Tumors of the Mesentery and Omentum...
27
Introduction Cross-sectional imaging techniques (ultrasound (US), computed tomography (CT) and magnetic resonance imaging (MRI)) will depict abdominal lesions in the connecting folds of tissue that constitute the mesentery (including small bowel mesentery, mesocolon, mesosig- moid and mesoappendix) and omentum (including both greater omentum or epiploon) and lesser omen- tum or gastrohepatic ligament. All of these folds of tis- sue are covered by peritoneum. Chapter Contents Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 447 Cystic Masses . . . . . . . . . . . . . . . . . . . . . . . . . . 448 Mesenteric/Omental Cysts . . . . . . . . . . . . . . . . . . 448 Lymphangioma . . . . . . . . . . . . . . . . . . . . . . . . 448 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 448 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 449 Enteric Duplication Cyst . . . . . . . . . . . . . . . . . . . 450 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 450 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 450 Enteric Cyst . . . . . . . . . . . . . . . . . . . . . . . . . . 451 Mesothelial Cyst . . . . . . . . . . . . . . . . . . . . . . . 451 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 451 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 452 Nonpancreatic Pseudocyst . . . . . . . . . . . . . . . . . . 452 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 452 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 452 Teratoma . . . . . . . . . . . . . . . . . . . . . . . . . . . 452 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 452 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 452 Cystic Mesothelioma . . . . . . . . . . . . . . . . . . . . . 453 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 454 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 454 Cystic Spindle Cell Tumor . . . . . . . . . . . . . . . . . . 455 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 455 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 455 Pseudomyxoma Peritonei . . . . . . . . . . . . . . . . . . 456 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 456 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 456 Miscellaneous Cystic Mesenteric/Omental Lesions . . . . . 456 Pancreatic Pseudocyst . . . . . . . . . . . . . . . . . . . . 456 Mycobacterium avium-intracellulare Adenopathy . . . . 456 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 456 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 457 Complicated Ascites . . . . . . . . . . . . . . . . . . . . . 457 Solid Masses . . . . . . . . . . . . . . . . . . . . . . . . . . . 457 Infectious Diseases . . . . . . . . . . . . . . . . . . . . . . . 457 Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . 457 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 458 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 458 Neoplasms . . . . . . . . . . . . . . . . . . . . . . . . . . . . 459 Lipoma, Liposarcoma . . . . . . . . . . . . . . . . . . . . 459 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 459 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 460 Neural Tumors (Neurofibroma, Schwannoma) . . . . . . 461 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 461 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 461 Malignant Mesothelioma . . . . . . . . . . . . . . . . . . 462 Pathologic Findings and Imaging Features . . . . . . . 462 Malignant Fibrous Histiocytoma . . . . . . . . . . . . . . 463 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 463 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 463 Spindle Cell Tumor (Leiomyoma/Leiomyosarcoma) . . . 464 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 464 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 464 Lymphoma, Metastasis . . . . . . . . . . . . . . . . . . . . 465 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 465 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 465 Miscellaneous Solid Mesenteric/Omental Lesions . . . . . . 466 Fibrosing Mesenteritis (Mesenteric Panniculitis) . . . . . 466 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 467 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 467 Fibromatosis (Desmoid Tumor) . . . . . . . . . . . . . . . 467 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 468 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 468 Castleman’s Disease . . . . . . . . . . . . . . . . . . . . . 469 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 469 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 469 Splenosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 469 Pathologic Findings . . . . . . . . . . . . . . . . . . . . 470 Imaging Features . . . . . . . . . . . . . . . . . . . . . . 470 Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . 470 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . 470 Tumors of the Mesentery and Omentum Hoon Ji, Pablo R. Ros 4.11
Transcript of Tumors of the Mesentery and Omentum...

Introduction
Cross-sectional imaging techniques (ultrasound (US),computed tomography (CT) and magnetic resonanceimaging (MRI)) will depict abdominal lesions in theconnecting folds of tissue that constitute the mesentery(including small bowel mesentery, mesocolon, mesosig-moid and mesoappendix) and omentum (includingboth greater omentum or epiploon) and lesser omen-tum or gastrohepatic ligament. All of these folds of tis-sue are covered by peritoneum.
Chapter
Contents
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . 447
Cystic Masses . . . . . . . . . . . . . . . . . . . . . . . . . . 448Mesenteric/Omental Cysts . . . . . . . . . . . . . . . . . . 448Lymphangioma . . . . . . . . . . . . . . . . . . . . . . . . 448
Pathologic Findings . . . . . . . . . . . . . . . . . . . . 448Imaging Features . . . . . . . . . . . . . . . . . . . . . . 449
Enteric Duplication Cyst . . . . . . . . . . . . . . . . . . . 450Pathologic Findings . . . . . . . . . . . . . . . . . . . . 450Imaging Features . . . . . . . . . . . . . . . . . . . . . . 450
Enteric Cyst . . . . . . . . . . . . . . . . . . . . . . . . . . 451Mesothelial Cyst . . . . . . . . . . . . . . . . . . . . . . . 451
Pathologic Findings . . . . . . . . . . . . . . . . . . . . 451Imaging Features . . . . . . . . . . . . . . . . . . . . . . 452
Nonpancreatic Pseudocyst . . . . . . . . . . . . . . . . . . 452Pathologic Findings . . . . . . . . . . . . . . . . . . . . 452Imaging Features . . . . . . . . . . . . . . . . . . . . . . 452
Teratoma . . . . . . . . . . . . . . . . . . . . . . . . . . . 452Pathologic Findings . . . . . . . . . . . . . . . . . . . . 452Imaging Features . . . . . . . . . . . . . . . . . . . . . . 452
Cystic Mesothelioma . . . . . . . . . . . . . . . . . . . . . 453Pathologic Findings . . . . . . . . . . . . . . . . . . . . 454Imaging Features . . . . . . . . . . . . . . . . . . . . . . 454
Cystic Spindle Cell Tumor . . . . . . . . . . . . . . . . . . 455Pathologic Findings . . . . . . . . . . . . . . . . . . . . 455Imaging Features . . . . . . . . . . . . . . . . . . . . . . 455
Pseudomyxoma Peritonei . . . . . . . . . . . . . . . . . . 456Pathologic Findings . . . . . . . . . . . . . . . . . . . . 456Imaging Features . . . . . . . . . . . . . . . . . . . . . . 456
Miscellaneous Cystic Mesenteric/Omental Lesions . . . . . 456Pancreatic Pseudocyst . . . . . . . . . . . . . . . . . . . . 456Mycobacterium avium-intracellulare Adenopathy . . . . 456
Pathologic Findings . . . . . . . . . . . . . . . . . . . . 456Imaging Features . . . . . . . . . . . . . . . . . . . . . . 457
Complicated Ascites . . . . . . . . . . . . . . . . . . . . . 457
Solid Masses . . . . . . . . . . . . . . . . . . . . . . . . . . . 457
Infectious Diseases . . . . . . . . . . . . . . . . . . . . . . . 457Tuberculosis . . . . . . . . . . . . . . . . . . . . . . . . . . 457
Pathologic Findings . . . . . . . . . . . . . . . . . . . . 458Imaging Features . . . . . . . . . . . . . . . . . . . . . . 458
Neoplasms . . . . . . . . . . . . . . . . . . . . . . . . . . . . 459Lipoma, Liposarcoma . . . . . . . . . . . . . . . . . . . . 459
Pathologic Findings . . . . . . . . . . . . . . . . . . . . 459Imaging Features . . . . . . . . . . . . . . . . . . . . . . 460
Neural Tumors (Neurofibroma, Schwannoma) . . . . . . 461
Pathologic Findings . . . . . . . . . . . . . . . . . . . . 461Imaging Features . . . . . . . . . . . . . . . . . . . . . . 461
Malignant Mesothelioma . . . . . . . . . . . . . . . . . . 462Pathologic Findings and Imaging Features . . . . . . . 462
Malignant Fibrous Histiocytoma . . . . . . . . . . . . . . 463Pathologic Findings . . . . . . . . . . . . . . . . . . . . 463Imaging Features . . . . . . . . . . . . . . . . . . . . . . 463
Spindle Cell Tumor (Leiomyoma/Leiomyosarcoma) . . . 464Pathologic Findings . . . . . . . . . . . . . . . . . . . . 464Imaging Features . . . . . . . . . . . . . . . . . . . . . . 464
Lymphoma, Metastasis . . . . . . . . . . . . . . . . . . . . 465Pathologic Findings . . . . . . . . . . . . . . . . . . . . 465Imaging Features . . . . . . . . . . . . . . . . . . . . . . 465
Miscellaneous Solid Mesenteric/Omental Lesions . . . . . . 466Fibrosing Mesenteritis (Mesenteric Panniculitis) . . . . . 466
Pathologic Findings . . . . . . . . . . . . . . . . . . . . 467Imaging Features . . . . . . . . . . . . . . . . . . . . . . 467
Fibromatosis (Desmoid Tumor) . . . . . . . . . . . . . . . 467Pathologic Findings . . . . . . . . . . . . . . . . . . . . 468Imaging Features . . . . . . . . . . . . . . . . . . . . . . 468
Castleman’s Disease . . . . . . . . . . . . . . . . . . . . . 469Pathologic Findings . . . . . . . . . . . . . . . . . . . . 469Imaging Features . . . . . . . . . . . . . . . . . . . . . . 469
Splenosis . . . . . . . . . . . . . . . . . . . . . . . . . . . 469Pathologic Findings . . . . . . . . . . . . . . . . . . . . 470Imaging Features . . . . . . . . . . . . . . . . . . . . . . 470
Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . 470
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . 470
Tumors of the Mesentery and Omentum
Hoon Ji, Pablo R. Ros
4.11

448 Hoon Ji, Pablo R. Ros
Although uncommon, mesenteric/omental tumorsare encountered in all age groups from infancy to thevery elderly. These tumors should be considered as pos-sible causes for a palpable abdominal mass, but they aremost commonly brought into the differential diagnosisof abdominal pathology once discovered by a radiolog-ic study. An increased awareness of both neoplastic andnon-neoplastic processes resulting in mesenteric mass-es aids the clinical radiologist in differentiating thesediseases.
Cross-sectional imaging techniques are able to clear-ly depict mesenteric and omental masses and determineif they are cystic or solid. To make this determination, apractical approach involving both cystic and solid pat-terns is used, highlighting the radiologic-pathologicfeatures that may allow a specific diagnosis.
Cystic Masses
Once it is determined that a cystic abdominal mass aris-es from the mesentery or omentum rather than a solidabdominal organ, the differential diagnosis includesprimary mesenteric/omental cyst, mesenteric teratoma,cystic mesothelioma, cystic spindle cell tumor (cysticleiomyoma/leiomyosarcoma), pseudomyxoma perito-nei, pancreatic pseudocyst, mycobacterium avium-intracellulare (MAI) adenopathy and complicated as-cites (Table 1) [1, 2].
Mesenteric/Omental Cysts
Mesenteric/omental cysts are rare: the incidence isabout 1 per 140,000 general hospital admissions and
about 1 per 20,000 pediatric hospital admissions [3–5].In a study from Egleston Children’s Hospital at EmoryUniversity from 1965–1994, 14 patients were treated formesenteric or omental cysts, which represents a preva-lence of about 1 case per 11,250 admissions [6].Approx-imately one third of cases occur in children youngerthan 15 [7]. Mesenteric cysts are 4.5 times more com-mon than omental cysts [8].
A classification of mesenteric/omental cysts basedessentially on histopathological features should includethe following six groups: (1) cysts of lymphatic origin(simple lymphatic cyst and lymphangioma); (2) cysts ofenteric origin (enteric cyst and enteric duplicationcyst); (3) cysts of mesothelial origin (simple mesothelialcyst, benign cystic mesothelioma, and malignant cysticmesothelioma); (4) cysts of urogenital origin; (5) ma-ture cystic teratoma (dermoid cysts), and (6) pseudo-cysts (infectious and traumatic cysts) (Table 2).
Lymphangioma
Lymphangioma is the most common subtype of mesen-teric/omental cyst and represents a congenital malfor-mation of the lymphatic vessels arising from the bowel[4]. Ninety-five percent of lymphangiomas are found inthe neck and axilla [9]. In cases with the mesenter-ic/omental lymphangioma, abdominal distention with apalpable mass is the most common clinical presentation[10].
Pathologic Findings
Lymphangiomas are large, thin-walled multiloculatedcystic masses lined with endothelium (Fig. 1). The con-tents may be chylous or hemorrhagic. Prominent stro-mal myxoid degeneration may occur rarely [11]. Lym-phangiomas are intimally attached to the bowel walland are the only type of mesenteric/omental cyst thatroutinely requires bowel resection for removal [10].
Table 1. Mesenteric/Omental Cystic Massesa
I. Mesenteric/Omental CystLymphangiomaEnteric duplication cystEnteric cystMesothelial cystNonpancreatic pseudocyst
II. NeoplasmsTeratomaCystic mesotheliomaCystic spindle cell tumor (leiomyoma/leiomyosarcoma)Pseudomyxoma peritonei
III. MiscellaneousPancreatic pseudocystMAI adenopathyComplicated ascites
a Modified from references 1 and 10
Table 2. Histologic Classification of Mesenteric/Omental Cystsa
Diagnosis Histologic Features
Lymphangioma Endothelial lining
Enteric duplication cyst Enteric lining, double musclelayer with neural elements
Enteric cyst Enteric lining, no muscle layer
Mesothelial cyst Mesothelial lining
Pseudocyst (nonpancreatic) No lining, fibrous wall
a From reference 3

Chapter 4.11 Tumors of the Mesentery and Omentum 449
Imaging Features
Plain radiograph and barium studies may demonstratea small bowel obstruction (frequently partial) and pos-sibly a noncalcified soft-tissue mass or displaced bowelloops [10]. US demonstrates lymphangiomas to be ane-choic, multiseptate masses (Fig. 2). On CT, they are mul-tiloculated, frequently seen surrounding or tethered bya loop of bowel from where they originate and withHounsfield units ranging from water (if the contents areserous) to fat (if the contents are chylous) attenuation[12]. CT allows differentiation of lymphangioma fromascites with separation of bowel loops, absence of fluid
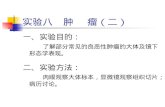
Fig. 1A, B. Lymphangioma: pathology. A Photomicrograph demon-strates a typical lymphangioma consisting of multiloculated cysticlesion with endothelial cell lining. B Resected specimen shows thelarge mass intimately attached to bowel
Fig. 2A–C. Lymphangioma: imaging features. A Ultrasonogram(US) demonstrates a large multilocular cystic mass in abdomen.B Enhanced CT scan of the abdomen demonstrates a multilocularcystic mass containing fluid of water attenuation. C T1-weightedMR image of the entire abdomen in the sagittal plane demon-strates a large mass centered in the mesentery. The high-intensityof the fluid corresponds to the fat seen in the chylous material typ-ically contained in lymphangiomas

450 Hoon Ji, Pablo R. Ros
in the perihepatic spaces and cul-de-sac, and focal sep-tations [13]. MRI is helpful to characterize the chylous(fatty nature) of the contents due to high signal inten-sity in T1-weighted images [14].
Enteric Duplication Cyst
Duplications of the alimentary tract are uncommoncongenital abnormalities. When an enteric duplication(usually attached to the bowel) migrates into the me-sentery, it becomes a mesenteric cyst [10]. Duplicationsare usually observed early in life, but a minority re-mains unsuspected until adulthood [15]. The clinicalpresentation may depend on the location of the duplica-tion and adjacent structures, and includes abdominaldistention, vomiting, bleeding, and a palpable abdomi-nal mass. The symptoms and signs produced by dupli-cations, however, are often vague [16]. Complicationssuch as perforation, intussusception, volvulus, and asso-ciated malignancy may occur [17].
Pathologic Findings
Enteric duplication cysts are usually small, thick-walledand unilocular with predominantly serous contents.The wall “reduplicates” the normal wall of the bowel andcontains all layers, including mucosa, circular and lon-gitudinal muscular layers and mesenteric plexus(Fig. 3). Gastric mucosa can be present in 17%–36% ofduplication cysts [18–20], and which may cause gas-trointestinal bleeding.
Imaging Features
By US, enteric duplication cysts have a thick wall similarin composition to the normal bowel wall. It containsmultiple layers, typically including an echogenic innermucosal layer and a hypoechoic outer muscular layer(Fig. 4). Enteric duplication cysts containing gastric mu-cosa may be demonstrated with uptake of technetium-
Fig. 3A, B. Enteric duplication cyst: pathology. A Photomicrographdemonstrates a typical enteric duplication cyst with thick walllined by enteric epithelium. B Gross specimen shows a thick-walled unilocular cystic mass with serous contents
Fig. 4A, B. Enteric duplication cyst: imaging features. A US demon-strates a small unilocular cystic lesion with multilayered wall.B Axial T1-weighted MR image demonstrates a low signal intensitylesion with thick wall (arrow)

Chapter 4.11 Tumors of the Mesentery and Omentum 451
99m sodium pertechnetate [19]. CT and MRI reveal acystic mass in the mesentery with a thick wall that en-hances after administration of contrast material. Atten-uation of the lesion on CT scans may be high due to themucoid-rich viscous fluid within the cyst [1, 20].
Enteric Cyst
Enteric cysts are lined with enteric (gastrointestinaltract) mucosa, and have a thin fibrous wall (without re-duplication of the bowel wall as in enteric duplicationcysts) [10, 21]. They are usually unilocular with serouscontents and a thin, smooth wall that cannot be visual-ized by CT or MRI [1, 10] (Fig. 5).
Mesothelial Cyst
Mesothelial cysts are the rarest type of mesenter-ic/omental cyst and are the result of a failure in the co-alescence of the mesothelially lined peritoneal surfaces[10]. The reported incidence varies between 1 in 30,000and 1 in 200,000 admissions [22]. Clinical presentationincludes an asymptomatic abdominal mass, vaguechronic abdominal complains, nausea, vomiting or diar-rhea [23].
Pathologic Findings
Mesothelial cysts are thin-walled with a characteristicmesothelial lining of the inner surface (Fig. 6).Althoughthey may occur in the mesentery, they are more com-mon in the greater omentum and mesocolon [4, 10].
Fig. 5. Enteric cyst: CT appearance. A well-defined cystic mass with attenuation in therange of water is seen in the mesentery, nearthe superior mesenteric vessels. Note thatthe wall is not perceptible by CT
Fig. 6A, B. Mesothelial cyst. A Photomicrograph demonstrates athin-walled cystic mass with mesothelial lining of the inner sur-face. B CT scan shows a large cystic mass displacing bowel loops

452 Hoon Ji, Pablo R. Ros
Imaging Features
US and CT demonstrate unilocular, thin-walled cysticmass (Fig. 6). They are indistinguishable radiologicallyfrom enteric cysts [1, 10, 22].
Nonpancreatic Pseudocyst
By definition, nonpancreatic pseudocysts have no innercellular lining and are thought to be the sequelae of ei-ther a mesenteric/omental hematoma or abscess [10].
Pathologic Findings
They are thick-walled cystic masses with no lining epi-thelium, usually septate and contain hemorrhagic orpurulent debris.
Imaging Features
Radiologically, nonpancreatic pseudocysts have a thickwall and may contain fluid-fluid levels corresponding tohemorrhagic or purulent contents [1, 10] (Fig. 7).
Teratoma
This uncommon benign cystic neoplasm of the me-sentery or omentum occurs primarily in infancy orchildhood but rarely in adult [24–26]. Implantation ofovarian teratoma in the mesentery or omentum hasbeen proposed for an explanation of its pathogenesis[27]. Clinical presentation is usually a palpable masswith associated manifestations, depending on its loca-tion.
Pathologic Findings
Grossly, teratomas of the mesentery/omentum are pre-dominantly cystic with solid areas that contain fat orcalcification. Histologic components include three ger-minal layer elements such as skin appendages, cartilage,bone, adipose tissue, and glial/glandular tissue [10, 24](Fig. 8).
Imaging Features
Radiographically, calcifications are frequently present.Sonography reliably demonstrates the mixed cystic andsolid nature of the teratoma (Fig. 9). The cystic compo-nent shows an anechoic area in the tumor. The solid
Fig. 7. Nonpancreatic pseudocyst, CT appearance. Enhanced CT ofthe abdomen demonstrates a thick-walled cystic mass with a fluid-fluid level, typical of pseudocyst containing hemorrhagic debris
Fig. 8A, B. Mesenteric teratoma, pathologic findings. A Photomi-crograph demonstrates a typical teratoma consisting of cartilage,skin appendages, and fat. B Gross specimen shows a well-demar-cated cystic mass with heterogeneous internal contents

Chapter 4.11 Tumors of the Mesentery and Omentum 453
component shows homogeneous moderate-intensityechoes, and sometimes even higher echogenic areascharacteristic of fat and calcification [24]. CT demon-strates a predominantly cystic tumor with attenuationin the range of water except for peripheral areas in thefat attenuation range [24, 26] (Fig. 10). Calcificationsmay be identifiable as well.
Cystic Mesothelioma
Cystic mesothelioma is a rare benign neoplasm of theperitoneum, unrelated to malignant peritoneal mesoth-elioma. Cystic mesothelioma is not a malignant mesoth-elioma that has undergone necrosis and cystic transfor-mation. It is unrelated to asbestos exposure [2]. Cystic
Fig. 9A, B. Mesenteric teratoma, plain film and US findings. A Supine film of the abdomen in an infant demonstrates multiple dystrophiccalcifications in the left upper quadrant. B US shows a well-demarcated mass and cystic nature of the lesion
Fig. 10. Teratoma of the lesser omentum, CTappearance. A bilobed cystic mass is seenwith attenuation in the range of water. A fo-cus of calcification is seen in the central sep-tation (arrow). Areas of fat are seen periph-erally (arrowheads)

454 Hoon Ji, Pablo R. Ros
mesothelioma is almost always encountered in middle-aged women who present with abdominal pain and/or apalpable mass. It is considered a low-grade malignancybecause it recurs locally, although generally it does notmetastasize [28].Although it may involve any peritonealor omental surface, it is much more frequently seen inthe pelvis.
Pathologic Findings
The tumor is composed of multiple cysts, ranging insize from a few millimeters (mm) to six centimeters(cm) and containing clear watery fluid. Histopathologicfinding shows multiple mesothelium-lined cysts sur-rounded by a fibrovascular stroma [29] (Fig. 11).
Imaging Features
By ultrasound, they appear as multiloculated cysticmasses, usually large. CT demonstrates a well-defined,non-calcified mass, although a few cases with calcifica-tion have been reported [30, 31]. Cystic mesotheliomacompresses and surrounds bowel loops, but typicallydoes not cause bowel obstruction (Fig. 12). MRI showsthe cystic masses that have hypointensity on T1-weight-ed images and intermediate or hyper signal on T2-weighted images, correlating with their watery-like con-tents [1, 32] (Fig. 13).
Fig. 11. Cystic mesothelioma, pathologicfinding. Photomicrograph demonstrates typ-ical findings of a cystic mesothelioma com-posed of mesothelium-lined cysts surround-ed by a fibrovascular stroma
Fig. 12A, B. Cystic mesothelioma, US and CT features. A US of theupper abdomen demonstrates a multiple cystic mass with septa-tions. B On CT scan, multiple water-density masses are seen in theabdomen, displacing loops of bowel without obstructing them

Chapter 4.11 Tumors of the Mesentery and Omentum 455
Cystic Spindle Cell Tumor
Spindle cell tumors in the mesentery/omentum andgastrointestinal tract (i.e., gastrointestinal stromal tu-mor, leiomyoma/leiomyosarcoma, schwannomas) canundergo central liquefactive necrosis and hemorrhage,appearing as complex cystic mesenteric/omental mass-es on US or CT [1, 33, 34].
Pathologic Findings
Grossly, cystic mesenchymal tumors are large masseswith internal debris and hemorrhage. They may invadethe surrounding structures such as the bowel or solidabdominal organs. Microscopic examination may revealfoci of myxoid degeneration, microcyst formationepithelioid or spindle cells with prominent cytoplasmicvacuolization. Immunohistochemical studies enabledifferential diagnosis of subsets of mesenchymal tu-mors [34, 35].
Imaging Features
US demonstrates a complex mass with large amounts ofinternal echoes [33] (Fig. 14). By CT, the mass has a low-attenuation central zone surrounded by irregular walls
Fig. 13A, B. Cystic mesothelioma, MRI appearance. A T1-weightedMR image demonstrates a multilocular low signal intensity lesionin pelvic cavity. B T2-weighted MR image shows high signal inten-sity of the lesion correlating of watery contents
Fig. 14A, B. Cystic spindle cell tumor (leiomyosarcoma), imagingfeatures. A US demonstrates a large complex cystic mass with het-erogeneous internal echoes. B Axial CT scan shows a large, well-defined cystic mass with solid portion, corresponding to viableportions of the tumor

456 Hoon Ji, Pablo R. Ros
and a high-attenuation peripheral rim, correspondingto viable tumor [1, 34, 36].
Pseudomyxoma Peritonei
Pseudomyxoma peritonei is defined as massive and dif-fuse involvement of the peritoneal cavity by a low-grademetastatic mucinous adenocarcinoma originating inthe ovary, appendix, or colon. It is most common inwomen aged between 50–70 [37]. Clinically the maincomplaints of pseudomyxoma include abdominal pain,abdominal distention, partial bowel obstruction, andfistula formation [38].
Pathologic Findings
Typically pseudomyxoma peritonei manifests as multi-ple discrete nodules containing mucin on the peritone-
um (Fig. 15). It may have solid and hemorrhagic areasand septal calcifications. Microscopically pseudomyxo-ma nodules are characterized by multifocal pools ofmucin with scant strips of mucinous epithelium or var-ying proportion of glandular and signet ring cell com-ponents [1, 2].
Imaging Features
Ultrasonography is useful to detect hypoechoic cysts orascites with scalloping of hepatic or splenic marginsdue to extrinsic pressure of adjacent peritoneal im-plants [39]. CT scans demonstrates myxomatous tumorcollections that are of low attenuation (Fig. 15). Areas ofhigh attenuation or solid component can be seen withinit. Calcifications may also be present. Pseudomyxomaperitonei may mimic ascites, but it should not be con-fused with the latter, Pseudomyxoma peritonei, unlikeascites, produces scalloping of the liver and spleen, aswell as encasement with displacement of the gastroin-testinal tract [2, 38]. Spread of mucinous material to thepleural cavity may occur, presumably through the con-genital pleuroperitoneal communication [40]. MRI maybe useful in assessment of small bowel obstruction inpatients with pseudomyxoma peritonei [41].
Miscellaneous Cystic Mesenteric/Omental Lesions
Pancreatic Pseudocyst
Pancreatic pseudocysts are common cystic masses, se-quelae of acute pancreatitis. The clinical history, labora-tory findings and classic CT appearance are usually di-agnostic of this entity.
Mycobacterium avium-intracellulare Adenopathy
Mesenteric adenopathy may have marked low attenua-tion by CT, mimicking the appearance of multiple cysticmasses, such as those caused by infection with Myco-bacterium avium-intracellulare (MAI) [42].
Pathologic Findings
Multiple conglomerated nodular masses are found inthe mesentery and/or omentum, often adherent to bow-el and other solid organs. Cross-sectional specimensshow that caseous or liquefactive substances in the cen-ter of the enlarged lymph nodes are surrounded by in-flammatory lymphatic tissue and preserved blood ves-sels [43].
Fig. 15A, B. Pseudomyxoma peritonei. A Enhanced CT scan of theabdomen demonstrates multiple cystic masses encasing the stom-ach and producing scalloping of the liver. B Gross specimen showsthe multiple discrete nodules containing mucin on the peritoneum

Chapter 4.11 Tumors of the Mesentery and Omentum 457
Imaging Features
MAI lymphadenopathy has extremely low attenuationby CT with an enhancing rim [44]. The anatomic distri-bution and specific enhancement patterns of lymphad-enopathy seen on contrast-enhanced CT or MRI can beuseful in differentiating between tuberculosis and un-treated lymphomas of the abdominal lymph nodes [44,45] (Fig. 16). Enlarged lymph nodes with a low-attenua-tion center can also be seen in pyogenic infection andWhipple’s disease [44, 46].
Complicated Ascites
Complicated ascites (hemorrhagic or infected) will ap-pear as a multiseptate pseudomass mimicking a lym-phangioma or cystic mesothelioma (Fig. 17).
Solid Masses
While the cystic masses involving the mesentery andomentum are mainly benign (teratoma, mesentericcyst) or malignant with low-aggressiveness (cystic me-sothelioma), solid masses are overtly malignant (me-sothelioma, leiomyosarcoma) or characterized by high-ly aggressive behavior (fibromatosis). There is a widerange of solid masses involving the mesentery andomentum [47] (Table 3).
Infectious Diseases
Tuberculosis
In the developing world, tuberculosis continues to be anendemia, while in the West it has experienced a recent
Fig. 16A, B. MAI mesenteric lymphadenopathy. A CT scan and BT1-weighted MR image of a patient with HIV and MAI infectionshow multiple well-circumscribed, almost cystic-appearing mass-es with enhancing rims
Fig. 17A, B. Infected ascites mimicking a multiseptate mass. A USand B CT scan demonstrate multi-septate cystic lesions thatproved to be infected ascites

458 Hoon Ji, Pablo R. Ros
resurgence. The increased incidence of tuberculosis hasbeen attributed to several causes, including the AIDSepidemic, intravenous drug abuse, and increased immu-nocompromised patients [48].
Mesenteric/omental tuberculosis occurs most fre-quently in immunocompromised patients. Tuberculosiswithin the abdomen can potentially infect all abdomi-nal organs. Possible mechanisms in development of ab-dominal tuberculosis include hematogenous or lym-phatic dissemination from a distant focus, usually in thelung, and ingestion of infected milk or sputum [49].
Pathologic Findings
The causative organism is usually M. tuberculosis homi-nis, or atypical mycobacteria (M. avium-intracellulare).As elsewhere in the body, tuberculosis in the abdomenforms granulomas with typical caseous necrosis(Fig. 18). These may present clinically as ulcers or mass-es (tuberculoma).
Grossly, tuberculous granulomas aggregate to con-fluent masses, replacing the fat in the greater omentumand forming the so-called “omental cake pattern” [50].
Imaging Features
Abdominal tuberculosis may mimic a large variety ofconditions such as lymphoma, inflammatory bowel dis-eases, or other gastrointestinal tumors. Lymphadenopa-thy in mesentery or omentum is a common manifesta-tion of abdominal tuberculosis.
CT demonstrates mesenteric and omental tubercu-lous masses with replacement of the normal fat by en-hancing, high-attenuation masses that may containsmall islands of normal fat (Fig. 19). Tuberculous ade-nopathy is often identified in the mesentery. Contrastenhanced CT most commonly demonstrates peripher-ally enhancing lymph nodes with low-density centersreflecting the usual findings of a peripheral inflamma-tory reaction and central caseous necrosis [40, 48, 49].
On MRI, tuberculous adenopathy shows T1 iso- orhypointensity and central T2 hyperintensity [45] (Fig.16). Similar patterns, however, may be seen with metas-tases of malignant neoplasms, Whipple’s disease, andlymphoma [46, 51].
Tuberculous peritonitis is the most common presen-tation of abdominal tuberculosis. The several patternsof tuberculous peritonitis are described: wet, fibrotic,and dry types. The wet type, characterized by largeamounts of free or loculated viscus fluid, is most com-mon. CT demonstrates the nonspecific appearance ofascitic fluid with high Hounsfield units (25–45 HU) [52](Fig. 20). The fibrotic-fixed type is less common andcharacterized by omental masses, matted and tetheredbowel loops and mesentery. The dry type is unusual andcharacterized by caseous nodules, fibrous calcified ornoncalcified peritoneal reaction, and dense adhesions.Similar peritoneal features may occur with carcinomat-
Table 3. Mesenteric/Omental Solid Massesa
I. Infectious DiseasesTuberculosis
II. NeoplasmsPrimary benign tumors– Lipoma– Neural tumors (neurofibroma, schwannoma,
paraganglioma, ganglioneuroma)Primary malignant tumors– Malignant mesothelioma– Malignant fibrous histiocytoma– Spindle cell tumors (leiomyoma/leiomyosarcoma)– LiposarcomaSecondary tumors– Peritoneal carcinomatosis– Mesentery/omental metastases (carcinoid tumor)– Lymphoma
III. MiscellaneousFibrosing mesenteritisFibromatosis or desmoid tumorCastleman’s disease
Splenosis
a Modified from [2] and [47]
Fig. 18A, B. Tuberculosis: pathologic findings. A Microscopic find-ing of a tuberculous nodule demonstrates an inflammatory granu-loma with typical caseous necrosis in the center. B Gross specimenshows multiple indurated nodules in the omentum

Chapter 4.11 Tumors of the Mesentery and Omentum 459
osis, mesothelioma, and non-tuberculous peritonitis.Although there are occasionally difficulties of a diffe-rential diagnosis, a high degree of clinical suspicion andthe imaging features may allow early diagnosis of mes-enteric and omental tuberculosis.
Neoplasms
Lipoma, liposarcoma
Lipoma/liposarcoma arises from adipose tissue and isthe most common soft tissue tumor. While in the retro-
peritoneum liposarcomas are the most common neo-plasms, in the mesentery lipomas are much more com-mon. Lipoma is the second most frequent mesentericprimary tumor after fibromatosis [2].
Pathologic Findings
Histologically, liposarcomas are classified as well-differ-entiated, myxoid, pleomorphic, and round-cell sub-types. Prognosis for patients with liposarcoma varies onthe basis of the histologic subtype [53, 54].
Fig. 19. Tuberculosis. Axial CT scan demon-strates mesenteric and omental high-attenu-ation masses that may contain small islandsof normal fat
Fig. 20. Tuberculous peritonitis. Contrast-en-hanced CT scan of abdomen shows nonspe-cific ascitic fluid with high Hounsfield units.Note the enhancement of thickened perito-neum

460 Hoon Ji, Pablo R. Ros
Imaging Features
Although the site of origin cannot be determined beforesurgery, the diagnosis of lipoma is made relatively easi-ly with US, CT, or MRI.Well-differentiated liposarcomascan have two subtypes: fatty or lipoma-like and fibrousor sclerosing liposarcoma. Lipoma and lipoma-like lip-osarcoma demonstrate a well-defined mass, with nega-tive attenuation values on CT images or with hyperin-tensity in T1-weighted MR images. It may be impossibleto differentiate this type of liposarcoma from benignlipoma, although internal septations are unusual for lip-oma [55]. The sclerosing type of liposarcoma demon-strates the CT attenuation or MR signal intensity that
approximate the characteristics of muscle, and enhanc-es homogeneously on contrast enhanced CT or MR im-ages. Less differentiated liposarcomas have myxoid andpleomorphic subtypes. Myxoid components show CTattenuation and MR signal intensity similar to that ofwater.After contrast enhancement, gradual reticular en-hancement can be seen within the myxoid components.Some areas of myxoid liposarcoma may enhance mark-edly. Pleomorphic components show similar attenua-tion than muscle on CT images and signal intensity onT1-weighted MR images (Fig. 21). On T2-weighted MRimages, however, they have signal intensity equal to thatof fat (Fig. 22). Thus the pleomorphic component differsfrom the sclerosing component in MR signal intensity.
Fig. 22. Liposarcoma, MRI appearance. T1-weighted spin-echo image demonstrates alarge mass in the mesentery with predomi-nantly high signal intensity (*). There areperipheral components of lower signal in-tensity corresponding to areas with sarco-matous contents (arrowheads). Note multiplefibrous septa
Fig. 21. Pleomorphic liposarcoma. Axial CTscan demonstrates a large mesenteric masswith mainly solid in density

Chapter 4.11 Tumors of the Mesentery and Omentum 461
The round-cell type liposarcoma demonstrates similarattenuation and signal intensity to that of muscle. It ap-pears heterogeneous, while the sclerosing component isrelatively homogeneous on contrast-enhanced CT im-ages [54].
The combination of two or more histologic compo-nents in a tumor occurs commonly and results in thecombined characteristics of the individual subtypes.
Neural Tumors (Neurofibroma, Schwannoma)
Most benign nerve sheath tumors are either schwanno-ma or neurofibroma [56]. Schwannoma arises fromSchwann cell of the peripheral nerve sheaths. Schwan-noma is a slow-growing benign tumor with favorableprognosis. It occurs without sex predominance in the30–60-year age group [57]. They generally occur as asolitary mass located in the deep soft-tissue commonlyin the head and neck, mediastinum, retroperitoneum,pelvis, presacral location or in an extremity [58]. Thepatient presents with a slowly expanding mass that may or may not be symptomatic, depending on its loca-tion.
Neurofibroma is a benign neoplasm consisting of fi-broblasts, Schwann cells and nerve’s elements that ex-pand and diffusely infiltrate the nerve. Neurofibromasmay appear sporadically, or in patients with neurofibro-matosis without a sex predilection. They rarely can de-generate into a neurofibrosarcoma.
Pathologic Findings
Schwannomas are composed of Antoni type A (cellularpattern) and B (sparsely cellular pattern) areas. Theselesions begin as solid tumors but as they become larger,they undergo spontaneous degeneration with areas ofhemorrhage and cystic changes.
Typically in the abdomen, neurofibromas are mas-sive and plexiform (involving multiple continuousnerves), or forming discrete masses along the samenerve. They are gelatinous in consistence and homoge-neous in composition.
Imaging Features
On CT they appear as well-circumscribed masses. Al-though the presence of calcification on histology iscommon, on CT calcification is not usually evident(Fig. 23). The majority of these tumors are hypervascu-lar, showing an intense contrast enhancement. Schwan-nomas are often heterogeneous and are generally isoin-tense to muscle on T1-weighted images and hyperin-tense on T2-weighted images. The presence of a low-sig-
nal capsule is more suggestive of a schwannoma than ofa neurofibroma [59].
On CT, neurofibromas appear of low-density becauseof their myxoid matrix. They displace vessels and in-volve the root of the mesentery without producing bow-el obstruction or biliary dilatation (Fig. 24). Simple neu-rofibromas are usually smooth, well-demarcated, ho-mogeneous, hypodense masses relative to muscle. Theyenhance homogeneously with contrast material. LowCT density less than muscle is related to the high lipidand water content in the mucinous matrix, entrapmentof perineural adipose tissue, and cystic degeneration[57].
On MRI a target pattern with peripheral hyperin-tense rim and central low intensity has been describedin 50% of peripheral nerve sheath tumors but this dis-tinguishing feature is unlikely to be present in schwan-nomas due to degenerative changes [60–62]. The highT2 signal, enhanced peripheral component of the tumorrepresents myxomatous tissue, whereas the central lowT2 signal, hypovascular area represents fibrous and col-lagenous material [62] (Fig. 25). This zonal pattern doesnot correlate histologically with the proportion of Anto-ni-A and Antoni-B type tissue present [63].
Fig. 23A, B. Schwannoma. A Axial CT scan demonstrates a smallwell-circumscribed, homogeneous soft tissue mass in the mesent-ery. B Cut section of resected specimen shows whitish mass withno necrosis

462 Hoon Ji, Pablo R. Ros
Malignant Mesothelioma
Malignant mesothelioma is the primary malignancy ofthe peritoneum. While the majority originate in thepleura, 25% of cases arise in the peritoneum. The asso-ciation of asbestos exposure is higher with peritonealthan with pleural mesothelioma. The prognosis is ex-tremely poor. It presents usually in men with a historyof prior asbestos exposure.
Pathologic Findings and Imaging Features
Three different types of peritoneal malignant mesothe-lioma are recognized histologically with differentgrowth patterns and radiological appearance: (1) carci-nomatous, (2) sarcomatous, and (3) biphasic or mixed.The carcinomatous type appears as diffuse thickeningof the peritoneum with small nodular plaques in themesentery, producing crowning, fixation and diffusethickening of the small bowel (Fig. 26). Both parietaland visceral peritoneum are involved. Sarcomatous,peritoneal mesothelioma presents as a large encapsulat-ed mass, similar in appearance to spindle cell tumors(leiomyoma/leiomyosarcoma) (Fig. 27). The biphasic ormixed type presents as both a band of tissue involvingthe peritoneal surfaces and masses. Regardless of thehistological subtype, pleural plaques and calcificationdue to asbestos exposure can be present in approxi-mately 70% of cases [64] (Fig. 27). Gadolinium en-hanced breath hold fat-saturated MRI may reveal moreperitoneal tumors than CT, especially when ascites ispresent.
Fig. 24. Neurofibroma. Contrast enhancedCT scan demonstrates low attenuation massinvolving mesenteric root and porta hepatis
Fig. 25A, B. Neurofibroma, MRI appearance. A Axial CT shows lowattenuation soft tissue mass in right pelvic cavity. B T2-weightedMR image demonstrates the high signal intensity of the lesion dueto myxoid component

Chapter 4.11 Tumors of the Mesentery and Omentum 463
Malignant Fibrous Histiocytoma
Malignant fibrous histiocytoma (MFH) is one of themost common sarcomas appearing in late adult life.Typically it appears in the fifth and sixth decades of life.It frequently occurs in the soft tissue of the extremities,the retroperitoneum and in the bone [65–69]. Despitethis ubiquity, involvement of the peritoneal cavity is un-common.
Pathologic Findings
MFH is typically manifested as a broad range of histo-pathological appearances and is currently classifiedinto four subtypes: storiform-pleomorphic, myxoid,giant cell, and inflammatory. Microscopically MFH con-sists of areas of spindle cells arranged in a storiformpattern, and pleomorphic areas with haphazardly ar-ranged sheets of fibroblasts and histiocytes [66, 67].Calcification is common [68–71].
Imaging Features
Imaging features of MFH are nonspecific and most ex-amples of MFH appear as heterogeneous solid masseswith areas of necrosis [68–71]. A variety of patternshave been reported on ultrasound, including hypoecho-ic, mixed (due to tumor necrosis) or predominantly an-
Fig. 26A, B. Malignant mesothelioma (carcinomatous form). A CTscan demonstrates thickening of both parietal and visceral perito-neum. Note how mesothelioma surrounds multiple loops of boweland extends into the mesentery. B Cut sections of the specimenshow the diffuse tumor infiltration and bowel wall thickening
Fig. 27A–C. Malignant mesothelioma (sarcomatoid form). A AxialCT scan and B resected specimen demonstrate large mass withsimilar imaging features to stromal cell tumor. C CT shows pleuralcalcification plaque suggestive of asbestos exposure

464 Hoon Ji, Pablo R. Ros
echoic with thick septa. MFH generally presents as a hy-poechoic or heteroechoic solid mass [69, 70].
On CT, MFH typically presents as a poorly marginat-ed or well-circumscribed mass, with a density similar toor slightly less than that of normal muscle and with hy-podense areas due to necrosis [68–71]. Eccentrically lo-cated lumpy and ring-like calcifications due to osteoidand chondroid metaplasia have been reported on CT in16% of abdominal MFH [71]. Tumor invasion of contig-uous organs are common [68]. Occasionally MFH withextensive necrosis may be manifested as a cystic tumor[72, 73]. Extensive intratumoral hemorrhage may occur,creating a cyst-like tumor that may be confused withhematoma [67, 74].
MRI demonstrates the tumor usually of intermediateto low signal intensity on T1-weighted images. With T2-weighted images, the tumors tend to be of high signalintensity, although often quite inhomogeneous central-ly [75].
Spindle Cell Tumor (Leiomyoma/Leiomyosarcoma)
Spindle cell tumor or smooth muscle tumor are pre-ferred terms for mesenteric/omental leiomyoma/leiom-yosarcoma. Leiomyosarcoma is more common in themesentery than leiomyoma [76].
Pathologic Findings
Grossly, spindle cell tumors usually have central areas ofnecrosis, adenoma and hemorrhage (Fig. 28). Leiomyo-sarcomas are usually large, with invasion of surround-ing structures. They often contain no fat or calcification[77, 78].
Imaging Features
By US and CT, leiomyosarcomas usually appear as largeand heterogeneous masses. They are predominantly
Fig. 28A, B. Spindle cell tumor (leiomyosarcoma): pathology.A Photomicrograph demonstrates tumors with spindle cells inbundles. B Gross specimen shows a large solid mass lesion withmultiple cystic spaces suggesting central necrosis
Fig. 29A, B. Spindle cell tumor (leiomyosarcoma). A Ultrasonogramand B contrast enhanced CT scan demonstrate a huge solid masswith heterogeneous center

Chapter 4.11 Tumors of the Mesentery and Omentum 465
solid with internal cystic spaces, correlating with areasof necrosis grossly [79] (Fig. 29).
On MRI the mass is usually heterogeneous with lowto intermediate signal intensity on T1-weighted imagesand with intermediate to high signal intensity on T2-weighted images. Intratumoral necrosis is evident as ahigh intensity central zone on T2-weighed images, with-out enhancement [77, 78].
Lymphoma, Metastasis
Peritoneal carcinomatosis, carcinoid metastases andlymphoma are three common secondary malignanciesthat may involve the mesentery and omentum.
Primary mesenteric lymphoma, usually non-Hodg-kin lymphoma, is a disease of the mesenteric lymphnodes that may appear as a localized process or a com-ponent of a more disseminated pattern of disease.A fewcases of mesenteric lymphomas observed in associationwith AIDS, immune thrombocytopenia, and dermatitisherpetiformis have been reported [80]. The clinicalpresentation of mesenteric lymphoma is much like thatof other mesenteric tumors, with abdominal pain and apalpable mass as the principal findings.
The vast majority of metastatic lesions of the me-sentery consist of mesenteric lymph nodes that have be-come secondarily involved in a neoplastic process of thetubular gastrointestinal tract. Distinguishing this pat-tern of tumor growth from primary mesenteric tumorsusually presents no difficulty because the gastrointesti-nal primary tumor is usually readily identifiable.
Pathologic Findings
The appearance is variable, with lymphoma and car-cinomatosis frequently appearing as multiple masseswith variable degrees of involvement and carcinoidmetastases seen typically as a mesenteric mass pro-ducing kinking and retraction of adjacent bowel loopsand with frequent calcification [81]. This is due to thenotable desmoplastic reaction seen with carcinoid tu-mors.
Imaging Features
CT is the preferred imaging modality for evaluation ofthe mesentery in patients presenting with lymphoma.With lymphoma, bulky paraaortic lymphadenopathy iscommon (Fig. 30). Enlarged lymph nodes may appear asdiscrete masses or as confluent soft tissue obliteratingthe mesenteric fat, resulting in loss of definition of fatplanes between the other organs. Many other lymphnode groups, such as retrocrural, gastrohepatic, parace-liac, periportal, peripancreatic, posterior iliac crest, andpelvic chains are frequently involved [82]. CT scans cancharacterize the lesion from the standpoint of size andmesenteric location and can raise the probability of thelymphoma diagnosis [83].
Carcinoid metastases are seen typically as mesenter-ic masses producing kinking and retraction of adjacentbowel loops and with frequent calcification [81]. This isdue to the notable desmoplastic reaction seen with car-cinoid tumors (Fig. 31).
Fig. 30. Lymphoma. Axial CT scan demon-strates an irregular marginated soft tissuenodule in mesentery. Note the para-aorticlymphadenopathy

466 Hoon Ji, Pablo R. Ros
MRI is able to demonstrate similar findings in carci-noid tumors, including the primary tumor, mesentericmetastases, and liver metastases. Liver metastases arecommonly hypervascular on postgadolinium images[84].
Miscellaneous Solid Mesenteric/Omental Lesions
Fibrosing Mesenteritis (Mesenteric Panniculitis)
Fibrosing mesenteritis is a rare condition that can bemistaken for a mesenteric neoplasm based on clinical,radiologic, and gross characteristics. Fibrosing mesen-teritis is part of the same process that includes otherterms such as mesenteric lipodystrophy, sclerosing (re-tractile) mesenteritis, and mesenteric panniculitis. They
Fig. 31. Carcinoid tumors involving mesent-ery. Axial CT scan demonstrates a soft tissuemass with peripheral radiating strands inmesentery. Note the calcification in the massand mural thickening of adjacent smallbowel
Fig. 32A, B. Sclerosing mesenteritis. A Barium follow-thorough demonstrates kinking and displacement of ileum due to the mass. B Grossspecimen shows mesenteric mass formation with encasing small bowel segments

Chapter 4.11 Tumors of the Mesentery and Omentum 467
are all infiltrative mesenteric processes, with fatty, in-flammatory and fibrosing components. The causativeagents are unknown, although an association with lym-phoma has been reported. The likely cause for fibrosingmesenteritis is trauma or other injury to the mesentery[85, 86]. Fibrosing mesenteritis has a self-limited course,with resection only necessary when there is mechanicalbowel obstruction.
Its presenting symptom is abdominal pain in mostpatients, although it has been anecdotally reported inassociation with fever, mesenteric calcifications, andprotein-losing enteropathy.
Pathologic Findings
Grossly, fibrosing mesenteritis shows a firm, rubbery, fi-brous mass that can be either focal or diffuse within thesmall intestinal mesentery. The root of the mesenteryand the tissues surrounding the superior mesentericvessels are invariably involved (Fig. 32).
Histologically it consists of hypertrophied fatty tis-sue, dense fibrous tissue, fat necrosis, or combinationsof these, along with a nonspecific chronic inflammatoryinfiltrate with possible calcification.
Imaging Features
Barium study may demonstrate kinking or displace-ment of bowel loops due to mesenteric fibrous mass for-mation within the intestinal mesentery (Fig. 32).
By CT, fibrosing mesenteritis may appear as a softtissue density or heterogeneous mass, with possible cal-
cifications [87, 88] (Fig. 33). Puckering of adjacent smallbowel loops are seen. In MRI, fibrosing mesenteritis ap-pears as a low signal intensity mass in all sequences,suggesting mature fibrotic tissue [89–91].
Fibromatosis (Desmoid Tumor)
Fibromatosis (desmoid tumor) is a non-neoplastic lo-cally aggressive growth of fibroblastic tissue. Mesenter-ic fibromatosis (MF) is considered the most commonprimary solid mass of the mesentery. These tumors areareas of progressive fibroblastic and fibrous prolifera-tion within the mesentery (and less frequently, the ret-roperitoneum or omentum) that can locally involve vas-cular structures and can constrict and obstruct thebowel. Although described as histologically benign le-sions, their infiltrative pattern of growth can ultimatelylead to life-threatening patterns of visceral involvement[92].
Although MF occurs sporadically, it may be associat-ed with familial adenomatous polyposis (FAP). MF isidentified in 20 percent of asymptomatic FAP patients[93]. MF was originally reported as a component ofGardner syndrome, a phenotypic pattern of FAP that, inaddition to intestinal adenomatous polyps, is also asso-ciated with bony abnormalities, pigmented ocular fun-dus lesions, and cutaneous epidermoid cysts and fibro-mas. Prior surgery and local trauma are also frequentlynoted preceding the formation of mesenteric fibromat-osis [94]. Although a causative relationship in fibromat-osis formation has not been firmly established, variousmutations of the APC gene have been identified in thesetumors [95].
Fig. 33. Sclerosing mesenteritis, CT appear-ance. Enhanced CT of the abdomen demon-strates a mass in the mesentery with multi-ple calcifications. Note also the retractionand puckering of multiple loops of smalland large bowel

468 Hoon Ji, Pablo R. Ros
Pathologic Findings
Fibromatosis is usually a large mass with no capsule. Itmay have whitish scar tissue within it. It rarely has areasof necrosis or hemorrhage because it is a mass with be-nign histologic features. Histologic specimen shows or-derly arrangement of fibroblasts with uniform spine-shaped nuclei admixed to a variable amount of collagenand mucoid matrix [93] (Fig. 34).
Imaging Features
Ultrasonography demonstrates homogeneous hypo-echoic mass with no signs compatible with cystic de-generation or areas of diminished echogenicity sugges-tive of necrosis [96] (Fig. 35). By CT imaging, a masswith sharply defined margins is seen with homoge-neous density that has variable attenuation or en-
Fig. 34A, B. Pathologic findings of fibromatosis. A Gross specimenof fibromatosis shows a solitary fibrotic mass with no internal ne-crosis or hemorrhage. B The lesion reveals benign collagenousmyxoid histologic components of typical fibromatosis
Fig. 35. Fibromatosis, US finding. Ultrasonogram demonstrates ahomogeneous soft tissue mass with no areas of diminished echog-enicity suggestive of necrosis
Fig. 36A, B. Fibromatosis, CT appearance. A Enhanced CT of the ab-domen demonstrates a very large homogeneous mass. B After ad-ministration of contrast, there is marked enhancement of themass, correlating with its hypervascular nature. The lack of areasof hemorrhage or necrosis is typical of mesenteric fibromatosis

Chapter 4.11 Tumors of the Mesentery and Omentum 469
hancement after contrast administration [97] (Fig. 36).MRI demonstrates fibromatosis as a mass with lowsignal intensity relative to muscle on T1-weightedimages and variable signal intensity on T2-weightedimages [98]. High signal intensity on T2-weighted im-ages may be seen from rapidly growing fibromatosis[99] (Fig. 37).
Castleman’s Disease
Castleman’s disease is an uncommon benign lymphop-roliferative disorder characterized by hyperplasia oflymphoid follicles [100]. Castleman’s disease may occuranywhere along the lymphatic chain, but the mediasti-num is the most common location (70%). Extrathoracicsites have been reported in the neck, axilla, pelvis, pan-creas, adrenal, mesentery, and retroperitoneum [101].Clinically, patients are usually asymptomatic, althoughsometimes associated with systemic manifestationssuch as fever, anemia, weight loss, night sweat, and poly-clonal hypergammaglobulinemia [102]. Castleman’sdisease with systemic symptoms is usually bad in prog-nosis.
Pathologic Findings
There are two major histologic variants: The hyaline-vascular type, which is more frequent, is characterizedby small hyaline-vascular follicles and interfollicularcapillary proliferation; the plasma cell type is character-ized by large follicles with intervening sheets of plasmacells [101].
Calcification and central stellate fibrosis is not un-common in hyaline-vascular Castleman disease [102].
Imaging Features
The characteristic feature of localized Castleman dis-ease at CT is a well-defined, homogeneous, single massof soft tissue attenuation with or without satellite nod-ules (Fig. 38). The degree of enhancement may varyfrom mild to strong according to the histologic type[103]. Typically dynamic CT reveals the early strong en-hancement and delayed washout in hyaline-vasculartype [104]. Plasma cell type does not show strong en-hancement. Small lumpy calcifications may be seen inthe center of the mass.
The central fibrosis in hyaline-vascular type may bedemonstrated as interspersed area of low attenuationon CT and hypointense on both T1- and T2-weightedMR images [105].
No radiologic finding is pathognomonic for dissem-inated Castleman’s disease [101, 106].
Splenosis
Splenosis is the autotransplantation of residual frag-ments of splenic tissue in the abdomen and occasional-ly in the pelvis or thorax, following splenectomy typical-ly performed for traumatic splenic injury. The mostcommonly involved site is the peritoneal cavity. These
Fig. 37A, B. Fibromatosis, MRI appearance. A Axial CT image dem-onstrates a homogeneously low attenuation mass in the mesent-ery. B Coronal T1-weighted spin-echo image demonstrates a largemass in the mesentery with muscle intensity and lack of areas ofnecrosis or hemorrhage

470 Hoon Ji, Pablo R. Ros
foci of splenic tissue subsequently grow and regeneratenodules of functional splenic tissue [107]. Splenosisrarely becomes symptomatic in cases with infarction orspontaneous hemorrhage of intraperitoneal nodule,gastrointestinal wall implant, or recurrence of hemato-logic diseases (congenital hemolytic anemia, idiopathicthrombocytopenic purpura, etc) [108].
Pathologic Findings
Peritoneal splenosis may exhibit multiple round or ovalperitoneal nodules. Nodules of splenosis do not exhibita well-defined hilus. Most are up to 3 cm across but nod-ules up to 7 cm in greatest dimension have been report-ed [107].
Histological finding of splenosis may vary, but it mayexhibit read and white pulp that appears histologicallyand immunohistochemically indistinguishable fromnormal or accessory spleen [109].
Imaging Features
The characteristic feature of splenosis at ultrasound,CT, and MRI is multiple well-defined, round or oval, ho-mogeneous masses of soft tissue attenuation [110].They enhance uniformly with intravenous contrast me-dium.
MRI usually demonstrates hypointense signal of thenodules on both T1- and T2-weighted MR images, iden-tical to those of the normal spleen [111].
If necessary, their splenic origin can be confirmedwith Tc-99m-tagged, heat-damaged red blood cells orsulfur colloid scintigraphy [112].
Conclusion
A wide range of entities may involve the mesentery andomentum. The radiologist must be aware of the patho-logical changes commonly encountered, not only forensuring improvement in interpretation of imaging fea-tures but also for formulating a reasonable differentialdiagnosis.
CT, US, or MR imaging allows detecting the origin ofan abdominal mass as mesenteric/omental and whetherit is solid or cystic in nature. If the mass is cystic, the dif-ferential diagnosis should include benign mesenter-ic/omental cysts, such as cystic teratoma, cystic mesoth-elioma, and pseudocyst. However, it is important to re-member that some malignant neoplasms, such as spin-dle cell tumors, can occasionally have massive cysticchange and appear cystic by imaging.
Although there is substantial overlap in imaging fea-tures, it should be remembered that most solid massesinvolving the mesentery/omentum are neoplastic andmost are secondary malignant tumors. It is also impor-tant to consider the possibility of tuberculosis or lym-phoma, since these entities are usually treated withmedical therapy, and surgery should be avoided.
Acknowledgements. The authors are grateful to SethLevine for editorial assistance in preparing the manu-script.
References
1. Stoupis C, Ros PR, Abbitt PL, Burton SS, Gauger J (1994) Bub-bles of the belly: imaging of cystic mesenteric or omentalmasses. RadioGraphics 14 : 729–737
2. Hamrick-Turner JE, Chiechi MV, Abbitt PL, Ros PR (1992)Neoplastic and inflammatory processes of the peritoneum,omentum, and mesentery: diagnosis with CT. RadioGraphics12 : 1051–1068
3. Kurtz R, Heimann T, Holt J (1986) Mesenteric and retroperi-toneal cysts. Ann Surg 203 : 109–112
4. Takiff H, Calabria R, Yin L (1985) Mesenteric cysts and intra-abdominal cystic lymphangiomas. Arch Surg 120 : 1266–1269
Fig. 38A, B. Castleman disease. A Axial CT scan demonstrates a softtissue mass (arrowheads) in peripancreatic portion. B Gadolin-ium-enhanced axial T1-weighted image illustrates a large massdisplacing the IVC posteriorly. The mass shows intense enhance-ment (nearly equal to kidneys)

Chapter 4.11 Tumors of the Mesentery and Omentum 471
5. Vanek V, Phillips A (1984) Retroperitoneal, mesenteric, andomental cysts. Arch Surg 119 : 838–842
6. Egozi E, Ricketts R (1997) Mesenteric and omental cysts inchildren. Am Surg 63 : 287–290
7. Bliss DJ, Coffin C, Bower R (1994) Mesenteric cysts in chil-dren. Surgery 115 : 571–577
8. Walker A, Putnam T (1973) Omental, mesenteric, and retro-peritoneal cysts: a clinical study of 33 new cases. Ann Surg178 : 13–19
9. Singh S, Baboo ML, Pathak IC (1971) Cystic lymphangiomain children: report of 32 cases including lesions atrrare sites.Surgery 69 : 947–951
10. Ros PR, Olmsted WW, Moser RP Jr, Dachman AH, HjermstadBH, Sobin LH (1987) Mesenteric and omental cysts: histolog-ic classification with imaging correlation. Radiology 164 :327–332
11. Ko SF, Ng SH, Shieh CS, Lin JW, Huang CC, Lee TY.1995) Mes-enteric cystic lymphangioma with myxoid degeneration: un-usual CT and MR manifestations. Pediatr Radiol 25 : 525–527
12. Davidson AJ, Hartman DS (1990) Lymphangioma of the ret-roperitoneum: CT and sonographic characteristic. Radiology175 : 507–510
13. Lugo-Olivieri CH, Taylor GA (1993) CT differentiation oflarge abdominal lymphangioma from ascites. Pediatr Radiol23 : 129–130
14. Stoupis C, Ros PR, Williams JL (1993) Hemorrhagic lym-phangioma mimicking hemoperitoneum: MR imaging diag-nosis. J Magn Reson Imaging 3 : 541–542
15. Forshall I (1961) Duplication of the intestinal tract. PostgradMed J 37 : 570–589
16. Anderson MC, Silberman WW, Shields TW (1962) Duplica-tions of the alimentary tract in the adult. Arch Surg 85 :94–108
17. Otter MI, Marks CG, Cook MG (1996) An unusual presenta-tion of intestinal duplication with a literature review. Dig DisSci 41 : 627–629
18. Royle SG, Doig CM (1988) Perforation of the jejunum secon-dary to a duplication cyst lined with ectopic gastric mucosa. JPediatr Surg 23 : 1025–1026
19. Lecouffe P, Spyckerelle C, Venel H, Meuriot S, Marchandise X(1992) Use of pertechnetate 99mTc for abdominal scanningin localising an ileal duplication cyst: case report and reviewof the literature. Eur J Nucl Med 19 : 65–67
20. Tong SC, Pitman M, Anupindi SA (2002) Best cases from theAFIP. Ileocecal enteric duplication cyst: radiologic-patholog-ic correlation. Radiographics 22 : 1217–1222
21. de Perrot M, Brundler M, Totsch M, Mentha G, Morel P (2000)Mesenteric cysts. Toward less confusion? Dig Surg 17 :323–328
22. Gourtsoyiannis NC, Bays D, Malamas M, Mouchtouris A(1993) Mesothelial cyst complicated by torsion: preoperativeimaging evaluation. Hepatogastroenterology 40 : 509–512
23. Sardi A, Parikh KJ, Singer JA, Minken SL (1987) Mesentericcysts. Am Surg 53 : 58–60
24. Bowen B, Ros PR, McCarthy MJ, Olmsted WW, Hjermstad BM(1987) Gastrointestinal teratomas: CT and US appearancewith pathologic correlation. Radiology 162 : 431–433
25. Whang SH, Lee KS, Kim PN, Bae WK, Lee BH (1990) Omentalteratoma in an adult: a case report. Gastrointest Radiol 15 :301–302
26. Ralls PW, Hartman B, White W, Radin DR, Halls J (1987)Computed tomography of benign cystic teratoma of theomentum. J Comput Assist Tomogr 11 : 548–549
27. Moon W, Kim Y, Rhim H, Koh B, Cho O (1997) Coexistent cys-tic teratoma of the omentum and ovary: report of two cases.Abdom Imaging 22 : 516–518
28. O’Neil JD, Ros PR, Storm BL, Buck JL, Wilkinson EJ (1989)Cystic mesothelioma of the peritoneum. Radiology 170 :333–337
29. Weiss SW, Tavassoli FA (1988) Multicystic mesothelioma. Ananalysis of pathologic findings and biologic behavior in 37cases. Am J Surg Pathol 12 : 737–746
30. Hasan AK, Sinclair DJ (1993) Case report: calcification in be-nign cystic peritoneal mesothelioma. Clin Radiol 48 : 66–67
31. Ozgen A, Akata D, Akhan O, Tez M, Gedikoglu G, Ozmen MN
(1998) Giant benign cystic peritoneal mesothelioma: US, CT,and MRI findings. Abdom Imaging 23 : 502–504
32. Bui-Mansfield LT, Kim-Ahn G, O’Bryant LK (2002) Multicys-tic mesothelioma of the peritoneum. AJR Am J Roentgenol178 : 402
33. Volk BA, Scholmerich J, Farthmann E, Gerok W, Wenz W(1983) Leiomyoblastoma of the stomach–a case report onultrasonographic differential diagnosis of cystic lesions inthe abdomen. Hepatogastroenterology 30 : 33–35
34. McFadden DW, Hiyama D, Moulton JS, Biddinger P (1993)Primary mesenteric leiomyosarcoma masquerading as apancreatic pseudocyst. Pancreas 8 : 647–9
35. Miettinen M, Monihan JM, Sarlomo-Rikala M, Kovatich AJ,Carr NJ, Emory TS, Sobin LH (1999) Gastrointestinal stromaltumors/smooth muscle tumors (GISTs) primary in theomentum and mesentery: clinicopathologic and immunohis-tochemical study of 26 cases. Am J Surg Pathol 23 : 1109–1118
36. Lee JT, Kim MJ, Yoo KS, Suh JH, Leong HJ (1991) Primaryleiomyosarcoma of the greater omentum: CT findings. JComput Assist Tomogr 15 : 92–94
37. Jivan S, Bahal V (2002) Pseudomyxoma peritonei. PostgradMed J 78 : 170–172
38. Sulkin TV, O’Neill H,Amin AI, Moran B (2002) CT in pseudo-myxoma peritonei: a review of 17 cases. Clin Radiol 57 :608–613
39. Lersch C, Frimberger E, Ott R, Classen M (2001) Gray-scalesonographic findings in a patient with pseudomyxoma peri-tonei. J Clin Ultrasound 29 : 186–191
40. Pestieau SR, Wolk R, Sugarbaker PH (2000) Congenital pleu-roperitoneal communication in a patient with pseudomyxo-ma peritonei. J Surg Oncol 73 : 174–178
41. Gollub MJ, DeCorato D, Schwartz LH (2000) MR enteroclysis:evaluation of small-bowel obstruction in a patient with pseu-domyxoma peritonei. AJR Am J Roentgenol 174 : 688–690
42. Pantongrag-Brown L, Krebs TL, Daly BD, Wong-You-CheongJJ, Beiser C, Krause B, Brown AE (1998) Frequency of abdom-inal CT findings in AIDS patients with M. avium complexbacteraemia. Clin Radiol 53 : 816–819
43. Klatt EC, Jensen DF, Meyer PR (1987) Pathology of Mycobac-terium avium-intracellulare infection in acquired immuno-deficiency syndrome. Hum Pathol 18 : 709–714
44. Yang ZG, Min PQ, Sone S, He ZY, Liao ZY, Zhou XP, Yang GQ,Silverman PM (1999) Tuberculosis versus lymphomas in theabdominal lymph nodes: evaluation with contrast-enhancedCT. AJR Am J Roentgenol 172 : 619–623
45. Kim SY, Kim MJ, Chung JJ, Lee JT, Yoo HS (2000) Abdominaltuberculous lymphadenopathy: MR imaging findings. Ab-dom Imaging 25 : 627–32
46. Horton KM, Corl FM, Fishman EK (1999) CT of nonneoplas-tic diseases of the small bowel: spectrum of disease. J ComputAssist Tomogr 23 : 417–428
47. Nicolas AI, Ros PR (1995) Marbles in the belly: imaging-path-ologic correlation of solid mesenteric/omental masses. Post-grad Radiol 15 : 51–73
48. Jadvar H, Mindelzun RE, Olcott EW, Levitt DB.1997) Still thegreat mimicker: abdominal tuberculosis. AJR Am J Roentge-nol 168 : 1455–1460
49. Hulnick DH, Megibow AJ, Naidich DP, Hilton S, Cho KC, Bal-thazar EJ (1985) Abdominal tuberculosis: CT evaluation. Ra-diology 157 : 199–204
50. Demir K, Okten A, Kaymakoglu S, Dincer D, Besisik F, Cevik-bas U, Ozdil S, Bostas G, Mungan Z, Cakaloglu Y (2001) Tu-berculous peritonitis–reports of 26 cases, detailing diagnos-tic and therapeutic problems. Eur J Gastroenterol Hepatol 13 :581–585
51. Yilmaz T, Sever A, Gur S, Killi RM, Elmas N (2002) CT find-ings of abdominal tuberculosis in 12 patients. Comput MedImaging Graph 26 : 321–325
52. Ha HK, Jung JI, Lee MS, Choi BG, Lee MG, Kim YH, Kim PN,Auh YH (1996) CT differentiation of tuberculous peritonitisand peritoneal carcinomatosis. AJR Am J Roentgenol 167 :743–748
53. Jelinek JS, Kransdorf MJ, Shmookler BM, Aboulafia AJ, Mala-wer MM (1993) Liposarcoma of the extremities: MR and CTfindings in the histologic subtypes. Radiology 186 : 455–459

472 Hoon Ji, Pablo R. Ros
54. Kim T, Murakami T, Oi H, Tsuda K, Matsushita M, Tomoda K,Fukuda H, Nakamura H (1996) CT and MR imaging of ab-dominal liposarcoma. AJR Am J Roentgenol 166 : 829–833
55. Munk PL, Lee MJ, Poon PY, Goddard KJ, Knowling MA, Has-sell PR (1996) Computed tomography of retroperitoneal andmesenteric sarcomas: a pictorial essay. Can Assoc Radiol J 47 :335–341
56. Enzinger FM, Weiss SM (1995) Benign tumors of peripheralnerves. In: Enzinger FM, Weiss SW (eds) Soft tissue tumors.St Louis, Mosby
57. Pui MH, et al (1998) Computed tomography of abdominalneurogenic tumours. Australas Radiol 42(3) : 183–187
58. Kim SH, Choi BI, Han MC, et al (1992) Retroperitoneal neu-rilemnoma: CT and MR findings. Am J Roentgenol 159 :1023
59. Cerofolini E, Landi A, DeSantis G, et al (1991) MR of benignperipheral nerve sheath tumors. J Comput Assist Tomogr15 : 593
60. Loke TKL, Yuen NWF, Lo KKL, et al (1998) Retroperitonealancient schwannoma: Review of clinico-radiological features.Australas Radiol 42(2) : 136–138
61. Suh JS, Abenoza P, Galloway HR, et al (1992) Peripheral (ex-tracranial) nerve tumors: correlation of MR imaging and his-tologic findings. Radiology 183 : 341
62. Varma DG, Moulopoulos A, Sara AS, et al (1992) MR imagingof extracranial nerve sheath tumors. J Comput Assist Tomogr16 : 448
63. Friedman DP, Tartaglino LM, Flanders AE (1992) Intraduralschwannomas of the spine: MR findings with emphasis oncontrast-enhancement characteristics. Am J Roentgenol158 : 1347
64. Ros PR,Yuschok TJ, Buck JL, et al (1991) Peritoneal mesothe-lioma: radiologic appearances correlated with histology. ActaRadiol 32 : 355–358
65. O’Brien JE, Stout AP (1964) Malignant fibrous xanthomas.Cancer 17 : 1445–58
66. Enzinger FM,Weiss SW (1995) Malignant fibrohistiocytic tu-mors. In: Enzinger FM, Weiss SW (eds) Soft tissue tumors.St Louis, MO: Mosby Year Book, pp 351–380
67. Weiss SW, Enzinger FM (1978) Malignant fibrous histiocyto-ma: an analysis of 200 cases. Cancer 41 : 2250–2266
68. Goldman SM, Hartman DS, Weiss SW (1986) The varied ra-diographic manifestations of retroperitoneal malignant fi-brous histiocytoma revealed through 27 cases. J Urol 135 :33–38
69. Ros PR, Viamonte M Jr, Rywlin AM (1984) Malignant fibroushistiocytoma; mesenchymal tumor of ubiquitous origin. AJR142 : 753–759
70. Bruneton JN, Drouillard J, Rogopoulos A, Laurent F, Nor-mand F, Balu-Maestro C, et al (1988) Extraretroperitoneal ab-dominal malignant fibrous histiocytoma. Gastrointest Radiol13 : 299–305
71. Ko SF,Wan YL, Lee TY, Ng SH, Lin JW, Chen WJ (1998) CT fea-tures of calcifications in abdominal malignant fibrous histio-cytoma. Clin Imaging 22 : 408–13
72. Castillo M, Davis PC, Takei YD, Schwartzberg DG, HoffmanJC Jr (1990) Intracranial cystic malignant fibrous histiocyto-ma in a child: sonographic and CT findings. Pediatr Radiol20: 194–5
73. Berry AD III, Reintjes SL, Kepes JJ (1988) Intracranial malig-nant fibrous histiocytoma with abscess-like tumor necrosis.J Neurosurg 69 : 780–784
74. Panicek DM, Casper ES, Brennan MF, Hajdu SI, Heelan RT(1991) Hemorrhage simulating tumor growth in malignantfibrous histiocytoma at MR imaging. Radiology 181 : 398–400
75. Munk PL, Sallomi DF, Janzen DL, et al (1998) Malignant fi-brous histiocytoma of soft tissue imaging with emphasis onMRI. J Comput Assist Tomogr 22 : 819–826
76. Fenoglio-Preiser CM, Pascal RR, Perzin KH (1990) Mesenchy-mal tumors. In: Leiomyosarcomas; tumors of the intestines.2nd series. Washington, DC: Armed Forces Institute of Pa-thology, 433–441
77. Arakawa A,Yasunaga T,Yano S, et al (1993) Radiological find-ings of the retroperitoneal leiomyosarcoma: report of twocases. Comput Med Imaging Graph 17 : 125
78. Hartman DS, Hayes WS, Choyke PL, et al (1992) From the ar-chives of the AFIP: leiomyosarcoma of the retroperitoneumand inferior vena cava: radiologic-pathologic correlation. Ra-diographics 12 : 1203
79. Lane RH, Stephens DH, and Reiman HM (1989) Primary ret-roperitoneal neoplasms: CT findings in 90 cases with clinicaland pathologic correlation. Am J Roentgenol 152: 83
80. Maya MM, Fried K, Gendal ES (1993) AIDS-related lympho-ma: an unusual cause of omental caking. AJR Am J Roentge-nol 160 : 661
81. Pantongrag-Brown L, Buetow PC, Carr NJ, Lichtenstein JE,Buck JL (1995) Calcification and fibrosis in mesenteric carci-noid tumor: CT findings and pathologic correlation. AJR AmJ Roentgenol 164 : 387–391
82. Einstein DM, et al (1991) Abdominal lymphadenopathy:spectrum of CT findings. Radiographics 11: 457
83. Kim Y, Cho O, Song S, Lee H, Rhim H, Koh B (1998) Peritoneallymphomatosis: CT findings. Abdom Imaging 23 : 87–90
84. Bader TR, Semelka RC, Chiu VC, Armao DM, Woosley JT(2001) MRI of carcinoid tumors: spectrum of appearances inthe gastrointestinal tract and liver. J Magn Reson Imaging 14 :261–269
85. Emory TS, Carr NJ, Sobin LH (1997) Sclerosing mesenteritis,mesenteric panniculitis and mesenteric lipodystrophy: a sin-gle entity? Am J Surg Pathol 21 : 392–398
86. Katz ME, Heiken JP, Glazer HS, Lee JKT (1985) Intraabdomi-nal panniculitis: clinical, radiographic, and CT features. AJR145 : 293–296
87. Mata JM, Inaraja L, Martin J, et al (1987) CT features of mes-enteric panniculitis. J Comput Asst Tomogr 11 : 1021–1023
88. Lawler LP, McCarthy DM, Fishman EK, Hruban R (2002) Scle-rosing mesenteritis: depiction by multidetector CT andthree-dimensional volume rendering. AJR Am J Roentgenol178 : 97–99
89. Kronthal AJ, Kang YS, Fishman EK, Jones B, Kuhlman JE,Tempany CM (1991) MR imaging in sclerosing mesenteritis.AJR Am J Roentgenol 156 : 517–519
90. Kakitsubata Y, Umemura Y, Kakitsubata S, Tamura S, Wata-nabe K, Abe Y, Hatakeyama K (1993) CT and MRI manifesta-tions of intraabdominal panniculitis. Clin Imaging 17 :186–188
91. Fujiyoshi F, Ichinari N, Kajiya Y, Nishida H, Shimura T, Naka-jo M, Matsunaga Y, Furoi A, Imaguma M (1997) Retractilemesenteritis: small-bowel radiography, CT, and MR imaging.AJR Am J Roentgenol 169 : 791–793
92. Dalen BP, Bergh PM, Gunterberg BU (2003) Desmoid tumors:a clinical review of 30 patients with more than 20 years’ fol-low-up. Acta Orthop Scand 74 : 455–459
93. Middleton SB, Clark SK, Matravers P, Katz D, Reznek R, Phil-lips RK (2003) Stepwise progression of familial adenomatouspolyposis-associated desmoid precursor lesions demonstrat-ed by a novel CT scoring system. Dis Colon Rectum 46 :481–485
94. Al Jadaan SA, Al Rabeeah A (1999) Mesenteric fibromatosis:case report and literature review. J Pediatr Surg 34 : 1130–1132
95. Tolg C, Poon R, Fodde R, Turley EA, Alman BA (2003) Genet-ic deletion of receptor for hyaluronan-mediated motility(Rhamm) attenuates the formation of aggressive fibromato-sis (desmoid tumor). Oncogene 22 : 6873–6882
96. Maconi G, Cristaldi M, Vago L, Rovati M, Elli M, SampietroGM, Nebuloni E, Sainaghi M, Taschieri AM, Bianchi Porro G(1998) Clinical, ultrasonographic and tomographic featureson the natural evolution of primary mesenteric fibromatosis:a case report. Hepatogastroenterology 45 : 1663–1666
97. Kawashima A, Goldman SM, Fishman EK, Kuhlman JE, Onit-suka H, Fukuya T, Masuda K (1994) CT of intraabdominal de-smoid tumors: is the tumor different in patients withGardner’s disease? AJR Am J Roentgenol 162 : 339–342
98. Quinn SF, Erickson SJ, Dee PM, et al (1991) MR imaging in fi-bromatosis: results in 26 patients with pathologic correlation.AJR 156 : 539–542
99. Healy JC, Reznek RH, Clark SK, Phillips RK, Armstrong P(1997) MR appearances of desmoid tumors in familial ade-nomatous polyposis. AJR Am J Roentgenol 169 : 465–472

Chapter 4.11 Tumors of the Mesentery and Omentum 473
100. Castleman B, Iverson L, Mercedez VP (1956) Localized medi-astinal lymph node hyperplasia resembling thymoma. Can-cer 9 : 822–830
101. Keller AR, Hochholzer L, Castleman B (1976) Hyaline vascu-lar and plasma-cell types of giant lymph node hyperplasia ofthe mediastinum and other locations. Cancer 29 : 670–681
102. Kim TJ, Han JK, Kim YH, Kim TK, Choi BI (2001) Castlemandisease of the abdomen: imaging spectrum and clinicopath-ologic correlations. J Comput Assist Tomogr 25 : 207–214
103. Meador TL, McLarney JK (2000) CT features of Castlemandisease of the abdomen and pelvis.AJR Am J Roentgenol 175 :115–118
104. Singletary LA, Karcnik TJ, Abujudeh H (2000) Hyaline vascu-lar-type Castleman disease: a rare cause of a hypervascularretroperitoneal mass. Abdom Imaging 25 : 207–209
105. Irsutti M, Paul JL, Selves J, Railhac JJ (1999) Castleman dis-ease: CT and MR imaging features of a retroperitoneal loca-tion in association with paraneoplastic pemphigus. Eur Ra-diol 9 : 1219–1221
106. Johnson WK, Ros PR, Powers C, Stoupis C, Segel KH (1994)Castleman disease mimicking an aggressive retroperitonealneoplasm. Abdom Imaging 19 : 342–344
107. Livingston CD, Levine BA, Lecklitner ML, Sirinek KR (1983)Incidence and function of residual splenic tissue followingsplenectomy for trauma in adults. Arch Surg 118 : 617–620
108. Katz DS, Moshiri M, Smith G, Meiner EM, Fruauff AA (1998)Spontaneous hemorrhage of abdominal splenosis. J ComputAssist Tomogr 22 : 725–727
109. Carr NJ, Turk EP (1992) The histological features of spleno-sis. Histopathology 21 : 549–553
110. Delamarre J, Capron JP, Drouard F, Joly JP, Deschepper B, Car-ton S (1988) Splenosis: ultrasound and CT findings in a casecomplicated by an intraperitoneal implant traumatic hemat-oma. Gastrointest Radiol 13 : 275–278
111. Lin WC, Lee RC, Chiang JH, Wei CJ, Chu LS, Liu RS, Chang CY(2003) MR features of abdominal splenosis. AJR Am J Roent-genol 180 : 493–496
112. Castellani M, Cappellini MD, Cappelletti M, Fedriga E, Res-chini E, Cerino M, Gerundini P (2001) Tc-99m sulphur colloidscintigraphy in the assessment of residual splenic tissue aftersplenectomy. Clin Radiol 56 : 596–598