cohe-sive aggregates. Well developed nuclearpalisading can be discerned at theperiphery of some cellular aggregates.Lymphoepithelioma-like carcinomasshow cohesive flat syncytia {364}.Spindle-shaped tumour cells have soli-tary large nuclei with huge nucleoli, inti-mately admixed with numerous smalllymphocytes.
Macroscopy and localization
Large cell carcinomas typically presentas large, peripheral masses, frequentlyidentified on chest radiographs, but
which may also involve subsegmental orlarge bronchi. The tumour often invadesvisceral pleura, chest wall, or adjacentstructures. Sectioning reveals a soft,pink-tan tumour with frequent necrosis,occasional hemorrhage and rarely, cavi-tation.Large cell neuroendocrine carcinomasare often peripheral. In contrast basaloidcarcinomas characteristically show exo-phytic bronchial growth {216}.
Tumour spread and staging
The pattern of spread of large cell carci-noma is similar to other non-small celllung carcinomas. Metastases occur mostfrequently to hilar or mediastinal nodesfollowed by metastases to the pleura,
liver, bone, brain, abdominal lymphnodes and pericardium {1875}.Micrometastases detected in hilar nodeshave no significant impact on prognosisin otherwise stage I tumours {703}.Specific subtypes of large cell carcino-ma differ in their pattern of spread,response to therapy and ultimate prog-nosis. Large cell neuroendocrine carci-noma {916,1272,1957,2028} combinedlarge cell neuroendocrine carcinoma{1709}, large cell carcinoma with rhab-doid phenotype {304,350,1803} andbasaloid carcinoma {216,1390} have aworse prognosis than classic large cellcarcinoma. Recent studies have report-
Fig. 1.39 Large cell neuroendocrine carcinoma. A Note numerous rosettes. B Palisading at the peripheryof the nests of tumour cells and rosettes can been seen. Necrosis is present and mitoses are numerousFrom Travis et al. {2024}. C High magnification shows details of rosettes and nuclei with vesicular chro-matin. D Palisading and rosette-like formations. Numerous mitoses. The nuclear chromatin is vesicular andmany cells have prominent nucleoli. From Travis et al. {2024}.
DC
A B
B CAFig. 1.41 Large cell neuroendocrine carcinoma. A Chromogranin immunostaining shows a granular cytoplasmic pattern. B NCAM (CD56) immunostaining with typ-ical membrane pattern. C TTF1 (thyroid transcription factor one) immunoreactivity with a typical nuclear pattern.
Fig. 1.40 A Ultrastructural aspect of neuroen-docrine cells in a large cell neuroendocrine carci-noma. Numerous dense core neurosecretory gran-ules are present in the cytoplasm. B Ultrastructuralfeatures in a combined large neuroendocrine car-cinoma showing within the same cell acinus for-mation with apical microvilli and typical neurose-cretory granules.
A
B

47Large cell carcinoma
ed both a better prognosis and betterresponse by lymphoepithelial like carci-noma to both chemotherapy and radia-tion therapy {302,324,331,340,770}. Theclinical behavior of clear cell carcinomais similar to typical large cell carcinomas{971}.Stage distribution for LCC at diagnosis isas seen in other NSCLC. Large cell neu-roendocrine carcinomas are often stageIII-IV at diagnosis. Basaloid carcinoma isfrequently operable at presentation butprognosis is worse than that of otherNSCLC and brain metastases are morefrequent {1390}.
Histopathology
Large cell carcinomasThese are, by definition, poorly differenti-ated tumours. It is a diagnosis of exclu-sion made after ruling out the presenceof a component of squamous cell carci-noma, adenocarcinoma or small cell car-cinoma. They consist of sheets or nestsof large polygonal cells with vesicularnuclei with prominent nucleoli, and amoderate amount of cytoplasm.Ultrastructurally minimal squamous orglandular differentiation is common.
Large cell neuroendocrine carcinomaLarge cell neuroendocrine carcinoma(LCNEC) shows histological featuressuch as organoid nesting, trabeculargrowth, rosettes and perilobular palisad-ing patterns, suggesting neuroendocrinedifferentiation {2024,2026} The tumourcells are generally large, with moderate
to abundant cytoplasm. Nucleoli are fre-quent, prominent and their presencefacilitates separation from small cell car-cinoma. Mitotic counts are typically 11 ormore (average 75) per 2 mm2 of viabletumour. Large zones of necrosis arecommon. Confirmation of neuroen-docrine differentiation is required usingimmunohistochemical markers such aschromogranin, synaptophysin andNCAM (CD56) {1128}. One positivemarker is enough if the staining isclearcut. Around 50% of LCNEC expressTTF-1 {1216,1892,1894}, but expressionof CK 1, 5, 10, 14, 20 (34ßE12) is uncom-mon {1892,1893}.
Combined large cell neuroendocrine car-cinomaA large cell neuroendocrine carcinomawith components of adenocarcinoma,squamous cell carcinoma, giant cell car-cinoma and/or spindle cell carcinoma.Like small cell carcinoma, a small per-centage of large cell neuroendocrinecarcinomas are histologically heteroge-neous. In view of the many shared clini-cal, epidemiologic, survival, and neu-roendocrine properties between largecell neuroendocrine carcinoma andsmall cell carcinoma, we have arbitrarilychosen to classify these tumours as combined large cell neuroendocrine car-
Fig. 1.43 Combined large neuroendocrine carcinoma. A NCAM (CD56) immunostaining in the large cell neuroendocrine component. Note the typical cell membranepattern. B Combined large neuroendocrine carcinoma associated with an adenocarcinoma. The large neuroendocrine carcinoma is immunostained with chromo-granin antibody.
BA
Fig. 1.42 This large cell neuroendocrine carcinoma is combined with an acinar adenocarcinoma. FromTravis et al. {2024}.

48 Tumours of the lung - Malignant epithelial tumours
cinoma until future studies better definetheir biologic behavior. Combinationswith small cell carcinoma also occur, butsuch tumours are classified as combinedvariants of small cell carcinoma.
Basaloid carcinomaThis tumour shows a solid nodular oranastomotic trabecular invasive growthpattern, with peripheral palisading.Tumour cells are relatively small,monomorphic, cuboidal fusiform, withmoderately hyperchromatic nuclei, finelygranular chromatin and absent or focalnucleoli. Cytoplasm is scant but nuclearmolding is absent. Mitotic rate is high(15-50 per 2 mm2). Squamous differenti-ation is absent. Most basaloid carcinomahave hyalin or mucoid degeneration inthe stroma. Frequent small cystic spacesare seen. Comedo type necrosis is com-mon. Rosettes are seen in one third ofcases. Immunohistochemical stains forneuroendocrine markers are geneallynegative. In 10% of cases, one neuroen-docrine marker may be positive in lessthan 20% of tumour cells. Cytokeratin
expression is as seen in NSCLC, andincludes CK 1, 5, 10, and 14 (34ßE12),markers. Basaloid carcinoma does notexpress TTF-1 {1892}.
Lymphoepithelioma-like carcinoma Pulmonary lymphoepithelial-like carcino-ma is characterized by a syncytialgrowth pattern, large vesicular nuclei,prominent eosinophilic nucleoli, andheavy lymphocytic infiltration {302,324,331,340,770} It has predominantly push-ing border, infiltrating in the form of dif-fuse sheets. The prominent lymphoidreaction consists of mature lymphocytesoften admixed with plasma cells and his-tiocytes with occasional neutrophils oreosinophils. The lymphoid component isseen even in metastatic sites. In rarecases, there is intratumoural amyloiddeposition. EBER-1 RNA is present in thenuclei of the large undifferentiated neo-plastic cells.
Clear cell carcinoma Clear cell carcinomas have large polygo-nal tumours cells with water-clear or
foamy cytoplasm. Tumour cells may ormay not contain glycogen.
Large cell carcinoma with rhabdoidphenotype In large cell carcinoma with rhabdoidphenotype, at least 10% of the tumourcell population must consist of rhabdoidcells, characterized by eosinophilic cyto-plasmic globules {304}, consisting ofintermediate filaments, which may bepositive for vimentin and cytokeratin{304,1803}. Pure large cell carcinomaswith a rhabdoid phenotype are very rare.Small foci of adenocarcinoma {1803},and positive neuroendocrine markersmay be seen. Ultrastruscturally theeosinophilic inclusions are composed ofaggregates of large intra cytoplasmicparanuclear intermediate filaments. Cellswith rhabdoid features may be seenfocally in other poorly differentiatedNSCLC.
Differential diagnosis
The differential diagnosis of large cellcarcinoma (NOS) includes poorly differ-entiated squamous cell carcinoma inwhich foci of keratinization and/or inter-cellular bridges are present and solidtype adenocarcinoma, where a minimumof 5 mucinous droplets are present in atleast 2 high power fields. The major dif-ferential diagnosis for LCNEC is atypicalcarcinoids (AC) and basaloid carcinoma.LCNEC is distinguished from atypicalcarcinoid primarily by a higher mitoticindex (11 or more per 2mm2) and usuallymore extensive necrosis. Differentialdiagnosis between LCNEC and basaloidcarcinoma is more difficult on H&E mor-phology alone and is usually achievedusing neuroendocrine markers, sinceboth tumours disclose palisading andone third of basaloid carcinoma showrosettes. Cytokeratins 1, 5, 10, 14 are
B CAFig. 1.45 Basaloid carcinoma. A Palisading is conspicuous at the periphery of the nests of tumour cells which are hyperchromatic, with relatively scant cytoplasm{2024}. B Lobular pattern with peripheral palisading, comedo type necrosis and some rosettes. C 34ßE12 immunostaining for cytokeratins 1, 5, 10, 14.
Fig. 1.44 Basaloid carcinoma at high magnification showing peripheral palisading and monomorphic cellswith dense chromatin and unconspicuous nucleoli.

expressed (34ßE12) in other NSCLC butare typically negative in LCNEC{1892,1893}. Basaloid carcinoma mustbe distinguished from poorly differentiat-ed squamous carcinoma. Although ini-tially described with 2 forms, one pureand one mixed, the latter is now consid-ered as the basaloid variant of squamouscell carcinoma. Occurrence of even focalsquamous differentiation favors the diag-nosis of basaloid variant of squamouscarcinoma. Small cell carcinoma entersthe differential diagnosis of basaloid car-cinoma due to their small cell size andhigh mitotic rate, but nuclear to cytoplas-mic ratio is higher in SCLC and nuclearchromatin is vesicular rather than finelygranular.The prominent inflammatory cell infiltrate,which characterises lymphoepithelioma-like carcinoma, may lead to considera-
tion of inflammatory pseudotumour,malignant lymphoma {1262}, or primarylymphoid hyperplasia of the lung. Apanel of immunohistochemical stainsallows recognition of the malignantepithelial cells, characteristically patchyin distribution, as well as CD8+ expres-sion by the lymphocytic infiltrate.Clear cell carcinoma of the lung resem-bles metastatic clear cell carcinomasarising in organs such as the kidney, thy-roid and salivary gland. If squamous orglandular differentiation is seen, thetumour is classified as a clear cell variantof squamous cell or adenocarcinoma,respectively.
Precursor lesions
There is no precursor lesion identified forlarge cell carcinoma except for basaloidcarcinoma. Adjacent squamous dyspla-
sia in one third of basaloid carcinoma,their pattern of infiltration, and both theirimmunophenotype and ultrastructurecharacteristic of bronchial reserve cells{216,222,1281}, supports an origin frombronchial preneoplastic lesions. Lympho-epithelioma-like carcinoma is charac-terised by the presence of EBV viralsequences, reflecting viral (EBER1)dependent transformation of lung epithe-lial cells.
Histogenesis
These tumours originate from a commonpluripotent progenitor cell capable ofmultidirectional differentiation {1282,2024}. Neuroendocrine differentiation inLCNEC does not imply origin from a spe-cific neuroendocrine cell. In contrast tocarcinoid tumours, LCNEC is not associ-ated with diffuse neuroendocrine hyper-
49Large cell carcinoma
Fig. 1.46 Lymphoepithelioma-like carcinoma. A Large tumour cells intermixed with a lymphoid infiltrate. Note the abundant cytoplasm, vesicular chromatin andprominent nucleoli. From Travis et al. {2024}. B Epstein-Barr virus-encoded small RNA (EBER RNA) expression in the nuclei of large undifferentiated neoplastic cellsbut not in the surrounding lymphocytic infiltrate. In situ hybridization.
BA
Fig. 1.47 A Rhabdoid type large cell carcinoma. Tumour cells have large globular eosinophilic cytoplasmic inclusions. The nuclear chromatin is vesicular and nucle-oli are prominent. From Travis et al. {2024}. B Clear cell carcinoma with numerous tumour cells showing clear cytoplasm.
BA

50 Tumours of the lung - Malignant epithelial tumours
plasia, tumourlets or MEN1 mutations{464} Cells of basaloid carcinoma dis-play the immunohistochemical and ultra-structural phenotype of reserve supra-basal bronchial cells. {216,222, 1281}Clear cell and rhabdoid variants of LCCprobably reflectf the pluripotent capacityof the LC progenitor cell.
Somatic genetics
Cytogenetics and CGH Large cell carcinoma of the lung is most-ly an aneuploid neoplasm with the high-est mean chromosome number and DNAcontent of all lung cancer types being inthe near triploid range or above {1581}.Accordingly, the karyotypes are complexand indicate a high chromosomal insta-bility {1330} of which the major biologicaleffect is probably the generation of DNAcopy number changes. The CGH patternof classical, non-neuroendocrine largecell carcinoma shows similarities to lungadenocarcinoma and squamous cell car-cinoma like overrepresentations on 1qand 3q {178,898}. In particular, thetumours harbour imbalances that havebeen associated with progression andmetastasis formation, e.g. amplificationsof 1q21-q22, 8q and deletion of 3p12-p14, 4p, 8p22-p23, 21q. Large cell neu-roendocrine carcinoma may carry verysimilar chromosomal imbalances assmall cell lung carcinoma {898,2051,2052}.
Molecular geneticsLarge cell carcinomas share the molecu-lar and genetic alterations commonlyseen in NSCLC, since it is a poorly differ-entiated tumour issued from the samestem cells, exposed to the same carcino-gens. K-ras mutations, P53 mutationsand Rb pathway alteration (loss ofP16INK4, hyperexpression of cyclin D1or E) occurs with the same frequency asin other NSCLC. Large cell neuroen-docrine carcinomas have P53 and Rbmutational patterns in addition to inacti-vation pathways similar to SCLC {212,215,217,1516,1622}: a high frequency ofP53 mutation, of bcl2 overexpression,lack of bax expression {217}, high telom-erase activity, but lower frequency of Rb/ P14ARF loss of protein, and of E2F1overexpression than SCLC {549,550}.They display a low frequency of P16 loss,cyclin D1 and cyclin E overexpression,and lack MEN1 mutation and allelic dele-tion. Fas is downregulated but its ligandFasL is strongly upregulated {2083}.
Prognosis and predictive factors
Clinical criteria Clinical prognostic criteria are not differ-ent from other NSCLC. The major criteri-on is performance status at diagnosisand the disease extension reflected bythe TNM and stage. Although most basa-loid carcinomas present as stage I-IItumours, they bear a dismal prognosis in
contrast with lymphoepithelioma-like car-cinoma, which present at extendedstage but have better prognosis thanNSCLC. A direct correlation betweenlarger tumour size and high stage andtitre of EBV serology has been demon-strated in lymphoepithelioma-like carci-noma {331}. There is no significant differ-ence in the prognosis between LCNECand SCLC after stratification by stage.There is a significantly shorter survival forstage I LCNEC as compared with stage INSCLC {1957} and stage I large cell car-cinoma {916}. The outcome of carefullystaged LCNEC may be better than prre-vious studies have indicated {2229}.
Histopathological criteria It is controversial whether the presenceof neuroendocrine differentiation demon-strated by immunohistochemistry hasany prognostic signficance in NSCLC(NSCLC-NED). Some studies indicate aworse prognosis {841,916,1566}, othersa better prognosis {289,1759} and othersshow no difference in survival {651,1833,1905}. In addition studies have suggest-ed NSCLC-NED have a better prognosis{735} or no difference in response tochemotherapy {1448}.
Genetic predictive factors The genetic predictive factors of largecell carcinoma should correspond tothose of general primary lung carcinoma.However, one variant of large cell carci-noma – large cell neuroendocrine carci-noma (LCNEC) – has specific geneticcharacters similar to SCLC: allelic lossesof 3p21, FHIT, 3p22-24, 5q21, 9p21, andthe RB gene. All of these markers corre-late with poor prognosis in neuroen-docrine carcinoma including LCNEC.Both p53 gene loss and point mutationalso correlate with poor survival {1516}.
Fig. 1.48 DNA copy number changes in 18 classical (non-neuroendocrine) large cell carcinomas detectedby CGH. Areas on the left side of the chromosome ideogram reflect loss of genetic material, those on theright side to DNA gains. DNA changes with 99% significance are coloured in blue, additional changes with95% significance are depicted in green. The proportion of pronounced DNA imbalances are visualised inred; they typically represent high copy amplifications or multiple copy deletions.

51Adenosquamous carcinoma
Definition
A carcinoma showing components ofboth squamous cell carcinoma and ade-nocarcinoma with each comprising atleast 10% of the tumour.
ICD-O Code 8560/3
Clinical features
Signs and symptoms The frequency of adenosquamous carci-noma is between 0,4-4% of lung carcino-mas {586,909,1445,1867,1950,2203}.Their incidence might be rising parallel tothe increase of adenocarcinoma {1868}.The majority of patients are smokers.Clinical presentation and behavior is sim-ilar to adenocarcinoma.
Imaging and relevant diagnostic proce-dures Since most tumours are peripheral theirdiagnosis can be assessed by bron-choscopy in segmental or subsegmentalbronchi, or by transthoracic needle biop-sy. However their recognition is samplingdependent, the likelihood of identifyingboth components in small samples issmall, and diagnosis is more definitive onsurgical samples. Radiographic featuresare not different from those of non-smallcell carcinoma; peripheral tumours mayshow central scarring and indentation orpuckering of the overlying pleura. Somemay display a rim of ground glass opa-city.
Macroscopy and localization
Adenosquamous carcinomas are usuallylocated in the periphery of the lung andmay contain a central scar. They aregrossly similar to other non-small cellcarcinomas.
Tumour spread and staging
Metastases usually show the same com-bination of squamous and glandular dif-ferentiation as the primary. The spread ofadenosquamous carcinoma is similar toother non-small cell carcinomas. Theyshow early metastases and a poor prog-nosis {84}.
Histopathology
As there is a continuum of histologicalheterogeneity with both squamous celland adenocarcinoma, the criterion of10% for each component is arbitrary.Since some squamous cell carcinomasshow focal mucin on histochemicalstains the adenocarcinoma component ismore easily defined if it shows an acinar,papillary or bronchioloalveolar pattern.Well-defined squamous cell carcinomaand adenocarcinoma are evident on lightmicroscopy, the squamous cell carcino-ma showing unequivocal keratin or intra-cellular bridges and the adenocarcinomashowing acini, tubules or papillary struc-tures. The diagnosis of an adenocarcino-ma component is difficult if it is confinedto a solid pattern with mucin formation.More than 5 mucin droplets per highpower field are then required for a diag-nosis of adenocarcinoma. The two com-ponents may be separate or may mergeand mingle. The squamous or the glan-dular component may be predominant ormay be seen in equal proportion. Thedegree of differentiation of each compo-nent is not interdependent and is vari-
able. A component of large cell carcino-ma may be present in addition to the 2other components but does not changethe diagnosis. The same stromal featureswith or without inflammation occur as inother non-small cell lung carcinomas.Cases with amyloid-like stroma havebeen described {2217}, as seen in sali-vary gland type neoplasms.Ultrastructural features are those ofsquamous carcinoma and adenocarci-noma. By electron microscopy featuresof both cell types are common buttumour classification is based on lightmicroscopy. Immunohistochemical find-ings also recapitulate both squamousand adenocarcinoma characteristics.They express cytokeratins with a widemolecular weight range includingAE1/AE3, CAM 5.2, KL1, and CK7 butusually not CK20. EMA is positive andTTF-1 positivity is confined to the adeno-carcinoma component.
Differential diagnosis
The differential diagnosis includesentrapment of alveolar or bronchiolar aci-nar structures within a squamous cell
Adenosquamous carcinoma E. BrambillaW.D. Travis
Fig. 1.49 Adenosquamous carcinoma. The tumour consists of squamous cell carcinoma (left) and papillaryadenocarcinoma (right). From Travis et al. {2024}.

52 Tumours of the lung - Malignant epithelial tumours
carcinoma. This should not be mistakenfor glandular differentiation of the cancer.Similarly, adenocarcinoma may be asso-ciated with squamous metaplasia ofentrapped bronchiolar structures.Mucoepidermoid carcinoma enters thedifferential diagnosis. Arising frombronchial glands, low-grade mucoepi-dermoid carcinoma are centrally locatedand show histologic features identical totheir salivary gland counterpart, with mix-ture of mucinous glands, intermediate orsquamoid cells, with no or mild atypia.High grade mucoepidermoid carcinomais more difficult to differentiate fromadenosquamous carcinoma. In favour ofmucoepidermoid carcinoma is the char-acteristic admixture of mucinous andsquamoid cells, a proximal exophyticendobronchial location, areas of classiclow grade mucoepidermoid carcinoma,absence of keratinisation or squamouspearl formation without overlying in situsquamous cell carcinoma {2217,2221},or tubular, acinar, and papillary growthpattern. These two lung tumours cannotbe distinguished reliably in all cases{1348}.
Histogenesis
The cell of origin is believed to be apluripotential bronchial reserve cell. Ithas been proposed that adenocarcino-mas according to their central (bronchial)or peripheral (alveolar parenchyma)location arise from two distant stem cells,bronchial epithelial and Clara cell typerespectively {402} with different mutation-al patterns. Since most adenocarcino-mas have mixed patterns combiningboth central (acinar, solid) and peripher-al (bronchioloalveolar, papillary) adeno-carcinoma patterns, it is likely they origi-nate, like adenosquamous carcinoma,from a common intermediate bronchial-Clara type II cell type.
Somatic genetics
There is no information specifically avail-able on adenosquamous carcinoma withregard to cytogenics and CGH, expres-sion profile and proteomics. The molecu-lar genetic alterations of each compo-nent are those characteristic of squa-mous and adenocarcinoma respectively.They may display Ras mutations similarto peripheral adenocarcinoma.
Prognosis and predictive factors
The histologic criteria for the diagnosis inthese studies vary, and should be kept inmind when comparing results. They havea poor prognosis with a 5-year survivalrate after resection of 62.5% for localizeddisease and 35% for resectable cases{909}. The prognosis is poorer than thatof stage I-II squamous carcinoma or ade-nocarcinoma, and this histological typewas shown to be an independent prog-nostic determinant at limited stage. The
SEER results report an overall 21% 5-year survival.
Genetic predictive factors There are no specific studies reported foradenosquamous carcinoma, althoughthey have been included in non-smallcell lung carcinomas. Ras and P53 muta-tions might be an unfavorable prognosticfactor in stage I tumours.
Fig. 1.50 Adenosquamous carcinoma showing a squamous cell lobule on the left, adjacent to an acinar ade-nocarcinoma on the right.

53Sarcomatoid carcinoma
Definition
Sarcomatoid carcinomas are a group ofpoorly differentiated non-small cell lungcarcinomas that contain a component ofsarcoma or sarcoma-like (spindle and/orgiant cell) differentiation. Five subgroupsrepresenting a morphologic continuumare currently recognized: Pleomorphiccarcinoma:, spindle cell carcinoma, giantcell carcinoma, carcinosarcoma and pul-monary blastoma.
ICD-O codes
Pleomorphic carcinoma 8022/3Spindle cell carcinoma 8032/3Giant cell carcinoma 8031/3Carcinosarcoma 8980/3Pulmonary blastoma 8972/3
Synonyms
An alternative classification recognizingmonophasic and biphasic varieties withthe latter further classified as homolo-gous or heterologous {2138} is not cur-rently recommended.
Epidemiology
These tumours are rare, accounting forapproximately only 0.3-1.3% of all lungmalignancies {584,1430,1695,2023,2029}.The average age at diagnosis is 60 years,and the male to female ratio is almost 4 to1 {218,330,337,443,1440, 1857}. Biphasicblastomas are exceptional in that theyafflict men and women equally with anaverage age in the fourth decade{1064,1665}.
Etiology
The factors implicated in the etiology ofsarcomatoid carcinomas are similar tothose involved in conventional histo-types. Tobacco smoking is the major fac-tor; more than 90% of patients with pleo-morphic carcinoma are heavy cigarettesmokers {443,584,1430,1440,2029}.Some cases may be related to asbestosexposure {557,584}.
Localization
Sarcomatoid carcinomas can arise in thecentral or peripheral lung. A predilection
for the upper lobes has been reported{443,584,1430,1695}. Pleomorphic carci-nomas are often large peripheraltumours with a tendency to invade thechest wall {584}.
Clinical features
Signs and symptoms Signs and symptoms are related totumour localization {443,584,1430,1440,1695,1857}. Since central endobronchialtumours tend to protrude into the luminaof large airways, patients often presentwith cough, haemoptysis, and progres-sive dyspnoea or fever due to recurrentpneumonia. Peripheral tumours, espe-cially pleomorphic carcinoma, grow tolarge sizes and often present with chestpain due to pleural or chest wall invasion.
Relevant diagnostic procedures Due to sampling issues and histologicheterogeneity the diagnosis of virtually all
sarcomatoid carcinomas requires a sur-gical specimen. Based on cytology or asmall biopsy specimens one might rarelysuspect a diagnosis of pleomorphic,spindle cell or giant cell carcinoma, how-ever it would be impossible to make adefinitive diagnosis.
Cytology
Pleomorphic carcinoma consists ofmalignant giant and/or spindle cells andepithelial components such as squa-mous or adenocarcinoma in smears{582,878}. The spindle and/or giant cellsoccur as cohesive aggregates of tumourcell, generally lacking any glandular orsquamous differentiation. The neoplasticspindle cells are pleomorphic and elon-gated, singly or in loose clusters, bun-dles or tissue fragments. Nuclei are soli-tary, large and spindled, with prominentnucleoli. Nuclear-to-cytoplasmic ratiosare high. Fragments of myxoid matrix
Sarcomatoid carcinoma B. CorrinY.L. ChangG. RossiM.N. KossK. Geisinger
M.R. WickO. Nappi
S.D. FinkelsteinY. Nakatani
Fig. 1.51 Pleomorphic and sarcomatous carcinoma. A Huge individual neoplastic cells some of which haveovoid nuclei and one or two tails of basophilic cytoplasm. Several cells are multinucleated. Note the abnor-mal mitotic figure. Cohesion is distinctly lacking (Diff-Quik stain). B Solitary, huge multinucleated tumourgiant cell in an aspiration biopsy of a giant cell carcinoma. The cell has multiple fused nuclei with coarsechromatin and distinct nucleoli (Diff-Quik stain).
BA

54 Tumours of the lung - Malignant epithelial tumours
material may also be identified, as maymalignant tumour giant cells. Both celltypes are usually positive for cytokeratinsin cell blocks.Spindle cell carcinoma features malig-nant spindle cells with nuclear hyper-chromasia and irregular, distinct nucleoli.Cohesion is generally better preservedthan with true sarcomas, but isolatedspindled epithelial cells may also beseen.Giant cell carcinoma is cellular in cyto-logical preparations and is characterizedby a marked lack of intercellular cohe-sion {420,1489}. Accordingly, numerousindividual multinucleated neoplasticgiant cells are present. The nuclei varyfrom round and smooth to highly irregularwith large nucleoli, which are often multi-ple, and coarse darkly stained chromatingranules. Cytoplasm may be abundant inthese cells. Another characteristic fea-ture is the smear background, whichincludes granular necrotic material and
neutrophil leukocytes. Neutrophilemperipolesis is also characteristic.When the malignant epithelial compo-nent is not evident within the smears, itcould be difficult or impossible to distin-guish a spindle cell or a giant cell carci-noma from a primary or metastatic spin-dle cell or pleomorphic sarcoma, respec-tively, based solely on cytomorphology{626,2182}. Here, immunocytochemistryperformed on the smears or cell blocks,or obtaining an additional sample maybe helpful.In carcinosarcoma, and blastoma thecytologic smears contain heterologoussarcomatous elements, such as malig-nant cartilage, bone, or skeletal muscle,in addition to obvious carcinoma.
Macroscopy
Peripheral tumours are usually greaterthan 5 cm, well circumscribed and fea-ture grey, yellow or tan creamy, gritty,mucoid and/or hemorrhagic cut surfaces
with significant necrosis. Sessile orpedunculated endobronchial tumoursare smaller and often infiltrate underlyinglung parenchyma {265,584,1213,1430,1440,1442,1695}. Peripheral pulmonaryblastomas are significantly larger thanmost NSCLC with a mean diameter of 10cm.
Tumour spread and staging
These very aggressive tumours metasta-size widely to the same sites as NSCLC,including unusual sites such as theesophagus, jejunum, rectum and kidney{154,265,330,584,1430}. Peripheraltumours usually present at a moreadvanced stage than central lesions. Ingeneral, stage at diagnosis is similar tothat reported for the other non-small celllung cancers {443,584,1213,1430,1440,1695}.
DC
BA
Fig. 1.52 A Pleomorphic carcinoma. Biphasic tumour with a clear-cut non-small cell carcinomatous component closely intermingled with a spindle cell carcino-matous component. B Mixed spindle cell carcinoma (SCC) and giant cell carcinoma (GCC). C Pleomorphic carcinoma consisting of a squamous cell carcinomawith a spindle cell component. D Pleomorphic carcinoma consisting of a mucinous adenocarcinoma (left) and spindle cell carcinoma (right). From Travis et al {2024}.

55Sarcomatoid carcinoma
Histopathology
Pleomorphic carcinomaA poorly differentiated non-small cell car-cinoma, namely squamous cell carcino-ma, adenocarcinoma or large cell carci-noma containing spindle cells and/orgiant cells or, a carcinoma consistingonly of spindle and giant cells. The spin-dle or giant cell component should com-prise at least 10% of the tumour andwhile the presence of adenocarcinomaor squamous cell carcinoma should bedocumented, foci of large cell carcinomaneed not be mentioned.Histologic sections demonstrate conven-tional non-small cell carcinoma, namelyadeno-, squamous cell or large cell sub-types, intimately associated with at least10% malignant spindle cells and/or giantcells. Mitotically active spindle cellsarranged haphazardly in a fascicular orstoriform growth pattern have varyingmorphologic appearances ranging fromepithelioid to mesenchymal sometimeswith occasional smooth muscle features.
The stroma may be fibrous or myxoid.Dyscohesive malignant giant cells arepolygonal, uni- or multinucleated, andhave dense eosinophilic cytoplasm andpleomorphic nuclei. Emperipolesis isoften present and large vessel invasionalong with extensive necrosis are com-monly seen. Rarely squamous cell carci-nomas have an angiosarcomatoid com-ponent that has been called pseudoan-giosarcomatous carcinoma. This is char-acterized by anastomosing channelslined by anaplastic, epithelioid cellsfocally aggregated in pseudopapillaeand forming spaces filled with erythro-cytes {1441,1442,1662}.
Spindle cell carcinoma This variant is defined as a non-small cellcarcinoma consisting of only spindle-shaped tumour cells. Identical to thespindle cell component of pleomorphiccarcinoma, cohesive nests and irregularfascicles of overtly malignant cells fea-ture nuclear hyperchromasia and distinct
nucleoli. Specific patterns of adenocarci-noma, squamous cell, giant cell or largecell carcinoma are not seen. Scatteredand focally dense lymphoplasmacyticinfiltrates surround and percolatethrough the tumoural mass. Rare caseswith prominent inflammatory infiltratesmay resemble inflammatory myofibrob-lastic tumour.
Giant cell carcinomaA non-small cell carcinoma composed ofhighly pleomorphic multi- and/ormononucleated tumour giant cells.Identical to the giant cell component ofpleomorphic carcinoma, this tumour iscomposed entirely of giant cells anddoes not have specific patterns of eitheradenocarcinoma, squamous cell or largecell carcinoma. This tumour consists ofvery large, multinucleated and bizarrecells. Nuclei are pleomorphic, and oftenmultilobed. The tumour cells are disco-hesive and tend to dissociate from eachother {19,20,88,218,584,686,1695,2023,2024}. There is generally a rich inflam-matory infiltrate, usually of neutrophils,which frequently invade the tumour cells.This phenomenon was initially thought torepresent phagocytosis by the tumourcells, but more probably reflectsemperipolesis (active penetration of theleukocytes into the tumour cells) {934}.By electron microscopy, aggregates ofparanuclear filaments and tonofibrilsmay be observed both in spindle cell andgiant cell carcinomas {19,20,124,337,584,1440,1664,1909,2023}. In giant cell
BAFig. 1.53 Spindle cell carcinoma. Immunoreactivity for A TTF-1 and B cytokeratin 7.
Fig. 1.54 Giant cell carcinoma. Numerous, often multinucleated giant cells. Prominent infiltrate of neu-trophils, some of which permeate the tumour cell cytoplasm (emperipolesis). From Travis et al. {2024}.
Fig. 1.55 TTF-1 expression in giant cell carcinoma(GCC).

56 Tumours of the lung - Malignant epithelial tumours
carcinoma, only very occasional desmo-somes are seen.
CarcinosarcomaThis variant is defined as a malignanttumour with a mixture of carcinoma andsarcoma containing differentiated sarco-matous elements, such as malignant car-tilage, bone or skeletal muscle.The tumour is histologically biphasic,with a mixture of a conventional non-small cell lung carcinoma and true sar-coma containing differentiated elements.The carcinomatous component is mostoften squamous cell carcinoma (45-70%), followed by adenocarcinoma (20-31%), and large cell carcinoma (10%){1061}. An epithelial component resem-bling so-called high grade fetal adeno-carcinoma can occur in nearly 20% ofcases, but the blastematous stroma ofpulmonary blastoma is lacking {1061,1436}. The malignant stroma often formsthe bulk of carcinosarcomas, and onlysmall foci of carcinoma may be seen. Asignificant component of these sarcomasis often poorly differentiated “spindlecell” sarcoma, but a careful searchalways shows areas of more specific sar-comatous differentiation, most oftenrhabdomyosarcoma, followed by osteo-sarcoma or chondrosarcoma or combi-nations of osteosarcoma and chon-drosarcoma {1061}. More than one differ-entiated stromal component can be pres-ent. While metastatic foci usually featureboth epithelial and mesenchymal com-
ponents, lesions may contain only onepattern.
Pulmonary blastomaThis is a biphasic tumour containing aprimitive epithelial component that mayresemble well-differentiated fetal adeno-carcinoma and a primitive mesenchymalstroma, which occasionally has foci ofosteosarcoma, chondrosarcoma or rhab-domyosarcoma {2024}.Pulmonary blastoma shows histologicallya biphasic pattern with malignant glandgrowing in tubules that resemble fetalbronchioles, embedded in a sarcoma-tous embryonic-appearing mesenchyme{1857}. The glycogen-rich, non-ciliatedtubules and primitive stroma resemblethat seen in fetal lung between 10-16weeks gestation (the pseudoglandular
stage of lung development) {2225}. Thetubules can be well differentiated, resem-bling those reported in well-differentiatedfetal adenocarcinomas, but they are usu-ally less abundant. The tubules may alsoresemble a high-grade fetal adenocarci-noma. These tubules are lined by pseu-dostratified, non-ciliated columnar cellsthat have clear or lightly eosinophiliccytoplasm. The nuclei of the epithelialcells are oval or round and fairly uniform,but there can be cytologic atypia in theform of large multinucleated cells {2225}.The glands often have subnuclear orsupranuclear vacuoles, producing anendometrioid appearance. The cytoplas-mic vacuoles are due to abundant glyco-gen, readily demonstrated in periodicacid-Schiff stains. There may be smallamounts of mucin within the glandular
Fig. 1.57 Carcinosarcoma. The dilated bronchialtree is filled with a fleshy, cream-coloured masses.
Fig. 1.56 Giant cell carcinoma (GCC) with discohesive growth pattern.
Fig. 1.58 Carcinosarcoma. This tumour consists of malignant cartilage (top left) and squamous cell carcino-ma (bottom right). From Travis et al. {2024}.

57Sarcomatoid carcinoma
lumens, but intracellular mucin is unusu-al. Similar to fetal adenocarcinomas,morular structures consisting ofsquamoid nests may be seen {605,917,1064,1435,2225}.Stromal cells generally have a blastema-like configuration. There is condensationof small oval and spindle cells in a myx-oid stroma around neoplastic glands,similar to the appearance of Wilm’stumour of the kidney. Small foci of adult-type spindle cell sarcoma (most com-monly showing a fascicular or storiformpattern) can be present. Foci of differen-tiated sarcomatous elements such asrhabdomyosarcoma, chondrosarcoma orosteosarcoma may be found {605,1064}.
Immunohistochemistry
Pleomorphic, spindle and or giant cellcarcinomaExpression of epithelial markers in thespindle and/or giant cell component of apleomorphic carcinoma is not requiredfor the diagnosis so long as there is acomponent of squamous cell carcinoma,
adenocarcinoma, or large cell carcinoma{218,584,1430,1695,2023,2024}. Sincethese are poorly differentiated tumours,in some cases, multiple keratin antibod-ies and EMA are necessary to demon-strate epithelial differentiation in the sar-comatoid component. When pure spin-dle cell carcinomas fail to stain with anyepithelial marker, separation from sarco-ma may be difficult. The tumour cellsoften co-express cytokeratin, vimentin,carcinoembryonic antigen, and smoothmuscle markers {20,88,337,584,1695}.TTF-1 may be positive in giant cell carci-nomas.
Carcinosarcoma The epithelial component of carcinosar-comas may stain with keratin antibodies.Chondrosarcoma will stain with S-100protein and rhabdomyosarcoma withmuscle markers.
Pulmonary blastoma The fetal adenocarcinoma component ofpulmonary blastomas will stain for
epithelial markers (keratin, EMA andCEA) and it may be positive for neuroen-docrine markers such as chromograninA as well in both morular and glandularcells {1064,1435}. The tumour cells canalso express specific hormones, such ascalcitonin, gastrin-releasing peptide,bombesin, leucine and methionineenkephalin, somatostatin and serotonin.This type of staining mimics that seen indeveloping fetal lung tubules {2225}. Theepithelial component of blastomas dif-fusely stains with antibodies to epithelialmarkers, such as cytokeratin, carcinoem-bryonic antigen, and epithelial mem-brane antigen. Pulmonary blastomasrarely stain with alpha-fetoprotein {1824}.Both Clara cell antigen and surfactantapoprotein are expressed in epithelialcells and particularly in morules {1435,2225}. Of interest, these antigens canalso be seen in developing fetal lungtubules, which show differentiationtowards Clara cells beginning at 13weeks of gestation and towards Type IIpneumocytes at 22 weeks {2225}.
DC
BA
Fig. 1.59 Pulmonary blastoma. A Biphasic appearance, with a fetal-type gland and embryonic stroma. B Solid nests of epithelial cells and glands adjacent to anarea of poorly differentiated spindle cell sarcoma. C The tumour consists of a spindle cell (left) and malignant glandular component (right). The glandular compo-nent resembles a well-differentiated fetal adenocarcinoma with endometrioid morphology. D Glandular pattern of a well-differentiated fetal adenocarcinoma withpalisading of nuclei and abundant clear cytoplasm. The spindle cell component has a primitive malignant mesenchymal pattern. From Travis et al. {2024}.

58 Tumours of the lung - Malignant epithelial tumours
Stromal cells of blastomas containvimentin and muscle-specific actin.Desmin and myoglobin or S-100 proteincan be seen when there is striated mus-cle or cartilage respectively. There isgenerally restriction of vimentin andcytokeratin to mesenchymal and epithe-lial tissues respectively {1064}, butvimentin can occur in glands and stromalcells can occasionally express cytoker-atin {2225}.
Differential diagnosis
The differential diagnosis for pleomor-phic carcinoma includes other tumoursin this section as well as both primaryand metastatic sarcomas. Identificationof areas of non-small cell carcinoma andimmunohistochemical confirmation ofepithelial differentiation aid in the distinc-tion.Pleomorphic carcinoma may be difficultto distinguish from reactive processesand sarcomas {390,391,1440,2139}. Agenerous sampling (at least one sectionper centimeter of tumour diameter) todisclose a clear-cut carcinomatous com-ponent may be helpful in pleomorphiccarcinomas, together with the use ofancillary techniques. It should be kept inmind that, although spindle cell carcino-mas are rare, they are more commonthan primary sarcomas of the lung {1440,2138}. Separation of spindle cell carcino-ma from cytokeratin-positive sarcomas,particularly synovial sarcoma may be dif-ficult {546,957,2236}. However, synovialsarcoma has a characteristic morpholo-gy, it tends to be only weakly or focallypositive for keratin and demonstration ofthe X:18 translocation can be helpful.Spindle cell carcinomas may show amarked inflammatory infiltrate and there-fore may be confused with an inflamma-tory myofibroblastic tumour or a localizedarea of organizing pneumonia; such atumour with particularly bland neoplasticcells has been referred to as an inflam-matory sarcomatoid carcinoma {390,391,1440,2139}. Features favouring carcino-ma include nuclear atypia coupled withbrisk mitotic activity, vascular invasion,and positive immunostaining for cytoker-
atins, epithelial membrane antigen andthyroid transcription factor-1.The differential diagnosis of giant cellcarcinoma includes not only other typesof lung carcinomas, but also primary andmetastatic sarcomas including pleomor-phic rhabdomyosarcoma, metastaticadrenocortical carcinoma, metastaticchoriocarcinoma and other pleomorphicmalignant tumours, most of which can bedistinguished by their own distinctivemarkers. Beta-HCG staining can be seenin up to 20-93% of non-small cell carci-nomas {207} and thus does not indicatea diagnosis of metastatic choriocarcino-ma, even if serum beta-HCG is elevated.Benign osteoclast-like giant cells canpopulate non-small cell carcinomas, butthese rare tumours should not be mistak-en for giant cell carcinoma {187}.The differential diagnosis of carcinosar-coma includes other tumours consideredin this section as well as metastaticlesions including teratomas arising fromthe female gynaecologic tract and malegenital tract.Biphasic blastoma should be distin-guished from a fetal adenocarcinoma,pleuropulmonary blastoma as well as pri-mary and metastatic sarcomas includingsynovial sarcoma. Immunohistochemicaland molecular studies in addition to mor-phologic features should differentiatethese tumours.
Histogenesis
Sarcomatoid carcinomas representmalignant epithelial neoplasms that haveundergone divergent connective tissuedifferentiation (“tumour metaplasia” or“divergence hypothesis”) and not “colli-sion” tumours (multiclonal hypothesis){431,866,1078,1440,1738,2002}. Thelight microscopic finding of transitionbetween epithelial and spindle cell com-ponents of most tumours, the finding ofcarcinoma in-situ in some, and theimmunohistochemical and ultrastructuralidentification of epithelial differentiation inthe spindle cell components support thistheory {745}. P53 mutational genotypingof a small number of pleomorphic carci-nomas, carcinosarcomas and blastomas
demonstrated identical mutations inspindle cells and epithelium, supportingthe contention that both epithelial andmesenchymal components originatefrom a single clone {189,866}.
Somatic genetics
Molecular studies have established thatthe epithelial and sarcomatoid compo-nents of pleomorphic carcinoma haveidentical molecular profiles, includingequivalent patterns of acquired allelicloss {431}, p53 mutation profile {866} andX chromosome inactivation {2002}. Ahigh percentage of pleomorphic carcino-mas were reported to have variantCYP1A12 {1624}. The molecular profilesof these tumours are not unlike those ofother non-small cell tumours. Mutationsin beta-catenin were recently shown inblastomas {1779,1801}.
Prognosis and predictive factors
Clinical criteria Clinical outcome is stage dependent butthese tumours have a worse prognosisthan conventional non-small cell carcino-mas {330,584,1261,1430,1695,1976}.Despite the fact that one half of patientspresent with stage I disease, the 5-yearsurvival is only 20% {218,584,1430,1695,2023,2029}. Adjuvant chemotherapy andradiotherapy do not appear helpful {330,443,584,1430,1440,1664,1695,1741,1870}.

59Carcinoid tumour
Definitions
Carcinoid tumours are characterized bygrowth patterns (organoid, trabecular,insular, palisading, ribbon, rosette-likearrangements) that suggest neuroen-docrine differentiation. Tumour cells haveuniform cytologic features with moderateeosinophilic, finely granular cytoplasm,and nuclei with a finely granular chro-matin pattern.Typical carcinoid (TC): A carcinoidtumour with fewer than 2 mitoses per 2 mm2 and lacking necrosis.Atypical carcinoid (AC): A carcinoidtumour with 2-10 mitoses per 2 mm2
and/or foci of necrosis.
ICD-O codes
Carcinoid 8240/3 Typical carcinoid 8240/3Atypical carcinoid 8249/3
Synonyms
The following synonyms have been used,but are no longer recommended.Typical carcinoid: Well differentiated neu-roendocrine carcinoma, Kultchitsky cellcarcinoma – grade 1, mature carcinoid.Atypical carcinoid: malignant carcinoid,moderately differentiated neuroen-docrine carcinoma, grade 2 neuroen-docrine carcinoma.
Localization
TC is uniformly distributed throughout thelungs {391,2026} whereas AC is morecommonly peripheral {128}.
Clinical features
Signs and symptoms Up to half of all bronchopulmonary carci-noids indentified as an incidental radi-ographic finding {580}. The most com-mon symptoms cough and haemoptysistypically relate to bronchial obstruction.Cushing’s syndrome due to ectopicACTH production is uncommon {2026}.The carcinoid syndrome is rare and onlyoccurs when there are widespreadmetastases {580}. MEN1 syndrome isanother rare association {1439}.
Imaging Carcinoid tumours are seen as welldefined pulmonary nodules {613}.Calcification is often seen. Cavitation andirregular margins are rare and pleuraleffusions are uncommon. Endobronchialtumours can sometimes be directlydemonstrated on CT and obstructiveatelectasis or consolidation and mucoidimpaction may be evident distal to themass. Because of their vascularity, carci-noid tumours often show intense contrastenhancement. PET scaning may be neg-
ative. TC and AC tumours are indistin-guishable radiographically.
Diagnostic procedures Carcinoid tumours can be diagnosedreliably by cytology of fine needle aspira-tion or bronchoscopic specimens, butsputum samples are often hypocellular{53,673,936,1329,1457,1940}. In mostcases the diagnosis can be made bybronchoscopic biopsy. However, separa-tion of TC from AC usually requires exam-ination of a resected specimen unlessmitoses and/or necrosis are seen on abronchoscopic biopsy.
Carcinoid tumour M.B. BeasleyF.B. ThunnissenPh.S. HasletonM. BarbareschiB. Pugatch
K. GeisingerE. Brambilla
A. GazdarW.D. Travis
Fig. 1.60 Bronchoscopic image of a typical carci-noid, presenting as a polypoid endobronchial mass.
Fig. 1.61 Carcinoid. A Loose aggregates of slightly irregular small sized tumor cells. Delicate, capillaries with loosely attached radiating tumor cells. Round or ovalnuclei with a irregular ‘salt and pepper’ chromatin pattern. B Aspiration biopsy showing the classic association of carcinoid tumor cells with arborizing delicatecapillaries. Note the striking uniformity of the neoplastic elements. Diff-Quik stain.
BA

60 Tumours of the lung - Malignant epithelial tumours
Cytology
Carcinoid tumours are generally identifi-able in cytological specimens althoughhaemorrhage may dilute brush samples{53,673,936,1329,1457,1940}. The neo-plastic cells are generally present bothindividually and in cohesive aggregates.The latter include acini, flat sheets, tra-beculae, and vascularized connectivetissue fragments; the latter typically pres-ent solely in aspiration smears {1329}.There is a striking uniformity of the neo-plastic cells. These are small and may bedifficult to distinguish from plasma cells,especially in aspiration specimens.Usually, they are oval with moderateamounts of cytoplasm. The latter isbasophilic and occasionally granular.The nuclei are uniformly round or ovoid.
Finely stippled chromatin granules givethe nucleus a characteristic “salt andpepper” pattern. Nucleoli are small andinconspicuous. Isolated tumour cellshave more peripheral nuclei. Infre -quently, carcinoids are composed ofspindle cells {421,566}.In most cytologic specimens, the smearbackground is clean but in aspirationbiopsies it often contains abundantbasophilic granular material.In AC, the neoplastic cells may be morepleomorphic and larger {619,942,1940}and the nuclei show slightly greater chro-matin staining.
Macroscopy
TC and AC both form firm, well demar-cated, tan to yellow tumours. TC in par-
ticular is typically associated withbronchi and are frequently endo-bronchial. The overlying mucosa may beintact or ulcerated. Squamous metapla-sia may be seen. Other bronchial carci-noids push down into the adjacent lungparenchyma. Association with an airwaymay not be readily evident in peripheraltumours {391,1844}.
Tumour spread and staging
At presentation approximately 10-15% ofTC have metastasized to regional lymphnodes and 5-10% of cases eventuallymetastasize to distant sites such as liveror bone. At presentation, 40-50% of AChave metastasized to regional lymphnodes and beyond with approximately20% Stage II, 15% Stage III and 10%Stage IV {128}. Although the TNM classi-fication applies to carcinomas of thelung, it has been used to stage carci-noids of the lung.
Histopathology
Carcinoid tumours are classically com-posed of uniform polygonal cells withfinely granular chromatin, inconspicuousnucleoli and scant to moderate amountsof eosinophilic cytoplasm {1844}.Oncocytic tumours have abundanteosinophilic cytoplasm {391,2026}.Rarely the tumour cell cytoplasm is clearor it may contain melanin {647,653}.Intracytoplasmic mucus is very unusual.Nuclear atypia and pleomorphism maybe quite marked, even in TC, but thesefeatures are unreliable criteria for distin-guishing TC from AC {2028}. Prominentnucleoli may be observed {1844,2026}. Avariety of growth patterns are encoun-tered frequently within one tumour. Themost common patterns are the organoidand trabecular, in which the tumour cellsare respectively arranged in nests orcords. Other patterns include spindle
B CAFig. 1.62 A Central bronchial carcinoid tumour in a 26 year old woman. B More peripherally located carcinoid tumour with bronchiectasis. C Typical carcinoid pre-senting as round, partially endobronchial mass. Note the post-stenotic pneumonia.
DCFig. 1.63 Typical carcinoid. A Tumour cells grow in an organoid nesting arrangement, with a fine vascularstroma. The moderate amount of cytoplasm is eosinophilic and the nuclear chromatin finely granular.B Prominent spindle cell pattern. C Trabecular pattern. D Oncocytic features with abundant eosinophiliccytoplasm. From W. Travis et al. {2024}.
BA

61Carcinoid tumour
cell, papillary, pseudoglandular, rosetteformation and follicular {391,1246,2026}.True gland formation is rare.There is generally a highly vascularizedfibrovascular stroma, but in sometumours the stroma is hyalinized, or itshows cartilage or bone formation {391}.Stromal amyloid is rare {35,537}. Theadjacent airway epithelium may showneuroendocrine cell hyperplasia, some-times associated with airway fibrosis, asdescribed in diffuse idiopathic neuroen-docrine cell hyperplasia {29,1317}. Thisis seen most often in association withperipheral carcinoids. In rare cases thereare also multiple tumourlets or multiplecarcinoid tumours {1314}.AC shows either focal necrosis ormitoses numbering between 2-10/2mm2
{2026,2028}. AC may exhibit all of thegrowth patterns and cytologic featureslisted above for TC.
ImmunohistochemistryMost carcinoid tumours stain for cytoker-atin but up to 20% may be keratin nega-tive {128,272,2026}. Neuroendocrinemarkers such as chromogranin, synapto-physin, Leu-7 (CD57) and N-CAM(CD56) are typically strongly positive,particularly in TC {600,2026,2028}.However, in AC, staining for these mark-ers may be patchy or focal. S-100 proteinmay highlight the presence of sustentac-ular cells {108,718}. Varying results arepublished for TTF-1 with some indicatingTC and AC are usually negative {1894}but others finding approximately a thirdof TC and most AC are positive {600,1513,2134}. The explanation for this dis-crepancy is not known. CD99, is alsopositive in many carcinoids {1565,2134}.Ki 67 is more often positive in AC than TCand is related to survival {416}. EMdemonstrates desmosomes and densecore neurosecretory granules {2110}.
Differential diagnosis
The differential diagnosis of carcinoidtumours includes separation from otherneuroendocrine tumours, and a widevariety of other tumours depending onthe cytology or pattern of the carcinoid. Itmay be difficult to address the differentialdiagnosis based on small specimensobtained by bronchoscopy or fine needleaspiration. Carcinoid tumourlets resem-ble TC and are only distinguished bysize, being less than 5 mm in diameter{373}. TC and AC are distinguished bythe criteria outlined above and this dis-tinction usually requires a surgical spec-imen. The high-grade neuroendocrinetumours, large cell neuroendocrine carci-noma (LCNEC) and small cell lung carci-noma (SCLC) are distinguished by hav-ing a mitotic rate greater than 10 / 2mm2.Ordinarily the rate is much higher thanthis, making these two tumours easilydistinguishable from AC. The presenceof large areas of necrosis is also againstthe diagnosis of AC {128, 2026,2028}.Pseudoglandular or gland-like patternsin carcinoid tumours can be mistakenwith adenocarcinoma, mucoepidermoidcarcinoma, and adenoid cystic carcino-ma. Adenocarcinomas usually showmore cytologic atypia, mucin productionand less staining for neuroendocrinemarkers than carcinoids. Mucoepi -dermoid carcinomas are negative forneuroendocrine markers and they pro-duce mucin. The solid component ofadenoid cystic carcinomas may be mis-taken for carcinoid, but these cells arenegative for neuroendocrine markers{1368}.The organoid nesting pattern of carci-noid tumours can be confused with para-gangliomas, which are very rare in thelung. The presence of S-100 positivesustentacular cells in some carcinoidsmay also cause confusion {108,718}. A
key discriminating feature is the lack ofcytokeratin staining in paraganglioma,which is frequently positive in carcinoids{391}. Glomus tumour may also resemblecarcinoid but it is positive for smoothmuscle actin and negative for neuroen-docrine markers {645}.Spindle cell carcinoids may be confusedwith various mesenchymal tumours, par-ticularly smooth muscle tumours; recog-nition of the finely granular nuclear chro-matin and organoid nesting pattern thiscan generally be resolved morphologi-cally and with appropriate immunohisto-chemical stains.Carcinoids with a prominent papillarypattern may be confused with sclerosinghemangioma but this tumour is negativewith neuroendocrine stains {488}.The epithelial pattern of a carcinoid canbe mimicked by metastatic breast orprostate carcinoma. Although the archi-tecture may be the same, the nuclei inthe latter have a more vesicular chro-matin pattern. In addition, immunohisto-chemistry is helpful for the distinctionsince PSA is positive in prostate carcino-ma, while neuroendocrine markers andTTF1 are negative {61,391}.
Grading
Carcinoid tumours are divided into thelow grade TC and intermediate grade ACbased on the criteria outlined above.
Histogenesis
Pulmonary carcinoid tumours are derivedfrom neuroendocrine cells known to existin normal airways. In fetal lung, neuroen-docrine cells are numerous and areknown to play an important role in lungdevelopment {539,761,1141}. They areless common in the lungs of adults, butvarious stimuli result in neuroendocrinecell hyperplasia {28,719,720}. However,none of these stimuli is recognized to be
B CAFig. 1.64 Typical carcinoid. A Strong cytoplasmic chromogranin staining. B The tumour cells show strong membranous staining for CD56. C Scattered tumour cellsshow strong cytoplasmic ACTH staining in patient presenting with Cushing syndrome due to ectopic ACTH production.

62 Tumours of the lung - Malignant epithelial tumours
of importance of carcinoid tumours. Thevery rare condition of diffuse idiopathicpulmonary neuroendocrine cell hyper-plasia (DIPNECH) is recognized to be apreinvasive lesion for carcinoids {29,2024}.
Somatic genetics
Cytogenetics and CGH Unbalanced chromosomal aberrationsas observed by comparative genomichybridization (CGH) are rare in carci-noids except underrepresentation of 11qmaterial including MEN1 gene in 0-50%of typical carcinoids and 50-70% of atyp-ical carcinoids {2052,2097}. Atypical car-cinoids but not typical carcinoids mayshow 10q and 13q underrepresentation{2097}.
Molecular geneticsCarcinoids have features of neuroen-docrine cells, in common with small celllung cancer and also share some genet-ic alterations. In general, atypical carci-noids (AC) have more extensive changesthan typical carcinoids. A distinctive fea-ture of carcinoids not found in other lungcancers is the frequent presence ofmutations of the MEN1 gene andabsence of its protein product, menin{463,1516}, even though virtually allbronchial carcinoids are sporadic andnot familial tumours. The mutations areaccompanied by allelic loss at the MEN1locus at 11p13. These features are alsofound in gastrointestinal carcinoids.Loss of heterozygosity (LOH) at 3p, 13q,9p21 and 17p is rare in TC but present inAC but at frequencies lower than inSCLC {1516}.
LOH at 3p (3p14.3-21.3) at has beenfound in 40% of AC, which is significant-ly lower than other NSCLC including thehigh-grade neuroendocrine tumoursLCNEC and SCLC (p<0,001). LOH at Rblocus (13p14) and retinoblastoma genepathway inhibitor (Rb) is rare in typicalcarcinoids {127,269,726,727} but pres-ent in 20% of AC {127}. Similarly, Rbexpression is normal in typical carcinoidsbut lost in 21% of atypical carcinoids.Cyclin D1 is overexpressed in 6% of TC{127} LOH is at 9p21 (P16) is observed ina few (20%) AC and TC {1516}. In con-trast to smoking associated lung cancersthat often show G:T transversions, ACshow P53 point mutation of an unusualtype (G:C to A:T transitions or nonsensemutations) {1516}. The p53 pathway isinfrequently affected and inactivated incarcinoids, and is extremely rare in TC.Accordingly P53 aberrant stabilization isnot seen in TC and seen in rare cases ofAC {217,1622}. Other proteins of Rb/P53pathways such as E2F1 are rarely affect-ed in TC but more often in AC. P14ARFprotein loss occurs in 6% of TC and 43%of AC {549,669}. Methylation of tumoursuppressor genes is infrequently seen inTC and AC {1814,2019}. Methylationindex was lower in carcinoids than inSCLC There was no difference in methy-lation frequencies and index between TCand AC except for RASSF1A methylation(a gene with functions similar to Ras),which is observed in 71% of AC (as fre-quently as in SCLC) and in 45% of TC{2019}. Caspase 8 promoter methylationoccurs in 18% of carcinoids {1814}.Except for this important proapoptoticmolecule, methylation and silencing of
tumour suppressor genes is relativelyrare in carcinoids compared to other lungcancers {1814,2017,2019}.
Expression profiles
Limited expression data are available forcarcinoid tumours. Those data, which areavailable, indicate that carcinoid tumoursare more similar to neuronal tumours thanto normal bronchial epithelial cells orsmall cell carcinoma {52}.
Prognosis and predictive factors
Clinical and histopathological criteriaThe overall 5- and 10-year survival ratesare worse for AC (61-73% and 35-59%)than TC (90-98% and 82-95%, p<0.001){128,1844,2028}. After separation of TCfrom AC, stage is the most importantprognostic factor {128,2028}. However,even with lymph node metastasis, TCcarries an excellent prognosis {1999}.With AC size over 3.5 cm also conveys aworse prognosis {128}. Further histo-pathological prognostic criteria (beyondnecrosis and mitoses) include vascularinvasion and nuclear pleomorphism{2028}. Negative predictors of prognosisin AC include mitotic rate, pleomorphism,and aerogenous spread, whereas pal-isading, papillary formation, and pseudo-glandular patterns are favourable prog-nostic features {128}.
Fig. 1.65 Atypical carcinoid. A Small necrotic focus. B A single mitosis is present in this high power field. The tumour cells show carcinoid morphology with mod-erate eosinophilic cytoplasm and finely granular nuclear chromatin. From Travis et al. {2024}.
BA

63Mucoepidermoid carcinoma
Definition
A malignant epithelial tumour character-ized by the presence of squamoid cells,mucin-secreting cells and cells of inter-mediate type. It is histologically identicalto the salivary gland tumour of the samename.
ICD-O code
Mucoepidermoid carcinoma 8430/3
Synonyms
Mucoepidermoid tumour.
Epidemiology
Mucoepidermoid tumours comprise lessthan 1% of all lung tumours {732,2040,2221}. They have an equal sex distribu-tion with a slight predilection for men andhave an age range of 3-78 years with50% of tumours occurring in individualsless than 30 years, and most patientspresenting in the third and fourth decade{811,2221}. There is a suggestion ofpredilection for Caucasians over Blacks.They form a significant proportion ofpediatric endobronchial tumours.
Etiology
There appears to be no association withcigarette smoking or other risk factors.
Localization
The majority arise from bronchial glandsin the central airways. Tumours with thishistology that are encountered in theperipheral lung should raise the question
of metastatic tumour or adenosquamouscarcinoma.
Clinical features
Signs and symptomsSigns and symptoms are related to thepolypoid endobronchial growth of thistumour and tracheal and large airway irri-tation {398,1011,1646}. Wheeze,haemoptysis, and recurrent pneumoniawith post-obstructive changes are mostoften noted, although up to 25% ofpatients may be asymptomatic.
ImagingChest radiographs and CT scansdemonstrate a well-circumscribed ovalor lobulated mass arising within thebronchus {612}. Calcification is occa-sionally seen. Post-obstructive pneumon-ic infiltrates are often noted, occasionallywith cavitation.
Macroscopy
Grossly, these tumours usually occur inthe main, lobar or segmental bronchi,ranging in size from 0.5-6 cm with anaverage size of approximately 2.2 cm{811,2221}. They are soft, polypoid, andpink-tan in colour often with cysticchange and a glistening mucoid appear-ance. Extension between bronchial carti-laginous plates is occasionally noted.Distal obstructive / cholesterol pneumo-nia may be seen. High-grade lesions areusually more infiltrative.
Tumour spread and staging
Low-grade mucoepidermoid tumoursspread to regional lymph nodes by localgrowth in less than 5% of cases,although distant spread rarely occurs.High-grade tumours involve not onlyregional nodes but may metastasize toliver, bones, adrenal gland, and brain.
Histopathology
On the basis of morphological and cyto-logical features, tumours are divided intolow and high-grade types. In low-gradetumours, cystic changes often dominateand solid areas typically comprise mucin
secreting and columnar epithelium form-ing small glands, tubules, and cysts.Necrosis is inconspicuous. These cystsoften contain inspissated mucus, whichhas a colloid-like appearance and fre-quently is calcified. The lining cells arecytologically bland with round to ovalnuclei, abundant eosinophilic, mucin-richcytoplasm, and infrequent mitotic fig-ures. Often, intimately admixed with thismucinous epithelium are non-keratinizingsquamoid cells that grow in a sheet-likepattern with intercellular bridges. Thethird cellular component is an intermedi-ate or transitional cell that is oval inshape, has a round nucleus and fainteosinophilic cytoplasm. The accompany-ing stroma is often oedematous with fociof dense stromal hyalinization, particular-ly around the glandular elements, thatmay have an amyloid-like appearance.Stromal calcification and ossification,with a granulomatous reaction is seenaround areas of mucus extravasation.High-grade mucoepidermoid carcino-mas are rare and have histologic featuresthat overlap with adenosquamous carci-noma {811,1445,2221}. They consistlargely of intermediate and squamoidcells with a minor component of mucinsecreting elements. They demonstratenuclear atypia with hyperchromatism,pleomorphism, brisk mitotic activity anda high nuclear to cytoplasmic ratio.These lesions often invade the pul-monary parenchyma and may be associ-ated with positive regional lymph nodes.Controversy exists in their separationfrom adenosquamous carcinoma.Criteria more typical of high grademucoepidermoid tumours include: (1)exophytic endobronchial growth, (2) sur-face epithelium lacking changes of in-situ carcinoma, (3) absence of individualcell keratinization and squamous pearlformation, (4) transitional areas to lowgrade mucoepidermoid carcinoma.
Histogenesis
Mucoepidermoid carcinomas are histo-logically similar to their counterparts inthe salivary glands and it has been pre-
Mucoepidermoid carcinoma S.A. YousemA.G. Nicholson
Fig. 1.66 Mucoepidermoid carcinoma. The well cir-cumscribed, light tan mass does not grossly infil-trate the underlying lung parenchyma.

64 Tumours of the lung - Malignant epithelial tumours
sumed that they are derived from primi-tive cells differentiating within the tra-cheobronchial mucous glands.
Somatic genetics
No consistent cytogenetic abnormalitieshave been noted with mucoepidermoidcarcinomas of the tracheobronchial tree.
Genetic susceptibility
No genetic susceptibilities are noted withmucoepidermoid tumours. It should benoted, however, that the pediatric popu-lation comprises a significant percentageof patients with this lesion.
Prognosis and predictive factors
Low-grade mucoepidermoid tumourshave a much better prognosis than high-grade tumours, the latter being similar tonon-small cell carcinomas {732,811,2221}. Low-grade tumours rarely metas-tasize with less than 5% of reportedcases metastasizing to regional lymphnodes. Children have a particularlybenign clinical course. Low-gradetumours are often treated with bron-choplastic procedures such as sleeveresection.High-grade mucoepidermoid carcino-mas are generally treated similar to non-
small cell carcinomas. Their prognosis ismuch more guarded as they tend tobehave as non-small cell carcinomas.Diagnostic features, which indicate ahigh likelihood of recurrence, metastasis,or death include constitutional signs andsymptoms including pain, weight loss,malaise. Positive margins of resection;positive hilar lymph nodes and localaggressive behaviour, such as chest wallinvasion are also adverse factors {398,732,2221}.
BAFig. 1.67 Mucoepidermoid carcinoma. A Mucoepidermoid carcinomas arise in the submucosa of the airways, in association with the tracheobronchial glands.Variably solid and cystic appearance. B Goblet cells containing abundant mucin and form glandular arrays with centrally located extracellular mucosubstance.Squamoid cells with a polygonal appearance, round nuclei, irregularly distributed chromatin, inconspicuous nucleoli and abundant cytoplasm. Intercellular bridgesand keratinization are absent. Transitional cells occupy an intermediate cytomorphology between squamoid and mucin producing elements.

65Adenoid cystic carcinoma
Definition
Adenoid cystic carcinoma is a malignantepithelial neoplasm, recapitulating itscounterpart in the salivary glands, with adistinctive histologic pattern of growth ofthe epithelial cells in cribriform, tubularand glandular arrays orientated aroundand associated with a variably mucinousand hyalinized basement membrane-richextracellular matrix, with the cells show-ing differentiation characteristics of ductlining and myoepithelial cells.
ICD-O code 8200/3
Synonyms
Cylindroma and adenocystic carcinoma.
Epidemiology
Adenoid cystic carcinoma of the lungand bronchus comprises less than 1% ofall lung tumours {809,2029}. It has anequal sex distribution and tends to occurin the fourth and fifth decades of life{1368}. In the majority of cases adenoidcystic carcinoma behaves in an insidiousand indolent fashion with multiple localrecurrences preceding metastases.
Etiology
There appears to be no association withcigarette smoking or other risk factor(s).
Localization
90% of cases originate intraluminallywithin trachea, main stem or lobarbronchi {1621}.
Clinical features
Presentation reflects proximal airwayobstruction with shortness of breath,cough, wheeze, chest pain and haemop-tysis described {833,1271,1487,1560,2014}. Radiographs show a centrallylocated mass that may have an endo-bronchial component or may formplaques or annular lesions in the wall ofbronchi {1271}. Extension into the pul-monary parenchyma is often present andoccasionally into mediastinal fat.
Macroscopy
Adenoid cystic carcinoma typically formsgray-white or tan polypoid lesions thick-ening the submucosa of the bronchus,sometimes with no alteration of the sur-face mucosa. It also may form diffuseinfiltrative plaques that extend in a longi-tudinal and/or circumferential fashionbeneath the submucosa. Size rangesfrom 1–4 cm with an average of 2 cm{1368}. A distinctive feature is that it hasdeceptively infiltrative margins, whichextend far beyond the localized nodulenoted grossly and therefore sampling ofperibronchial soft tissue is worthwhile.
Tumour spread and staging
Staging of adenoid cystic carcinomas isperformed according to the AJCC andUICC TNM staging system. Adenoid cys-tic carcinoma is predisposed to recurwithin the lung parenchyma, the pleura,chest wall, and mediastinum beforemetastasizing late to liver, brain, bone,spleen, kidney, and adrenal glands.Regional lymph node metastases areseen in approximately 20% of cases andsystemic metastases in approximately40%.
Histopathology
Architecturally, adenoid cystic carcinomaoften breaches the cartilaginous plateextending into the pulmonary parenchy-ma, hilar and mediastinal soft tissues. Itsgrowth pattern is typically heteroge-neous, with neoplastic cells arranged incribriform arrays, tubules or solid nests.The most characteristic cribriform pat-tern shows cells surrounding cylinders ina sclerotic acid mucopolysaccharide-rich basement membrane-like material.The neoplastic cells are small with scantcytoplasm and dark hyperchromatic
Adenoid cystic carcinoma S.A. YousemA.G. Nicholson
Fig. 1.69 Adenoid cystic carcinoma growing in the typical pattern in the submucosa of the airway. Note pre-served, intact respiratory mucosa.
Fig. 1.68 Adenoid cystic carcinoma arising withinthe bronchus.

66 Tumours of the lung - Malignant epithelial tumours
nuclei that are oval to angulated, andshow infrequent mitotic figures.Occasionally, these cells form tubuleslined by two to three cells, with the lumi-nal cells having a low cuboidal appear-ance and the peripheral cells forming amyoepithelial layer. Perineural invasion isseen in 40% of cases and extensionalong vascular structures, bronchi andbronchioles, and lymphatics is charac-teristic.Immunoperoxidase stains show that theneoplastic cells have a variable ductaland myoepithelial phenotype, the cellsexpressing cytokeratin but also vimentin,smooth muscle actin, calponin, S-100protein, p63, and GFAP. The surrounding
matrix recapitulates a basement mem-brane like material in that it stains posi-tive with antibodies directed at Type IVcollagen, laminin, and heparin sulfate.
Histogenesis
Adenoid cystic carcinoma is derivedfrom a primitive cell, presumably of tra-cheobronchial gland origin, which showsdifferentiation characteristics of ductaland myoepithelial cells.
Prognosis and predictive factors
The behavior of adenoid cystic carcino-ma is one of multiple recurrences withlate metastases and survival needs to beanalyzed over a prolonged period (10-15
years) {398,1271,1560,1621}. Patientsare prone to develop local recurrencebecause of difficulty obtaining clear mar-gins and it is recommended that marginsof resection be analyzed by frozen sec-tion at the time of primary surgery.Primary treatment is surgery with supple-mental radiation, especially by linearaccelerator. Poor prognosis is related tostage of the tumour at the time of diag-nosis, the presence of positive margins,and a solid cellular growth pattern.
DC
BA
Fig. 1.70 Adenoid cystic carcinoma. A Adenoid cystic carcinoma was historically termed cylindroma: neoplastic cells typically form cylinders of basophilic mucoidand basement membrane-like material surrounded by hyperchromatic angulated epithelial cells. B Cylinders are surrounded by small hyperchromatic cells withdense oval nuclei having scant eosinophilic cytoplasm. Occasional tubular differentiation is noted. C Finger-like stromal structure. Cohesive cells with oval nucleiand little cytoplasm. Bronchial brushing. Papanicolaou stain. D Translucent hyaline globule surrounded by small uniform epithelial cells. Bronchial brushing.Papanicolaou stain.

The tracheobronchial tree may be thesite of origin for a wide variety of salivarygland tumours {1187,1364,1563,1883,1883}. These include epithelial-myoep-ithelial carcinoma, acinic cell carcinoma,carcinoma ex pleomorphic adenoma andmalignant endobronchial myxoid tumour.Of these only epithelial-myoepithelialcarcinomas have been analysed in sig-nificant numbers.
Definition
Epithelial-myoepithelial carcinomas con-sist of myoepithelial cells with spindlecell, clear cell or plasmacytoid morphol-ogy and varying amounts of duct-form-ing epithelium.
ICD-O code 8562/3
Synonyms
Adenomyoepithelioma, myoepithelioma,epithelial-myoepithelial carcinoma, epi-thelial-myoepithelial tumour, epimyo-epithelial carcinoma, epithelial-myoepi-thelial tumour of unproven malignantpotential and malignant mixed tumourcomprising epithelial and myoepithelialcells.
Epidemiology
Age ranges from 33 to 71 years with nosex predominance.
Etiology
There appears to be no association withcigarette smoking or other risk factor(s).
Localization
The tumors are nearly all endobronchialin location.
Clinical features
Presenting symptoms and imagingreflect airway obstruction {639,1480,2037}.
Macroscopy
The cut surface ranges from solid togelatinous in texture and white to gray incolour {639,1480,2037}.
Histopathology
Tumours comprise myoepithelial cellsthat are spindled or rounded and containeosinophilic or clear cell cytoplasm, plusa variable proportion of duct-formingepithelium {639,1480,2037}.Occasional purely myoepitheliomatoustumours are described. Ducts are typi-cally lined by a dual layer of cells, com-prising an inner layer of cuboidal cells
with eosinophilic cytoplasm and an outerlayer of cells with predominantly clearcytoplasm. Mitotic activity is generallylow. Generally, the inner layer of ductsstains for MNF116 and EMA and theouter layer plus solid components stainfor SMA and S-100, although there maybe some overlap.
Prognosis and predictive factors
Surgical resection is the treatment ofchoice and usually curative, although laterecurrence may occur {639,1480, 2037}.
Epithelial-myoepithelial carcinoma S.A. YousemA.G. Nicholson
DCFig. 1.71 Epithelial-myoepithelial carcinoma. A This tumour is composed of clear cell nests (left) and glands(right) some of which have a double layer of cells with an inner layer of eosinophilic cells and an outer layerof clear cells. B The inner layer of ductal cells is immunostained by cytokeratin 7. C The outer layer ofmyoepithelial cells is immunostained by smooth muscle actin. D The outer layer of myoepithelial cells isimmunostained by S100 protein.
BA
67Epithelial-myoepithelial carcinoma

68 Tumours of the lung - Preinvasive epithelial lesions
Definition
A precursor lesion of squamous cell car-cinoma arising in the bronchial epitheli-um. Squamous dysplasia and carcinomain situ are a continuum of recognizablehistologic changes in the large airways.They can occur as single or multifocallesions throughout the tracheobronchialtree. Dysplasia or carcinoma in situ mayexist as an isolated finding or as abronchial surface lesion accompanyinginvasive carcinoma
ICD-O code
Squamous cell carcinoma in situ 8070/2
Synonyms and historical annotation
Squamous atypia, angiogenic squamousdysplasia, bronchial premalignancy,preinvasive squamous lesion, high-grade intraepithelial neoplasia, earlynon-invasive cancer.The existence of central airway squa-mous lesions regarded as progenitors ofsquamous carcinoma has been recog-nized for decades {93}. They were initial-ly graded according to complicateddescriptive criteria including the loss ofcilia, thickness (number of cell layers) of
the epithelium, the degree of atypia andthe percentage of atypical cells {94,95},but a manageable and reproducibleclassification was recently published{1465,2024}.
Clinical features
Squamous dysplasia is nearly alwaysasymptomatic but occurs in individualswith heavy tobacco exposure (more than30 pack years of cigarette smoking) andwith obstructive airway disease {849,1389}. Pre-invasive squamous bronchiallesions are found more frequently in menthan in women {1118}.
Relevant diagnostic procedures
Sputum cytology examinationCurrently, the only non-invasive test thatcan detect pre-invasive lesions is spu-tum cytology examination {620,993}.
20% of patients with greater than a 30pack year history of smoking, airwayobstruction with forced expiratory vol-ume 1 (FEV1) <70% of expected havemoderate dysplasia or worse by fluores-cence bronchoscopy {1533}. Of thosewith moderate atypia on sputum cytol-ogy, at least 55% have dysplasiadetectable by fluorescence bron-choscopy. Sputum atypia as an inde-pendent variable in predicting dysplasiaat fluorescence bronchocoscopy has notyet been tested in a controlled trial eval-uating high-risk smokers with airwayobstruction.
White-light bronchoscopyApproximately 40% of cases of carcino-ma in situ can be detected by white-lightreflectance bronchoscopy. About 75% ofdetected carcinoma in situ lesions
Squamous dysplasia and
carcinoma in situ
W.A. FranklinI.I. WistubaK. GeisingerS. LamF.R. Hirsch
K.M. MullerG. Sozzi
E. BrambillaA. Gazdar
Fig. 1.73 Bronchscopy images of squamous dysplasia and carcinoma in situ. A Nodular carcinoma in-situof the left lower lobe. White-light image. B Carcinoma in situ right upper lobe with focal thickening of thebronchial bifurcation and slight irregularity of the bronchial mucosa. C Carcinoma in situ upper divisionalbronchus, left upper lobe. Focal increase in vascularity was observed under white-light bronchoscopy.D Carcinoma in situ left upper lobe. The lesion is visible as an area of reddish-brown fluorescence underautofluorescence bronchoscopy {1117,1120}, using the LIFE-Lung Device. E Severe dysplasia left upperlobe. No abnormality under white-light bronchoscopy. F Same case as E. The dysplastic lesion is visible asan area of reddish fluorescence under autofluorescence bronchoscopy {1117,1120}, using the Onco-LIFEDevice (Xillix Technologies Inc. Vancouver, Canada).
Fig. 1.72 Carcinoma in situ at the bronchus bifurca-tion. Note the plaque-like greyish lesions resem-bling leukoplakia.
ED
CA B
F

69Squamous dysplasia and carcinoma in situ
appear as superficial or flat lesions; theremaining 25% have a nodular or poly-poid appearance {967,1423}. Becausenodular/polypoid lesions are elevatedfrom the adjacent normal mucosa,lesions as small as 1-2 mm in diametercan be seen. Flat or superficially spread-ing lesions greater than 1-2 cm in surfacediameter are generally visible as areas offocal thickening, increase in vascularityor marked irregularity of the mucosa. Flatlesions 5-10 mm in diameter usually pro-duce non-specific thickening, redness,fine roughening, loss of luster or a slightincrease in granularity which are difficultto distinguish from inflammation or squa-mous metaplasia {2057}. Lesions <5 mmare usually invisible on white light bron-choscopy. Bronchial dysplasia usuallypresents as non-specific mucosalswelling or thickening at a bronchialbifurcation.
Autofluorescence bronchoscopyPre-invasive lesions that have subtle orno visible findings on white-light bron-choscopy can be localized by autofluo-
rescence imaging using a violet or bluelight for illumination instead of white-lightand special imaging sensors attached toa fiberoptic bronchoscope for detectionof the abnormal autofluorescence {1117,1120}. Dysplastic and malignant tissueshave a significant decrease in the greenautofluorescence intensity relative to thered autofluorescence. These pre-inva-sive lesions are identified by their brownor brownish-red autofluorescence.Lesions as small as 0.5 mm can be local-ized by this method.
Cytology
Sputum cytological classificationschemes for preneoplastic lesions havebeen published by Saccomanno {1717}and Frost {621} and consist of gradationsof microscopic abnormality similar tothose observed in histological sectionsfrom lower airways of smokers.Squamous metaplasia presents in spu-tum smears as individual cells, but most-ly as flat loosely cohesive clusters. Thecytologic manifestations of dysplasiaoccur as increasingly severe cellular
changes, ranging from mild, moderate,and severe atypia to carcinoma in situ(CIS) {1717}. There are progressive alter-ations including increasing variability incellular and nuclear sizes, increasinglyvariable nuclear-to-cytoplasmic ratios,increasing proportions of cells with cyto-plasmic eosinophilia (orangeophilia),increasing coarseness of chromatingranularity until a pyknotic-like pattern isreached in CIS, increasing irregularity inthe distribution of chromatin granules,and increasing irregularities in the out-lines of nuclear membranes {844,1717,1718}. This last feature first appears inmoderate atypia {1717}. According toKoprowska et al {1055}, it is this deviationfrom smooth nuclear outlines that is moststrongly associated with the presence ofcarcinoma.
Localization and macroscopy
Foci of carcinoma in situ usually arisenear bifurcations in the segmentalbronchi, subsequently extending proxi-mally into the adjacent lobar bronchusand distally into subsegmental branches.
Fig. 1.74 Carcinoma in situ. The bronchial mucosa is replaced with atypical squamous cells extending from the surface to the base of the epithelial. Note the severenuclear polymorphism, hyperchromasia and enlarged nuclei.

70 Tumours of the lung - Preinvasive epithelial lesions
The lesions are less frequent in the tra-chea. Bronchoscopically and grosslythere is often no macroscopical alter-ation. When gross abnormalities arepresent, focal or multi-focal plaque-likegreyish lesions resembling leukoplakia,nonspecific erythema and even nodularor polypoid lesions may be seen.
Histopathology
A variety of bronchial epithelial hyper-plasias and metaplasias may occur thatare not regarded as preneoplasticincluding goblet cell hyperplasia, basalcell (reserve cell) hyperplasia, immaturesquamous metaplasia, and squamousmetaplasia. The term preinvasive doesnot imply that progression to invasion willnecessarily occur. These lesions repre-sent a continuum of cytologic and histo-logic changes that may show some over-lap between defined categories. Squa -mous dysplasia does not invade the stro-ma. The basement membrane remainsintact and is variably thickened. Theremay be vascular budding into the epithe-lium, termed angiogenic squamous dys-plasia {986}. The latter lesion has alsobeen previously reported as micropapil-lomatosis {724, 1407}.
ImmunohistochemistryA series of immunohistochemicalchanges accompany squamous dyspla-sia. These include increased expressionof EGFR {607,1101,1710}, HER2/neu
{608}, p53 {145,211,1251}, MCM2{1966}, Ki-67 {607,1149,1966}, cytoker-atin 5/6 {54}, bcl-2 {211}, VEGF{602,1126}, maldistribution of MUC1,and loss of several proteins includingFHIT {1855}, folate binding protein{609,676}, and p16 {213,1122}. A linearprogression of proliferative activity,assessed with immunohistochemicalstaining for the proliferation marker Ki-67(MIB-1), correlates with the extent andgrade of the preneoplasia {1966}. Loss ofRAR-beta expression is very frequent inthe bronchial epithelium of smokers{1252,2017}. Type IV collagen staininghighlights discontinuities in basementmembranes that increase from basal cellhyperplasia to dysplasia, progressing todestruction in carcinoma in situ and inva-sive carcinoma {657}. Changes alsooccur in matrix metalloproteinase (MMP)and tissue inhibitor of metalloproteinase(TIMP) expression corresponding to pro-gression in severity of dysplasia, in situcarcinoma and invasive carcinoma{657}.
Electron microscopy There is an increase in atypical basalcells with loss of polarity. The nuclei showconsiderable hyperchromasia, and varia-tions in shape with numerous invagina-tions. The number of nucleoli isincreased, and so-called pseudoinclu-sion bodies may be seen within thenuclei. Some cells exhibit atypical devel-
opment via an atypical array oforganelles {711,712,1407}. A specialfeature is seen in the basement mem-brane in CIS. It is subdivided by multipletentacle-like cytoplasmic protrusions,which vary considerably in shape andsize but are always directed towards andbetween the fibrous structures of thebasement membrane {711,712,1407}.
Histogenesis
The stem cell for the squamous epitheli-um of the proximal airway is not certain,but it is presumed that the basal cellsrepresent a relatively quiescent zone thatis the precursor for preneoplastic epithe-lium. It is of interest that these cellsexpress a different cytokeratin profilewith high levels of cytokeratin 5/6 and arethe only cells in the normal respiratorymucosa and express significant levels ofepidermal growth factor receptor. In theearliest preinvasive lesions, this basalzone is expanded with phenotypicchanges that mirror the quiescent basalzone in normal epithelium including theoverexpression of EGFR, transformationfrom cytokeratin 5/6 negative to positive,and increased proliferative activity withhigh expression of Ki-67 and MCM2. It iswidely supposed that low grade changessuch as basal cell hyperplasia and squa-mous metaplasia may (with or withoutmicropapillomatosis) progress throughmild, moderate and severe dysplasia upto carcinoma in situ {392,994,2022} toinvasive carcinoma. However, such aprogression is rarely observed in individ-ual subjects and the predictive power ofspecific grades of premalignant changefor the future development of invasivecarcinoma is still under investigation.
Somatic genetics
Cytogenetics and CGH Relatively few cytogenetic studies havebeen performed on preneoplastic lesionsbecause of their small size and becauseof the difficulty of identifying them {1449,1854}. Classic cytogenetic studies arefurther limited by the necessity for short-term cultures and the inability to identifythe cell of origin of metaphase spreads.For these reasons most analyses haveutilized fluorescence in situ hybridization(FISH) for detection of chromosomal ornumerical changes in bronchial epithelialcells. As part of the field effect resultingfrom widespread smoking damage to theentire upper aerodigestive tract, cytoge-
Fig. 1.75 Preinvasive lesions. Sequential molecular changes during the multistage pathogenesis of squa-mous cell lung carcinoma. Molecular changes occurring during lung pathogenesis may commence early(normal or slightly abnormal epithelium), at an intermediate (dysplasia) stage, or relatively late (carcinomain situ, invasive carcinoma).

71Squamous dysplasia and carcinoma in situ
netic changes may be detected both inpreneoplastic lesions as well as histolog-ically normal appearing cells. Numericalchanges of chromosme 7 are frequentand may predict risk for cancer develop-ment {1147,2245}. Only one study todate has performed comparative genom-ic hybridization on preneoplastic lesionsand found that numerical alterations ofchromosome 3 were the most frequentchange {813}.
Molecular genetics Precise microdissection of epithelial cellsfollowed by molecular genetic analysis ofsuch lesions has provided a sequence ofmolecular changes similar to thatobserved in other epithelial cancers{844,2161}. These studies have also indi-cated similarities and differencesbetween the sequential changes leading
to central and peripheral tumours. Thehistological changes preceding squa-mous cell carcinomas are well docu-mented because of accessibility of theselesions, and the developmentalsequence of molecular changes is non-random. DNA aneuploidy is frequent indysplastic lesions particularly in high-grade lesions. Small foci of allelic lossare common at multiple sites in thebronchial epithelium and persist longafter smoking cessation {1549}.LOH occurs at one or more chromosome3p regions and 9p21 early in neoplasticdevelopment, commencing in histologi-cally normal epithelium. Later changesinclude 8p21-23, 13q14 (RB) and 17p13(P53) being detected frequently in histo-logically normal epithelium {1236,2157,2158,2162}. In contrast, allele loss at5q21 (APC-MCC region) mutations has
been detected at the carcinoma in situstage, and P53 mutations appear at vari-able times {1900,2157,2162}. Chromo -some 3p losses in normal epithelium,basal cell hyperplasia and squamousmetaplasia are small and multifocal,commencing at the central (3p21) regionof the chromosomal arm, while in laterlesions such as carcinoma in situ, allelicloss is present along nearly all of theshort arm of chromosome 3p {2157,2158}. The clonal patches of bronchialepithelium having molecular changes(allelic loss and genetic instability) areusually small, and have been estimatedto be approximately 40,000 to 360,000cells {1549}. p16INK4a methylation hasalso been detected at early stages ofsquamous preinvasive lesions with fre-quency increasing during histopatholog-ic progression from basal cell hyperpla-
Table 1.11Microscopic features of the squamous dysplasia and carcinoma in situ.
Abnormality Thickness Cell size Maturation/orientation Nuclei
Mild Dysplasia Mildly increased Mildly increasedMild anisocyto-sis,Pleomorphism
Continuous progression of maturation frombase to luminal surfaceBasilar zone expanded with cellular crowd-ing in lower thirdDistinct intermediate (prickle cell) zonepresentSuperficial flattening of epithelial cells
Mild variation of N/C ratioFinely granular chromatinMinimal angulationNucleoli inconspicuous or absentNuclei vertically oriented in lower thirdMitoses absent or very rare
ModerateDysplasia
Moderatelyincreased
Mild increase incell size; cellsoften smallMay have mod-erate anisocyto-sis, pleomor-phism
Partial progression of maturation from baseto luminal surfaceBasilar zone expanded with cellular crowd-ing in lower two thirds of epitheliumIntermediate zone confined to upper third ofepitheliumSuperficial flattening of epithelial cells
Moderate variation of N/C ratioFinely granular chromatinAngulations, grooves and lobulations pres-entNucleoli inconspicuous or absentNuclei vertically oriented in lower two thirdsMitotic figures present in lower third
SevereDysplasia
Markedlyincreased
MarkedlyincreasedMay havemarked anisocy-tosis, pleomor-phism
Little progression of maturation from baseto luminal surfaceBasilar zone expanded with cellular crowd-ing well into upper thirdIntermediate zone greatly attenuatedSuperficial flattening of epithelial cells
N/C ratio often high and variableChromatin coarse and unevenNuclear angulations and folding prominentNucleoli frequently present and conspicu-ousNuclei vertically oriented in lower two thirdsMitotic figures present in lower two thirds
Carcinoma in situ
May or may notbe increased
May be markedlyincreasedMay havemarked anisocy-tosis, pleomor-phism
No progression of maturation from base toluminal surface; epithelium could be invert-ed with little change in appearanceBasilar zone expanded with cellular crowd-ing throughout epitheliumIntermediate zone absentSurface flattening confined to the mostsuperficial cells
N/C ratio often high and variableChromatin coarse and unevenNuclear angulations and folding prominentNucleoli may be present or inconspicuousNo consistent orientation of nuclei in rela-tion to epithelial surfaceMitotic figures present through full thick-ness
creo

72 Tumours of the lung - Preinvasive epithelial lesions
sia to squamous metaplasia to carcino-ma in situ {140}. Detection of suchchanges in sputum samples may be ofpredictive value in identifying smokers atincreased risk of developing lung cancer{141}. Similar changes have beendetected in telomerase activation {2199}.While weak telomerase RNA expressionis detected in basal layers of normal andhyperplastic epithelium, dysregulation oftelomerase expression increases withtumour progression with moderate tostrong expression throughout the multi-layers of the epithelium in squamousmetaplasia, dysplasia and carcinoma insitu.While specific premalignant changesassociated with SCLC have not beenidentified, extensive genetic damageoccurs in the accompanying normal andhyperplastic bronchial epithelium and ischaracteristic of SCLC tumours {2160}.These changes are much more extensivethan changes accompanying similarepithelia from lung resections of patientswith squamous cell carcinoma or adeno-carcinoma. These findings suggestmajor differences in the pathogenesis ofthe three major lung cancer types.Our knowledge of the changes preced-ing peripheral tumours is much more lim-ited, mainly because of the inability to
identify and have access to such lesions.However, careful examination of lungcancer resections indicates that periph-eral tumours, especially adenocarcino-ma, may be accompanied by specificmorphologic changes known as atypicaladenomatous hyperplasia (AAH). Theadvent of CT scans for the detection ofearly lung cancers has greatly increasedthe identification of such lesions, both insmokers with and without lung cancer{844,2078}. Inflation of the lungs prior tofixation greatly enhances the ability todetect these lesions. Multiple molecularchanges have been described in theselesions {1021} including aneuploidy, rasgene mutations, COX-2 over expression,active proliferation, 3p and 9p deletions,K-ras codon 12 mutations, and disrup-tion of the cell cycle control, but p53gene aberrations are rare and telom-erase activation is absent.
Prognostic factors
Carcinoma in situ, being a preneoplasticlesion, is classified as “Stage 0 disease.”Resection of specific lesions at this stagemeans 100% curability, although fre-quent multifocality means that other fociare liable to present elsewhere in the air-ways. In general, higher grades of dys-plasia are more closely associated with
synchronous invasive carcinomas,although the prognostic significance ofidentifying dysplasia in isolation is uncer-tain. Currently, there are no recommen-dations to screen asymptomatic individu-als with a history of dysplasia for devel-opment of invasive lesions {1119,1408,1860}. There are no data to allow predic-tion of progression to invasive disease,depending on grade of dysplasia. It islikely that severe dysplasia/CIS carries ahigh risk. Progression of disease, fromthe early stages, probably takes manyyears.
Genetic predictive factors There is a general consensus thatnumerous genetic and molecular abnor-malities occur in very early stages of lungcarcinogenesis including hyperplasiaand metaplasia and even in normalappearing bronchial epithelium in smok-ers {1236,2162}. None of these isolatedmolecular abnormalities have beenshown to predict progression to cancer,but their cumulative rate may be associ-ated with the risk of cancer in thebronchial tree {926}..

73Atypical adenomatous hyperplasia
Definition
Atypical adenomatous hyperplasia(AAH) is a localised proliferation of mildto moderately atypical cells lininginvolved alveoli and, sometimes, respira-tory bronchioles, resulting in focal lesionsin peripheral alveolated lung, usually lessthan 5mm in diameter and generally inthe absence of underlying interstitialinflammation and fibrosis.
Synonyms
Atypical alveolar cuboidal cell hyperpla-sia {1807}, alveolar epithelial hyperplasia{1434}, atypical alveolar hyperplasia{288}, atypical bronchioloalveolar cellhyperplasia {2123}, bronchioloalveolarcell adenoma {1316}.
Background
AAH is a putative precursor of peripheralpulmonary adenocarcinoma, includingbronchioloalveolar carcinoma (BAC){1807}; the ‘adenoma’ in an adenoma-carcinoma sequence in the peripherallung {1318}. Epidemiological, morpho-logical, morphometric, cytofluorometricand genetic evidence support thishypothesis {392,994,1021,1378,2022}. AAH is most frequently found as an inci-dental histologic finding in lungs alreadybearing primary cancer, especially ade-nocarcinoma. Lungs with very high num-
bers of AAH (>40) have been reported inconjunction with multiple synchronousperipheral primary adenocarcinomas orBAC {51,333,1316,1434,1928,2123}.Autopsy studies have reported AAH in 2-4% of non-cancer bearing patients{1879,2206,2207}.AAH has been reported in up to 19% ofwomen and 9.3% of men with lung can-cer and up to 30.2% and 18.8%, respec-tively, in women and men with pulmonaryadenocarcinoma {333}. In Japan, thisgender relationship is inconsistent {1429,2123}. Almost all Caucasians reportedwith AAH have been smokers, while inJapan, an association is not clear. Dataon the association of AAH with either apersonal or family history of malignancyare conflicting {334,1429,1960}.
Clinical features
Signs and symptoms There are no clinical signs or symptomsdirectly referable to AAH. The lesions areusually encountered as incidental find-ings at gross or, more often, microscopicexamination of lung.
Imaging Radiological experience of AAH is large-ly confined to screening studies usingHigh Resolution CT scanning (HRCT){979,1108}, though some have been
described during follow-up of patientswith lung cancer {1038,1198}. In thiscontext, small non-solid nodules, alsodescribed as localised areas of pureground glass opacity (GGO), may beidentified as areas of increased opacifi-cation with distinct borders, not com-pletely obscuring the underlying lungparenchyma on CT scan, measuring 2-24mm in diameter, and typically not visu-alized on chest radiographs. Resectionof GGOs has shown a range of patholo-gy including benign disease in up to30%, AAH in 10-77%, BAC in up to 50%and invasive adenocarcinoma in 10-25%of cases {979,1038,1108,1431}.
Relevant diagnostic procedures AAH may rarely be visualised radiologi-cally and a presumptive diagnosis made.Most likely as part of an HRCT screening
Atypical adenomatous hyperplasia K. M. KerrA.E. FraireB. PugatchM.F. VazquezH. KitamuraS. Niho
Cancer type Prevalence
All primary lung cancerAdenocarcinomaSquamous cell carcinomaLarge cell carcinomaMetastatic disease
Table 1.12 AAH in lung cancer resection specimens. From references: {33,1041,1316,1387,1434,2123}
Fig. 1.76 Atypical adenomatous hyperplasia. A Unusually prominent AAH lesion. Alveolar spaces are visible within the lesion. B AAH (center) detected incidentallyin a lung resected for mucinous adenocarcinoma, present on the left.
BA
9 - 21%16 - 35%3 - 11%
10 - 25%4 - 10%

74 Tumours of the lung - Preinvasive epithelial lesions
programme for lung cancer, any detect-ed lesion, which necessitates furtherinvestigation, can be sampled by fineneedle aspiration or local resection.
Cytology
A diagnosis of AAH cannot be made ona cytology specimen. This issue is dis-cussed further in the chapter on adeno-carcinoma.
Macroscopy and localization
Most lesions are only incidentally foundat microscopy but AAH may be visible onthe cut surface of lung as discrete, greyto yellow foci ranging from less than 1mmto, rarely, over 10mm {408,994}. Most areless than 3mm. AAH is easier to see byflooding the lung surface with water, orafter tissue fixation with Bouin’s fluid{1316}. Occasionally the alveolar spaceswithin the lesion create a stippled patternof depressions. AAH lesions are moreoften found close to the pleura {1434}and in the upper lobes {1429}. It is likelythat most occur as multiple lesions.
Histopathology
AAH is a discrete parenchymal lesionarising often in the centriacinar region,close to respiratory bronchioles. Thealveoli are lined by rounded, cuboidal,low columnar or ‘peg’ cells, which haveround or oval nuclei. Up to 25% of thecells show intranuclear inclusions {1434}and many have light microscopic {1434}and ultrastructural {1022} features ofClara cells and type II pneumocytes.Ciliated and mucous cells are neverseen. Double nuclei are common;mitoses are extremely rare. There issome blending with normal alveolar lin-ing cells peripherally, but most lesionsare well defined. The alveolar walls maybe thickened by collagen, occasionalfibroblasts and lymphocytes. Lesionswith these components in abundanceare unusual. These interstitial changesdo not extend beyond the limits of thelesion, as defined by the epithelial cellpopulation.Cellularity and cytological atypia vary.Many lesions show a discontinuous liningof cells with small nuclei and minimalnuclear atypia. Fewer show a more con-tinuous single cell layer with moderateatypia. Pseudopapillae and tufts may bepresent. Some authors separate lesionsinto low and high grades: LGAAH andHGAAH {1023,1040}. This practice is not
universally accepted, has no known clin-ical significance, its reproducibility isuntested, and this panel does not recom-mend it. The features of AAH fall short ofthose accepted as BAC. This issue isaddressed in the discussion on BAC.The postulated progression of disease,apparent from the increasingly atypicalmorphology, is supported by numerousmorphometric and cytofluorometric stud-ies {1375,1379,1438}. AAH and non-mucinous BAC probably represent acontinuum of progression of pulmonaryalveolar intraepithelial neoplasia.AAH must be distinguished from reactivehyperplasia, secondary to parenchymalinflammation or fibrosis, where the alveo-lar lining cells are not the dominant fea-ture and are more diffusely distributed.Generally, AAH cannot be identified inthe presence of inflammatory or fibrosingdisease. Distinction between more cellu-lar and atypical AAH and BAC is difficult.BAC is generally >10mm in size, has amore pleomorphic, homogeneouscolumnar cell population, which isdensely packed with greater cell-cellcontact, overlap, mild stratification, and,usually, a less graded, more abrupt tran-sition to adjacent alveolar lining cells.True papillae suggest papillary adeno-carcinoma.
ImmunohistochemistryAAH expresses SPA, CEA {1640}, MMPs{1084}, E-cadherin, ß-catenin, CD44v6
and TTF-1. The expression of oncogeneand tumour supressor gene products(TP53, C-ERB2, RB, MST1(p16),WAF1/CIP1 (p21) and FHIT) essentiallyreflects neoplastic progression from AAHto BAC and invasive adenocarcinomas{802,995,1021,1100}. In contrast to thedata on TP53 mutations, TP53 proteinaccumulation seems to occur early in theproposed sequence of events {995}.
Histogenesis
The origin of AAH cells is still unknownbut the differentiation phenotype derivedfrom immunohistochemical and ultra-structural features suggests an alveolarorigin. Surfactant apoprotein {1041}, andClara cell specific 10kDd protein {1021,1379} are expressed in almost all AAHlesions. Ultrastructurally, cytoplasmiclamellar bodies and nuclear branchingmicrotubles, both typical of type II pneu-mocytes {768,1021,1316,1521}, andelectron-dense Clara cell-type granules{1021,1434,1521} are found. AAH cellsare likely derived from a progenitor cellwith the potential for both type II pneu-mocyte and Clara cell differentiation.
Somatic genetics KRAS. Mutations of the K-ras gene, par-ticularly at codon 12, are specific forperipheral lung adenocarcinomas, asopposed to bronchogenic carcinoma,suggesting an alternative pathway ofperipheral lung tumourigenesis {287,
Fig. 1.77 Atypical adenomatous hyperplasia showing localised centriacinar alveolar wall thickening andincreased numbers of alveolar lining cells. From Travis et al. {2024}.

75Atypical adenomatous hyperplasia
402}. K-ras codon 12 mutations arereported in 15-39% of AAH lesions, andup to 42% of concurrent adenocarcino-mas. Most of the time, the K-ras muta-tions are different. One study found K-rascodon 12 mutations in 15% of AAH, 33%of ‘early’ BAC and 24% of ‘advanced’BAC. {1021}, suggesting that K-rascodon 12 mutation is a very early event inthe development of peripheral adenocar-cinoma {1021,2126}.TP53. Abnormalities of the P53 gene(17p), with impaired protein function,promote neoplastic transformation inaffected cells. Many lung adenocarcino-mas show missense mutations of the P53gene with abnormal nuclear protein
accumulation. LOH and mutations of theP53 gene are very rare in AAH comparedwith adenocarcinoma; however p53 pro-tein overexpression is frequent in AAH{1021}. P53 mutation has been demon-strated with increasing frequency in theprogression from AAH, through BAC toearly invasive adenocarcinoma {1836}.LOH Allelic-specific losses at 3p and 9ploci have been detected in AAH {1044,2187}. Some AAH lesions have shownLOH in 9q {51} and both 17q {2187} and17p {51} LOH in the 3p and 9p loci prob-ably occurs at a very early stage andmay represent the earliest and crucialevent in neoplastic transformation, with17p events occurring later.
FHIT. The fragile histidine triad (FHIT)gene (3p) is deleted in many lung carci-nomas {1856}.p16INK4. Loss and inactivation plays animportant role in the pathogenesis oflung carcinoma. However, loss of expres-sion of p16INK4 is relatively rare in bothAAH and adenocarcinoma {1021}. TSC. A recent study on lung adenocar-cinoma with concurrent multiple AAHlesions showed frequent LOH of tuber-ous sclerosis complex (TSC)-associatedregions (TSC1 at 9q and TSC2 in 16p),suggesting that these are candidate locifor tumour suppressor genes in peripher-al lung adenocarcinoma {1949}.Aneuploidy. FISH studies of AAH haveshown frequent aneuploidy of chromo-some 7. The percentages of aneuploidcells and mean chromosome copy num-ber increased from AAH to invasive ade-nocarcinomas, suggesting increasingpolyploidy during malignant change{2245}. Some cases of AAH have beenshown to be monoclonal, suggesting thatit is a true preneoplastic lesion {1475}.
Prognosis and predictive factors
Assuming that AAH is always multifocal,several studies have compared post-operative survival in groups of patientswith, and without AAH {333,1198,1927,1960}. None showed any difference inoutcome.There is no indication for surgical ormedical therapy in patients without can-cer who are incidentally found to haveAAH. In such a clinical setting, carefulfollowup is warranted.
B CAFig. 1.79 Atypical adenomatous hyperplasia. A Transmission electron photomicrograph of a formalin-fixed AAH lesion showing a cuboid AAH cell having many intra-cytoplasmic small inclusion bodies and granules. Note scattered short microvilli on the free surface of the cell, the irregular contour of the nucleus and basal mem-brane. B Light photomicrograph of a thin section of a formalin-fixed, epoxy-resin-embedded AAH lesion showing a cell with an intranuclear inclusion body at themiddle upper portion as well as several binucleated cells. Toluidine blue stain. C Immunostaining with a mouse monoclonal antibody against surfactant apoproteinA (PE10), showing uniformly strong positive staining of the cytoplasm of almost all the AAH cells as well as many nuclear inclusion bodies.
DCFig. 1.78 Atypical adenomatous hyperplasia. A,B Slightly thickened alveolar walls are lined by an intermit-tent single layer of cuboidal cells. Occasional large cells are present. C Cuboidal pneumocytes line thealveolar walls with gaps between the adjacent cells. D Slightly thickened alveolar walls lined by an inter-mittent single layer of cuboidal cells, some with apical cytoplasmic snouts.
BA

76 Tumours of the lung - Preinvasive epithelial lesions
Definition
Diffuse idiopathic pulmonary neuroen-docrine cell hyperplasia (DIPNECH) is ageneralised proliferation of scattered sin-gle cells, small nodules (neuroendocrinebodies), or linear proliferations of pul-monary neuroendocrine cells (PNCs)that may be confined to the bronchialand bronchiolar epithelium, include localextraluminal proliferation in the form oftumourlets, or extend to the developmentof carcinoid tumours. It is sometimesaccompanied by intra- and extraluminalfibrosis of involved airways, but otherpathology that might induce reactivePNC proliferation is absent.
Synonyms
The entity of DIPNECH was not fullyrecognised and named until 1992 {29},but cases with its clinical and pathologi-cal features appear in the literature fromthe early 1950s {570}.
Clinical features
Signs and symptoms DIPNECH may occur at any age, butpresents typically in the fifth or sixthdecades, and is perhaps commoner inwomen {29,74,1150,1317}. The history isone of a very slowly worsening dry coughand breathlessness, often over manyyears, sometimes misdiagnosed as mild
bronchial asthma. Physical examinationusually reveals no signs, but pulmonaryfunction tests show an obstructive ormixed obstructive/restrictive pattern ofimpairment with reduced diffusingcapacity.
Imaging Plain thoracic radiography is often nor-mal, but tomographic scanning reveals amosaic pattern of air trapping, some-times with nodules and thickenedbronchial and bronchiolar walls {1150}.Multiple nodules corresponding totumourlets or carcinoid tumours may bepresent.
Macroscopy and localization
The early lesions of DIPNECH are invisi-ble to the naked eye, but tumourlets andmicrocarcinoids, when present, can bejust discerned as small, gray-white nod-ules, the latter often well-demarcatedand resembling ‘miliary bodies’. Largercarcinoid tumours are firm, homoge-neous, well-defined, grey or yellow-whitemasses. The lesions of DIPNECH usuallyaffect one or both lungs uniformly.
Histopathology
Histopathological examination revealswidespread proliferation of PNCs {29,74,1317}. The earliest lesions comprise
increased numbers of individual cells,small groups, or larger, nodular aggre-gates, confined to the bronchial or bron-chiolar epithelium, the larger lesionsbulging into the lumen, but not breachingthe subepithelial basement membrane.The bronchiolar wall sometimes is fibroti-cally thickened. Bronchiolar occlusionmay occur due to fibrosis and/or PNCproliferation. These are sufficient for thediagnosis of DIPNECH providing otherdefining criteria are met. In particularinflammatory or fibrous lesions that mightcause secondary PNC hyperplasia arenot seen. However, more advancedlesions are often present. These developwhen the proliferating PNCs breakthrough the basement membrane toinvade locally, developing a conspicuousfibrous stroma to form small (2-5 mm)aggregates traditionally known as‘tumourlets’. This proliferation of PNCs issometimes accompanied by intra- andextramural fibrosis of the involved air-ways that often obliterates them, but thesurrounding lung is otherwise unremark-able. Once PNCs reach a size of 5mm orgreater, they are classified as carcinoids.
Differential diagnosis Clinically and on imaging, DIPNECH maybe indistinguishable from other diffuselung diseases characterised by cough,
Diffuse idiopathic pulmonary
neuroendocrine cell hyperplasia
J.R. GosneyW.D. Travis
Fig. 1.80 Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia. A The bronchiolar epithelium is almost entirely replaced by proliferating neuroendocrinecells. B Hyperplastic neuroendocrine cells form a nest at the base of the bronchiolar epithelium. From Travis et al {2024}.
BA

77Diffuse idiopathic pulmonary neuroendocrine cell hyperplasia
breathlessness, mixed obstructive/restrictive pulmonary impairment and anodular pattern of pulmonary infiltration,so that the diagnosis is usually impossi-ble to make without recourse to biopsy.Histopathologically, DIPNECH must bedistinguished from the PNC proliferationthat may accompany a variety of pul-monary conditions, particularly chronicinflammatory diseases such asbronchiectasis and chronic lung abscess{717}; in the latter situation, progressionof the proliferation to carcinoid tumoursdoes not occur. DIPNECH must also bedistinguished from the proliferation ofPNCs not uncommonly seen adjacent toperipheral carcinoids {29,1317}.
Histogenesis
As with neuroendocrine neoplasms aris-ing in the lungs, the origin of the prolifer-ating PNCs that characterize DIPNECHis likely to be a yet-to-be-defined uncom-mitted precursor cell that is stimulated byunknown influences to differentiate along
a neuroendocrine line. However, thePNCs that proliferate in DIPNECH arefound in normal lungs of adults {719,1141}.
Somatic genetics
There are no genetic markers of DIP-NECH such that it might be possible todistinguish it genetically from the limited,reactive, reversible proliferative responseof PNCs that occurs after pulmonaryinjury. It is of interest, however, that allel-ic imbalance at the 11q13 region thatclosely approximates to the MEN1tumour suppressor gene appears to berare in tumourlets, but is present in themajority of carcinoid tumours {581}.
Prognosis and predictive factors
DIPNECH is a slowly progressive condi-tion with a benign course spanning manyyears. Associated carcinoid tumours areindolent and atypical features have notbeen described. There are no predictivehistologic or genetic data for DIPNECH.

78 Tumours of the lung - Benign epithelial lesions
Definition
A papillary tumour consisting of delicateconnective tissue fronds with a squa-mous epithelial surface. Squamous papil-lomas can be solitary or multiple and canbe exophytic or inverted.
ICD-O codes
Squamous cell papilloma 8052/0Exophytic 8052/0Inverted 8053/0
Epidemiology
Solitary squamous papillomas are veryrare representing less than 0.50% oflung tumours at one large institution{1612}. Exophytic lesions far outnumberthe inverted growth pattern {592}.Solitary squamous papillomas are seenpredominantly in men, with a medianage of 54 years {592}. Juvenile and adultlaryngotracheal papillomatosis rarelyinvolve the lower respiratory tract arealways related to laryngotracheal papil-lomatosis {1223}.
Etiology
An association with human papillomavirus (HPV) subtypes 6 and 11 suggestsa possible pathogenetic role for the virus{592}. Human papilloma virus subtypes16,18 and 31/33/35 in squamous papillo-mas associated with carcinomas and insquamous cell carcinomas have beenreported, suggesting that HPV infectionmight be related to tumoural progression{139,1611,1612}. More than half ofpatients are tobacco smokers, but an eti-ologic role has not been established{592,1937}.
Localization
Papillomas are endobronchial.
Clinical features
While up to one-third of lesions are inci-dental radiographic findings, patientsmost often present with obstructivesymptoms. Computed tomographyscans demonstrate a small endo-bronchial protuberance or nodular air-way thickening. Involvement of distal air-
ways may lead to nodular opacitiesand/or thin-walled cavity nodules {2213}.An endobronchial biopsy may be diag-nostic, but distinction from well-differenti-ated squamous cell carcinoma can bedifficult, especially with superficial tissuefragments. Bronchoscopic cytologicspecimens will only demonstrate thesquamous nature of the lesion.Parakeratotic cells, cytologic atypia andviral cytopathic effect should not be mis-interpreted as invasive carcinoma{1677}.
Macroscopy
Solitary squamous papillomas arisefrom the wall of either mainstem bronchior major subdivisions and appear ascauliflower-like tan-white soft to semi-firm excrescences protruding intobronchial lumens. Tumours range from0.7-9.0 cm with a median of 1.5 cm.Distal airways may be bronchiectaticwith secondary atelectasis and consoli-dation {965}.
Tumour spread and staging
Squamous papillomas may recur at theiroriginal site and laryngotracheal papillo-matosis can spread into the lower respi-ratory tract. It has been suggested thatelectrical or laser fulguration is responsi-ble for alveolar parenchymal seeding.
Histopathology
Squamous papillomas are composed ofa loose fibrovascular core covered bystratified squamous epithelium.Exophytic lesions feature orderly squa-mous maturation from the basal layer tothe superficial flattened and oftentimeskeratinized cells. Acanthosis may beprominent. While non-keratinized epithe-lium may resemble transitional epitheli-um, the squamous nature of these cellshas been demonstrated ultrastructurallyand use of this term is discouraged. Over20% of solitary squamous papillomasfeature wrinkled nuclei, binucleate formsand perinuclear halos, i.e., koilocytosisrelated to HPV infection {592}. Scattered
D.B. FliederF. Thivolet-BejuiH. Popper
Squamous cell papilloma
Fig. 1.81 Exophytic squamous papilloma. Mature squamous epithelial cells are growing in an exophytic pap-illary pattern on the surface of thin fibrovascular cores. The papilloma is attached to the underlyingbronchial wall by a stalk. .

79Squamous cell papilloma
dyskeratotic cells, large atypical cellsand occasional mitotic figures above thebasal layer can be seen. Dysplasiashould be graded according to the WorldHealth Organization classification {2024}.Squamous cell carcinoma infrequentlyarises in solitary squamous papillomas{1611,1612}.Inverted lesions feature both exophyticand random invaginations of squamousepithelium. The basal lamina investingthe endophytic nests is continuous withthe basal lamina underlying the surfaceepithelium. Basal cells are perpendicularto the basement membrane while centralcells are parallel and whorling. Tumourcan involve adjacent seromucinousglands.Alveolar parenchymal involvement mani-fests as either well circumscribed solidintraalveolar nests of cytologically blandnon-keratinizing squamous cells sur-rounded by hyperplastic type II pneumo-cytes or large cysts lined by similarbenign epithelium. Lower respiratorytract involvement with laryngotrachealpapillomatosis is morphologically similarwith the exception that virtually all lesionsfeature viral cytopathic effect. Neitherimmunohistochemical nor in situhybridization studies are helpful in diag-nosis.
Differential diagnosisInflammatory endobronchial polyps mayshow focal squamous metaplasia butgenerally have voluminous granulationtissue-like stroma and subepithelialdense lymphoplasmacytic infiltrates witha lack of continuous proliferative epithe-lial surface. Well-differentiated squa-mous cell carcinoma can be entirelypapillary and endobronchial, but usuallydemonstrates malignant cytologic fea-tures if not also stromal invasion and/orangiolymphatic invasion. Entrappedglands within the papillary stalk of abenign papilloma should not be mistakenfor invasion. Inverted papillomas with
even minimal cytologic atypia may beindistinguishable from invasive squa-mous cell carcinoma. Parenchymaldestruction, cellular pleomorphism, lossof maturation, prominent dyskeratosisand hyperkeratosis favour a diagnosis ofcarcinoma.
Precursor lesions-Histogenesis
Squamous papillomas most likely arisefrom metaplastic respiratory epithelium.
Prognosis and predictive factors
While solitary squamous papillomas areconsidered benign lesions, the presenceof focal cytologic atypia, a recurrencerate approaching 20% and reports ofsquamous cell carcinomas arising atpapilloma excision sites indicate a lowmalignant potential. Thus, lesions should
be completely excised when feasible.Human papilloma virus subtyping maybe prognostically significant as condylo-matous papillomas have malignantpotential {1611,1612,1937,2030}. Solita -ry papillomas may progress to papillo-matosis, but lower respiratory tractinvolvement usually represents spread ofjuvenile or rarely adult laryngotrachealpapillomatosis. Papillomatosis may belethal even in the absence of malignanttransformation owing to obstructive com-plications. Increased topoisomerasealpha II and p53 expression along withreduced RB gene protein product andp21 expression may serve as markers oftransformation to so-called invasivepapillomatosis and squamous cell carci-noma {753}.
DCFig. 1.82 A Squamous cell papilloma. Acanthotic epithelium features parakeratosis and dyskeratotic cells.B Squamous cell papilloma. In situ hybridization staining for human papillomavirus subtypes 6/11.C Inverted squamous cell papilloma. Mature squamous epithelial cells are growing in an inverted papillarypattern within the lumen of this bronchus. From Flieder et al {592} and Travis et al. {2024}. D Inverted squa-mous cell papilloma. Mature squamous cells are growing in an papillary configuration with an inverted pat-tern of growth. From Flieder et al. {592} and Travis et al. {2024}
BA

80 Tumours of the lung - Benign epithelial lesions
Definition
A papillary tumour lined by ciliated ornon-ciliated columnar cells, with varyingnumbers of cuboidal cells and gobletcells.
ICD-O code 8260/0
Synonym
Columnar cell papilloma
Epidemiology
Glandular papillomas are exceedinglyrare. An equal sex distribution and medi-an age of 68 years are establishedbased on the few reported cases{85,118,592,1858}.
Etiology
No specific etiologies have been impli-cated in the evolution of glandular papil-lomas.
Localization
Endobronchial
Clinical features and diagnostic proce-
dures
Individuals present with obstructivesymptoms including wheezing orhaemoptysis {592}; a minority areasymptomatic and radiographic studiesdemonstrate either a small endo-bronchial protuberance or nodular air-way thickening. While bronchoscopicbiopsy can identify a central lesion, com-plete excision is necessary for definitivediagnosis.
Macroscopy
Glandular papillomas are white to tanendobronchial polyps that measure from0.7-1.5 cm. Bronchiolar lesions canappear solid without obvious papillaryfronds.
Histopathology
Central lesions have relatively non-inflamed thick arborizing stromal stalkswith prominent thin-walled blood vesselsor hyalinization covered by glandularepithelium. Necrosis is absent.Pseudostratified or columnar epitheliumlacks micropapillary tufts and cellulardesquamation. Epithelium can be non-ciliated or ciliated, cuboidal or columnaror a mixture and interspersed mucin-richcells can be seen. The cytoplasm can beclear and the nuclei lack atypia andmitoses. Peripheral lesions demonstrateattachment to bronchiolar mucosa andcontain scattered ciliated cells.
Differential diagnosisPrimary and metastatic papillary adeno-carcinomas feature epithelial crowding,malignant cytologic features and often
show bronchial wall invasion.Inflammatory polyps and the papillaryvariant of mucus gland adenoma lacktrue fibrovascular stromal cores andinflammatory polyps lack a proliferativeepithelial component. Papillary adeno-mas are parenchymal lesions withoutattachment to airways and usuallydemonstrate type II pneumocyte differ-entiation.
Prognosis and predictive factors
Glandular papillomas are benigntumours that may recur following incom-plete resection, but neither extension intoalveolar parenchyma nor malignanttransformation has been reported {85,118,592,1858}.
D.B. FliederF. Thivolet-BejuiH. Popper
Glandular papilloma
Fig. 1.83 Glandular papilloma. Columnar epithelial cells proliferate in a papillary fashion along the surface offibrovascular cores From Flieder et al. {592} and Travis et al. {2024}.

81Mixed squamous cell and glandular papilloma
Definition
Mixed squamous and glandular papillo-ma is an endobronchial papillary tumourshowing a mixture of squamous andglandular epithelium. One-third of theepithelium should be composed of thesecond epithelial type.
ICD-O code 8560/0
Synonyms
These tumours were formely called tran-sitional papillomas {1072}.
Epidemiology
Mixed papillomas are exceedingly rarewith seven cases reported in the world lit-erature. An equal sex distribution andmedian age of 64 years are compiledfrom the few reported cases {592,1858}.
Etiology
No specific etiologies have been impli-cated in the evolution of mixed papillo-mas. Human papilloma virus has notbeen detected in the few cases studied.60% of patients are tobacco smokers,but an etiologic role has not been estab-lished {592}.
Clinical features and diagnostic proce-
dures
Individuals present with obstructivesymptoms {592,1858}. While endo-bronchial biopsy can demonstrate theneoplastic nature of a central lesion,complete excision is necessary for defin-itive diagnosis.
Macroscopy
Endobronchial lesions are tan to red,polypoid and measure from 0.2-2.5 cm.A lobar preference is not seen.
Histopathology
Endobronchial lesions are composed offibrovascular cores with scattered lym-phoplasmacytic infiltrates lined by squa-mous and glandular epithelium.Pseudostratified ciliated and nonciliatedcuboidal to columnar cells with occa-sional mucin-filled cells are distinct fromacanthotic and focally keratinizing squa-
mous epithelium. Squamous atypia rang-ing from mild to severe dysplasia can beseen but viral cytopathic change has notbeen reported. Glandular atypia andnecrosis are not seen.
Differential diagnosisThis is the same as for pure squamousand glandular papillomas.
Prognosis and predictive factors
Complete resection appears to be cura-tive {592}.
D.B. FliederF. Thivolet-BejuiH. Popper
Mixed squamous cell and
glandular papilloma
Fig. 1.84 Mixed squamous cell and glandular papilloma. Flieder et al. {592} and Travis et al. {2024}.

82 Tumours of the lung - Benign epithelial lesions
Definition
A solitary well-circumscribed peripherallung tumour consisting of a network ofspaces lined by a simple low cuboidalepithelium associated with a variably thinand inconspicuous to thick spindle cell-rich stroma, sometimes with a myxoidmatrix.
ICD-O code 8251/0
Synonyms
This tumour has been mistakenly report-ed under the term lymphangioma.
Epidemiology
This tumour is very rare. The age range is39-74 years (mean, 53 years), with aslight female predominance {194,252,624,792,1054,1297,1464,1514,1782,1811,1822,2219}.
Localization
Alveolar adenoma has been reported inall five lobes with a predilection for theleft lower lobe {1116}. Most tumours areintraparenchymal peripheral or subpleur-al although a hilar location has beennoted.
Clinical features
Patients are usually asymptomatic andthe tumour is an incidental radiographic
finding. {1116}. Chest X-ray and CTappearances are those of a well circum-scribed, homogenous, non-calcified,solitary mass, although one report,unconfirmed histologically, raises thepossibility of multifocality {624}. Contrastenhancement on CT and MRI displayscystic spaces with central fluid and rimenhancement {624}.
Macroscopy
Tumours measure from 0.7-6.0 cm andfeature well demarcated smooth, lobulat-ed, multicystic, soft to firm and pale yel-low to tan cut surfaces {252}.
Histopathology
Alveolar adenomas are well-circum-scribed unencapsulated multicysticmasses with ectatic spaces filled witheosinophilic granular material. Spacesare lined by cytologically bland flattened,cuboidal and hobnail cells. Cysticspaces are usually larger in the centre ofthe lesion and squamous metaplasia canbe seen. The myxoid and collagenousinterstitium varies in thickness and con-tains scattered to dense groups of cyto-logically bland spindle cells.
Immunohistochemistry Epithelial lining cells are type 2 pneumo-cytes that stain for broad-spectrum ker-
atin, CEA, surfactant protein and TTF-1while stromal cells show focal positivityfor smooth-muscle actin and muscle-specific actin and negativity for desmin ,TTF-1, proSPB, proSPC and CC10 {252}.Low proliferation indices in both theepithelial and mesenchymal cells havebeen reported {194,1297}.
Electron microscopyBy electron microscopy, lining cells con-tain lamellar bodies, blunt surfacemicrovilli and cell junctions of the zonulaadherens type.
Differential diagnosis
Lymphangioma, sclerosing heman-gioma, and adenocarcinoma includingbronchioloalveolar carcinoma comprisethe differential diagnosis. Cytokeratinpositivity of cells lining the cystic spacesdifferentiates this lesion from a lymphan-gioma {252}. The single architecturalgrowth pattern, large ectatic spaceslacking blood and stromal cell negativityfor TTF-1 discern the tumour from a scle-rosing haemangioma {252,1464}. Thewell-circumscribed growth pattern, lackof lepidic growth and cytologic atypiadiscern alveolar adenoma from bronchi-oloalveolar carcinoma {252}. Primary andmetastatic spindle cells tumours may
L.M. BurkeD.B. Flieder
Alveolar adenoma
Fig. 1.85 Alveolar adenoma. A This tumour nodule is circumscribed, but not encapsulated. There are large cysts and smaller spaces resembling alveoli. From Burkeet al. {252} and Travis et al {2024}. B This whole-mount section demonstrates the well circumscribed nature of the multicystic neoplasm.
BA

83Alveolar adenoma
also become cystic, with foci resemblingalveolar adenoma.
Histogenesis
This lesion appears to represent a com-bined proliferation of alveolar pneumo-cytes and septal mesenchyme {252,1514}.
Somatic genetics
The neoplastic nature of alveolar adeno-ma was demonstrated in a cytogeneticstudy of one tumour. A pseudodiploidkaryotype, 46,XX, add (16) (q24), wasdescribed and fluorescence in situhybridization studies revealed the add(16) (q24) to be a der(16)t(10;16)(q23;q24) {1682}.
Prognosis and predictive factors
Alveolar adenomas are benign tumoursand surgical excision is curative.
Fig. 1.86 Alveolar adenoma. A Cystic spaces of varying sizes are filled with eosinophilic fluid and PAS-pos-itive granular material. Intervening stroma is focally prominent. B Alveolus-like spaces are lined by flat orcuboidal pneumocytes on the surface of a thin layer of vascular connective tissue resembling an alveolarwall. A few macrophages are present within the alveolar-like spaces. From Burke et al. {252} and Travis etal. {2024}.
A
B

84 Tumours of the lung - Benign epithelial lesions
Definition
Papillary adenoma is a circumscribedpapillary neoplasm consisting of cytolog-ically bland cuboidal to columnar cellslining the surface of a fibrovascular stro-ma.
ICD-O code 8260/0
Synonyms
Bronchiolar adenoma, papillary adeno-ma of type II pneumocytes, type II pneu-mocyte adenoma, adenoma of type IIpneumocytes, peripheral papillarytumour of type II pneumocytes.
Epidemiology
The papillary adenoma is a rare tumourwith less than 20 cases reported.Individuals range in age from 7-60 years(mean 32 years) and males predominate{484,555,579,635,808,1103,1376,1483,1858,2185}.
Etiology
The etiology in humans is unknown but asimilar lesion can be chemically inducedin mice {974}.
Localization
The tumour has no lobar predilection andinvolves alveolar parenchyma but not air-ways {484,555,579,635,808,1103,1376,1483,1858,2185}.
Clinical features
Individuals are usually asymptomaticand the tumour is incidentally noted onchest radiographs as a well-defined pul-monary nodule {484,555,579,635,808,1376,1483,1858,2185}.
Macroscopy
Grossly, the tumour is a well defined,sometimes encapsulated, soft, spongy tofirm mass with a granular gray white/brown cut surface measuring from 1.0-4.0 cm {484,555,579,635,808,1376,1483,1858,2185}. Although generallyseparate from the airways, protrusion intothe lumen of a small bronchiole canoccur {1483}.
Histopathology
Papillary adenomas are generally wellcircumscribed but infiltrative growth hasbeen described. The tumour has a papil-lary growth pattern sometimes mixedwith more solid areas. Focally inflamedfibrovascular cores are lined withcuboidal to columnar epithelial cells withround to oval nuclei. Cilitated {635,1376}and oxyphilic cells {555,579} can beseen. Occasional eosinophilic intranu-clear inclusions are noted but nuclearatypia and mitosis are rare to absent.Intracellular mucin is not present.
Immunohistochemistry and electronmicroscopyBoth type II and Clara cells can be foundin papillary adenomas resulting in posi-tive staining for broad-spectrum cytoker-atin, Clara cell protein, TTF-1 and surfac-tant apoprotein as well as CEA.Neuroendocrine markers are negative{484,555,579,635,808,1376,1483,1858,2185}. Ultrastructurally lamellar bodies,surface microvilli, with membrane boundelectron dense deposits have beenobserved {635,2185}.
Differential diagnosisSclerosing haemangioma demonstratesvaried architectural growth patternsincluding hemorrhagic, sclerotic andsolid tumour cell growth {488}. Alveolaradenoma does not display a papillarygrowth pattern, Clara cells or ciliatedcells {252}. Papillary adenocarcinomasincluding metastatic thyroid carcinomaand bronchioloalveolar carcinoma havea greater degree of cellular proliferationwith micropapillary tufts and nuclearpleomorphism. Papillary carcinoidtumour has granular cytoplasm and afinely granular chromatin pattern.
Histogenesis
Pulmonary papillary adenoma is thoughtto arise from a multipotential stemcell/immature bronchioloalveolar cell thatdifferentiates towards type II pneumo-cytes, Clara cells or ciliated respiratoryepithelial cells {555,635,1483,1858}.
Prognosis and predictive factors
Papillary adenoma is benign and surgi-cal excision is curative. {484,555,635,808,1103,1376,1483,2185}.
D.B. FliederPapillary adenoma
Fig. 1.87 Papillary adenoma. Cuboidal epithelial cells line the surface of the fibrovascular cores. From Traviset al. {2024}.

85Mucous gland adenoma
Definition
A benign predominantly exophytictumour of the tracheobronchial seromuci-nous glands and ducts featuring mucus-filled cysts, tubules, glands and papillaryformations lined by a spectrum of epithe-lium including tall columnar cells, flat-tened cuboidal cells, goblet cells, onco-cytic cells and clear cells.
ICD-O code 8480/0
Synonyms
Bronchial cystadenoma, mucous celladenoma, polyadenoma, bronchial ade-noma arising in mucous glands
Epidemiology
The tumour is extremely rare {1561}.There is no sex predilection and tumourshave been reported in both children andthe elderly with a mean age of 52 years{543,1077}.
Localization
Most tumours are central but peripherallesions have been described {543,2117}.
Clinical features
Individuals present with signs and symp-toms of obstruction. Radiographic stud-ies demonstrate a coin lesion. CT scansmay show a well-defined intraluminalmass with air-meniscus sign {1109}.Excision is usually required for definitivediagnosis {472}.
Macroscopy
Grossly, white-pink to tan, smooth andshiny tumours with gelatinous mucoidsolid and cystic cut surfaces measurefrom 0.7-7.5 cm (mean 2.3 cm) {543}.
Histopathology
Mucous gland adenomas are well-cir-cumscribed, predominantly exophyticnodules above the cartilaginous plates ofthe bronchial wall. Tumours comprisenumerous mucin-filled cystic spaces andnon-dilated microacini, glands, tubulesand papillae may also be seen. Neutraland acid-mucin filled cysts are lined by
cytologically bland columnar, cuboidal orflattened mucus secreting cells.Oncocytic and clear cell change canalso be seen as well as focal ciliatedepithelium. Hyperchromasia, pleomor-phism and mitoses are rare while squa-mous metaplasia only involves overlyingsurface respiratory epithelium. Bands ofspindle cell-rich stroma may be hyalin-ized or with prominent lymphocytesand/or plasma cells.
Immunohistochemistry and EMImmunohistochemistry demonstratessimilar staining to non-neoplasticbronchial glands with epithelial cells pos-itive for EMA, broad-spectrum cytoker-atins and CEA. Focal stromal cell positiv-ity for broad-spectrum keratins, smooth-muscle actin and S-100 protein indicatea myoepithelial component. Proliferatingcell nuclear antigen and Ki-67 stainingperformed in several cases demonstraterare tumour cell positivity {543}.Mucinous and myoepithelial cell typeshave been identified by electronmicroscopy {543,804}.
Differential diagnosisLow-grade mucoepidermoid carcinomaincluding the papillary and cystic vari-ants may closely mimic mucus glandadenoma. Despite architectural similari-ties, the presence of squamous andintermediate cells confirms mucoepider-moid carcinoma. Mucinous cystadeno-mas are located in the lung peripheryand consist of a cystic lesion filled withmucus and lined by uniform, blandmucus cells. Adenocarcinomas are usu-ally infiltrative and feature cytologic atyp-ia, mitoses and necrosis.
Histogenesis
The tumour is postulated to arise from themucus glands of the bronchus.
Prognosis and predictive factors
Mucus gland adenomas are benign andconservative lung-sparing bronchoscop-ic or sleeve resection is recommended{543}.
D.B. FliederF. Thivolet-BejuiH. Popper
Mucous gland adenoma
DCFig. 1.88 Mucous gland adenoma. A Endobronchial mass is comprised of numerous mucin-filled cysticspaces, microacini, glands, tubules and papillae. B Papillary fronds are a minor architectural pattern. CNeutral and acid-mucin filled cysts are lined by cytologically bland columnar, cuboidal or flattened mucussecreting cells. D Glands lined by columnar epithelium with small basally oriented nuclei and abundant api-cal mucinous cytoplasm. From Travis et al. {2024}.
BA

86 Tumours of the lung - Benign epithelial lesions
Definition
A tumour with both epithelial and con-nective tissue differentiation consisting ofglands intermingled with myoepithelialcells in a myxoid and chondroid stroma.
ICD-O code 8940/0
Synonym
Benign mixed tumour
Epidemiology
Although rare, pulmonary pleomorphicadenoma has been reported in individu-als ranging from 11-74 years, but mostoften affects those in their sixth and sev-enth decades of life. A gender predilec-tion is not seen {803,1364,1727,1958}.
Etiology
No specific etiologies have been impli-cated in the evolution of the tumour.
Localization
Most tumours are centrally located endo-bronchial polypoid masses but peripher-al lesions occur {803,1364,1727,1958}.
Clinical features
Tumours most often present with obstruc-tive symptoms {1364}. A minority oflesions are incidental X-ray findingsdemonstrating either discrete endo-bronchial mass with minimal bronchialwall thickening or well-circumscribedperipheral nodules. Cytologic and bron-choscopic biopsy material can suggestthe diagnosis but complete excision isrequired for a definitive diagnosis.
Macroscopy
Tumours range in size from 1.5-16 cm{803,1364,1727,1958}. Typically, endo -bron chial lesions are usually associatedwith a major or secondary bronchus andare polypoid, with some degree of lumi-nal occlusion. Peripheral lesions are notintimately associated with airways.Tumours are circumscribed, unencapsu-lated with a gray-white, rubbery or myx-oid cut surface.
Histopathology
Pulmonary pleomorphic adenomas arebiphasic like their salivary gland counter-part, but do not often feature either aprominent glandular component or chon-droid stroma. Rather, tumours exhibit fea-tures of the so-called “cellular mixedtumour” manifesting sheets, trabeculaeor islands of epithelial and/or myoepithe-lial cells and a myxoid matrix. Whenpresent, ducts composed of an outerlayer of myoepithelial cells and an innerlayer of epithelial cells containing smallamounts of periodic acid-Schiff (PAS)-positive luminal secretion. Mitotic activity,pleomorphism and necrosis are unusual.
ImmunohistochemistryDuctal and myoepithelial cells stain forboth low-molecular weight and broadspectrum keratin while myoepithelial andstromal cells are positive for vimentin,smooth-muscle actin and glial fibrillaryacidic protein. S-100 protein immunore-activity can also be seen in both epithe-lial and myoepithelial cells {1364,1727}.
Differential diagnosis
Pulmonary pleomorphic adenoma mustbe discerned from head and neck oreven breast metastasis by thorough clin-ical history and examination. A solitarytumour associated with a cartilage-bear-ing airway suggests a pulmonary origin.The morphologic differential diagnosisincludes hamartoma, pulmonary blas-toma and carcinosarcoma. Hamartomasusually show cartilage and other mes-enchymal elements while the lattertumours feature obviously malignant stro-ma and epithelium.
Histogenesis
This neoplasm with epithelial and con-nective tissue differentiation is regardedas arising from the submucosal bronchialgland epithelium. However, peripheraland subpleural locations unrelated tobronchi raise the possibility that thetumour may originate from a primitivestem cell.
Prognosis and predictive factors
Pleomorphic adenomas of the lungexhibit a spectrum of clinical behaviorranging from benign to malignant. On thebasis of several studies, small well-cir-cumscribed lesions are cured with lobec-tomy while larger, infiltrative or poorly cir-cumscribed lesions tend to recur andmetastasize. Tumours with greater than 5mitoses per 10 high-power fields may beassociated with aggressive behavior{1364}, but in the absence of malignantcytology, necrosis and angiolymphaticinvasion such lesions should be diag-nosed as benign pleomorphic adenomarather than carcinoma ex pleomorphicadenoma.
Other benign salivary gland-like tumours
Well-defined salivary gland tumoursincluding monomorphic adenoma, onco-cytoma, and myoepithelioma areextremely rare primary lung tumours{429,1812,1883,1977,2037}. Adenomy -oepithelioma {2037} is discussed underepimyoepithelial carcinoma in the sec-tion on malignant salivary gland tumours.In the absence of known salivary glandprimaries and exclusion of mimics suchas metastatic and primary malignanciesincluding typical carcinoid tumour, thesesolitary lesions in the lung can be diag-nosed as primary lung neoplasms.
D.B FliederF. Thivolet-BejuiH. PopperC. Moran
Pleomorphic adenoma
Fig. 1.89 Pleomorphic adenoma. Sheets of epithe-lial and/or myoepithelial cells are embedded in amyxoid matrix.

87Mucinous cystadenoma
Definition
A localized cystic mass filled with mucinand surrounded by a fibrous wall lined bywell-differentiated columnar mucinousepithelium.
ICD-O code 8470/0
Epidemiology
This exceedingly rare tumour is mostoften seen in both men and women intheir sixth and seventh decades of life{730,1067,1068,1699}. Most reportedcases occur in tobacco-smokers but nospecific etiologies have been implicatedin the evolution of the tumour {730,1067,1068,1699}.
Localization
These tumours are usually located in theperipheral lung.
Clinical features and diagnostic proce-
dures
Mucinous cystadenoma are asympto-matic lesions that present as incidentalrounded well demarcated masses on X-ray and CT scans {1067,1068}. Fine nee-dle aspirates and transbronchial biop-sies may sample mucin or goblet cells,but a definitive diagnosis requires surgi-
cal excision and complete histologicsampling.
Macroscopy
Grossly, unilocular mucous-filled cystsmeasure from less than 1.0-5.0 cm andare not associated with airways. Cystwalls are thin (0.1 cm) and lack muralnodules {1067,1068}.
Tumour spread and staging
One instance of tumour seeding the pari-etal pleura (so-called pleuralpseudomyxoma) has been reported{730}.
Histopathology
Microscopically, the cystic lesion is filledwith mucus and the fibrous connectivetissue wall is lined by a discontinuouslayer of low cuboidal to tall columnar,mucin-secreting epithelium. Lining cellsfeature basally located hyperchromaticnuclei and abundant cytoplasmic mucin.Focal cellular stratification, papillaryinfoldings and rare mitoses may be seen,but micropapillary fronds, necrosis andovert cytologic atypia are by definitionabsent. Foreign body giant cell reactionassociated with extravasated mucus andstromal chronic inflammation are promi-
nent adjacent to areas of denudedepithelium.
Immunohistochemistry
Lesional epithelium is broad-spectrumkeratin positive, rarely CEA positive andsurfactant-associated protein A negative{1067,1699}. Proliferating cell nuclearantigen and Ki-67 antibodies stain lessthan 10% and 5% of lesional cell nuclei,respectively {1699}.
Differential diagnosis
Mucinous cystadenoma should not beconfused with mucinous cystadenocarci-noma or the colloid mucinous variant ofadenocarcinoma. Mucus extravasation,lepidic spread of epithelium beyond thefibrous capsule or into adjacent lunginvasion or cytologic anaplasia indicatesadenocarcinoma. Other considerationsinclude mucinous bronchioloalveolarcarcinoma, and non-neoplastic lesions,such as congenital cystic adenomatoidmalformation as well as developmentaland post-infectious bronchogenic cysts.
Prognosis and predictive factors
Mucinous cystadenomas are benigntumours. Complete excision is curative.
D.B. FliederF. Thivolet-BejuiH. PopperB. Pugatch
Mucinous cystadenoma
Fig. 1.90 Mucinous cystadenoma. A A subpleural cystic tumour is surrounded by a fibrous wall and contains abundant mucus. From Travis et al. {2024}. B Columnarepithelial cells line the wall of the cyst. Most of the nuclei are basally oriented but there is focal nuclear pseudostratification. The apical cytoplasm is filled withabundant mucin. From Travis et al. {2024}.
BA

88 Tumours of the lung - Lymphoid / histiocytic tumours
Definition
Pulmonary marginal zone B-cell lym-phoma of mucosa-associated lymphoidtissue (MALT) is an extranodal lymphomacomprising morphologically heteroge-neous small B-cells, cells resemblingmonocytoid cells, and/or small lympho-cytes, with scattered immunoblasts andcentroblasts-like cells. There is plasmacell differentiation in a proportion of thecases. The infiltrate is in the marginalzone of reactive B-cell follicles andextends into the interfollicular region. Theneoplastic cells typically infiltrate thebronchiolar mucosal epithelium, forminglymphoepithelial lesions.
ICD-O code 9699/3
Synonyms
The term pseudolymphoma is consid-ered obsolete, and lymphocytic intersti-tial pneumonia is now limited to inflam-matory lesions. Terms such as BALT(bronchial associated lymphoid tissue)lymphoma and BALTOMA should nowalso be avoided.
Historical annotation
Primary pulmonary non-Hodgkin’s lym-phoma was originally defined as a lym-phoma that presented primarily in thelungs, with or without hilar node involve-ment but without clinical evidence of dis-ease elsewhere {1731}. Those tumours
not fulfilling these criteria were classifiedas pseudolymphomas, but this term isnow obsolete as most of these cases arenow believed to be neoplastic and therare localized reactive lesions are classi-fied as nodular lymphoid hyperplasia.Early series of pulmonary lymphomawere categorised according to lymphnode classifications {1063,2041}, but it isnow accepted that the majority of casesarise from bronchial mucosa-associatedlymphoid tissue (MALT) {21,137,407,577,1104,1176,1467}. The REAL classifica-tion currently recommends the term‘Marginal Zone B-Cell Lymphoma of theMucosa-Associated Lymphoid Tissue(MALT) Type’ for those with ‘low-grade’features and ‘diffuse large B-cell non-Hodgkin’s lymphoma’ for those with‘high-grade’ features.
Epidemiology
Approximately 70-90% of primary pul-monary lymphomas are marginal zonelymphomas of MALT type but theyaccount for less than 0.5% of all primarylung neoplasms and a similarly low pro-portion of all lymphomas {21,1063,1176}.Patients tend to be in their fifth, sixth orseventh decades, with a slight male pre-ponderance. Presentation in youngerpatients is rare without underlyingimmunosuppression {21,137,407,577,1176,1467}.
Etiology
Pulmonary marginal zone B-cell lym-phomas of MALT type are thought toarise in acquired MALT secondary toinflammatory or autoimmune processes.Bronchial MALT is not thought to be anormal constituent of the humanbronchus, and it likely develops as aresponse to various antigenic stimuli, forexample smoking {1659} and autoim-mune disease {1469}. However, a com-mon association, as seen between gas-tric lymphomas of MALT origin andHelicobacter pylori infection {2171}, hasnot been found. The etiology of mostcases of pulmonary MALT lymphoma isnot known.
Localization
Tumours have no zonal or lobar predis-position, are typically peripheral in loca-tion, and range from solitary nodules todiffuse bilateral disease (the pattern thatmimics lymphocytic interstitial pneumo-nia).
Clinical features
The most common presentation is amass discovered on a chest radiographin an asymptomatic patient, with sympto-matic patients presenting with cough,dyspnoea, chest pain and haemoptysis.Previous or synchronous MALT lym-phomas at other extranodal sites are notuncommon. A monoclonal gammopathymay be present, but if present may indi-cate pulmonary involvement by lympho-plasmacytic lymphoma in a patient withWaldenstrom macroglobulinemia. Rarelypatients manifest systemic or ‘B’ symp-toms.Chest radiographs and high resolutioncomputerized tomograph (HRCT) scan-ning show multiple, solitary masses oralveolar opacities with associated airbronchograms. HRCT scans may alsoshow airway dilatation, positiveangiogram signs and haloes of groundglass shadowing at lesion margins{1014}. Diagnosis can be made by broncho-scopic or transbronchial biopsy,although not infrequently a surgical lungbiopsy will be required. Broncholaveolarlavage and fine-needle aspiration biopsyspecimens can be diagnostic of lym-phoma if a clonal B-cell population canbe demonstrated, but the specific type oflymphoma can rarely be diagnosed bythese techniques.
Macroscopy
Nodular areas of pulmonary involvementby pulmonary marginal zone B-cell lym-phomas of MALT type typically show aconsolidative mass that is yellow tocream in colour, not dissimilar in textureto the cut surface of a lymph nodeinvolved by lymphoma. Rarely, tumoursare focally cystic.
A.G. NicholsonN.L. Harris
Marginal zone B-cell lymphoma of the
mucosa-associated lymphoid tissue
(MALT) type
Fig. 1.91 Marginal zone B-cell lymphoma of MALT.Macroscopy. A diffuse consolidation of the middlelobe with a solid cream-coloured cut surface thatis similar in texture to the cut surface of a lymphnode involved by lymphoma.

89MALT lymphoma
Histopathology
Pulmonary marginal zone B-cell lym-phomas of MALT type generally appearas a diffuse infiltrate of small lymphoidcells, which surround reactive folliclesthat are typically smaller and less con-spicuous than those arising in the stom-ach. Follicles, best seen when highlight-ed with a CD21 stain, may be overrun bytumour cells (follicular colonisation).Tumours are composed of lymphocyte-like, lymphoplasmacytic-like, centrocyte-like (marginal zone), or monocytoid Bcells, which are all thought to be varia-tions of the same neoplastic cell {904,1104}. Infiltration of bronchial, bronchio-lar and alveolar epithelium (lymphoep-ithelial lesions) is characteristic but notpathognomonic, since this phenomenoncan be seen in non-neoplastic pul-monary lymphoid infiltrates. Plasma cellsmay be numerous and may accumulatealong bronchovascular bundles or inter-lobular septa and may or may not showlight chain restriction. Scattered trans-formed large cells (centroblasts andimmunoblasts) are typically seen, butthese are in the minority. The term, mar-ginal zone B-cell lymphoma of MALTtype refers only to tumours with a pre-dominance of small cells (‘low grade’).Areas with sheets of large cells shouldreceive a separate diagnosis of diffuse
large B-cell lymphoma. Lymphoid cellsoften track along bronchovascular bun-dles and interlobular septa at the periph-ery of masses but alveolar parenchymais destroyed towards their centres.Airways are often left intact, correlatingwith the presence of air bronchogramson HRCT. Central sclerosis may also be afeature. Giant lamellar bodies are seen inabout 20% of cases, most likely reflect-ing the indolent nature of the neoplasm{1576}. Vascular infiltration, pleuralinvolvement and granuloma formationare not uncommon, but have no prog-nostic significance. Necrosis is very rare.Amyloid deposition forming nodules witha ring of lymphoma cells can be seen.
Immunophenotype
The neoplastic cells are monoclonal Bcells, and may be identified by CD20 orCD79a staining, with a variable reactiveT-cell population in the background.Light chain restriction is present in allcases if studied in fresh tissue; it can bedemonstrated in paraffin sections in avariable proportion of the cases depend-ing on the laboratory. Cytoplasmic secre-tory immunoglobulin indicating plasma-cytic differentiation is observed in about30% of cases. The majority of the casesexpress mu heavy chain, but someexpress gamma or alpha. They are
CD5-, CD10-, CD23-, BCL6-, and CD43is expressed in some cases. The tumourcells are usually BCL2+ in contrast toreactive monocytoid B cells. Stains forfollicular dendritic cells (FDC) such asCD21, CD23, and CD35 highlight reac-tive follicles and often demonstrateexpanded meshworks associated withdisrupted follicles overrun by tumourcells. The proliferation fraction (Ki67) isusually very low (<10%); residual folliclesshow numerous Ki67+ cells. Stains forcytokeratin highlight lymphoepitheliallesions.
Differential diagnosis
From the clinical and imaging aspect, thedifferential diagnosis includes sarcoido-sis, bronchioloalveolar cell carcinoma,organizing pneumonia, infections andrarer alveolar filling disorders and amyloi-dosis. The histologic differential diagno-sis includes lymphocytic interstitial pneu-monia, nodular lymphoid hyperplasia,extrinsic allergic alveolitis, inflammatorymyofibroblastic tumour and plasma cellgranuloma.In relation to lymphocytic interstitialpneumonia, pulmonary marginal zone B-cell lymphomas of MALT type tend toinfiltrate and destroy the alveolar archi-tecture, with greater widening of alveolarsepta by the lymphoid infiltrate.Lymphoepithelial lesions may be seen inreactive conditions, but are more promi-nent in the lymphomas. Using immuno-histochemical stains, the presence ofexpanded infiltrates of B cells outside offollicles is characteristic of MALT lym-phoma, while in reactive infiltrates. Bcells are present as small aggregates orfollicles with a peribronchial and/or sep-tal distribution. Demonstration ofimmunoglobulin light chain restriction isimportant in this differential diagnosis,but is optimally done on fresh frozen tis-sue; anaylsis of immunoglobulin heavygene rearrangement by PCR can also bevery helpful.Nodular lymphoid hyperplasia (NLH)refers to the rare occurrence of one orseveral pulmonary nodules consisting ofreactive lymphoid cells {1066}. Patientshave similar presentation and epidemiol-ogy to those with pulmonary marginalzone B-cell lymphomas of MALT typealthough associated lymphadenopathyand pleural effusions suggest the diag-nosis of lymphoma {611}.
DCFig. 1.92 Marginal zone B-cell lymphoma of MALT. A Cytology. Loosely cohesive and single cells with wellpreserved nuclei without nuclear molding. Occasional prominent nucleoli. Bronchial brushing.Papanicolaou stain. B A monotonous population of small lymphoid cells diffusely infiltrates the lung. FromTravis et al., {2024}. C Lymphoepithelial lesions are highlighted by this cytokeratin stain. D Neoplastic lym-phoid cells stain for CD20, indicating B-cell phenotype.
BA

90 Tumours of the lung - Lymphoid / histiocytic tumours
Histologically, NLH comprises numerousreactive germinal centres with well-pre-served mantle zones and interfollicularsheets of mature plasma cells, with vary-ing degrees of interfollicular fibrosis.Plasma cells may show Russell bodies,but not Dutcher bodies. Invasion of thevisceral pleura or invasion of bronchialcartilage are not found. Immunohisto -chemical stains demonstrate a reactivepattern of B cells and T cells. In particu-lar, the germinal centers stain for the B-cell marker CD20, while interfollicularlymphocytes are immunoreactive forCD3, CD43 and CD5 {10}. Antibodies toCD45RA stain the mantle zone lympho-cytes, but stains for bcl-1 and bcl-2 donot decorate the follicles. The CD20-pos-itive lymphocytes do not co-expresseither CD43 or CD5. Staining forimmunoglobulin light chains shows apolyclonal pattern among the plasmacells. Molecular genetic analysis hasshown no rearrangement of theimmunoglobulin heavy chain gene {10}.Assays for the chromosomal rearrange-ment t(14;18) have been negative.Pulmonary marginal zone B-cell lym-phomas of MALT type may produce amy-loid and must be distinguished fromnodular amyloidomas {430}. The mor-phologic finding of a dense plasma cellinfiltrate, light chain restriction in plasma
cells, numerous B cells expressing CD20and coexpression of CD43 by B cellshave been shown to be useful in con-firming the diagnosis of lymphoma.The differential diagnosis, particularly onsmall biopsy specimens, also includesother small B-cell lymphomas, such asfollicular lymphoma, mantle cell lym-phoma, small lymphocytic lymphoma(CLL) and lymphoplasmacytic lym-phoma. Lack of CD5 is helpful in exclud-ing small lymphocytic and mantle celllymphoma, lack of cyclin D1 in excludingmantle cell lymphoma, and lack of CD10and BCL6 in excluding follicular lym-phoma. Distinction from lymphoplasma-cytic lymphoma requires finding thecharacteristic morphologic features ofpulmonary marginal zone B-cell lym-phomas of MALT type (follicles and mar-ginal zone differentiation) or the charac-teristic clinical features of lymphoplas-macytic lymphoma (disseminated dis-ease with bone marrow involvement andmacroglobulinemia).
Histogenesis
Lymphocytes within bronchial MALT.
Somatic genetics
Immunoglobulin genes are clonallyrearranged. Rearrangements can bedetected by Southern blot in all cases if
fresh or frozen tissue is used.Amplification of the immunoglobulinheavy chain gene from paraffin sectionswith the polymerase chain reaction candetect monoclonality in 60% of marginalzone lymphomas {137,1467}.T(11;18)(q21;q21) translocation, is themost common genetic abnormality inpulmonary marginal zone B-cell lym-phoma of MALT type (50-60% of cases).T(1;14) or trisomy 3 may also occur. Thet(11;18) involves the API2 anti-apoptosisgene on chromosome 11 and a recentlyrecognized gene called MLT on chromo-some 18, and produces a fusion protein.Both the t(1;14) and the t(11;18) lead tonuclear Bcl-10 expression {1504}. Onerecent study has shown that t(11;18) andaneuploidy are primarily mutually exclu-sive events, especially in the lung, sug-gesting different pathogenetic pathwaysin the development of this type of lym-phoma. Both abnormalities were associ-ated with recurrent disease {1104}.
Tumour spread and staging
It has been recommended that caseswith unilateral or bilateral pulmonaryinvolvement be staged as IE, and caseswith regional lymph node (hilar/mediasti-nal) involvement be staged as IIE {2053}.When distant spread occurs, there ispreferential spread to other mucosalsites rather than to lymph nodes (just asother lymphomas of MALT origin mayspread to the lung) {407,1467}.
Prognosis and predictive factors
In patients with resectable disease, sur-gery has resulted in prolonged remission{2053}, but for those with either bilateralor unresectable unilateral disease, treat-ment has been governed by the princi-ples that apply to more advanced nodallymphomas. Indeed, elderly patients withasymptomatic lesions may well be fol-lowed up without treatment. Five-yearsurvival for marginal zone lymphomas ofMALT origin is quoted at 84-94%{577,1176,1467}. A small percentage ofMALT lymphomas progress to diffuselarge B-cell lymphoma.
Fig. 1.93 Marginal zone B-cell lymphoma of MALT. The lymphoid cells infiltrate the bronchiolar epitheliumforming lymphoepithelial lesions. From Travis et al. {2024}.

91Primary pulmonary diffuse large B-cell lymphoma
Definition
Diffuse large B-cell non-Hodgkin’s lym-phoma (DLBCL) is a diffuse proliferationof large neoplastic B lymphoid cells withnuclear size equal to or exceeding nor-mal macrophage nuclei or more thantwice the size of a normal lymphocyte.Primary pulmonary DLBCL is used fortumours that are localized to the lungs atpresentation.
ICD-O code 9680/3
Synonyms
High-grade MALT lymphoma has beenused for these tumours, but this termshould no longer be used.
Epidemiology
DLBCL comprise about 5-20% of primarypulmonary lymphomas {21,407,577,1063,1176,1467}. Patients usually pres-ent between 50-70 years of age, similarto patients with pulmonary marginal zoneB-cell lymphoma of MALT type. There isno sex predisposition. Primary pul-monary DLBCL may occur as a compli-cation of immunosuppression for allo-grafts.
Etiology
The etiology of most diffuse large B-celllymphomas is not known. However, anassociation between diffuse large B-cellnon-Hodgkin lymphomas arising in thelung and collagen vascular diseases,both with and without fibrosing alveolitis,has been reported {1469}. Other associ-ations of B-cell lymphomas include AIDSand immunodeficiency conditions.
Localization
Tumours have no zonal or lobar predis-position, and are typically peripheral inlocation.
Clinical features
Patients are nearly always symptomaticand present with cough, haemoptysis
and dyspnoea. Some patients complainof systemic (‘B’) symptoms. Imagingshows solid and often multiple masses.
Macroscopy
Nodules are typically solid and cream-coloured, and may also exhibit paler andsofter areas that correlate with necrosis.
Tumour spread and staging
It has been recommended that caseswith unilateral or bilateral pulmonaryinvolvement be staged as IE, and caseswith regional lymph node (hilar/mediasti-nal) involvement be staged as IIE {2053}.
Histopathology
DLBCL of the lung are morphologicallysimilar to DLBCL in other sites. Tumoursconsist of diffuse sheets of large, blasticlymphoid cells, 2-4 times the size of nor-mal lymphocytes, infiltrating and destroy-ing the lung parenchyma. Vascular infil-tration and pleural involvement are com-monly seen, but lymphoepithelial lesionsare rare. Necrosis is common.
ImmunohistochemistryThe neoplastic cells are of B-cell pheno-type, expressing pan-B antigens (CD20,CD79a) with a variable reactive T-cellpopulation in the background. Monotypicimmunoglobulin light chain expressionmay be detected if frozen tissue is avail-able.
Differential diagnosis
The differential diagnosis includes othermalignant tumours, including undifferen-tiated carcinoma of either large cell orsmall cell type, some variants ofHodgkin’s lymphoma, anaplastic largecell lymphoma and rarely germ celltumours. The diagnosis can usually bemade using an immunohistochemicalpanel including cytokeratins, placentalalkaline phosphatase, CD20, CD3,CD30, ALK1, CD15, CD45 and EMAPrimary pulmonary DLBCL must be dis-
tinguished from mediastinal large B-celllymphoma infiltrating the lung. Know -ledge of the clinical features, includingthe age and sex of the patient and thepresence of a mediastinal mass, isimpor tant in establishing the correctdiagnosis. A lung biopsy in a youngwoman showing DLBCL should raise thesuspicion of mediastinal large B-cell lym-phoma. Distinction from pulmonary lym-phomatoid granulomatosis may be diffi-cult as both entities show a B-cell pheno-type and angiocentricity and necrosismay not be apparent on a small biopsyspecimen. In lymphomatoid granulo-matosis, the T-cell infiltrate is usuallymuch more prominent than in DLBCL.Identification of Epstein-Barr virus maybe of value as atypical B-cells in lym-phomatoid granulomatosis and immuno -deficient patients are usually positive,whilst those in immunocompetentpatients with diffuse large B-cell lym-phoma are negative {1716}.
Histogenesis
DLBCL originates from proliferatingperipheral B cells and or dedifferentaitionof bronchial MALT lymphocytes.
Somatic genetics
Immunoglobulin genes are clonallyrearranged. Evidence of monoclonalityvia amplification of the immunoglobulinheavy chain gene with the polymerasechain reaction can be demonstrated inabout 25% of DLBCL {1467}. Little isknown about genetic abnormalities in pri-mary pulmonary DLBCL.
Prognosis and predictive factors
Patients may inadvertently undergoresection for localised disease , but areusually treated with combination chemo -therapy as for DLBCL in other sites, oftenwith high response rates to adriamycin-based regimens {1203, 1320}. Overall,five-year survival ranges from 0-60%{577,1176,1467}.
A.G. NicholsonN.L. Harris
Primary pulmonary diffuse large B-cell
lymphoma

92 Tumours of the lung - Lymphoid / histiocytic tumours
Definition
Lymphomatoid granulomatosis (LYG) isan extranodal angiocentric and angiode-structive lymphoproliferative disorder,composed of a polymorphous infiltrate ofatypical appearing Epstein Barr virus-infected B cells and numerically moreabundant admixed reactive T cells {752}.Lymphomatoid granulomatosis shows aspectrum of histologic grade and clinicalaggressiveness, which is related to theproportion of EBV positive large B cells.LYG may progress to an EBV positive dif-fuse large B-cell lymphoma.
ICD-O code 9766/1
Synonyms and historical annotation
These lesions were first described nearly30 years ago by Averill Liebow, whocould not decide whether they were avariant of Wegener’s granulomatosis or amalignant lymphoma - hence, the unusu-al name “lymphomatoid granulomatosis”{1182}. More recently, the term “angio-centric immunoproliferative lesion” (AIL)was proposed, which included what wenow know as nasal-type NK/T-cell lym-phoma, and suggested that the diseaseis a lymphoproliferative disorder with thecapability of evolving into lymphoma{919} Neoplasms of T or NK-cell originwith an angiocentric growth patternshould not be classified as LYG, butrather as extranodal peripheral T-cell
lymphomas. The term LYG is currentlypreferred.
Epidemiology
LYG is rare. It typically presents in mid-dle-aged adults (although both youngerand older patients have been reported){562,969,1062,1182,1603}. The diseasecan occur as an apparently idiopathiclesion, but it more often occurs inpatients who have been immunosup-pressed. Examples include patients whohave AIDS or Wiskott-Aldrich syndrome,those who have had organ transplants orwho have been treated for acute lym-phoblastic lymphoma or follicular lym-phoma and those who have agnogenicmyeloid metaplasia {1468}. In patientswithout known prior immunodeficiency,anergy, impaired in vitro responsivenessto mitogens, diminished humoral andcell-mediated responsiveness toEpstein-Bar virus and decrease in total Tcells, CD4 and CD8 lymphocytes, haveall been reported {920,2154}.
Etiology
LYG is an EBV-driven B-cell lymphoprolif-erative disorder, probably arising in abackground of immunodeficiency inmost cases.
Localization
Masses or nodules can involve a varietyof organs, most often lung and centralnervous system, and kidney; skin may beinvolved (in the form of ulcerated or non-ulcerated subcutaneous nodules, erythe-matous dermal papules or plaques){131}.
Clinical features
There is a complex array of symptoms,corresponding to the sites of involve-ment. Up to 70% of patients show bilat-eral, usually peripheral, lung nodules thatmeasure up to 9 cm. in diameter {969,1062,1603}. Cavitation may or may notbe present. Other radiographic patternsinclude diffuse reticulonodular or alveolarinfiltrates, localized infiltrates or a solitarymass. The upper respiratory tract can be
involved by ulcero-destructive lesionsbut lymphadenopathy is infrequent.
Macroscopy
The lungs usually show yellow-white well-demarcated masses that can have asolid or granular, cheesy appearance.They often have a “cannon ball” appear-ance. They may be cavitated. Similarmasses can be found in other organs,such as the kidney or brain.
Histopathology
The lymphoid infiltrate often surroundsmuscular pulmonary arteries and veinsearly in the course of the disease, andtypically invades the walls of these ves-sels. Necrosis is a frequent, although notuniversal, feature of the disease and itcan range from extensive in larger mass-es or high-grade lesions to minimal inlow-grade lesions.LYG consists of small round lympho-cytes, some of which may show slightcytologic atypia and variable numbers ofatypical large mononuclear lymphoidcells in a background of histiocytes andoccasional plasma cells {969,1062,
M.N. KossN. L. Harris
Lymphomatoid granulomatosis
Fig. 1.95 Lymphomatoid granulomatosis. The lungshows multiple yellow-white necrotic masses.
Fig. 1.94 Lymphomatoid granulomatosis. The chestradiograph shows multiple bilateral cavitary mas -ses.

93Lymphomatoid granulomatosis
1182}. Eosinophils and neutrophils areusually not conspicuous. The large cellsresemble immunoblasts; some of theatypical cells may have double nuclei,suggesting Reed-Sternberg cells, butclassic Reed-Sternberg cells are notseen. Despite the term “granulomatosis”in the name, epithelioid granulomas andgiant cells are almost always absent.Sample size is important: Less than 30%of transbronchial biopsies are diagnos-tic, so a surgical lung biopsy will be nec-essary in most cases to achieve a diag-nosis {1603}.There is a histologic grading system forLYG that is based on the number of atyp-ical large EBV-infected cells {1192}.Grade 1 lesions contain few or no EBV-infected cells (less than 5 per high-powerfield), usually lack necrosis, and arepolymorphous. Grade 2 lesions havescattered EBV-infected cells (5-20 perhigh-power field) and foci of necrosis
(extensive at times), but they remainpolymorphous; this is the classic andmost frequently encountered type ofcase. Grade 3 lesions show sheets ofEBV-infected cells, necrosis, and cellularmonomorphism, and are considered asubtype of diffuse large B-cell lymphoma{919}.
ImmunophenotypeLYG is a T-cell-rich, B-cell lymphoprolifer-ative process, as shown by a number ofstudies, both in lung and in other sites,such as skin {131,752,776,1382,1468,1973}.
Histogenesis
EBV-infected peripheral B cell.
Genetics and pathogenesis
In grade 2 and 3 lesions, the B-cells areeither clonal or oligoclonal by methodssuch as VJ-PCR and Southern blot and
appear to be proliferating, at least byproliferation indices {751,919}. The EBVsequences also are typically clonal.Different monoclonal B-cell clones canoccur in different sites in the samepatient {131,2154}. In grade 1 lesions,monoclonality can be more difficult todemonstrate, possibly because of thepaucity of neoplastic B cells, or alterna-tively because some of these lesionsmay not be truly neoplastic The T cellsthat are so abundant in LYG are poly-clonal by molecular methods {751}.These results suggest that in most casesLYG is a T-cell-rich B-cell lymphoma.However, some grade 1 cases may beEBV driven polyclonal lymphoprolifera-tions, and grade 2 cases may be similarto polymorphous, monoclonal post-trans-plant lymphoproliferative disorders(PTLD), in which some degree of immun-odeficiency allows proliferation of clonalEBV+ B cells. These cases may evolve
DC
BA
Fig. 1.96 Lymphomatoid granulomatosis. A The lesion is well demarcated, with a central area of bland necrosis and a rim of residual lymphoid tissue. B Lymphomatoid granulomatosis (grade 2). The lesion shows a mixed cell population of small lymphocytes, macrophages and a single immunoblast with a promi-nent nucleolus. C Vasculitis in lymphomatoid granulomatosis. The arterial wall is infiltrated by small lymphocytes. D Lymphomatoid granulomatosis (grade 3), con-taining sheets of markedly atypical cells, consistent with large cell lymphoma.

94 Tumours of the lung - Lymphoid / histiocytic tumours
into an autonomous, monomorphous dif-fuse large B-cell lymphoma, analogousto the situation in PTLD {751,919,920}.EBV in a partially immunocompetent hostmay explain the vascular damage that isa hallmark of the disease. Chemokines,such as IP-10 and Mig, elaborated as aresult of the EBV infection may beresponsible for vascular damage by pro-moting T-cell adhesion to endothelialcells {1994}.
Differential diagnosis
Some lesions that are histologically simi-lar to LYG do not show atypical EBV-infected B cells, but rather contain atypi-cal cells that are CD3+ T cells {1382,1417}. These T-cell lesions are peripher-al T-cell lymphomas, that, because theyare angiocentric and polymorphous, arehistologically similar to LYG {1382}.Cases of enteropathy-associated T-celllymphoma and of acute T-cell lym-phoblastic leukemia have been confusedas cases of LYG in some series {1468}. T-cell lymphomas of other types, such asnasal-type CD56+ NK/T-cell lymphomasmay also mimic LYG histologically.Immunophenotypic analysis to demon-strate the B or T/NK-cell nature of thelarge cells is important in distinguishingthese entities. In many peripheral T cell
lymphomas the proliferation fraction ofthe T cells (Ki67+) is higher than that ofthe T cells in LYG. The diagnosis of LYGshould be made only in cases in whichthe proliferating large cells are B cells.Cases of grade 1 LYG may lack EBV-pos-itive B cells. Skin lesions also often havevery few EBV-infected B cells and aresubject to sampling problems {131}.These cases give rise to a differentialdiagnosis of reactive inflammatoryprocesses. Clinical correlation and biop-sy of other sites may be necessary toestablish the diagnosis.
Prognosis and predictive factors
Outcome is variable. Patients may showwaxing and waning of their disease.When disease is confined to the lung, orskin, it may resolve without treatment (14-27% of patients) {919,920}. Still, the mostcommon result is death, with median sur-vival of 2 years {919}. The histologicgrade of the lesion is correlated with out-come {969,1192}. Most patients havegrades 1 or 2 disease. Only one-third ofpatients with grade 1 lesions progress tomalignant lymphoma (grade 3), whereastwo-thirds of patients with grade 2lesions develop lymphoma (all patientswith grade 3 lesions have lymphoma bydefinition) {1192}. It is less clear whether
stage of disease correlates with out-come: one study reported a worse prog-nosis in patients with neurologic lesions,while another did not {969,1062}. Lesionsin the central nervous system are often ofhigh histological grade. Long-term sur-vival may occur even in untreatedpatients with grade 1 and 2 lesions, par-ticularly those whose disease is restrict-ed to lung {969,1062}. Currently, grade 3lesions are typically treated as diffuselarge B cell lymphoma {1168} withaggressive chemotherapy; grade 1 and2 lesions are often treated with interferonalpha 2b {920,2154}.
Table 1.13 Immunoprofile of lymphomatoid granulomatosis. From references {776,1382,2154}.
B cells (immunoblasts)CD20+, CD79a+, CD30+ (EBV-induced), CD43+/-, CD15-EBV+ (by in situ hybridization for EBER 1/2 RNA or by immunohistochemistry for LMP)
T cellsCD3+, CD4+, CD8+Cytotoxic markers: TIA-1, granzyme B
B CAFig. 1.97 Lymphomatoid granulomatosis (grade 2). A Immunohistochemical staining for CD3 shows the numerous background lymphocytes to be T cells. Scatteredlarger atypical lymphocytes (B-cells) are negative. B The same microscopic field stained for CD20. The scattered large immunoblastic cells are B cells. C Doublelabeling in situ hybridization for Epstein-Barr Virus with immunohistochemical staining for CD20. Immunohistochemical staining for CD20 (brown) decorates cellswhich are also positive for EBV by in situ hybridization (black). From Guinee et al. {752}.
creo

95Pulmonary Langerhans cell histiocytosis
Definition
Pulmonary Langerhans cell histiocytosis(PLCH) is an interstitial lung diseasecaused by the proliferation ofLangerhans cells and their associatedchanges in the lung. Most affectedpatients are adults and in most the lungis the sole site of involvement.Many Langerhans cell proliferation syn-dromes are considered clonal and neo-plastic {919} but clonality studies onPLCH in adults suggests that this mayrepresent a reactive proliferation ofLangerhans cells {2218}.
ICD-O code 9751/1
Synonyms
Pulmonary histiocytosis X, pulmonaryeosinophilic granuloma, pulmonaryLangerhans cell granulomatosis.
Epidemiology
PLCH is an uncommon form of interstitiallung disease {2025,2075,2076}. The sexpredilection has varied in series; it isprobably roughly equal. The mean age atdiagnosis is approximately 40 years with
a broad range (18-70 years) when chil-dren with disseminated LCH syndromesare excluded {2075,2076}.
Etiology
95% or more of patients are current orformer cigarette smokers {2075,2076}.
Localization
Predominantly upper and mid zones withsparing of the costophrenic angles.
Clinical features
Signs and symptomsPatients may be asymptomatic (15-25%),or may present with pulmonary symp-toms (cough, dyspnoea, chest pain) orwith systemic complaints (malaise,weight loss, fever) {2025,2075,2076}.Approximately 15% of adults with PLCHhave extrapulmonary involvement{2075}. PLCH in adults may rarely be partof a systemic Langerhans cell histiocyto-sis or Langerhans cell sarcoma, whichare best considered a neoplastic haema-tologic problem {919}.Pulmonary function studies are abnormalin most (85% or more) patients and
include (in order of frequency) restrictivedeficits, obstructive deficits, isolateddecreased diffusing capacity, and mixedrestrictive/obstructive deficits {2076}.
ImagingChest radiographs show interstitial lungdisease with predilection for the mid andupper lung zones {2025,2075,2076}.High-resolution CT scanning is distinc-tive, most typically showing nodules ornodules and cystic change with mid andupper lung zone predilection {2025,2075,2076}.
Macroscopy
The gross findings depend on the extentof involvement and the amount of scar-ring. Small nodules, generally 2-5 mm insize (rarely up to 2 cm), may be palpated{2025}. In progressive disease there isextensive interstitial fibrosis with or with-out associated emphysematouschanges.
Histopathology
Histologically most cases of PLCH showconcomitant changes of smoking includ-ing emphysema and respiratory bronchi-olitis {2025,2075,2076}. The lesions ofPLCH begin as cellular proliferations ofLangerhans cells along small airways,primarily bronchioles and alveolar ducts.As the lesions enlarge, rounded or stel-late nodules develop and the bronchiolo-centricity is less easy to discern. Thenodules undergo a natural history fromcellular lesions rich in Langerhans cellsto fibrotic lesions which, in their end-stage, are entirely devoid of identifiableLangerhans cells. In healed PLCH casesthe diagnosis is possible based on thepresence of stellate centrilobular scar-ring in the setting of typical HRCTchanges.Langerhans cells are recognized by theirdistinctive morphology with paleeosinophilic cytoplasm and delicatenuclei with prominent folding of thenuclear membranes {919,2025,2075,2076}. Their presence may be confirmedwith S-100 protein and/or CD1a staining.
T.V. ColbyW.D. Travis
Pulmonary Langerhans cell
histiocytosis
Fig. 1.98 Pulmonary Langerhans cell histiocytosis. Multiple nodular interstitial infiltrates with focal centralcavitation. The edge of the nodular infiltrates shows a stellate shape. From Travis et al. {2024}.

96 Tumours of the lung - Lymphoid / histiocytic tumours
The morphologic features are sufficientlycharacteristic that immunohistochemicalstaining is unnecessary for diagnosis inclassic cases.
Precursor lesions
Langerhans cell hyperplasia in associa-tion with smoking {2075}.
Histogenesis
Proliferation of Langerhans cells {2075}.
Somatic genetics
Yousem et al used the X-linked polymor-phic human androgen receptor assay(HUMARA) locus to assess clonality infemale patients with pulmonary LCH andfound that seven (29%) were clonal and17 (71%) were nonclonal. A nonclonalpopulation was found in three of sixcases with multiple nodules. In one biop-sy with five nodules, two nodules wereclonal with one allele inactivated, onenodule was clonal with the other alleleinactivated, and two nodules were non-clonal. These findings indicate that pul-
monary LCH appears to be primarily areactive process with clonal proliferationof Langerhans cells developing in thesetting of nonclonal Langerhans cellhyperplasia, probably in response toantigens in cigarette smoke {2218}.
Treatment
Steroids have been the mainstay therapyfor PLCH {2075,2076}. With the recogni-tion of the association of PLCH with ciga-rette smoking, smoking cessation is alsoimportant. Refractory cases mayrespond to immunosuppressive therapy.Some cases of PLCH clear spontaneous-ly, making the effects of treatment difficultto determine.
Prognosis and predictive factors
Approximately 15% of patients have pro-gressive respiratory disease that may befatal or lead to lung transplantation{2076}. Progression may be slow, span-ning decades and be dominated by clin-ical features of obstructive lung disease.Predictors of shorter survival include
older age, lower forced expiratory vol-ume in one second (FEV1), higher resid-ual volume, lower ratio of FEV1 to forcedvital capacity, and reduced carbonmonoxide diffusing capacity {2076}.
Pulmonary involvement byother haematolymphoid malignancies
The lung may rarely be the primary site ofpresentation of most types of lymphomasrecognized in lymph nodes {391} includ-ing both non-Hodgkin lymphoma (folliclecenter cell lymphoma, mantle cell lym-phoma, intravascular large B-cell lym-phoma, anaplastic large-cell lymphoma,etc.) and Hodgkin lymphoma. Primaryplasmacytomas are also recognized. Thelung is also a very common site ofrelapse in patients who already carry adiagnosis of lymphoma.Similarly, virtually any leukaemia mayaffect the lung, either primarily (and bethe initial site of presentation) or inpatients with known disease {391}.
Table 1.14Table 1. Classification of Langerhans cell histiocytosis in adults.
Single-organ diseaseLung (occurs in isolation in > 85% of cases with lung involvement)BoneSkinPituitaryLymph nodesOther sites; thyroid, liver, spleen, brain
Multisystem involvementMultiorgan disease with lung involvement (in 5-15% of cases with lung involvement)Multiorgan disease without lung involvementMultiorgan histiocytic disorder
Fig. 1.100 Pulmonary Langerhans cell histiocytosis.CD1a shows an infiltrate of strongly positiveLangerhans cells in the interstitium along an alveo-lar duct.
BAFig. 1.99 Pulmonary Langerhans’ cell histiocytosis. A Langerhans’ cells are readily recognizable by theirdistinctive morphology with pale cytoplasm and delicate folded nuclei. Interspersed eosinophils and pig-mented alveolar macrophages are also common. B The infiltratre consists of Langerhans cells with a mod-erate amount of eosinophilic cytoplasm and nuclei with prominent grooves. From {2024}.
creo

Definition
Pulmonary epithelioid haemangioen-dothelioma (PEH) is a low-to-intermedi-ate-grade vascular tumour composed ofshort cords and nests of epithelioidendothelial cells embedded in a myxo-hyaline matrix. The tumours are distinc-tive for their epithelioid character, sharplydefined cytoplasmic vacuoles, intraalve-olar and intravascular growth and centralhyaline necrosis. High-grade epithelioidvascular tumours are called epithelioidangiosarcomas.
ICD-O code
Epithelioid haemangioendothelioma9133/1
Angiosarcoma 9120/3
Synonyms and historical annotation
Epithelioid haemangioendothelioma waspreviously called intravascular ‘scleros-ing’ bronchioloalveolar tumour (IVBAT) inthe lung.
Clinical features
Signs and symptomsMost patients with PEH are Caucasian,80% are women. The mean age is 36with a range of 12-61 years {435,533,2120}. The presentation is usually indo-lent and almost half of the patients areasymptomatic. Symptomatic patientsmay present with pleuritic chest pain,dyspnoea, mild nonproductive cough,haemoptysis, and clubbing. PEH mayrarely present with alveolar hemorrhage
{225,298} or as thromboembolic disease{2205}. Up to 15% of patients may havesubstantial liver involvement. PEH withhistology similar to that seen in the lungoccur in the liver, bone and soft tissue{510,536,1227,1453}.
ImagingCT scans or chest x-rays characteristi-cally demonstrate multiple, bilateral,small nodules 1-2 cm in size. However,PEH may present as a solitary lung mass{1399}. The radiographic pattern of themultiple smaller lesions may mimic thatof pulmonary Langerhans’ cell histiocyto-sis {1606}. Occasionally the lung nodulesmay appear calcified {1212}. The mostcommon initial interpretation of the radi-ographic picture is that of metastatictumour or old granulomatous disease.
Macroscopy and localization
The most common gross appearance ofPEH is that of a 0.3-2.0 cm circum-scribed mass of gray-white or gray-tanfirm tissue with occasional yellow flecks{435,2081}. The center of the nodulesmay be calcified and the cut surfacereveals a cartilaginous consistency. PEHmay involve the pleura in a patternresembling diffuse malignant mesothe-lioma {424,1184,2222,2239}.
Histopathology
Low power histologic examinationreveals round to oval-shaped nodules,which typically have a central sclerotic,
hypocellular zone and a cellular periph-eral zone. The necrotic center of the nod-ules sometimes can be calcified andossified. The tumour typically spreadsinto adjacent bronchioles and alveolarspaces in a micropolypoid manner andcan be seen passing through pores ofKohn in alveolar walls. Extensive lym-phangitic spread may mimic metastaticcarcinoma. The intercellular stroma con-sists of an abundant matrix that mayappear chondroid, hyaline, mucinous ormyxomatous. Intracellular vacuoles arecommon, sometimes creating a signet-ring appearance, and suggest anattempt to form unicellular vascularchannels. The nuclei of the tumour cellsare usually round to oval. Intranuclearcytoplasmic inclusions are common.
Immunohistochemistry and electron
microscopy
Commonly used endothelial markersinclude CD31, CD34 and factor VIII (vonWillebrand factor), and most PEHexpress these markers {462}. Recently,Fli1 (a member of the ETS family of DNAbinding transcription factors) andFKBP12 (a cytosolic FK506 binding pro-tein interacting with calcineurin) havebeen shown to be reliable endothelialmarkers {599,828}. In epithelioid hae-mangioendotheliomas, CD31, CD34 andFli1 protein are more sensitive and reli-able markers than von Willebrand factor.Vimentin is strongly positive and presentin abundance in these tumour cells in
W.D. TravisH.D. TazelaarM. Miettinen
Epithelioid haemangioendothelioma /
Angiosarcoma
97Epithelioid haemangioendothelioma / angiosarcoma
B CAFig. 1.101 Epithelioid haemangioendothelioma. A Tumour nodule showing increased cellularity at the periphery and abundant eosinophilic stroma with focal necro-sis in the center. B Abundant eosinophilic stroma; cells have prominent cytoplasmic vacuoles or intracytoplasmic lumina. From Travis et al. {2024}. C CD31 stain.The tumour cells stain positively; several show prominent cytoplasmic vacuoles.

comparison with normal endothelialcells. Focal cytokeratin expression isreported in 20-30% of cases.Angiosarcomas are also known toexpress endothelial markers such as vonWillebrand factor, CD31, CD34 and Fli1in the majority of cases. Among them,von Willebrand factor is more specific,but least sensitive. It is often present in aminority of cases with focal weak stain-ing. CD31 is relatively specific andextremely sensitive, being positive inabout 90% of the cases. Cytokeratin isexpressed in about 30% of the cases,emphasizing the importance of antibodypanels to distinguish these vasculartumours from carcinoma {1184,1308}.Electron microscopic studies reveal anexternal lamina or basement membranesurrounding the tumour cells and occa-sional tight junctions {409,1798,2122}.Pinocytotic vesicles may be seen.Conspicuous 100-150 µm thick cytofila-ments are present. Weibel-Palade bod-ies have been described, but may not bedetectable in every case.Intracytoplasmic lumens are characteris-tically present.
Differential diagnosis
The differential diagnosis of PEHincludes a variety of benign non-neo-plastic conditions such as old granulo-matous disease, organizing infarcts,amyloid nodules; several benign neo-plasms such as hamartomas, sclerosinghaemangioma, and chemodectomas;and malignant neoplasms such asmesothelioma, adenocarcinoma (bothprimary and metastatic), angiosarcoma,chondrosarcoma, or leiomyosarcoma.Most of these considerations can beexcluded by recognition of the charac-teristic architecture of the nodular lesionsof PEH with a cellular periphery and acentral zone, which is often necrotic. The
possibility of lung metastases should beconsidered since EH can also arise in theliver, soft tissue, and bone. When thesetumours metastasize to the lungs, theymay present with histologic featuresidentical to cases of PEH {510,536,2081}. In the presence of a dominantmass in an extrapulmonary site, the lunginvolvement may represent metastaticdisease. Some cases of multifocal bilat-eral pulmonary disease suggestingmetastases, do not have extrathoracictumours {435}.Grading: PEH are low or intermediategrade tumours. High grade epithelioidvascular tumours are called epithelioidangiosarcoma, and show more nuclearatypia (mitoses, nucleoli, hyperchromaticchromatin) and less eosinophilic matrixand may have spindle cell foci.Epithelioid angiosarcomas also tend topresent as large solitary masses.
Histogenesis
Epithelioid haemangioendotheliomas arederived from endothelial cells.
Somatic genetics
Little is known about the genetics ofepithelioid haemangioendothelioma. Intwo cases an identical chromosomaltranslocation involving chromosomes 1and 3 [t(1;3)(p36.3;q25)] was detected{1295}. In another case karyotypingrevealed several clonal abnormalities: acomplex unbalanced translocation [7;22]involving multiple breakpoints (confirmedby fluorescence in situ hybridization), aRobertsonian t(14;14), and loss of the Ychromosome {208}. Monosomy for chro-mosome 11 was noted in a subset of thetumour cells {208}.
98 Tumours of the lung - Mesenchymal tumours
Fig. 1.102 Epithelioid angiosarcoma. The tumour cells show marked cytologic atypia with large hyperchro-matic nuclei, vesicular chromatin, prominent nucleoli and mitotic activity.

Definition
Pleuropulmonary blastoma is a malig-nant tumour of infancy and early child-hood arising as a cystic and/ or solid sar-comatous neoplasm, in the lung or lessoften from the parietal pleura {99,1231}.The cystic component is lined by benignmetaplastic epithelium that may be ciliat-ed. This embryonic or dysontogeneticneoplasm of the lung and/or pleura is thenosologic counterpart to other like neo-plasms of childhood including Wilmstumour, neuroblastoma, hepatoblastomaand retinoblastoma.
ICD-O code 8973/3
Synonyms
Rhabdomysarcoma arising in congenitalcystic adenomatoid malformation, pul-monary blastoma of childhood, pul-monary sarcoma arising in mesenchymalcystic hamartoma, embryonal rhab-domysarcoma arising within congenitalbronchogenic cyst, pulmonary blastomaassociated with cystic lung disease,pleuropulmonary blastoma in congenitalcystic adenomatoid malformation {565}.
Epidemiology
Owing to the fact that the pleuropul-monary blastoma came to be recognizedas a clinicopathologic entity in 1989, sys-tematic data are not available on its inci-dence. There are presently over 100cases registered with The Pleuropulmo-nary Blastoma Registry (www.ppbreg-
istry.org). It is certainly less common thanWilms tumour, neuroblastoma and evenhepatoblastoma. Approximately 25% ofcases are accompanied by an apparentconstitutional and heritable predisposi-tion to dysplastic or neoplastic disease inkeeping with a familial cancer syndrome{1620}. Cystic nephroma, ovarian ter-atoma, multiple intestinal polyps, and asecond pleuropulmonary blastoma havebeen observed in affected children {910,1025,1115,1393,1593}.
Age and sex distributionThe age at diagnosis ranges from onemonth to 12 years, with a median age of2 years. Most are diagnosed at or before4 years of age {1619}. The male tofemale ratio is approximately equal.
Etiology
The origin of this tumour remainsunknown, but it may represent the expres-sion of the mesodermally derived thoracicsplanchnopleural mesenchyme in theabsence of any neoplastic epithelial ele-ments, as in a classic pulmonary blas-toma {1231 Since one type of pleuropul-monary blastoma is exclusively cystic, acontroversial suggested origin is fromcongenital cystic adenomatoid malforma-tion {1207}.
Localization
Pleura and/or lung.
Clinical features
The clinical manifestations are variableand depend on age and pathologic type.Respiratory distress with or without pneu-mothorax is the most common presenta-tion of the cystic pleuropulmonary blas-toma in the first 12-18 months of life {892,1619}. Asymptomatic lesions may beincidental findings during investigation ofseemingly unrelated clinical problems{1544,1545,1619}. Fever, chest pain andcough are the presenting complaints inthe 2-4 year old child with a cystic andsolid or exclusively solid neoplasm,which may be suspected initially to bepneumonia or empyema.
ImagingUnilateral, rarely bilateral, localized air-filled cysts are a common finding onimages that have been obtained subse-quent to the onset of respiratory distress{468,1207,1545,1619,1650}. A pneu-mothorax is rarely present. Septal thick-ening or an intracystic mass(es) is anoth-er feature which should suggest the pos-sibility of something other than a con-genital adenomatoid malformation orcongenital lobar emphysema. Other pat-terns of masses lesions and/ or cysts aredescribed {99}.
Macroscopy
Three basic pathologic types are current-ly recognized with associated gross andmicroscopic features {468,2173}. Thepurely cystic pleuropulmonary blastomais characterized as a filmy, thin-walledmulticystic structure, which collapsesafter resection {321}. Another pattern is asolid, firm to gelatinous creamy white,sometimes hemorrhagic tumour, measur-ing over 15 cm in greatest dimension andweighing over 500 g. The solid tumoursmay occupy an entire lobe or lung and ina minority of cases, the mass has arisenfrom the visceral or parietal pleura,including the dome of the diaphragm.
Histopathology
The purely cystic or type I pleuropul-monary blastoma is characterized by thepresence of a multicystic structure linedby respiratory type epithelium beneathwhich is a population of small primitivemalignant cells with or without apparentrhabdomyoblastic differentiation Themalignant cells may be identified as acontinuous or discontinuous cambiumlayer-like zone, but may be difficult tofind. Small nodules of fetal appearingcartilage or a hyalinzed septal stroma arefeatures which should prompt carefulsearch for malignant cells, if they are notinitially apparent. Type II pleuropul-monary blastoma shows partial or com-plete overgrowth of the septal stroma bysheets of primitive small cells withoutapparent differentiation, embryonal rhab-
99Pleuropulmonary blastoma
L.P. DehnerH.D. TazelaarT. Manabe
Pleuropulmonary blastoma
Fig. 1.103 Type I pleuropulmonary blastoma, pre-senting as round, sharply circumscribed multicysticlesion.

domysarcoma or fascicles of a spindlecell sarcoma with the formation ofplaques or nodules. Other examples oftype II tumours are those with a grosslyvisible solid component and microscopi-cally identifiable type I foci. Type IIItumours are solid. The solid areas of thetypes II and III neoplasms have mixedblastematous and sarcomatous features.Nodules of malignant appearing carti-lage, small aggregates of anaplastic andpleomorphic appearing cells, fibrosarco-ma-like areas, rhabdomyosarcomatousfoci and condensed blastema-likeislands separated by loosely arrayedshort spindle cells may also be seenalone, or in combination. Foci of necro-sis, haemorrhage and fibrosis are vari-ably present. Though respiratory epitheli-um may be entrapped within a field oftumour, neoplastic epithelial elementshave not been seen in this tumour type todate, in contrast to the classic pulmonaryblastoma. The primitive small cell patternwith or without apparent rhabdomyoblas-tic differentiation is seen in the purelycystic lesion whereas a more complexmixed sarcomatous pattern is present inthose neoplasms with a solid compo-nent.
Immunohistochemistry
Based upon the microscopic features,the immunophenotype is predictable inthat most neoplastic cells are reactive forvimentin, and the only cytokeratin-posi-tive cells are the respiratory-type cellslining the cysts and the entrapped smallairspaces within solid areas of thetumour. Muscle specific actin anddesmin are consistently expressed incells identifiable histologically as rhab-domyoblastic and less consistently in theprimitive small cells in the cambiumlayer-like subepithelial zones in the cysticareas {1619}. The nodules of cartilageexpress S-100 protein. Immunohistoche-mistry is useful in the differential diagno-sis in those rare cases of a cystic syn-ovial sarcoma of the lung and chest wall{546}. When the latter is a consideration,epithelial membrane antigen, cytokeratinand CD99 are useful since these threemarkers are not expressed in the pleu-ropulmonary blastoma.
Histogenesis
The cell of origin for pleuropulmonaryblastoma is not known. However, it is
probably derived from primitive mes-enchymal cells in the lung and or pleura.
Somatic genetics
Several reports have documented gainsin chromosome 8 detected by karyotyp-ing and fluorescence in situ hybridization{111,910,991,1035,1107,1492,1620,1773,2073,2196}. Though this findingappears to be consistent in thesetumours, gains in chromosome 8 havebeen observed in infantile fibrosarcoma,desmoid fibromatosis and mesoblasticnephroma. It is interesting that the lattertumour has been reported on occasion inchildren who also have a pleuropul-monary blastoma. An unbalancedtranslocation between chromosomes 1and X has been described resulting inaddition copies of 1q and Xq and loss ofpart of Xp. Mutations in p53 are alsoreported.
Prognosis and predictive factors
The pure cystic or type I pleuropul-monary blastoma has a generallyfavourable prognosis of 80-90% 5-yeardisease-free survival, whereas the typesII and III have a poorer outcome of lessthan 50% {1569,1619}. The importanceof recognizing this neoplasm in its cysticform has been emphasized in the recent
literature {1545,1941}. It would appearthat the occult type II neoplasm withmicroscopic overgrowth of the septalareas, and without the formation ofgrossly visible masses or plaques, mayhave a similar favourable outcome as thetype I pleuropulmonary blastoma. Thesetumours locally recur and have apredilection for metastasis to the brain-spinal cord and skeletal system {1619}.Ocular and pancreatic metastases havealso been reported {494,1115,2100}.
100 Tumours of the lung - Mesenchymal tumours
Fig. 1.104 A Type I pleuropulmonary blastoma. Narrow band of primitive round cells beneath the cuboidalepithelium. B Cystic tumour with a type 2 pneumocyte epithelial lining beneath which is a cellular cambi-um layer of spindle cell and epithelioid rhabdomyoblasts. C Type II pleuropulmonary blastoma.Differentiated rhabdomyoblasts with abundant eosinophilic cytoplasm are present beneath the epithelium.This tumour showed solid as well as cystic areas. D Type III pleuropulmonary blastoma. A portion of thetumor is composed of interlacing fibrosarcoma-like foci. This tumour was purely solid.
DC
A B

Definition
A benign tumour composed of hyaline ormyxohyaline cartilage. It is usually foundin Carney triad (gastric stromal sarcoma,pulmonary chondroma and paragan-glioma).
ICD-O code 9220/0
Synonyms
Osteochondroma, chondroma
Clinical features
Signs, symptoms and imaging These are usually asymptomatictumours. Radiologically, they appear ascircumscribed lesions with “pop-corn”calcification, usually multiple, and pre-dominantly in young women {292,689,2006}.
Macroscopy and localization
These are peripheral solid lesions, whichmay be calcified and easily enucleatedat surgery.
Histopathology
These lesions consist of encapsulatedlobules of hypocellular neoplastic carti-laginous tissue. Features of malignancyare absent {292,689,2006}.
Differential diagnosisPulmonary hamartoma (mesenchymo-ma), in the majority of cases, shows cleft-like spaces between cartilaginous lob-ules lined by a component of respiratory
epithelium, with, less often, other differ-entiated mesenchymal elements.Metastatic chondrosarcoma may also beconsidered. Clinical history and cytologi-cal evidence of malignancy will aid dis-tinction.
Prognostic factors
These patients are cured upon removalof their pulmonary chondroma. Clinicalproblems in these patients are more like-ly to relate to their gastric leiomyosarco-mas or paragangliomas {294,1772}.
101Chondroma
J.A. CarneyH.D. TazelaarT. Manabe
Chondroma
Fig. 1.105 Chondroma. Circumscribed, bosselatedtumour composed of white glistening, irregularly-shaped lobules, some with a bluish tinge.
Fig. 1.106 Chondroma. A Encapsulated, hypocellular (left) to moderately cellular (right) tumour with dis-persed cells set in a chondromyxoid stroma. A fibrous capsule with spicules of mature bone containing mar-row fat separates the tumour from the surrounding compressed pulmonary parenchyma. B Paucicellulartumour featuring elongated fusiform and stellate cells with eosinophilic cytoplasm and hyperchromatic,polymorphic nuclei set in a loose chondromyxoid matrix.
B
A

Definition
An interstitial and peribronchovascularproliferation of uniform, plump to morefusiform cells arranged in broad, interlac-ing fascicles; cellularity and mitotic activ-ity may be marked. This spindle cell neo-plasm is reminiscent of the congenitalinfantile fibrosarcoma.
ICD-O codes 8827/1
Synonyms
Congenital fibrosarcoma, congenitalleiomyosarcoma, congenital bronchopul-monary leiomyosarcoma, congenital pul-monary myofibroblastic tumour, congeni-
tal mesenchymal malformation of lung,neonatal pulmonary hamartoma
Epidemiology
This rare neoplasm is documented in theliterature as individual case studies withless than 15 cases to date {45,930,1001,1082,1284}.
Etiology
This tumour occurs sporadically and hasneither syndromic association nor rele-vant maternal history, at least to date.
Clinical features
As a congenital tumour, it is recognizedshortly after birth although the pregnancymay be complicated by polydramniosand non-immune hydrops fetalis.However, its detection by prenatal ultra-sonography should be anticipated {45,930,1001,1082,1284}.
Macroscopy
The well-circumscribed, non-encapsulat-ed mass has a smooth or multinodularsurface with or without fine trabecula-tions. The cut surface has a tann-grey toyellow-tan fleshy appearance. Haemo -rrhage and necrosis are variable fea-tures. The maximum dimension variesfrom 5-10 cm and the tumour may weighin excess of 100 gms. The bronchus isoften distorted or totally obliterated.
Histopathology
The lung parenchyma is replaced by fas-cicles of uniform spindle cells {903},arranged in intersecting fascicles with orwithout a herringbone pattern. The nucleiare elongated and have finely dispersedchromatin, an absence of pleomorphismor anaplasia and variable mitotic activity.Atypical mitotic figures are not present.Bronchial invasion is often seen, and theperibronchial distribution is implicit in thename. The growth may diffusely obliter-ate the parenchyma or form islands andnodules of spindle cells with inter-spersed foci of uninvolved parenchyma{930}. Tumour growth in septa or on thepleural surface may occur. In less cellu-
lar perivascular areas, the tumour cellsappear less sarcomatous with a morefibromyxoid or myofibroblastic prolifera-tion. Cystic foci of haemorrhage may bepresent.
Immunoprofile and electron microscopyA myofibroblastic immunophenotype isnot demonstrable in all cases.The spindle cells are consistently posi-tive for vimentin whereas staining fordesmin and smooth muscle actin isabsent or restricted to isolated cells{1082,1284}. Ultrastructural studies sug-gest myofibroblastic differentiation{1284}. Muscle specific actin immunore-activity is present in less than 5% of thecells and desmin reactivity may beobserved on rare occasion. This tumouris considered to be identical with, or atleast related to, the lesions reported ascongenital leiomyosarcoma, fibrosarco-ma, and fibro-leiomyosarcoma. Immuno -profiles in the tumours diagnosed assuch are non-specific and have beenreported to express neuron-specific eno-lase, alpha-smooth muscle actin, HHF 35actin and muscle-specific actin {382}.Desmin, S-100 protein, CD34, CD57,CD68, factor XIIIa, and CAM 5.2 are alsooccasionally expressed.
102 Tumours of the lung - Mesenchymal tumours
W.D. TravisL.P. DehnerT. ManabeH.D. Tazelaar
Congenital peribronchial
myofibroblastic tumour
Fig. 1.108 Congenital peribronchial myofibroblastictumour. The resected tumour required a pneumec-tomy in a 7-week-old female. The cross-sectionreveals a circumscribed, tan-grey, multinodularmass measuring 10 cm in greatest dimension.
Fig. 1.107 Congenital peribronchial myofibroblastictumour. A Plain view chest roentegenographshows opacification of the right hemithorax of a 7-week-old female who presented with respiratorydistress. B Computed tomogram reveals a well cir-cumscribed mass lesion with a collage of high andlow density foci, representing areas of tumour andcompressed uninvolved parenchyma."
A
B

Imaging
A large mass lesion partially or totallyopacifying the hemithorax is the usualappearance on a plain chest radiograph.Computed tomography reveals a well-circumscribed heterogeneous mass {45,930,1001,1082,1284}.
Somatic genetics
One case has been reported with a com-plex karotype which included a t(8;10)(p11.2;p15) translocation {45}. Althoughthese tumours resemble congenital-infantile fibrosarcoma and congenital
mesoblastic nephroma in their gross andmicroscopic features, there are noreports to date of the detection oft(12;15) (p13;q25-26) translocation in acongenital peribronchial myofibroblastictumour {1734}.
Prognosis and predictive factors
Surgical resection of the involved lobe orlung is the treatment of choice. However,the presence of fetal hydrops with its ownassociated morbidity and mortality maycompliate the clinical outcome.
103Congenital peribronchial myofibroblastic tumour
Fig. 1.109 Congenital peribronchial myofibroblastic tumour. A There is an extensive infiltrate of spindle cells along lymphatic routes: pleura, septa and broncho-vascular bundles. B The spindle cells resemble smooth muscle cells and inflitrate around bronchial cartilage, epithelium and vessels. From Travis et al. {2024}.
BA

104 Tumours of the lung - Mesenchymal tumours
Definition
A diffuse proliferation of lymphatic vas-cular spaces and smooth muscle, dis-tributed with the normal lymphatics of thelungs, pleura and mediastinum.
Synonyms
Lymphangiomatosis, lymphangiectasis,lymphatic dysplasia
Clinical features
The process affects children and youngadults of both sexes who present withprogressive symptoms of “asthma,” dys-pnoea or haemoptysis {230,563,832,925,1319,1637,1933,1985,2039}.
ImagingChest radiographs show increased inter-stitial markings. Computed tomographyshows smooth thickening of the interlob-ular septa, major fissures, central air-ways and pleura.
Macroscopy and localization
There is prominence of the bronchovas-cular bundles and other structures,including pleura, interlobular pulmonarysepta, and mediastinum, reflecting thelymphatic distribution of the disease.
Histopathology
Anastomosing endothelial-lined spacesof varying size are diffusely distributedalong lymphatic routes in pleura,intralobular septa, and bronchovascularsheaths and often contain acellular,sometimes eosinophilic, material {230,563,832,925,1319,1637,1933,1985,2039}. Variable numbers of spindle cellswith bland oval to cigar shaped nucleiare present between channels. Masslesions and cysts are not identified. Intra-alveolar siderophages are often presentin surrounding lung parenchyma.
Immunophenotype and electron microscopyThe immunophenotypic profile of the lin-ing cells is compatible with endothelium(FVIIIrAg positive, vimentin positive, UEApositive) {1985}. The spindle cells com-
monly express vimentin, desmin, actin,and progesteron receptor but are nega-tive for estrogen receptor, keratin, andHMB-45. Ultrastrucurally, the spindlecells resemble smooth muscle cells.
Differential diagnosis
In lymphangiectasis the lymphatic ves-sels are not increased in number and donot anastamose {230,563,832,925,1319,1637,1933,1985,2039}.Lymphangioleiomyomatosis exhibits amore random distribution in association
with cysts. Kaposi sarcoma does notexhibit the complex anastomosing lym-phatic channels. In diffuse pulmonaryhaemangiomatosis vascular spaces areblood-filled and in interstitial emphysemaspaces are airfilled and lack smoothmuscle.
K.O. LeslieH.D. Tazelaar
Diffuse pulmonary lymphangiomatosis
Fig. 1.110 Diffuse pulmonary lymphangiomatosis. A The pleura and septa are infiltrated by a proliferation oflymphatics. B The lymphatic proliferation infiltrating along the interlobular septa are highlighted withtrichrome stain. From Travis et al. {2024}.
A
B

105Inflammatory myofibroblastic tumour
Definition
Inflammatory myofibroblastic tumour is asubgroup of the broad category of“inflammatory pseudotumours” and iscomposed of a variable mixture of colla-gen, inflammatory cells, and usuallycytologically bland spindle cells showingmyofibroblastic differentiation.
ICD-O code 8825/1
Synonyms
Inflammatory myofibroblastic tumour hasacquired a wide array of synonymsincluding the following {654,1259,1292}:inflammatory pseudotumour, plasma cellgranuloma, fibroxanthoma, fibrous histio-cytoma, pseudosarcomatous myofibrob-lastic tumour, and invasive fibroustumour of the tracheobronchial tree.
Epidemiology
Inflammatory myofibroblastic tumour hasan equal sex distribution and occurs inall ages, though most occur in individu-als less than 40 years {654,1850}.Inflammatory myofibroblastic tumour isthe most common endobronchial mes-enchymal lesion in childhood.
Etiology
Some believe inflammatory myofibrob-lastic tumour is a reactive inflammatorycondition, others that it represents a low-grade mesenchymal malignancy {1292}.Pulmonary lesions have been associatedwith previous viral infections, and somereports have indicated an associationwith HHV8 {707}.
Localization
Chest radiographs show a solitary masswith regular borders in 80% of the cases{309,384}. The mass may have a spicu-lated appearance and if endobronchialin location, may be accompanied by apost-obstructive pneumonia and atelec-tasis.
Clinical features
The clinical presentation of patients withinflammatory myofibroblastic tumour is
protean, with signs and symptoms relat-ing to the site of involvement {38,381,384}. Endobronchial lesions present withcomplaints reflecting bronchial irritation,with cough, wheeze, haemoptysis, andchest pain. Constitutional symptoms arerare. Peripheral pulmonary parenchymalnodules are often asymptomaticalthough local invasion into the chest wallmay elicit pleuritic or chest wall pain.
Macroscopy
These lesions are typically solitary roundrubbery masses, which have a variabledegree of a yellowish-gray discolorationreflecting the histiocytic component ofthe inflammatory infiltrate. The size rangeis wide (1-36 cm) with an average size of3.0 cm {38,381,384}. The lesions do notappear encapsulated and local involve-ment of hilar soft tissues or chest wall isseen in 5-10% of cases. Gritty calcifica-tion is occasionally noted. Cavitation israre.
Tumour spread and staging
Inflammatory myofibroblastic tumour isusually localised. Involvement of the
chest wall, mediastinum, or pleura israre, as are recurrences and metastases.
Histopathology
Inflammatory myofibroblastic tumourcontains a mixture of spindle cells show-ing fibroblastic and myofibroblastic dif-ferentiation arrayed in fascicles, or withstoriform architecture. The spindle cellshave oval nuclei, fine chromatin, incon-spicuous nucleoli, and abundant bipolarlightly eosinophilic cytoplasm. Mitosesare infrequent. Cytologic atypia is notobvious. Admixed with the spindle prolif-eration, and often obscuring it, is aninflammatory infiltrate containing lympho-cytes, plasma cells, and histiocytes,including Touton type giant cells. Plasmacells may be prominent and are oftenassociated with lymphoid follicles. Thespindle cells, in rare instances, will infil-trate blood vessels or the pleura.
ImmunohistochemistryPulmonary and extrapulmonary inflam-matory myofibroblatic tumours (IMT)show similar immunoprofiles {384,1636,2223}. Immunostains demonstrate that
S.A. YousemH.D. TazelaarT. ManabeL.P. Dehner
Inflammatory myofibroblastic tumour
Fig. 1.111 Inflammatory myofibroblastic tumour, containing Touton-like giant cells, foamy histiocytes, andabundant inflammatory cells, all within the context of the background bland spindle cell proliferation.

106 Tumours of the lung - Mesenchymal tumours
the spindle cells express vimentin andsmooth muscle actin, and rarely desmin{107,309,882}. They fail to express myo-genin, myoglobin, CD117 (cKit) and S-100 protein. Focal cytokeratin reactivity isnoted in about one third of the cases,perhaps due to alveolar entrapment.Expression of ALK1 and p80 is noted inIMT in about 40% of the cases. {312,322,383,401,741}. P53 immunoreactivity israre and reported in association withrecurrence and malignant transformation{882}.
Histogenesis
Inflammatory myofibroblastic tumour is aproliferation of cells showing myofibrob-lastic differentiation.
Somatic genetics
Inflammatory myofibroblastic tumour ismost often euploid, but may occasionallybe aneuploid {170,882}. Similarly, somecases may show TP53 mutations. IMT
show clonal changes in 2/3 of casesinvolving chromosome 2 at the 2p23location of the ALK gene {1771,1842,1895,1896,2223}. Translocations involv-ing the ALK gene to chromosome 5 cre-ate ALK fusion gene products, which arethought to play a role in the developmentof malignancy {1701}. Few inflammatorymyofibroblastic tumours have completecytogenetics reported, and they indicatethe presence of ring chromosomes andtranslocations involving chromosome 1,2, 4, and 5.
Prognosis and predictive factors
In most instances complete excision ofpulmonary inflammatory myofibroblastictumour leads to excellent survival {654}.A minority (5%) of inflammatory myofi-broblastic tumours may show extrapul-monary invasion, recurrence or metas-tases, recurrence usually occurring incases, which were incompletely excised.Histologic features that may be associat-
ed with a poor prognosis include focalinvasion, vascular invasion, increasedcellularity, nuclear pleomorphism withbizarre giant cells, a high mitotic rate(greater than 3/50 hpf), and necrosis{38,381,384}.
DC
BA
Fig. 1.112 Inflammatory myofibroblastic tumour. A Spindle cells growing in interlacing fascicles. B Spindle cells with myxoid stroma and mild chronic inflammato-ry infiltrate. C Numerous foamy histiocytes give this lesion a fibroxanthomatous appearance. D Prominent lymphocytes and plasma cells infiltrate among the myofi-broblastic cells in this lesion. From Travis et al. {2024}.

107Lymphangioleiomyomatosis
Definition
Lymphangioleiomyomatosis (LAM) is awidespread interstitial infiltrate of imma-ture short spindle cells resemblingsmooth muscle cells, usually associatedwith cystic change, most commonlyoccurring in women of reproductive age.
ICD-O code 9174/1
Synonyms
Lymphangiomyomatosis
Clinical features
LAM is very rare with an estimated inci-dence of 1 per 1,000,000 in the UnitedStates, France, and United Kingdom. Itmost often occurs as a sporadic disease,but also occurs in women with tuberoussclerosis complex (TSC). Among womenwith TSC, 26-39% show radiographic evi-dence of LAM {414,610,1391}. Renalangiomyolipomas occur in most TSCpatients and in approximately 50% ofsporadic LAM patients {97}. LAM is thethird most frequent cause of TSC-relateddeath, after renal disease and braintumours {303}. LAM has been reported inboth postmenopausal women and in atleast one man {92}.
Signs and symptomsThese include progressive dyspnoea onexertion, pneumothorax (often recurrent),cough, haemoptysis and chylous pleuraleffusions.
Imaging
Chest radiograph may be normal, but asthe disease progresses, it typicallyshows diffuse reticular infiltrates withhyperinflation. Computed tomographyshows cystic lesions between 2-20 mm,uniformly distributed in both lungs.
Macroscopy and localization
In advanced cases the lungs show dif-fuse cystic changes from apex to base.Early lesions may show only a few scat-tered cysts.
Histopathology
The two major lesions of lymphangio -leiomyomatosis are cysts and immaturesmooth muscle proliferation. The variablysized cystic spaces are lined by plaque-like or nodular aggregates of smooth-muscle-like spindle cells. These may beadmixed with more rounded epithelioidcells, perhaps representing perivascularepitheliod cells (PECs) or epithelioidsmooth muscle cells. Micronodular pneu-mocyte hyperplasia may also be presentin patients with tuberous sclerosis.
ImmunohistochemistryThe cells of lymphangioleiomyomatosisshow smooth muscle differentiation andexpress. alpha-smooth muscle actin anddesmin, as well as vimentin. Unlike nor-mal smooth muscle cells, however, theyalso show immunoreactivity with amelanocytic marker, HMB-45 {200,1083}. Not all the cells stain, but whenpresent, together with consistent histo-logical changes, is highly specific andsensitive for LAM. Estrogen and proges-teron receptors are present in somecases {153,393}.
Differential diagnosis
Benign metastasizing leiomyoma is notusually associated with cysts and thenodules of smooth muscle are generallylarger than those seen in LAM.Emphysema lacks the spindle cells.Langerhans’ cell histiocytosis shows thepathognomonic cells, eosinophils andhas a characteristic gross andmicroanatomical distribution.
H. TazelaarE.P. HenskeT. ManabeW.D. Travis
Lymphangioleiomyomatosis
Fig. 1.113 Lymphangioleiomyomatosis. The lungshows diffuse cystic changes characteristic oflymphangioleiomyomatosis.
Fig. 1.114 Lymphangioleiomyomatosis. Cystic spaces are surrounded by abnormal smooth muscle bundles.From Travis et al. {2024}.

Histogenesis
The perivascular epithelioid cell (PEC)has been suggested.
Somatic genetics
Germline mutations in both TSC1 andTSC2 are associated with LAM, includingmissense mutations in the final exon ofTSC2 (exon 41) {610,1885}. No geno-type-phenotype correlation has beenidentified. Most women with sporadicLAM do not have germline TSC2 genemutations {86,1747}, but TSC2 mutationshave been found in angiomyolipomas,lymph nodes, and microdissected pul-monary LAM cells from sporadic LAMpatients {297,961,1747,1839}. Thesemutations are not present in morphologi-cally normal kidney or lung, or in theperipheral blood, indicating that they
arise somatically, and leading to thehypothesis that LAM cells migrate ormetastasize to the lung from angiomy-olipomas or lymph nodes. LAM can recurafter lung transplantation {174,1477,1495}. In one case, a somatic TSC2 genemutation was used to prove that recur-rent LAM cells in the allograft lung arosefrom the patient’s native LAM {961} con-sistent with hypothesis that LAM cellsmigrate in vivo.
Prognosis and predictive factors
The prognosis for women with pulmonaryLAM is variable. Progression is commonwith a median survival of 8 to 10 yearsfrom diagnosis {1019,1260,1983}. Anelevated TLC and a reduced FEV1/FVCratio are associated with poor survival{1019}. Kitaichi showed that patients with
a predominantly cystic type of LAM hada worse prognosis than those with a pre-dominantly muscular type {1019}. Matusiet al recently showed that the 5- and 10-year survivals for LAM patients were100% for LAM histology score (LHS)-1,89.9% and 74.6% for LHS-2 and 59.1%and 47.3% for LHS-3, respectively{1260}. He also found that increasingdegrees of hemosiderin deposition wereassociated with higher LHS scores(p=0.029) and a worse prognosis(p=0.0012) {1260}.
108 Tumours of the lung - Mesenchymal tumours
H.D. TazelaarD.B. Flieder
Pulmonary vein sarcoma
Definition
A sarcoma arising in a pulmonary veinwhich almost always shows features ofleiomyosarcoma.
ICD-O code 8800/3
Epidemiology
Pulmonary vein sarcomas are rarer thanpulmonary artery sarcomas and lessthan 20 cases have been reported{1512}.
Clinical features
The tumours tend to occur in womenranging from 23-67 years (mean 49years). The most common presentingsymptoms are dyspnoea, haemoptysisand chest pain. In most cases, the clini-cal impression is that of a left atrial orlung tumour.
Macroscopy and localization
The tumours are generally fleshy-tanand tend to occlude the lumen of theinvolved vessel. They range from 3.0-20.0 cm in greatest dimension. Invasionof either wall of the vein to involve hilarstructures of pulmonary parenchyma iscommon.
Histopathology
The majorities of pulmonary vein sarco-mas show smooth muscle differentiationand, therefore, represent leiomyosarco-mas. They are moderate to highly cellu-lar spindle cell neoplasms with varyingdegrees of mitotic activity and necrosis.Epithelioid morphology may be present.Immunohistochemically, the tumours are
reactive with antibodies to vimentin,desmin and actin, confirming the pres-ence of smooth muscle differentiation. Aberrant keratin reactivity may beobserved in as many as 40% of cases.
Fig. 1.115 Pulmonary vein sarcoma. The wall of the vein is infiltrated by spindle and pleomorphic sarcoma cells.

109Pulmonary artery sarcoma
Definition
A sarcoma of the large pulmonary arter-ies with two types. Intimal sarcomas havean intraluminal polypoid growth patternand usually show fibroblastic or myofi-broblastic differentiation. Mural sarco-mas are considered distinct from intimalsarcomas, and are classified separatelyaccording to the histologic subtype as insoft tissue sarcomas (leiomyosarcoma).
ICD-O code 8800/3
Synonyms
Intimal sarcoma of the pulmonary arteryhas been used interchangeably with pul-monary artery sarcoma, since intimalsarcomas comprise the vast majority ofpulmonary artery sarcomas. Mural sarco-mas are exceedingly rare.
Epidemiology
Pulmonary artery sarcomas are a raretumour with only a few hundred casesreported. The incidence is unknown andprobably underestimated, since manycases are still misdiagnosed as pul-monary embolism preoperatively andmay remain unrecognized if not exam-ined histologically. The average age atdiagnosis is 49.3 years (range 13-81years) with a roughly equal sex distribu-tion {419,1079,1488}.
Localization
These tumours occur in the pulmonarytrunk, most commonly, right pulmonary
artery, left pulmonary artery, pulmonaryvalve, and, least often, the right ventricu-lar outflow tract {419}.
Clinical features
The most common presenting symptomis dyspnoea, followed by, in decreasingorder, chest / back pain, cough, haemop-tysis, weight loss, malaise, syncope,fever, and rarly sudden death {419}.These clinical findings are often indistin-guishable from those of chronic throm-boembolic disease, but progressiveweight loss, anemia and fever are unusu-al for benign pulmonary vascular dis-eases and should raise a suspicion formalignancy {1547}. Common physicalsigns include systolic ejection murmur,cyanosis, peripheral oedema, jugularvenous distension, hepatomegaly, andclubbing {1547}.
ImagingRadiologic findings overlap with those ofchronic thromboembolic disease, but therate of preoperative diagnosis hasincreased remarkably in the last decadewith advances in imaging {419,959,973}.Solid appearing expansion of the proxi-mal pulmonary artery branches is highlysuggestive of a sarcoma, especially inthe presence of pulmonary nodules, car-diac enlargement and decreased vascu-larity {419}. The features in computedtomography (CT) and magnetic reso-nance imaging (MRI) that favor a diagno-sis of sarcoma over thrombi include: het-
erogeneous soft tissue density, smoothvascular tapering without abrupt narrow-ings and cut-offs {973}, and unilateralcentral pulmonary emboli {419,973}.Vascularization in sarcomas may beseen with bronchial arteriography {419}.
Macroscopy and localization
Intimal sarcomas resemble mucoid orgelatinous clots filling vascular lumens.Distal extension may show smooth taper-ing of the mass. The cut surface mayshow firm fibrotic areas and bony/grittyor chondromyxoid foci may be present inmural lesions. Haemorrhage and necro-sis are common in high-grade tumours.Most cases have bilateral pulmonaryartery involvement, although one side isusually dominant.
Tumour spread and staging
Pulmonary artery sarcomas metastasizeprimarily to the lung and mediastinum(50%). Distant metastases have beenreported in 16% cases {419}. There is norecognized staging sytem.
Histopathology
Intimal sarcomas typically show a prolif-eration of spindle cells in a myxoid back-ground, alternating with hypocellular col-lagenized stroma. Recanalized thrombimay be intimately admixed, especially astumour extends distally. Some intimaland most mural tumours will show foci ofmore differentiated sarcomas: osteosar-coma, chondrosarcoma or rhabdomyo-sarcoma {101,182,246,1285,1488,1559,1816}.
Immunohistochemistry / ElectronmicroscopyMost intimal sarcomas show immunohis-tochemical and ultrastructural evidenceof myofibroblastic differentiation {101,182,246,1285,1488,1559,1816}. Thetumour cells, in general, exhibit strongand diffuse immunoreactivity for vimentin{728}. Osteopontin expression can alsobe expressed {667}. Reactivity forsmooth muscle actin is variable. Tumorcells may express desmin or endothelial
J. E. YiH.D. TazelaarA. BurkeT. Manabe
Pulmonary artery sarcoma
BAFig. 1.116 Pulmonary artery sarcoma (PAS). A Axial CT scan showing large tumor mass (arrow) outlined bycontrast material straddling the bifurcation of the pulmonary artery and extending into the left lower lobebranches. B Gross photograph of PAS resected by pulmonary thromboendarterectomy procedure.

110 Tumours of the lung - Mesenchymal tumours
markers, such as factor VIII, CD31, andCD34 when they show evidence ofsmooth muscle or vascular differentiation{728}.
Differential diagnosis and grading
The diagnosis is fairly straightforward inmost cases, though some thrombi mayhave highly cellular foci. Metastasesshould always be excluded. There is nospecific grading system; NCI andFNCLCC systems for soft tissue sarcomacan be used.
Histogenesis
Intimal sarcomas presumably arise frompluripotential mesenchymal cells of theintima {246,1488}, but primitive cells ofthe bulbus cordi in the trunk of pul-monary artery have been also proposedas the origin {1285}.
Somatic genetics
Comparative genomic hybridizationrevealed frequent gains or amplificationof 12q13-q15 with amplification ofSAS/CDK4, MDM2 and GLI. In addition,
there was amplification of PDGF receptorA on 4q12. Less consistent alterationshave been identified including losses on3p, 3q, 4q, 9p, 5p, 6p, and 11q.
Prognosis and predictive factors
Overall prognosis is very poor regardlessof therapy with the mean survival rangingfrom 14-18 months {246,485,1488}.Surgical resection is the single mosteffective modality for short-term palliationand the role of adjuvant therapy is yet tobe determined {55,485}.
DC
BA
Fig. 1.117 Pulmonary artery sarcoma (PAS). A Spindle cell proliferation, alternating with hypocellular collagenous stroma. B PAS intimately incorporated withrecanalizing thrombi. C PAS with myofibroblastic differentiation as shown by smooth muscle actin (SMA) immunostain in inset. D Chondrosarcomatous area with-in a pulmonary artery sarcoma.

111Pulmonary synovial sarcoma
Definition
Pulmonary synovial sarcoma (SS) is amesenchymal spindle cell tumour, whichvariably displays areas of epithelial dif-ferentiation. While it can be seen as ametastasis from an extrapulmonary site,it also occurs in the lung in the absenceof primary elsewhere.
ICD-O codes
Synovial sarcoma 9040/3Synovial sarcoma, spindle cell
9041/3Synovial sarcoma, biphasic
9043/3
Synonyms
Synovial cell sarcoma, malignant syn-ovioma, synovioblastic sarcoma
Clinical features
Pulmonary SS usually presents in youngto middle age adults and shows no gen-der predilection {68,546,694,850,957,1777,1992,2234,2236}. Cough, oftenwith haemoptysis is the most commonclinical manifestation, followed by chestpain. Low-grade fever and weight lossare rare. These tumours can also presentas incidental tumours on chest X-ray.Prognosis is in general poor with almosthalf of patients dying of disease (mean23 months) {68,546,694,850,957,1777,
1992,2234,2236}. However, prolongedsurvival without disease, over 5 years,has occurred.
Macroscopy and localization
Pulmonary SS are usually peripheral,well-circumscribed but non-encapsulat-ed, solid tumours. Size ranges between0.6-17.0 cm (mean 5.6 cm) {546}. Rarecases involving the tracheobronchial treewith formation of an endobronchial masshave been described. Occasionally, thetumour diffusely infiltrates chest wall ormediastinal structures. The cut surface ofthe tumour can show cystic degenerativechanges and necrosis.
Tumour spread and staging
Pulmonary SS mainly spreads and recursregionally, involving chest wall, pericardi-um, diaphragm, paraspinal soft tissue.Direct extension to the abdominal cavitymay also occur {68,546,694,850,957,1777,1992,2234,2236}. Metastases tomediastinal lymph nodes are extremelyuncommon (5%). Systemic metastases,mainly to liver, bone, brain, and lung,occur in almost a quarter of patients.
Histopathology
Histologic features of pulmonary SS areidentical to its soft tissue counterpart{68,546,694,850,957,1777,1992,2234,
2236}. Both biphasic and monophasicsubtypes have been described.Monophasic SS, the most common pul-monary subtype is comprised solely ofthe spindle cell component. The spindle-cell component consists of interweavingfascicles of densely packed elongatedcells. This subtype often displays aprominent haemangiopericytomatousvascular pattern, and focal areas ofdense hyaline fibrosis. Biphasic SS com-prises both epithelial and spindle com-ponents. Epithelial areas contain cleft-like glandular spaces with scatteredtubulo-papillary differentiation. The cellsare cuboidal with moderate eosinophiliccytoplasm, round nuclei with granularchromatin and occasional nucleoli.Mucoid secretions are commonly seen.Care should be taken not to confuse theepithelial component with entrappedalveolar epithelium that will be TTF-1positive and could be mistaken forbiphasic synovial sarcoma {2234}. Thecells contain scant cytoplasm with ovalnuclei. Most pulmonary SS contain focalnecrosis. Mitotic activity varies greatly (5-25/10HPF). Calcification and mast cellinfiltrates may be seen.
ImmunohistochemistryMost synovial sarcomas show immunore-activity for cytokeratins (CK) and/or
M.C. AubryS. SusterH.D. TazelaarT. Manabe
Pulmonary synovial sarcoma
Fig. 1.118 Synovial sarcoma. A Round to oval and spindle shaped cells with minimal cytoplasm, hyperchromatic nuclei, inconspicuous mitoses and only slight fibrousstroma. B Alternating myxoid and cellular areas with some vessels showing hyalinization.
BA

112 Tumours of the lung - Mesenchymal tumours
epithelial membrane antigen (EMA){410}. The intensity of staining is moreprominent in the epithelial rather than thespindle cell component. EMA tends to beexpressed more often and more widelythan CK. In monophasic lesions, reactiv-ity may be scanty. Cytokeratins 7 and 19are particularly useful because synovialsarcoma cells express these types ofcytokeratins, and these are generallynegative in other spindle cell sarcomas{1306,1838}. Vimentin is usuallyexpressed in the spindle cells of synovialsarcoma. Intranuclear and intracyto-plsmic immunoreactivity for S-100 pro-tein can be identified in up to 30% of thetumours {585,749}. BCL-2 and CD99 arefrequently positive {469,1652,1908}CD34 is virtually usually negative {2064}.Desmin is absent but focal reactivity formuscle specific actin or smooth muscleactin is noted on occasion in monopha-sic synovial sarcomas. Lastly, given thedifferential diagnosis with mesothelioma,
it is relevant to note that synovial sarco-mas commonly contain foci of calretinin-positive cells {1310}.
Differential diagnosisThe most important and common differ-ential diagnosis is metastatic SS to thelung, which needs to be excluded with athorough clinical and radiologic exam.Otherwise the differential diagnosis iswide and includes both more commonepithelial and other rare mesenchymaltumours, such as spindle cell carcinoma,malignant mesothelioma, small cell carci-noma, thymoma, pleuropulmonary blas-toma, localized fibrous tumour, fibrosar-coma, smooth muscle tumour, and malig-nant peripheral nerve sheath tumour andEwing sarcoma. The distinction is usuallymade on the basis of histologic andimmunohistochemical features. In diffi-cult cases, detection of specific cytoge-netic/molecular abnormality might beuseful.
Histogenesis
This remains unknown, though is thoughtto be a totipotential mesenchymal cell.
Somatic genetics
The cytogenetic hallmark of synovial sar-coma is the t (X; 18)(p11; q11) {68,546,850,957,1992}. This translocation resultsusually in the fusion of the SYT gene onchromosome 18 to either the SSX1 orSSX2 gene on chromosome X. Thetranslocation has been found in >90% ofSS, regardless of histologic type and thefusion transcript, identified either byFISH, RT-PCR, or real time PCR, is con-sidered specific. The translocation or thefusion transcript was present in all evalu-ated pulmonary SS.

113Hamartoma
Definition
Pulmonary hamartomas are benign neo-plasms composed of varying proportionsof mesenchymal tissues, such as carti-lage, fat, connective tissue and smoothmuscle, typically combined withentrapped respiratory epithelium.
Synonyms
The popular term chondroid hamartomadenotes the usual predominance of car-tilagenous matrix. Other terms includebenign mesenchymoma, hamartochon-droma, chondromatous hamartoma, ade-nochondroma and fibroadenoma of thelung.
Epidemiology
The population incidence is 0.25%{1065} with a two- to four-fold male pre-dominance and peak incidence in thesixth decade {2066}. Hamartomas arerare in children.
Localization
Hamartomas are usually peripheral andless than 4 cm in diameter. About 10%arise endobronchially {2006,2066}.
Clinical features
Presentation is typically as an asympto-matic, solitary, well-circumscribed nod-ule on routine chest x-ray. Hamartomasrepresent approximately 7-14% of coinlesions. Multiple lesions are rare.Occasionally, the distinctive radiograph-ic appearance of “popcorn calcification”
is seen. Endobronchial lesions tend tocause symptoms due to bronchialobstruction {2006,2066}.
Macroscopy
Parenchymal tumours are multilobulated,white or gray, firm masses that “shell out”from the surrounding parenchyma. Theconsistency is cartilaginous, with occa-sional gritty specks of dystrophic calcifi-cation or bone. Endobronchial lesions,which tend to be more lipomatous, aresituated within the larger airways asbroad-based polyps.
Histopathology
Hamartomas are composed predomi-nantly of lobulated masses of mature car-tilage surrounded by other bland mes-enchymal elements such as fat, smoothmuscle, bone, and fibrovascular tissue.These latter elements rarely predomi-nate. Clefts of respiratory-type epitheliumfrequently extend as slit-like spacesbetween the lobules of mesenchymalcomponents. In endobronchial hamar-tomas, adipose tissue may predominate,and epithelial inclusions tend to be shal-low or absent. Cytologic diagnosis ofchondroid hamartoma is based onrecognition of the mesenchymal compo-nents. Immunohistochemistry and ultra-structural studies rarely contribute to thediagnosis.
Differential diagnosis
Hamartomas are separated frommonomorphic benign soft tissue tumoursby the presence of at least two mes-enchymal elements, and from chon-drosarcoma by the lack of cytologicatypia. “Cystic mesenchymal hamar-toma” refers mainly to neoplasms of chil-dren, is readily distinguishable fromchondroid hamartoma, and is preferablyclassified as pleuropulmonary blastoma.Hamartomas must also be distinguishedfrom bronchopulmonary chondromasthat tend to be multiple in Carney’s triad(pulmonary chondromas, epithelioid gas-tric smooth muscle tumours and extra-adrenal paraganglioma). These consistsolely of cartilage without cleft-likespaces lined by respiratory epithelium.
Histogenesis
Histogenesis is unknown, althoughgenetic studies indicate a neoplasticrather than hamartomatous origin {2006,2066}.
Somatic genetics
Pulmonary hamartomas have a high fre-quency of genetic mutations, similar tothose seen in other benign mesenchymalneoplasms such as lipomas. Mostnotable are mutations of high-mobilitygroup (HMG) proteins, a family of non-histone, chromatin-associated proteins,which are important in regulating chro-matin architecture and gene expression.Mutations in the regions 6p21 and12q14-15 are most commonly found{591,824,982,983}.
Prognosis and predictive factors
Conservative surgery is appropriate,either by enucleation or wedge resectionfor parenchymal lesions or by bron-choplastic resection for endobronchiallesions. Recurrence or sarcomatoustransformation is exceedingly rare{2066}.
A.G. NicholsonJ.F. Tomashefski Jr.H. Popper
Hamartoma
BAFig. 1.119 A Hamartoma, ‘shelled-out’ of the lung parenchyma, with a lobulated cream-coloured externalsurface. B Hamartoma, specimen radiograph. The irregularly shaped white area represents "popcorn" cal-cification.

114 Tumours of the lung - Miscellaneous tumours
DC
BA
Fig. 1.120 Hamartoma. A A bisected, circumscribed hamartoma revealing lobules of firm cartilagenous tissue interspersed by fibrovascular and adipose tissue.Focal cystic change is also seen. B At low power, a hamartoma shows lobules of cytologically bland cartilagenous tissue interspersed by mature adipose tissue.Focal ossification. C Lobules of mature cartilage with deep clefts lined by bronchiolar type epithelium From Travis et al. {2024}. D Adjacent to the cartilage are fatvacuoles and a spindle cell mesenchymal stroma. The cleft-like space is lined by bronchiolar-type epithelium From Travis et al. {2024}.

115Sclerosing haemangioma
Definition
A lung tumour with a distinctive constel-lation of histologic findings including:solid, papillary, sclerotic, and haemor-rhagic patterns. Hyperplastic type IIpneumocytes line the surface of the pap-illary structures. Cholesterol clefts,chronic inflammation, xanthoma cells,haemosiderin, calcification, laminatedscroll-like whorls, necrosis, and maturefat may be seen.
ICD-O code 8832/0
Synonyms and historical notation
Pneumocytoma, papillary pneumocy-toma {992}. It was named sclerosinghaemangioma as it was originallybelieved to be vascular in origin due toprominent angiomatoid features. Currentconsensus favors a benign or very low-grade neoplasm arising from primitiverespiratory epithelium.
Epidemiology
Sclerosing haemangioma predominantlyaffects middle-aged adults (median =46, from 11–80 years-old) {1456,1859},with a female predominance (80% ofcases) {488}. It is rare in western coun-tries. In East Asia (e.g Japan), its fre-quency is higher and is similar to that ofcarcinoid tumour.
Localization
Most tumours are solitary and peripheral;4% of cases are multiple {1153}. The
tumour may involve visceral pleura (4%),mediastinum (1%), and rarely occurs asendobronchial polyps (1%) {488}.
Clinical features
Most patients are asymptomatic (80%).Haemoptysis, cough, and thoracic painmay occur. Chest x-ray shows a solitary circumscribed mass, rarely calcified,and occasionally cystic. CT scans showa well-circumscribed mass with marked
contrast enhancement, and foci ofsharply marginated low attenuation andcalcification {890}. By MRI, a haemor-rhagic component may help differentiateSH from other coin lesions {627}.
Macroscopy
SH presents as a well-circumscribedmass without a preferential lobar distri-bution. Size ranges from 0.3-8 cm.Sections show a solid, grey to tan-yellow
M. Devouassoux-ShisheboranA.G. NicholsonK. LeslieS. Niho
Sclerosing haemangioma
B CAFig. 1.121 Sclerosing haemangioma. A CT scan shows a circumscribed, solid yellow tan mass lying within the posterior segment of the left upper lobe. B Sclerosinghaemangioma, presenting as a well-circumscribed solid white tumour at its periphery. C Well-circumscribed unencapsulated nodule with a mixture of papillary,solid and sclerotic patterns.
Table 1.15 Immunoprofile of sclerosing haemangioma. From M. Devouassoux-Shisheboran et al. {488}.
Markers
Pan-cytokeratinEMALow molecular weight keratin (CAM 5.2)Cytokeratin 7Cytokeratin 20High molecular weight keratin (CK 5/6; K903)TTF-1Pro-Sp A and pro-SpBClara cell antigenVimentinS-100 proteinSMAFactor VIIICalretinin Estrogen receptorsProgesterone receptorsChromograninSynaptophysinLeu-7
EMA (epithelial membrane antigen); CK 5/6 (cytokeratin 5/6), K903 (keratin 903), TTF-1 (thyroid transcrip-tion factor-1), pro-SpA and pro-SpB (surfactant apoproteins A and B), SMA (smooth muscle actin).
Round cells(% of cases)-+ membranous+ focal (17%)+ focal (31%)--+ nuclear (92%)--+----+ (7%)+ (61%)---
Surface cells(% of cases)++ membranous++--+ nuclear (97%)+++---------
creo

116 Tumours of the lung - Miscellaneous tumours
surface with foci of haemorrhage andoccasionally cystic degeneration {1464}or calcification.
Tumour spread and staging
These tumours may spread to regionallymph nodes in approximately 1% ofcases {488,1009,1334}. Rarely SH maypresent in the mediastinum withoutapparent connection to the lung {1728}.
Histopathology
Two cell types occur: round stromal cellsand surface cells, both of which arethought to be neoplastic in origin {970}.Round cells are small with well-definedborders and centrally located round tooval bland nuclei with fine dispersedchromatin, an absence of discerniblenucleoli. Mitotic index is low (usually lessthan 1 per 10 high power fields). Theircytoplasm is eosinophilic but may befoamy or vacuolated with a signet ringappearance. Cuboidal surface cells dis-play the morphology of bronchiolarepithelium and activated type II pneumo-cytes. They may be multinucleated, ordemonstrate clear, vacuolated, foamycytoplasm or intranuclear inclusions.Focal mild to marked nuclear atypia canbe seen in either cell type. 1. Papillary pattern: complex papillaelined by cuboidal surface cells. The stalkof the papillary projections contains theround cells. It can be sclerotic or occa-sionally myxoid.2. Sclerotic pattern: dense foci of hyalinecollagen at the periphery of the haemor-rhagic areas, within papillary stalks, orwithin the solid areas.3. Solid pattern: sheets of round cells,with scattered cuboidal surface cellsforming small tubules.4. Haemorrhagic pattern: large blood-filled spaces lined by epithelial cells orfoci of haemorrhage and debris contain-ing haemosiderin deposits, foamymacrophages, and cholesterol clefts,rarely surrounded by granulomatous andchronic inflammation.Calcifications sometimes display apsammoma-like configuration. Lamellarstructures in the spaces between papil-lae are also encountered. Rarely, maturefat may be seen. Neuroendocrine cells,isolated or in solid nests (tumourlets)may rarely occur SH combined with typi-cal carcinoid has been described{1153}.
ImmunohistochemistryRound cells express TTF-1 and EMA, butare pancytokeratin negative. Surfacecells express TTF-1, epithelial membraneantigen (EMA), surfactant apoprotein Aand pancytokeratin.
Cytopathology
Trans-thoracic fine needle aspirationcytology {655} typically shows a moder-ately cellular, dual cell population.Round cells are small, round or spindle-shaped, with granular cytoplasm, uni-form nuclei arranged in cohesive papil-lary clusters or in flat pavement-type ori-entation. The nuclei may be atypical, butthe absence of nucleoli helps in distin-guishing SH from adenocarcinoma.Hyalinized stromal tissue fragments maybe seen. Foamy macrophages, haemo-siderin, and red cells are seen in thebackground
Differential diagnosis
The differential diagnosis includes clearcell tumours involving the lung (metasta-tic renal cell carcinoma, clear cell ‘sugar’tumours, and clear cell carcinomas of thelung), carcinoids and papillary pul-monary epithelial neoplasms. SH can beusually be distinguished from these bybland cytology, heterogeneous architec-ture and a characteristic immunostainingpattern.
Histogenesis
Since the first description in 1956 {1183},vascular {1183}, mesothelial {972}, mes-enchymal {883}, epithelial {1751}, andneuroendocrine {2180} origins havebeen postulated. Immunohistochemicalfindings suggest that sclerosing hae-mangioma derives from primitive, undif-ferentiated respiratory epithelium.Molecular studies have demonstrated
Fig. 1.122 Sclerosing haemangioma. A The tumour is circumscribed, but not encapsulated and shows asclerotic and papillary pattern. From Travis et al. {2024}. B Cytokeratin (AE1/AE3) staining shows positivestaining of the surface cells but negative staining of the round cells. C EMA shows membranous stainingof round and surface cells.
B C
A

117Sclerosing haemangioma
the same monoclonal pattern in both theround and surface cells, consistent witha true neoplasm rather than a hamar-toma {1474} There is no normal counter-part for the neoplastic stromal cell recog-nized in the human lung.
Prognosis and predictive factors
Sclerosing haemantioma behaves in aclinically benign fashion. No recurrenceor disease-related deaths have beenreported. Reported cases with hilar ormediastinal lymph node involvement donot have a worse prognosis {1464,2198}.
Fig. 1.125 Sclerosing haemangioma. A Sclerotic, solid and papillary patterns are present . B In this haem-orrhagic pattern the tumour forms ectatic spaces filled with red blood cells that are surrounded by type IIpneumocytes. From Travis et al. {2024}.
A
B
Fig. 1.123 These epithelioid cells of sclerosing hae-mangioma are growing in the solid pattern. FromTravis et al. {2024}.
Fig. 1.124 Sclerosing haemangioma TTF-1 (thyroidtranscription factor-1) is expressed in tumour cells.

118 Tumours of the lung - Miscellaneous tumours
Definition
Clear cell tumours are benign tumoursprobably arising from perivascularepithelioid cells (PEC). They comprisecells with abundant clear or eosinophiliccytoplasm that contain abundant glyco-gen.
ICD-O code 8005/0
Synonyms
Other terms include ‘sugar tumour’ in thelung and PEComa (perivascular epithe-lioid cell-oma), or myomelanocytomas atother sites.
Epidemiology
This tumour is extremely rare. There is aslight female predominance, with agerange of 8-73 years.
Etiology
There is a very rare association withtuberous sclerosis and lymphangi-oleiomyomatosis {594}.
Localization
Most are solitary and peripheral in loca-tion.
Clinical features
Clear cell tumours are generally asymp-tomatic and discovered incidentally{646}.
Macroscopy
Tumours are usually about 2 cm in diam-eter (range 1 mm to 6.5 cm) {59,646}.They are well circumscribed and solitary,with red-tan cut surfaces.
Histopathology
Clear cell tumours comprise rounded oroval cells with distinct cell borders andabundant clear or eosinophilic cyto-plasm. There is mild variation in nuclearsize, nucleoli may be prominent, butmitoses are usually absent. The pres-ence of necrosis is extremely rare andshould lead to consideration of malig-nancy {646}, as should significant mitoticactivity and an infiltrative growth pattern{1984}. Thin-walled sinusoidal vesselsare characteristic. Due to the glycogen-rich cytoplasm, there is usually strongdiastase-sensitive PAS positivity {1127}.
Immunohistochemistry and electron
microscopy
Tumours stain most consistently for HMB-45 {59,646,648,652,1127}. Electronmicroscopy shows abundant free andmembrane bound glycogen {646,648,1127}. Melanosomes have also beenidentified {646,648,1127}.
Differential diagnosis
Clear cell tumours are distinguished fromclear cell carcinomas, both primary andmetastatic, on the basis of a lack of cyto-
logic atypia, the presence of thin-walledsinusoidal vessels within the tumour, pos-itive staining for S-100 and HMB-45(melanocytic markers) and negativestaining for cytokeratins. Metstatic renalcell carcinomas may contain intracyto-plasmic glycogen but show necrosis andstain for epithelial markers. Granular celltumours stain for S-100 but not for HMB-45 and do not contain abundant glyco-gen in their cytoplasm. Metastaticmelanomas and clear cell sarcomas willhave a similar immunophenotype andultrastructure, but the tumour cells willnot show significant atypia and there isusually a history of a previous neoplasm.
Histogenesis
Recent data suggest a pericytic originand clear cell tumours have been pro-posed to represent one of the family ofPEComas, neoplasms originating fromthe perivascular epithelioid cells (PEC){201}.
Prognosis and predictive factors
Virtually all tumours have been cured byexcision {646,652,1127}.
A.G. NicholsonClear cell tumour
B CAFig. 1.126 Clear cell tumour. A The abundant cytoplasmic glycogen is stained with periodic acid-Schiff (PAS). B The glycogen is removed in this PAS stain with dia-stase digestion. C The tumour cells stain positively with immunohistochemistry for HMB-45. From Travis et al. {2024}.

119Teratoma
Definition
Teratomas are tumours consisting of tis-sues derived from more than one germcell line. They may be mature or imma-ture. Criteria for pulmonary origin areexclusion of a gonadal or other extrago-nadal primary site and origin entirelywithin the lung.
ICD-O code
Teratoma mature 9080/0Teratoma immature 9080/3
Epidemiology
The majority of cases occur in the sec-ond to fourth decades (range 10 monthsto 68 years) with a slight female prepon-derance.
Localization
Teratomas are more common in theupper lobes, principally on the left side{78,1373,1931}.
Clinical features
Patients present most often with chestpain, followed by haemoptysis, coughand pyothorax {78,1373,1969}.Expectoration of hair (trichoptysis) is themost specific symptom {1373,1971,2056}. Radiologically, the lesions are typ-ically cystic masses, often with focal cal-cification {1373}.
Macroscopy
Tumours range from 2.8-30 cm in diame-ter. They are generally cystic and multi-loculated, but may rarely be predomi-nantly solid, the latter tending to beimmature. Cysts are often in continuitywith the bronchi and may have an endo-bronchial component {1373}.
Tumour spread and staging
Pulmonary mature teratomas are benign.Rupture may result in spillage of cystcontents that may cause bronchopleuralfistulas and a marked inflammatory andfibrotic reaction.
Histopathology
Mesodermal ectodermal and endoder-mal elements are seen in varying propor-tions {78}. Most pulmonary teratomas arecomposed of mature, often cystic somat-ic tissue, although malignant or immatureelements may occur. Of 31 casesreviewed, 65% were benign and 35%were malignant {1373}. Mature teratomasof the lung generally take the form ofsquamous-lined cysts similar to those ofthe ovary, also known as dermoid cysts.Malignant elements consisted of sarco-ma and carcinoma. Immature elements,such as neural tissue, infrequently occur.In mature teratomas, thymic and pancre-atic elements are often seen.
Differential diagnosis
Metastatic teratoma requires exclusionvia thorough clinical investigation. Ofnote, teratomas treated by chemothera-py often comprise wholly mature ele-ments in their metastases {268}.Carcinosarcomas, pleuropulmonaryblastomas and pulmonary blastomas donot recapitulate specific organ struc-tures.
Histogenesis
Pulmonary teratomas are thought to arisefrom ectopic tissues derived from thethird pharyngeal pouch.
Prognosis and predictive factors
Surgery is the treatment of choice with allmature teratomas being cured {1373}.Complete surgical resection may becomplicated if the tumour has rupturedwith bronchopleural fistula and a markedfibroinflammatory reaction. Resection ofmalignant teratomas has also led to pro-longed disease remission, although mostcases were unresectable and died within6 months of diagnosis.
Other germ cell tumours
Germ cell malignancies other than imma-ture teratomas are extremely rare andrequire exclusion of an extrapulmonaryprimary. They should also be distin-guished from carcinomas of the lung(including pleomorphic and giant cellcarcinomas), which may produce alpha-foetoprotein, chorionic gonadotrophins,or placental lactogen.Most cases reported as choriocarcinomaof the lung are pleomorphic carcinomaswith ectopic beta-HCG production.Instead of a dual population of cytotro-phoblasts and syncytiotrophoblasts typi-cal of choriocarcinoma, there is a contin-uous spectrum of morphology from largeto pleomorphic tumour cells.
A.G. NicholsonTeratoma
BAFig. 1.127 Mature teratoma. A Mature cartilage, glands and pancreatic tissue. B Pancreatic tissue with aci-nar and ductal epithelium. From Colby et al. {391} and Travis et al. {2024}.

120 Tumours of the lung - Miscellaneous tumours
Definition
Intrapulmonary thymomas are epithelialneoplasms histologically identical tomediastinal thymoma thought to arisefrom ectopic thymic rests within the lung{1238,1367}.
ICD-O code 8580/1
Epidemiology
Sex distribution differs between series,with one series showing a female pre-ponderance {1367} whilst others showgreater equality. Ages range from 17-77years, with a median of about 50 years.
Localization
Tumours may be hilar or peripheral.Pleural tumours are addressed in thepleural chapter.
Clinical features
Symptoms include cough, weight loss,chest pain, fever and dyspnoea.Tumours may occasionally be asympto-matic. Myasthenia gravis has been rarelydescribed {1367}.
Macroscopy
Sizes range from 0.5-12cm. Tumours areusually circumscribed encapsulated soli-tary masses although multiple cases aredescribed. The cut surface is frequentlylobulated and may be focally cystic, withvariable coloration.
Histopathology
Intrapulmonary thymomas show thesame features as those arising in themediastinum (see thymus chapter).
Immunohistochemistry
Immunohistochemical stains for keratinand epithelial membrane antigen high-light the epithelial cells scattered againstthe variable lymphoid cell background.Staining CD5 may stain the epithelial ele-ments and the lymphocytes stain forCD1a {632,1609}.
Differential diagnosis
Predominantly epithelial thymomas maybe mistaken for carcinomas and spindlecell carcinoids, and lymphocyte-rich vari-ants for lymphoma and small cell carci-
noma {1367}. Conversely, radiographicstudies and/or surgical inspection mustexclude primary mediastinal thymomasinfiltrating the lung. Thymomas usuallylack cytologic atypia and have a morelobulated architecture than small andnon-small cell carcinomas.
Histogenesis
Probable derivation from thymic epithe-lial rests.
Prognosis and predictive factors
Surgical resection appears the treatmentof choice with disease-free survival inmost patients when tumour is confined tothe lung. However, invasive tumours willlikely require additional treatment. Nodalinvolvement is also described and nodaldissection should therefore be consid-ered.
A.G. NicholsonC. Moran
Intrapulmonary thymoma
Fig. 1.128 Thymoma. A This pleural tumour shows lobules of epithelial cells surrounded by thick bands of fibrous stroma. B The tumour consists of a mixture ofthymic epithelial cells with a few lymphocytes. From Travis et al. {2024}.
BA

121Melanoma
Definition
Melanomas are malignant tumoursderived from melanocytes. Criteria for aprimary pulmonary origin include an infil-trating tumour arising from junctionalchange in the bronchial epithelium, aconcomitant naevus-like lesion, no histo-ry of previous melanoma and no tumourdemonstrable at another site at the timeof diagnosis.
ICD-O code 8720/3
Epidemiology
Metastatic melanoma to the lungs iscommon, but primary pulmonarymelanoma is extremely rare.
Localization
Most cases are endobronchial but originin the trachea is also described {515,928}. Solitary melanomas in peripherallung are usually metastatic.
Clinical features
There is an equal sex distribution, with amedian age of 51 years (range 29-80years) {928,1522}. Presentation is withobstructive symptoms.
Macroscopy
Most tumours are solitary and polypoid{928,2152}, although cases of ‘flat’melanomas have been described in the
trachea {1374}. Most show variable pig-mentation.
Histopathology
The tumour is typically lobulated andulcerative. Architecturally and cytologi-cally, the tumour cells are similar to thoseof melanoma at other sites. Often, thetumour spreads in Pagetoid fashion with-in the adjacent bronchial mucosa andrarely, benign nevus-like lesions can alsobe seen {928,2152}. Immunohistoche-mistry shows positivity for S-100 proteinand HMB-45. Ultrastructural analysisshows melanosomes within the cyto-plasm {2152}.
Differential diagnosis
Metastatic disease is the most commondifferential diagnosis and it may beimpossible to prove primary pulmonaryorigin with absolute certainty. Bronchialcarcinoids may be pigmented, but willstain for neuroendocrine markers and aretypically cytokeratin positive.
Precursor lesions
No precursor lesion is recognized.Nevus-like proliferation of melanocyticcells can be seen in the mucosa adja-cent to some primary pulmonarymelanomas, but benign naevi are notknown to occur in the bronchus andthese may be a cytologically bland form
of tumour spread, rather than a precursorlesion.
Histogenesis
It is uncertain whether they arise frommelanocytic metaplasia or from cells thatmigrated during embryogenesis.
Prognosis and predictive factors
Once pulmonary origin has been con-firmed, treatment is by surgical resec-tion,. Prognosis varies between series,but is generally poor {2152}. However,some patients remain free of disease forup to 11 years {928}.
A.G. NicholsonMelanoma
Fig. 1.129 Primary malignant melanoma. A Polypoid endobronchial mass with spread along the adjacent bronchial mucosa. B Tumour cells infiltrate the bronchialmucosa and involve the epithelium in a pagetoid fashion. From Colby et al. {391} and Travis et al. {2024}.
BA
Fig. 1.130 Cytology of an aspirate of metastaticmalignant melanoma. Highly pleomorphic and dis-sociated malignant cells. Note the presence ofnuclear pleomorphism, massive nucleoli, andoccasional nuclear pseudoinclusion.

122 Tumours of the lung - Secondary tumours
Definition
Tumours in the lung that originate fromextra-pulmonary sites or that are discon-tinuous from a primary tumour elsewherein the lung.
Synonyms
Secondary tumours in the lung.
Epidemiology
Most common sources of metastatictumours to lung, in relative order of fre-quency: breast, colon, stomach, pan-creas, kidney, melanoma, prostate, liver,thyroid, adrenal, male genital, femalegenital.At autopsy, the lungs are involved withtumour spread from extra-pulmonarysolid malignancies in 20-54% of cases{13,426,558,935,1692,2148} and in 15-25% of cases the lungs are the sole siteof tumour spread {558}. In some 3-7% ofcases of diagnosed primary lungtumours, there is another known primarycancer elsewhere {2202}.
Pathogenesis
Secondary tumours are the commonestform of lung neoplasm and the lungsreceive the most secondary tumours ofany organ. This is because the lungs arethe only organ to receive the entire bloodand lymph flow and they have the dens-
est capillary network in the body, thatnetwork also being the first encounteredby tumour cells entering the venousblood via the ductus lymphaticus {548,578,2237}. Also there is probablyfavourable “seed and soil” deposition inthe lungs as orignally proposed by Pagetin 1889 {1531}.
Localization
Some generalizations apply to second-ary tumours in the lungs. They are usual-ly, peripheral, have more discrete bor-ders, are harder to reach with fiberbron-choscopy forceps and less often shedcells for cytological examination thanlung primaries. Pulmonary metastases usually presentas multiple, bilateral pulmonary nodulesbut can also appear as solitary masses{13,319,442,935,1784,1961,2129}.Metastatic tumour nodules to the lungscan be present in any intrathoracic loca-tion but are most common in the lowerlobes {13,126,290,595,781,922,1605}.
Clinical features
Signs and symptoms Most patients with lung metastases donot have pulmonary symptoms. The fewwith endobronchial spread simulate pri-mary tumours by causing cough,haemoptysis, wheezing, and signs of
obstruction such as obstructive pneumo-nia, atelectasis, dyspnoea and fever{2131}. Those with pleural infringmentand/or effusion may have chest painand/or dyspnoea. Those with vascular orlymphangitic spread may have signs ofcor pulmonale.The following considerations are impor-tant in estimating the likelihood of alesion in the lung being metastatic in apatient with known extrapulmonarymalignancy: the patient’s age, smokinghistory, stage of the extrathoracic pri-mary, cell type and the disease free inter-val {2131}.
Imaging Typical metastatic disease to the lungspresents radiographically as multiplewell-defined pulmonary nodules.Cavitation may be present and in rareinstances, the margins of the nodulesmay be poorly defined. Calcification isuncommon but may be seen withmetastatic osteogenic sarcoma, ter-atomas and certain adenocarcinomas.On CT, more nodules are routinelydetected and their distribution and inter-nal characteristics are better defined.Endobronchial metastases are uncom-mon but when present cause the samepatterns of atelectasis as with primarylung neoplasms. When mediastinal or
D.H. DailP.T. CagleA.M. MarchevskyA. KhoorK. Geisinger
Metastases to the lung B. PugatchS.D. Finkelstein
K. KerrC. Brambilla
Fig. 1.131 A Metastatic carcinoma, intra-arterial spread. Small artery with endoluminal cancer cells and focal thrombus. B Metastatic adenocarcinoma, lymphaticspread. Lymphatic spaces are distended by metastatic adenocarcinoma.
BA

123Metastases to the lung
hilar lymph nodes are involved, CT scan-ning detects enlargement much earlierthan conventional radiographs. In lym-phangitic carcinomatosis the interstitialmarkings of the lung become prominentand irregular.
Relevant diagnostic procedures Routine chest radiography is the mosteffective means of detection. CT scansgive higher resolution, sometimes show-ing additional lesions that are hard todetect on plain chest radiographs. Attimes, perfusion scans are useful fordetecting tumour emboli. PET scans arevery helpful, although inflammatory con-ditions can also be PET scan positive.Pulmonary function tests are rarely help-ful except when there is endobronchialobstruction or extensive endovasularspread.Sputa, bronchial washes, brushes andlavages, and fine needle apirations,either transtracheal, transbronchial ortransthoracic, are as helpful in detectingmetastasis as they are with primary lungtumours. Transbronchial biopsy is valu-able with proximal lesions but less sowith small peripheral ones.
Cytology
Generally, there is little to allow distinc-tion of primary neoplasms from metas-
tases on morphology alone {582}.However, immunocytochemical, cytoge-netic, and molecular analyses, can beapplied directly to cytological materialjust as readily as to histological speci-mens.Metastatic colonic carcinoma classicallypresents in smears as cohesive flatsheets with peripheral nuclear palisad-ing, elongated nuclei, and a backgroundof necrotic debris. Similarly, signet ringcell carcinomas are more likely to bemetastatic from sites such as the stom-ach. Lobular adenocarcinoma of thebreast may also have a sufficiently dis-tinct morphology: the tumour cells arerelatively small and homogeneous withsolitary nuclei without hyperchromatismor prominent nucleoli, and may possesscytoplasmic vacuoles. Linear arrays oftumour cells without well developednuclear molding may be present.Squamous cell carcinomas metastatic tothe lungs generally do not have any dis-tinguishing morphological attributes{582}.Melanomas typically show little intercellu-lar cohesion and melanin pigment issometimes evident {618}.In the paediatric population, mosttumours fall into the small round cell cat-egory and the primary neoplasm is oftenknown at the time of detection of metas-
tases {672}. A major distinguishing pointis lymphoreticular versus nonlym-phoreticular. For the former, diagnosticfeatures in the smears include an almosttotal lack of intercellular cohesion, rela-tively finely granular chromatin, and lym-phoglandular bodies in the background.
Macroscopy
Metastatic neoplasms presenting withmultiple pulmonary nodules are variablein gross appearance according to theirsite of origin, histopathology and patternof spread {1605,1961} They vary in sizefrom small, miliary lesions (e.g.melanoma, ovarian carcinoma, germ cellneoplasms) to large, confluent, “cannon-ball” masses (e.g. sarcomas, renal cellcarcinoma) {781,1605}. Metastatic ade-nocarcinomas are usually firm, grey-tanwith areas of necrosis and haemorrhage{1633}. Mucin-secreting adenocarcino-mas of gastrointestinal, pancreatic,breast, ovary and other site origin exhib-it a wet, slimy, glistening yellow-tan sur-face {13,126,935}. Metastatic colonicadenocarcinomas usually exhibit exten-sive necrosis with/without cavitation{595}. Metastatic squamous cell carcino-mas have a grey, dry surface with punc-tate areas of necrosis {13,126,442}.Renal cell carcinomas usually present asyellow nodule/s {1605}. Metastatic sarco-mas and malignant lymphomas usuallyhave a firm, grey, glistening, “fish-flesh”surface. Metastatic angiosarcomas tendto exhibit a dark red, haemorrhagic sur-face, while melanomas may be black.
Histopathology
Patterns of spread of metastatic neo-plasms to the lung are well known{442,911,1590,1605} but are seldomhelpful in identifying the site of origin ofthe metastatic neoplasm. Metastatictumour emboli (e.g. sarcomas, others)may occlude the main pulmonary arteryor present as multiple pulmonary emboli(breast, stomach, others) {90,876}.Metastatic neoplasms may also presentas single or multiple endobronchial poly-poid lesions (e.g. head and neck, breast,kidney, others), interstitial thickening dueto lymphangitic spread (e.g. lung, breast,gastrointestinal, others), cavitary lesions(e.g. squamous cell carcinoma, sarco-mas, teratoma, others) pleural nodules ordiffuse areas of consolidation that simu-late a pneumonia (e.g. pancreas, ovary,others).
DCFig. 1.132 Secondary tumours. A Multiple nodules of similar size, metastatic from cholangiocarcinoma.From Dail and Hammar {434}. B Large tumour thrombus to main pulmonary artery. From Colby et al. {391}. C Metastatic renal cell carcinoma, situated in major brochus. D Metastatic leiomyosarcoma. Higher grosspower of cystic metastatic uterine leiomyosarcoma. From Dail and Hammar {434}.
BA

124 Tumours of the lung - Secondary tumours
ImmunohistochemistryThis is a valuable tool for the distinctionbetween primary and metastatic lungneoplasms. For example, approximately80% of primary lung adenocarcinomasexhibit nuclear TTF-1 immunoreactivity,an epitope that can also be seen in thy-roid neoplasms but is absent in otheradenocarcinomas {138,352,704,773,1564}. Thyroid neoplasms exhibit cyto-plasmic thyroglobulin immunoreactivitywith a high frequency; this is absent inprimary lung tumours and it is useful todemonstrate thyroglobulin negativity inTTF-1 positive lung tumours to exclude ametastasis from the thyroid. Primary ade-nocarcinomas of the lung usually exhibitkeratin 7 and variable keratin 20 cyto-plasmic immunoreactivity unless thetumour expresses mucin {184,366,368}.In contrast, colonic adenocarcinomasexhibit a cytoplasmic keratin profile ofCK 20 positive/ CK 7 negative as well asCDX-2. {184,352,366,368,704,766,773,1307,2082}. Breast neoplasms canexhibit nuclear immunoreactivity forestrogen receptor, a finding that isabsent in primary lung lesions {976,1528,1657,1737}. Renal cell carcinomasusually stain weakly with keratinAE1/AE3, and keratin 7 and exhibitstrong cytoplasmic vimentin immunore-activity. Metastatic carcinomas of theovary usually express immunoreactivityfor CA125, N-cadherin, vimentin, oestro-gen receptor, and inhibin and negativeCEA immunoreactivity {976,1486,2189}.
Differential diagnosis
Some adenocarcinomas have character-istic histopathological features. Forexample, a cribriform pattern character-izes colonic adenocarcinoma {595}.Necrosis with nuclear debris is also com-mon in metastatic colonic adenocarcino-mas. Renal cell carcinomas typicallyhave clear cells arranged in nests sur-rounded by a rich vascular network{1605}. In squamous cell carcinoma,severe dysplasia or in situ carcinomafavours a primary lung neoplasm{13,935}.
Somatic genetics
Cytogenetics and CGH In poorly differentiated secondary neo-plasms of unknown primary site in whichconventional light microscopic, immuno-histochemical, and electron microscopictechniques fail to yield a specific diagno-
sis, cytogenetic analysis promises toincrease diagnostic acuity. However,information on nonrandom (recurrent)chromosomal aberrations in solidtumours is currently limited.When data from different cytogeneticstudies are combined, a pattern of non-random genetic aberrations appears{1890}. As expected, some of theseaberrations are common to differenttypes of tumours {270}, whereas othersare more tumour-specific. For example,recent studies suggest that CGH analy-sis may be helpful in separating benignmesothelial proliferation, malignantmesothelioma, and metastatic adenocar-cinoma {1427}. Continued technicalrefinement of cytogenetic techniques willlead not only to improved understandingof tumour pathobiology, but also togreater clinical applicability.
Molecular genetic alterations Many of the same molecular geneticalterations of tumour suppressor genesand oncogenes can be found in both pri-mary pulmonary carcinomas and inmetastatic carcinomas. Only thosemolecular genetic markers that are spe-cific or relatively restricted to metastaticcarcinomas are candidates for diagnosisof a metastasis with identification of theprimary site. For diagnostic purposes,expression of putative primary site spe-cific molecular markers can be most con-veniently accomplished by reverse-tran-
scriptase-polymerase chain reactionamplification (RT-PCR) and immunohisto-chemistry. Adenocarcinomas metastaticto the lungs are a common problem indifferential diagnosis due to theirhistopathologic resemblance to primarylung adenocarcinomas. Among themolecular markers that are specific orrelatively restricted for site of origin ofadenocarcinomas are prostate specificantigen for prostate, mammaglobin 1 forbreast, TFF2 for pancreas, pepsinogen Cfor stomach, PSCA for pancreas, metal-lothionein IL for pancreas, uroplakin II forbladder, MUC II for colon, A33 for colon,lipophilin B for breast, ovary and prostateand glutathione peroxidase 2 for colonand pancreas. Diagnostic genesdetectable by RT-PCR are recognized fora number of sarcomas that might metas-tasize to the lung. Examples include theSYT-SSX fusion genes in synovial sarco-mas and EWS-ETS fusion genes in theEwings family of sarcomas. There ispromise that comparative molecular pro-files may enable recognition of primaryversus metastatic tumours in the lung{1681,1745,1750}.
Fig. 1.133 Metastatic prostate carcinoma staining for prostate specific antigen. Typically, PSA is notexpressed in primary lung tumours.