Tuberculosis and Biologicscenterfortuberculosis.mayo.edu/uploads/7/1/7/3/71735537/... · ©2014...
51
©2014 MFMER | slide-1 Tuberculosis and Biologics Speaker: Leonard H. Calabrese, D.O.
Transcript of Tuberculosis and Biologicscenterfortuberculosis.mayo.edu/uploads/7/1/7/3/71735537/... · ©2014...

©2014 MFMER | slide-1
Tuberculosis and Biologics
Speaker: Leonard H. Calabrese, D.O.

©2014 MFMER | slide-2
DISCLOSURES
• CONSULTANT Genentech, BMS, Abbvie, Jansen UCB Pfizer Regeneron Crescendo

©2014 MFMER | slide-3
Tuberculosis and Biologics
• Concept of IMIDS and development of biologics
• TNF inhibitors
• Biology
• Epidemiology of TB
• MOA implications
• Other Biologics
• T cell, B cell, IL1, IL6, IL17, IL12/23
• Jakatinibs
• Screening recommendations and controversies

©2014 MFMER | slide-4
Damage / Destruction / Symptoms
(RA, SLE, PsA, IBD, AS, MS)
Inflammation
(TNF, IL-1, IL-6, IL-17,
IL-23, IL-18, IL-15, Others)
Immune-Mediated Inflammatory Diseases
Initiation
Susceptibility
Triggers
Accelerants
Immune responses Adaptive Innate
DM, CHF, Alzheimer's, Transplant, Sepsis, Allergy, Vasculitis, ASO, HIV
Slide credit: clinicaloptions.com

©2014 MFMER | slide-5
Evolution of Biologics for IMIDS
1940s
Gold
Hydroxychloroquine
Corticosteroids
Etanercept
1950s 1960s 1970s 1980s 1990s 2000s
D-Penicillamine
Methotrexate
Auranofin
Azathioprine
Infliximab
Adalimumab
Golimumab
Certolizumab
Anakinra
Leflunomide
Rituximab
Abatacept
Tocilizumab
Ustikinumab
Belimumab
Natalizumab
Canakinumab
Rilonacept
Tofacitinib
Vedolizumab Secukinumab
Slide credit: clinicaloptions.com

The History of TNF and the Development of
Anti-TNFs for Inflammatory Diseases
1893 1975
Coley notes
tumor necrosis
1975 Old
characterizes
TNF
1985 1988 1991 1998 1999 2006 2016
Beutler isolates
& sequences
cachectin /
Aggarwal TNF
1982-1988
Analysis of
inflammatory
synovial fluid
TNF, Il-1, IL-6
First TNFR- Ig
fusion protein
developed
1993-1999
Development
of Etanercept
1998 Infliximab
1999
Adalimumab
Over 3.0 Million
treated
Certolizumab
Golimumab
William B. Coley
(1862-1936)
hemorrhagic regression in 25%In vitro:
Molecular: 56 °C stable, ~150 kDa

©2014 MFMER | slide-7
Tumor Necrosis Factor (TNF-α)
• TNF (alpha) translated as a 233 aa, 26kD pro-protein - initially membrane bound /cleaved by TACE
• Secreted as a 17kD molecule that homotrimerizes to be active
• Present in pico to atomolar concentrations
• Produced by a wide variety of cells in response to variety of danger signals
• Membrane-bound and soluble forms of TNF-α


Effects of Low TNF Concentrations
Low
TNF
Activation, microbicidal activity
Eosinophils
Activation,IL-1, IL-6, IL-8, GM-CSF, microbicidal activity, release from bone marrow
Adhesion molecules
(ICAM-1),
extravasation
T, B lymphocytes
IL-6, TNF, prostaglandins, GM-CSF
chemokines, microbicidal activity
Macrophages
Neutrophils
Ab production, proliferation,
GC formation
Activated B
lymphocytes
Apoptosis, survival
IL-2R, IFNγ, IL-4, IL-5
Activated ThO
Antiviral state, ICOSL Host cell
Apoptosis, survival,
cytotoxicity
Activated CTL
Target cell MHC class I
MHC class II Antigen Presenting Cell

Effects of Moderate TNF Concentrations
Moderate TNF
Bone remodeling
IL-6, IL-8, TNF
GM-CSF, IL-6,
IL-8 proliferation
Endothel., Fibrocytes
Hematopoisis
Smooth muscle
Proliferation, collagen Epithelium
IL-1, IL-6
Macrophages
Fever, prostaglandins Brain
Bone marrow Acute phase
proteins
Hepatic cells
Prostaglandins,
TNF, GM-CSF, collagenase,
proliferation
Stromal cells
Coagulation Blood vessels
Glucocorticoids Adrenal glands
Apoptosis, necrosis due to
blood vessel blockage
Tumor cells
Osteoblasts Alk. phosphatase
Collagenase Osteoclasts

Effects of High TNF Concentrations
High TNF
IL-1, IL-6, TNF
Bone Destruction Fibrosis
Endotoxic
Shock
Osteoclasts Fibroblasts
Multiple Cell Types

©2014 MFMER | slide-12
Etanercept
(Enbrel®)
Infliximab
(Remicade®)
Human
recombinant
receptor/Fc fusion
protein
Monoclonal
antibody
Adalimumab (Humira®)
Golimumab (Simponi®)
= murine = human
Three classes of anti-TNF and 5 drugs
Adapted from Hanauer SB. Gastroenterol Disord 2004;4(Suppl. 3):S18-24.
IgG1
Fc IgG1
Fc
Fab
Receptor
PEGylated
humanized
Fab′ fragment
Certolizumab
pegol
(Cimzia™)
PEG

©2014 MFMER | slide-13
The Role of TNF in Tuberculosis
• TNF is critical in the formation of granulomas and for maintaining their structural integrity
• TNF is a macrophage-activating factor
• Excessive and prolonged inhibition of TNF signaling leads to exacerbation of TB
0 10 20 30 40 50 0
2
4
6
8
10
100 200 300
Wildtype
TNF knockout
Anti-TNF mAb
Days After Infection
Log
10 c
fu/L
ung
Flynn, JL, et al. Immunity. 1995;2:561-572.
Mohan VP, et al. Infect Immun. 2001;69:1847-1855.

©2014 MFMER | slide-14
TB in infliximab treated patients Keane NEJM 345:1098-1104,2001

©2014 MFMER | slide-15
RA and Tuberculosis l August 2010 l 15
TNF- Antagonist Therapy and TB
• Atypical clinical presentation
• 50% extrapulmonary
• 15%–20% disseminated
• Median time to onset
• Infliximab (INF)=12 weeks; (range, 1–52 weeks)1
• Etanercept (ETN)=11.5 months; (range, 1–20 months)2
TNF=tumor necrosis factor
1. Keane J et al. N Engl J Med. 2001;345:1098-1104. 2. Mohan AK et al. Clin Infect Dis.
2004;39:295-299.

©2014 MFMER | slide-16
Hematologic Events
Addition of Warning Information in Anti-TNF Labels Over Time
Infections Sepsis
Hypersensitivity
Neurologic Events
Malignancies
Tuberculosis
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
CHF
Hepatotoxicity
HSTCL
HBV
ENBREL® (etanercept) Prescribing Information, Immunex Corporation.
HUMIRA® (adalimumab) Prescribing Information, Abbott Laboratories.
CIMZIA® (certolizumab pegol) Prescribing Information, UCB Inc.
FDA web site. Available at: http://www.fda.gov.
REMICADE® (infliximab) Prescribing Information, Centocor Ortho Biotech, Inc.
SIMPONI™ (golimumab) Prescribing information, Centocor Ortho Biotech, Inc.
Data collected during clinical trials and postmarketing surveillance
Pediatric malignancy
Leukemia
Invasive fungal infections
Nu
mb
er
of
Pa
tie
nts
Ex
po
se
d (
in t
ho
us
an
ds)
400
200
0
800
600
1,000
1,200

©2014 MFMER | slide-17
Tuberculosis
TB in US
6
TB in US
Crohn Inflix
9
TB in US RA
on Infliximab
41 +
TB in all non US
RA and Crohn’s patients
224
TB in RA
US pts
6
TB in US
high risk groups
>32
Incidence of TB per
100,000 pts years
Dye C et al, JAMA 1999
+Wolfe, Arth & Rheum 2001
*Gomez-Reino Arth Rheum 2003
TB in SPAIN
Infliximab
1,893*

©2014 MFMER | slide-18
TB Risk
• RA TB risk based on pop. risk2,3
• Swedish RA patients (low risk): RA patients have 2-fold increase of TB2
• Korean RA patients (high risk): have a 9-fold increase in TB3
• TNF inhibitors magnify the risk of TB from 9- to over 30-fold
1. Winthrop K. EULAR 2005, #SP0005; 2. Askling J, et al. Arthritis Rheum 52:1986-92, 2005 3. Seong SS, et al. 2007 Apr;34(4):706-11
Relative Risk
9
2
1
General population
RA no TNF-antagonist
RA with TNF-antagonist
30
Korea Sweden
No TNF
No TNF
+TNF
+TNF
NL

©2014 MFMER | slide-19
Anti-TNF and tuberculosis (TB): reactivation of latent TB
Keane J, et al. N Engl J Med. 2001;345:1098-1104
Infusion Number
% of Patients
0
20
40
60
1 2 3 4 5 6 7 8 9 10
• 70 cases of TB after infliximab
• TB occurs early after treatment

©2014 MFMER | slide-20
TNF Antagonists and TB Risk
Wallis R., et al., Lancet ID, 2008.
Infliximab Adalimumab E:I
Wallis et al (AERS) 17 weeks (248) 48 weeks (39) 1:2·8
Wolfe et al (NDB) 21 weeks (4) ~ n/a
Keane et al (AERS) 12 weeks (70) ~ n/a
Askling et al (ARTIS) 19 weeks (11) 32 weeks (6) 1:1·7
Brassard et al (PharMetrics) 17 weeks (19) 79 weeks (32) 1:4·6
Total (weighted mean) 16·2 weeks 59·6 weeks 1:3·7
Data are median time to onset (number of cases). Patients treated for any indication are included.
AERS=US Food and Drug Administration Adverse Event Reporting System. ARTIS=Anti-Rheumatic
Treatment in Sweden. I:E=Infliximab to etanercept ratio. NDB=National Databank for Rheumatic
Diseases. RATIO=Recherche sur Anti-TNF et Infections Opportunistes.
Time to Onset of Tuberculosis After Initiation of TNF
Antagonist Therapy

©2014 MFMER | slide-21
Differential Risk of TB Between Antibodies and Receptor Constructs
Numerous studies demonstrate differential effect in SIR for granulomatous infections between Abs (INFLX) and receptor (ETN) with lesser data n other molecules
Progression of M tuberculosis infection
Wallis R Lancet ID 2008,
Infliximab Etanercept I:E p value
Aspergillosis 8·63 (17) 6·19 (7) 1·39:1 0.243
Candidiasis 10·15 (20) 5·31 (6) 1·91:1 0.061
Coccidioidomycosis 5·58 (11) 0·88 (1) 6·34:1 0.013
Cryptococcosis 5·08 (10) 7·08 (8) 0·72:1 0.179
Histoplasmosis 18·78 (37) 2·65 (3) 7·09:1 <0.0001
Listeriosis 8·63 (17) 0·88 (1) 9·81:1 0.0006
Non-tuberculosis myocobacterioses 11·17 (22) 6·19 (7) 1·80:1 0.066
Nocardiosis 3·55 (7) 0·88 (1) 4·03:1 0.090
Salmonellosis 0 (0) 1·77 (2) n/a 0.031
Tuberculosis 53·81 (106) 28·32 (32) 1·90:1 <0.0001

©2014 MFMER | slide-22
RA and Tuberculosis l August 2010 l 22
Adapted from Dixon WG et al. Ann Rheum Dis. 2010:69:522-528.
UK Biologic Registry Patients On Drug*
DMARD
n=3232
All TNFi
n=10,712
ETN
n=5521
INF
n=3718
ADA
n=4857
Person-y 7345 28,477 12,744 8069 7634
Cases of TB (n) 0 27 5 11 11
Rate/100,000
person-y (95% CI) 0
95
(63–138)
39
(13–92)
136
(68–244)
144
(72–258)
IRR, adjusted for
age, sex, entry year
(95% CI)
-- -- Referent 3.1
(1.0–9.5)
4.2
(1.4–12.4)
*On drug: patient-years and adverse events were attributed to each drug only while the patient was actively receiving that drug.
TB Risk in Anti-TNF Therapy: Numbers and Rates of Incident TB, Including Switchers

©2014 MFMER | slide-23
RATIO (Research Aligned on Tolerance of bIOtherapies): a French prospective observatory
• Collections of all cases of:
• Opportunistic infections including TB
• Lymphomas
• Occurring on anti-TNF whatever the indication of use from February 2004 to February 2007 all over France
• Number of patients treated with anti-TNF in France during the 3 year 2004–2006 period
• 57,711 patients-year
• Mean age 53.2 (SD 15.8)
• Sex ratio : 49.1 % of males
• Repartition between the drugs during the 3 year 2004–2006 period
• 49% etanercept
• 33% infliximab
• 18% adalimumab
Tubach et al, Arthritis Rheum. 2009;60:1884-1894.

©2014 MFMER | slide-24
69 TB cases for 3 years: Clinical characteristics
TB cases (n=69)
Age (years) 58.5 ± 15.4 (61.0)
Median time since first anti TNF treatment start 12.0 months
Median time since last anti TNF treatment start 9.9 months
Underlying inflammatory disease
Rheumatoid arthritis
Ankylosing spondylitis
Psoriatic arthritis
Crohn’s disease or UC
Cutaneous psoriasis
Behçet’s disease
40
15
3
9
1
1
Duration of the underlying inflammatory disease before TB
(years)
11.2 ± 8.8 (8.3)
Tubach et al, Arthritis Rheum. 2009 Jul;60(7):1884-94.

©2014 MFMER | slide-25
Risk factors of TB
• Tuberculin Skin Test result
• > 10 mm: 4
• Between 5 and 10 mm: 11
• < 5 mm: 30
• Unknown or not done: 24
• TST < 5 mm: 30/45 (66%)
• No case in patient with correct previous prophylactic anti-TB
• In France the most common prophylactic regimen is isoniazid + Rifampicin for 3 months
Tubach et al, Arthritis Rheum. 2009 Jul;60(7):1884-94.

©2014 MFMER | slide-26
RATIO: Anti-TNF therapy and non-TB opportunistic infections
• Median time to occurrence of non-TB OI after start of anti-TNF
• 16.2 (6.0–26.0) months
• Median time since start of last anti-TNF
• 8.7 (3.1–20.4) months
• Underlying disease
• RA – 26
• SpA – 3
• Inflammatory colitis – 8
• Psoriasis – 1
• Other – 5
9.3
23.3
67.4
0
10
20
30
40
50
60
70
80
90
100
Etanercept Adalimumab Infliximab
Pro
po
rtio
n o
f p
ati
en
ts (
%)
Last anti-TNF received
(n=43)
Salmon-Ceron, et al. Ann Rheum Dis. 2011 Apr;70(4):616-623.

©2014 MFMER | slide-27
Analysis of the Estimation of the Standardized Incidence Ratio (SIR) for the Risk of Tuberculosis
Tubach, et al., Arth Rheum, 2009.
Risk of Tuberculosis in RA (N=40) Risk of Tuberculosis in SPA (N=18)
Risk is lower than in the
French population
Risk is higher than in the
French population
Only Adalimumab or
only infliximab
Only Etanercept
Adalimumab or
infliximab
Etanercept
All anti-TNF
SIR=26.2 [18.4-31.2] p<0.0001 n=31
SIR=24.9 [17.9-34.5] p<0.0001 n=36
n=0
SIR=2.1 [0.8-5.7] p<0.13 n=4
SIR=12.4 [9.1-16.9] p<0.0001 n=40
0 10 20 30 40
STR
Risk is lower than in the
French population
Risk is higher than in the
French population
Adalimumab
or infliximab
Etanercept
All anti-TNF
SIR=15.1
[9.4-24.3]
p<0.0001 n=17
SIR=1.35
[0.2-9.6]
p<0.77 n=1
0 10 20 30 40
STR
SIR=9.7
[6.1-15.4]
p<0.0001 n=18

©2014 MFMER | slide-28
Risk of TB with Anti-TNF
Tubach, et al., Arth Rheum, 2009.
Time from Onset of Last Anti TNF Treatment and First Symptoms of
Tuberculosis According to the Last Anti TNF Received
Time from onset of last anti TNF treatment (months)
Cum
ula
tive f
requency o
f
tuberc
ulo
sis
0 6 12 18 24 30 36 42 48 54 60 0
10
20
50
60
70
30
40
Total
Infliximab
Adalimumab
Etanercept

©2014 MFMER | slide-29
RA and Tuberculosis l August 2010 l 29
Nontuberculous (NTM) Disease
• Environmental mycobacteria
• Lung, skin and soft tissue, disseminated disease
• M. avium, M. kansasii, M. chelonae, M. abscessus
• Surveyed IDSA EIN
• One-fourth of US infectious disease specialists
• Reported 1876 TB or NTM cases
• 49 (2.6%) associated with biologics
• 32 cases NTM vs 17 TB
• Mycobacterium avium complex was most common (n=16)
EIN=Emerging Infections Network; IDSA=Infectious Diseases Society of America

©2014 MFMER | slide-30
30
*In this case etanercept was used as well, but symptoms worsened while the patient received INF. ND = no data available; NC = no cases identified. Tsiodras S, et al. Mayo Clin Proc. 2008;83(2):181-194.
Invasive Fungal Infections with TNF Inhibitor Therapy
• MEDLINE and PubMed database search from 1966-2007 (N = 281)
• Median time until onset of invasive fungal infection:
• INF: 55 days
• ETN: 144 days
• Median age of patient when developing invasive fungal infection was 58 years
• Histoplasmosis most prevalent invasive fungal infection (30%)
• Pneumonia was the most common pattern of infection (32%)
• 29 fatalities (32%) among the 90 cases for which outcome information was available of the total 281 cases
11 44 226 Total
2 1 3 Tinea or pityriasis
versicolor (n=6)
NC NC 1 Prototheca species (n=1)
NC NC 1* Sporothrix species (n=1)
4 8 72 Histoplasma species (n=84)
NC 2 27 Coccidioides species (n=29)
ND ND ND Blastomyces species (n=2)
1 10 17 Cryptococcus species (n=28)
1 9 54 Candida species (n=64)
1 NC 3 Zygomycetes (n=4)
2 14 48 Aspergillus species (n=64)
ADA ETN INF Infectious Agents
Fungal Infections Associated with TNF Inhibitor Therapy

©2014 MFMER | slide-31
RA and Tuberculosis l August 2010 l 31
More TB Risk With Monoclonals?
• Drug mechanisms differ
• Greater TNF- binding
• Transmembrane and soluble TNF-
• Forms stable complex
• Longer half-life
• Apoptosis of monocytes and T lymphocytes
• Interferon-gamma downregulation
• Differential granuloma penetration

©2014 MFMER | slide-32
Differential Effects on TNF Blockers on TB Immunity - Results
Infliximab and adalimumab block T cell activation, whereas etanercept does not
T cell activation (CD69 expression)
Infliximab and adalimumab reduced the proportion of TB-reactive T cells by 50 to
70%, and of PHA-reactive T cells, by 30 to 47% (P<0.05). Etanercept had no
effect.
Wallis R., et al., J. Inf. Dis 194:486-92, 2006.
Stimulus M.tb CF
Cell type CD4 CD4 CD8
PHA
No TNF blocker 0.73% 14.4% 11.1%
Etanercept 0.60% 15.1% 9.1%
Adalimumab 0.37% 10.5% 7.8%
Infliximab 0.22% 10.1% 5.9%
% CD69 + cells at 24 hrs

©2014 MFMER | slide-33
RA and Tuberculosis l August 2010 l 33
Interferon- Downregulation
Adapted from Saliu OY et al. J Infect Dis. 2006;194:486-492.
Drug Level
IFN
-γ, %
Co
ntr
ol V
alu
e
ETN
ADA
INF
70
90
None Trough Peak Supra
20
30
40
50
60
80
100

©2014 MFMER | slide-34
TNF necessary for granuloma homeostasis and especially
membrane TNF on monocytes and lymphocytes
Why a difference of effects on granuloma between Mc Abs and the soluble receptor ?

©2014 MFMER | slide-35
CFP10
Activation of specific anti-TB T cells on anti-TNF
• In patients with latent TB, addition of anti-TNF to a culture of specific anti-TB T cells
• more important of specific T-cell activation with monoclonal antibodies
200
160
120
80
40
0
0 0.4 1 4 10 40 mg/ml
Pro
life
rati
on
(S
I)
CFP10
40
30
20
10
0
0 0.4 1 4 10 40 mg/ml
IFN
gam
ma
(n
g/m
l)
Ifx
Ada
Eta
In vitro effects of TNF antagonists on anti-mycobacterial immune responses
PBS
Hamdi, Mariette et al, ART 2006, Saliu et al, JID 2006

©2014 MFMER | slide-36
RA and Tuberculosis l August 2010 l 36
Granuloma Penetration
• Acute TB infection (mouse)
• Large bacillary load and death
• No difference between anti-TNFs
• Chronic TB infection (mouse)
• Monoclonal antibodies=death (1 month)
• Etanercept=60% alive at 6 months
• Lung path: etanercept with less penetration of granulomas
Plessner HL et al. J Infect Dis. 2007;195:1643-1650.

©2014 MFMER | slide-37
Evolution of Biologics for IMIDS
1940s
Gold
Hydroxychloroquine
Corticosteroids
Etanercept
1950s 1960s 1970s 1980s 1990s 2000s
D-Penicillamine
Methotrexate
Auranofin
Azathioprine
Infliximab
Adalimumab
Golimumab
Certolizumab
Anakinra
Leflunomide
Rituximab
Abatacept
Tocilizumab
Ustikinumab
Belimumab
Natalizumab
Canakinumab
Rilonacept
Tofacitinib
Vedolizumab Secukinumab
Slide credit: clinicaloptions.com

©2014 MFMER | slide-38
Immunocompetence With New and Emerging Biologic Therapies
• Immunocompetence is defined as the capacity of the integrated immune response to defend against infections and malignancies
• An increased rate of infections is the gold standard, but:
• Clinical trials are generally underpowered for rare events
• Data collected across clinical trials and databases of such events are not uniform
• Diseases such as RA,CD are confounded by an increased baseline risk of SIEs
RA, rheumatoid arthritis; SIE, serious infectious event.
Looney RJ et al. Clin Immunol. 2007;123:235-243.

©2014 MFMER | slide-39
BLACK BOX INHERITENCE
Serious Infection Risk
weigh tx benefit vs. risk in pts w/ chronic or recurrent infection;
pulmonary and extrapulmonary tuberculosis (TB), invasive fungal
infections, and other opportunistic infections observed, incl. fatal;
most infections occur in combo w/ other immunosuppressants;
evaluate for TB risk factors and screen for latent TB infection before
and during tocilizumab tx; initiate anti-TB tx before tocilizumab tx;
monitor for infection s/sx during and after tocilizumab tx; since active
TB has developed in pts w/ negative tuberculin skin test, monitor all
pts for active TB s/sx; D/C tocilizumab tx if serious infection occurs
COMPLEX SINCE BIOLOGICS IN IMIDS ARE GENERALLY USED IN
COMBINATION WITH GC AND NB-DMARDS ( MTX etc)

©2014 MFMER | slide-40
J Rheum 2014

©2014 MFMER | slide-41
Other New Agents
• Ustikinumab IL12/23 inhibitor
• ?
• Secukinumab anti-IL17
• ?
• Others
• Vedolizumab
• Anti-IL23
• others

©2014 MFMER | slide-42
• JAK inhibitor
Blocks innate and adaptive immunity
• Cellular selectivity for JAKs
Jak3, Jak1 > Jak2 >> Tyk2
• Effective in variety of preclinical models
• Investigated in a large clinical trial
program in humans
Tofacitinib a Jakatinib
O'Shea JJ, et al. Nat Rev Rheumatol. 2013;9(3):173-182.

©2014 MFMER | slide-43
Tofacitinib: JAK Usage by Cytokines
JAK3 JAK1>>Jak2
Cytokines in the
Pathogenesis of RA
IL-7 IL-23
IL-15 IL-1
IL-21 IL-17
IL-6 IL-18
IFNα and IFNβ TGF-β
IL-10 TNF
IL-12
• Common gamma chain
IL2,IL7,IL9,IL15,IL21
• Blocks Th1
• Blocks Th17
• Decreased NK cells
NK = natural killer; TGF = transforming growth factor. O'Shea JJ, et al. Nat Rev Rheumatol. 2013;9(3):173-182.

©2014 MFMER | slide-44

©2014 MFMER | slide-45
SCREENING for TB in IMIDS
• Anergy
• Recommendations
• IGRA vrs TST
• Retesting

©2014 MFMER | slide-46
Anergy in Rheumatoid Arthritis: Assessment of Reactivity to Multiple Antigens
0
10
20
30
40
0 1 2 3 4 5 6
Controls (n=67) RA Patients (n=104)
%
RA
Patients
or
Contr
ols
Emery et al, Annals Rheum Dis 43: 430-434, 1984
Reagents: tuberculin, tetanus toxoid, diphtheria toxoid,
streptococcus, candida, trichophyton, proteus
# of individual antigens with positive reaction

©2014 MFMER | slide-47

©2014 MFMER | slide-48
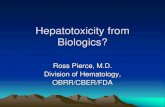
Number of TB Reports per Month vs. Patient Exposure (US) With Infliximab
# o
f R
eport
ed T
B C
ases
(4 m
onth
movin
g a
vg)
Feb 2000 - August 2002
0
5
10
15
20
25
30
0 20000 40000 60000 80000 100000 120000 140000 160000 180000
# o
f Patie
nts
Tre
ate
d
Du
ring
Pre
vio
us 6
Mo
nth
s
TB Cases PSUR Period Exposure
Post-Approval
TB Education Program Initiated
Centecor, Data on file

©2014 MFMER | slide-49
3 IR Therapy

©2014 MFMER | slide-50
Re-test?
• No formal recommendations
• Complex issues with IGRA given adjunctive immunosuppression, effects of disease activity etc
• Most C level data suggests re-test only on the basis of clinical risk

©2014 MFMER | slide-51
Conclusions
• Biologic therapies for IMIDS increase the risk of TB reactivation as well as inhibit the defense against newly acquired granulomatous infections
• The preponderance of data are for TNFi and much our current practice is based on extrapolation
• Current screening has been effective at reducing the occurrence of active TB