Tumor Proportion Score (TPS): 81.5% PD-L1 High
4
303.974.7580 | 7575 W. 103 rd Ave., #102. | Westminster, CO 80021 | flagshipbio.com CLIA 06D2058865 | CAP 8860624 | Roberto Gianani, MD, FACP, Medical Director © 2019 Ordered By: Washington University Patient ID: R359A12T Date: June 20, 2020 Results Figure 1: Native image Diagnosis: NSCLC Histologic Subtype: Adenocarcinoma Stain: DAKO PharmDx 22c3 Electronic Signature Dr. XXXXXXX 12-Jul-2019 Expression Level TPS Staining Pattern Negative for PD-L1 Expression <1% Partial or complete cell membrane staining (≥ 1+) in < 1% of viable tumor cells Low PD-L1 Expression 1–49% Partial or complete cell membrane staining (≥ 1+) in <1-49% of viable tumor cells High PD-L1 Expression ≥50% Partial or complete cell membrane staining (≥ 1+) in ≥50% of viable tumor cells Table 1: Scoring Interpretation for 22C3 PD-L1 staining in NSCLC Abbreviations: TPS; Tumor Proportion Score, NSCLC; Non-small cell lung cancer Figure 2: Markup image where red objects denote a PD- L1 positive tumor cell and blue objects denote a PD-L1 negative tumor cell Tumor Proportion Score (TPS): 81.5% Interpretation: PD-L1 High Analysis PD-L1 protein expression as measured by the 22C3 assay in non-small cell lung cancer (NSCLC) is determined using the Tumor Proportion Score (TPS), which is the percentage of viable tumor cells showing partial or complete membrane staining at any intensity. Pembrolizumab is approved as a single agent for first-line treatment of patients with Stage III NSCLC, who are not candidates for surgical resection or definitive chemoradiation, or metastatic NSCLC, and whose tumors express PD-L1 (TPS >= 1%) as determined by PD-L1 22C3 immunohisochemistry, with no EGFR or ALK genomic tumor aberrations. Pembrolizumab is approved in combination with pemetrexed and platinum chemotherapy, as first-line treatment of patients with metastatic nonsquamous NSCLC with no EGFR or ALK genomic tumor aberrations. Pembrolizumab is approved in combination with carboplatin and either paclitaxel or paclitaxel protein-bound, as first-line treatment of patients with metastatic squamous NSCLC. PD-L1 Analysis
Transcript of Tumor Proportion Score (TPS): 81.5% PD-L1 High

303.974.7580 | 7575 W. 103rd Ave., #102. | Westminster, CO 80021 | flagshipbio.comCLIA 06D2058865 | CAP 8860624 | Roberto Gianani, MD, FACP, Medical Director © 2019
Ordered By: Washington UniversityPatient ID: R359A12TDate: June 20, 2020
Results
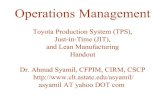
Figure 1: Native image
Diagnosis: NSCLC Histologic Subtype: AdenocarcinomaStain: DAKO PharmDx 22c3
Electronic SignatureDr. XXXXXXX12-Jul-2019
Expression Level TPS Staining Pattern
Negative for PD-L1 Expression <1% Partial or complete cell membrane staining (≥ 1+) in < 1% of viable tumor cells
Low PD-L1 Expression 1–49% Partial or complete cell membrane staining (≥ 1+) in <1-49% of
viable tumor cells
High PD-L1 Expression ≥50% Partial or complete cell membrane staining (≥ 1+) in ≥50% of viable tumor cells
Table 1: Scoring Interpretation for 22C3 PD-L1 staining in NSCLC
Abbreviations: TPS; Tumor Proportion Score, NSCLC; Non-small cell lung cancer
Figure 2: Markup image where red objects denote a PD-L1 positive tumor cell and blue objects denote a PD-L1 negative tumor cell
Tumor Proportion Score (TPS): 81.5%Interpretation: PD-L1 High
Analysis
PD-L1 protein expression as measured by the 22C3 assay in non-small cell lung cancer (NSCLC) is determined using the Tumor Proportion Score (TPS), which is the percentage of viable tumor cells showing partial or complete membrane staining at any intensity.
Pembrolizumab is approved as a single agent for first-line treatment of patients with Stage III NSCLC, who are not candidates for surgical resection or definitive chemoradiation, or metastatic NSCLC, and whose tumors express PD-L1 (TPS >= 1%) as determined by PD-L1 22C3 immunohisochemistry, with no EGFR or ALK genomic tumor aberrations.
Pembrolizumab is approved in combination with pemetrexed and platinum chemotherapy, as first-line treatment of patients with metastatic nonsquamousNSCLC with no EGFR or ALK genomic tumor aberrations. Pembrolizumab is approved in combination with carboplatin and either paclitaxel or paclitaxel protein-bound, as first-line treatment of patients with metastatic squamous NSCLC.
PD-L1 Analysis

303.974.7580 | 7575 W. 103rd Ave., #102. | Westminster, CO 80021 | flagshipbio.comCLIA 06D2058865 | CAP 8860624 | Roberto Gianani, MD, FACP, Medical Director © 2019
TME AnalysisResearch Use Only

303.974.7580 | 7575 W. 103rd Ave., #102. | Westminster, CO 80021 | flagshipbio.comCLIA 06D2058865 | CAP 8860624 | Roberto Gianani, MD, FACP, Medical Director © 2019
PD-L1 As a Diagnostic and Therapeutic Target
The cell membrane ligand Programmed Death Ligand 1 (PD-L1) is overexpressed in many tumor types, including colorectal, lung, breast, and bladder cancers. PD-L1 binds to its receptor PD-1, expressed on the surface of host immune T-cells. Besides tumor cell overexpression, PD-L1 can be expressed on hematopoietic cells, including T and B lymphocytes, macrophages, dendritic cells, and mast cells. Binding of PD-L1 to PD-1 inhibits T-cells from recognizing the tumor cells as foreign, allowing the tumor to evade the host immune system. Given this interaction, immunotherapy blockade of the PD-L1:PD-1 immune checkpoint has been shown to be an effective therapy in cancer treatment. Blocking of PD-L1:PD-1 binding restores host immune response and can be effective as a monotherapy or in combination with other therapeutic agents. Multiple drugs targeting PD-L1 or PD-1 have been approved by the FDA1, with many other monotherapy or combination therapies currently in various stages of clinical trials.
The Companion Assay Strategy
Companion IHC diagnostics are antibody clones developed to be diagnostics specific to which drug is used, i.e. Dako 28-8 for Nivolumab, Dako 22C3 for Pembrolizumab, Roche/Ventana SP142 for Atezolizumab, and Roche/Ventana SP263 for Durvalumab. Each companion diagnostic is evaluated differently based on which drug, indication, and line of therapy is considered for treatment2 (Table 1). According to FDA guidelines, each companion diagnostic must be run on the autostainer platform specific to the developed the diagnostic.
Table 1: List of Approved PD-L1 Checkpoint Inhibitors and Diagnostics*
Drug Diagnostic Indication Opdivo 28-8 (Dako pharmDx) UC, NSCLC, HNSCC Keytruda 22C3 (Dako pharmDx) UC, NSCLC, HNSCC, GC, ESCC, CC Imfinzi 73-10 (Dako pharmDx) UC Tecentriq SP142 (Roche Ventana) UC, NSCLC, TNBC, SCLC Bavencio SP263 (Roche Ventana) UC
*Not necessarily exhaustive. UC = Urothelial Carcinoma, HNSCC = Head and Neck Squamous Cell Carcinoma, GC = Gastric Cancer, ESCC = Esophageal Squamous Cell Carcinoma, CC = Cervical Cancer, TNBC = Triple-Negative Breast Cancer, SCLC = Small Cell Lung Cancer
Optimizing the PD-L1 Paradigm for Patient Selection Using Image Analysis
Diagnostic scoring parameters and cutoffs of positivity are established during the co-development of a drug and its companion diagnostic assay. These scoring paradigms have been developed based on response profiles and pathologist ability to reproduce assay scoring criteria3. As more patients are evaluated with the described methods of diagnosis it is important to consider other hallmarks of PD-L1 expression, such as immune cell subtypes, PD-L1 status, and tumor content. Continuous monitoring of additional endpoints can contribute to new paradigms which show a higher benefit to the selection of patients that will respond to anti-PD1 or anti-PD-L1 therapy.
Considering the Immune Cell And Microenvironmental Landscape in PD-L1 Assessments
Previously established PD-L1 scoring paradigms can consider expression of PD-L1 in the tumor cells, immune cells, or all of these in combination. Patient improvements upon treatment with PD-L1 therapy have shown correlation with both tumor and immune cell PD-L1 expression4. Additional guidance on PD-L1 evaluation can include instructions to the pathologist to consider lymphocyte and macrophage expression in addition to the broadly described immune cell expression5. The importance of evaluating immune cell subtypes when assessing PD-L1 is becoming more clear as the knowledge of immune checkpoints expands, however the growing field of knowledge is creating a challenging situation for pathologists to consider all of these parameters at the point of tissue evaluation. The image analysis solution that reduces pathologist burden while integrating the pathologist in to review is thus critical to stay current with the evolving literature on PD-L1 in tumors6.
PD-L1 Expression on Lymphocytes
While most previous literature has focused on the interaction between tumor-expressed PD-L1 and immune cell PD-1, new findings support the notion that immune cell expression of PD-L1 can also be a prognostic indicator of response or survival. In general, T cells which express PD-L1 provide an additional source of PD-L1 mediated immunosuppression in addition to tumor cell PD-L1. Recent literature is investigating the role of immune cell PD-L1 and evidence is building that immune cell PD-L1 cannot be ignored in favor of tumor cell evaluations alone.
Evidence in NSCLC studies have shown therapeutic benefit of PD-1 checkpoint inhibition in patients with either tumor cell or immune cell PD-L1 expression, indicating a non-redundant role of PD-L1 expression in either population. One NSCLC study in particular demonstrates a critical role of immune cell PD-L1 as an indicator of pre-existing immunity and active immune suppression in the tumor microenvironment7. This study shows significant evidence that immune cell PD-L1 expression alone is a relevant biomarker for identifying patients that respond to Atezolizumab therapy. Tumors with PD-L1 expression on the immune cells showed a distinct molecular profile indicative of Treg-associated response.
TME AnalysisResearch Use Only

303.974.7580 | 7575 W. 103rd Ave., #102. | Westminster, CO 80021 | flagshipbio.comCLIA 06D2058865 | CAP 8860624 | Roberto Gianani, MD, FACP, Medical Director © 2019
In another study of a population of melanoma patients8, PD-L1 expression in the lymphocyte populations, especially T cells, showed correlation with altered immune climate which negatively impacted on patient outcomes. In this study, PD-L1 expression in T cells showed significant correlation with a higher presence of Tregs, CTLA-4+ Tregs, dendritic cells, and high Kynurenine/Tryptophan ratio in serum. High kyn/trp ratios can indicate activity of Indoleamine 2,3-dioxygenase (IDO), itself a target of IO therapeutics such as IDO-1 inhibition. It was also demonstrated that higher levels of PD-L1 positive T cells were associated with a shorter time between patient sampling and relapse or death. Similar studies indicate PD-L1 expression on cytotoxic and helper T cells may be predictive biomarkers of resistance to CTLA-4 therapy.
PD-L1 Expression on Macrophages
As with the lymphocyte population, most previous literature assessing PD-L1 generally describes PD-L1 expression in ‘immune cells’ without attributing PD-L1 to a specific cellular subpopulation. Besides lymphocytes, another prominent immune cell expressor of PD-L1 is the macrophage population. Recent studies have begun to investigate PD-L1 expression in the macrophage population, and evidence is building that macrophage PD-L1 plays a very important role in patient response to PD-L1 checkpoint inhibition.
In a retrospective study examining PD-L1 expression on immune cell subtypes in PD-L1 checkpoint-treated and untreated NSCLC patients9, the majority of non-neoplastic cells found to express PD-L1 were the CD68 positive (general macrophage) cell population. PD-L1 was significantly higher in macrophages in both the tumor and stromal compartments as compared to other immune cells interrogated (lymphocytes, NK cells). Interestingly, high PD-L1 expression in macrophages correlated with high tumor PD-L1, as well as levels of CD8 and CD68. High PD-L1 expression in macrophages was correlated with a better overall survival in patients treated with single therapy PD-L1 checkpoint inhibitors (pembrolizumab, nivolumab, atezolizumab). Taken together, these data suggest macrophage expression of PD-L1 is indicative of overall immune cell activity and supports evidence that patients with immune-active tumors, rather than immune cell deserted/cold tumors tend to respond better to checkpoint inhibitors.
Another study in patients with primary testicular lymphoma supports mounting evidence that macrophage PD-L1 is associated with higher overall survival of patients in general. In this particular study, the PD-L1 status of macrophages, T-cells, and B-cells was measured via multiplexed immunostaining and measured against patient outcomes. The results of this study revealed a heterogeneous population of macrophages across all tumors, and tumors with high PD-L1 positive macrophages were a prevalent subpopulation. High infiltration of PD-L1 positive macrophages were significantly correlated with favorable overall patient survival, whereas the PD-L1 expression on tumor cells or all CD68 negative cells alone were not associated with favorable response. The proportion of PD-L1 positive macrophages to either all cells measured, or in the macrophage population itself were both significant indicators of overall survival.
References:
1. https://www.fda.gov/medical-devices/vitro-diagnostics/list-cleared-or-approved-companion-diagnostic-devices-vitro-and-imaging-tools 2. Torlakovic, E., Lim, H.J., Adam, J. et al. “Interchangeability” of PD-L1 immunohistochemistry assays: a meta-analysis of diagnostic accuracy. Mod Pathol
33, 4–17 (2020). doi:10.1038/s41379-019-0327-4 3. Kulangara K, Zhang N, Corigliano E, et al. Clinical Utility of the Combined Positive Score for Programmed Death Ligand-1 Expression and the Approval of
Pembrolizumab for Treatment of Gastric Cancer. Arch Pathol Lab Med. 2019;143(3):330-337. doi:10.5858/arpa.2018-0043-OA 4. Fehrenbacher L, Spira A, Ballinger M, et al. Atezolizumab versus docetaxel for patients with previously treated non-small-cell lung cancer (POPLAR): a
multicentre, open-label, phase 2 randomised controlled trial. Lancet. 2016;387(10030):1837-1846. doi:10.1016/S0140-6736(16)00587-0 5. PD-L1 IHC 22C3 pharmDx Interpretation Manual – NSCLC, Agilent Dako 6. ilva MA, Ryall KA, Wilm C, Caldara J, Grote HJ, et al. (2018) PD-L1 immunostaining scoring for non-small cell lung cancer based on immunosurveillance
parameters. PLOS ONE 13(6): e0196464. doi:10.1371/journal.pone.0196464 7. Kowanetz M, Zou W, Gettinger SN, et al. Differential regulation of PD-L1 expression by immune and tumor cells in NSCLC and the response to treatment
with atezolizumab (anti-PD-L1). Proc Natl Acad Sci U S A. 2018;115(43):E10119-E10126. doi:10.1073/pnas.1802166115 8. Brochez L, Meireson A, Chevolet I, Sundahl N, Ost P, Kruse V. Challenging PD-L1 expressing cytotoxic T cells as a predictor for response to
immunotherapy in melanoma. Nat Commun. 2018;9(1):2921. Published 2018 Jul 26. doi:10.1038/s41467-018-05047-1 9. Liu Y, Zugazagoitia J, Ahmed FS, et al. Immune Cell PD-L1 Colocalizes with Macrophages and Is Associated with Outcome in PD-1 Pathway Blockade
Therapy. Clin Cancer Res. 2020;26(4):970-977. doi:10.1158/1078-0432.CCR-19-1040 10. Pollari M, Brück O, Pellinen T, et al. PD-L1+ tumor-associated macrophages and PD-1+ tumor-infiltrating lymphocytes predict survival in primary
testicular lymphoma. Haematologica. 2018;103(11):1908-1914. doi:10.3324/haematol.2018.197194
TME AnalysisResearch Use Only