TUMORS OF THE LIVER AND BILIARY TRACT · cas Hepato-Pancreato-Biliary Association (AHPBA) and the...
27
DOI 10.2310/7800.2250 01/14 © 2014 Decker Intellectual Properties Inc gastrointestinal tract and abdomen TUMORS OF THE LIVER AND BILIARY TRACT Gabriela M. Vargas, MD, Purvi Parikh, MD, FACS, and Kimberly M. Brown, MD, FACS* Liver Tumors anatomic considerations A necessary prerequisite to the discussion of liver tumors and their treatment is a clear understanding of internal liver anatomy and a common point of reference for the terminol- ogy used in describing liver resections. In 2000, the Ameri- cas Hepato-Pancreato-Biliary Association (AHPBA) and the International Hepato-Pancreato-Biliary Association (IHPBA) presented the work of the AHPBA/IHPBA Terminology Committee at the annual meeting in Brisbane, Australia. The results of this work to standardize terminology for descrip- tions of hepatic anatomy and resections have been widely accepted as standard nomenclature. 1 The basis for the Brisbane terminology is that the internal vascular and biliary anatomy determines the anatomic divi- sions rather than surface markings [see Figure 1]. The hepatic artery and bile duct follow a similar pattern of branching, whereas the portal vein branching on the left side has a variation due to the fetal umbilical vein traveling from the umbilical cord to the left portal vein. The postnatal remnant of this structure (round ligament) carries blood away from the liver. The first-order division of the proper hepatic artery and the common hepatic duct into the right and left hepatic arteries and right and left hepatic ducts, respectively, results in division of the liver into two parts, referred to as the right and left hemilivers (or the right and left livers) [see Figure 1 and Table 1]. In this system of terminology, the term lobe is never used to denote a hemiliver, because it bears no rela- tion to the internal vascular anatomy. The plane between these two zones of vascular supply is called a watershed. The border watershed of the first-order division is a plane that intersects the gallbladder fossa and the fossa for the inferior vena cava and is called the midplane of the liver. The second-order division divides each of the hemilivers into two parts, referred to as sections. The right hemiliver comprises the right anterior section and the right posterior section. These sections are supplied by a right anterior sectional artery and a right posterior sectional artery and are drained by a right anterior sectional hepatic duct and a right posterior sectional hepatic duct. The left hemiliver compris- es the left medial section and the left lateral section. These sections are supplied by a left medial sectional hepatic artery and a left lateral sectional hepatic artery and are drained by a left medial sectional hepatic duct and a left lateral sectional hepatic duct. The third-order division divides the liver into nine seg- ments, each of which has its own segmental artery and bile duct [see Figure 1 and Table 1]. The caudate lobe, a unique portion of the liver that is separate from the right and left hemilivers, is also referred to as segment 1. The left lateral section comprises segments 2 and 3; the left medial section comprises segment 4 (which is sometimes further divided into segments 4a and 4b); the right anterior section com- prises segments 5 and 8; and the right posterior section comprises segments 6 and 7. Following this terminology, one describes a hepatic re- section or ablation by the anatomic portions of the liver involved [see Table 1]. Resection or ablation of a lesion that involves less than a segment would reference the segment in which the lesion is located. Resection of an anatomic segment would be described as a segmentectomy of the ap- propriate segment. Resection of segments 2 and 3, 4a and 4b, 5 and 8, or 6 and 7 would be termed a sectionectomy. Re- section of segments 2 to 4 is a “left hepatectomy” or “left hemihepatectomy,” whereas resection of segments 5 to 8 is a “right hepatectomy” or “right hemihepatectomy.” If the caudate lobe is resected with the hemihepatectomy, that should be noted. Resections involving more than the ana- tomic hemiliver are referred to as “extended right hemi- hepatectomy” or “extended left hemihepatectomy,” with specification of which additional segments were removed. The terms right trisectionectomy and left trisectionectomy are also appropriate. primary liver cancers Hepatocellular Carcinoma Hepatocellular carcinoma (HCC), also termed hepatoma, is the most common primary liver cancer worldwide. It is seen more frequently in men than in women. HCC develops in the background of chronic liver disease, which has pro- gressed from acute liver injury to fibrosis to cirrhosis and, ultimately, carcinoma. 2 In sub-Saharan Africa and Southeast Asia, where HCC is more prevalent than in the Western Hemisphere and Europe, hepatitis B virus (HBV) infection is responsible for most cases. In the United States, HCC age- adjusted incidence rates have doubled in the last decades. 3 The rise in incidence has been linked to a concomitant rise in hepatitis C virus infection. 4 Other important risk factors in the development of cirrhosis and subsequently HCC include alcoholism, aflatoxin B1 exposure, a 1 -antitrypsin deficiency, obesity, hemochromatosis, primary biliary cirrhosis, and nonalcoholic steatohepatitis (NASH). Clinical presentation HCC typically presents with non- specific symptoms such as abdominal pain, weight loss, anorexia, jaundice, and malaise. Physical examination find- ings may include hepatomegaly and ascites. In a patient with known liver disease, HCC often presents as an acute deterioration of previously stable liver function, including the appearance of ascites, encephalopathy, or jaundice. Screening high-risk individuals for HCC can reduce mortality from HCC. 5 Serum a-fetoprotein (AFP) testing and * The authors and editors gratefully acknowledge the contribu- tions of the previous authors, Steven M. Strasberg, MD, FACS, FRCSC, FRCS(Ed), and David C. Linehan, MD, FACS, to the development and writing of this chapter. Scientific American Surgery
Transcript of TUMORS OF THE LIVER AND BILIARY TRACT · cas Hepato-Pancreato-Biliary Association (AHPBA) and the...

DOI 10.2310/7800.2250
01/14
© 2014 Decker Intellectual Properties Inc
gastrointestinal tract and abdomen
T U M O R S O F T H E L I V E R A N D B I L I A R Y T R A C T
Gabriela M. Vargas, MD, Purvi Parikh, MD, FACS, and Kimberly M. Brown, MD, FACS*
Liver Tumors
anatomic considerations
A necessary prerequisite to the discussion of liver tumors and their treatment is a clear understanding of internal liver anatomy and a common point of reference for the terminol-ogy used in describing liver resections. In 2000, the Ameri-cas Hepato-Pancreato-Biliary Association (AHPBA) and the International Hepato-Pancreato-Biliary Association (IHPBA) presented the work of the AHPBA/IHPBA Ter minology Committee at the annual meeting in Brisbane, Australia. The results of this work to stand ardize terminology for descrip-tions of hepatic anatomy and resections have been widely accepted as standard nomenclature.1
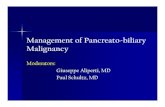
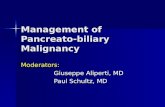
The basis for the Brisbane terminology is that the internal vascular and biliary anatomy determines the anatomic divi-sions rather than surface markings [see Figure 1]. The he patic artery and bile duct follow a similar pattern of branching, whereas the portal vein branching on the left side has a variation due to the fetal umbilical vein traveling from the umbilical cord to the left portal vein. The postnatal remnant of this structure (round ligament) carries blood away from the liver.
The fi rst-order division of the proper hepatic artery and the common hepatic duct into the right and left hepatic arteries and right and left hepatic ducts, respectively, results in division of the liver into two parts, referred to as the right and left hemilivers (or the right and left livers) [see Figure 1 and Table 1]. In this system of terminology, the term lobe is never used to denote a hemiliver, because it bears no rela-tion to the internal vascular anatomy. The plane between these two zones of vascular supply is called a watershed. The border watershed of the fi rst-order division is a plane that intersects the gallbladder fossa and the fossa for the inferior vena cava and is called the midplane of the liver.
The second-order division divides each of the hemilivers into two parts, referred to as sections. The right hemiliver comprises the right anterior section and the right posterior section. These sections are supplied by a right anterior sectional artery and a right posterior sectional artery and are drained by a right anterior sectional hepatic duct and a right posterior sectional hepatic duct. The left hemiliver compris-es the left medial section and the left lateral section. These sections are supplied by a left medial sectional hepatic artery and a left lateral sectional hepatic artery and are drained by a left medial sectional hepatic duct and a left lateral sectional hepatic duct.
The third-order division divides the liver into nine seg-ments, each of which has its own segmental artery and bile duct [see Figure 1 and Table 1]. The caudate lobe, a unique
portion of the liver that is separate from the right and left hemilivers, is also referred to as segment 1. The left lateral section comprises segments 2 and 3; the left medial section comprises segment 4 (which is sometimes further divided into segments 4a and 4b); the right anterior section com-prises segments 5 and 8; and the right posterior section comprises segments 6 and 7.
Following this terminology, one describes a hepatic re-section or ablation by the anatomic portions of the liver involved [see Table 1]. Resection or ablation of a lesion that involves less than a segment would reference the segment in which the lesion is located. Resection of an anatomic segment would be described as a segmentectomy of the ap-p ropriate segment. Resection of segments 2 and 3, 4a and 4b, 5 and 8, or 6 and 7 would be termed a sectionectomy. Re-section of segments 2 to 4 is a “left hepatectomy” or “left hemihepatectomy,” whereas resection of segments 5 to 8 is a “right hepatectomy” or “right hemihepatectomy.” If the caudate lobe is resected with the hemihepatectomy, that should be noted. Resections involving more than the ana-tomic hemiliver are referred to as “extended right hemi-hepatectomy” or “extended left hemihepatectomy,” with specifi cation of which additional segments were removed. The terms right trisectionectomy and left trisectionectomy are also appropriate.
primary liver cancers
Hepatocellular Carcinoma
Hepatocellular carcinoma (HCC), also termed hepatoma, is the most common primary liver cancer worldwide. It is seen more frequently in men than in women. HCC develops in the background of chronic liver disease, which has pro-gressed from acute liver injury to fi brosis to cirrhosis and, ultimately, carcinoma.2 In sub-Saharan Africa and Southeast Asia, where HCC is more prevalent than in the Western Hemisphere and Europe, hepatitis B virus (HBV) infection is responsible for most cases. In the United States, HCC age-adjusted incidence rates have doubled in the last decades.3 The rise in incidence has been linked to a concomitant rise in hepatitis C virus infection.4 Other important risk factors in the development of cirrhosis and subsequently HCC include alcoholism, afl atoxin B1 exposure, a1-antitrypsin defi ciency, obesity, hemochromatosis, primary biliary cirrhosis, and nonalcoholic steatohepatitis (NASH).
Clinical presentation HCC typically presents with non-specifi c symptoms such as abdominal pain, weight loss, anorexia, jaundice, and malaise. Physical examination fi nd-ings may include hepatomegaly and ascites. In a patient with known liver disease, HCC often presents as an acute deterioration of previously stable liver function, including the appearance of ascites, encephalopathy, or jaundice.
Screening high-risk individuals for HCC can reduce mortality from HCC.5 Serum a-fetoprotein (AFP) testing and
* The authors and editors gratefully acknowledge the contribu-tions of the previous authors, Steven M. Strasberg, MD, FACS, FRCSC, FRCS(Ed), and David C. Linehan, MD, FACS, to the development and writing of this chapter.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 2
20 mm may be diagnosed by imaging with a specifi city of greater than 99%.6 To properly diagnose HCC radiographi-cally and distinguish HCC from other tumors, such as chol-angiocarcinoma, a four-phase study (CT or MRI) is required: unenhanced, arterial, venous, and delayed phases. On US, most nodules will appear hypoechoic, but lesions may also appear as isoechoic, as hyperechoic, or of mixed echogenici-ty. Contrast-enhanced US has fallen out of favor as a diag-nostic tool.7 Currently, positron emission tomography (PET) has no role in the diagnosis of HCC.8 Patients with lesions exhibiting characteristic features for HCC, or with an elevat-ed AFP, do not require a biopsy. An algorithm for the management of suspicious liver nodules is summarized in Figure 3 [see Figure 3].
Staging Preoperative staging for HCC requires assess-ment of tumor extent and the degree of underlying liver dysfunction. A high-quality multiphase cross-sectional imaging study of the abdomen is performed to assess the size, location, and number of liver tumors, as well as any evidence of extrahepatic disease. CT of the chest is indicated to exclude lung metastases. Bone scans are reserved for
ultrasonography (US) are the two most widely employed screening strategies. Screening should be performed in a setting with standardized processes for follow-up of results and quality control procedures, particularly given the operator dependence of US. Current guidelines recommend US and AFP testing every 6 to 12 months for patients with cirrhosis of viral or nonviral etiology and HBV carriers with-out cirrhosis. In addition, patients with HBV or hepatitis C virus (HCV)-associated cirrhosis should be referred to a hepatologist for treatment of the viral hepatitis as treatment can improve HCC outcomes in these patients.
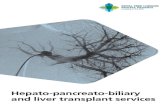
Diagnostic studies HCCs are hypervascular lesions whose blood supply is primarily from the hepatic artery; therefore, on multidetector computed tomographic (CT) imaging, the lesion typically appears hyperintense during the arterial phase and hypodense (referred to as “washout”) during the delayed phases [see Figure 2].6 Magnetic reso-nance imaging (MRI) is more sensitive than CT for the detection of HCC. On T2-weighted MRIs, the lesion usually appears hyperintense; whereas its appearance is variable on T1-weighted images. Up to 60 to 70% of HCCs of 10 to
Inferior Vena Cava
Right Hemiliver (Right Liver)
Right PosteriorSection
Right AnteriorSection
Left MedialSection
Left LateralSection
Left Hemiliver (Left Liver)
Right Hepatic Vein
7
8
2
1
3
4
5
6
FalciformLigament
Portal Vein
Common Bile Duct
Common Hepatic Artery
Left Hepatic Vein
Middle Hepatic Vein
Figure 1 Anatomic divisions of the liver according to the International Hepato-Pancreato-Biliary Association and the Americas Hepato-Pancreato-Biliary Association (IHPBA/AHPBA)-sanctioned terminology, including fi rst-order divisions (hemilivers), second-order divisions (sections), and third-order divisions (segments). Each segment has a numeric designation. Segments 2, 3 and 4 comprise the left hemiliver, segments 5–8 comprise the right hemiliver, and segment 1 is also referred to as the caudate lobe.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 3
Table 1 Brisbane 2000 Terminology for Hepatic Anatomy and Resections from the IHPBALevel of Division
Preferred Anatomic Term
Corresponding Couinaud Segments Preferred Term for Surgical Resection* Comments
First order (hemiliver)
Right hemiliverorRight liver
5–8 (± caudate lobe) Right hepatectomyorRight hemihepatectomy (stipulate ±
caudate lobe)
The border or watershed separating the two hemilivers is a plane that intersects the gallbladder fossa and the IVC fossa; this plane is referred to as the midplane of the liver
Left hemiliverorLeft liver
2–4 (± caudate lobe) Left hepatectomyorLeft hemihepatectomy (stipulate ±
caudate lobe)
Second order (section)
Right anterior section 5, 8 Right anterior sectionectomy The borders or watersheds separating the sections within the hemilivers are planes referred to as the right intersectional plane (for which there is no surface marking) and the left intersectional plane (which passes through the umbilical fissure and the attachment of the falciform ligament)
Right posterior section 6, 7 Right posterior sectionectomy
Left medial section 4 Left medial sectionectomy
Left lateral section 2, 3 Left lateral sectionectomy
— 4–8 (± caudate lobe) Right trisectionectomy (preferred)orExtended right hepatectomyorExtended right hemihepatectomy
(stipulate ± caudate lobe)
— 2, 3, 4, 5, 8 (± caudate lobe)
Left trisectionectomy (preferred)orExtended left hepatectomyorExtended left hemihepatectomy
(stipulate ± caudate lobe)
Third order (segment)
Segments 1–8 Any segment Segmentectomy (stipulate segment—e.g., segmentectomy 7)
The borders or watersheds of the segments are planes referred to as the intersegmental planesTwo contiguous
segmentsAny two segments in
continuityBisegmentectomy (stipulate
segment—e.g., bisegmentectomy 7, 8)
IHPBA = International Hepato-Pancreato-Biliary Association; IVC = inferior vena cava.*It is also permissible to refer to any resection in terms of its third-order components. Thus, a left hemihepatectomy may be referred to as a resection segments 2 to 4 (or 1 to 4).
a b
Figure 2 Computed tomographic imaging with intravenous contrast showing characteristic features for hepatocellular carcinoma: (a) hyperin-tense appearance on arterial imaging and (b) hypointense “washout” appearance in the venous phase.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 4
symptomatic patients. The Child-Pugh classifi cation and the Model for End-Stage Liver Disease (MELD) scores are commonly used to report the severity of liver disease in cirrhotic patients. Surgical resection is typically performed only in Child class A patients with no or minimal portal hypertension.
Staging systems for HCC include the American Joint Committee on Cancer (AJCC) Tumor-Node-Metastasis (TNM) staging system [see Table 2 and Table 3], the Barcelona Clinic Liver Staging System (BCLC), the Okuda system, and the Cancer of the Liver Italian Program (CLIP) system. The AJCC system is based on pathologic features of resected tumors and is therefore applicable only to a small subset of HCC patients. The BCLC is the staging system most commonly used in clinical practice to guide management. The BCLC has been used in several major clinical trials and therefore is able to provide meaningful comparisons between the outcomes reported in the study populations and individual patients. In addition, no other classifi cation system has successfully linked staging stratifi cation with treatment options and estimates of life expectancy.7
Management Patients with HCC are best managed with a multidisciplinary approach. Treatment options for patients
Figure 3 Algorithm summarizing the evaluation of a liver nodule in a patient with risk factors for hepatocellular carcinoma. Adapted with permission from Bruix J et al.6 CT = computed tomography; HCC = hepatocellular carcinoma; MDCT = multidetector computed tomography; MRI = magnetic resonance imaging; US = ultrasonography.
Table 2 American Joint Committee on Cancer TNM Clinical Classifi cation of Adult Primary
Liver CancerPrimary tumor (T) TX Primary tumor cannot be assessed
T0 No evidence of primary tumorT1 Solitary tumor without vascular
invasionT2 Solitary tumor with vascular invasion;
multiple tumors, none > 5 cm in greatest dimension
T3 Multiple tumors > 5 cm in greatest dimension or tumor involving major branch of portal or hepatic vein
T4 Tumor or tumors with direct invasion of adjacent organs (other than gallbladder or visceral peritoneum
Regional lymph nodes (N)
NX Regional lymph nodes cannot be assessed
N0 No regional lymph node metastasisN1 Regional lymph node metastasis
Distant metastasis (M)
MX Distant metastasis cannot be assessedM0 No distant metastasisM1 Distant metastasis
Repeat US at 3 months
Growing/changingcharacter
Investigateaccording to
size
Other contrast-enhanced study (CT
or MRI)
Arterial hypervascularityAND venous or delayed
phase washout
Arterial hypervascularityAND venous or delayed
phase washout
4-phase MDCT/dynamiccontrast-enhanced MRI
Yes
Yes
HCC
Stable
No
No
Biopsy
Liver nodule
> 1 cm< 1 cm
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 5
with early-stage disease, which is defi ned by the Milan cri-teria (one nodule < 5 cm, or two or three nodules all < 3 cm, no gross vascular invasion or extrahepatic spread) include resection, ablation, and transplantation. For patients without cirrhosis and limited disease, resection is the preferred treatment, although ablation may be an equally effective, less invasive option.9 In patients with Child class A cirrhosis without evidence of portal hypertension and adequate liver function, either liver resection or transplantation may be pursued. Due to HCCs’ growth along the portal veins, ana-tomic resections are associated with lower recurrence rates and are preferred over nonanatomic resections when possi-ble. Resection margins of at least 2 cm should be achieved when a nonanatomic resection is performed. The extent of resection is dependent on the location of the tumor and the disease burden. In most patients without cirrhosis, 60 to 75% of the liver may be excised without compromise to hepatic function. When the function of the hepatic remnant is in question, portal vein embolization of the side to be resected may be done preoperatively to induce hypertrophy of the future remnant. Inadequate size of the future remnant is a contraindication to resection.
When surgical resection is not possible and the tumor burden meets the Milan criteria, transplantation is the treatment of choice. The MELD scoring system currently gives exception points to patients with HCC to decrease the waiting time to transplantation. Radiofrequency ablation (RFA), transarterial chemoembolization (TACE) with cispla-tin or doxorubicin drug-eluting beads, and embolization with yttrium-90 radiolabeled beads are available treatment options for transplantation-bridging therapy, unresectable disease, or tumor burden in excess of the Milan criteria.10
Sorafenib, a tyrosine kinase inhibitor, is the fi rst-line treatment for patients with HCC who are not candidates for other treatment modalities.7 Additionally, phase I trials studying the feasibility of stereotactic body radiotherapy (SBRT) for primary HCC have demonstrated positive results for local control and improved survival.11,12 Currently, SBRT is used for Child-Pugh class A patients with one to three tumors with a cumulative diameter of less than 6 cm without evidence of extrahepatic disease.13 An algorithm summarizing the management of HCC is shown in Figure 4 [see Figure 4].
Prognosis The prognosis depends on the degree of tumor involvement and extent of liver function impairment. Patients with early disease and preserved liver function
have 5-year survival ranging from 50 to 75% with treatment. Patients with intermediate-stage disease have 3-year sur-vival of up to 50% without treatment. Advanced disease carries the worst prognosis, with only 50% of patients surviving 1 year.7
Intrahepatic Cholangiocarcinoma
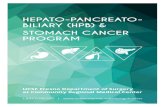
Intrahepatic cholangiocarcinoma (ICC) refers to the group of tumors originating in the epithelium of the peripheral biliary tree. Anatomically, these tumors are defi ned as aris-ing from the secondary bile ducts or more peripherally and do not involve the hepatic duct confl uence. Cholangio-carcinomas are divided into three macroscopic histologic subtypes that may also be seen in combination: mass form-ing, periductal infi ltrating, and intraductal growing [see Figure 5]. Worldwide, ICC represents approximately 10 to 20% of all primary liver malignancies.14 Men are more com-monly affected, and Asians are twice as likely as whites and blacks to be affected.15 Risk factors for the development of ICC have not been well established, although there appears to be an association between chronic infl ammation, such as chronic calculi, choledochal cysts, liver fl uke infections, and hepatitis B or C infection, and the development of ICC. In addition, alcohol abuse, diabetes, and obesity have also been implicated.13,16
Clinical presentation Early in their course, ICCs are often asymptomatic. Similar to HCCs, they are likely to present with nonspecifi c symptoms such as abdominal discomfort, fever, or weight loss. Jaundice as an initial presentation is rare.
Diagnostic studies Unlike HCC, there are no character-istic radiographic fi ndings associated with ICC. ICC may appear as an irregular or well-defi ned soft tissue mass along the intrahepatic ducts. US, contrast-enhanced CT, and MRI are useful to establish the presence of a mass and to deter-mine resectability by establishing the relationship of the mass to the nearby vessels and biliary tree. CT and MRI are comparable in diagnostic accuracy.17 Enhancement on delayed-phase imaging is suggestive of cholangiocarcinoma. PET has not been shown to be useful in diagnosing ICC but may be benefi cial in the detection of regional and distant metastases or identifying an occult primary tumor.18,19 The initial workup of a patient suspected of ICC should include laboratory studies: liver function tests, AFP (expected to be normal), carcinoembryonic antigen (CEA), cancer antigen (CA) 125, and CA 19-9. Since these tumor markers are not specifi c serum markers for cholangiocarcinoma, extrahe patic malignancies must be excluded by cross-sectional imaging of the chest, abdomen, and pelvis; endoscopy; and mam-mography before a defi nite diagnosis of ICC can be established.
Staging ICC is staged using the AJCC TNM cancer stag-ing system. The seventh edition of the staging manual was updated to provide a staging system for ICC independent of HCC and extrahepatic cholangiocarcinoma [see Table 4].20 The tumor category is based on three major prognostic factors: tumor number, vascular invasion, and direct extra-hepatic tumoral extension. The node category is based on
Table 3 American Joint Committee on Cancer Staging System for Adult Primary Liver CancerStage T N M
I T1 N0 M0
II T2 N0 M0
IIIA T3 N0 M0
IIIB T4 N0 M0
IIIC Any T N1 M0
IV Any T Any N M1
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 6
the presence or absence of regional lymph node metastases. The metastasis category is based on the presence or absence of distant disease.13,21
Management The management of ICC is best app-roached with a multidisciplinary team. Prior to surgical intervention, distant metastatic disease must be ruled out and the adequacy of the future liver remnant must be estab-lished. Metastatic disease to the celiac or retroperitoneal lymph nodes is considered a contraindication to resection. Partial hepatectomy with negative margins is the only potentially curative option and is associated with improved survival compared with patients who do not undergo resec-tion or who have residual disease. The extent of liver resec-tion is determined by tumor size and location, with 80% of patients requiring hemi- or extended hemihepatectomies for complete tumor removal. Some groups, due to the poor prognosis conferred by lymph node involvement, recom-mend a lymphadenectomy. Left-sided tumors tend to spread toward the gastrohepatic ligament and along the lesser curve of the stomach, whereas right-sided tumors drain to the hepatoduodenal ligament. However, left-sided tumors may also follow a “right-sided” drainage pattern in 50% of
cases. Despite the known prognostic infl uence of lymph node involvement, routine lymphadenectomy is not associ-ated with improved survival, which may explain why it has not been universally adopted.
The role of adjuvant therapy in ICC is unclear. 5-Fluorouracil (5-FU) has largely been replaced by gemcitabine-containing regimens, based on data from pancreatic cancer and unresectable biliary tract cancers. However, a retro-spective review of patients undergoing chemotherapy in an adjuvant or neoadjuvant setting failed to show a difference in survival with either approach.
Orthotopic liver transplantation (OLT) for ICC is limited by unacceptably high recurrence rates.17 However, some institutions have reported acceptable survival rates with protocols using pretransplantation chemoradiation.22 Stud-ies comparing OLT and resection report similar survival,23 but given the shortage of donor organs, ICC is considered a contraindication for OLT.
Prognosis Long-term survival is poor. A population-based analysis of patients with ICC undergoing curative intent surgery between 1973 and 2010 found a median overall survival of 27.3 months. One-, 3-, and 5-year overall
Figure 4 Algorithm for the management of hepatocellular carcinoma.82 HCC = hepatocellular carcinoma; RFA = radiofre-quency ablation; TACE = transarterial chemoembolization; UNOS = United Network for Organ Sharing.
HCC identified
Resectioncandidate
Liver transplantcandidate
Not livertransplantcandidate
1 lesion ≤ 5 cm3 lesions ≤ 3 cmNo metastases
No vascularinvasion
SorafenibYes
No cirrhosisChild class A
No metastasesLiving donor
liver transplantdonor
UNOS list
Orthotopic livertransplant
Neoadjuvanttherapy
RFA TACE/Yttrium90 Palliative care
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 7
survival was 77.5%, 44.3%, and 30.7%, respectively.24 Factors associated with worse outcomes include increasing number of lesions, N1 disease, large tumor size, and vascular invasion.25
secondary cancers
Colorectal Metastases
In 2012, it was estimated that 143,000 Americans would be diagnosed with colorectal cancer. Over 50% of those patients will go on to develop metastatic disease, with the
liver being the isolated site of metastases in half of these patients.26,27
Clinical presentation Most patients with colorectal liver metastases (CRLMs) are asymptomatic. Synchronous tumors are identifi ed through preoperative staging or intra-operative examination of the liver. Fluorodeoxyglucose-PET imaging is indicated in patients with potentially resectable metastatic disease seen on a contrast-enhanced CT scan. Metachronous tumors are identifi ed through posttreatment surveillance, either by cross-sectional imaging or routine
a
b
c
d
Mass Forming andPeriductal Infiltrating
Tumor
Tumor
Tumor
Tumor
Mass Forming
Intraductal Growth
Periductal Infiltrating
Figure 5 Macroscopic subtypes of intrahepatic cholangiocarcinoma.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 8
CEA levels. Symptomatic advanced disease may present with abdominal pain, distention, weight loss, or hepatic insuffi ciency.
Diagnostic studies CLRMs can be identifi ed by US, CT, PET/CT, or MRI. US has been largely replaced by cross-sectional imaging studies as the latter are more sensitive for the detection of CRLMs and not user dependent. On CT, CLRMs are visualized more prominently in the portal venous phase as hypodense lesions. For small, subcenti-meter indeterminate lesions, MRI may be helpful in further characterization. PET/CT is not recommended for routine surveillance in patients who have undergone resection of a colorectal cancer. Patients with T3 or T4 tumors and/or node-positive disease are followed with yearly CT scans of the chest/abdomen/pelvis for 5 years. PET/CT is obtained when there is a high clinical suspicion for metastatic disease but equivocal cross-sectional imaging or to evaluate for extrahepatic disease in a patient with potentially resectable liver metastases.
Management Surgical resection offers the only potential for cure in patients with isolated CRLM. The principles of determining resectability include the following: (1) complete anatomic resection must be possible while maintaining adequate hepatic function, (2) the primary tumor must be amenable to R0 resection, and (3) there should be no unre-sectable extrahepatic disease. The considerations regarding the extent of resection and the use of portal vein emboliza-tion are similar to those for HCC. In contrast to HCC, non-anatomic resections are as effective as anatomic resections as long as negative margins are obtained. One-centimeter margins should be the goal when feasible. In appropriately
selected patients and experienced teams, synchronous re-section of the primary tumor and liver metastases can be performed.
The introduction of oxaliplatin, irinotecan, and mono-clonal antibodies such as bevacizumab has allowed down-sizing and subsequent resection of hepatic metastases previously considered unresectable. After treatment with chemotherapy, patients should be restaged and resectability reassessed. If complete radiologic response is seen on CT or PET scans, surgical resection should still be undertaken as a complete pathologic response is infrequent. The response to chemotherapy is considered a marker for the biologic behavior of the tumor, and resection of disease that progresses on modern chemotherapy should be undertaken with caution.
In patients with extensive bilobar disease who are appro-priate surgical candidates, a two-stage approach can be an effective strategy to achieve complete resection. The use of thermal ablation with radiofrequency or microwave energy as an adjunct to resection has also expanded the number of patients eligible for curative intent surgery. Ablation should be reserved for small (≤ 3 cm and ideally ≤ 1 cm) lesions that are not near major vessels or bile ducts. Patients who have unresectable disease or who are poor surgical candidates may be treated with ablation or chemoembolization, with or without systemic therapy. Ablation in this setting may be performed by open, laparoscopic, or percutaneous methods. Reevaluation for resection should be performed after 2 months of systemic chemotherapy and every 2 months thereafter.28–31 Recurrences following hepatectomy may be managed by repeat liver resection, local ablative or chemo-embolization techniques, systemic chemotherapy, or a multimodality approach.32
Prognosis Patients with untreated CRLMs have a me-dian survival of less than 1 year.32 In contrast, patients with treated CRLMs can experience 5-year overall survival of up to 50 to 60%.33–36 Recurrence after resection remains a common problem, with more than 70% of patients develop-ing a second hepatic recurrence.37 Five-year overall survival following a second hepatectomy ranges from 31 to 73%.32
Neuroendocrine Metastases
Neoplasms originating from neural or endocrine struc-tures form the family of tumors known as neuroendocrine tumors (NETs). NETs may arise from nerve plexuses, extra-adrenal paraganglia, thyroid, parathyroid, adrenal glands, and specialized elements of the endocrine system (islet cell tumors, carcinoids, large cell and small cell carcinomas).38 The presence of liver metastases is dependent on the pri-mary tumor site, T stage, tumor differentiation, and tumor grade. NETs of the intestine and pancreas are frequently metastatic at the time of diagnosis.39
Clinical presentation The clinical presentation of meta-static NET is dependent on the functionality of the primary tumor. Functional tumors secrete hormones and/or monoamines from the tumor cells. Carcinoid tumors secrete serotonin, which produces a constellation of symptoms known as carcinoid syndrome. Patients with carcinoid syndrome may present with fl ushing, diarrhea, wheezing,
Table 4 AJCC Seventh Edition TNM Staging System for Intrahepatic Cholangiocarcinoma
T: Primary tumors (T) TX Primary tumor cannot be assessed T1 Solitary tumor, no vascular invasion T2 T2a Solitary tumor, vascular invasion T2b Multiple tumors, possible vascular invasion T3 Tumor perforates the serosa (visceral peritoneum) or
directly invades local extrahepatic structures T4 Tumor plus periductal invasion
N: Regional lymph nodes (N) NX Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Regional lymph node metastasis
M: Distant metastasis (M) MX Distant metastasis cannot be assessed M0 No distant metastasis M1 Distant metastasis
Staging Stage 0 Tis N0 M0 Stage I T1 N0 M0 Stage II T2 N0 M0 Stage III T3 N0 M0 Stage IVA T4 N0 M0, Any T N1 M0 Stage IVB Any T Any N M1
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 9
abdominal cramping, and heart palpitations. Gastrinomas may present with peptic ulcers secondary to excessive gas-trin secretion (Zollinger-Ellison syndrome). Insulinomas typically present with hypoglycemia. Glucagonomas may present with rash, hyperglycemia, and diarrhea. VIPomas produce excess vasoactive intestinal peptide (VIP), which presents with severe watery diarrhea, hypokalemia, and achlorhydria. Patients with nonfunctional tumors typically present with nonspecifi c symptoms, and often the diagnosis of stage IV disease is an incidental fi nding.
Diagnostic studies Patients presenting with metastatic NETs require pathologic examination of the metastases, assessment of disease burden by multiphasic CT or MRI, biochemical analysis to assess for functionality, and serum tumor markers to rule out hereditary syndromes when sus-pected. The minimal biochemical workup should include circulating chromogranin A and specifi c tumor markers in suspected clinical syndromes [see Table 5].39 Somatostatin receptor imaging and harmonic imaging (abdominal US with contrast agents) coupled with Doppler imaging are helpful diagnostic studies if available.
Management The treatment approach to the patient with neuroendocrine metastases is illustrated in Figure 6 [see Figure 6]. Surgical resection with curative intent remains the gold standard in the treatment of liver metastases. The following minimal requirements must be met for curative intent surgery: (1) resectable liver disease, (2) absence of right heart insuffi ciency in patients at risk for development of carcinoid heart disease, (3) absence of unresectable lymph node or extra-abdominal metastases, and (4) absence of diffuse or unresectable peritoneal carcinomatosis.39 The ben-efi t of debulking resections requires further analysis and is currently not recommended. Liver transplantation is a
Table 5 Neuroendocrine Tumors and Their Corresponding Biochemical Markers83
Tumor Markers
Carcinoid 5-HIAA (24 hr urine) and chromogranin A
PanNET Chromogranin A
Gastrinoma Gastrin
Insulinoma Proinsulin, insulin/glucose ratio, and C-peptide
VIPoma VIP
Glucagonoma Glucagon, blood glucose, and CBC
Pheochromocytoma/paraganglioma
Metanephrines (plasma and urine), catecholamines (urine), and dopamine (urine)
Pituitary Growth hormone/IGF-1, prolactin, LH/FSH, TSH, alpha subunits, and ACTH
Ectopic hormones ACTH, GRH, and GHRH
Other pancreas Somatostatin, pancreatic polypeptide, calcitonin, PTH-related peptide
ACTH = adrenocorticotropic hormone; CBC = complete blood count; FSH = follicle-stimulating hormone; GHRH = growth hormone–releasing hormone; GRH = gonadotropin-releasing hormone; 5-HIAA = 5-hydroxyindoleacetic acid; IGF-1 = insulinlike growth factor–1; LH = luteinizing hormone; panNET = pancreatic neuroendocrine tumor; PTH = parathyroid hormone; TSH = thyroid-stimulating hormone; VIP = vasoactive intestinal peptide.
Figure 6 Treatment approach to neuroendocrine neoplasm liver metastases.39 TACE = transarterial chemoembolization; TAE = transcatheter arterial embolization.
treatment option in highly selected patients presenting with life-threatening hormonal disturbances related to a function-al NET or in patients with diffuse unresectable liver metas-tases refractory to standard medical or surgical therapies.
Bilobardisease
Confirmation of neuroendocrine neoplasm.Resection of primary tumor
and no evidence ofextrahepatic disease
Diffusedisease
Livertransplan-
tation
Selectcases
Molecular targetedtherapy
Chemo-therapy
Somatos-tatin
analogues
TACE orTAE
Two-stepoperation
One-stepoperation
Nonsurgicalcandidate
Surgicalcandidate
Resection
Unilobardisease
Surgicalcandidate
Nonsurgicalcandidate
Ablation orTACE
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 10
Locoregional techniques, including thermal ablation with radiofrequency or microwave energy, or selective hepatic transcatheter arterial embolization (TAE) or chemoemboli-zation (TACE), may be used in conjunction with surgical resection or medical therapy. The response to locoregional therapies is largely dependent on tumor size. RFA is not recommended for lesions greater than 5 cm in size. Laser-induced thermotherapy is more precise than RFA and is suitable for larger tumors (up to 7 cm). TAE and TACE are typically reserved for patients whose tumors are not amena-ble to surgical therapy. Contraindications to TAE and TACE include portal vein thrombosis, poor liver function, the pres-ence of a hepatopulmonary shunt, or severe comorbidities. In addition, TAE and TACE should be used with caution in potential liver transplantation candidates as arterial throm-bosis is likely to complicate arterial reconstruction during transplantation.
Control of hormonal hypersecretion symptoms and pro-phylaxis against carcinoid crisis should be performed prior to surgical resection or locoregional therapies. The gold standard for long-term medical therapy is treatment with somatostatin analogues. These compounds have a low side-effect profi le and are very effective at controlling symptoms and retarding tumor growth.38 Everolimus is an inhibitor of mammalian target of rapamycin (mTOR) and may be effec-tive when given in conjuction with somatostatin analogues to prolong survival in advanced carcinoid tumors or as single-agent treatment in pancreatic NETs.40 Everolimus and sunitinib, a tyrosine kinase inhibitor, are associated with prolonged disease-free survival in metastatic pancreatic NET.41
Controversies Patient selection and timing of liver trans-plantation are subjects of controversy. Most of the available published data on liver transplantation for NET are single-institution retrospective studies with small sample sizes. The benefi t of liver transplantation in this setting has not been well established.42 Radiolabeled somatostatin ana-logues have also been used to treat advanced carcinoid tumors, with encouraging results in nonrandomized studies.43
Prognosis The prognosis for metastatic NET is better than that for metastatic adenocarcinoma. Histologic differ-entiation and tumor grade are the strongest predictors of survival. Five-year survival of 60 to 80% has been achieved with complete surgical resection. In contrast, the 5-year survival rate in unresectable disease is approximately 30%.39
noncolorectal, nonneuroendocrine metastases
Liver metastases from other primary sites in the absence of extrahepatic disease can be managed according to the same approach employed for CRLMs, although the outcome is less satisfactory. Tumors that have been treated in this way with acceptable results include breast cancers, renal cell cancers, gastric cancers, acinar cell cancers of the pancreas, and ovarian cancers.
benign or premalignant hepatic lesions
With the extensive use of US and cross-sectional imaging, benign asymptomatic or questionably symptomatic liver
lesions are increasingly identifi ed. Solid lesions may arise from epithelial elements, such as hepatic adenoma or focal nodular hyperplasia (FNH), or mesenchymal elements, of which hemangioma is the most common. Cystic lesions identifi ed within the liver include benign simple hepatic cysts, bile duct cysts, and biliary cystadenoma or cystadeno-carcinoma. The precise identifi cation of these lesions is often possible with high-quality imaging, and biopsy is rarely indicated. Treatment options depend on the potential for complications, including malignant transformation or hemorrhage, and the presence of symptoms.
Hemangioma
Hepatic hemangioma is the most common liver tumor, with an incidence of 3 to 20%, equal distribution between left and right hepatic lobes, and an approximately 5:1 male-to-female ratio.44 The term giant hemangioma describes lesions greater than 4 or 10 cm, depending on the source. Giant hemangiomas may have a more aggressive pattern of growth than smaller lesions, which tend to remain stable over time.
These tumors are congenital vascular malformations, with cavernous vascular spaces, a fl at endothelial lining, and fi brous septations. They are usually asymptomatic, inciden-tal fi ndings, but pain and local compressive symptoms may result from the size and particular location of a tumor. Other rare presentations include hemorrhage, infl ammatory changes, and coagulopathy. In the absence of these rare acute complications, liver function and coagulation labora-tory profi les are normal.
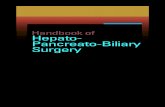
Imaging offers a reliable diagnosis in many cases. US reveals a hyperechoic, well-demarcated mass, with an absence of vascularity on color Doppler imaging. CT criteria diagnostic for hemangioma include a hypodense lesion in the precontrast phase; nodular, peripheral enhancement followed by central enhancement in the arterial phase; and persistent contrast enhancement on delayed series. On MRI, hemangioma classically appears as a hypointense lesion on T1-weighted imaging and a hyperintense lesion on T2-weighted sequences, and following contrast administra-tion, the enhancement pattern is similar to that on CT: early peripheral irregular enhancement pattern followed by progressive central fi lling and homogeneous enhancement on delayed imaging [see Figure 7]. Atypical enhancement patterns, including rapid and slow fi lling, are not uncom-mon and present a dilemma in a patient known to have or suspected of having a malignancy.
Treatment of asymptomatic hemangioma, irrespective of size, is observation, with no need for surveillance imaging. Indications for operation include severe pain, compressive symptoms, hemorrhage, or uncertain diagnosis with a sus-picion of malignancy. Surgical resection by means of a formal anatomic resection or an enucleation is the treatment of choice. Traditional open and laparoscopic approaches can be employed, based on the lesion anatomy and surgical team experience.45 Arterial embolization, hepatic arterial ligation, and radiation have been described but are ineffec-tive. Liver transplantation has been described for patients with complications from unresectable giant hemangiomas.46
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 11
Focal Nodular Hyperplasia
FNH is most commonly diagnosed in female patients in the third to fi fth decades of life. It is a completely benign process and the second most common benign liver tumor after hemangioma. Unlike hepatocellular adenoma, there is no relationship between oral contraceptive use and the growth of FNH and thus no reason to avoid the use of oral contraceptives in a patient with FHN. The histology of FNH is that of benign hepatocellular hyperplasia, forming
nodules with fi brous septations. This architecture is thought to arise from a vascular malformation inducing a reactive hyperplasia. The fi brous septations appear grossly as a cen-tral scar, identifi able on both pathologic and radiologic examination. FNH is usually a solitary lesion, but 20 to 30% of patients will have more than one.
FNH typically appears as a hypoechoic lesion on US or may be isoechoic with a hyperechoic central scar. Large ectatic peripheral feeding vessels may be identifi ed using
a b
c d
Figure 7 Magnetic resonance images of a giant hemangioma showing typical appearance (a) on a T1-weighted image, (b) on a T2-weighted im-age, (c) in the early postcontrast phase, and (d) on delayed imaging.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 12
color Doppler imaging. Contrast-enhanced CT [see Figure 8] reveals a hypodense lesion in the precontrast phase, rapid arterial enhancement, often with a less dense central scar, and an isodense or hyperdense lesion in the portal venous phase. FNH is a well-demarcated lesion, and feeding vessels may be seen on CT as well. FNH appears hypointense or isointense, with a hypointense central scar on unenhanced T1-weighted MRIs, and on T2-weighted images, these lesions are isointense or slightly hyperintense, with a strongly hyperintense-appearing central scar. In postcontrast images, there is arterial enhancement followed by an isointense appearance in the portal venous phase. Longer delay will show hyperintensity in the central scar. In lesions without a central scar, the diagnosis may be diffi cult. In cases of diag-nostic uncertainty, a core-needle biopsy, either percutane-ous or operative, will demonstrate histologic fi ndings con-sistent with FNH—hepatocytes in a trabecular pattern with fi brous septations.
FNH should be managed nonoperatively. There is no malignant potential and no risk of rupture, bleeding, or other complications. In cases of diagnostic uncertainty or a clear demonstration of symptoms, open or laparoscopic resection of the lesion with a surrounding margin of normal hepatic parenchyma allows for controlled division of any feeding vessels.
Adenoma
Hepatocellular adenoma is a rare tumor, associated with oral contraceptive and androgen steroid use. The incidence is estimated at 0.1 per 100,000 in non–oral contraceptive users and three to four per 100,000 in long-term oral contra-ceptive users. The estrogen content and duration of expo-sure infl uence the risk of hepatocellular adenoma. These lesions may present with pain, abdominal fullness, abnor-mal liver function tests, or complications such as bleeding. The risk of symptoms increases with increasing size, par-ticularly greater than 5 cm, with as high as a 20 to 40% risk of spontaneous bleeding. Malignant transformation occurs in approximately 10% of cases.47
Most patients have a solitary lesion, but multiple lesions may be seen in up to 30% of patients. Adenomatosis is a condition where 10 or more adenomas are present through-out the hepatic parenchyma. Histologically, adenomas consist of benign hepatocytes with an absence of normal liver architecture. Cellular atypia may make distinction from HCC diffi cult.
On US, hepatocellular adenoma is a well-demarcated, hyperechoic mass with internal heterogeneity. Unenhanced CT images demonstrate a hypodense mass, which enhances heterogeneously in the arterial phase and washes out to an isodense or hypodense appearance in the portal venous phase. In addition to the absence of central scar, features distinguishing adenoma from FNH may include a smooth surface, tumor capsule, and internal hemorrhage in the adenoma.48 Unenhanced MRI reveals a hyperintense or iso-intense lesion on T1-weighted images and a mildly hyperin-tense lesion on T2-weighted images. Adenomas are usually hyperintense, with a heterogeneous pattern in the arterial phase.
Small adenomas (≤ 3 cm) may be observed, and oral con-traceptive use stopped, with some reports of regression and resolution.49 Molecular profi ling may further guide decision making based on the prognosis.50 Complete surgical resec-tion with negative margins is the standard of care for hepa-tocellular adenomas greater than 4 cm in diameter. There is no need for extended margins, and open or laparoscopic approaches are acceptable depending on the tumor location and surgical team expertise.
In cases of ruptured adenoma, initial hemorrhage control is often possible with selective hepatic arterial embolization, avoiding an emergent operation with attendant mortality of 8%. After recovery from hemorrhage and resolution of peritumoral hematoma, the tumor can be more precisely localized by imaging, and a less extensive, elective resection can be performed.
Patients with multiple adenomas have risks for bleeding and malignancy similar to those of patients with solitary adenomas of similar size. If anatomically feasible, patients should undergo resection of all lesions greater than 4 cm, either in a single or staged operation. When tumor volume or location precludes resection, patients should be closely followed with examination, serial AFP levels, and surveil-lance imaging to detect malignant transformation. Resection of a single malignant lesion is appropriate. Resection and liver transplantation have been described for patients with multiple malignancies arising in adenomatosis, but the
a
b
Figure 8 Focal nodular hyperplasia as imaged by computed tomog-raphy in the (a) arterial phase and (b) venous phase. The arrow points to a feeding vessel.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 13
prognosis is extremely poor. Liver transplantation for hepa-tocellular adenomatosis in the absence of malignancy is an extremely uncommon indication for liver transplantation.51
Cystic Disease of the Liver and Biliary Tree
Cystic lesions may be found within the liver or involving the extrahepatic biliary tree. Nonparasitic cysts within the liver are a common fi nding on cross-sectional or ultrasound imaging or may be discovered incidentally at laparotomy or laparoscopy. Although the majority of cysts are benign and asymptomatic, a thoughtful, organized approach will ensure intervention only in those cases in which patients are likely to benefi t. Liver abscess (infectious cyst) and hydatid cyst are not discussed here.
bile duct cysts
Bile duct cysts are most frequently identifi ed and treated in the young child; however, 20% of patients will present with symptomatic or asymptomatic bile duct cysts as adults. Cystic malformation can occur anywhere along the intrahe-patic and extrahepatic biliary tree, which makes the term choledochal cyst a misnomer. The precise etiology is unknown, but the most commonly accepted hypothesis is that an anomalous pancreaticobiliary duct junction promotes refl ux of pancreatic juice into the common bile duct. The resulting infl ammation causes ectasia and, eventually, dilation.
Bile duct cysts are classifi ed based on anatomic location, extent of involvement, and gross morphology [see Figure 9]. The majority of bile duct cysts are type I. In adults, bile duct cysts may present as incidental fi ndings on cross-sectional imaging or with symptoms including pain, jaundice, nausea/vomiting, cholangitis, or pancreatitis. Patients may have undergone cholecystectomy, due to the overlap of symptoms, or may have evidence of biliary cirrhosis from chronic obstruction at presentation.
Bile duct cysts may be fi rst identifi ed on US or CT for sym ptoms mimicking cholecystitis. However, for precise anatomic information to guide treatment planning, cholan-giography via percutaneous transhepatic cholangiography (PTC), endoscopic retrograde cholangiopancreatography (ERCP), and magnetic resonance cholangiopancreatogra-phy (MRCP) are the studies of choice. Initial treatment should address acute issues such as biliary obstruction or cholangitis.
The ultimate goal of treatment for extrahepatic bile duct cysts is complete excision of the abnormal duct, usually
with a biliary-enteric anastomosis. In patients with type IV disease, the extent of intrahepatic involvement and degree of cirrhosis and/or portal hypertension all infl uence treat-ment planning. Complete extrahepatic cyst excision with biliary-enteric anastomosis can be combined with hepatic lobectomy for unilateral intrahepatic disease. With bilobar involvement, there is a risk of recurrent obstruction, hepato-lithiasis, and stricture of the biliary-enteric anastomosis; some authors recommend fi xing the Roux limb to the anterior abdominal wall to facilitate future percutaneous interventions.
In type V disease, limited involvement may allow for resection as an initial and perhaps defi nitive treatment. Liver transplantation is indicated in patients with un-successful treatment by resection and with diffuse type V disease that has progressed to cirrhosis and/or portal hypertension.
Nonparasitic Cystic Tumors of the Liver and Biliary Tree
simple hepatic cyst
Simple hepatic cysts are the most common of the cystic lesions in the liver, occurring in up to 18% of the popula-tion.52 These congenital cysts do not communicate with the biliary tree, and the exact etiology is not known. Simple cysts are lined by epithelium that secretes water and electro-lytes in concentrations similar to serum. Patients may have a single cyst or multiple cysts and are usually asymptomatic at presentation. If present, symptoms may include pain, full-ness, early satiety, or jaundice. Hemorrhage into a cyst can precipitate symptoms and can alter the radiologic appear-ance of the cyst to that resembling a biliary cystadenoma.
US demonstrates a smooth, contoured anechoic lesion with a well-defi ned interface between tissue and fl uid. In the absence of hemorrhage, the lesion is homogeneous. Internal septations or echoic debris in the cyst suggests hemorrhage. On CT images, simple cysts appear as homogeneous round or oval lesions with density similar to water.
The differential diagnosis of an intrahepatic cystic lesion includes an abscess, hydatid cysts, hematoma, hemangioma, and necrotic tumor. Needle aspiration and serologic testing can be helpful in cases of diagnostic uncertainty. An asymp-tomatic simple hepatic cyst requires no treatment. Symp-toms are unlikely unless the cyst is large (> 8 to 10 cm) and stretching the liver capsule. A diagnostic aspiration can help identify whether symptoms resolve with decompression of
Figure 9 Todani classifi cation of bile duct cysts.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 14
the cyst and thus defi nitive treatment would be expected to confer benefi t to the patient. Simple aspiration of fl uid has a 100% rate of cyst recurrence.
Aspiration combined with injection of a sclerosing agent such as ethanol or minocycline has been used to try to reduce the recurrence rate. Patients experience pain and side effects from diffusion of alcohol, and recurrence is still com-mon. The infl ammation induced by sclerotherapy changes the composition of the cyst fl uid, making it viscous and opaque.
In a patient with a large, exophytic, symptomatic simple hepatic cyst, cyst fenestration involves excising the free wall of a cyst that protrudes from the surface of the liver, establishing a wide area of connection between the cyst and the peritoneal cavity. The cyst fl uid freely moves into the peritoneum, where it is absorbed. This can be done via a laparoscopic or an open approach. The cyst wall should be sampled and sent to Pathology to exclude cystadenoma at the time of fenestration. Follow-up in the absence of symptoms is not indicated.
biliary cystadenoma and cystadenocarcinoma
Biliary cystadenoma is a rare cystic tumor within the liver, with the potential to degenerate into a malignant cystadeno-carcinoma. Cystadenoma is usually a multiloculated, mucin-containing lesion of unknown etiology. Patients may present with pain, fullness, nausea, early satiety, or jaundice or may be asymptomatic. There are usually no laboratory abnor-malities in the absence of jaundice.
Imaging fi ndings may overlap with those of a simple cyst. Typically, a cystadenoma appears as an irregular fl uid-containing lesion with internal septations and mural nod-ules. On US, the cyst is anechoic, with irregular margins and internal echoes from septations and nodules. On CT, cystadenoma appears as a hypodense structure, and the internal features may be less well visualized, particularly on noncontrast images. MRI demonstrates a hypointense lesion on T1-weighted images and a hyperintense lesion on T2-weighted images, with heterogeneous internal features [see Figure 10].
Imaging is usually diagnostic for cystadenoma, although a simple cyst with internal hemorrhage may have a similar appearance; serologic tests for hydatid disease can help in cases where parasitic disease is in the differential. CA 19-9 is suggestive of cystadenoma over a simple hepatic cyst when elevated. Cyst aspiration is not necessary but if per-formed yields mucin-containing fl uid, usually with elevated CA 19-9 levels. Treatment for cystadenoma in the medically fi t patient is complete excision with a rim of normal paren-chyma.
Biliary cystadenocarcinoma is an extremely rare tumor thought to arise from a cystadenoma [see Figure 10]. A pre-operative diagnosis is best obtained through a US-guided needle aspiration biopsy of a soft tissue component. Tumor projects into the cyst and extends into the liver. There is a potential for extrahepatic metastases.53 Treatment is complete surgical excision and is associated with a 3-year survival of 55%.54
Biliary Tract Cancer
With an annual incidence of 7,500 new cases of cancer of the biliary system in the United States, approximately two thirds are bile duct cancers (cholangiocarcinoma); the remainder are cancers of the gallbladder. Over the last 30 years, the worldwide ratio of the extrahepatic and intra-hepatic cholangiocarcinoma has increased from 1:2 to 1:1, compromising 3% of all malignancies.55 Most patients are diagnosed in the fi fth through the seventh decade of life, with a higher predominance in males.
The etiology of cholangiocarcinoma is unknown. Most cases are sporadic, but several conditions have an increased risk of developing cholangiocarcinoma. Risk factors include primary sclerosing cholangitis (PSC), an autoimmune dis-ease characterized by infl ammation of the periductal tissues, ultimately resulting in multifocal strictures of the intrahe-patic and extrahepatic bile ducts. Patients with PSC have a lifetime risk of 8 to 20% of developing cholangiocarcinoma.56 The development of cholangiocarcinoma in patients with choledochal cysts or Caroli disease has a 3 to 28% lifetime risk.57 Hepatolithiasis, also known as recurrent pyogenic cholangiohepatitis or Oriental cholangiohepatitis, is pre-valent in Asia and shows an increased risk of cholangio-carcinoma. Finally, several radionuclides and chemical carcinogens, including thorium, radon, nitrosamines, dioxin, and asbestos, may be associated with an increased risk of cholangiocarcinoma.
ICC is described in detail under the “Primary Liver Cancers” section of this chapter. Macroscopically, extrahe-patic bile duct cancer may be sclerosing, nodular, or papillary. Microscopically, cholangiocarcinoma is most commonly a tubular adenocarcinoma, but papillary adeno-carcinoma, signet cell carcinoma, mucoepidermoid carcino-ma, and other histologic variants of cholangiocarcinoma may be observed. The type of growth pattern and location of the bile duct cancer affect clinical presentation, treatment, and prognosis.
extrahepatic cholangiocarcinoma
Extrahepatic cholangiocarcinomas may be further sub-divided into distal and hilar cholangiocarcinomas, with the
Figure 10 T2-weighted magnetic resonance image of biliary cystad-enoma, demonstrating internal septations.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 15
former arising in the intrapancreatic or retroduodenal por-tion of the bile duct and the latter arising above it, up to and including involvement of the bifurcation of the common hepatic duct. In presentation, most hilar cholangiocarcino-mas (also known as upper duct cholangiocarcinomas or Klatskin tumors) arise just below the union of the right and left hepatic ducts, at the union of the ducts, or in the main right or left hepatic duct. Cancer of the midportion of the bile duct at the usual insertion point of the cystic duct is more likely to be an extension of a gallbladder cancer than a primary cholangiocarcinoma. Perihilar tumors may be fur-ther classifi ed according to the AJCC staging criteria and the
Bismuth-Corlette system for establishing the prognosis and planning further treatment [see Figure 11].56
Distal Cholangiocarcinoma
Clinical presentation The most common presentation of distal cholangiocarcinomas is painless jaundice. Other manifestations of biliary obstruction, such as acholic stools, dark urine, and pruritis, are also prevalent. Abdominal pain, fatigue, malaise, and weight loss can also occur with advanced disease. Signs of advanced bile duct cancer of the lower duct include right upper quadrant abdominal tenderness, hepatomegaly, and a palpable gallbladder.
Type I
Type II
Type IIIa
Type IIIb
Type IV
Figure 11 Bismuth-Corlette classifi cation system of perihilar cholangiocarcinoma.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 16
Cholangitis is unusual in the absence of previous biliary tract manipulation.
The differential diagnosis for patients with these pre-sentations includes primary and metastatic hepatobiliary and pancreatic neoplasms and benign biliary strictures due to conditions such as pancreatitis, PSC, choledocholithiasis, Mirizzi syndrome, benign infl ammatory pseudotumors, and postoperative strictures. The most common cause of the benign stricture of the intrapancreatic bile duct is pancreati-tis, which may be diffuse or focal. Iatrogenic injuries rarely involve the intrapancreatic portion of the bile duct, although such injuries can occur in this area as a consequence of force-ful instrumentation. Sclerosing cholangitis may affect this section of this bile duct but usually affects other areas of the biliary tree as well.
Diagnosis In patients with extrahepatic cholangiocarci-noma, laboratory tests are usually consistent with the pres-ence of obstructive jaundice with elevation of total bilirubin and mildly elevated alkaline phosphatase. Tumor markers (CEA, CA 19-9, and CEA in combination with CA 19-9) may be useful in differentiating patients from PSC; however, their sensitivities and specifi cities are too low for use in screening or diagnosis in the general population.
Axial imaging reveals dilation of the intrahepatic bile ducts, the gallbladder, and the extrahepatic bile ducts down to the level of the pancreatic head, where the dilatation terminates abruptly. Usually, no mass is visible. Transab-dominal US that reveals dilation of the biliary tree in the absence of cholelithiasis suggests a possible biliary or pan-creatic malignancy and should prompt contrast-enhanced spiral CT scanning. CT scan fi ndings of distal cholangiocar-cinomas include dilation of the intra- and extrahepatic bile ducts and the gallbladder, with or without a mass in the head of the pancreas. In addition to offering information on the site of the lesion, the CT scan can inform staging and planning of therapies, including the presence or absence of local vascular invasion, regional lymphadenopathy, distant metastasis, and liver atrophy. If CT imaging fails to demon-strate the tumor itself, further studies may be required.
For distal cholangiocarcinomas, patients are assessed by ERCP, which shows a focal stricture, and ERCP brushings are diagnostic in about 50% of cases. Recently, MRCP is being used more commonly in this setting. Unlike con-ventional cholangiography, MRCP is noninvasive, does not require contrast material to be injected in the biliary ductal system, and allows for visualization of the bile duct both proximal and distal to the stricture. Endoscopic ultrasono-graphy (EUS) may be helpful in that it is more sensitive for small tumors than CT. Needle biopsy is directed toward the mass through the narrowest part of the bile duct. A negative biopsy result does not rule out a small bile duct cancer. The most accurate modality for diagnosing cholangiocarcinoma in patients with PSC who present with a dominant biliary stricture is EUS–fi ne-needle aspiration, with sensitivity and specifi city reaching 80 and 100%, respectively.58 “Spyglass” cholangioscopy, in which a small endoscope is directed into the biliary tree along a catheter placed by duodenoscopy, facilitates direct biopsy of the bile duct wall and lesions that project into the lumen. Additional studies are not routinely indicated. The role of PET scanning in the evaluation of
patients with cholangiocarcinoma continues to be studied but is not well established.
A particularly challenging situation can arise in patients with PSC, 20 to 50% of whom will develop a benign domi-nant biliary stricture.56 The diagnostic steps for differentiat-ing benign neoplasms from malignant tumors are essentially the same for distal cholangiocarcinoma as for pancreatic cancer. As noted, resection may be required to make the diagnosis. In any patient presenting with jaundice and a focal stricture of the bile duct, distal cholangiocarcinoma should be strongly suspected. Mass-forming bile duct cancers may also arise in the intrapancreatic duct but, for obvious reasons, are diffi cult to differentiate from pancre-atic adenocarcinomas.
Staging Surgical staging of the distal cholangiocarcino-mas is usually straightforward. These tumors are usually remote from major vascular structures and thus are not subject to the same local staging considerations as adenocar-cinomas of the pancreatic head. The exception is a tumor that extends to the top of the retroduodenal portion of the bile duct. At this point, the bile duct is apposed to the portal vein and the hepatic artery, and these structures may be invaded by bile duct tumors in this location. Chest CT should be performed prior to treatment.
Surgical management Distal cholangiocarcinoma is resected with a pancreaticoduodenectomy. The main criteria for resectability include the absence of metastatic disease and lack of involvement of the portal and superior mesen-teric veins, the hepatic artery, and superior mesenteric artery. This operation is well described in the periampullary and pancreatic adenocarcinoma.
Hilar Cholangiocarcinoma
Hilar cholangiocarcinoma is a sporadically occurring tumor that is associated with patients who have PSC, ulcer-ative colitis, or parasitic infestation. It is slow growing and locally invasive and metastasizes to the lymph nodes ahead of systemic spread, even though liver and peritoneal metas-tases may occur. Most hilar cholangiocarcinomas are charac-terized as diffusely infi ltrating cancers, mass forming, and papillary ingrowths. The tumors are further divided by the location in the upper biliary tree.
Clinical presentation The early symptoms of hilar chol-angiocarcinoma are nonspecifi c. Abdominal pain or dis-comfort, jaundice, anorexia, weight loss, and pruritus are the most common but are seen in only about one third of patients. Fever or cholangitis is uncommon at the initial presentation. It is not uncommon for patients with hilar cholangiocarcinoma to have undergone a recent cholecystec-tomy; pain and jaundice can be mistaken for symptoms of cholelithiasis. In some patients, pruritis precedes jaundice by some weeks and should be investigated promptly, espe-cially if associated with abnormal liver function tests. These patients may have elevated bilirubin, alkaline phosphatase, or c-glutamyltransferase.
The physical fi ndings are nonspecifi c as well. Jaundice and long-standing pruritis may cause patients to have mul-tiple excoriations of the skin. The liver may feel enlarged as
chapter on
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 17
a result of biliary obstruction, and the gallbladder is decom-pressed and nonpalpable.
Bacterial contamination of bile is relatively common in patients with hilar cholangiocarcinoma. Endoscopic or per-cutaneous instrumentation and previous operation signifi -cantly increase the incidence of bacterial contamination and the risk of infection. The presence of infection at the time of surgery increases postoperative morbidity and mortality. Escherichia coli, Klebsiella species, and Enterococcus species are often the most common pathogens.
When cholangiocarcinoma originates in one of the hepatic ducts, the duct may become obstructed for a considerable period before jaundice becomes apparent. The gradual and prolonged unilateral biliary obstruction or portal venous occlusion may cause atrophy of the obstructed portion of the liver. Long-standing biliary obstruction may cause moderate atrophy, whereas compromise of the portal infl ow will cause rapid and severe atrophy of involved segments. Contralat-eral hypertrophy is the expected consequence.
Diagnosis Diagnostic investigations are directed to elu-cidate the cause of biliary tract obstruction. Axial imaging is preferable to ERCP in the jaundice patient. US is nonin-vasive and may show the level of biliary obstruction and tumor extension into the bile duct and/or the periductal tis-sues. Doppler US is highly accurate in predicting vascular involvement, particularly portal venous invasion and resect-ability. CT is also an important study to determine the level of biliary obstruction, vascular involvement, and liver atrophy.
More recently, MRCP has emerged as a powerful investi-gative tool and has almost replaced ERCP or PTC for the preoperative assessment of hilar cholangiocarcinoma.59 MRCP may reveal obstruction in isolated ducts not seen on ERCP or PTC and provides information about the patency of hilar vascular structures, the presence of nodal or distant metastases, and the presence of lobar atrophy. Using data from cross-sectional imaging and MRCP, a multidisciplinary team with expertise in this disease can recommend treat-ment options, including the role of selective biliary decom-pression [see Figure 12].
ERCP has fallen out of favor in diagnosing hilar cholan-giocarcinoma because it is invasive, requires injection of dye above the malignant stricture, and often is unable to delin-eate the proximal extent of disease, which is required to determine the feasibility of reconstruction. Once the dye has been injected, stents must be placed to prevent post-ERCP cholangitis. This process may involve insertion of bilateral stents, including a stent in the atrophic hemiliver. Bilateral stenting is disadvantageous because the aim is to encourage atrophy of the hemiliver to be resected and hypertrophy of the hemiliver to be retained, and insertion of a stent in the atrophic side negates that aim. Whether stents should be employed in treating hilar cholangiocarcinoma is debatable, but if a stent is inserted, only the side to be retained should be intubated. Although ERCP may provide some useful information, PTC displays the intrahepatic bile ducts more reliably and has been the preferred study.
ERCP does have one signifi cant advantage in that it allows brushing to be obtained. Standard brushing tech-niques at this high level in the biliary tree are even less
sensitive than those at lower levels, but spyglass technology has opened this area of the biliary tree to direct biopsy on a routine basis. EUS has been employed to obtain diagnostic tissue, with some degrees of success; however, because the biopsy needle passes through the peritoneal cavity, there are concerns for tumor seeding. Such tumor seeding has not been a problem for distal cholangiocarcinomas because the biopsy tract is entirely within the future resection specimens. In many cases, a tissue diagnosis cannot be obtained pre-operatively, and the diagnosis is based on the presence of focal hilar stricture that causes jaundice.
Alternative diagnosis Focal strictures of the upper bile ducts are strongly suggestive of cancer, but cholangiocarci-nomas must also be differentiated from other diagnoses. Alternative diagnoses can be expected in 10 to 15% patients. The most common of these are gallbladder carcinoma, Mirizzi syndrome, and idiopathic infl ammatory benign tumors. Gallbladder carcinoma usually has a thickened, irregular gallbladder wall with infi ltration into segments IV and V of the liver, selective involvement of the right portal pedicle, and obstruction of the common hepatic duct with occlusion of the cystic duct on endoscopic cholangiography. Mirrizzi syndrome is a benign condition resulting from a large gallstone impacted in the neck of the gallbladder with pericholecystic and periductal infl ammation and fi brosis that can obstruct the proximal bile duct, which is often dif-fi cult to distinguish from a malignant cause. Hepatic infl am-matory pseudotumors and benign fi brosing disease can mimic hilar cholangiocarcinomas but do not involve blood vessels.
The fi nding of a smooth, tapered stricture on cholangio-graphy suggests a benign stricture. Diagnostic assessments based on the cholangiographic appearance of the stricture are unreliable, so hilar cholangiocarcinoma must remain the
Figure 12 Magnetic resonance cholangiopancreatographic image depicting a hilar cholangiocarcinoma. The mass is present at the bifur-cation (arrow), and the proximal intrahepatic ducts are all dilated. There is no visualization of the distal duct leading to the duodenum.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 18
leading diagnosis. In most cases, hilar cholangiocarcinoma cannot be ruled out without exploration. The alternative conditions that are encountered in the operating room can be addressed at the time. Relying on the results of percuta-neous needle biopsy or biliary brush cytology is dangerous and misleading. In the absence of clear contraindications, exploration is indicated in all patients in whom there is suspicion of hilar lesions.
Iatrogenic causes should be considered if the patient has had a cholecystectomy. Strictures often present years after the operation secondary to ischemic injury to the bile duct. The presence of clips close to or indenting the duct is a clue that such injury is a possibility. Choledocholithiasis may also cause strictures, especially if a history of recurrent pyo-genic cholangitis is present.
Staging Surgical staging of hilar cholangiocarcinoma, unlike that of distal cholangiocarcinoma, requires exact knowledge of the macroscopic upper extent of the tumor in the bile duct. Furthermore, invasion of hepatic arteries and portal veins is common and affects resectability. Thus, surgi-cal staging also requires accurate determination of the extent of hepatic arterial or portal venous invasion and assessment of the degree of atrophy.
The AJCC staging system for cholangiocarcinoma does not adequately account for resectability. Recently, Jarnagin and colleagues proposed the Blumgart staging system, which incorporates local tumor extent.60 In this system, tumors are classifi ed according to three factors: bile duct involve-ment according to the Bismuth-Corlette system, portal vein invasion, and hepatic lobar atrophy [see Table 6].
Surgical management Because complete surgical re-section is the only potentially curative therapy for patients with cholangiocarcinoma, all patients should be considered for surgical exploration. However, there is potential for signifi cant morbidity and mortality associated with cholan-giocarcinoma resection, and all patients considered for re-section should receive preoperative treatment for correctable medical comorbidities, such as malnutrition, coagulopathy, and treatable cardiac, pulmonary, and renal disease.
The use of preoperative stenting is no longer routine and may increase the rate of infectious complications. However, selective application of stenting in patients may be bene-fi cial. Advantages to stenting include decompressing an ob-structed biliary tree (in patients with a bilirubin > 10 mg/dL, to allow hepatic function to improve) and providing patients suffering from malnutrition, biliary sepsis, or other medical
Table 6 Staging of Cholangiocarcinoma20,60
Staging System Stage Tumor Node Metastasis
AJCC TNM 0 Tis N0 M0 Distal IA T1 N0 M0
IB T2 N0 M0IIA T3 N0 M0IIB T1 to T3 N1 M0III T4 Any N M0IV Any T Any N M1
Tis, carcinoma in situ; T1, confined to bile duct; T2, beyond bile duct; T3, invades gallbladder, pancreas, duodenum without involving celiac axis or SMA; T4, celiac axis or SMA; N1, regional LN metastasis; M1, distant metastasis
Perihilar 0 Tis N0 M0I T1 N0 M0II T2a–b N0 M0IIIA T3 N0 M0IIIB T1–3 N1 M0IVA T4 N0–1 M0IVB Any T
Any TN2Any N
M0M1
Tis, carcinoma in situ; T1, confined to bile duct; T2a, beyond bile duct; T2b, tumor invades adjacent hepatic parenchyma; T3, invades unilateral branches of the PV or HA; T4, invades main PV or HA; N1, regional LN metastasis; N2, metastasis to periaortic, pericaval, SMA, celiac nodes; M1, distant metastasis
Blumgart T stage: criteria perihilar
T1 Tumor involving biliary confluence ± unilateral extension to second-order biliary radicals
T2 Tumor involving biliary confluence ± unilateral extension to second-order biliary radicals and ipsilateral PV involvement ± ipsilateral hepatic lobar atrophy
T3 Tumor involving biliary confluence plus bilateral extension to second-order biliary radicals; or unilateral extension to second-order biliary radicals with contralateral PV involvement; or unilateral extension to second-order radicals with contralateral hepatic lobar atrophy; or main or bilateral PV involvement
AJCC = American Joint Committee on Cancer; HA = hepatic artery; LN = lymph node; PV = portal vein; SMA = superior mesenteric artery; TNM staging system: T = pri-mary tumor, N = regional lymph nodes, M = distant metastasis.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 19
problems time to recover before an elective operation. If biliary stenting is applied, we recommend decompressing the side of the liver to be retained and waiting until the serum bilirubin falls to 3 mg/dL.
A reasonable strategy is to proceed to operation if (1) the patient is relatively young (< 70 years), (2) there are no seri-ous comorbid conditions, (3) the jaundice had been present for less than 4 weeks, (4) the serum bilirubin concentration is lower than 10 mg/dL, and (5) the future remnant liver will include more than 35% of the total liver mass. Patient-related contraindications include severe medical comorbi-dities, especially major cardiopulmonary disease, cirrhosis, and metastatic disease. Blumgart and colleagues proposed local tumor-related criteria for resectability.60 Tumor-related contraindications include encasement or occlusion of the main portal vein or hepatic artery either bilaterally or prox-imal to the bifurcation, involvement of the bilateral second-ary ducts or unilateral ducts with contralateral vascular compromise, and hepatic lobe atrophy with contralateral secondary duct or portal vein involvement.
There are two objectives in the therapy of hilar cholan-giocarcinoma: (1) complete tumor excision with negative margins and (2) restoration of biliary-enteric continuity. The surgery for hilar cholangiocarcinoma includes removal of the extrahepatic biliary tree and bile duct bifurcation, the side of the liver with greater ductal involvement, extensive hilar lymphadenectomy, and then reconstruction of biliary-enteric continuity. Many centers advocate caudate resection because the caudate has short bile ducts that enter the pos-terior surfaces of the main right and left bile ducts at the bifurcation of the common hepatic duct. When the future remnant liver will include less than 30 to 35% of the total liver mass, portal vein embolization of the side to be re sected may be performed to induce hypertrophy of the remnant. Some centers have advocated resection of the portal venous bifurcation and anastomosis of the main and remnant portal vein to avoid dissection in the hilum with the poten-tial for tumor dissemination. Liver transplantation has been used successfully to manage Bismuth-Corlette type IV tumors (extending to the bilateral secondary bile ducts) [see Figure 12] and is usually performed after neoadjuvant chemoradiation therapy and staging laparotomy in highly selected patients.
Adjuvant therapy Adjuvant chemotherapy, radiothera-py, or chemoradiotherapy is commonly offered to patients. Several small trials of adjuvant chemotherapy have been reported, but these demonstrated only low partial-response rates and no major survival benefi t. Two separate trials showed no benefi t of adjuvant external beam and intralumi-nal radiation therapy.61,62 At present, there are no data to support the routine use of adjuvant or neoadjuvant che-motherapy or radiation therapy except in the context of a clinical trial.
Palliation Palliative treatment for cholangiocarcinoma is important because many patients with hilar cholangiocar-cinoma are not suitable for resection. In this setting, manage-ment options include some form of biliary decompression or supportive care. Jaundice alone is not an indication for
biliary decompression. Current indications for biliary decom-pression for unresectable patients are to provide symptom-atic relief for intractable pruritis, treat cholangitis, gain access for intraluminal radiotherapy, and allow hepatic function recovery in patients receiving chemotherapy.
Endoscopic placement of biliary stents has low complica-tion rates and high rates of symptomatic relief for patients with biliary obstruction caused by unresectable tumors, especially distal cholangiocarcinoma. The effectiveness of biliary stents is limited because of frequent obstruction and the need for replacement. Self-expanding metallic biliary stents have improved patency rates but are more diffi cult to change when they become obstructed. Hilar tumors are more diffi cult to traverse with the endoscopic technique. The failure rates and incidence of subsequent cholangitis are high. Most patients with unresectable hilar tumors are not candidates for endoscopic biliary drainage.
Percutaneous transhepatic biliary drainage and sub-sequent placement of a self-expanding metallic stent can be performed in most patients with unresectable hilar cholan-giocarcinoma. Satisfactory drainage of only 25 to 30% of functional hepatic parenchyma is required for resolution of jaundice. Often hilar cholangiocarcinoma obstructs more than one region of the duct and two or more stents must be placed for adequate drainage. Revision of these percutane-ous drains is relatively straightforward, and they can be kept internalized for physiologic excretion into the small intestine.
For patients who are found to have carcinomatosis at the time of exploratory laparoscopy, laparoscopic cholecys-tectomy was traditionally recommended, to prevent sub-sequent development of acute cholecystitis related to biliary stent–induced cystic duct obstruction. The value of doing a prophylactic cholecystectomy is unproven and should be performed only if it can be done safely. Endoscopic or per-cutaneous stenting should be performed postoperatively.
For patients who are found to have unresectable disease at the time of open exploration, surgical biliary enteric bypass offers more durable palliation than percutaneous or endoscopic stenting. Patients with unresectable distal cholangiocarcinoma should undergo choledocho- or hepa-ticojejunostomy. The palliative options for patients with unresectable hilar cholangiocarcinoma include tumor de-bulking with Roux-en-Y hepaticojejunostomy and intra-operative placement of Silastic transhepatic catheters. The Roux-en-Y hepaticojejunostomy is most commonly done to segment III hepatic ducts. The segment III hepatic duct can be approached by following the falciform ligament into the recess of the left lobe in the umbilical fi ssure.
External-beam radiation and transcatheter brachytherapy may help with pain relief and biliary decompression; however, the effects of radiation on survival are confl icting. Recently published data from a clinical trial indicate that the combination of gemcitabine plus cisplatin should be offered to patients with advanced bile duct cancer. Of nearly 60% patients who were enrolled in the phase III clinical trial that had locally advanced cholangiocarcinoma, the gemcitabine-cisplatin combination was associated with prolongation of overall and progression-free survival compared with ad-ministration of gemcitabine alone.61 Finally, photodynamic
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 20
therapy, which involves a photosensitizer to be injected and direct illumination via cholangiography to allow for tumor cell death, has shown some promising results. A random-ized study in patients with unresectable cholangiocarcinoma suggested improved survival with bilary stenting combined with photodynamic therapy compared with biliary stenting alone.63 However, because of the limitations and fl aws in the study, the improved survival observed with photodynamic therapy is attributed to better biliary decompression rather than the reduction of tumor burden. Additional study of this modality is necessary.
Outcomes Extrahepatic cholangiocarcinoma resectabi-lity rates are reported to range from 30 to 50%.64 The pro-portion of patients undergoing resection was far greater for distal lesions than for hilar lesions. Complication rates after operation of cholangiocarcinoma range from 10 to 60% depending on the location of the tumor. Perihilar resections have the highest rates of complication. Overall mortality rates range from 0 to 15%. Long-term survival rates for chol-angiocarcinoma depend on tumor location and are highest for intrahepatic tumors and lowest for perihilar tumors. In the Johns Hopkins series, the 5-year survival for R0-resected intrahepatic, perihilar, and distal tumors was 63%, 30%, and 27%, respectively.62 Survival following resection of cholan-giocarcinoma depends on several factors, especially margin status, lymph node status, tumor size, and differentiation. When R0 patients are analyzed, lymph node status remains a signifi cant predictor of survival. Palliated patients have a median survival of less than 12 months.65 The median over-all survival among patients treated with the combination of gemcitabine and cisplatin was 11.7 months compared with 8.1 months in patients treated with gemcitabine alone.61
gallbladder carcinoma
Gallbladder cancer is rare in most Western countries and is associated with a poor prognosis due to late presentation and a lack of effective therapy. However, there have been an increasing number of early-stage cases found incidentally with some hope of cure. It is the most common malignancy of the biliary tract and fi fth most common malignancy of the gastrointestinal tract. In the United States, there are an esti-mated 6,500 new cases, with 3,200 deaths from gallbladder cancer annually.
Worldwide, the highest incidence rates occur among populations in the Western part of South America (e.g., Chile and Peru), North American Indians, Mexican Ameri-cans, and northern India. The highest worldwide incidence is in Delhi, India, at 21.5 per 100,000; by comparison, in the United States, the overall incidence is 2.5 per 100,000.66 The incidence of gallbladder cancer parallels that of choleli-thiasis, increasing with age and two to six times higher in women than in men.
The best characterized risk factor for the development of gallbladder carcinoma is chronic infl ammation associated with gallstones, which raises the question of whether gall-stones predispose to gallbladder carcinoma. The prevalence of cholelithiasis is greater than 25 million individuals, but only 0.5 to 3% of patients who undergo a laparoscopic cho-lecystectomy for symptomatic cholelithiasis are diagnosed
with gallbladder cancer.67 However, 70 to 90% of patients diagnosed with gallbladder cancer have gallstones present at the time of diagnosis. Gallstone size directly increases the relative risk of developing gallbladder cancer; patients with stones less than 3 cm have a relative risk of developing cancer of 2.5 compared with patients with stones greater than 3 cm, which has a relative risk of 10. However, there is no recommendation for prophylactic cholecystectomy in asymptomatic patients with large stones.
Other risk factors implicated for the development of gall-bladder cancer include porcelain gallbladder, adenomatous polyps of the gallbladder, chronic infection with Salmonella typhi, carcinogen exposure (e.g., miners exposed to radon), and abnormal pancreaticobiliary duct junction (APBDJ). The incidence of gallbladder cancer was previously reported to range from 12.5 to 60% in patients with porcelain gall-bladder; however, modern series have shown a much lower incidence that is closer to 5 to 10%.68 The type of calcifi cation seems to be associated with the degree of risk; stippled classifi cation of the mucosa is higher risk than diffuse intra-mural calcifi cation. Patients with APBDJ have a long com-mon channel formed by an abnormally proximal junction of the pancreatic and common bile duct and elevated sphincter of Oddi pressures that create a predisposition to refl ux of pancreatic exocrine secretions into the bile ducts. APBDJ appears to increase the risk of biliary cancers, especially gallbladder cancers.69
Pathogenesis
Chronic infl ammation of the gallbladder mucosa related to gallstones is hypothesized to be the major factor leading to malignant transformation in most cases of gallbladder cancer. The progression from dysplasia to carcinoma in situ to invasive carcinoma over a 15-year period has been de-scribed for gallbladder cancer. Chronic infl ammation from stones or other processes is postulated to be the inciting event in the dysplasia to carcinoma pathway. The molecular changes associated with this progression are under investi-gation: K-ras mutations appear to be relatively uncommon, whereas TP53 mutations are prevalent and tend to arise early during this progression.66
Eighty percent of primary gallbladder carcinomas are adenocarcinomas. Other histologic types include small cell cancer, squamous cell carcinoma, lymphoma, and sarcoma. Gallbladder carcinomas are also classifi ed according to mor-phology as infi ltrative, nodular, or papillary. Infi ltrative or nodular cancers have a more diffuse pattern of growth that is diffi cult to recognize on imaging studies. These lesions are more likely to invade the liver and have usually metasta-sized to lymph nodes by the time of diagnosis. Papillary cancers are associated with a better prognosis because they tend to grow within the gallbladder lumen and are less likely to invade the liver or metastasize to lymph nodes.
Clinical Presentation
Patients with gallbladder cancer are asymptomatic or have symptoms such as abdominal pain, anorexia, nausea, and vomiting that may be impossible to differentiate from symptomatic cholelithiasis or cholecystitis. In early stages of the disease in which the tumor is confi ned to the wall of the
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 21
gallbladder, the symptoms are usually those of biliary colic from associated stones, and the cancer is silent. Gallbladder cancer is discovered incidentally during performance of cholecystectomy or on specimen processing. With advanced disease, patients can present with weight loss, obstructive jaundice (from tumor invasion into the biliary tree), and duodenal obstruction. On physical examination, patients with advanced disease may have a palpable abdominal mass, hepatomegaly, or ascites. Jaundice occurs in about 50% of patients and is a poor prognostic sign because it signifi es extension of the tumor beyond the gallbladder and ob struction of the extrahepatic ducts. Most gallbladder cancer patients with jaundice have unresectable tumors.
Diagnosis
Laboratory studies are generally nonspecifi c in gallblad-der cancer. Serum alkaline phosphatase, alanine amino-transferase, and aspartate aminotransferase levels may be elevated, especially in the presence of advanced hepatic invasion or metastasis. CEA and CA 19-9 levels have been shown to be elevated in gallbladder cancer in 18 to 30% of patients, respectively; however, they lack suffi cient sensitiv-ity or specifi city to be useful in clinical decision making for individual patients.
The initial imaging study performed for a patient with gallbladder symptoms includes US. Findings suggestive of gallbladder cancer on US are mural thickening or calcifi ca-tion, a gallbladder mass greater than 1 cm in diameter, and loss of the normal gallbladder wall–liver interface. The diag-nostic accuracy of this examination is greater than 80% for gallstones but only 50% for gallbladder cancer.70
CT scanning should be performed on patients suspected of having gallbladder cancer. Findings for gallbladder cancer include a mass protruding into the gallbladder lumen or completely replacing the gallbladder and focal or diffuse thickening of the gallbladder wall. CT scanning also shows information on the presence or absence of distant metasta-ses, regional lymph node involvement, and local invasion into the liver and porta hepatis [see Figure 13]. The extent of
adjacent liver involvement is particularly important in plan-ning the extent of liver resection. The fi nding of para-aortic or peripancreatic nodal disease beyond the head of the pancreas on imaging precludes surgical resection. Imaging should also include the chest because this is a common site of distant disease. Recently, PET has proved to be the most sensitive modality to determine distant metastasis and can reduce unnecessary explorations.
MRI and MRCP can offer additional information on local invasion, particularly in the porta hepatitis. They may not be necessary if CT fi ndings are adequate. Similarly, endoscopic or percutaneous cholangiography is not routinely indicated; however, it may be used for palliation or preoperative man-agement of jaundice. EUS offers greater accuracy in assess-ing gallbladder wall penetration by masses and regional lymph node involvement. Selective application of EUS in patients with a gallbladder mass can help in the determina-tion of whether the mass is nonneoplastic. In addition, EUS-guided biopsy is an effective technique in cases in which a tissue diagnosis is required. Percutaneous US- or CT-guided biopsy is a useful technique for confi rming the diagnosis in patients with unresectable tumors but is not recommended for surgical candidates because of potential tumor seeding.
Staging
Gallbladder cancer can spread locally through direct invasion of the liver or adjacent organs such as the colon or duodenum. High-risk hepatic areas for local extension are segments IVb and V. Dissemination also occurs via lym-phatics, which run just beneath the muscle layer of the gall-bladder wall, which accounts for the 80% of lymph node involvement in T2–T4 disease. The third route of dissemina-tion is hematogenous, and the sites most involved are the lung and brain. Finally, gallbladder carcinoma can spread directly via the peritoneum. Gallbladder cancer has the ability to seed the peritoneum, surgical wounds, and laparo-scopic port sites. Therefore, advanced disease should be ap-p roached with a diagnostic laparoscopy before a laparotomy is attempted.
The newest edition of the AJCC, published in 2010, con-tains important modifi cations to the staging of gallbladder cancer contained in the older editions. N stage now includes N1 (metastasis to cystic duct, common bile duct, hepatic artery, and/or portal vein lymph nodes) and N2 (metastasis to periaortic, pericaval, superior mesenteric artery, and/or celiac artery lymph nodes) designations. Stage classi fi cations have also been revised to better refl ect patient outcomes [see Table 7].
Surgical Treatment
Surgical resection is the only known potentially curative treatment for gallbladder cancer. Unfortunately, most pa-tients present with advanced disease, and curative resection is feasible in only 10 to 30% of patients. The overall 5-year survival for patients with gallbladder cancer is less than 5%, with a median survival of 5 to 8 months.71 An aggressive surgical approach to advanced regional disease has shown the potential for long-term survival.
Treatment for gallbladder cancer is primarily based on the T stage of the tumor. Factors such as age, nutritional status,
Figure 13 Computed tomographic scan depicting a gallbladder carcinoma.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 22
and cardiopulmonary and hepatic function must also be considered. Contraindications for surgical resection include liver metastases, malignant ascites, peritoneal metastases, distant disease, extensive involvement of the hepatoduode-nal ligament, encasement or occlusion of major vessels, and poor performance status. Studies also show that para-aortic lymph node involvement has a survival similar to distant metastasis in gallbladder cancer and is considered a con-traindication for surgery.71
Early lesions: Tis and T1a For patients with early Tis and T1a stage cancers where invasion is limited to the lamina propria, a simple cholecystectomy is the treatment of choice. Typically, these tumors are diagnosed incidentally in cholecystectomy specimens because they are usually not obvious in imaging studies. Since these tumors do not invade the muscular layer, a simple cholecystectomy dis-sects the perimuscular layer and, theoretically, should be curative. There is minimal chance of lymph node involve-ment, but it is crucial to get negative margins along the gall-bladder wall and the cut edge of the cystic duct. If the cystic duct margin is positive, it is necessary to resect the common bile duct with biliary reconstruction to obtain a negative
margin. Overall, the cure rates with simple cholecystectomy to negative margins are 85 to 100%.72 Laparoscopic and open cholecystectomies have shown equal survival rates and local control rates. However, if a patient has suspected gallblad-der cancer or a high-risk polypoid lesion, the laparoscopic approach should not be performed because of the increased risk of peritoneal spread and seeding if there is spillage of gallbladder contents, as well as the possibility of trocar site implantation.
T1b and T2 lesions The management of T1b lesions, which invade the muscularis but do not extend into the perimuscular connective tissue, has been controversial. T2 lesions invade the perimuscular connective tissue but do not go beyond the serosa or into the liver. T1b lesions have a 15% rate of lymph node metastasis, and in T2 lesions, regional lymph node metastases are found in 40 to 80% of cases.73 Invasion of the perimuscular connective tissue of the gallbladder increases the chance of extension into the adjacent hepatic parenchyma. A simple cholecystectomy is not appropriate treatment for these tumors because the re-section plane is subserosal and can leave cancer cells in the serosa that can extend into the liver. In patients who have only received a simple cholecystectomy, reexploration reveals residual tumor in 40 to 76% of cases.74
For T1b or T2 lesions, as long as preoperative and intra-operative staging shows no obvious metastases or unresect-able local disease, the gallbladder is resected en bloc with a minimum of a 2 cm hepatic parenchyma margin, and lym-phadenectomy is performed. Lymphadenectomy consists of dissection of lymph node beds in the porta hepatis, gastroduodenal ligament, and gastrohepatic ligament and a Kocher maneuver with removal of the lymph nodes along the posterior duodenum and behind the pancreatic head [see Figure 14]. Some studies show that to perform an ade-quate porta hepatis dissection, it is necessary to resect the extrahepatic bile duct and undertake a biliary reconstruc-tion. Extrahepatic resection should be performed in patients who present with obstructive jaundice resulting from inva-sion of tumor and for tumors located in the neck of the gallbladder or in the cystic duct. However, it is unclear if extrahepatic resection is of any benefi t to patients who are not jaundiced.
There is convincing evidence that such radical surgery is associated with improved survival for patients with T1b and T2 gallbladder cancer. In published series, the 5-year sur-vival rate for patients with T1b gallbladder cancer having undergone radical resection averages 87.5%, whereas it averages only 61.3% in patients who underwent simple cholecystectomy alone.75 In T2 lesions, extended resection or radical cholecystectomy (61%) is associated with a much better overall survival than simple cholecystectomy alone (19%).76 Extended cholecystectomy can be performed with minimal morbidity and a 1% mortality rate.
T3 lesions The most controversial aspect of the surgical treatment of gallbladder cancer involves patients with non-metastatic locally advanced tumors that perforate the gall-bladder serosa or directly invade the liver and/or adjacent organ. Historically, these patients were documented to have extremely poor survival and surgical resection was thought
Table 7 AJCC Staging of Gallbladder Carcinoma (7th edition), 2010
T: Primary tumors (T) Tx Primary tumor cannot be assessed T0 No evidence of primary tumor Tis Carcinoma in situ T1 Tumor invades lamina propria or muscular layer T1a Tumor invades lamina propria T1b Tumor invades muscular layer T2 Tumor invades perimuscular connective tissue; no
extension beyond serosa or into liver T3 Tumor perforates the serosa (visceral peritoneum)
and/or directly invades the liver and/or one other adjacent organ or structure, such as the stomach, duodenum, colon, pancreas, omentum, or extrahepatic bile ducts
T4 Tumor invades main portal vein or hepatic artery or invades two or more extrahepatic organs or structures
N: Regional lymph nodes (N) NX Regional lymph nodes cannot be assessed N0 No regional lymph node metastasis N1 Metastases to nodes along the cystic duct, common bile
duct, hepatic artery, and/or portal vein N2 Metastases to periaortic, pericaval, superior mesenteric
artery, and/or celiac artery lymph nodes
M: Distant metastasis (M) MX Distant metastasis cannot be assessed M0 No distant metastasis M1 Distant metastasis
Staging Stage 0 Tis N0 M0 Stage I T1 N0 M0 Stage II T2 N0 M0 Stage IIIA T3 N0 M0 Stage IIIB T1–T3 N1 M0 Stage IVA T4 N0–1 M0 Stage IVB Any T N2 M0 Any T Any N M1
AJCC = American Joint Committee on Cancer.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 23
to be futile. However, numerous small studies have docu-mented that with varying levels of extended resections, long-term survival is possible in highly selected patients. Diagnostic laparoscopy should be strongly considered before exploratory laparotomy in locally advanced T3 tumors to identify patients with peritoneal seeding of the cancer prior to an open operation. If the tumor locally invades the colon, duodenum, or liver, complete local re-section is indicated and can improve survival if negative margins can be obtained.
A 25 to 44% 5-year survival rate can be achieved with radical surgery.77 The extent of hepatic resection is deter-mined by the local invasion of the liver. Lesions that have
minimal extension into the liver can usually be approached with simple wedge or segment IVb and V resection. As the lesion size increases or vascular structure are affected, more extensive resections are required. It does not appear that anatomically based resections have any survival benefi t over plain wedge resection, but to obtain R0 resection in T3 lesions, larger liver resections are necessary.
T4 lesions Patients with a T4 lesion that invades the main portal vein or hepatic artery or invades two or more extrahepatic organs or structures meet the criteria for unre-sectability. Anecdotal reports of superradical procedures involving resection of the main portal vein and/or common
Extent of Node Clearance
a
e
d
c
b
Figure 14 Lymph node designations used to describe the extent of dissection in a radical cholecystectomy for gallbladder carcinoma. (a–e) Lymph node fi eld.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 24
hepatic artery exist, but these procedures are associated with increased morbidity and mortality rates and are unlikely to confer any survival benefi t. There is no evidence to support debulking cholecystectomy to prevent subsequent episodes of cholecystitis.
incidental gallbladder cancer
Incidental fi nding of malignancy after laparoscopic chole-cystectomy occurs in 1 to 2% of laparoscopic cholecy-stectomies and represents a relatively new and challenging problem in the treatment of gallbladder cancer.78 A majority of these patients will have T1a mucosal lesions. For Tis and T1a, no further resection is necessary if the cystic duct mar-gins are negative for tumor, and the 5-year survival rate for these patients is 85 to 100%.72
Patients who are found to have T1b lesions on pathologic review of the gallbladder should be appropriately staged and, in the absence of distant disease and peritoneal spread, offered liver resection to improve long-term survival.76 Before resection, staging with imaging and possible laparos-copy should be performed to rule out distant disease or peritoneal spread. Some authors also advocate resection of port sites at the time of resection, but this remains con-troversial.
During routine cholecystectomy, suspicion of cancer should be considered if the procedure is more diffi cult or unusual than expected. Conversion to an open operation to prevent spillage and seeding should be considered. If a sus-picious lesion is identifi ed, a frozen section can be performed to confi rm the diagnosis and to assess the depth of tumor invasion. If the diagnosis of T2 or greater gallbladder cancer is confi rmed, the surgeon can proceed to an open radical cholecystectomy. Another choice is to perform simple chole-cystectomy, closure, and image-guided staging and then refer the patient to a local hepatobiliary expert. Long-term survival is the same if the extended cholecystectomy is per-formed at the initial operation or during a later operation.76
Unfortunately, some patients present with extensive peritoneal seeding or port-site disease even though their primary cancer was small or undetected after routine chole-cystectomy. Port-site seeding after laparoscopic cholecy-stectomy with presentation as advanced disease had been reported in 5 to 20% of cases.79 Recognition of this problem has prompted surgeons to use extraction bags and to adopt a liberal policy of converting to an open procedure if there is any question of a cancer because perforation and spillage have been reported to lead to a high rate (40%) of port-site recurrence.79
Adjuvant Therapy
Currently, there are limited clinical trial data to support adjuvant treatment postresection because no prospective randomized trials have been performed. However, adjuvant chemotherapy is commonly administered after resection of gallbladder cancers. In the National Comprehensive Cancer Network guidelines, 5-FU- or gemcitabine-based chemo-therapy should be considered except in Tis or T1a and N0 patients. Some studies suggest that external-beam or intra-operative radiation therapy alone or in combination with
5-FU is associated with diminished rates of local recurrence. The impact of these regimens on survival is unclear; no data derived from prospective randomized clinical trials on the effi cacy of these regimens exist.
Palliation
The most common problem with gallbladder cancer is palliation because most patients are unresectable at presen-tation. The outcome for these patients is poor, and chemo-therapy offers minimal increase in survival. Patients who present with locally unresectable or metastatic disease have an overall dismal prognosis, often with survival of less than 1 year. The majority of patients require palliation for pain, jaundice, and possibly intestinal obstruction. Minimal morbidity is important for any palliative procedures, con-sidering that median survival in this group may be only 2 to 4 months. If unresectable disease is encountered during an exploratory laparotomy, jaundice and obstruction can be treated with choledochojejunostomy and gastrojejunostomy depending on the location of the tumor. Biliary obstruction can also be treated with endoscopic or percutaneous drain-age. In general, operative exploration should be avoided because median survival is already poor; endoscopic stent placement for biliary or intestinal obstructions can offer these patients symptom relief without the need for postsur-gical recovery. Chemotherapy and radiotherapy have been largely unsuccessful in treating this disease. Response rates are low, but occasionally disease stabilization can be achieved for a few months. Patients can also be referred for enrolment in a clinical trial or offered 5-FU- or gemcitabine-based chemotherapy or best supportive care.
Outcomes
The National Cancer Data Base reports 5-year survival rates for patients with T1N0, T2N0, and T3N0 (or node-negative) disease at 39%, 15%, and 5%, respectively.80 How-ever, more contemporary surgical series suggest that sub-stantially improved outcomes can be achieved in resectable gallbladder cancers. In these reports, 5-year survival rates following resection of T1 lesions range from 85 to 100%. With radical resection of T2, T3, and T4 lesions, 5-year sur-vival is 80 to 90%, 15 to 63%, and 2 to 25%, respectively.81
Financial Disclosures: Gabriela M. Vargas, MD, Purvi Parikh, MD, FACS, and Kimberly M. Brown, MD, FACS, have no fi nancial relationships to disclose. This chapter was previously authored by Steven M. Strasberg, MD, FACS, FRCSC, FRCS(Ed), and David C. Linehan, MD, FACS, with disclosure made at the time of initial publication. This chapter has been reviewed, updated, and rereleased by the authors listed.
References
1. Strasberg S, Belghiti J, Clavien PA, et al. The Brisbane 2000 terminology of liver anatomy and resections. HPB 2000;2:333–9.
2. Seeff LB. Introduction: The burden of hepatocellular carci-noma. Gastroenterology 2004;127(5 Suppl 1):S1–4.
3. Altekruse SF, McGlynn KA, Reichman ME. Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J Clin Oncol 2009;27:1485–91.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 25
4. Hassan MM, Frome A, Patt YZ, El-Serag HB. Rising preva-lence of hepatitis C virus infection among patients recently diagnosed with hepatocellular carcinoma in the United States. J Clin Gastroenterol 2002;35:266–9.
5. Zhang BH, Yang BH, Tang ZY. Randomized controlled trial of screening for hepatocellular carcinoma. J Cancer Res Clin Oncol 2004;130:417–22.
6. Bruix J, Reig M, Rimola J, et al. Clinical decision making and research in hepatocellular carcinoma: pivotal role of imaging techniques. Hepatology 2011;54:2238–44.
7. Bruix J, Sherman M; American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology 2011;53:1020–2.
8. Sacks A, Peller PJ, Surasi DS, et al. Value of PET/CT in the management of primary hepatobiliary tumors, part 2. AJR Am J Roentgenol 2011;197:W260–5.
9. Tohme S, Geller DA, Cardinal JS, et al. Radiofrequency ablation compared to resection in early-stage hepatocellular carcinoma. HPB 2013;15:210–7.
10. Schwartz M, Roayaie S, Konstadoulakis M. Strategies for the management of hepatocellular carcinoma. Nat Clin Pract Oncol 2007;4:424–32.
11. Tse RV, Hawkins M, Lockwood G, et al. Phase I study of individualized stereotactic body radiotherapy for hepato-cellular carcinoma and intrahepatic cholangiocarcinoma. J Clin Oncol 2008;26:657–64.
12. Cárdenes HR, Price TR, Perkins SM, et al. Phase I feasibility trial of stereotactic body radiation therapy for primary hepatocellular carcinoma. Clin Transl Oncol 2010;12:218–25.
13. National Comprehensive Cancer Network. Clinical practice guidelines in oncology (NCCN guidelines) hepatobiliary cancers. v2.2012. Available at: http://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf (accessed March 20, 2013).
14. Sia D, Tovar V, Moeini A, Llovet JM. Intrahepatic cholan-giocarcinoma: pathogenesis and rationale for molecular therapies. Oncogene 2013;32:4861–70.
15. Shaib Y, El-Serag HB. The epidemiology of cholangiocarci-noma. Semin Liver Dis 2004;24:115–25.
16. Palmer WC, Patel T. Are common factors involved in the pathogenesis of primary liver cancers? A meta-analysis of risk factors for intrahepatic cholangiocarcinoma. J Hepatol 2012;57:69–76.
17. Petrowsky H, Hong JC. Current surgical management of hilar and intrahepatic cholangiocarcinoma: the role of resec-tion and orthotopic liver transplantation. Transplant Proc 2009;41:4023–35.
18. Kim JY, Kim MH, Lee TY, et al. Clinical role of 18F-FDG PET-CT in suspected and potentially operable cholangio-carcinoma: a prospective study compared with conven-tional imaging. Am J Gastroenterol 2008;103:1145–51.
19. Petrowsky H, Wildbrett P, Husarik DB, et al. Impact of integrated positron emission tomography and computed tomography on staging and management of gallbladder cancer and cholangiocarcinoma. J Hepatol 2006;45:43–50.
20. Edge SB. American Joint Committee on Cancer: AJCC Cancer Staging Manual. 7th ed. New York: Springer; 2009.
21. American Joint Committee on Cancer summary of changes: understanding the changes from the sixth to the seventh edition of the AJCC Cancer Staging Manual. Available at:
http://www.cancerstaging.org/staging/index.html (acces-sed March 22, 2013).
22. Hong JC, Petrowsky H, Kaldas FM, et al. Predictive index for tumor recurrence after liver transplantation for locally advanced intrahepatic and hilar cholangiocarcinoma. J Am Coll Surg 2011;212:514–20; discussion 20–1.
23. Hong JC, Jones CM, Duffy JP, et al. Comparative analysis of resection and liver transplantation for intrahepatic and hilar cholangiocarcinoma: a 24-year experience in a single center. Arch Surg 2011;146:683–9.
24. de Jong MC, Nathan H, Sotiropoulos GC, et al. Intrahepatic cholangiocarcinoma: an international multi-institutional analysis of prognostic factors and lymph node assessment. J Clin Oncol 2011;29:3140–5.
25. Hyder O, Hatzaras I, Sotiropoulos GC, et al. Recurrence after operative management of intrahepatic cholangiocarci-noma. Surgery 2013;153:811–8.
26. Tzeng CW, Aloia TA. Colorectal liver metastases. J Gastro-intest Surg 2013;17:195–202.
27. Fedorowicz Z, Lodge M, Al-asfoor A, Carter B. Resection versus no intervention or other surgical interventions for colorectal cancer liver metastases. Cochrane Database Syst Rev 2008;(2):CD006039.
28. National Comprehensive Cancer Network. Clinical practice guidelines in oncology colon cancer. Available at: http://www.nccn.org/professionals/physician_gls/pdf/colon.pdf (accessed March 6, 2013).
29. Pawlik TM, Olino K, Gleisner AL, et al. Preoperative che-motherapy for colorectal liver metastases: impact on hepatic histology and postoperative outcome. J Gastrointest Surg 2007;11:860–8.
30. Rivoire M, De Cian F, Meeus P, et al. Combination of neoadjuvant chemotherapy with cryotherapy and surgical resection for the treatment of unresectable liver metastases from colorectal carcinoma. Cancer 2002;95:2283–92.
31. Adam R, Avisar E, Ariche A, et al. Five-year survival following hepatic resection after neoadjuvant therapy for nonresectable colorectal. Ann Surg Oncol 2001;8:347–53.
32. Lam VW, Pang T, Laurence JM, et al. A systematic review of repeat hepatectomy for recurrent colorectal liver metastases. J Gastrointest Surg 2013;17:1312–21.
33. Choti MA, Sitzmann JV, Tiburi MF, et al. Trends in long-term survival following liver resection for hepatic colorectal metastases. Ann Surg 2002;235:759–66.
34. Abdalla EK, Vauthey JN, Ellis LM, et al. Recurrence and outcomes following hepatic resection, radiofrequency abla-tion, and combined resection/ablation for colorectal liver metastases. Ann Surg 2004;239:818–25; discussion 25–7.
35. Minagawa M, Makuuchi M, Torzilli G, et al. Extension of the frontiers of surgical indications in the treatment of liver metastases from colorectal cancer: long-term results. Ann Surg 2000;231:487–99.
36. House MG, Ito H, Gönen M, et al. Survival after hepatic resection for metastatic colorectal cancer: trends in out-comes for 1,600 patients during two decades at a single institution. J Am Coll Surg 2010;210:744–52, 52–5.
37. Jones RP, Jackson R, Dunne DF, et al. Systematic review and meta-analysis of follow-up after hepatectomy for colorectal liver metastases. Br J Surg 2012;99:477–86.
38. Rindi G, Wiedenmann B. Neuroendocrine neoplasms of the gut and pancreas: new insights. Nat Rev Endocrinol 2012;8:54–64.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 26
39. Pavel M, Baudin E, Couvelard A, et al. ENETS Consensus Guidelines for the management of patients with liver and other distant metastases from neuroendocrine neoplasms of foregut, midgut, hindgut, and unknown primary. Neuro-endocrinology 2012;95:157–76.
40. Pavel ME, Hainsworth JD, Baudin E, et al. Everolimus plus octreotide long-acting repeatable for the treatment of advanced neuroendocrine tumours associated with car-cinoid syndrome (RADIANT-2): a randomised, placebo-controlled, phase 3 study. Lancet 2011;378:2005–12.
41. Yao JC, Shah MH, Ito T, et al. Everolimus for advanced pancreatic neuroendocrine tumors. N Engl J Med 2011;364:514–23.
42. Le Treut YP, Grégoire E, Klempnauer J, et al. Liver trans-plantation for neuroendocrine tumors in Europe-results and trends in patient selection: a 213-case European Liver Transplant Registry study. Ann Surg 2013;257:807–15.
43. Villard L, Romer A, Marincek N, et al. Cohort study of somatostatin-based radiopeptide therapy with [(90)Y-DOTA]-TOC versus [(90)Y-DOTA]-TOC plus [(177)Lu-DOTA]-TOC in neuroendocrine cancers. J Clin Oncol 2012;30:1100–6.
44. Trotter JF, Everson GT. Benign focal lesions of the liver. Clin Liver Dis 2001;5:17–42, v.
45. Nguyen KT, Gamblin TC, Geller DA. World review of laparoscopic liver resection-2,804 patients. Ann Surg 2009;250:831–41.
46. Ferraz AA, Sette MJ, Maia M, et al. Liver transplant for the treatment of giant hepatic hemangioma. Liver Transpl 2004;10:1436–7.
47. Farges O, Dokmak S. Malignant transformation of liver adenoma: an analysis of the literature. Dig Surg 2010;27:32–8.
48. Ichikawa T, Federle MP, Grazioli L, Nalesnik M. Hepatocel-lular adenoma: multiphasic CT and histopathologic fi nd-ings in 25 patients. Radiology 2000;214:861–8.
49. Aseni P, Sansalone CV, Sammartino C, et al. Rapid dis-appearance of hepatic adenoma after contraceptive withdrawal. J Clin Gastroenterol 2001;33:234–6.
50. Bioulac-Sage P, Laumonier H, Laurent C, et al. Hepatocel-lular adenoma: what is new in 2008. Hepatol Int 2008;2:316–21.
51. Vennarecci G, Santoro R, Antonini M, et al. Liver transplan-tation for recurrent hepatic adenoma. World J Hepatol 2013;5:145–8.
52. Carrim ZI, Murchison JT. The prevalence of simple renal and hepatic cysts detected by spiral computed tomography. Clin Radiol 2003;58:626–9.
53. Iemoto Y, Kondo Y, Nakano T, et al. Biliary cystadenocarci-noma diagnosed by liver biopsy performed under ultraso-nographic guidance. Gastroenterology 1983;84:399–403.
54. Barthet M, Garcia T, Payan MJ, et al. Biliary cystadenocar-cinoma: a rare tumor of the liver. Dig Surg 1992;9:285–7.
55. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2012;62:10–29.
56. Lazaridis KN, Gores GJ. Cholangiocarcinoma. Gastroenter-ology 2005;128:1655–67.
57. Nakeeb A, Pitt HA, Sohn TA, et al. Cholangiocarcinoma. A spectrum of intrahepatic, perihilar, and distal tumors. Ann Surg 1996;224:463–73; discussion 73–5.
58. DeWitt J, Misra VL, Leblanc JK, et al. EUS-guided FNA of proximal biliary strictures after negative ERCP brush cytology results. Gastrointest Endosc 2006;64:325–33.
59. Clary B, Jarnigan W, Pitt H, et al. Hilar cholangiocarcinoma. J Gastrointest Surg 2004;8:298–302.
60. Jarnagin WR, Fong Y, DeMatteo RP, et al. Staging, resecta-bility, and outcome in 225 patients with hilar cholangiocar-cinoma. Ann Surg 2001;234:507–17.
61. Valle J, Wasan H, Palmer DH, et al. Cisplatin plus gem-citabine versus gemcitabine for biliary tract cancer. N Engl J Med 2010;362:1273–81.
62. DeOliveira ML, Cunningham SC, Cameron JL, et al. Cholangiocarcinoma: thirty-one-year experience with 564 patients at a single institution. Ann Surg 2007;245:755–62.
63. Zoepf T, Jakobs R, Arnold JC, et al. Palliation of nonresect-able bile duct cancer: improved survival after photody-namic therapy. Am J Gastroenterol 2005;100:2426–30.
64. Hemming AW, Reed AI, Fujita S, et al. Surgical manage-ment of hilar cholangiocarcinoma. Ann Surg 2005;241:693–9; discussion 9–702.
65. Singhal D, van Gulik TM, Gouma DJ. Palliative manage-ment of hilar cholangiocarcinoma. Surg Oncol 2005;14:59–74.
66. Wistuba II, Gazdar AF. Gallbladder cancer: lessons from a rare tumour. Nat Rev Cancer 2004;4:695–706.
67. Misra S, Chaturvedi A, Misra NC, Sharma ID. Carcinoma of the gallbladder. Lancet Oncol 2003;4:167–76.
68. Schnelldorfer T. Porcelain gallbladder: a benign process or concern for malignancy? J Gastrointest Surg 2013;17:1161–8.
69. Elnemr A, Ohta T, Kayahara M, et al. Anomalous pancre-aticobiliary ductal junction without bile duct dilatation in gallbladder cancer. Hepatogastroenterology 2001;48:382–6.
70. Sato M, Ishida H, Konno K, et al. Localized gallbladder carcinoma: sonographic fi ndings. Abdom Imaging 2001;26:619–22.
71. Wakai T, Shirai Y, Yokoyama N, et al. Early gallbladder carcinoma does not warrant radical resection. Br J Surg 2001;88:675–8.
72. Downing SR, Cadogan KA, Ortega G, et al. Early-stage gallbladder cancer in the Surveillance, Epidemiology, and End Results database: effect of extended surgical resection. Arch Surg 2011;146:734–8.
73. Abramson MA, Pandharipande P, Ruan D, et al. Radical resection for T1b gallbladder cancer: a decision analysis. HPB 2009;11:656–63.
74. Bartlett DL, Fong Y, Fortner JG, et al. Long-term results after resection for gallbladder cancer. Implications for staging and management. Ann Surg 1996;224:639–46.
75. Ito H, Matros E, Brooks DC, et al. Treatment outcomes associated with surgery for gallbladder cancer: a 20-year experience. J Gastrointest Surg 2004;8:183–90.
76. Fong Y, Jarnagin W, Blumgart LH. Gallbladder cancer: comparison of patients presenting initially for defi nitive operation with those presenting after prior noncurative intervention. Ann Surg 2000;232:557–69.
77. Chijiiwa K, Noshiro H, Nakano K, et al. Role of surgery for gallbladder carcinoma with special reference to lymph node metastasis and stage using western and Japanese classifi ca-tion systems. World J Surg 2000;24:1271–6; discussion 7.
Scientific American Surgery

01/14
gastro tumors of the liver and biliary tract — 27
78. Choi SB, Han HJ, Kim CY, et al. Incidental gallbladder cancer diagnosed following laparoscopic cholecystectomy. World J Surg 2009;33:2657–63.
79. Shoup M, Fong Y. Surgical indications and extent of resec-tion in gallbladder cancer. Surg Oncol Clin North Am 2002;11:985–94.
80. Donohue JH, Stewart AK, Menck HR. The National Cancer Data Base report on carcinoma of the gallbladder, 1989–1995. Cancer 1998;83:2618–28.
81. Shen CM, Niu GC, Cui W, et al. The improvement of surgi-cal treatment for patients with gallbladder cancer: analysis of 208 consecutive cases over the past decade. J Gastrointest Surg 2012;16:2239–46.
82. Brunicardi FC, Anderson DK, Billiar TR, et al. Schwartz’s principles of surgery. 9th ed. New York (NY): McGraw-Hill Companies, Inc.; 2009.
83. National Comprehensive Cancer Network. Neuroendocrine tumors. v1.2013. Available at: http://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf (ac-cessed March 17, 2013).
Acknowledgments
Figure 1 Tom MooreFigures 5, 11, and 14 Christine KenneyFigure 9 Elizabeth Hayden
Scientific American Surgery