Environmental Emergencies CHAPTER 22. Thermoregulatory Emergencies.
Upload
kimmer-collison-risCategory
view
115download
1
Triaging FP Triaging FP Emergencies/UrgenciesEmergencies/Urgencies
By Kimmer Collison-RisBy Kimmer Collison-Ris
MSN, FNP-BC, WOCN, MS CAMMSN, FNP-BC, WOCN, MS CAM

IntroductionIntroduction Triaging is the first step in caring for Triaging is the first step in caring for
urgencies/emergenciesurgencies/emergencies Phone triage needs to be a direct set of Phone triage needs to be a direct set of
assessment questionsassessment questions Clinical triage involves visual inspection & Clinical triage involves visual inspection &
assessment of vital signs to assessassessment of vital signs to assess Your quick, calm response to urgencies is Your quick, calm response to urgencies is
vital to the delivery of care emergenciesvital to the delivery of care emergencies The provider is team leader in an The provider is team leader in an
emergency & directs care by delegationemergency & directs care by delegation

Remember your: ABC’sRemember your: ABC’s
AirwayAirway BleedingBleeding CirculationCirculation Level of ConsciousnessLevel of Consciousness PainPain Location of problemLocation of problem

Triaging PatientsTriaging Patients High priority for:High priority for:
Very young/oldVery young/old High fever >103.0F & if uncontrolled, prolongedHigh fever >103.0F & if uncontrolled, prolonged Decreased LOC? Head injury?Decreased LOC? Head injury? Cardiac sx: Chest pain, tightnessCardiac sx: Chest pain, tightness Breathing sx: chest tightness, sob, meds not working, painful Breathing sx: chest tightness, sob, meds not working, painful
breathingbreathing Sudden weakness, confusion, immobility, sev painSudden weakness, confusion, immobility, sev pain Neurological symptomsNeurological symptoms Concurrent med illness: Diabetic?Asmatic? Chemo?Concurrent med illness: Diabetic?Asmatic? Chemo?
Think ABC:Think ABC: airway, bleeding, circulation, sev. Painairway, bleeding, circulation, sev. Pain
Lower Priority for:Lower Priority for: Chronic problemChronic problem Stable kid, adultStable kid, adult Ongoing injury/back pain/joint painOngoing injury/back pain/joint pain

Common Complaints/IllnessesCommon Complaints/Illnesses FeverFever Diarhea/nausea/vomitingDiarhea/nausea/vomiting Dizziness/weaknessDizziness/weakness Headache/EaracheHeadache/Earache Sleepy/irritable/lethargic patientSleepy/irritable/lethargic patient Severe cold/cough/sore throat symptomsSevere cold/cough/sore throat symptoms Stomach aches/constipationStomach aches/constipation Chest pain/irregular heart rate/chest tightnessChest pain/irregular heart rate/chest tightness Depression/suicidal ideationDepression/suicidal ideation Fussy/irritable/inconsolable babyFussy/irritable/inconsolable baby Lethargic/weakness/difficult swallowing/talkingLethargic/weakness/difficult swallowing/talking Backpain/Foot painBackpain/Foot pain Rashes, allergic reaction, facial swelling, itchingRashes, allergic reaction, facial swelling, itching Wound/skin infections/draining skin rashWound/skin infections/draining skin rash Head injuryHead injury Breathing ProblemsBreathing Problems

Answering the PhoneAnswering the Phone Identify yourself as an RNIdentify yourself as an RN Ask the problemAsk the problem Direct questions via triage bookDirect questions via triage book Avoid getting sidetracked w/other issuesAvoid getting sidetracked w/other issues Triage for urgency vs emergencyTriage for urgency vs emergency
Poss dehydration, LOC changes, very young/old?Poss dehydration, LOC changes, very young/old? Bleeding, weakness, high fevers, severe pain?Bleeding, weakness, high fevers, severe pain? Chronic problems are not an urgency/emergencyChronic problems are not an urgency/emergency
Stable pt not an urgency or an emergencyStable pt not an urgency or an emergency Ask home treatments triedAsk home treatments tried Give instructions for home care until apptGive instructions for home care until appt Give instructions for when to go to ERGive instructions for when to go to ER

Urgencies vs EmergenciesUrgencies vs Emergencies Medical UrgencyMedical Urgency
Diabetic high/low blood sugarDiabetic high/low blood sugar High blood pressureHigh blood pressure Severe Headache (not the worst ever)Severe Headache (not the worst ever) Laceration (w/in 6 hours) or burnLaceration (w/in 6 hours) or burn Lethargic pt, breathing difficultiesLethargic pt, breathing difficulties
Medical EmergencyMedical Emergency Uncontrolled AirwayUncontrolled Airway Shock symptomsShock symptoms Uncontrolled Bleeding w/pulseUncontrolled Bleeding w/pulse High Blood pressure w/headacheHigh Blood pressure w/headache Worst HA or Back pain everWorst HA or Back pain ever Active Chest PainActive Chest Pain

Advising Clients to call EMSAdvising Clients to call EMS
Unresponsive patientUnresponsive patient Active chest painActive chest pain Difficulty BreathingDifficulty Breathing ChokingChoking Bleeding w/a pulseBleeding w/a pulse Patient who’s fallen/can’t get up/sev painPatient who’s fallen/can’t get up/sev pain Patient who can’t movePatient who can’t move
Performing Timely VisitsPerforming Timely Visits Keep patient/family members calm, limit peopleKeep patient/family members calm, limit people Take vitals: T, P, BP, R, Ox sat, Peak flowTake vitals: T, P, BP, R, Ox sat, Peak flow Do visual triage assessmentDo visual triage assessment Ask quick problem:Ask quick problem: Direct visit questions Direct visit questions Have pt/family responses brief/to the pointHave pt/family responses brief/to the point Chart as you goChart as you go Determine urgency vs emergencyDetermine urgency vs emergency Give quick verbal/written teaching instructionsGive quick verbal/written teaching instructions Explain when to f/u w/providerExplain when to f/u w/provider

Visual ScanVisual Scan Alert?Alert? Oriented?Oriented? Confused?Confused? Irritability/cooperationIrritability/cooperation Lethargic?Lethargic? Bleeding?Bleeding? Asymetric?Asymetric? Interaction w/family/providerInteraction w/family/provider Respiratory Distress?Respiratory Distress? Level of Pain?Level of Pain? Diaphoretic?Diaphoretic? Dry mucous membranes?Dry mucous membranes? Severe pain?Severe pain?
Newborns/InfantsNewborns/Infants Triage questions:Triage questions:
Age of patientAge of patient Feeding problemsFeeding problems Vomiting/diarheaVomiting/diarhea Fussy/irritabilityFussy/irritability Low body temperatureLow body temperature Alertness/playfulness/sleepiness/lethargyAlertness/playfulness/sleepiness/lethargy # of wet diapers# of wet diapers
SDA Provider visit for sick newborn/infantSDA Provider visit for sick newborn/infant Babies should be assessed if concern existsBabies should be assessed if concern exists

Sick InfantsSick Infants Don’t manifest the same as older kidsDon’t manifest the same as older kids Can change status quicklyCan change status quickly Listen to parents: they are experts on their kidsListen to parents: they are experts on their kids Be concerned if child not regarding parent’s faceBe concerned if child not regarding parent’s face Bring in for:Bring in for:
Inconsolable, shrill cryingInconsolable, shrill crying Lethargy, too sleepy, difficult to arouseLethargy, too sleepy, difficult to arouse Poor feeding or large emesis post feedingPoor feeding or large emesis post feeding Vomiting or diarrhea sx Vomiting or diarrhea sx Floppiness, seizures/convulsionsFloppiness, seizures/convulsions Blood in diaper or frequent watery stoolsBlood in diaper or frequent watery stools Lack of tears or dry mucous membranes or decreased outputLack of tears or dry mucous membranes or decreased output Sunken facial featuresSunken facial features

Sick KidsSick Kids Remember standard triage questionsRemember standard triage questions
Age, length of illness, concurrent sxAge, length of illness, concurrent sx Severity, feeding, urine/stool outputSeverity, feeding, urine/stool output Fevers (need actual number, not estimation)Fevers (need actual number, not estimation)
Kids are exposed to freq infectionsKids are exposed to freq infections Ask about change in behaviorAsk about change in behavior
Kids aren’t normally lethargic/sleepy/inactiveKids aren’t normally lethargic/sleepy/inactive Increase in irritability, clingyness, inconsolabilityIncrease in irritability, clingyness, inconsolability
Home care Instructions:Home care Instructions: Take temperatures call if >100.5FTake temperatures call if >100.5F Keep hydrated w/more than water: popsickles, pedialyteKeep hydrated w/more than water: popsickles, pedialyte Tylenol for temperatures, keep coolTylenol for temperatures, keep cool Fluids/HOB elevation/Humidification/avoidance of milk for Fluids/HOB elevation/Humidification/avoidance of milk for
coughscoughs BRATT diet for diarheaBRATT diet for diarhea
Provider visit if: young, severe sx, not improvingProvider visit if: young, severe sx, not improving

Elderly IllnessElderly Illness Remember standard triage questionsRemember standard triage questions
Age, length of illness, concurrent sxAge, length of illness, concurrent sx Severity, feeding, urine/stool outputSeverity, feeding, urine/stool output Fevers (need actual number, not estimation)Fevers (need actual number, not estimation)
Elderly usually don’t have temps but manifest illness as confusionElderly usually don’t have temps but manifest illness as confusion Ask about change in behaviorAsk about change in behavior
lethargic/sleepy/inactive/irritabilitylethargic/sleepy/inactive/irritability Decrease in activity or previous independenceDecrease in activity or previous independence
Home care Instructions:Home care Instructions: Monitor mental statusMonitor mental status Keep hydrated w/more than water: popsickles, soups, gatoraidKeep hydrated w/more than water: popsickles, soups, gatoraid Consider staying w/elderly adult till improvedConsider staying w/elderly adult till improved Fluids/HOB elevation/Humidification/avoidance of milk for coughsFluids/HOB elevation/Humidification/avoidance of milk for coughs BRATT diet for diarheaBRATT diet for diarhea Remember med regimen, take fsbs if approp, Remember med regimen, take fsbs if approp,
Provider visit if: confused, weak, severe sx, not improvingProvider visit if: confused, weak, severe sx, not improving

FeverFever Definition:Definition: Need documented temp of 100F or >Need documented temp of 100F or > Concern in elderly (usually don’t mount response)Concern in elderly (usually don’t mount response) Hot flashes/chills not indication of feverHot flashes/chills not indication of fever Tx w/analgesics if >100.5 (Tylenol/ibuprofen)Tx w/analgesics if >100.5 (Tylenol/ibuprofen) Watch for febrile seizures under age of 5 yearsWatch for febrile seizures under age of 5 years Keep temps below 104 in adults/kidsKeep temps below 104 in adults/kids Kids have higher temps than adultsKids have higher temps than adults Don’t treat temps in kids w/ASA Don’t treat temps in kids w/ASA Cool down patient w/cool cloths, ice packs behind Cool down patient w/cool cloths, ice packs behind
neck, armpits, and groin areaneck, armpits, and groin area Remove extra clothing to stabilizeRemove extra clothing to stabilize Avoid use of alcohol bathsAvoid use of alcohol baths

VomitingVomiting Young/old at risk for dehydrationYoung/old at risk for dehydration Assess length of time, frequencyAssess length of time, frequency Ask what pt is able to keep downAsk what pt is able to keep down Any diarrhea concurrently?Any diarrhea concurrently? If unable to eat/drink or young/old pt bring inIf unable to eat/drink or young/old pt bring in Home instructions:Home instructions:
Water is not enough to rehydrateWater is not enough to rehydrate Give ice/fluids after vomiting w/in 15minGive ice/fluids after vomiting w/in 15min Gatoraid for lg children/adults or diluted for kidsGatoraid for lg children/adults or diluted for kids Pedialyte for babies/children w/ea episode of vomitingPedialyte for babies/children w/ea episode of vomiting Hold milk for 48-72h following vomitingHold milk for 48-72h following vomiting Hold formula for 24-72h and give pedialyte as substituteHold formula for 24-72h and give pedialyte as substitute Give clear liquids for 24-72h for gut rest/rehydrationGive clear liquids for 24-72h for gut rest/rehydration Advance to soft diet of soups, sandwichesAdvance to soft diet of soups, sandwiches Avoid heavy meals for 3-4daysAvoid heavy meals for 3-4days
DiarrheaDiarrhea Caution in young/old: risk of dehydrationCaution in young/old: risk of dehydration Length of time & frequency?Length of time & frequency? Quality of stool:Quality of stool:
watery, color, consistency, odorwatery, color, consistency, odor Assess precipitating event:Assess precipitating event: Provider visit for temp, cramping, frequency, or age factorsProvider visit for temp, cramping, frequency, or age factors
Food? Daycare? Family illness? Recent travel?Food? Daycare? Family illness? Recent travel? Home care Instructions:Home care Instructions:
BRATT diet for kids-adultsBRATT diet for kids-adults Bananas, rice, applesauce, tea, toastBananas, rice, applesauce, tea, toast
Rehydrate w/Pedialyte or GatoraidRehydrate w/Pedialyte or Gatoraid Apply vomiting suggestions on dilutionsApply vomiting suggestions on dilutions Avoid Peptobismol in babies/young kidsAvoid Peptobismol in babies/young kids Peppermint, chamomile, or ginger tea for stomach crampingPeppermint, chamomile, or ginger tea for stomach cramping Avoid milk x 1-2 wks following Avoid milk x 1-2 wks following

DehydrationDehydration Serious & needs quick reversalSerious & needs quick reversal Hydrate outpt w/salty fluids/broth/sports drinksHydrate outpt w/salty fluids/broth/sports drinks Don’t need full gut rest as can worsen sxDon’t need full gut rest as can worsen sx Counsel that water IS NOT adequate aloneCounsel that water IS NOT adequate alone Occurs w/high fevers & gastroenteritis Occurs w/high fevers & gastroenteritis Worse for young & Elderly-send to ER for eval if 2 or more Worse for young & Elderly-send to ER for eval if 2 or more
signs/sx occur belowsigns/sx occur below Signs/SymptomsSigns/Symptoms
Sunken eyes, dry mucous membranesSunken eyes, dry mucous membranes Lethargy, inconsolability, irritabilityLethargy, inconsolability, irritability Lack of tearsLack of tears Confusion in adultsConfusion in adults Rapid heart rateRapid heart rate Output >input (ie: vomiting/diarhea >PO intake)Output >input (ie: vomiting/diarhea >PO intake)

Heat ExhaustionHeat Exhaustion Occurs in very young/old quicklyOccurs in very young/old quickly Need 1 c fluid every hour in hot weatherNeed 1 c fluid every hour in hot weather
Water is insufficient treatmentWater is insufficient treatment Need salty foodsNeed salty foods Pedialyte for kids/Gatoraid for adultsPedialyte for kids/Gatoraid for adults
Symptoms include:Symptoms include: HeadacheHeadache Weakness, dizzinessWeakness, dizziness Body aches/crampingBody aches/cramping VomitingVomiting Elevated body temperatureElevated body temperature
Treatment:Treatment: Stabilize body temperature to normalStabilize body temperature to normal Provide cool environment & restProvide cool environment & rest Salty rehydration fluids every 15 minSalty rehydration fluids every 15 min Control vomitingControl vomiting Give tylenol for headache/stabilize body temperatureGive tylenol for headache/stabilize body temperature

HeadacheHeadache Triage questions:Triage questions:
Patient questionsPatient questions Hx of migraines, headaches, triggersHx of migraines, headaches, triggers Recent head trauma, fall, hypertensionRecent head trauma, fall, hypertension Concurrent fever, dizziness, confusion?Concurrent fever, dizziness, confusion?
ASAP Provider visitASAP Provider visit Home Care:Home Care:
Dark room, quiet, Imitrex injectionDark room, quiet, Imitrex injection HydrationHydration Consider triggersConsider triggers Treat nausea/vomitingTreat nausea/vomiting Have pt track headache trends at homeHave pt track headache trends at home Provider visit if visual changes/tx failures, or persistence in Provider visit if visual changes/tx failures, or persistence in
symptoms/qualitysymptoms/quality Turf to ER:Turf to ER:
““Worst headache ever”Worst headache ever” Call 911-don’t have private transportCall 911-don’t have private transport

Dizziness/WeaknessDizziness/Weakness Triage questions:Triage questions:
Age of patientAge of patient Past medical hx:Past medical hx:
• Migraines, diabetes, hypertension, cardiac history, CVA hxMigraines, diabetes, hypertension, cardiac history, CVA hx Severity, onset, history of sx, length of timeSeverity, onset, history of sx, length of time Triggers?Triggers?
• Allergies, sinusitis, meds, foodAllergies, sinusitis, meds, food Concurrent illness?Concurrent illness?
• URI, HTN, migraineURI, HTN, migraine• speaking/walking/swallowingspeaking/walking/swallowing
SDA Provider visitSDA Provider visit Home care instructions:Home care instructions:
Rest, note severity, re occurrenceRest, note severity, re occurrence Have someone drive the patientHave someone drive the patient Hydrate & control temp, nausea/vomiting/diarrheaHydrate & control temp, nausea/vomiting/diarrhea

Head InjuryHead Injury Triage questions:Triage questions:
What is their LOC?What is their LOC? When & how did it occur?When & how did it occur? Type of impact: sports, vehicle accident, fall?Type of impact: sports, vehicle accident, fall? Blackout, see stars, lose time, consciousness?Blackout, see stars, lose time, consciousness?
How did you treat?How did you treat? Ice, neuro checks, tylenol/ibuprofen, restIce, neuro checks, tylenol/ibuprofen, rest
Perform visual InspectionPerform visual Inspection Visable bleeding, bruising, laceration?Visable bleeding, bruising, laceration? Perform neuro checks & take vital signsPerform neuro checks & take vital signs
Have Provider evaluation asapHave Provider evaluation asap Give homecare verbal/written instructionsGive homecare verbal/written instructions

Chest PainChest Pain Duration, location, radiation, quality, timing, Duration, location, radiation, quality, timing,
precipitating events?precipitating events? Quickly assess PMHx, HTN, Hyperlip, Obesity, OD, Quickly assess PMHx, HTN, Hyperlip, Obesity, OD,
Fam hx, sudden cardiac death, comorbidities?Fam hx, sudden cardiac death, comorbidities? If in office: call for provider, then call 911, give 325mg If in office: call for provider, then call 911, give 325mg
ASA, EKG, may give nitro, 02, sats, vs, delegate help, ASA, EKG, may give nitro, 02, sats, vs, delegate help, stay w/pt, keep calmstay w/pt, keep calm
When in doubt tx as cardiac firstWhen in doubt tx as cardiac first Know pre-menopausal women sx (fatigue)Know pre-menopausal women sx (fatigue) Know diabetic or pain tx’d pts differencesKnow diabetic or pain tx’d pts differences Chest pain often subtle not “classic crushing”Chest pain often subtle not “classic crushing” Often is GI in nature (GERD or Gallbladder)Often is GI in nature (GERD or Gallbladder)

Breathing ProblemsBreathing Problems Know sx of resp distress (however subtle)Know sx of resp distress (however subtle)
Wheezing vs silent air movement, cyanosisWheezing vs silent air movement, cyanosis PHx of RAD/Asthma/COPDPHx of RAD/Asthma/COPD Precipitating event? Illness vs irrit. exposurePrecipitating event? Illness vs irrit. exposure Assess Oxy sat, Peakflow, lungs asapAssess Oxy sat, Peakflow, lungs asap
Worry if sats 93% or less or visual cyanosisWorry if sats 93% or less or visual cyanosis Provide Neb tx/Oxygen asapProvide Neb tx/Oxygen asap Treat or Turf? Obtain 2Treat or Turf? Obtain 2ndnd opinion if nec opinion if nec Anaphylaxis tx: Epipen/call 911 (got 15 min)Anaphylaxis tx: Epipen/call 911 (got 15 min) Position pt for best breathing-fowlers/tripod positionPosition pt for best breathing-fowlers/tripod position Keep pt/family calm for best breathingKeep pt/family calm for best breathing Stabilize or safe transort vs EMS assistStabilize or safe transort vs EMS assist
Abdominal PainAbdominal Pain ASAP Provider visit:ASAP Provider visit:
Young/old patient orYoung/old patient or Severe painSevere pain
Triage questions:Triage questions: Patient agePatient age Severity of painSeverity of pain Length of timeLength of time Sx: temp/nausea/vomiting/constipation/diarrhea?Sx: temp/nausea/vomiting/constipation/diarrhea? Treatments tried?Treatments tried?
STI/Pelvic InfectionSTI/Pelvic Infection AskAsk
Cramping, fevers, backpain, length of timeCramping, fevers, backpain, length of time When was last pelvic exam, hx of STI’s?When was last pelvic exam, hx of STI’s? Is Abd/pelvic/back pain manageable w/analgesics?Is Abd/pelvic/back pain manageable w/analgesics? Pt able to keep food/fluids down?Pt able to keep food/fluids down?
Provider visit if:Provider visit if: Severe back or pelvic/abd painSevere back or pelvic/abd pain Fevers w/nausea/vomitingFevers w/nausea/vomiting Pelvic Exam w/copious discharge and/or cervical Pelvic Exam w/copious discharge and/or cervical
motion tendernessmotion tenderness Fevers, weak, achy, unable to keep fluids down-ERFevers, weak, achy, unable to keep fluids down-ER
MiscarriageMiscarriage Miscarriage if >8 wksMiscarriage if >8 wks Length of bleeding/crampingLength of bleeding/cramping Immediate Provider visit:Immediate Provider visit:
Does pt have documented serum hcg/pregnancy test with Does pt have documented serum hcg/pregnancy test with bleeding and/or cramping?bleeding and/or cramping?
Labs: Need to monitor serum hcg levels/CBCLabs: Need to monitor serum hcg levels/CBC Any temps, fevers, vaginal discharge?Any temps, fevers, vaginal discharge? Diagnostics: Pelvic ultrasoundDiagnostics: Pelvic ultrasound Bedrest until provider visitBedrest until provider visit Get a pad count of spotting/blood lossGet a pad count of spotting/blood loss Can’t stop process once it startsCan’t stop process once it starts If Heavy Bleeding: send to ER or call OB MD for evalIf Heavy Bleeding: send to ER or call OB MD for eval

Cough/ColdCough/Cold Triage questions:Triage questions:
Age of patientAge of patient Severity & length of sxSeverity & length of sx Fever >100.5 FFever >100.5 F Presence of sore throat, diff breathing, swallowing, coughPresence of sore throat, diff breathing, swallowing, cough Ask about rashes, lethargy, confusion, sleepiness, feedingAsk about rashes, lethargy, confusion, sleepiness, feeding Past medical hx: diabetic, asthmatic, illnessesPast medical hx: diabetic, asthmatic, illnesses Concurrent fever/nausea/vomiting/diarheaConcurrent fever/nausea/vomiting/diarhea Exposure to ill personsExposure to ill persons
If young/old or ill get SDA Provider visitIf young/old or ill get SDA Provider visit Home care Instructions:Home care Instructions:
Control temps w/tylenol, light bedding or clothingControl temps w/tylenol, light bedding or clothing Treat cold sx w/freq fluids/avoid milk productsTreat cold sx w/freq fluids/avoid milk products Remember cough drops/HOB elevationRemember cough drops/HOB elevation Remember freq hand washing, covering of mouth, wipe down surfacesRemember freq hand washing, covering of mouth, wipe down surfaces
Sore ThroatSore Throat ASAP Provider if visit:ASAP Provider if visit:
Severe sore throat pain >24hSevere sore throat pain >24h Fevers controlled w/tylenol or ibuprofenFevers controlled w/tylenol or ibuprofen Difficulty swallowing/fullness in throatDifficulty swallowing/fullness in throat Send to ER if: sev neck fullness, stridor, sob, diff Send to ER if: sev neck fullness, stridor, sob, diff
swallowing & can’t get in to apptswallowing & can’t get in to appt Rapid strept + throat clx for bact sensitivitiesRapid strept + throat clx for bact sensitivities Supportive care: Supportive care:
• Anesthetic spray, decongestant, pain controlAnesthetic spray, decongestant, pain control• Avoid milk products, hob elevated, humidifierAvoid milk products, hob elevated, humidifier• Nasal irrigation, salt water gargles, mouth care 2x dailyNasal irrigation, salt water gargles, mouth care 2x daily• Freq fluids/soups/clear liquids/gatoraidFreq fluids/soups/clear liquids/gatoraid• f/u in 2-3d if elevated temps contf/u in 2-3d if elevated temps cont

Sprain/StrainSprain/Strain Best assessment/treatment is w/in first day of injuryBest assessment/treatment is w/in first day of injury Assess thoroughly: Assess thoroughly:
for circulation, mobility, strength, malposition, pain, for circulation, mobility, strength, malposition, pain, bruising, point tendernessbruising, point tenderness
Institute RICE therapyInstitute RICE therapy rest,ice, compression, elevation for 24-72hrest,ice, compression, elevation for 24-72h
Compression:Compression: Wrap w/ace using width equal to width of limb to be Wrap w/ace using width equal to width of limb to be
wrappedwrapped Reassess in 3-7d (Reassess in 3-7d (Consider xray if not improvedConsider xray if not improved)) Place pt on analgesic pain schedulePlace pt on analgesic pain schedule
Tylenol for bone pain/inflammationTylenol for bone pain/inflammation Ibuprofen for MSK pain/spasm/inflammationIbuprofen for MSK pain/spasm/inflammation

FracturesFractures Provider likely to Treat in office if:Provider likely to Treat in office if:
No compromise in CMS & only 1 area affectedNo compromise in CMS & only 1 area affected Stabilize/Imobilize till xray readStabilize/Imobilize till xray read Begin RICE (rest, ice, compression, elevation)Begin RICE (rest, ice, compression, elevation) Analgesics Analgesics (Tylenol/ibuprofen higher dose regimen)(Tylenol/ibuprofen higher dose regimen) Xray: PA, Lat, oblique Xray: PA, Lat, oblique (obtain STAT reviewed verbal report)(obtain STAT reviewed verbal report) Splint or cast prn (may need to splint in flexed position w/ace for Splint or cast prn (may need to splint in flexed position w/ace for
sev days to allow for decrease in swelling)sev days to allow for decrease in swelling)
Provider likely send to ER if:Provider likely send to ER if: CMS compromise (insensate, electrical pain, pallor)CMS compromise (insensate, electrical pain, pallor) Protruding bone (tx for shock, stabilize for safe Protruding bone (tx for shock, stabilize for safe
transport)transport) Severe pain or poss mult. sitesSevere pain or poss mult. sites If patient is shocky call EMS vs have private transportIf patient is shocky call EMS vs have private transport

RashesRashes Present as body rash w/red, raised wheelsPresent as body rash w/red, raised wheels Very itchy!!! Very itchy!!!
Try to prevent scratching, secondary infectionTry to prevent scratching, secondary infection Can be caused by allergy, stress, exposure to irritantCan be caused by allergy, stress, exposure to irritant
Get precipitating factors if possibleGet precipitating factors if possible Involves trunk, body, extremitiesInvolves trunk, body, extremities Responds to antihistamines well-tx for several daysResponds to antihistamines well-tx for several days
Diphenhydramine 25-50mg q6h x 3d, then tid x 2d, then Diphenhydramine 25-50mg q6h x 3d, then tid x 2d, then bid x2dbid x2d
Topical treatment reliefTopical treatment relief Think antihistamine relief, oral steriods, calamine, luke Think antihistamine relief, oral steriods, calamine, luke
warm oatmeal baths, topical steriod creamswarm oatmeal baths, topical steriod creams Follow up in 7d or sooner if worsensFollow up in 7d or sooner if worsens

Skin Infection?Skin Infection? Likely Urgency:Likely Urgency:
Located on face (eye, mouth, ear) or groinLocated on face (eye, mouth, ear) or groin Presents w/honey colored crusts over erythemaPresents w/honey colored crusts over erythema Small abscess or mod Diabetic ulcer w/o spreading Small abscess or mod Diabetic ulcer w/o spreading
erythema or sm burn not involving hand, face, footerythema or sm burn not involving hand, face, foot Have provider assess ASAPHave provider assess ASAP
Provider Likely to send to Emergency if:Provider Likely to send to Emergency if: uncontrolled bleeding, red streak w/lymphadnopathy uncontrolled bleeding, red streak w/lymphadnopathy
& fever & hypotensive, or if w/o circulation & pale & fever & hypotensive, or if w/o circulation & pale (think nec fasciitis till proven otherwise)(think nec fasciitis till proven otherwise)
Presents w/blistering abscess w/spreading erythemaPresents w/blistering abscess w/spreading erythema Significant skin breakdown in short time periodSignificant skin breakdown in short time period Deep abscess of arm, leg, groin, peri area, foot, handDeep abscess of arm, leg, groin, peri area, foot, hand
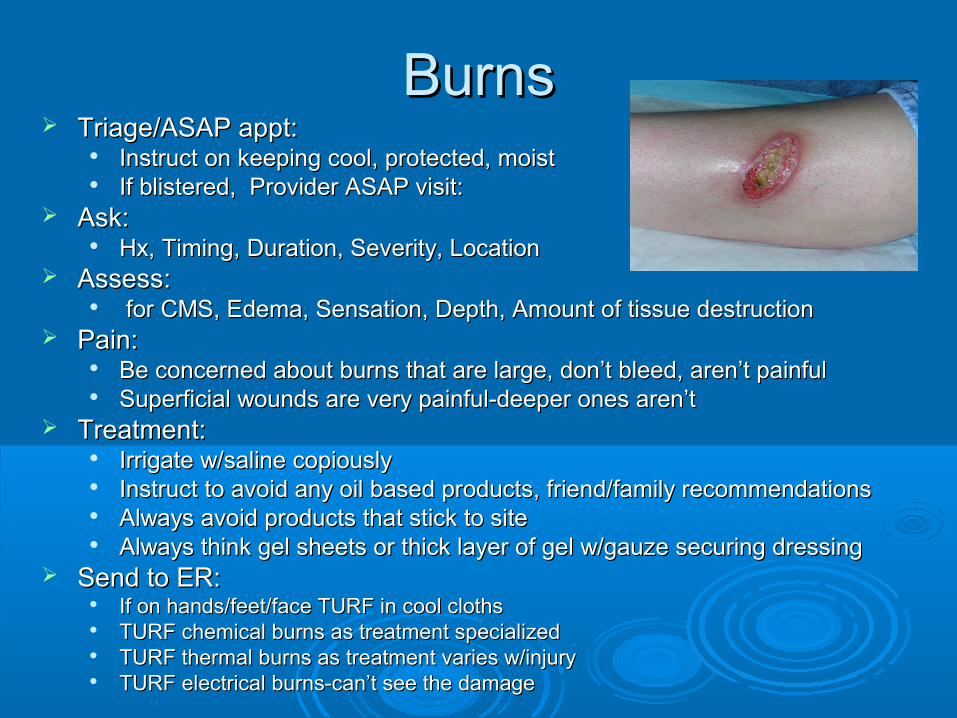
BurnsBurns Triage/ASAP appt:Triage/ASAP appt:
Instruct on keeping cool, protected, moistInstruct on keeping cool, protected, moist If blistered, Provider ASAP visit:If blistered, Provider ASAP visit:
Ask: Ask: Hx, Timing, Duration, Severity, LocationHx, Timing, Duration, Severity, Location
Assess:Assess: for CMS, Edema, Sensation, Depth, Amount of tissue destructionfor CMS, Edema, Sensation, Depth, Amount of tissue destruction
Pain: Pain: Be concerned about burns that are large, don’t bleed, aren’t painfulBe concerned about burns that are large, don’t bleed, aren’t painful Superficial wounds are very painful-deeper ones aren’tSuperficial wounds are very painful-deeper ones aren’t
Treatment:Treatment: Irrigate w/saline copiouslyIrrigate w/saline copiously Instruct to avoid any oil based products, friend/family recommendationsInstruct to avoid any oil based products, friend/family recommendations Always avoid products that stick to siteAlways avoid products that stick to site Always think gel sheets or thick layer of gel w/gauze securing dressingAlways think gel sheets or thick layer of gel w/gauze securing dressing
Send to ER: Send to ER: If on hands/feet/face TURF in cool clothsIf on hands/feet/face TURF in cool cloths TURF chemical burns as treatment specializedTURF chemical burns as treatment specialized TURF thermal burns as treatment varies w/injuryTURF thermal burns as treatment varies w/injury TURF electrical burns-can’t see the damageTURF electrical burns-can’t see the damage
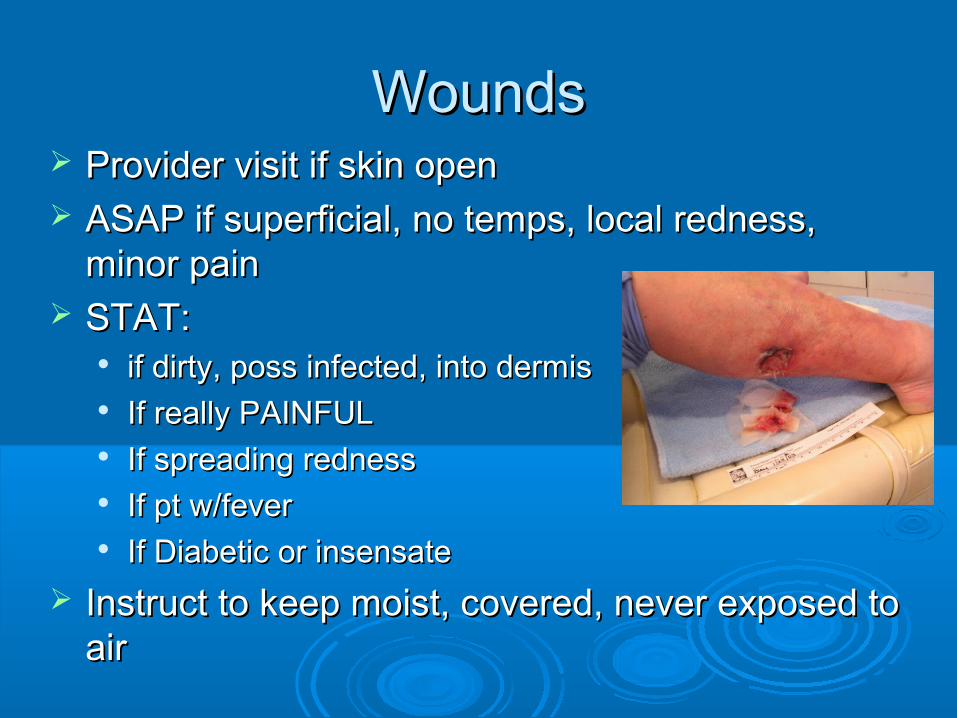
WoundsWounds Provider visit if skin openProvider visit if skin open ASAP if superficial, no temps, local redness, ASAP if superficial, no temps, local redness,
minor painminor pain STAT:STAT:
if dirty, poss infected, into dermisif dirty, poss infected, into dermis If really PAINFULIf really PAINFUL If spreading rednessIf spreading redness If pt w/feverIf pt w/fever If Diabetic or insensateIf Diabetic or insensate
Instruct to keep moist, covered, never exposed to Instruct to keep moist, covered, never exposed to airair

Severe Allergic ReactionSevere Allergic Reaction
Occurs w/food, meds,exposureOccurs w/food, meds,exposure Look for sx of resp distress, throat swellingLook for sx of resp distress, throat swelling Call 911 for EMS assist if resp distressCall 911 for EMS assist if resp distress Give IM Epi (adult or junior dose, repeat in 15 min. if sx Give IM Epi (adult or junior dose, repeat in 15 min. if sx
not stable)not stable) Presents w/severe HivesPresents w/severe Hives May respond to IM SteriodsMay respond to IM Steriods Diphenhydramine is not that helpful at firstDiphenhydramine is not that helpful at first Note allergy in pt’s chartNote allergy in pt’s chart Rx: Epipen x 2 (instruct pt to have at all times)Rx: Epipen x 2 (instruct pt to have at all times) Instruct pt to take this rx seriously, second event more Instruct pt to take this rx seriously, second event more
severesevere

Diabetic UrgencyDiabetic Urgency Symptoms of Unstable blood sugarSymptoms of Unstable blood sugar
ConfusionConfusion DiaphoresisDiaphoresis TachycardiaTachycardia HypotensiveHypotensive Low oxygen satLow oxygen sat ShakinessShakiness Loss of consciousnessLoss of consciousness
Low blood sugar Treatment:Low blood sugar Treatment: Monitor fsbs every 15-30 minMonitor fsbs every 15-30 min Give Instant glucose if less than 60Give Instant glucose if less than 60 Give carbohydrate/protein combo food productGive carbohydrate/protein combo food product Monitor/manage/observe in clinic for 1-2 hours till stableMonitor/manage/observe in clinic for 1-2 hours till stable Send to ER if can’t stabilize w/in 2h beloSend to ER if can’t stabilize w/in 2h belo shakinessshakiness

Diabetic UrgenciesDiabetic Urgencies Additional FSBS <60Additional FSBS <60
Give glucose and repeat fsbs every 15-30 minGive glucose and repeat fsbs every 15-30 min Remember slow change occursRemember slow change occurs Give carb & protein vs straight juiceGive carb & protein vs straight juice Keep them for >1 hourKeep them for >1 hour
FSBS >350FSBS >350 Give short acting insulin and repeat in 30 minGive short acting insulin and repeat in 30 min Give glasses of water to dilute downGive glasses of water to dilute down Keep for 1-2h in clinicKeep for 1-2h in clinic Refer to ER if 400 or greater or w/neuro changesRefer to ER if 400 or greater or w/neuro changes
Assess if >350 is the patient’s normAssess if >350 is the patient’s norm May not be treated as an urgency/emergencyMay not be treated as an urgency/emergency Hemoglobin A1C may indicate if patient runs high normallyHemoglobin A1C may indicate if patient runs high normally

Hypertensive Urgency?Hypertensive Urgency?
Patient has BP of 160/95 – 170/102Patient has BP of 160/95 – 170/102 Has documented uncontrolled high bpHas documented uncontrolled high bp Patient reports not taking HTN medsPatient reports not taking HTN meds Pt w/HA and elevated bp who appears Pt w/HA and elevated bp who appears
otherwise stableotherwise stable Send home to take medsSend home to take meds Set up f/u BP check w/RN in next 1-3dSet up f/u BP check w/RN in next 1-3d

Hypertensive EmergencyHypertensive Emergency Requires EMS transport to ERRequires EMS transport to ER Give 325mg rapid acting ASAGive 325mg rapid acting ASA Call 911, give oxygen, get EKG, repeat vsCall 911, give oxygen, get EKG, repeat vs Patient who presents with 2 or more sx:Patient who presents with 2 or more sx:
BP 180/105 or greaterBP 180/105 or greater ““terrible” headacheterrible” headache DizzinessDizziness ConfusionConfusion WeaknessWeakness Difficulty walkingDifficulty walking Chest PainChest Pain Difficulty speaking/understandingDifficulty speaking/understanding

Emergency ResponseEmergency Response Know your resources-Call for Provider STATKnow your resources-Call for Provider STAT Ask someone to call 911Ask someone to call 911 Ask someone to bring E-kit & oxygen & DefibAsk someone to bring E-kit & oxygen & Defib Do visual scan Do visual scan Remember ABC’sRemember ABC’s Get vital signs & pulse oximetry, q5-15minGet vital signs & pulse oximetry, q5-15min Keep room calm/stableKeep room calm/stable Position pt for best airwayPosition pt for best airway Stay w/patient-DON’T LeaveStay w/patient-DON’T Leave Be ready to give report to EMS when they arriveBe ready to give report to EMS when they arrive

Know your ResourcesKnow your Resources
Onsite Medical Staff helpOnsite Medical Staff help Where are your emergency supplies?Where are your emergency supplies? Role of onsite Nurses/Med AssistsRole of onsite Nurses/Med Assists When to call safe transportWhen to call safe transport When to call 911When to call 911 Local ER phone NumbersLocal ER phone Numbers Maps of local ERsMaps of local ERs Know what your ER’s can doKnow what your ER’s can do
Prioritize needsPrioritize needs ABC’sABC’s Ask for help w/other patients/making Ask for help w/other patients/making
calls/obtaining itemscalls/obtaining items Second opinion from colleague welcomeSecond opinion from colleague welcome Stay calm, focusedStay calm, focused Keep treatment/simpleKeep treatment/simple Keep client/family calmKeep client/family calm

Calling in a ProviderCalling in a Provider For Unstable patientFor Unstable patient Patient w/symptoms that require treatmentPatient w/symptoms that require treatment Emergency/Urgency situationsEmergency/Urgency situations CLEARLY Explain level of priority:CLEARLY Explain level of priority:
High: I need provider help STAT room 1High: I need provider help STAT room 1• Have someone stay w/ptHave someone stay w/pt• Go get E-kit, oxygen, ox sat, defib for standby careGo get E-kit, oxygen, ox sat, defib for standby care
Mod: I have an urgency in room 1Mod: I have an urgency in room 1 Low: I’m concerned, could you assess when you have Low: I’m concerned, could you assess when you have
a moment?a moment?

SummarySummary Know when to “Treat or Turf”Know when to “Treat or Turf” Know difference between “non-Urgency, Know difference between “non-Urgency,
urgency and Emergency”urgency and Emergency” Know how to treat basics in clinicKnow how to treat basics in clinic Know what is beyond your time/abilitiesKnow what is beyond your time/abilities Know how to ask for helpKnow how to ask for help Keep things simple-focus on problem at Keep things simple-focus on problem at
handhand Know when to f/u-remind pt/family of thatKnow when to f/u-remind pt/family of that
Now, Go Get’em!Now, Go Get’em!