Trends in Biomedical Science Damage to the Brain - Neurological trauma.
153
Trends in Biomedical Science Damage to the Brain - Neurological trauma
-
Upload
shanon-shields -
Category
Documents
-
view
215 -
download
0
Transcript of Trends in Biomedical Science Damage to the Brain - Neurological trauma.

Trends in Biomedical Science
Damage to the Brain - Neurological trauma

Disease Number Yearly Cost
Drugs - Illegal 22,000,000 $276,000,000,000
Drugs – Nicotine (US) 70,000,000? $138,000,000,000
Drugs – Nicotine Korea 3,920,000,000,000 won
Drugs - Alcohol (US) 14,000,000 $185,000,000,000
Alzheimer 5,000,000 $100,000,000,000
Pain 97,000,000 $100,000,000,000
Major Depression $70,000,000,000
Trauma 1,400,000 $60,000,000,000
Stroke 700,000 $51,200,000,000
Dyslexia 60,000,000
Anxiety 24,800,000
Head injury is a leading cause of death and disability in Korea. It usually results from an avoidable accident.
In 1998 the annual incidence was 236/100,000 person, 334/100,000 for males and 136/100,000 for females.

Of the causes, 62.5% were road traffic accidents, and 15.6% were falls.
An operation was performed in 20.2% of the cases with a mortality of 4.0% in average.
Overall fatality rate was 8.2%, or 19/100,000 population.

In developed countries, trauma is known as the leading cause of disability and death among children, accounting for approximately 1/3 of all deaths in children aged 0-14 yr old.

Traumatic head injury (THI) is one of the most common injuries associated with disability and is a leading cause of non-fatal injury in children.

Korean figures for THI

For many people who sustain a TBI, the effects of the injury are not obvious. The injury may not even be seen by neuroimaging in some cases.

Traumatic Brain Injury (TBI)Many years of productive life are
lost, and many people have to suffer years of disability after brain injury.
It also involves great costs for individuals, families and society.
Many lives can be saved and years of disability spared through better prevention.

By 2020, road traffic crashes will go from ninth to third place in the world ranking of cost of disease and will be in second place in developing countries.
World Health Organization

In the US, cost to society for TBI has been estimated at between $48 and $83.5 billion per year.
Only 12.5% is direct cost (e.g. hospitalization, physician costs).

Most TBI patients are young and most useful to society. The indirect costs (reduced or loss of productivity) represent the greatest cost.
Some patients have very bad behavioral and psychological difficulties which effect the family and society as well.

TBI most commonly occurs among infants and children, individuals 15 to 29 years of age, and the elderly (65+).Sex: The male to female incidence of TBI has been estimated to be 2 to 1.
The major causes of TBI are road accidents, violent acts, falls, and sports-related injury.
A head injury usually occurs in less than 200 msec.

TBI and the military (especially US military)
Soldiers train or fight. The fighting in Afghanistan and Iraq has included new tactics and weapons (such as improvised explosive devices), and higher rates of injury to the head and neck region than in past fights.
Estimates indicate that TBI causes significant death or other health problems.
You can download and read some of the latest publications on this subject at
Nutrition and Traumatic Brain Injury: Improving Acute and Subacute Health Outcomes in Military Personnel
Cognitive Rehabilitation Therapy for Traumatic Brain Injury: Evaluating the Evidence

Traumatic brain damage is a result of:
immediate mechanical damage of brain tissue (primary injury) and
indirect (delayed or secondary injury) processes.

The primary injury can be reduced by:
• prevention, such as-– education of potential victims (e.g.
don’t drink and drive), and – laws for individual and public
safety,
• and protection, such as– use of safety equipment (eg.
airbags, helmets).

Among soldiers serving in countries such as Iraq and Afghanistan over 20% of injuries involve TBI.
Types of Injury

Inertia injury is caused by sudden acceleration or deceleration.
(see http://neuroscience.uth.tmc.edu/s4/chapter12.html Figure
12.1)

TBI causes local mechanical and/or biochemical disruption of the axonal cytoskeleton. Organelles are continually sent to the site. This causes axonal swelling. Because of this swelling the end of the axon is lost.
(see http://neuroscience.uth.tmc.edu/s4/chapter12.html Figure
12.1)




Impact injury. (e.g. getting hit with a baseball bat or car windscreen)
Impact injuries often have bleeding and swelling.
(see http://neuroscience.uth.tmc.edu/s4/chapter12.html Figure
12.2)



Penetrating injury. (e.g. gun shots)

Penetrating injuries often cause post-traumatic epilepsy.
Memory and temporal lobe damage.
Memory is the most severely affected and most frequently reported symptom by TBI patients and their relatives.
Anterograde amnesia (impairment in ability to recall newly acquired information) as well as retrograde amnesia (impairment in ability to recall old memories) is observed.
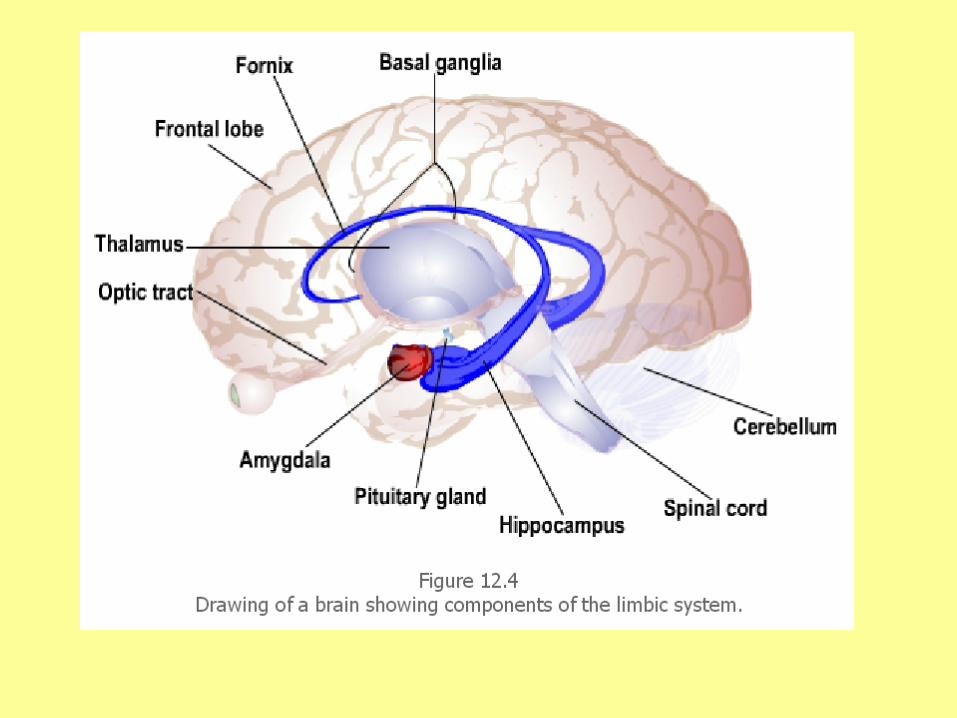
Damage to the temporal lobe, especially the hippocampus, is associated with memory impairments.
Neurons in the hippocampus express high levels of glutamate receptors and often die as a result of TBI.

There are cognitive and behavioral problems in about 2/3 TBI patients.
The other 1/3 have motor problems.
The Effects of TBIThe first phase of brain cell death
(primary necrosis) is at the time of injury and is immediate.
Secondary necrosis occurs over hours or days by programmed cell death (apoptosis).
During this phase, there is the possibility of saving cells that would otherwise die.

Problems are related to the region damaged.
Damage to temporal, frontal, orbital and parietal regions result in cognitive impairments, involving memory, attention, information processing speed, intellectual functioning, language, executive functions and visuospatial ability.

Behavioral changes are common after severe brain injury, with personality change, slowness, irritability, bad temper, fatigue, rapid mood change and depression.

The orbital frontal regions affect impulsivity, anger control, aggressiveness, acting sexually and social judgment.
Damage to these regions can cause release of previously inhibited behaviors and make it difficult to interpret social signals.

TBI and AlzheimerHead injury may be a risk factor for
Alzheimer’s disease. Brains from patients who died as a
consequence of head trauma have shown amyloid beta (Aβ) deposition.
Demential pugilistica (punch-drunk syndrome) is also associated with memory loss and diffuse Aβ deposition.

Carriers of the apolipoprotein E4 (apoE4) allele have an increased risk for developing Alzheimer’s disease.
Head-injured patients with apoE4 are more than twice as likely as those without apoE4 to develop the disease.

Molecular Mechanisms of Secondary Injury
Traumatic injury to the central nervous system includes a secondary injury.
There is progressive cellular damage resulting from degradative biochemical processes that occur as a response to the primary injury.

Figure 1: The major pathways associated with the progression of secondary injury after a traumatic brain injury.
Park E et al. CMAJ 2008;178:1163-1170
©2008 by Canadian Medical Association

©2008 by Canadian Medical Association
Figure 1: The major pathways associated with secondary injury after TBI. Circulatory derangements involve narrowing (1) and loss of microvasculature, and the blood–brain barrier may break down as a result of astrocyte foot processes swelling (2). Proliferation of astrocytes (“astrogliosis”) (3) is a characteristic of injuries to the central nervous system, and their dysfunction results in a reversal of glutamate uptake (4) and neuronal depolarization through excitotoxic mechanisms. Calcium influx (5) starts molecular cascades resulting in delayed cell death or dysfunction as well as delayed axonal disconnection. In neurons, calcium and zinc influx though channels in the AMPA and NMDA receptors results in excitotoxicity (6), generation of free radicals, mitochondrial dysfunction and postsynaptic receptor modifications. These mechanisms don’t happen everywhere but are dependent on the subcellular routes of calcium influx and the degree of injury. Calcium influx into axons (7) starts protein degradation cascades that result in axonal disconnection (8). Inflammatory cells release proinflammatory cytokines (9) that contribute to the activation of cell-death cascades or postsynaptic receptor modifications.

Knowing about secondary injury as a progressive biochemical disorder means that there is some time when effective pharmacotherapy can be used.

Excitatory amino acid receptors.
Levels of extracellular excitatory amino acids (e.g. glutamate and aspartate) are increased following brain trauma.
http://neuroscience.uth.tmc.edu/s4/chapter12.html
figure 12.6

Glutamate and aspartate activate cell surface receptors causing sodium and calcium ions to go into the cell.
Influx of sodium leads to neuronal swelling and increased intracellular calcium causes cell death.

Antagonists for NMDA and non-NMDA receptors have been shown to be neuroprotective in experimental TBI.
Clinical trials using excitatory amino acid blockers, however, have shown discouraging results and unwanted side effects.

Neurons in the hippocampus have many glutamate receptors and often die as a result of TBI.
What do you think would happen then?

Damage to the hippocampus would result in memory problems.One of the diagnostic measures of TBI is the length of time that someone goes through before they get back their full ability to remember.

Calcium ions. Increases in intracellular calcium can occur in different ways including, NMDA receptors, calcium channels and release of calcium from intracellular stores.
Continuous high levels of intracellular calcium are toxic.
High levels of calcium cause activation of proteases, lipases, generation of free radicals and impairment of mitochondrial function leading to energy failure.

Proteolytic mechanisms of cell death.
A family of proteases are activated by elevated intracellular calcium.
These proteolyze many cellular proteins including cytoskeletal proteins, excitatory amino acid receptors, cell adhesion molecules and enzymes.

Breakdown of cytoskeletal proteins, excitatory amino acid receptors, cell adhesion molecules and enzymes, causes structural and functional alterations leading to cellular death.

Phospholipases. Elevated intracellular calcium phospholipases, enzymes that degrade membrane lipids, increase following TBI.

Breakdown of membrane lipids result in loss of cellular integrity, ionic imbalance and cell death.

Free radicals. Free radicals are highly reactive molecules that damage neuronal, glial and vascular membrane phospholipids and cause oxidation of cellular proteins and nucleic acids.

The brain is easily hurt by oxidative injury.
The brain contains high concentrations of peroxidizable fatty acids.
The brain has few protective antioxidant enzymes and endogenous antioxidant compounds.
Free radicals cause widespread cellular and vascular damage.

Several drugs have been tested for their ability to protect free radical-mediated damage. Some have been shown to be neuroprotective in experimental models. However, clinical trials have not supported these findings.

Secondary injury includes pathological processes that can continue to develop over days, weeks or even months, after the primary injury.

For example, neurons in the CNS that are synaptically connected not only release neurotransmitters but also neurotrophic factors (e.g. BDNF) that are needed for their survival.

Damage to the axon of a neuron as a result of primary injury leads to its disconnection from the post-synaptic neuron.

This results in reduced neurotrophic factors leading to eventual degeneration (by apoptosis or programmed cell death) of the post-synaptic neuron.
(see http://neuroscience.uth.tmc.edu/s4/chapter12.html Figure 12.7)
Secondary injuries develop over time after the primary injury, they may provide an opportunity for therapeutic intervention.

Neurological Trauma.
Review

Traumatic Brain Injury (TBI)What is the leading cause of death and
disability in children and young adults around the world?
What is involved in nearly half of all trauma deaths?
How can many lives can be saved and years of disability spared?

Traumatic Brain Injury (TBI)What is the leading cause of death and
disability in children and young adults around the world?
Traumatic brain injury.What is involved in nearly half of all
trauma deaths? Traumatic brain injury.How can many lives can be saved and
years of disability spared?Preventing traumatic brain injury.

More data can help in preventing traumatic brain injury (TBI), especially on reducing the impact of road traffic accidents.
By 2020, road traffic crashes will go from ninth to third place in the world ranking of cost of disease and will be in second place in developing countries.
A lot can be done to reduce the effects of TBIs.

In the US, cost to society for TBI has been estimated at between $48 and $83.5 billion per year.
Only 12.5% is direct cost (e.g. hospitalization, physician costs).
What do some patients have which effect the family and society as well?

What do some patients have which effect the family and society as well?
Psychological and behavioral problems

What three groups are most affected by TBI?
What is the ratio of males to females with TBI?
TBI most commonly occurs among infants and children, individuals 15 to 29 years of age, and the elderly (65+).Sex: The male to female incidence of TBI has been estimated to be 2 to 1.

What are the major causes of TBI?
How fast does a head injury occur?

The major causes of TBI are road accidents, violent acts, falls, and sports-related injury.
A head injury usually occurs in less than 200 msec.
What are two ways that result in traumatic brain damage?

Traumatic brain damage is a result of (immediate mechanical damage of brain tissue, or primary injury) and indirect (delayed or secondary injury) processes.

How can the primary injury be lessened?

The primary injury can be lessened through prevention and protection.
How is inertia injury caused?What does it do?

Inertia injury is caused by sudden acceleration or deceleration.
TBI causes local mechanical and/or biochemical disruption of the axonal cytoskeleton.
Organelles are continually sent to the site. This causes axonal swelling. Because of this swelling the end of the axon is lost.

What are impact injuries?What do impact injuries often have?

Impact injury. (e.g. getting hit with a baseball bat)
Impact injuries often have bleeding and swelling.
(see http://neuroscience.uth.tmc.edu/s4/chapter12.html Figure
12.2)

Penetrating injury. (e.g. gun shots)
2/3 TBI patients - cognitive and behavioral problems.
1/3 - motor problems.
What happens when different regions of the brain are damaged?

Problems are related to the region damaged.
Damage to temporal, frontal, orbital and parietal regions result in cognitive impairments, involving memory, attention, information processing speed, intellectual functioning, language, executive functions and visuospatial ability.
What are some behavioral changes common after severe brain injury?

Behavioral changes –personality change, slowness, irritability, bad temper, fatigue, rapid mood change and depression.

What do the orbital frontal regions affect?
What can damage to the orbital frontal region cause?

The orbital frontal regions affect impulsivity, anger control, aggressiveness, sexual acting out and social judgment.
Damage to the orbital frontal region can cause release of previously inhibited behaviors and make it difficult to interpret social signals.
Is TBI a risk factor for Alzheimer’s disease?

Epidemiological studies have suggested that head injury may be a risk factor for Alzheimer’s disease.
Brains have shown amyloid beta (Aβ) deposition. Ex fighters with punch-drunk syndrome also have
memory loss and diffuse Aβ deposition.

Molecular Mechanisms of Secondary Injury

In TBI what is secondary injury?

Secondary injury.degradative biochemical processes →
progressive cellular damage
What does knowing about secondary injury as a progressive biochemical disorder mean for treatment?

Knowing about secondary injury as a progressive biochemical disorder means that there is some time when effective pharmacotherapy can be used.
What levels of biochemicals are increased following brain trauma?

Levels of extracellular excitatory amino acids (e.g. glutamate and aspartate) are increased following brain trauma.

What do glutamate and aspartate do to the cell?
What then happens to the cell?

Glutamate and aspartate activate cell surface receptors causing sodium and calcium ions to go into the cell.
Influx of sodium leads to neuronal swelling and increased intracellular calcium causes cell death.

What has been shown to be neuroprotective in experimental TBI?
What have clinical trials shown?

Antagonists for NMDA and non-NMDA receptors - neuroprotective in experimental TBI.
Clinical trials using excitatory amino acid blockers → discouraging results and unwanted side effects.

What do neurons in the hippocampus have?
What often happens to these neurons as a result of TBI?
Neurons in the hippocampus have many glutamate receptors.
These neurons often die as a result of TBI.

What results from damage to the hippocampus?What is a possible diagnostic measures of TBI?

Damage to the hippocampus would result in memory problems.A diagnostic measure of TBI is the length of time that someone goes through before they get back their full ability to remember.

Calcium ions. How can increases in intracellular calcium occur?
Calcium ions. Increases in intracellular calcium can occur in different ways including, NMDA receptors, calcium channels and release of calcium from intracellular stores.

What do high levels of calcium cause?

Continuous high levels of intracellular calcium are toxic.
High levels of calcium cause activation of proteases, lipases, generation of free radicals and impairment of mitochondrial function leading to energy failure.

A family of proteases are activated by elevated intracellular calcium.
What do these proteolyze?

Proteases activated by elevated
intracellular calcium. These proteolyze many cellular
proteins including cytoskeletal proteins, excitatory amino acid receptors, cell adhesion molecules and enzymes.
What do breakdown of cytoskeletal proteins, excitatory amino acid receptors, cell adhesion molecules and enzymes, cause?

Breakdown of cytoskeletal proteins, excitatory amino acid receptors, cell adhesion molecules and enzymes, causes structural and functional alterations leading to cellular death.
Phospholipases. Elevated intracellular calcium phospholipases, enzymes that degrade membrane lipids, increase following TBI.
What do they breakdown?
What happens to the cell?

Breakdown of membrane lipids result in loss of cellular integrity, ionic imbalance and cell death.
What are Free radicals?
What do they do?
Free radicals. Free radicals are highly reactive molecules that damage neuronal, glial and vascular membrane phospholipids and cause oxidation of cellular proteins and nucleic acids.

Why is the brain easily hurt by oxidative injury?
The brain contains high concentrations of peroxidizable fatty acids.
The brain has few protective antioxidant enzymes and endogenous antioxidant compounds.
Free radicals cause widespread cellular and vascular damage.

The brain contains high concentrations of peroxidizable fatty acids.
The brain has few protective antioxidant enzymes and endogenous antioxidant compounds.
Free radicals cause widespread cellular and vascular damage.

How long can the pathological processes secondary injury continue to develop?

Pathological processes can continue to develop over days, weeks or even months, after the primary injury.

Neurons in the CNS that are synaptically connected release neurotransmitters but also something else.
What do they release?

Neurons in the CNS that are synaptically connected release neurotrophic factors (e.g. BDNF) that are needed for their survival.

What happens after damage to the axon of a neuron as a result of primary injury?

Damage to the axon of a neuron as a result of primary injury leads to its disconnection from the post-synaptic neuron.

What does this disconnection result in?

This results in reduced neurotrophic factors leading to eventual degeneration (by apoptosis or programmed cell death) of the post-synaptic neuron.
(see http://neuroscience.uth.tmc.edu/s4/chapter12.html Figure 12.7)

Secondary injuries develop over time after the primary injury, they may provide an opportunity for therapeutic intervention.

Why is traumatic brain injury important?

What can reduce the effects of TBI?

Explain what happens with primary injury.

Inertia injury - local mechanical and/or biochemical disruption of the axonal cytoskeleton. - causes axonal swelling. - the end of the axon is lost.

Impact injuries often have bleeding and swelling.

Penetrating injury. (e.g. gun shots)

What sort of problems are related to TBI?

What happens because Secondary Injury of TBI?
Progressive cellular damage resulting from degradative biochemical processes.

Levels of extracellular excitatory amino acids (e.g. glutamate and aspartate) are increased.

These activate cell surface receptors causing sodium and calcium ions to go into the cell.
→ neuronal swelling and increased intracellular calcium → cell death.

Neurons in the hippocampus often die.

Increases in intracellular calcium by NMDA receptors, calcium channels and release of calcium from intracellular stores.

High levels of calcium → activation of proteases, lipases, generation of free radicals and reduce mitochondrial function → energy failure.

Proteases are activated → proteolyze many cellular proteins - cytoskeletal proteins, excitatory amino acid receptors, cell adhesion molecules and enzymes.
→ structural and functional alterations → cellular death.

Phospholipases → degrade membrane lipids→ loss of cellular integrity, ionic imbalance and cell death

Free radicals → damage neuronal, glial and vascular membrane phospholipids and cause oxidation of cellular proteins and nucleic acids.

The brain - high concentrations of peroxidizable fatty acids
- few protective antioxidant enzymes and endogenous antioxidant compounds
→ easily hurt by oxidative injury.
→ free radicals cause widespread cellular and vascular damage.

synaptically connected neurons – TBI → disconnected → no neurotrophic factors → degeneration of the post-synaptic neuron.