Tumori Neuroendocrini Percorsi...
35
Transcript of Tumori Neuroendocrini Percorsi...


Tumori NeuroendocriniPercorsi Diagnostico-Terapeutici
Dr. Renato CannizzaroSOC Gastroenterologia Oncologica
CRO IRCCS- Aviano

NEUROENDOCRINE TUMORS
• Neuroendocrine Tumors are ill-understood, enigmatic malignancies
• An increased clinical and pathological focus as well as the advent of biochemical and immunohistochemical diagnostic technology has led to a greater awareness of the disease


MEN I • NETs may occur as part of multiple endocrine
neoplasia type 1 (MEN1), • An autosomal dominant disorder associated
with the gene locus MEN1 located on 11q13. • Its protein product (menin) is involved in
transcriptional regulation and genome stability.

CLINICAL PICTURES
• Primary GEP-NETs can be:– Asymptomatic – May present with obstructive symptoms (pain, nausea,
and vomiting)– The syndromes are typically seen in patients with
secretory tumours.

BIOCHEMICAL TESTS INNEUROENDOCRINE TUMORS
Specific• 24h urinary 5-HIAA • S-Gastrin• S-Insulin• S- C-peptide• S- Pro-insulin• S-VIP• S-Glucagons• S-Somatostatin
Generalised• Cromogranin A,B,C• Pancreatic polypeptide • β-HCG

DIAGNOSTICA DELLE NEOPLASIE NEUROENDOCRINE GEPDiagnostica strumentale
• TAC spirale• Scintigrafia con analoghi marcati della
somatostatina (Octreoscan)• Endoscopia e Ecoendoscopia (EUS)• Risonanza Magnetica • PET/CT• DOTATOC• Enteroscopia con videocapsula• Enteroscopia S/DB• Endomicroscopia

Tumori Neuroendocrini
Totale pazienti:
178 (92F, 86 M)
Età media: 59 anni (22-88)
Sede NET N°Tumori %Stomaco 36 18.4Ileo 34 17.3Pancreas 28 14.3Fegato 23 11.7Retto 22 11.2Colon 11 5.6Duodeno 11 5.6Digiuno 9 4.6Polmone 6 3.1Intestino 3 1.5Appendice 1 0.4Colecisti 1 0.4Sigma 1 0.4Tenue 1 0.4N.S. 10 5.1TOTALE 196* 100* Alcuni pazienti riportano NET in più sedi.
Casistica raccolta nel periodo 2003-2014 presso la S.O.C. di Gastroenterologia Oncologica del CRO
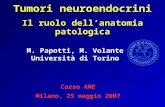
Tumore neuroendocrino del cardias
• M, 69 anni• Disfagia• Metastasi epatiche

Tumore neuroendocrino del bulbo

Carcinoma neuroendocrino scarsamente differenziato

ENDOSCOPIA CAPSULARE DEL TENUE
Tumore neuroendocrino dell’ileo

Tumore neuroendocrino dell’ultima ansa ileale
• F, 38 anni• Dolenzia in fossa iliaca
dx• Emicolectomia dx con
resezione ultima ansa ileale
• Carcinoide con 2 lindonodi metastatici
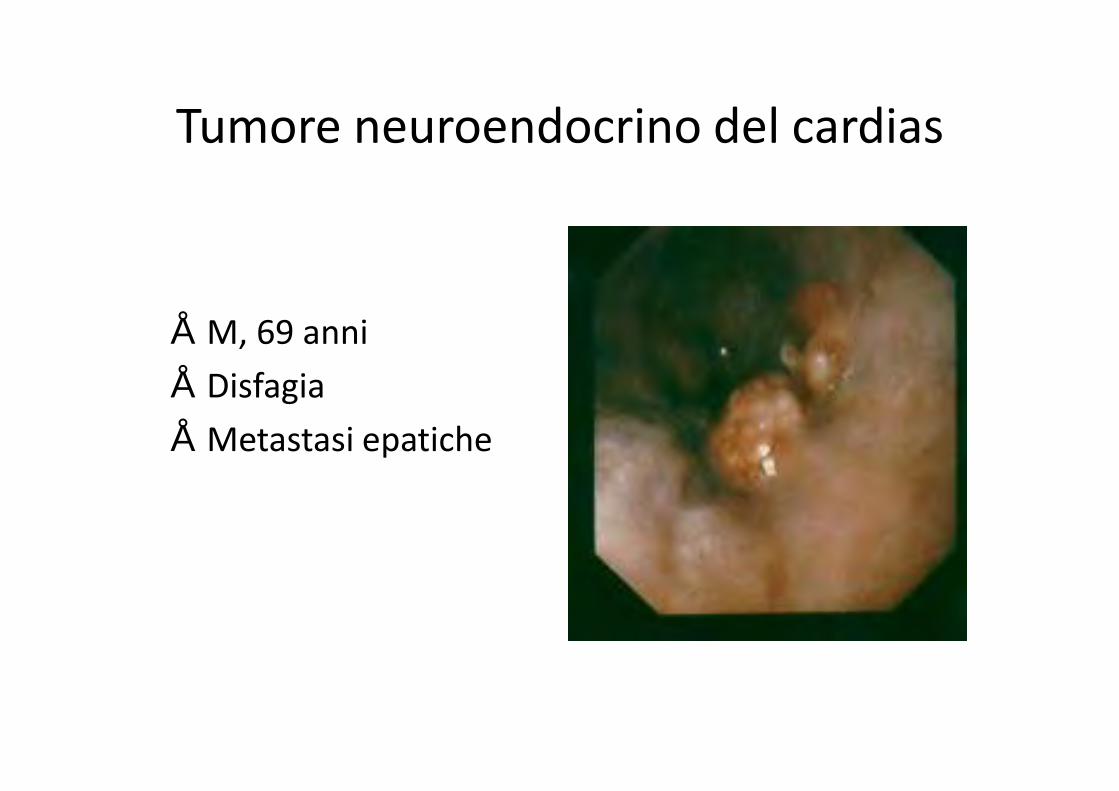
NET
• M, 41 anni• Alvo diarroico• Chirurgia: resezione ileale
laparoscopica• Tumore Neuroendocrino G1
cm 0.7• Il tumore infiltra lo strato
superficiale della tonaca muscolare
• 1 linfonodo metastatico su 13
• T2N1
Videocapsula
Enteroscopia
Minisonda
Minisonda

Mosaic reconstructions (A, B, and C) and images (a, a’, b, b’, and c) obtained with pCLE in a HGNEC (A, a and a’) and in two poorly differentiated adenocarcinoma patients (B, b, b’ and
C, c).

NEUROENDOCRINE TUMORSTREATMENT
The aim of treatment should be curative where possible but is palliative in the majority of cases.
These patients often maintain a good quality of life for a long period despite having metastases.
Although the rate of growth and malignancy are variable, the aim should always be to maintain a good quality of life for as long as possible.

NEUROENDOCRINE TUMORSTREATMENT
Endoscopy- SurgeryHormonal Therapy InterferonChemiotherapyEmbolisation of hepatic arteryLiver resectionLiver TransplantationNEW DRUGS

NEUROENDOCRINE TUMORS
SURGERYThis is the only curative treatment for NETs.
Conduct of surgery with intent to cure is dependent on the method of presentation and stage of disease.

TERAPIA ENDOSCOPICA
• Tumori neuroendocrini ben differenziati• Basso indice proliferativo• Dimensioni < 1 cm• Localizzati nella mucosa e/o nella sottomucosa
GI a livello di tutte le sedi raggiungibili da un endoscopio e quindi esofago, stomaco, duodeno, colonretto
• Intestino tenue

GASTRIC NET
World J Gastrointest Endosc 2011

DUODENAL NET
World J Gastrointest Endosc 2011

RECTAL NET
World J Gastrointest Endosc 2011

CARCINOIDI RETTALI
• Diametro massimo della lesione di 10 mm• Assenza di aree depresse od ulcerate sulla
lesione (valutazione endoscopica)• Non invasione della muscolare propria• Assenza di adenopatie loco-regionali (staging
EUS)

Resezione endoscopica a tutto spessore di NET rettale

October 2013 | Volume 8 | Issue 10 | e76462
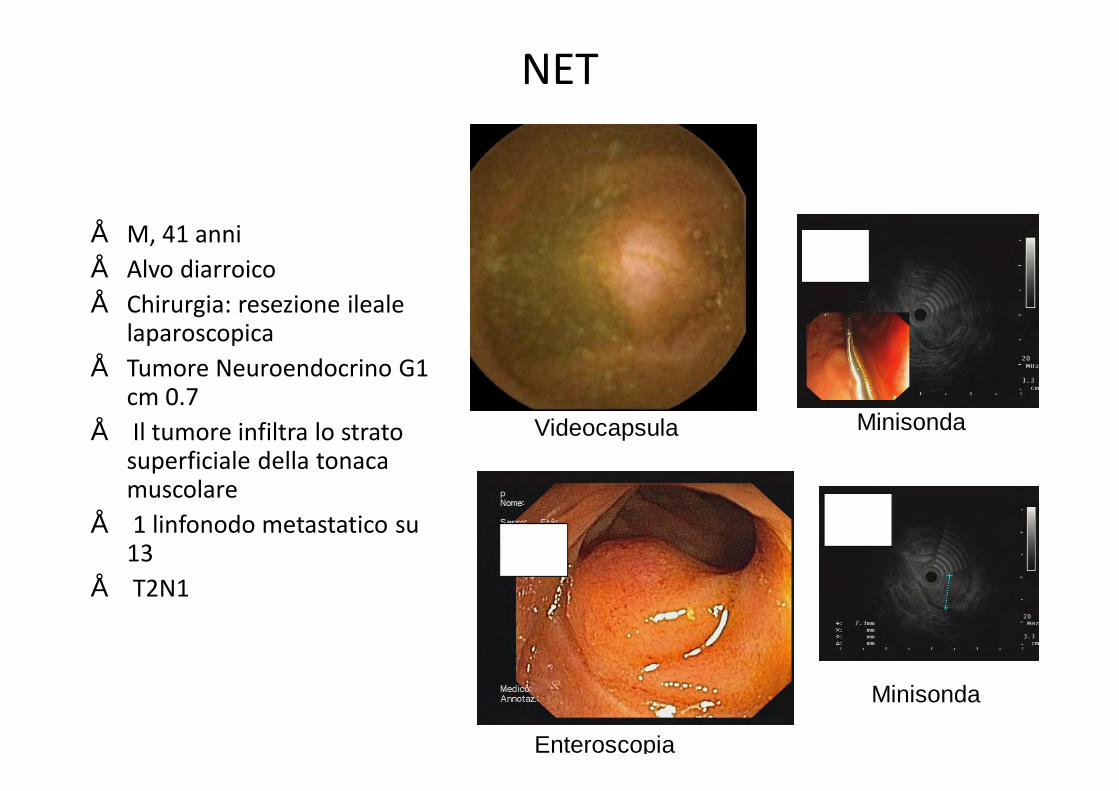
Netazepide (YF476) is a potent, highly selective and orally-active gastrin/CCK-2receptor antagonist.
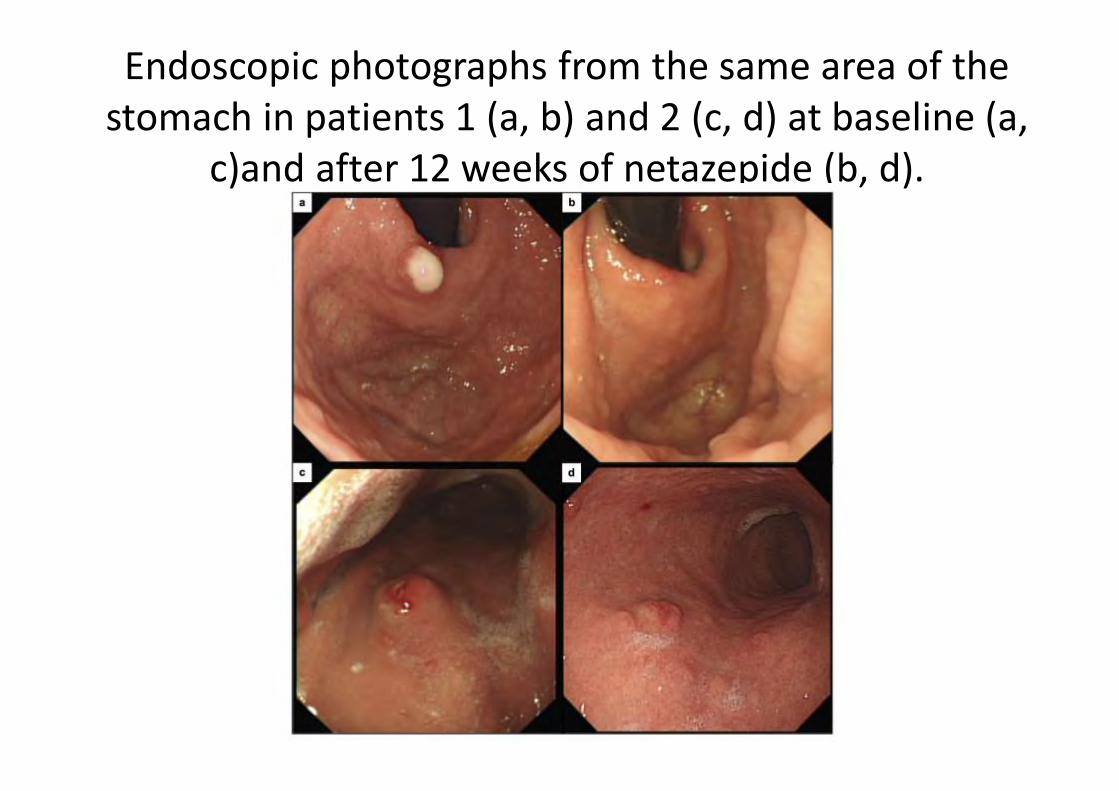
Endoscopic photographs from the same area of the stomach in patients 1 (a, b) and 2 (c, d) at baseline (a,
c)and after 12 weeks of netazepide (b, d).


29
Lo Studio PROMID
Octreotide LAR vs placebo P=0.000072HR= 0.34 [95% CI: 0.20–0.59]
Octreotide LAR: 42 pazienti / 26 eventiMediana 14.3 mesi [95% CI: 11.0–28.8]
Placebo: 43 pazienti / 40 eventiMediana 6.0 mesi [95% CI: 3.7–9.4]
Tempo (mesi)
Pro
porz
ione
sen
za p
rogr
essi
one
0
0.25
0.5
0.75
1
0 6 12 18 24 30 36 42 48 54 60 66 72 78
Rinke A, et al. J Clin Oncol 2009; 27: 4656-4663.

30

31
The CLARINET core study: key data from the primary publication
Caplin M., et al. Lanreotide in Metastatic EnteropancreaticNeuroendocrine Tumors. New Engl J Med 2014;371(3):224–33

32 Caplin M., et al. Lanreotide in Metastatic Enteropancreatic Neuroendocrine Tumors. New Engl J Med 2014;371(3):224–33
CLARINET®
Screening12–24 weeks Lanreotide Autogel 120 mg every 28 days (s.c.)
Study aim and designA
im • To compare effect of lanreotide Autogel 120 mg vs. placebo on PFS in non-functioning enteropancreatic NETs
• International randomized double-blind placebo-controlled phase 3 study D
esig
n
Study visits (weeks)
24 48 72 961 (Baseline)
36 12
Placebo every 28 days (s.c.)CT/MRI scan 1
CT/MRI scan 2
1:1 randomization
*ClinicalTrials.gov NCT00353496; EudraCT 2005-004904-35. PFS, progression-free survival; s.c., subcutaneous.
CLARINET(Controlled study of Lanreotide Antiproliferative Response In NET)*

33 Caplin M., et al. Lanreotide in Metastatic Enteropancreatic Neuroendocrine Tumors. New Engl J Med 2014;371(3):224–33
CLARINET®
Patient disposition
101 received lanreotide Autogel120 mg 103 received placebo
53 completed the study without events
26 completed the study without events
21 withdrawals9 due to investigator decision
(PD)3 due to AEs 5 withdrew consent2 protocol violations2 other reasons
18 withdrawals6 due to investigator decision
(PD)3 due to AEs 3 withdrew consent2 protocol violations4 other reasons
Events*: 30 PD (centrally assessed) and 2 deaths
Events*: 58 PD (centrally assessed) and 2 deaths
204 patients randomly allocated
*Two deaths occurred in lanreotide group after withdrawal for another reason and two deaths occurred and two PDs detected in placebo group after withdrawal for another reason; †despite a central assessment of PD. AEs, adverse events.

34 Caplin M., et al. Lanreotide in Metastatic Enteropancreatic Neuroendocrine Tumors. New Engl J Med 2014;371(3):224–33
CLARINET®
PFS (primary endpoint): significantly prolonged with lanreotideAutogel 120 mg vs. placebo
with 53% risk reduction of disease progression or death with Somatuline120mg versus placebo
Data are from the ITT population. P-value derived from stratified log-rank test; HR derived from Cox proportional hazards model. HR, hazard ratio; ITT, intention-to-treat.
Lanreotide Autogel 120 mg32 events/101 patientsmedian, not reached during the 24 months
Placebo60 events/103 patientsmedian, 18.0 months [95% CI: 12.1, 24.0]
Lanreotide Autogel 120 mg vs. placebop<0.001 HR=0.47 [95% CI: 0.30, 0.73]
Pat
ient
s al
ive
and
with
no
prog
ress
ion
(%)
0 3 6 9 12 18 24 270
10
20
30
40
50
60
70
80
90
100
Time (months)
101 94 84 78 71 61103 101 87 76 59 43
40Numbers of patients at risk of death or PD
26 00
65% at 24 months
33% at 24 months

C.R.O. AVIANOIstituto Nazionale Tumori