Tubulocystic epithelium
14
Kidney International, Vol. 39 (1991), pp. 450—463 Tubulocystic epithelium PATRICIA D. WILSON and ANN C. SHERWOOD Department of Physiology and Biophysics, UMDNJ—Robert Wood Johnson Medical School, Piscataway, New Jersey, USA Pathology of human renal cystic disease There are several pathologic conditions in humans which result in tubulocystic enlargement in the kidney [1, 2]. In some cases, renal cystic development is genetically determined and maybe the primary disease event (Table 1). The most common example is autosomal dominant polycystic kidney disease (ADPKD) which is estimated to afflict 1 in 1000 live births [3]. Autosomal recessive polycystic kidney disease (RPKD) occurs less frequently (1 in 100,000 live births), but is more aggressive in its course since it is usually lethal to infants within their first year. Another significant inherited condition leading to renal tubule cyst formation is the nephronophthisis-medullary cystic disease complex, which has been described as an autosomal recessive trait in the juvenile form and autosomal dominant in the adult form of disease. Tubulocystic enlargement may also occur sporadically in association with hereditary syndromes, such as von-Hippel Lindau disease and tuberous sclerosis. In yet other cases, renal tubule cysts may develop in small or large numbers in response to non-genetic factors. For instance, simple cysts occur with increasing frequency with advancing age, but rarely compromise renal function. By contrast, ac- quired renal cystic disease, which affects approximately 40% of non-ADPKD patients receiving hemodialysis for end-stage re- nal failure, may result in the development of multiple cysts [4]. Additional reports have described renal cysts after long-term administration of lithium chloride [5] and exposure to diphenyl- amine [6]. A renal tubule cyst is defined as a segment of the nephron enlarged to a diameter of 200 microns or more, and consists of a fluid-filled, distended sac lined by a single layer of epithelium. It would seem from the pattern of occurrence in humans and from experimental studies in animals and tissue culture, that renal tubule cysts can form in response to genetic, non-genetic and toxic influences. Although there is a common end prod- uct—a tubulocystic epithelium lining a fluid-filled expanded lumen—it maybe spurious to consider that the mechanism(s) of cyst formation are necessarily identical in all cases. Conceptu- ally, it seems more likely that several pathogenetic pathways converge on a single means of phenotypic expression. The following discussion will center on what little is known about the cell biology and underlying mechanisms governing cyst formation in human genetic polycystic kidney diseases (ADPKD, RPKD), but will draw occasionally on results ob- tained from some appropriate experimental models (Table 2), © 1991 by the International Society of Nephrology when parallels or contrasts have bearing on studies in human tissues. RPKD is a rare but lethal form of polycystic kidney disease. It occurs with an estimated frequency of 1 in 10,000 and typically children are born with enlarged, malfunctioning, mul- ticystic kidneys. For these reasons, this form of disease has been studied rarely, but recently a mutant mouse strain C57/6J (cpk) has been characterized and shown to represent an excel- lent animal model for this disease [7, 8]. This fortunate circum- stance does not apply to the more common ADPKD, which affects approximately 500,000 people in United States. No known animal model has been characterized. This disease typically shows a slow progression in which renal cysts increase in number and size, gradually replacing normal renal tubule mass and leading to renal insufficiency in the fourth decade of life, although symptoms of reduced ability to concentrate the urine and hypertension often precede loss of renal function [9, 10]. Classical, pioneering microdissection studies of ADPKD kidneys in the early stages of development of the disease showed that cysts can arise as focal dilations originating from any proximal or distal segment of the nephron [11—13]. This was later confirmed by discriminatory lectin staining patterns [14]. In addition, ion and pH analysis of cyst fluid aspirated from ADPKD kidneys had shown wide variations and led to the broad classification of two types of cysts, designated "proxi- mal" and "distal" [15—171. Macroscopic examination of end- stage ADPKD kidneys shows that cyst enlargement is asyn- chronous and can reach enormous proportions. Cyst size commonly ranges < 1 mm to > 10 cm. This contrasts with RPKD where cysts derive exclusively from distal collecting tubules, and cysts are smaller and more homogeneous in size. The genes responsible for ADPKD and RPKD have not yet been isolated, although a major ADPKD gene (ADPKD-1) is known to be linked to a highly polymorphic marker on the short arm of chromosome 16 [18]. However, it appears that in approximately 10% of cases of ADPKD, the gene on chromo- some 16 is not responsible, since families with inheritance of ADPKD unlinked to the 3'HVR region of the a-globin locus have now been found in United States and in Europe [19—21]. The apparent existence of a minimum of two alleles for ADPKD has not only complicated certainty of diagnosis, but unfortu- nately increases the complexity of the task of isolating and characterizing this genetic defect at the molecular level. How- ever, significant progress has been made by several laboratories towards this goal. Progress has also been made at the cellular level. Light and electron microscopy of human ADPKD kidneys shows that 450
Transcript of Tubulocystic epithelium

Kidney International, Vol. 39 (1991), pp. 450—463
Tubulocystic epitheliumPATRICIA D. WILSON and ANN C. SHERWOOD
Department of Physiology and Biophysics, UMDNJ—Robert Wood Johnson Medical School, Piscataway, New Jersey, USA
Pathology of human renal cystic disease
There are several pathologic conditions in humans whichresult in tubulocystic enlargement in the kidney [1, 2]. In somecases, renal cystic development is genetically determined andmaybe the primary disease event (Table 1). The most commonexample is autosomal dominant polycystic kidney disease(ADPKD) which is estimated to afflict 1 in 1000 live births [3].Autosomal recessive polycystic kidney disease (RPKD) occursless frequently (1 in 100,000 live births), but is more aggressivein its course since it is usually lethal to infants within their firstyear. Another significant inherited condition leading to renaltubule cyst formation is the nephronophthisis-medullary cysticdisease complex, which has been described as an autosomalrecessive trait in the juvenile form and autosomal dominant inthe adult form of disease. Tubulocystic enlargement may alsooccur sporadically in association with hereditary syndromes,such as von-Hippel Lindau disease and tuberous sclerosis. Inyet other cases, renal tubule cysts may develop in small or largenumbers in response to non-genetic factors. For instance,simple cysts occur with increasing frequency with advancingage, but rarely compromise renal function. By contrast, ac-quired renal cystic disease, which affects approximately 40% ofnon-ADPKD patients receiving hemodialysis for end-stage re-nal failure, may result in the development of multiple cysts [4].Additional reports have described renal cysts after long-termadministration of lithium chloride [5] and exposure to diphenyl-amine [6].
A renal tubule cyst is defined as a segment of the nephronenlarged to a diameter of 200 microns or more, and consists ofa fluid-filled, distended sac lined by a single layer of epithelium.It would seem from the pattern of occurrence in humans andfrom experimental studies in animals and tissue culture, thatrenal tubule cysts can form in response to genetic, non-geneticand toxic influences. Although there is a common end prod-uct—a tubulocystic epithelium lining a fluid-filled expandedlumen—it maybe spurious to consider that the mechanism(s) ofcyst formation are necessarily identical in all cases. Conceptu-ally, it seems more likely that several pathogenetic pathwaysconverge on a single means of phenotypic expression. Thefollowing discussion will center on what little is known aboutthe cell biology and underlying mechanisms governing cystformation in human genetic polycystic kidney diseases(ADPKD, RPKD), but will draw occasionally on results ob-tained from some appropriate experimental models (Table 2),
© 1991 by the International Society of Nephrology
when parallels or contrasts have bearing on studies in humantissues.
RPKD is a rare but lethal form of polycystic kidney disease.It occurs with an estimated frequency of 1 in 10,000 andtypically children are born with enlarged, malfunctioning, mul-ticystic kidneys. For these reasons, this form of disease hasbeen studied rarely, but recently a mutant mouse strain C57/6J(cpk) has been characterized and shown to represent an excel-lent animal model for this disease [7, 8]. This fortunate circum-stance does not apply to the more common ADPKD, whichaffects approximately 500,000 people in United States. Noknown animal model has been characterized. This diseasetypically shows a slow progression in which renal cysts increasein number and size, gradually replacing normal renal tubulemass and leading to renal insufficiency in the fourth decade oflife, although symptoms of reduced ability to concentrate theurine and hypertension often precede loss of renal function [9,10]. Classical, pioneering microdissection studies of ADPKDkidneys in the early stages of development of the diseaseshowed that cysts can arise as focal dilations originating fromany proximal or distal segment of the nephron [11—13]. This waslater confirmed by discriminatory lectin staining patterns [14].In addition, ion and pH analysis of cyst fluid aspirated fromADPKD kidneys had shown wide variations and led to thebroad classification of two types of cysts, designated "proxi-mal" and "distal" [15—171. Macroscopic examination of end-stage ADPKD kidneys shows that cyst enlargement is asyn-chronous and can reach enormous proportions. Cyst sizecommonly ranges < 1 mm to > 10 cm. This contrasts withRPKD where cysts derive exclusively from distal collectingtubules, and cysts are smaller and more homogeneous in size.
The genes responsible for ADPKD and RPKD have not yetbeen isolated, although a major ADPKD gene (ADPKD-1) isknown to be linked to a highly polymorphic marker on the shortarm of chromosome 16 [18]. However, it appears that inapproximately 10% of cases of ADPKD, the gene on chromo-some 16 is not responsible, since families with inheritance ofADPKD unlinked to the 3'HVR region of the a-globin locushave now been found in United States and in Europe [19—21].The apparent existence of a minimum of two alleles for ADPKDhas not only complicated certainty of diagnosis, but unfortu-nately increases the complexity of the task of isolating andcharacterizing this genetic defect at the molecular level. How-ever, significant progress has been made by several laboratoriestowards this goal.
Progress has also been made at the cellular level. Light andelectron microscopy of human ADPKD kidneys shows that
450

Wilson and Sherwood: Tubulocyslic epithelium 451
Table 1. Renal tubular cystic disease
Disease entity Causative factors Reference
Autosomal dominant Genetic: gene 1, on [3, 18]polycystic chromosome 16kidney disease gene 2, unknown [191(ADPKD)
Autosomal recessive Genetic: gene and [1]polycystic kidney chromosomedisease (RPKD) unknown
Polycystic kidney Genetic: autosomal [1]disease: medullary dominanttype
Juvenile Genetic: autosomal [11
nephronophthisis recessiveAcquired renal Dialysis, drugs [4, 5]
cystic diseaseSimple cysts Advancing age [3]von-Hippel Lindau Associated with [21
disease hereditary(cerebroretinal syndromeangiomatosis)
Tuberous sclerosis Associated with [21(Bouneville' s hereditarydisease) syndrome
Table 2. Experimental models of renal cystic disease
TubuleCausative agent affected Species Reference
In VivoGenetic CT Cpk mouse [7, 81Drugs: diphenyl CT Rat [321
thiazolephenol II CT Rat [591
Corticoids CT Rat, rabbit, [168]hamster
In VitroMetanephric PT Mouse [124]
organ culture,hydrocortisone
Monolayer PT,TAL,CT Human [231ADPKDepithelia
Explant ADPKD PT,TAL,CT Human [281epithelia
Monolayer RPKD CT Human [169]epithelia
Monolayer RPKD CT Mouse [1701epithelia
MDCK cell line in "Distal" Dog [1711collagen gel
Abbreviations are: PT, proximal tubule; CT, collecting tubule; andTAL, thick ascending limb of Henle's loop.
cysts are lined by a single layer of polarized epithelium, inwhich rudimentary microvilli and intercellular tight junctionsline the apical cell surface at the lumenal aspect of the epithelialsheet lining the cyst [22—24]. So few differentiated characteris-tics of the original tubule segment remain that it is usuallyimpossible, in fixed tissue slices, to determine the derivation ofcysts based solely on morphological characteristics. Even at afunctional level, isolated cystic epithelia have such dramaticallyaltered levels of marker enzyme activities and diminishedresponses to hormone induction that characterization is dif-ficult. However, these types of studies have provided insight
into certain ADPKD-associated symptoms. For instance, thelack of ability of arginine vasopressin (AVP) to stimulateadenylate cyclase in cyst lining epithelia [23], would help toexplain the concentrating defect which occurs early in ADPKDpatients. The mechanism of this modification is not caused by acomplete inability to increase cAMP levels in ADPKD epithe-ha, since forskolin and PGE2 generate a cAMP induction,although this was < 50% of the normal response [23, 25, 26].These observations suggest an additional pre-cAMP lesion atthe level of AVP-receptor interaction, and/or faulty transduc-tion of the signal via modified interactions with membrane Gproteins which act as the link between hormone-stimulatedreceptors and the catalytic subunit of adenylate cyclase. Apossible explanation of hypertension, another early symptom ofADPKD patients, has been suggested by studies at the cellularlevel. Using specific antibodies and tissue sections from 19cases of ADPKD using specific antibodies, both an increase innumber and an abnormal localization of renin-containing cellsimmunolocalization showed 50% of these cells were seen in thethin attenuated blood vessels that supply the walls of cysts, andothers were seen in the intervening in fibrous tissue [27].
Models of renal cystic disease
The morphological characterization of cyst lining cells assimple epithelia has been confirmed and is retained in tissueculture, both in flat, two-dimensional monolayers grown ondried collagen [23], and in three-dimensional explants embed-ded in collagen gels [28, 29]. Although the ADPKD epithelialcells contain relatively few organelles and are morphologicallyless specialized than renal proximal tubules, thick ascendinglimbs of Henle or collecting tubule cells in vivo or in vitro, theyremain polarized with apical tight junctions and microvillifacing upward in the dish. ADPKD epithelial are similar tonormal microdissected human renal tubules in vitro [29], intheir requirement for type 1 collagen or some other matrixprotein to establish this polarity. To confirm the validity ofprimary culture monolayers of microdissected human ADPKDcysts as a model system, a series of comparative studies wascarried out in freshly isolated human cysts and confluentcultures. Good correlations were seen between the levels ofmarker enzyme activities and adenylate responsiveness tohormones, which suggested the suitability of this primaryculture system as an in vitro model system for the analysis ofrenal cyst formation. Since these ADPKD epithelia grow easilyand rapidly in culture and can be maintained in primary culturefor up to six weeks or passaged for up to 15 transfers, thisprovides a practical, reliable and reproducible system for theanalysis of cellular alterations in ADPKD epithelia [23]. Theadvantages of viable epithelial monolayers are numerous andobvious, allowing for direct comparisons with similar epitheliaderived from normal renal proximal convoluted and straighttubules (PCT, PST), cortical and medullary thick ascendinglimbs of Henle's loop (cTAL, mTAL) and cortical and medul-lary collecting tubules (CCT, MCT) [25]. This is by no meansthe only model available for analysis of cyst formation, but isone of the few employing human-derived epithelia. Some othercommonly used model systems are listed in Table 2. Evaluationof every cellular model of cyst formation and its relevance tothe mechanisms underlying human cyst formation in ADPKDand RPKD is beyond the scope of this review.

452 Wilson and Sherwood: Tubulocystic epithelium
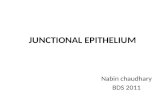
Fig. 1. Electron micrograph of a cyst lining epithelial cell from an ADPKD kidney, undergoing mitosis. Note the absence of a nuclear membraneand chromosome condensation. Organdies are distributed at the periphery. Fixation was 2.5% glutaraldehyde in 100 m sodium cacodylate buffercontaining 5% sucrose for 4 hours. x 3,360.
Theories of polycystic kidney disease
Over the years there have been several theories to explain thederivation of renal cysts. Originally the obstruction theory wasfavored [30]. This suggested that fluid accumulation was theresult of occlusion of the renal tubule at a point distal to theglomerulus, and thus a build-up of pressure resulted in cystformation. This theory has now been discounted since measure-ments of intracystic pressures are not sufficiently high toaccount for tubular distension [31]. Also, it has been demon-strated that the majority of cysts become isolated from theirnephron of origin as an early event and not late as thoughtpreviously.
This theory gave way to one of increased compliance of thecystic basement membrane. This still holds some sway as aunifying concept which could explain the systemic nature ofcyst development in several organs of patients with ADPKD[101. Major basement membrane alterations are seen in drug-induced cyst formation in rats [321, in cultured human ADPKDcells and in the later stages of dominant and recessive cysticdisease. However, measurements of compliance in acquiredand mouse ADPKD cysts were not consistent with increasedelasticity as the exclusive cause of cyst expansion [331.
This theory has now given way slightly to one favoring
hyperplasia. The presence of hyperplastic nodules in ADPKDcysts was originally reported by Evan, Gardner and Bernstein[34] and confirmed by others in ADPKD and cystic diseasesthat predispose to malignant transformation, such as von-Hippel Lindau disease [24]. Although the occurrence of hyper-plastic nodules is not sufficiently frequent or extensive toinvoke obstruction as a universal course of cyst formation,calculations of cell height and cyst size suggest that cell divisionmust occur during cyst enlargement [35]. This has been con-firmed by detection of mitotic profiles in cyst lining epithelial ofADPKD kidneys in vivo (Fig. 1). Mitotic figures have not beenseen in electron micrographs of normal human renal tubules.
To explain formation of cysts instead of solid tumors, theremust be an accompanying defect which results in fluid accumu-lation, presumably by secretion [36], since cysts have beenshown to close off from their nephron segment of origin earlyafter the onset of expansion. The ability of cysts to accumulatefluid very rapidly has been confirmed in vivo by injection of3H-water, the majority of which was detected in cyst fluids afterfive hours [371.
It can be concluded that whichever defective gene product isresponsible for ADPKD or RPKD, the two basic criterianecessary for cyst formation to occur are increased epithelial
S

a12 34 5678
Wilson and Sherwood: Tubulocystic epithelium 453
cell proliferation and altered fluid and transport. Alterations inthe proliferative potential of epithelia can be the result of:modified epithelial/stromal interactions; altered susceptibilitiesor synthesis of peptide growth factors; or abnormal expressionof growth related genes including protooncogenes. Renal fluidtransport is directed by electrochemical ion gradients estab-lished by the sodium pump and normally results in reabsorp-tion. Fluid accumulation in renal cysts could therefore be theresult of alterations in ion pumping or reflect alterations ofpolarity of cell structure and/or function. Evidence for each ofthese alterations will be considered.
The proliferative defect in tubulocystic epithelia
Matrix alterations
Stromal-epithelial interactions are of central importance inthe patterning of growth and differentiation in the developingkidney [381. Although the precise mechanisms involved are notfully understood, it is clear that the dynamic composition of theextracellular matrix is responsible, at least in part, for control ofall normal epithelial cell migration, spatial organization, prolif-eration and differentiation. It is therefore not surprising thatbasement membrane defects are commonly found in diseasesassociated with loss of normal cell division, including humantumors of the breast [391, ovary [401, and in chemical carcino-gen-induced rat mammary tumors [411. The structural defectsdescribed include thinning, attenuation, layering and thickeningof the basement membrane. Similar descriptions have beenreported for the basement alterations seen surrounding therenal medullary cysts of nephronophthisis [42], in pathologicalspecimens of human ADPKD [23, 43, 441, and in diphenyithia-zole-induced renal cystic disease in rats [45]. Thickening hasalso been described in renal aging and in diabetes [461.
In the kidney, as in all organs, the basement membraneseparates epithelia from the underlying interstitium and servesseveral functions, including cell adhesion, tensile strength andpermselectivity. Normal renal tubule basement membranes aremade up of type IV collagen, and the non-collagenous glyco-proteins laminin, entactin and heparan sulfate proteoglycans[reviewed in 47]. The interstitial components include types I, IIIand V collagen [48] and their relative abundance is develop-mentally regulated in the kidney [48, 49]. Morphological alter-ations in basement membranes in renal cysts could derive fromalterations in any of these extracellular matrix components andcould reflect defects in synthesis, post-translational modifica-tions, secretion, extracellular assembly or degradation. Studiesof the structural component of type IV collagen, and laminin B Iand B2 chains which influence adhesion, growth and differen-tiation in cpk mice, showed that steady state levels of mRNAswere altered with the progression of RPKD. There was, how-ever, no correlation between gene expression as determined byNorthern blot analysis and protein expression as measured byimmunofluorescence, since basement membrane staining be-came weaker and mRNA levels increased in endstage kidneys[50]. Our own findings have also shown that human ADPKDepithelia continue to synthesize immunoreactive laminin andtype IV collagen in vitro and in vivo [43, 44]. It is also of interestthat steady state levels of type IV collagen mRNAs increasedsignificantly in ADPKD, but not markedly until the final stagesof disease progression (Fig. 2, courtesy of Dr. J.T. Norman,
Fig. 2. Northern blot of total RNA probed with 32P-cDNA for type IVcollagen, (HT2I, Dr. D. Prockop, Jefferson, PA). Lanes 1 and 2,normal adult kidney; lanes 3 and 4 early stage ADPKD; lanes 5, 6, 7 and8 end-stage ADPKD kidney. Note increase in steady state levels of typeIV collagen mRNA, particularly in end-stage kidneys. Courtesy of Dr.iT. Norman, UCLA Division of Nephrology.
UCLA). Thus, alterations in the structural component of cysticbasement membranes may occur, but that as a late event isunlikely to be a primary change initiating cyst enlargement. Nochanges were found in type I collagen, laminin B 1 mRNA, orprotein expression.
More dramatic alterations were seen in the heparan sulfateproteoglycan (HSPG) component of cystic basement mem-branes. This integral component of the basement membraneconsists of a core protein with glycosaminoglycan (GAG) sidechains. These molecules can vary considerably in size in atissue specific fashion [5 1—53] but are thought to belong to asingle gene family. Proteoglycans have been assigned roles incell adhes4on [54], interstitial collagen and fibronectin binding[551, and cell proliferation [56—58]. In several cell systemsproteoglycans have been shown to inhibit cell proliferation. Inthis context it maybe important to note that both in drug-induced cystic development and in human ADPKD culturedepithelia, reduced structural integrity of the heparan sulfateproteoglycan component of basement membranes has beenreported [23, 45], and in both conditions this was associatedwith increased epithelial cell proliferation [23, 43, 44, 59].Despite a rapid incorporation of H2[35S04] into human ADPKDmonolayers, no complete basement membrane structure wassynthesized. Instead, ruthenium red positive spheroids weresecreted on the basal surfaces of confluent monolayers. Immu-noprecipitation studies in normal and ADPKD cultures in whichshort-term labelling with 35S-methionine was used as an indexof core protein synthesis, no differences were found (Fig. 3,courtesy Dr. J. Hassell, Pittsburgh). This suggests that alter-ations in HSPG synthesis does not occur at the level of proteinprecursor synthesis, but rather at a later step when sulfated sidechains (GAG) are inserted into the core protein. It remains to bedetermined whether the structural abnormality of ADPKDbasement membrane HSPG is due to inappropriate post-trans-lational processing or to differential degradation, presumablycontrolled by the action of extracellular proteases [60]. Thus, itis possible to speculate that a reduction in the integrity of thenormal spatial deposition of FISPG in the basement membranesof cystic epithelia could result in some loss of inhibition of cellproliferation.
Cell growth is under the control of several interactive intra-cellular and extracellular factors. An abnormality in cell growthcontrol, such as the limited hyperplasia seen in cyst formation,could be the result of abnormalities at any of these levels ofcontrol. Extracellular controlling factors fall into two catego-ries: insoluble and soluble. The former includes extracellularmatrix proteins as discussed above and the latter includespeptide growth factors.

— S S HSPG core— • LamininA
Laminin Bs200 — a
abcN p abc
454 Wilson and Sherwood: Tubulocystic epithelium
Fig. 3. Autoradiogram ofimmunoprecipitation of laminin A and Bchains (lane b) and HSPG core protein (lanec) in confluent cultures of normal proximaltubule (N) and ADPKD (P) epithelia. Cellswere labelled with 35S-methionine (1 mCi/mi)for 1 hour at 37°C. Lane a shows controlsamples incubated with pre-immune serum.Courtesy of Dr. J. Hassell, University ofPittsburgh, School of Medicine.
Growth factor abnormalitiesOrderly cell division depends on an exquisite coordination of
events that regulate the cell cycle during which cells progressfrom one mitosis to the next. During this cycle, cells initiated bya mitogenic stimulus pass through: a quiescent phase (G1),during which RNA and protein synthesis take place; followedby S phase, during which DNA synthesis takes place; and afterDNA replication has stopped, into G2 phase which culminatesin mitosis [61]. In the normal kidney, rapid cycling of prolifer-ating cells takes place during certain specific stages of fetalorganogenesis, but after epithelial cell differentiation into highlysegmented nephron units is complete, division stops and cellsremain in the prereplicative (G0) state. Thus, in normal adultkidneys, the mitotic index in renal tubules is very low (0.1%),reflecting the very low level of cell renewal. Renal tubule cellsare not, however, irrevocably "terminally" differentiated,since they can be stimulated to re-enter the cell cycle andcomplete several rounds of cell division in response to injury invivo or by the addition of serum or specific growth factors invitro [62—64].
Several factors act in concert to control epithelial cell prolif-eration including: interactions with specific extracellular matrixproteins [65]; the mitogenic influence of cell type specificsoluble growth factors; and the expression of cell cycle regu-lated genes [reviewed in 661. Certain growth factors are knownto act at specific stages of the cell cycle. For instance, platelet-derived growth factor (PDGF) and fibroblast growth factor(FGF) exert mitogenic effects on cells early in the cell cycle, atthe G0/G1 interface, and are thus termed competence factors."Entry" factors, such as epidermal growth factor (EGF) and
insulin act early in G1. Progression factors act later in G1 andinclude insulin-like growth factors (IGF-1, IGF-2) and glücocor-ticoids [67]. Switches in and out of G1 are thought to be themajor determinants of post-embryonic cell proliferation, andtherefore, defective control would lead to conditions such ashyperplasia.
Abnormal cell proliferation maybe the result of aberrantexpression of normal mitogenic pathways, the molecular medi-ators of which are a family of peptide growth factors thatcirculate in the blood or are released locally and interact withtarget cells through specific receptors. These types of growthfactors have three potential modes of action: endocrine, inwhich their action is analogous to that of hormones, in thatfactors released from a distant site exert effects on different celltypes in a remote target tissue, after circulation; paracrine, inwhich growth factors released from one cell type stimulateproliferation of different cell types nearby, without involvementof systemic circulation; and autocrine, in which growth factorsproduced by one cell type have direct mitogenic effects on thesame cell [68]. Since a prerequisite for growth factor response isoccupancy of specific cell surface receptors, an increasedresponse to normal mitogenic regulators in cystic hyperplasiacould simply be the result of increased receptor number oraffinity. Alternatively, since many growth factor receptorscontain tyrosine kinase activity, alterations in phosphorylationand/or alterations in cellular substrate may be crucial. Afterbinding to receptors, a cascade of events is initiated leading todiverse early cellular responses including increased phosphati-dylinositol turnover, expression of competence genes, activa-tion of phospholipase A2, changes in cell shape and ion changes

Wilson and Sherwood: Tubulocystic epithelium 455
[69]. The relationship between these alterations and the laterevent of stimulation of DNA synthesis is unclear.
Normal renal tubule epithelia possess receptors for a widevariety of growth factors and the kidney is itself, a rich sourcefor several growth factors [70]. Therefore, it is possible that inthe hyperplasia underlying cyst formation, there might beinappropriate growth factor and/or growth factor receptorexpression in the affected epithelia. Under normal conditions inthe kidney, there is a balance between mitogenic and inhibitorygrowth factors, which presumably normally favors inhibitionsince so little cell renewal takes place. An overexpression ofmitogenic growth factors or loss of sensitivity to inhibitoryfactors are therefore potential mechanisms underlying the inap-propriately increased epithelial proliferation in renal cyst en-largement.
Epidermal growth factor (EGF) is a 6.1 kD peptide, whichacts via interaction with a specific, high-affinity 170 kD receptorwhich possesses intrinsic tyrosine kinase activity [71, 721.Overexpression of EGF receptors has been demonstrated inseveral human cancers and tumorigenic cell lines [73—76] and inliver regeneration [77]. The normal adult kidney has beenshown to be a major source of EGF mRNA, although relativelylittle peptide is stored there [78]. Immunoreactivity for EGF hasbeen detected in distal tubule cells including thick ascendinglimbs, distal convoluted tubules, and medullary collecting tu-bules and EGF receptors are paradoxically present on thebasolateral membranes of proximal tubule cells. The normalrole of EGF in the kidney is unclear at present, but it has beenclearly demonstrated as a potent mitogen for primary culturesof rabbit proximal tubules and cortical collecting tubules [63,79] and for the proximal and distal tubule-derived cell lines,LLC-PK1 and MDCK [80, 81]. Since EGF had been detected inhuman breast cyst fluid, although virtually undetectable inplasma [82], we were prompted to examine the localization ofEGF and its receptor in ADPKD tissues and cultured cells. Themitogenic action of EGF was significantly (5 1%) increased incultured ADPKD epithelial monolayers by comparison to age-matched control cultures derived from human proximal tubules,thick ascending limbs or collecting tubules. Examination ofimmunoreactivity showed that not only cyst-lining epithelialcells but also cyst fluids contained large amounts of immuno-fluorescence. This was particularly marked in the small cysts inthe early stages of development of the disease [83, 84]. Thiscorrelated with radioimmunoassay findings in which detectablelevels of EGF were found in ADPKD and von-Hippel Lindaucyst fluid contents [851. In addition, EGF has been shown toexert hyperplastic effects in cystic proximal tubules in mousemetanephric organ culture [86]. This, therefore, suggests thathypersensitivity to EGF can lead to the hyperplasia necessaryfor cystic enlargement in the kidney. In ADPKD, EGF receptorimmunoreactivity has been demonstrated on apical as well asbasal cell surfaces of cyst lining epithelia, and specific bindingof '251-EGF was demonstrable both on the apical and basalsurfaces of ADPKD epithelia grown to confluence on perme-able membrane supports. These results support the notion thatpart of the hyperplastic response underlying increased cellproliferation in cyst formation is an autocrine effect, since inADPKD, EGF is synthesized by the epithelia cells lining thecysts, secreted apically into the cyst lumen, and is capable ofinteracting with the same cells by virtue of apically located
receptors. It is also conceivable that these increased levels ofEGF are partially responsible for the inhibition of the hydrooso-motic effects of AVP, as has been demonstrated experimentallyin rabbit CCT [871. It is also of note that EGF has been reportedto decrease sodium reabsorption [881, which may have someimpact on fluid accumulation. It would also be of interest toexamine the occurrence and effects of TGFa in cystic disease,since this structural homolog of EGF is transiently synthesizedduring fetal renal development and expression of the gene forboth TGFa and its receptor are frequently associated withcarcinomas [89].
The overall proliferative response of any cell type in vivoreflects the effects of interactions between several growthfactors [90]. In the kidney, it is likely that TGF/3 interactionswould be important, since under normal conditions this is apotent inhibitor of renal tubule proliferation. In fact, TGF2was first isolated from a renal epithelial-derived cell line, BSC-l[91]. TGF1 and 2 belong to the same gene family [92] and aremultifunctional growth factors which exert differential effectsaccording to the target cell type. They have been shown to bemitogenic for cells of mesodermal origin, including fibroblasts,but inhibit cell division of epithelia. In the normal kidney, as inother organs, it has been shown that TGF/3 antagonizes themitogenic action of EGF, dexamethasone and insulin [83, 85,93]. TGFf3 is a ubiquitous, 25 kD peptide [941 which interactswith the equally ubiquitous membrane receptors [95]. Little isknown about the mechanism of TGFI3 receptors 1961, exceptthat they do not possess tyrosine kinase activity [971. Adisturbance in the normal balance between positive and nega-tive growth regulators, such as TGF/3 could be responsible foruncontrolled cell growth as has been demonstrated in humanbreast tumor cells [98], retinoblastoma cells [991, and tumor-promoter-stimulated mouse epidermis cells [1001. Our studieson the effects of TGF on ADPKD epithelial proliferation invitro showed a marked loss of inhibitory activity of TGF/3 withregard to EGF, dexamethasone and insulin mitogenesis [83, 84],and, therefore, suggests a further potential mechanism for theenhanced proliferation of ADPKD cyst lining epithelia. Itremains to be determined whether the alterations in TGF/3sensitivity are due to a decreased number of receptors ordecreased proteolytic activation [101, 102].
Other growth factors relevant to renal development, includ-ing IGF-l and 2 [103], have been tested for possible discrimi-natory proliferative effects in cultures of human normal renaltubule and ADPKD epithelia, but little difference has beenseen. It was of interest, however, that a significant proliferativeresponse to PDGF was found in ADPKD fibroblasts and thatimmunoreactivity for this peptide was demonstrated in cystlining epithelia. This appears to be a case of abnormal paracrineregulation of fibroblast proliferation exerted by tubulocysticepithelia, and may correlate with findings that BSC-l cellssecrete a PDGF-like protein [1041. This may therefore haverelevance with regard to fibrosis, which is another characteris-tic of ADPKD and medullary cystic kidneys.
Cell-cycle regulated gene expressionLittle is known about the expression of cell-cycle regulated
genes in the kidney. During embryonic renal development theN-myc proto-oncogene has been demonstrated by in situ hy-bridization to be confined to differentiating epithelial cells [1051.

456 Wilson and Sherwood: Tubulocystic epithelium
In adult rabbits, during proliferative renal repair after acutenephrotoxic injury, transient increases in steady-state mRNAlevels were seen: for the proto-oncogenes c-fos, c-myc andc-Ha-ras; for the growth-regulated structural protein genesvimentin and f3-actin; and for the transport protein genesNaK-ATPase, ADP-ATP translocase and calcyclin [621. Asingle study in the cpk mouse model of RPKD using similartechniques has demonstrated an increase in c-myc proto-onco-gene, but paradoxically this was not seen until late in theprogression of the disease [1061. This was a surprising finding,since c-fos and c-myc are usually associated with proliferationin the early stages. Further studies will be required to charac-terize early response genes at stages of disease developmentthat correlate with the onset of proliferation. The involvementof c-myc in renal cystic development is further implicated byrecent reports that transgenic mice with the c-myc gene developrenal cysts and die prematurely of renal failure [107].
Fluid transport defects in renal cyst formation
Alterations in NaK-ATPase
NaK-ATPase is a ubiquitous, heterodimeric, integral mem-brane protein responsible for establishing and maintaining theelectrochemical gradients for Na and K. In polarized epithe-ha, such as renal tubules, NaK-ATPase enzyme complexesare segregated in basolateral membranes only, consistent withits function of vectorial active pumping of Na out of cells intothe blood. In light of its major reabsorptive function, it is notsurprising that the kidney is a rich source of NaK-ATPase.Distribution is non-uniform along the nephron and the numberof pump units correlates with the hydrolytic activity of individ-ual nephron segments, being maximal in thick ascending limbsof Henle and distal convoluted tubules (5 x l0 enzyme U/cell),high in proximal convoluted tubules, lower in proximal straighttubules and collecting tubules, and barely detectable in thinlimbs of Henle's loop [108].
The NaK-ATPase enzyme complex is made up of twodissimilar types of subunit (a and /3). The larger (100 kD) asubunit is a polypeptide which spans the cell membrane at leastsix times and is the catalytic moiety, bearing the phosphoryla-tion-ATP and ouabain-binding sites. The smaller (55 kD) /3subunit is a glycoprotein with a single membrane spanningregion and is essential for correct insertion of the enzymecomplex into the appropriate cell membrane [109, 110]. Eachsubunit is synthesized separately as a product of distinct geneson separate chromosomes. The a subunit is encoded by a highlyconserved multigene family and several isoforms have beendetected in various species, including three in humans, thegenes for which are located on different chromosomes (Table3). The expression of these isoforms is developmentally regu-lated [111, 112] and tissue dependent [109, 113, 114], the aisoform predominating in the kidney [1151. Although biochem-ical data concerning the existence of multiple isoforms of the /3subunit are sparse, multiple mRNAs have been isolated insheep and rat [116], and Fambrough has demonstrated twoisoforms in chicken [1171. Thus, there is a complex pattern ofNaK-ATPase subunit isoform expression, and this can bespecifically and differentially modulated by sodium flux andpressure changes [118, 1191. Like all proteins, NaK-ATPasesubunit precursors are synthesized on ribosomes, translocated
Table 3. NaK-ATPase isoforms
Protein Transcript Chromosome
a-subunit
/3-subunit
aaallI/3
/32
aAaBaCaD 11091all! [1111
37??1 [172]1 [172]? [173]
into the endoplasmic reticulum and processed in the Golgi,where maturation of the glycosylated /3 subunit involves con-version of high mannose oligosaccharide side chains. It isgenerally suggested that equimolar amounts of a and /3 subunitform a2 132 complexes inserted into plasma membranes withmost of the a subunit on the intracellular side and most of the /3subunit on the extracellular side. Tamkun and Fambrough [1201have also shown that a significant proportion of NaK-ATPase subunits may remain unassembled and intracellular,and may present an additional means for rapid post-transla-tional modification.
NaK-ATPase activity in the kidney can be increasedsignificantly by several means, including the steroid hormonesaldosterone [121, 122], thyroid hormone [123, 124] and triiodo-thyronine [124], in remnant kidneys [125] and by increasedcellular Na concentration [1261. A significant finding by Avneret al [124] showed that the induction of NaK-ATPase bytriiodothyronine in metanephric organ cultures was associatedwith proximal tubule cyst formation. Subsequent studies haveshown that increased NaK-ATPase activity is also a consis-tent property of RPKD in the cpk mouse [86] and in humanADPKD tissues [23, 127—129]. Since NaK-ATPase is theactive sodium pump enzyme and sodium ions are the majorosmotic determinant in the kidney, it is not surprising thatincreased NaK-ATPase would accompany conditions ofincreased ion and fluid transport.
Membrane polarity defectsNormal renal tubule epithehia are highly polarized cells with a
different complement of proteins in their apical membranesfrom that in their basolateral membranes [reviewed in 130, 131].Apical tight junctions separate these two sets of proteins andprevent them from intermixing within the lipid bilayer of theplasma membrane [1321. Establishment of epithehial polarity inthe kidney occurs early in fetal development [131] and is underthe control of the laminin A chain [65]. Typically, renal tubuleepithelia apical brush border membranes are characterized bythe presence of sodium-coupled transporters, brush border andcoated pit-specific antigens, and ectoenzymes anchored bycovalent links to glcosyl-phosphatylinositol (GPI) includingalkaline phosphatase, y-glutamyl transpeptidase and renaldipeptidase [133, 134]. Renal tubule basolateral membranescontain receptors for basement membrane proteins, hormoneand growth factor receptors, the Cl/HC03 exchanger, andthe sodium pump enzyme NaK-ATPase.
A loss of membrane protein polarity would be catastrophicfor renal tubule function and can be induced experimentally inmonolayer cultures of renal epithelia by deprivation of extra-

Wilson and Sherwood: Tubulocystic epithelium 457
cellular calcium, or in vivo in rat kidney proximal tubules bylimited ischemic insult [131, 135]. In both cases a mixing ofmembrane proteins was seen, including NaK•ATPase andalkaline phosphatase, and this was consistent with a loss in theintegrity of tight junctions. After repair by restoration of normal(mM) concentrations of calcium or restoration of blood flow,newly synthesized proteins were correctly inserted into polar-ized membranes.
The precise intracellular mechanisms by which Na K-ATPase subunits are sorted and targeted to basolateral mem-branes remains obscure, although a role for the expression of /3subunit in directing the a chain to the membrane is clear. It isnot known, however, whether fatty acid acylations play a rolein targeting and docking proteins. Once in the membrane,polarity of NaK-ATPase is maintained by interactions withmembrane-associated proteins which are linked to the actincytoskeleton [136]. It has also been proposed that a complexinteraction with soluble pools of these proteins (fodrin andankyrin) maybe involved in insoluble complex formation [1371.
A dramatic and consistent finding in 20 specimens of ADPKDkidneys has been that, in cystic epithelia, all immunoreactivityfor the a subunit of NaK-ATPase was localized exclusivelyon the apical cell membranes, lining the fluid-filled cyst lumens[127—1291. This was shown to be a functionally competentenzyme by cytochemical staining techniques, ouabain sensitiv-ity and biochemical assays on isolated apical and basolateralmembrane vesicles [1291. This defect was seen very early in theonset of tubule dilation in ADPKD kidneys which containedsome cystic and some normal regions. In those kidneys,NaK-ATPase location in normal, non-dilated tubules wasexclusively basolateral [127]. ADPKD monolayers grown onpermeable membrane supports in which apical and basal mediacompartments were separated showed apical membrane immu-no- and enzyme cytochemical staining and vectorial of trans-port of 22NaCI from basal to apical media which was inhibitableby ouabain [129]. Thus, an early defect in cyst formation inADPKD was the reversal of polarized insertion of NaK-ATPase into apical membranes with consequent redirection ofnet Nat-transport from the serosa into the tubule lumen.Similar apical NaKtATPase is found in the choroid plexuswhere it is associated with the vectorial transport of sodiumfrom the plasma into the cerebrospinal fluid [138]. However, inthis case there is also a reversal of polarity of several othermembrane proteins, such as Na/H antiporter to the basalsurface and Ca2-ATPase in the apical membrane surface. Thisis not the case in ADPKD epithelia where the Nat/H f antiportremained apical, and the anion exchanger and basement mem-brane proteins remained basal in location. A survey of severalpolarized markers led to the conclusion that there was a specificmislocation of NaK-ATPase to the apical membranes ofcystic epithelia, rather than a complete reversal of cell polarity.This was confirmed morphologically by the presence of apicaltight junctions and rudimentary microvilli and basal laminin,type IV collagen and HSPG immunostaining [127, 129]. Anadditional example of apical NaK-ATPase has been seen inassociation with four cases of human arachnoid cysts [139], andmay suggest this as a general mechanism associated with fluidsecretion.
It has been demonstrated directly, by infusion of 3H-waterinto ADPKD patients, that ADPKD cyst walls are highly
permeable to water [37], since 80% of radioactive label hadaccumulated in cyst fluids after five hours. This suggests thatADPKD cell membranes are different from normal ascendinglimbs of Henle which are impermeable to water, and to collect-ing tubules which are impermeable in the absence of vasopres-sin. Since vasopressin has no effect on ADPKD epithelia withregard to increasing cAMP second messenger [23], it is unlikelyto have any effect on water permeability in cysts. Thus,permeability to water could reflect a proximal tubule origin, orconceptually more likely, an increase in membrane fluidity.
It seems that some general properties are characteristic of thefluid expansion observed in cyst development, including in-creased NaK-ATPase activity and reversal of vectorial fluidtransport from normal to apical cell surfaces. This capacity forfluid secretion has also been demonstrated in experimentally-derived MDCK cell cysts in collagen gels [140]. Anothergeneral feature in MDCK and in metanephric organ culture wasthat cyst formation could be inhibited by ouabain, furtherconfirming dependence on NaK-ATPase [141]. In ADPKDepithelia in vitro, apically applied ouabain also inhibitedNaK-ATPase and 22NaC1 transport into the apical medium,but basally applied ouabain had no effect, further confirming themislocation of NaK-ATPase to the apical membranes ofADPKD epithelia [142].
Cytoskeletal alterations in renal cystic diseaseThe epithelial cell cytoskeleton is comprised of microfila-
ments (actin), microtubules (tubulins), and intermediate fila-ments (cytokeratins) [reviewed in 143]. These structural pro-teins confer cell-type specific size, shape, and motility.Intermediate filament proteins are highly insoluble and arethought to be present largely in filamentous form [144]. Micro-filaments and microtubules, however, may exist in both solubleand insoluble pools and thus contribute to the morphology ofthe cell and to the viscoelastic properties of the cytoplasm[144—146]. Since cellular morphology may change profoundlywith the growth and differentiation state of the cell, it is notsurprising that the nature of the cytoskeletal proteins expressedin a cell together with their localization and associations withbinding proteins may change.
In polarized cells, microfilaments and intermediate filamentsare major components inserting into intercellular junctions, andhence are essential for the maintenance of membrane polarity[143, 147]. Actin is also a major component of the corticalcytoskeleton, the filamentous web observed just beneath theplasma membrane, and is particularly prominent in the terminalweb, at the apical aspect of epithelial cells with a brush border,such as renal proximal tubules [147]. Actin appears to play arole in anchoring integral membrane proteins, including en-zymes and transporters, via interactions with ankyrin, fodrinand related proteins [136, 137, 148, 149]. Cytokeratins share therole of establishing intercellular junctions with microfilaments,and recent experiments indicate that they may also bind ankyrinor fodrin [144]. Convincing evidence implicates microtubules inthe transport of organelles and in the delivery of apical mem-brane proteins to the correct domain [150—154].
The importance of the cytoskeleton in renal cyst formation isjust beginning to be explored. As discussed above, renal cystformation requires expansion of tubules by limited hyperplasia.The observed defects in basement membranes in cystic epithe-

458 Wilson and Sherwood: Tubulocystic epithelium
lia might have impact on, or even be directed by the actincytoskeleton via intracellular-extracellular interactions [148,149, 155]. Cells with a proliferative defect share some proper-ties with the transformed phenotype of tumor cells including aloss of specialized ultrastructure and aberrant basement mem-brane attachments. A direct association between growth abnor-malities and cytoskeletal properties in cystic epithelia remainsto be explored.
The role of microtubules in cell division is well characterizedwhile the function of microfilaments and intermediate filamentsis not so clearly understood. The expression of intermediatefilament protein genes is highly cell-type specific [144, 145].Cytokeratins are the major intermediate filament proteins foundin epithelial cells while vimentin predominates in cells ofmesenchymal origin [144]. Although some renal epithelia are infact derived from embryonic mesoderm, fully differentiatedtubule cells express cytokeratins typical of their epithelialnature [156—158]. It is of interest, however, that coexpressionrats treated with daunomycin showed coexpression of cytoker-atins and vimentin in renal epithelia, which was correlated withthe degree of cystic expansion and proliferation [158]. How-ever, coexpression of these proteins was also observed inseveral other diseases and may represent a non-specific re-sponse to tubule injury.
The actin cytoskeleton also responds to the growth state ofthe cell. Expression of different isoforms of actin can beinduced in cells treated with tumor promoters, agents whichfacilitate but cannot initiate neoplastic transformation [159].Although actin isoform expression has not yet been character-ized in renal development, a novel isoform is transiently ex-pressed in intestinal epithelia from neonatal mice [160]. Thesignificance of multiple actin isoforms, which differ only by afew amino acids [161], is not fully understood, but it could bethat different isoforms have different affinities for specificbinding proteins. Our studies have shown that actin is exces-sively abundant in epithelia from ADPKD renal tissue [128,162]. The altered actin content appears to result from a post-translational change or a change in isoform expression, sincedifferences in mRNA levels for f3-actin in ADPKD cells cannotaccount for the excessive amounts of actin observed [129].mRNA levels for /3-actin have also been measured in recessivePKD in cpk mice and no significant differences were detected[50]. In addition to the increased abundance of actin protein inADPKD cells, immunoperoxidase and fluorescence studieshave shown colocalization with apical NaK-ATPase in cystlining epithelia. Visualization of ADPKD cyst epithelial actinfilaments with rhodamine-conjugated phalloidin also showed aconsistent codistribution with the calpactin II (lipocortin I), thecalcium-phospholipid actin binding protein [163]. In addition,calpactin II is excessively abundant in ADPKD [162]. Thisobservation is of particular interest because calpactin II is alsoa major substrate for the tyrosine kinase activity of the epider-ma! growth factor receptor [1641. The phosphorylation of thisprotein correlates with the activation of phospholipase A2 andsubsequent release of plasma membrane arachidonate [165,166]. Our hypothesis is that the over-abundance of calpactin IImay be an amplification response to prolonged stimulation ofthe EGF pathway in ADPKD epithelia, since EGF is a potentmitogen for these cells and is present in large quantities in cyst
lining epithelia and cyst fluid of expanding cysts, as discussedabove.
The fluid accumulation defect in cystic epithelia, in whichaltered targeting and/or anchoring of membrane transport pro-teins appear to play a role, also implicate modifications in thecytoskeleton. The importance of intact cytoskeletal elements innormal cellular processes, including secretion, is clear. Thus,there could be a fundamental role for cytoskeletal abnormalitiesin the initiation or maintenance of tubulocystic disease in whichseveral cellular processes are perturbed.
As described above, Nelson et a! have shown that theNaK-ATPase is anchored in the basolateral membrane ofcultured kidney cells (MDCK cells) to the actin cytoskeletonvia ankyrin and fodrin [136, 137]. Microtubules do not appear tohave a direct effect on the targeting or anchoring of basolateralmembrane proteins, but microtubular disruption by coichicineand vinblastine has suggested their integrity is essential fortransport of apically destined proteins to the correct plasmamembrane domain [150—154], although the possibility that theeffects of these agents were due to perturbation of the Golgicould not be ruled out. An analogous process appears to act inthe delivery of secretory vesicles to the apical surface ofpolarized cells, and calpactin I has recently been implicated inthe fusion process required for regulated secretion events [167].The possibility that apically-destined membrane proteins aredelivered via the same processes as secretory granules remainsto be established, Thus, it can be speculated that the specificmistargeting of NaK-ATPase to the apical plasma membranein ADPKD cyst enlargement, might be the result of alterationsof interaction with those cytoskeletal proteins responsible forNaK-ATPase intracellular targeting or anchoring. Alterna-tive possibilities remain to be explored including: possiblemodifications in fatty acid acylation targeting and anchoring;altered Golgi processing of NaK-ATPase subunits; and al-terations at the level of the gene NaK-ATPase a and /3subunits.
Conclusions and perspectives
The evidence presented suggests that numerous cellularchanges can occur during the initiation and progression of renalcystic diseases of genetic and non-genetic origin. At least twobasic criteria are necessary for cystic expansion of renal tu-bules: aberrant epithelial cell proliferation and lumenal fluidaccumulation. Epithelial cell growth can be regulated by insol-uble factors in the extracellular matrix and by soluble peptidefactors. Both mechanisms are implicated in renal cystic devel-opment since abnormalities of heparan sulfate proteog!ycanmatrix deposition and decreased sensitivity to TGFI3 have beendemonstrated, thus potentially reducing inhibitory regulation ofepithelial proliferation. In addition, hypersensitivity to theepithelial mitogen, EGF has been found in genetic polycystickidney disease, where it is thought to be an autocrine factor andis associated with the presence of aberrant apical membranereceptors and increased protein amounts of the intracellularEGF receptor tyrosine kinase substrate, lipocortin. IncreasedNaK-ATPase activity is also a common feature of renalepithelial cysts of genetic and non-genetic origin and is associ-ated with the observed fluid accumulation. In human autosomaldominant polycystic kidney disease (ADPKD), a specific rever-sal of polarity of NaK-ATPase location has been demon-

Wilson and Sherwood: Tubulocystic epithelium 459
strated in the apical membranes of cyst lining epithelia, andshown to be responsible for basal to apical transport of Na andcan be inhibited by apically applied ouabain.
Little information is available concerning the sequence ofevents necessary to result in the phenotypic expression of renaltubule cysts. However, it is clear from studies on early stages ofdevelopment of RPKD in cpk mice and in ADPKD kidneys with> 50% morphologically-normal renal tubules, that the enhancedactivity and reversed membrane polarity of NaK-ATPase isan early event. The presence of immunoreactive EGF in thefluid of small cysts in early stage ADPKD kidneys also suggestautocrine EGF production might be an early modification. Bycontrast, alterations in the type IV collagen components ofcystic basement membranes appear to be later events. Theproliferative and fluid transport defects appear to be coordi-nated in cyst formation, and must be a different process fromthe hyperplasia of tumor formation in which rapid uncontrolledgrowth leads to solid cell masses. Nevertheless, completeanalysis of expression of growth related genes, including pro-tooncogenes during cystic development, would be instructive.
It maybe speculated that one of the observed defects in cysticepithelia could be a primary change to which all the othermanifestations are linked in a secondary fashion. For instance,there are well documented relationships between the actin-based cytoskeleton and NaK4-ATPase polarity [136, 137],secretion [148—1521, matrix [153—155, 1681 and growth factorreceptor substrate interactions [1631. In addition, there is evi-dence of tight interactions between matrix proteins and growthfactors [169—171], matrix and polarity [172—1731 and intracellu-lar and extracellular Na ion contents and proliferation [174,175]. Until more evidence has been collected in normal renaltubule epithelia, however, the primary defect will remain elu-sive. The sobering possibility must also be considered that noneof the changes documented to date is the underlying cause, butmerely reflect the effects of cystic enlargement. A search foralterations at the fundamental levels of signal transduction andtranscription factors remains to be explored.
Acknowledgments
This work was supported in part by NIH R01 DK 40698 and P01 DK34039. Tissue was procured by National Disease Research Interchangeand International Institute for the Advancement of Medicine, Philadel-phia, Pennsylvania, USA. The authors are indebted to Dr. J.T. Normanand Dr. J. Hassell for their generous contributions of experimentaleffort and discussion, to Eugene Guerra for technical assistance and toMrs. Gloria Trechock in typing the manuscript. Additional thanks arealso due to Dr. C.R. Burrow, whose detailed sleuthing and criticalevaluations were not only stimulating but gave an added dimension tothe discussion.
Reprint requests to Patricia D. Wilson, M.D., Department of Phys-iology and Biophysics, UMDNJ-Robert Wood Johnson MedicalSchool, 674 Hoes Lane, Piscataway, New Jersey 08854-5635, USA.
References
1. MCKUSICK V: Mendelian inheritance in man.2. BERNSTEIN J: The classification of renal cysts. Nephron 11:91—
100, 19733. DALGAARD OZ: Polycystic disease of the kidneys, in Disease of
the Kidney, edited by STRAUSS MB, WELT LG, Boston, LittleBrown & Co., 1963, pp. 1223—1258
4. DUNNILL MS, MILLARD PR, OLIvER D: Acquired cystic diseaseof the kidneys: A hazard of long-term intermittent maintenancehemodialysis. J C/in Pathol 30:868-.877, 1977
5. HESTBECH J, HANSEN HE, AMDISEN A, OLSEN S: Chronic renallesions following long-term treatment with lithium. Kidney mt12:205—213, 1977
6. GARDNER KD, SOLOMON 5, FITZGERREL WW, EvAN AP: Func-tion and structure in the diphenylamine-exposed kidney. J Cl/nInvest 57:796—806, 1970
7. PREMINGERGM, KOCH WE, FRIED FA, MCFARLAND E, MURPHYE, MANDELL J: Murine congenital polycystic kidney disease: Amodel fur studying development of cystic disease. J Urol 127:556—560, 1982
8. AVNER ED, STUDNICKI FE, YOUNG MC, SWEENEY WE, PIESCONP, ELLIS D, FETTERMAN GH: Congenital murine polycystickidney disease. 1. The ontogeny of tubular cyst formation. PediatrNephrol 1:587—596, 1987
9. MARTINEZ-MALDONADO M, YIUM JJ, EKNOYAN G, SuKI WN:Adult polycystic kidney disease: Studies of the defect in urineconcentration. Kidney mt 2:107—113, 1972
10. GABOW PA, IKLE DW, HOLMES JH: Polycystic kidney disease.Progressive analysis of nonazotemic patients and family members.Ann Intern Med 101:238—247, 1984
11. BAERT L: Hereditary polycystic kidney disease (adult form): Amicrodissection study of two cases at an early stage of the disease.Kidney mt 13:519—525, 1978
12. LAMBERT PP: Polycystic disease of the kidney. Arch Pathol
44:34—58, 194713. POTTER EL: Normal and Abnormal Development of the Kidney.
Chicago, Year Book, 197214. FARAGGLANA T, BERNSTEIN J, STRAUSS L, CHIRG J: Use of lectins
in the study of histogenesis of renal cysts. Lab Invest 53:575—579,1985
15. GARDNER KD: Composition of fluid in twelve cysts of a polycystickidney. N Engl J Med 28 1:985—988, 1969
16. HUSEMAN R, GRADY A, WELLING D, GRANTHAM JJ: Macropunc-ture study of polycystic kidney disease in adult human kidneys.Kidney mt 18:375—385, 1980
17. GRANTHAM JJ: Polycystic kidney disease: a predominance ofgiant nephrons. Am J Physiol 244:F3—Fl0, 1983
18. REEDERS ST, BREUNING MH, DAVIES KE, NICHOLLS RD, JAR-MAN AP, HIGGS DR, REARSON PL, WEATHERALL Di: A highlypolymorphic DNA marker linked to adult polycystic kidney dis-ease on chromosome 16. Nature 317:542—544, 1985
19. KIMBERLING Wi, FAIN PR, KENYON JB, GOLDGAR D, SUJANSEYE, GABOW PA: Linkage heterogeneity of autosomal dominantpolycystic kidney disease. N Engl J Med 319:913—918, 1988
20. ROMEO G, DavoTo M, COSTA G, RoNCuzzi L, CATIZONE L,ZUCCHELLI P, GERMINO GG, KEITH T, WEATHERALL Di, REED-ERS ST: A second genetic locus for autosomal dominant polycystickidney disease. Lancet July 2, 8—10, 1988
21. NORBY S, SORENSEN AWS, BOESEN P: Non-allelic genetic heter-ogeneity of autosomal dominant polycystic kidney disease? inGenetics of Kidney Disorders. Prog C/in Biol Res 305:83—88, 1989
22. CUPPAGE FE, HUSEMAN RA, CHAPMAN A, GRANTHAM JJ: Ultra-structure and function of cysts from human adult polycystickidneys. Kidney Irn 17:372—381, 1980
23. WILSON PD, SCHRIER RW, BRECKON RD, GABOw PA: A newmethod for studying human polycystic kidney disease epithelia inculture. Kidney mt 30:371—378, 1986
24. BERNSTEIN J, EVAN AP, GARDNER KD: Epithelial hyperplasia inhuman polycystic kidney diseases. Am JPathol 129:92—101, 1987
25. WILSON PD, DILLINGHAM MA, BRECKON R, ANDERSON Ri:Defined human renal tubular epithelia in culture: Growth, charac-terization and hormonal response. Am J Physiol 248:F436—F443,1985
26. VANPUTTEN V, PRZEKWA5 i, GABOW P. SCHRIER RW, GRANOTY: Parathyroid hormone and vasopressin resistance in autosomaldominant polycystic kidney disease epithelial cells. (abstract) AmSoc Nephrol, 1989, p. l92A
27. GRAHAM PC, LINDOP GBM: The anatomy of the renin-secretingcell in adult polycystic kidney disease. Kidney mt 33:1084—1090,1988

460 Wilson and Sherwood: Tubulocystic epithelium
28. MCATEER JA, CARONE FA, GRANTHAM JJ, KEMPSON ST, GARD-NER KD, EVAN AP: Explant culture of human polycystic kidney.Lab Invest 59:126—136, 1988
29. WILSON PD: Characteristics of microdissected normal humanrenal tubules and polycystic kidney epithelia grown in culture.Proc MDRJ 2nd mt Conference, The Use of Human Tissue andOrgans for Research, 1985, pp. 151—157
30. EVAN AP, GARDNER KD: Nephron obstruction in nordihydroguai-aretic acid-induced renal cystic disease. Kidney mt 15:7—19, 1979
31. BJERLE P, LINDQUIST B, MICHAELSON G: Pressure measurementsin renal cysts. ScandJ Lab C/in Invest 27:135—138, 1971
32. CARONE FA, ROWLAND RG, PERLMAN SG, GAN0TE CE: Thepathogenesis of drug-induced renal cystic disease. Kidney mt5:411—421, 1974
33. GRANTHAM JJ, DONOSO VS, EVAN AP, CARONE FA, GARDNERKD: Viscoelastic properties of tubule, basement membranes inexperimental renal cystic disease. Kidney mt 32:187—197, 1987
34. EVAN AP, GARDNER KD, BERNSTEIN J: Polypoid and papillaryepithelial hyperplasia: A potential cause of ductal obstruction inadult polycystic disease. Kidney mt 16:743—750, 1979
35. WELLING LW, WELLING D: Theoretical models of cyst formationand growth. Scanning Microsc 2:1097—1102, 1988
36. GRANTHAM JJ, GEISER JL, EVAN AP: Cyst formation and growthin autosomal dominant polycystic kidney disease. Kidney mt31:1145—1152, 1987
37. JACOBSSON K, LINDQVIST B, MICHAELSON G, BJERLE P: Fluidturnover in renal cysts. Acta Med Scand 202:327—329, 1977
38. EKBLOM P, VESTWEBER D, KEMLER R: Cell-matrix interactionsand cell adhesion during development. Ann Rev Cell Biol 2:27—47,1986
39. HALTER SA, GLICK AD: Basement membrane changes in humanbreast tissue in explant culture: A morphometric and ultrastruc-tural study. Ultrastruct Pathol 4:23—34, 1983
40. STENBACH F, WA5ENIUS V: Basement membrane structures intumors of the ovary. EurJ Obstet Gynec ReprodBiol20:357—371,1985
41. ORMEROD EJ, WARBURTON MJ, GUSTERSON B, HUGHES CM,RUDLAND PS: Abnormal deposition of basement membrane andconnective tissue components in dimethylbenzanthracene-in-duced rat mammary tumours: An immunocytochemical and ultra-structural study. Histochem J 17:1155—1166, 1985
42. COHEN AH, H0YER JR: Nephronophthisis a primary tubularbasement membrane defect. Lab Invest 55:564—572, 1986
43. Wnso PD, HRENIUK D, GABOW PA: Relationship betweenabnormal extracellular matrix and escessive growth of humanadult polycystic kidney disease epithelia. J Cell Physiol (in press)
44. WILSON PD, HRENIUK D, GABOW PA: Influence of extracellularmatrix components on the enhanced growth response of polycys-tic kidney disease epithelia. (abstract) J Cell Biol 107:796, 1988
45. KANWAR YS, CARONE FA: Reversible changes of tubular cell andbasement membrane in drug-induced renal cystic disease. Kidneymt 26:35—43, 1984
46. HALEY DP, BULGER RE: The aging male rat: Structure andfunction of the kidney. Ann JAnat 167:1—13, 1983
47. MARTINEZ-HERNANDEZ A, AMENTA A: The basement membranein pathology. Lab Invest 48:656-677, 1983
48. EKBLOM P, LEHTONEN E, SAXEN J, TLMPL R: Shift in collagentype as an early response to induction in the metanephric mesen-chyme. J Cell Biol 89:267—283, 1981
49. MARTINEZ-HERNANDEZ A, GAY S, MILLER EJ: Ultrastructurallocalization of type V collagen in rat kidney. J Cell Biol 92:343—349, 1982
50. EBIHARA I, KILLEN PD, LAURIE GW, HUANG T, YAMADA Y,MARTIN GR, BROWN KS: Altered mRNA expression of basrnentmembrane components in a murine model of polycystic kidneydisease. Lab Invest 58:262—269, 1988
51. HAsSELLJR, LEYSHON WC, LEDBETTERSR, TYREEB, SUZUKI S,KATO M, KIMATA K, KLEINMAN H: Isolation of two forms ofbasement membrane proteoglycans. J Biol Chem 260:8098—8105,1985
52. KLEIN DJ, BROWN DM, OEGEMA TR, BRENCHLEY PE, ANDER-SON JC, DICKINSON MAJ, HORIGAN EA, HASSELL JR: Glomerular
basement membrane proteoglycans are derived from a largeprecursor. J Cell Biol 106:963—970, 1988
53. STOW JL, FARQUHAR MG: Distinctive populations of basementmembrane and cell membrane heparan sulfate proteoglycans areproduced by cultured cell lines. J Cell Biol 105:529—539, 1987
54. COUCHMAN JR. AUSTRIA R, WOODS A, HUGHES RC: Adhesiondefective BHK mutant has cell surface heparan sulfate proteogly-can of altered properties. J Cell Physiol 136:226—236, 1988
55. SAUNDERS S, BERNFELD M: Cell surface proteoglycan bindsmouse mammary epithelial cells to fibronectin and behaves as areceptor for interstitial matrix. J Cell Biol 106:423—430, 1988
56. YAMAGUCHI Y, RUOSLAHTI E: Expression of human proteoglycanin Chinese hamster ovary cells inhibits cell proliferation. Nature336:244—246, 1988
57. HAMATI HF, BRITTON EL, CAREY DJ: Inhibition of proteoglycansynthesis alters extracellular matrix deposition, proliferation andcytoskeletal organization of rat aortic smooth muscle cells inculture. J Cell Biol 108:2495—2505, 1989
58. CASTELLOT JJ, ADDONIZIO ML, ROSENBERG R, KARNOVSKY MJ:Cultured endothelial cells produce a heparin-like inhibitor ofsmooth muscle cell growth. J Cell Biol 90:372—379, 1981
59. CARONE FA, HOLLENBERG PF, NAKAMURA S, PUNYARIT P,GLOGOWSKI W, FLOURET G: Tubular basement membrane changeoccurs pan passu with the development of cyst formation. Kidneylnt 35:1034—1040, 1989
60. WERB Z, DINGLE JT, REYNOLDS JJ, BARRETT AJ: Proteoglycan-degrading enzymes of rabbit fibroblasts and granulocytes. Bio-chem J 173:949—958, 1978
61. BASERGA R: The cell cycle. N Engl J Med 304:453—459, 198162. NORMAN iT, BOHMAN R, FISCHMANN G, BOWEN JW, MCDON-
OUGH A, SLAMON D, FINE L: Patterns of mRNA expressionduring early cell growth differ in kidney epithelial cells destined toundergo compensatory hypertrophy versus regenerative hyperpla-sia. Proc NatI Acad Sd USA 85:6768—6772, 1988
63. WILSON PD, HORSTER M: Differential response to hormones ofdefined distal nephron epithelia in culture. Am J Physiol 24:C 166—C174, 1983
64. WILSON PD, ANDERSON RJ, BRECKON RD, NATHRATH WJ,SCHRIER RW: Retention of differentiated characteristics by cul-tures of defined rabbit kidney epithelia. J Cell Physiol 130:245—254, 1987
65. EKBLOM P: Developmentally regulated conversion of mesen-chyme to epithelium. FASEB J 3:2141—2150, 1989
66. RITTLING SR, BASERGA R: Expression of growth-related genes insenescent human diploid fibroblasts, in Growth Control DuringCell Aging, edited by WANG E, WARNER HR, New York, CRCPress, 1989, pp. 19—29
67. PARDEE AB: G1 events and regulation of cell proliferation. Sci-ence 246:603—608, 1989
68. SPORN M, ROBERTS AB, WAKEFIELD LM, ASSOIAN R: Trans-forming growth factor /3: Biological function and chemical struc-ture. Science 233:532—534, 1986
69. ROZENGURT E: Early signals in the mitogenic response. Science234:162—166, 1986
70. MENDLEY SR, TOBACK FG: Autocrine and paracrine regulation ofkidney epithelial cell growth. Ann Rev Physiol 51:33—50, 1988
71. CARPENTER G, ZENDEGUI JG: Epidermal growth factor, its recep-tor and related proteins. Exp Cell Res 164:1—10, 1986
72. DEFIZE LHK, BOONSTRA J, MEISENHELDER J, KRUIJER W,TERTOOLEN LGJ, TILLY BC, HUNTER T, VAN BERGEN PM,MOOLENAAR WH, DE LAAT SW: Signal transduction by epidermalgrowth factor occurs through the subclass of high affinity recep-tors. J Cell Biol 109:2495—2507, 1989
73. FABRICANT RN, DELARCO JE, TODARO GJ: Nerve growth recep-tors on human melanoma cells in culture. Proc NatI Acad Sci USA74:565—569, 1977
74. HOLLSTEIN MC, SMITS AM, GALIANA C, YAMASAKI H, BoS JL,MANDARD A, PARTENSKY C, MONTESANO R: Amplification ofepidermal growth factor receptor gene but no evidence of rasmutations in primary human oesophageal cancers. Cancer Res48:5119—5123, 1988
75. Ro J, NORTH SM, GALLICK GE, HORTOBAGYI GN, GUTTERMANJU, BUCK M: Amplified and overexpressed epidermal growth

Wilson and Sherwood: Tubulocystic epithelium 461
factor receptor gene in uncultured primary human breast carci-noma. CancerRes48:161—164, 1988
76. DI FloRa PP, PIERCE JH, FLEMING TP, HAZAN R, ULLRICH A,KING AR, SCHLESSINGER J, AARONSON SA: Overexpression ofthe human EGF receptor confers an EGF-dependent transformedphenotype to NIH 3T3 cells. Cell 51:1063—1070, 1987
77. JOHNSON AC, GARFIELD SH, MERLINO GT, PASTAN I: Expres-sion of epidermal growth factor receptor proto-oncogene mRNAin regenerating rat liver. Biochem Biophys Res Commun 150:412—418, 1988
78. FISHER DA, SALIDO EC, BARAJAS L: Epidermal growth factor andthe kidney. Annu Rev Physiol 5 1:67—80. 1989
79. NORMAN J, BADIE-DEZFOOLY B, NORD E, KURTZ I, SCHLOSSERJ, CHAUDHARI A, FINE L: EGF-induced mitogenesis in proximaltubular cells: Potentiation by angiotensin II. Am J Physiol 253:F299—F309, 1987
80. MULLIN JM, MCGINN MT: Epidermal growth factor-inducedmitogenesis in kidney epithelial cells (LLC-PKI). Cancer Res48:4886—4891, 1988
81. GOODYER PR, KACHRA Z, BELL C, ROZEN R: Renal tubular cellsare potenetial targets or epidermal growth factor. Am J Physiol255:Fll9l—F1l96, 1988
82. BOCCARDO F, VALENTI G, ZANARDI 5, CERRUTI G, FASSIO T,BRUZZI P, DE FRANCHIS V, BARRECA A, DEL MONTE P, MINUT0F: Epidermal growth factor in breast cyst fluid: Relationship withintracystic cation and androgen conjugate content. Cancer Res48:5860—5863, 1988
83. WILSON PD, Du J, GUERRA E, NORMAN iT: Autocrine, endocrineand paracrine regulation of growth abnormalities in autosomaldominant polycystic kidney disease. FASEB J (submitted forpublication)
84. DAS K, GABOW PA, WILSON PD: Abnormal growth factor re-sponse by human adult polycystic kidney disease epithelia in vitro.(abstract) Kidney mt 35:225, 1988
85. MOSKOWITZ D, BONAR SL, MARCUS MD, CLAYMAN RV, AVNERED: Epidermal growth factor content of human and mouse (cpk)renal cyst. (abstract) Clin Res 37:497A, 1989
86. AVNER ED, SWEENEY WE: Epidermal growth factor induceshyperplastic tubular cysts and increased Na-K-ATPase activity invitro. (abstract) Am Soc Nephrol 1989, p. 24
87. BREYER MD, JACOBSON HR, BREYER JA: Epidermal growthfactor inhibits the hydroosmotic effect of vasopressin in theisolated perfused rabbit cortical collecting tubule. J Clin Invest82:1313—1320, 1988
88. VEHASKARI VM, HERING-SMITH KS, MosKowITz DW, WEINERID, HAMM LL: Effect of epidermal growth factor on sodiumtransport in the cortical collecting tubule. Am J Physiol 256:F803—F809, 1989
89. DERYNCK R: Transforming growth factor a. Cell 54:593—595, 198890. SPORN MB, ROBERTS AB: Peptide growth factors are multifunc-
tional. Nature 332:217—219, 198891. TUCKER RF, SHIPLEY GD, MOSES HL, HOLLEY RW: Growth
inhibitor from BSC-l cells closely related to platelet type btransforming growth factor. Science 226:705—707, 1984
92. DUKE P, HANSEN P, IWATA KK, PIELER C, FOULKES JG: Iden-tification of another member of the transforming growth factortype f3 gene family. Proc Nod Acad Sci USA 85:4715—4719, 1988
93. MULDOON LL, RODLAND KD, MAGUN BE: Transforming growthfactor f3 modulates epidermal growth factor-induced phosphoi-nositide metabolism and intracellular calcium levels. J Biol Chem263:5030—5033, 1988
94. FLANDERS KC, THOMPSON NL, CISSEL DS, VAN OBBERGHEN-SCHILLING E, BAKRE CC, KASS ME, ELLINGSWORTH LR, RoB-ERTS AB, SPORN MB: Transforming growth factor-/31: Histochem-ical localization with antibodies to different epitopes. J Cell Biol108:653—660, 1989
95. CHEIFETZ S, LIKE B, MASSAGUE J: Cellular distribution of type Iand type II receptors for transforming growth factor /3. J BiolChem 261:9972—9978, 1986
96. BOYD FT, MASSAGUE J: Transforming growth factor-$ inhibitionof epithelial cell proliferation linked to the expression of a 53-kDamembrane receptor. J Biol Chem 264:2272—2278, 1989
97. SPORN MB, ROBERTS AB, WAKEFIELD LM, DE CROMBROGGHE B:
Some recent advances in the chemistry and biology of transform-ing growth factor-beta. J Cell Biol 105:1039—1045, 1987
98. KNABBE C, LIPPMAN ME, WAKEFIELD LM, FLANDERS KC,KASID A, DERYNCK R, DICKSON RB: Evidence that transforminggrowth factor-/3 is a hormonally regulated negative growth factorin human breast cancer cells. Cell 48:417—428, 1987
99. KIMCHI A, WANG X, WEINBERG RA, CHEIFETZ 5, MASSAGUE J:Absence of TGF-/3 receptors and growth inhibitory responses inretinoblastoma cells. Science 240:196—198, 1988
100. AKI-IURST RJ, FEE F, BALMAIN A: Localized production of TGF-13mRNA in tumour promoter-stimulated mouse epidermis. Nature331:363—365, 1988
101. O'CoNNoR-McCOURT MD, WAKEFIELD LM: Atent transforminggrowth factor-$ in serum. J Biol Chem 262:14090-14099, 1987
102. LYONS RM, KESKI-OJA J, MOSES HL: Proteolytic activation oflatent growth factor-$ from fibroblast-conditioned media. J CellBiol 106:1659—1665, 1988
103. HAMMERMAN MR: The growth factor hormone-insulin-likegrowth factor axis in the kidney. Am J Physiol 257:F503—F514,1989
104. KARTHA S, BRADHAM DM, GROTENDORST GR, TOBACK FG:Kidney epithelial cells express c-sis protooncogene and secretePDGF-like protein. Am J Physiol 255:F800—F806, 1988
105. HIRVONEN H, SANDBERG M, KALIMO H, HUKKANEN V, VuoiioE, SALMI TT, ALITALO K: The N-myc-proto-oncogene and IGF-IIgrowth factor mRNAs are expressed by distinct cells in humanfetal kidney and brain. J Cell Biol 108:1093—1104, 1989
106. COWLEY BD, SMARDO FL, GRANTI-IAM JJ, CALVET JP: Elevatedc-myc protooncogene expression in autosomal recessive polycys-tic kidney disease. Proc Nail Acad Sci USA 84:8394—9398, 1987
107. TRUDEL M, D'AGATI V, CONSTANTINI F: The c-myc oncogeneinduces kidney cysts in transgenic mice. (abstract) Kidney mt35:364, 1989
108. KATZ AL: Overview: Role of Na-K-ATPase in kidney function, inThe Na,K-Pump, Part B, Cellular Aspects, New York, AlanLiss Inc., 1988, pp. 207—232
109. SHULL MM, LINGREL JB: Multiple genes encode the humanNa,K-ATPase catalytic subunit. Proc Nail Acad Sd USA84:4039—4043, 1987
110. GEERING K: Overview: Biosynthesis, membrane insertion andmaturation of Na,K-ATPase, in The Na,K-Pump, Part B,Cellular Aspects, New York, Alan Liss Inc., 1988, pp. 19—33
Ill. SVERDLOV ED, AKOPYANZ NS, PETRUKHIN KE, BROUDE NE,MONASTYRSKAYA OS, MODYANOV NN: Na,K-ATPase: Tissuespecific expression of genes coding for a-subunit in diverse humantissues. FEBS Lett 239:65—68, 1988
112. HERRERA VL, EMANUEL JR, RUIZ-OPAZO N, LEVENSON R,NADAL-GINARD B: Three differentially expressed Na,K-ATPasea subunit isoforms: Structural and functional implications. J Cell
Biol 105:1855—1865, 1987113. EMMANUEL JR, GARETZ 5, STONE L, LEVENSEN R: Differential
expression of Na,K-ATPase a and /3 subunit mRNAs in rattissues and cell lines. Proc Nat/Acad Sci USA 84:9030—9034, 1987
114. SHYJAN AW, LEVENSEN R: Antisera specific for the al, a2, a3and /3 subunits of the Na,K-ATPase: Differential expression of aand /3 subunits in rat tissue membranes. Biochem 28:4531—4535,1989
115. MERCER RW, SCHNEIDER JW, BENZ EJ: Molecular cloning andcharacterization of a-subunit isoforms of the Na,K-ATPase, inThe Na,K-Pump, Part B, Cellular Aspects, New York, AlanLiss Inc, 1988, pp. 119—126
116. YOUNG RM, SHULL GE, LINGREL JB: Multiple mRNAs from ratkidney and brain encode a single Na,K-ATPase /3 subunitprotein. J Biol Chem 262:4905—4910, 1987
117. FAMBROUGH DM, BAYNE EK: Multiple forms of (Na K)-ATPase in the chicken. J Biol Chem 258:3926—3935, 1983
118. BOWEN JW, MCDONOUGH A: Pretranslational regulation of Na-K-ATPase in cultured canine kidney cells by low K. Am JPhysiol 252:C179—C189, 1987
119. HERRERA VL, CHOBANIAN AV, RUIZ-OPAZO N: Isoform-specificmodulation of NaK-ATPase a-subunit gene expression in hy-pertension. Science 241:221—230, 1988
120. TAMKUN MM, FAMBROUGH DM: The (Na=K)-ATPase of chick

462 Wilson and Sherwood: Tubulocystic epithelium
sensory neurons. Studies on biosynthesis and intracellular trans-port. J Biol Chem 261:1009—1019, 1986
121. DOUCET A: Function and control of Na-K-ATPase in singlenephron segments of the mammalian kidney. Kidney ml 34:749—760, 1988
122. VERREY F, SCFIAERER E, ZOERKLER P, PACCOLAT MP, GEERINGK, KRAEHENBUHL JP, ROSSIER BC: Regulation of aldosterone ofNa,K-ATPase mRNAs, protein synthesis and sodium transportin cultured kidney cells. J Cell Biol 104:1231—1237, 1987
123. GUERNSEY DL, EDELMAN IS: Loss of thyroidal inducibility ofNa,K-ATPase with neoplastic transformation in tissue culture. JBiolChem 261:11956—11961, 1986
124. AVNER ED, SWEENEY WE, PIEsco NP, ELLIS D: Triiodothyro-nine-induced cyst formation in metanephric organ culture: Therole of increased Na-K-adenosine triphosphatase activity. J LabClin Med 109:441—453, 1987
125. SALEHMOGHADDAM S, BRADLEY T, MIKHAIL N, BADIE-DEZ-FOOLY B, NORD E, TRIZNA W, KHEYFETS R, FINE L: Hypertro-
phy of basolateral Na-K pump activity in the proximal tubule ofthe remnant kidney. Lab Invest 53:443—450, 1985
126. WOLITSKY BA, FAMBROUGH DM: Regulation of the (Na-K)-ATPase in cultured chick skeletal muscle. Modulation of expres-sion by the demand for ion transport. J Biol Chem 261:9990—9999,1986
127. WILSON PD, HRENIUK D: Altered polarity of NaK-ATPase in
epithelia with a genetic defect and abnormal basement membrane.(abstract) J Cell Biol 105:1760, 1987
128. WILsoN PD: Cystic epithelia in vitro, in Proceedings of thePolycytic Kidney Foundation, TP&T Inc., 1988
129. WILsoN PD, SHERWOOD AC, PALLA K, Du J, WATSON R,NORMAN JT: Reversed polarity of NaK-ATPase: Mistocationto apical plasma membranes in human polycystic kidney diseaseepithelia. J Clin Invest (submitted for publication)
130. HANDLER iS: Overview of epithelial polarity. Ann Rev Physiol51:729—740, 1989
131. RODRIGUEZ-BOULAN E, NELSON WJ: Morphogenesis of the po-larized epithelial cell phenotype. Science 245:718—725, 1989
132. SIM0N5 K, FULLER SD: Cell surface polarity in epithelia. Ann RevCell Biol 1:243—288, 1985
133. Low MG: Glycoryl-phosphatidylinositol: A versatile anchor forcell surface proteins. FASEB J 3:1600—1608, 1989
134. LIsANrI MP, SARGIACOMO M, GRAEVE A, SALTIEL AR, ROD-RIGUEZ-BOULAN E: Polarized apical distribution of glyconyl-phosphatidylinositol anchored proteins in a renal epithelial cellline. Proc NatlAcad Sci USA 85:9557—9561, 1988
135. MOLIT0RIs BA, WILSON PD, SCHRIER RW, SIMON FR: Ischemiainduces partial loss of surface membrane polarity and accumula-tion of putative calcium ionophores. J Clin Invest 76:2097—2105,1985
136. NELSON WJ, HAMMERTON RW: A membrane-cytoskeletal corn-
plex containing NaK-ATPase, ankyrin and fodrin in Madin-Darby canine kidney (MDCK) cells. Implications for the biogen-esis of epithelial cell polarity. J Cell Biol 108:893—902, 1989
137. NELSON Wi, VESHNOCK Pi: Ankyrin binding to (Na,K')-AT-Pase and implications for the organization of membrane domainsin polarized cells. Nature 328:533—536, 1987
138. SPECTOR R, JOHANSON CE: The mammalian choroid plexus. SciAm :68—74, 1989
139. Go KG, HOUTHOFF H, HARTSUIKER J, BLAAUW EH, HAVINGAP: Fluid secretion in arachnoid cysts as a clue to cerebrospinalfluid absorption at the arachnoid granulation. J Neurosurg 65:642—648, 1986
140. GRANTHAM JJ, UCHIC M, CRAGOE EJ, KORNI-IAUS J, GRANTHAMJA, DoNoso V, MANGOO-KARIM R, EVAN A, MCATEER J:Chemical modification of cell proliferation and fluid secertion inrenal cysts. Kidney mt 35:1379—1389, 1989
141. AVNER ED, SWEENEY WE, ELLIS D: In vitro modulation oftubular cyst regression in murine polycystic kidney disease.Kidney mt 36:960—968, 1989
142. WILSON PD, PALLA K, GUERRA E, HRENIUK D: Effects ofreversed polarity of NaK-ATPase on vectorial Na transport incultured human polycystic kidney disease epithelia. Am Soc
Nephol 1989, p. 414
143. COUDRIER E, KERJASCHKI D, LOUVARD D: Cytoskeleton organi-zation and submembranous interactions in intestinal and renalbrush borders. Kidney mt 34:309—320, 1988
144. STEINERT PM, RooP DR: Molecular and cellular biology ofintermediate filaments. Ann Rev Biochem 57:593—626, 1988
145. POLLARD TD, COOPER JA: Actin and actin-binding proteins. AnnRev Biochem 55:987—1036, 1986
146. KIRSCHNER MW: Microtubule assembly and nucleation. mt RevCytol 54: 1—71, 1978
147. MOOSEKER MS, TILNEY LG: Organization of actin-filament-mern-brane complex: Filament polarity and membrane attachment inthe microvilli of intestinal epithelial cells. J Cell Biol 67:725—743,
1975148. GEIGER B: A 130K protein from chicken gizzard: Its localization at
the termini of microfilament bundles in cultured chicken cells. Cell18:193—205, 1978
149. BURRIDGE K, FERAMISCO R: Microinjection and localization of a130K protein in living fibroblasts: A relationship to actin. Cell19:587—595, 1980
150. BENNETT G, CARLET E, WILD G, PARSONS S: Influence ofcolchicine and vinbiastine on the intracellular migration of secre-tory and membrane glycoproteins. Am J Anat 170:545—566, 1984
151. BLOK J, GINSEL A, MOLDER-STAPEL A, ONDERWATER ii, DAEMSWT: The effect of colchicine on the intracellular transport of3H-fucose-labelled glycoproteins in the absorptive cells of cul-tured small intestine tissue. Cell Tissue Res 215:1—12, 1981
152. DANIELSEN EM, COWELL GM, POULSON SS: Biosynthesis ofmicrovillar proteins: Evidence for an intracellular sorting takingplace in or shortly after exit from the Golgi complex. Eur JBiochem 152:493—499, 1983
153. RINDLER Mi, IvANov IE, SABATINI DD: Microtubule acting
drugs lead to non-polarized delivery of the influenza hernagglutininto the cell surface of polarized Madin-Darby canine kidney cells.JCellBio! 104:231—241, 1987
154. ACHLER C, FILMER D, MERTE C, DRENCKHAHN D: Role ofmicrotubules in polarized delivery of apical membrane proteins tothe brush border of intestinal epithelium. J Cell Biol 109:179—189,1989
155. HYNES RO, DESTREE AT: Relationships between fibronectin(LETS protein) and actin. Cell 15:875—866, 1978
156. HOLTHOFERH, MIETTINEN A, PASSIVO R, LEI-ITO VP, LINDRI E,ALTHAN 0, VIRTANEN i: Cellular origin and differentiation of
renal carcinomas: A fluorescent microscopic study with kidneyspecific antibodies, intermediate filament antibodies and lectins.Lab Invest 49:317—326, 1983
157. BAcHMANN 5, KRIZ W, KUHN C, FRANKE WW: Differentiation ofcell types in the human kidney by immunofluorescence micros-copy using antibodies to intermediate filament proteins and des-moplakins. Histochem 77:365—394, 1983
158. GRONE H, WEBER K, GRONE E, HELMCHEN U, OSBORN M:Coexpression of keratin and vimentin in damaged and regenerat-ing tubular epithelia of the kidney. Am J Pathol 129:1—8, 1987
159. GERSTENFELD LC, FINER MH, BOEDTKER H: Altered /3-actingene expression in phorbol myristate acetate treated chondrocytesand fibroblasts. Mol Cell Biol 5:1425—1433, 1985
160. HARTMAN AL, SAWTELL NW, LESSARD JL: Expression of actinisoforms in developing rat intestinal epithelium. J Histochem
Cyrochem 37:1225—1233, 1989161. VANDEKERCKHORE i, WEBER K: At least six different actins are
expressed in a higher mammal: An analysis based on the aminoacid sequence of the amino-terminal tryptic peptide. J Mo! Biol126:783—792, 1978
162. SHERWOOD AC, WILSON PD: Actin cytoskeleton in autosomaldominant polycystic kidney disease epithelial cell. (abstract) Kid-ney mt 37:229, 1989
163. KLEE CB: Ca2-dependent phospholipid-(and membrane-) bindingproteins. Biochem 27:6645—6653, 1988
164. SAWYER ST, COHEN S: Epidermal growth factor stimulates thephosphorylation of the calcium-dependent 35,000 dalton substratein intact A-431 cells. J Biol Chem 260:8233—8236, 1985
165. DAVIDSON FF, DENNIS EA: Biological relevance of lipocortinsand related protein inhibitors of phospholipase A2. BiochemPharm 38:3645—3651, 1989

Wilson and Sherwood: Tubulocys tic epithelium 463
166. FLOWER RJ: Lipocortin and the mechanism of action of theglucocorticoids. BrJ Pharmacol 94:987—1015, 1988
167. NAKATA T, SOBUE K, HIROKAWA N: Conformational change andlocalization of calpactin I complex involved in exocytosis asrevealed by quick freeze deep-etch microscopy and immunocyto-chemistry. J Cell Biol 110:13—25, 1990
168. WooDs A, COUCHMAN JR, HooK M: Heparan sulfate proteogly-cans of rat embryo fibroblasts. A hydrophobic form may linkcytoskeleton and matrix components. J Biol Chem 260:10872—
10879, 1985169. BAssoLs A, MASSAGUE J: Transforming growth factor /3 regulates
the expression and structure of extracellular matrix chondroitin!dermatan sulfate proteoglycans. J Biol Chem 263:3039—3045, 1988
170. THOMPSON KL, AssolAN R, ROSNER MR: Transforming growthfactor /3-increased the transcription of the genes encoding epider-mal growth factor and fibronectin in normal rat kidney fibroblasts.JBiol Chem 263:19519—19524, 1988
171. PANAYOTOU G, END P, AUMAILLEY M, TIMPI R, ENGEL J:Domains of laminin with growth-factor activity. Cell 56:93—101,
1989
172. PARRY G, CULLEN B, KAETZEL CS, KRAMER R, Moss L: Regu-lation of differentiation and polarized secretion in mammaryepithelial cells maintained in culture: Extracellular matrix andmembrane polarity influence. J Cell Biol 105:2043—2051, 1987
173. RAPRAEGER A, JALKANEN M, BERNFJELD M: Cell surface proteo-glycan associates with the cytoskeleton at the basolateral cellsurface of mouse mammary epithelial cells. J Cell Biol 103:2683—
2696, 1986174. WALSH-REITZ MM, GLUCK SL, WAACK 5, TOBACK FG: Lowering
extracellular Na concentration releases autocrine growth factorsfrom renal epithelial cells. ProcNatl Acad Sci USA 83:4761—4768,1986
175. STANTON B, KAI55LING 5: Regulation of renal ion transport andcell growth by sodium. Am J Physiol 257:F1—F10, 1989