Tuberculosis and Infection Control
55
ONLINE SELF-STUDY TUBERCULOSIS & INFECTION CONTROL UNC ENVIRONMENT, HEALTH & SAFETY
Transcript of Tuberculosis and Infection Control
ONLINE SELF-STUDY
TUBERCULOSIS & INFECTION CONTROL
UNC ENVIRONMENT, HEALTH & SAFETY

TB is an infection that is caused by Mycobacterium tuberculosis. M.TB has the potential to cause disease in every organ system, but most commonly affects the lungs. TB infects 1/3 of the world's population and causes approximately 1.7 million deaths each year.
TB was not a major public health problem until the industrial revolution. During this time, people lived in crowded urban conditions that aided the spread of TB.
2
Introduction
Introduction
TB has higher incident rates in the following groups:
o Blackso Asianso Pacific Islanderso Alaskan Nationso Foreign Born (Asia, Africa, Caribbean, Latin America)o Hispanicso Prison Inmateso Alcoholics and IV Drug Userso Elderlyo Household Contacts
3
Epidemiology
According to the CDC, TB Rates have been on a steady decline in the United States since 1993. In 2010, a total of 11,181 tuberculosis (TB) cases were reported in the United States; 296 of cases occurred in North Carolina.

TRANSMISSION
Tuberculosis is carried in airborne particles, known as droplet
nuclei, that are produced when persons with pulmonary or laryngeal tuberculosis sneeze, cough, or speak. Infection occurs when a susceptible person inhales droplet nuclei containing tuberculosis, which reach the alveoli of the lungs.
The majority of infectious patients have pulmonary disease; however aerosolization of droplet nuclei generated during surgical dressings of TB skin lesions has been implicated in the spread to healthcare workers. Cough – inducing procedures such as pentamidine treatments, bronchoscopy, and intubation/suctioning have shown to have the greatest risk of transmission for healthcare providers.
5
Transmission

Infection Routes and Symptoms
Pulmonary TB is characterized by destruction of lung tissue with the formation of infected lesions and cavities. Bacterial populations in cavities are very high and individuals with cavity disease are highly infectious.
In the first few weeks following initial infection, the mycobacteria multiply freely in the lungs. This process lasts for weeks and the bacteria are carried through the body by the bloodstream. In most cases, the immune system will not exhibit any clinical evidence of the TB disease. The only evidence of infection will be a positive reaction to the TB skin test, which usually occurs within 3 – 9 weeks after the initial infection. These individuals are not infectious to others. For a small portion, < 1% of newly infected persons, the initial infection progresses rapidly to clinical illness. Only approximately 5-10% of infected individuals will develop active disease at some point in their lives with the greatest risk during the two years following initial infection. Factors such as poor nutrition, immunosuppressive therapy, AIDS, and deterioration in health contribute to the progression from infection to active disease.
6
Transmission

Reinfection
Studies have shown that some HIV infected persons acquired infection with a new TB stain even while on treatment for their initial TB infection . However, except for the HIV-infected population, reinfection does not occur in developed countries with a low incidence rate of TB in the general population such as the U.S. Reinfection has occured in countries with a very high incidence of TB disease.
7
Transmission

THE TB SKIN TEST
Infection Routes and Symptoms
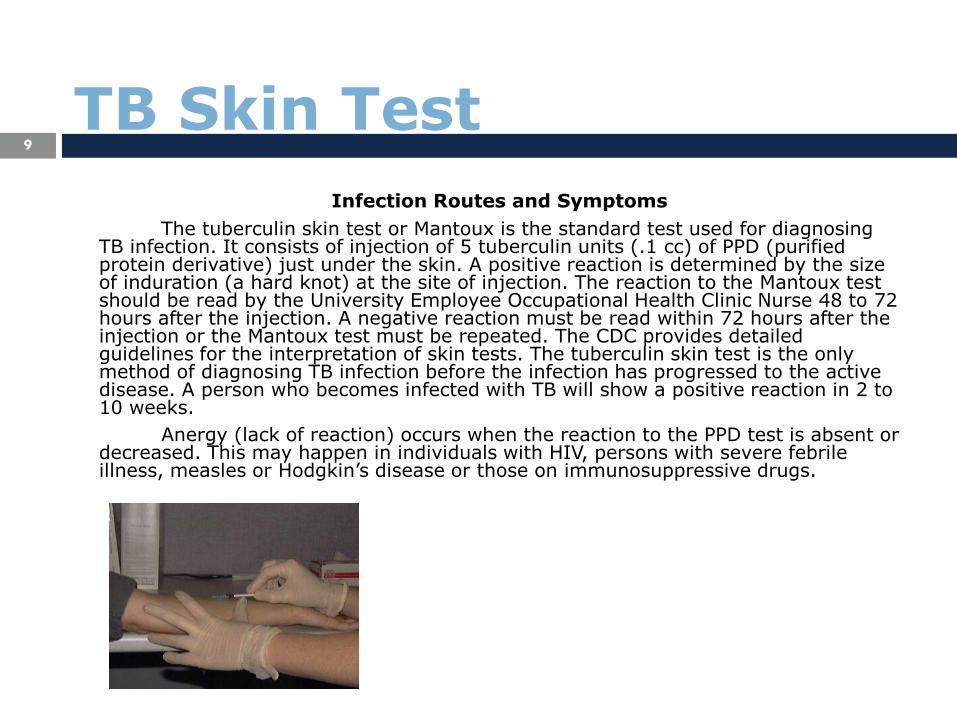
The tuberculin skin test or Mantoux is the standard test used for diagnosing TB infection. It consists of injection of 5 tuberculin units (.1 cc) of PPD (purified protein derivative) just under the skin. A positive reaction is determined by the size of induration (a hard knot) at the site of injection. The reaction to the Mantoux test should be read by the University Employee Occupational Health Clinic Nurse 48 to 72 hours after the injection. A negative reaction must be read within 72 hours after the injection or the Mantoux test must be repeated. The CDC provides detailed guidelines for the interpretation of skin tests. The tuberculin skin test is the only method of diagnosing TB infection before the infection has progressed to the active disease. A person who becomes infected with TB will show a positive reaction in 2 to 10 weeks.
Anergy (lack of reaction) occurs when the reaction to the PPD test is absent or decreased. This may happen in individuals with HIV, persons with severe febrile illness, measles or Hodgkin’s disease or those on immunosuppressive drugs.
9
TB Skin Test

Tuberculosis Screening
As part of a comprehensive tuberculosis control program, the
UEOHC screens every employee initially upon employment and annually for tuberculosis. This involves the completion of a tuberculosis screening form and placement of a tuberculin skin test (PPD). Employees with a documented history of a positive skin test will complete the tuberculosis screening form only. If an employee develops symptoms of tuberculosis disease, they should notify the UEOHC immediately.
10
TB Skin Test

TB Testing of Healthcare Personnel
All healthcare personnel will receive the tuberculin skin test upon employment. Excluded are those individuals who have had a previous positive reaction or who have completed therapy for active TB. The results of the PPD testing of healthcare personnel will be used in the risk assessment for the facility. Healthcare personnel are to be retested annually. If an employee is exposed to a potentially infectious patient and infection control procedures were not followed, he/she will be given the tuberculin skin test. A negative test is to be repeated after 12 weeks. If PPD induration is greater than 5 mm or symptoms of TB are present, the employee will receive a chest x-ray.
Exposed employees who have had a previous positive PPD are required annually to contact the UEOHC for TB symptom review. During the symptom review, TB follow up may be identified, (i.e. a chest x-ray).
11
TB Skin Test

New Employee Responsibility
All new employees must complete a TB screening questionaire as described in the Tuberculosis Control Plan (Appendix F). The history will provide the following information: history of PPD placement; history of treatment for positive PPD; history of active tuberculosis; and any presence of signs and symptoms of active TB. All employee healthcare records are confidential.
12
TB Skin Test

Continuous Employee Responsibility
All employees are responsible not only for having their annual tuberculosis screening but are also responsible for reporting to UEOHC when signs and symptoms of active tuberculosis occur. UEOHC staff will assist the employee with diagnosis and treatment. If diagnosed by their personal physician, the employee must inform the UEOHC of the diagnosis. This is necessary for making decisions regarding when the employee can safely return to work and identifying coworkers and patients that must be skin tested. UEOHC keeps information about the employee with tuberculosis confidential.
Healthcare workers who are HIV positive or immunocompromised due to medications or treatments should consult with UEOHC to evaluate work status and potential voluntary work reassignment to prevent tuberculosis exposure.
TB Skin Test13

TREATMENT OF TB

Treatment of TB15
Latent TB infection (LTBI) refers to individuals who are infected with M. tuberculosis but do not have actual disease. These individuals do not have any symptoms and are not infectious to others. Studies have shown that treatment of LTBI can substantially reduce the risk of TB infection progressing to disease. Treatment consists of antibiotic therapy. There are several treatment regimens available. Individuals with TB should be evaluated by the University Employee Occupational Health Clinic to discuss treatment options.

16
Symptoms of TB Disease
All healthcare workers must be aware of the signs and symptoms to rapidly identify potentially undiagnosed TB cases as well as the potential development of disease in themselves.
Symptoms of TB include:• A productive cough, lasting greater than 3 weeks• Fever, night sweats• Loss of appetite• Weight loss• Bloody sputum• Fatigue
Treatment of TB
Diagnosis
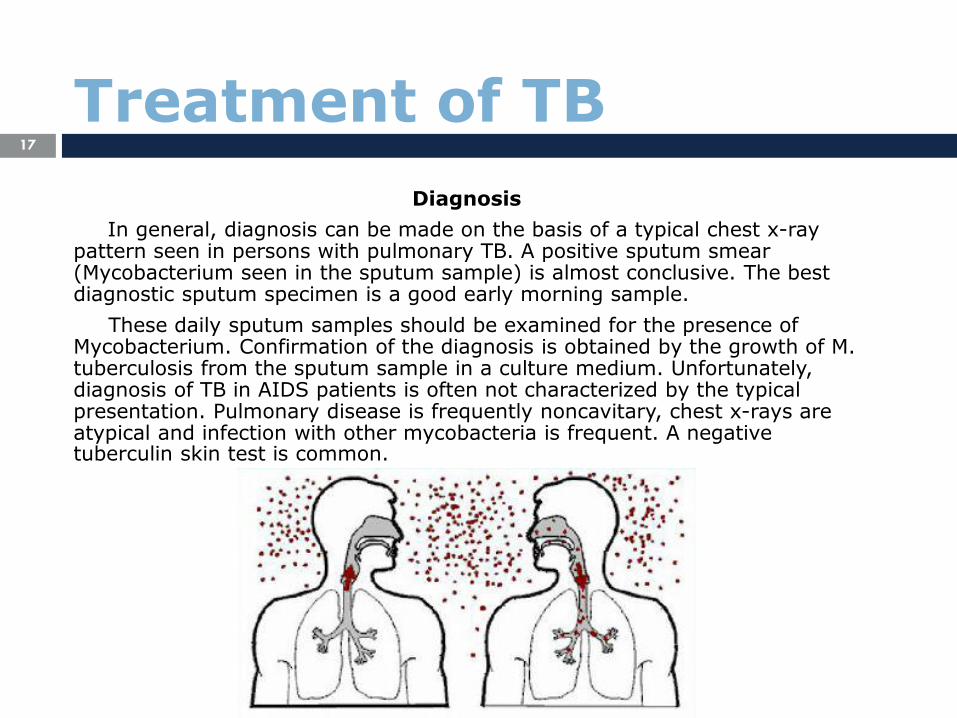
In general, diagnosis can be made on the basis of a typical chest x-ray pattern seen in persons with pulmonary TB. A positive sputum smear (Mycobacterium seen in the sputum sample) is almost conclusive. The best diagnostic sputum specimen is a good early morning sample.
These daily sputum samples should be examined for the presence of Mycobacterium. Confirmation of the diagnosis is obtained by the growth of M. tuberculosis from the sputum sample in a culture medium. Unfortunately, diagnosis of TB in AIDS patients is often not characterized by the typical presentation. Pulmonary disease is frequently noncavitary, chest x-rays are atypical and infection with other mycobacteria is frequent. A negative tuberculin skin test is common.
17
Treatment of TB

Combinations of the antibiotics isoniazid (INH),
rifampin ethambutol, streptomycin, and pyrazinamide (PZA) are used to effectively treat TB. Antibiotics for TB are available free from the health department. For an employee exposed at work, the antibiotic treatment will be covered by UNC's Workers' Compensation.
While on therapy, patients are monitored for side effects that may be caused by the antibiotics. Isoniazid (INH) has caused liver toxicity in some patients. This occurrence is rare for people under the age of 35, but has a somewhat greater incidence for people over 35. Liver function should be monitored in patients receiving treatment with INH. Liver toxicity is also the most important complication of rifampin treatment.
18
Treatment of TB
TB CONTROL PLAN

The policies and procedures for management of patients with known or
suspected tuberculosis is based upon guidelines from the CDC and OSHA regulations. The Tuberculosis Control Plan can be found at http://intranet.unchealthcare.org UNCH Infection Control Manual.
Early recognition and isolation of patients who may have infectious tuberculosis are critical elements in preventing transmission of disease. Patients with known or suspected tuberculosis should be placed on Airborne Precautions in a designated isolation room (see engineering controls below). Detailed guidelines for initiation and termination of isolation for tuberculosis can be found in the Tuberculosis Control Plan.
North Carolina’s public health laws require notification of the health Department within 24 hours of TB diagnosis. The physician should call the patient’s local Health Department and then complete a Communicable Disease Report Card and forward it to Hospital Epidemiology. The health department is responsible for skin testing the patient’s household members and other close contacts.
20
TB Control Plan

DRUG RESISTANCE
Factors that contribute to drug resistance are prior TB treatment, infection acquired in countries where resistance is prevalent, and non compliance with antibiotic therapy. Drug resistance should be suspected in any patient who does not have a rapid response to standard therapy. Healthcare workers are responsible for ensuring that their patients are compliant with therapy.
22
Drug Resistance
DISCHARGE

At the time of discharge from the hospital, the physician is responsible for notifying the patients’ local health department of their discharge and ensuring an adequate supply of medications until the patient has a follow-up visit. In addition, a follow-up appointment must be made for the patient with their local health department or other heathcare facility. It is important for this appointment to be scheduled as soon as discharge is anticipated to prevent discharge delays.
24
Discharge

ISOLATION FOR TB

Isolation Facilities
Appropriate isolation rooms are required for preventing the spread of infectious droplet nuclei. An isolation room must have 6-12 air exchanges per hour, directional air flow from the hallway to the room and direct exhaust of the room air to the outside.
In the event that the patient must leave the isolation room for tests or procedures, the patient should wear a respirator.
26
Isolation for TB

Isolation Procedures
Patients placed in TB isolation will be instructed in procedures to prevent TB transmission, and the reasons for their being placed in isolation.
The door to the room must always be kept closed. Patients who have active TB will be scheduled to avoid contact with immunocompromised patients. Cough inducing procedures should be avoided if possible, and if necessary, done in TB isolation facilities. Thirty minutes should pass before the room is utilized for other patients.
TB isolation may be discontinued when the patient is on effective therapy, is improving clinically, and has 3 consecutive negative sputum AFB smears.
27
Isolation for TB

RESPIRATORY PROTECTION

Administrative controls, isolation facilities and
procedures may not fully protect health care workers from
infectious droplet nuclei in settings where high risk
procedures are performed. TB respirators are required for
healthcare workers who enter rooms where patients with
active TB are being isolated.
Respirator devices will meet the following criteria:
o Ability to filter particles 1 µm in size with a filter efficiency of > 95%
o Ability to be quantitatively fit tested for face-seal leakage of no greater
than 10%
o Respirators with exhalation valves do not filter exhaled air and
therefore are not to be used by operating room personnel or patients
with TB.
29
Respiratory Protection
Respiratory Protection Program
The respiratory protection program includes medical screening, annual fit testing, and annual training. Medical screening is conducted to determine whether the employee is physically able to wear a respirator. The employee must complete the "Medical Evaluation for Respirator Use" form found in the Environment Health and Safety Manual. Completed forms should be taken to University Employees Occupational Health Clinic at the time of the fit-testing appointment. A fit test is used to determine whether the respirator wearer is able to obtain a satisfactory fit.
A respirator cannot be worn by healthcare workers with facial hair that comes between the sealing surface of the mask and face, or if facial hair interferes with valve function. Bearded healthcare workers should contact Environment, Health and Safety to obtain alternative respiratory protection. Training will be provided to personnel who receive respirators and will include selection, use and storage of respirators as well as their limitations.
30
Respiratory Protection

INFECTION CONTROL
Infection Control Goal
The goal of infection control is to prevent
infections among patients and personnel. To
accomplish this goal, every employee needs to
have an understanding of the basic principles of
disease transmission and methods to prevent
infections.
32
Infection Control

Health Care Associated Infections
Health care associated infections are a major source of morbidity and mortality, affecting more than 2 million patients per year in the United States. The economic burden is estimated to be more than 8 billion dollars per year. At UNC Clinics and UNC Hospitals, the most frequently occurring health care associated infections are those related to IV devices (bloodstream), urinary tract infections pneumonia, and surgical wound infections.
Healthcare workers play a vital role in the prevention of health care associated infections by practicing basic infection control measures. It is important to recognize that the principles of infection control have not changed but the challenges of infection control are greater today than ever. Patients are becoming infected with antibiotic resistant organisms such as multi-drug resistant tuberculosis (MDR-TB) or Vancomycin-resistant enterococcus (VRE) and oxacillinresistant staphylococcus aureus (ORSA). Strict adherence to infection control practices is essential to prevent the spread of these organisms. Infection control also plays a vital role in the care of the patient who may be immunosuppressed due to organ transplantation or AIDS, and those that are undergoing invasive procedures now common in most ICU settings. Incorporating good infection control practices, such as the simple act of handwashing, is an essential component of modern healthcare.
33
Infection Control

Elements of the Infectious Process
In order for an infection to occur, certain elements must be present. These elements include:
o an infectious agent such as a virus, bacteria, or fungus
o a method of travel or transmission such as carriage on respiratory droplets or by transient carriage on hands
o a susceptible host or person at risk of acquiring the infection
o a means of entering and exiting the human body such as the respiratory tract and the gastrointestinal tract.
The principles of infection control are based upon the control of the above elements, thereby preventing the occurrence of an infection. For example, the appropriate cleaning and disinfection of endoscopes removes potentially infectious agents and thereby prevents infection. The following infection control guidelines are designed to assist the healthcare worker in preventing the transmission of infectious agents among patients and personnel.
34
Infection Control

Immunizations
Immunizations serve as a tool to protect a person from being
a "susceptible host". With adequate immunization, the person’s
immune system produces protective antibodies so that infection
is prevented or clinical disease does not develop. All employees
are required to have documented immunity to measles, mumps,
rubella, and varicella. Hepatitis B vaccine is provided for
employees with occupational exposure to blood and body fluids.
All employees involved in patient care are strongly encouraged
to receive an annual flu vaccine. All of these vaccines are
available from the University Employee Occupational Health
Clinic and is free to employees.
35
Infection Control
Infection Control Manual
The Infection Control Manual contains numerous infection control
policies and serves as an important resource for employees in the
prevention of infection. The Exposure Control Plan for Bloodborne
Pathogens and Tuberculosis can be found in the Infection Control
Manual. Infection Control Manuals are available in all patient care
areas of the Hospitals and University clinics. Additionally, these
policies can be found at the EHS website TB Exposure Control Plan,
Exp. Control Plan for BBP, or UNC Healthcare’s intranet –
http://intranet.unchealthcare.org.
36
Infection Control

TYPES OF PRECAUTIONS

Handwashing: Simple and Effective
Handwashing is the simplest but most important means of
preventing the spread of infection.
Every healthcare worker should wash their hands for fifteen
seconds using an approved antimicrobial soap (Bactoshield or
Alcare) and water or waterless alcohol agent if hands are not
visibly soiled:
o before and after patient contact
o after removing gloves
o upon arriving and departing work
o whenever skin contamination is suspected
No artificial nails or extenders should be worn by those who
provide direct patient care.
38
Types of Precautions
Standard Precautions
Standard Precautions are followed for all patients regardless
of their diagnosis or presumed infectious status. Standard
Precautions apply to:
o blood
o all body fluids, secretions, and excretions (except sweat)
o nonintact skin
o mucous membranes
Healthcare workers must recognize that all body fluids may
be potentially infectious and learn to protect themselves from
direct contact with these fluids.
39
Types of Precautions

Isolation Precautions
Isolation precautions are designed to prevent the transmission
of infection based upon the recognized method of transmission
for the infecting organism. The precaution categories are
Standard Precautions, Contact Precautions, Droplet Precautions,
and Airborne Precautions.
40
Types of Precautions

Contact Precautions
Contact Precautions are followed to prevent infections that are
transmitted by direct body surface to body surface contact or via indirect
contact with a contaminated object. Examples of infections transmitted via
the contact route include rotavirus and infections caused by antibiotic-
resistant bacteria.
Contact precautions are followed when the patient must be placed
in a private room. Gloves are worn by those entering the room and removed,
with hands washed thoroughly with an antimicrobial soap upon exiting. A
gown is required to be worn if contact with potentially contaminated surfaces
(e.g., direct contact with patient, bed linen, beside table) is anticipated.
41
Types of Precautions

Droplet Precautions
Droplet Precautions are used to prevent transmission of infections
spread by respiratory droplets. Infectious droplets are released when the
infected person sneezes or coughs. These droplets are heavy and usually fall
rapidly within 3 feet of the patient. Examples of infections transmitted via the
droplet route are pertussis (whooping cough) and meningococcal meningitis.
When following droplet precautions the infected patient must be placed in
a private room. All people entering the room must wear a surgical mask to
prevent the infectious droplets from impacting mucous membranes.
42
Types of Precautions

Airborne Precautions
Airborne Precautions are used to prevent the transmission of infections spread by the airborne route. These infectious particles are so small that they can remain suspended in the air for long periods of time and carried on air currents. Examples of infections spread by the airborne route include varicella (chickenpox), tuberculosis and measles. When following airborne precautions the patient must be placed in a private room with special ventilation (details regarding ventilation are included in the Isolation Precautions Policy located in the Infection Control Manual). Respirators are worn by personnel if the patient has or is suspected of having tuberculosis. Respirators are worn for chickenpox or measles only if the employee entering has not had the disease or has not been immunized. Visitors should wear a tightfitting surgical mask if the patient has or is suspected of having tuberculosis. Surgical masks are worn for chickenpox or measles only if the visitor has not had the disease or has not been immunized.
43
Types of Precautions

Protective Precautions
Protective Precautions are designed to protect the patient with
impaired resistance to infection. The patient’s susceptibility to
infection is dependent upon the severity and duration of their
immunosuppression.
o The patient must be placed in a private room that has special positive
pressure ventilation.
o The patient should wear a tight-fitting surgical mask when they leave
their room.
o Additional guidelines should be indicated on the Protective Isolation
sign posted outside the patient’s door.
44
Types of Precautions

Isolation Precautions Signs
An Isolation Precautions sign will be placed in a visible location
outside the patient’s room when Contact, Droplet, Airborne
Precautions or Protective Precautions are required. All
employees and visitors must carefully follow the instructions
provided on the sign to prevent disease transmission to
themselves and to other patients.
45
Types of Precautions

OTHER INFECTION CONTROL INFORMATION
Infectious Agents and Bioterrorism
Unfortunately, the threat of biological agents as a means of
terrorism exists in our society. The UNC Health Care System and
Infection Control have a written response plan to address such
an event. Employees can review the Bioterrorism Plan at the
Hospitals’ website, http://intranet.unchealthcare.org.
47
Other Infection Control Information

Renovation/Construction
Renovation and construction activities within the Hospitals
generate dust and debris that must be contained and removed
carefully. Construction dust, including dust released from the
removal of ceiling tiles, can contain molds capable of causing
serious infections in immunocompromised patients (i.e., burn,
transplant, patients requiring Protective Precautions). Plastic and
solid wall barriers are used to contain dust and debris within the
construction site. Employees should be aware of the importance
of these barriers and refrain from altering or damaging the
barrier in any way. If a barrier is observed to be damaged or
inadequate, the employee should contact their supervisor and
Infection Control.
48
Other Infection Control Information

Storage of Patient Supplies
Patient supplies must be stored in a manner that protects them
from contamination and assures their quality. The following
guidelines will ensure safe storage and compliance with healthcare
facility regulations.
o No patient care supply should be stored on the floor (even if still in the
shipping carton).
o Patient care supplies must be stored at least 8 inches from the floor if stored
on open shelving.
o Sterile patient care supplies must be stored at least 5 inches from the ceiling
if stored on open shelving.
o If patient care supplies are stored in the Dirty Utility Room, they must be
stored within closed cabinets.
o No patient care supplies can be stored on an open shelf or closed cabinet
that is beneath a sink.
o Always inspect supplies for expiration dates and discard if expired.
49
Other Infection Control Information
Single-Use Patient Care Devices
Many patient care items are intended for single use only. This
means that the item or instrument should be disposed of
immediately after the initial use. FDA regulations prohibit the
resterilization and reuse of single-use medical devices. All
employees should be knowledgeable of a medical device’s
intended use and follow manufacturer’s directions for use and
disposal. If you are uncertain regarding whether a device is
intended for single or multiple uses, contact your supervisor or
Infection Control.
50
Other Infection Control Information

Refrigerators
Safe refrigeration applies not only to foods but also to
maintaining medications and specimens at appropriate
temperatures. It is important to remember that foods/drinks,
medications, and specimens should be stored in separate
refrigerators. Under no circumstances should specimens and
foods/drinks be stored in the same refrigerator. When space is
limited, foods/drinks and medications can be stored in the same
refrigerator after inspection and approval by Hospital
Epidemiology. Every refrigerator used for patient care items
should have a thermometer inside and the temperature checked
and recorded daily. If the temperature falls outside the
appropriate range (33° - 45° F), contact the maintenance
department to inspect the refrigerator.
51
Other Infection Control Information

Children Visitation
In order to prevent the potential transmission of childhood
diseases such as chickenpox to patients and employees, certain
visitation restrictions apply to children 12 years of age or
younger. Any child who may be sick or incubating a
communicable disease should not visit within the Hospitals. In
addition, no children can visit in an ICU, the Burn Center, the
Bone Marrow Unit, or visit a patient who requires Isolation
Precautions without a physician’s order and communicable
disease screening. When children visit in an isolation room, they
must wear any protective garments required and must be
accompanied by an adult responsible for their supervision and
compliance with the required precautions.
52
Other Infection Control Information

Sick Leave
An obvious but often overlooked component of infection control
is to stay home when you are sick. Employees should exercise
good judgment and report to their supervisor concerning their
ability to work. When needed, the UEOHC can assist in
evaluating an employee’s work status. Employees diagnosed
with a communicable disease such as chicken pox or zoster
(shingles), should report the diagnosis to UEOHC. UEOHC will
determine the need for screening of any exposed coworkers and
determine when the employee can return to work.
53
Other Infection Control Information

COMPLETION AND POST TEST
You have completed this self-study unit. Please call
Environment, Health and Safety if you have any questions or
want further discussion.
In order for you to receive credit for this course, you
need to complete a short multiple choice test. To take this test,
you may click on the highlighted post-test now.
55
Completion and Post Test













![Infection Control Guidelines in Tuberculosis [compatibility mode]](https://static.fdocuments.net/doc/165x107/54532ec8af795984568b5d48/infection-control-guidelines-in-tuberculosis-compatibility-mode.jpg)