Treatment of Stroke in the Emergency Department Jim Holliman, M.D., F.A.C.E.P. Professor of...
64
Treatment of Stroke in the Emergency Department Jim Holliman, M.D., F.A.C.E.P. Professor of Emergency Medicine Director, Center for International Emergency Medicine M. S. Hershey Medical Center Pennsylvania State University Hershey, Pennsylvania, U.S.A.
-
Upload
magdalene-melton -
Category
Documents
-
view
221 -
download
0
Transcript of Treatment of Stroke in the Emergency Department Jim Holliman, M.D., F.A.C.E.P. Professor of...

Treatment of Stroke in the Emergency Department
Jim Holliman, M.D., F.A.C.E.P.Professor of Emergency Medicine
Director, Center for International Emergency MedicineM. S. Hershey Medical CenterPennsylvania State UniversityHershey, Pennsylvania, U.S.A.

Stroke Lecture Outline
Classification and epidemiologyRisk factorsSigns and symptomsAssessment in the E.D.TreatmentComparison of results of trials of
thrombolytic agentsProposed neuroprotective agents

Stroke ClassificationDefined as neurological impairment caused
by disruption in blood supply to a region of the brain
2 major categories :–Ischemicƒ Due to occlusion of brain blood vesselƒ Rarely causes death in first hour
–Hemorrhagicƒ Due to rupture or leak of a brain blood vesselƒ Can be fatal at onset or cause rapid death

Types of Ischemic StrokeIn U.S., 75 % of strokes are ischemicTwo etiologies :
–Clots develop locally in brain vessel (thrombosis)–Clots migrate from elsewhere (embolism)
Two classes :–Strokes involving carotid artery distributionƒ Called anterior circulation or carotid territory strokes & affect cerebral hemispheres
–Strokes involving vertebrobasilar arteriesƒ Called posterior circulation or vertebrobasilar territory strokes & affect brainstem or cerebellum

CT scan showing lacunar infarct in right centrum semiovale

Ischemic infarct from left middle cerebral artery ; its wedge shape suggests embolic stroke from atrial fibrillation

Posterolateral thalamic infarct which caused contralateral falling and tilting

Types of Hemorrhagic StrokeTwo classes :
–Subarachnoid hemorrhage (SAH)ƒ Bleeding onto surface of brainƒ Most common cause is berry aneurismƒ 5 % due to arteriovenous malformation
–Intracerebral hemorrhage (ICH)ƒ Bleeding into parenchyma of brainƒ Most common cause is hypertensionƒ Amyloid angiopathy is common cause in elderly

Right putamen hemorrhage presenting as sudden left hemiparesis

Large subarachnoid hemorrhage

Another large subarachnoid hemorrhage

Right temperoparietal bleed (note also left temporal encephalomalacia)

Subarachnoid hemorrhage from a ruptured aneurism

Left sided ICH causing left sided weakness

Basal ganglia hemorrhage

Large right intracerebral hemorrhage causing hemiparesis and obtundation

Hemorrhagic infarct from left middle cerebral artery

Stroke Epidemiology
Third leading cause of death in U.S.A.> 500,000 cases per year> 100,000 deaths per yearLeading cause of brain injury in adultsLeading cause of long term disabilityMay be much higher percent of cases
due to hemorrhage in some countries (such as Korea)

Concept of Stroke as "Brain Attack"
Goal of this is to emphasize need to evaluate and treat stroke similar to the current standard rapid scheme for acute myocardial infarction ("heart attack")
Involves 4 components :–Education of at-risk patients–Early recognitionof stroke symptoms & signs–Prompt prehospital evaluation & transport–Rapid emergency department evaluationƒ May involve stroke team or stroke center

Transient ischemic attacks (TIA's)
Prior stroke–4 to 14 % recurrence per year
Carotid bruitAge > 55
–However, 25 % are younger than 65
Male genderFamily history
High blood pressureSmokingHeart diseaseDiabetes mellitusHypercoagulable
states (see next slide)
PolycythemiasSickle Cell AnemiaAfrican race
Risk Factors for Stroke

Hypercoagulable States Increasing Risk for Stroke
PregnancyUse of birth control pills (oral
contraceptives with estrogens)CancerProtein S deficiencyProtein C deficiency

TIA's and StrokeTIA is a reversible episode of focal dysfunction of
the brain or eye secondary to transient occlusion of an artery
Typically Sx last < 30 minutes, but can last up to several hours
5 % of TIA cases have stroke in < 1 month12 % of TIA cases have stroke by one yearIf > 70 % carotid narrowing with TIA, carotid
endarterectomy is effective to prevent strokeDaily aspirin or ticlopidine effective prophylactically
in some patients


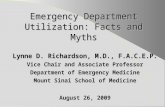
Arch angiogram ; closed arrow denotes right internal carotid artery stenosis ; arrowhead denotes left internal carotid stenosis ; the open arrows denote patent vertebral arteries

Stroke Symptoms
Findings much more common in hemorrhagic stroke :–Headache (could be only symptom)–Depressed level of consciousness–Nausea / emesis–Photophobia–Neck pain or stiff neck
Most ischemic strokes do not have headache

Common Symptoms & Signs of Ischemic Stroke
If carotid (anterior) circulation :–Motor weakness or paralysisƒ Usually unilateralƒ May have facial palsy
–Numbness or paresthesiasƒ Usually same side as weakness
–Language or speech disturbanceƒ Aphasia or dysarthria
–Visual disturbance (usually monocular)ƒ Painless blurring or visual field loss

Right frontal thrombotic infarct, probably older than one day

Common Symptoms & Signs of Ischemic Stroke
If vertebrobasilar (posterior) circulation :–Vertigo, often with nystagmus–Visual disturbancesƒ Diplopia, may have bilateral blurringƒ Ocular palsyƒ Dysconjugate gaze
–Paralysis, may be focal or all 4 limbs–Numbness, may be focal or all 4 limbs–Dysarthria–Ataxia, may be only one limb

Prehospital Management of Suspected Stroke
Rapid evaluation, & determine time of onset–Can use Cincinatti Prehospital Stroke Scale–Rule out hypoxia (check pulse oximetry)–Rule out hypoglycemia (check fingerstick blood sugar)ƒ Remember that hypoglycemia can present as any focal neuro sign which may mimic stroke
–Rule out possible spine traumaƒ Neck & back immobilization if history unclear or possible fall after onset of symptoms
–Minimize total field time if stroke suspected

The Cincinatti Prehospital Stroke Scale
Facial Droop (have patient show teeth or smile)
–Normal–Abnormal (one side with less movement or droop)
Arm Drift (have patient close eyes & hold arms out)–Normal–Abnormal (one arm does not move or drifts down)
Speech (have patient say a simple sentence)–Normal–Abnormal (word slurring, inappropriate words, mute)

Initial Emergency Department Management of the Stroke Victim
Airway management–Oropharyngeal or tongue muscle paralysis can cause airway obstruction–May need suction frequently if difficulty swallowing–May need nasopharyngeal airway–Check pulse oximetry & start supplemental oxygen on all patients (even if oximetry okay)–Immobilize cervical spine if possible fall or history unclear, & obtain radiographs

Initial Emergency Department Management of the Stroke Victim
(cont.)
Breathing management–Watch for apnea–If unconscious, usually endotracheal intubation (after use of meds such as lidocaine, benzodiazepine, etomidate, etc. ) and mechanical ventilation indicated–Abnormal patterns (such as Cheyne-Stokes) are indication also for intubation & controlled ventilation

Initial Emergency Department Management of the Stroke Victim
(cont.)Circulation management
–Check fingerstick blood sugar if not done yet (and treat with IV 50 % dextrose bolus if low)–Place intravenous line with normal saline TKOƒ Hypotonic fluids contraindicated
–Treat hypotension with fluid bolus +/- pressors–Hypertension usually does NOT need emergent Rx (exception is some acute bleeds)ƒ Labetolol, nitroprusside are safest agents (but require close continuous BP monitoring)

Initial Emergency Department Management of the Stroke Victim
(cont.)Further care routinely indicated :
–Obtain lab studies (see next slide) & EKG–Rapid but complete physical exam–If seizure, treat with IV benzodiazepine followed by IV diphenylhydantoin loading (18 mg/kg)–Obtain STAT head computed tomography scan
ƒ Goal is to have scan done & read in < 45 minutes from time of E.D. arrival
–Monitor vital signs frequently –May need foley or nasogastric tube–Alert appropriate consultants

Lab Studies to Routinely Consider For Stroke Patients
Complete Blood Count (CBC)Clotting Studies (platelet count, PT, PTT)Electrolytes, Calcium, MagnesiumBlood Urea Nitrogen (BUN), creatinineBlood sugarMedication levels (such as digoxin)Toxin, alcohol, or carboxyhemoglobin levels if
exposure suspectedNote Arterial Blood Gas NOT always indicated
(may cause problem if thrombolytic used)

Considerations on Calling Consultants on Stroke Cases
If Stroke Response Team already designated, call them early
May otherwise need to wait till after CT scan is read to call correct consultant for admission–Neurosurgeon if :ƒ Intracranial hemorrhage or traumaƒ Mass lesion such as tumorƒ Hydrocephalus or shunt complication
–Neurologist if ischemic stroke–Neuroradiologist if angiographic procedure needed–Nephrologist if dialysis or hemoperfusion needed–Intensivist if mechanical ventilation needed

Differential Diagnosis of StrokeCraniocerebral and / or cervical traumaMeningitis / encephalitisHypertensive encephalopathyIntracranial cyst or tumorSeizure with postictal Todd's ParalysisComplicated migraineHyperglycemia (nonketotic hyperosmolar
coma)HypoglycemiaMedication overdose or toxin exposure

Flipped T waves from subarachnoid hemorrhage

Aspects of Computed Tomography for Stroke
Scan can be normal in ischemic stroke5 to 10 % of SAH cases have normal scan
–Lumbar punture then indicated if SAH suspected & scan is normal–Lumbar puncture will exclude later use of thrombolytics
Magnetic Resonance Imaging (MRI) can show some ischemic lesions missed by CT scan, but is not as good as CT in detecting hemorrhage

73 year old male presenting with aphasia, neglect, & visual field deficits ; CT (on left) was normal but MRI (on right) showed bilateral occipital infarcts

Subtle changes in right temporal area in scan done 4 hours after infarct

CT scan of same patient on prior slide 24 hours later showing obvious temporal infarct

General Treatment Considerations for Stroke
Reverse anticoagulants if hemorrhageTreat fever with aggressive coolingGenerally only treat hypertension if :
–Systolic BP > 220 mg Hg–Diastolic BP > 120 mm Hg–Mean BP > 130 mm Hg–Usually do NOT drop < 140 systolic or 100 diastolic–Labetolol, enalapril, or nitroprusside are best
May need direct Rx of increased intracranial pressure (ICP)
Consider nimodipine (60 mg PO q 4h) if SAH & consciousNote heparin never shown by itself to be of benefit

CT scan on left shows left hemispheric infarct on day one ; CT scan on right shows bleed occurring on day 2 after treatment with heparin


Treatment of Increased Intracranial Pressure in Stroke
Avoid hypotonic or overload of fluidsKeep head of bed elevated 30 degreesHyperventilation to pCO2 of 26 to 30 mm HgMannitol 0.5 to 2 gm/kg IV bolusesFurosemide (0.2 to 1.0 mg/kg) or
acetazolamide (250 to 500 mg) IVBarbiturates (thiopental or phenobarbital 1 to
5 mg/kg IV)–Cause cardiorespiratory depression so should only be used in ventilated monitored patients

General Considerations for Use of Thrombolytics for Stroke
Most studies have shown increased mortality and / or morbidity in patients treated with thrombolytics compared to placebo
Only the 1995 NINDS study alledgedly showed benefit–Treated patients 12 % more likely to have minimal or no disability at 3 months–NO improvement in mortality however–Follow-on studies from community hospitals show low enrollment and poorer outcomes than reported in this study at academic centers only

Features of the NINDS StudyReported in 1995
Conducted by the National Institute of Neurological Disorders and Stroke (NINDS) rt-PA Stroke Study Group
Randomized controlled trialUniv. of Cincinatti was lead center for study (8
academic centers enrolled patients)624 patients enrolled from January 1991 to
October 1994 in 2 part sequential studyAlteplase (Activase, recombinant tPA) used in
treatment arm at dose of 0.9 mg/kg (90 mg max.)

Inclusion Patient Selection Criteria for the NINDS Study
Ischemic stroke with :–Clearly defined time of onset–Measureable deficit on the National Institutes of Health Stroke Scale (NIHSS)–No evidence of hemorrhage on CT scan
Had to start to receive thrombolytic within 3 hours (180 minutes) since onset of Sx
No anticoagulants or antiplatelet agents given for 24 hours after Rx

Exclusion Criteria for the NINDS r-tPA Study
Prior stroke or head trauma within 3 monthsMajor surgery within 14 daysHistory of intracranial hemorrhageRapidly improving or minor symptomsSymptoms suggestive of SAHGI or urinary tract hemorrhage within 21 daysArterial puncture at noncompressible site within 7 daysSeizure at onset of strokeAnticaogulants or heparin within 48 hoursHigh PTT, PT > 15 sec., Platelets< 100,000Serum glucose < 50 or > 400 mg/dlBP > 185 systolic or > 110 diastolic, or "if aggressive Rx
required to reduce BP to these limits"

Results of the NINDS r-tPA Study
No significant differences in functional outcome in Part 1 of study (333 patients)
Overall 3 month mortality 21 % in placebo and 17 % in tPA group (p=NS)
In Part 2 patients treated in 91 to 180 minutes, improvement was 40 % in placebo group and 35 % in tPA group
NIHSS score was significantly different (favoring tPA) only in Part 2 patients treated within 90 minutes, and in the combined Parts 1 and 2 patients treated within 90 minutes, but not in other subgroups

Adverse Bleeding Results in the r-tPA Treated Patients in the
NINDS StudySymptomatic intracranial hemorrhage occurred in 7
% of tPA and < 1 % of placebo patients in first 36 hours– 4 more tPA and 2 more placebo patients had symptomatic bleeds in next 3 months
–61 % of patients with symptomatic bleeds died in 3 months
"Serious" systemic bleeds occurred in 5 tPA patients and zero placebo patients
Minor bleeding occurred in 23 % of tPA patients and 3 % of placebo patients

Precautions About Overextrapolation of the NINDS
Study ResultsNo improvement in overall mortalityOnly 12 % absolute (30 % relative)
improvement in functionResults are from academic centers with
strong interests in the study & dedicated stroke response teams
Only applies to small % of total stroke patients
Requires strict adherence to protocols

The NIH Stroke Scale (NIHSS) EXAM ITEM SCORE RANGE
Level of consciousness (LOC) 0 to 3 LOC Questions 0 to 2 LOC Commands 0 to 2 Best Gaze 0 to 2 Visual Fields 0 to 3 Facial Palsy 0 to 3
Motor Arm and Leg 0 to 9 Limb Ataxia 0 to 9 Sensory 0 to 2 Best Language 0 to 3 Dysarthria 0 to 9 Extinction & Inattention 0 to 2 Distal Motor Function 0 to 2

Interpretation of NIH Stroke Scale Numbers
Scale range is from zero (normal) to max. of 42
Those with minor deficits (scale <4) are not candidates for thrombolysis–Exceptions may be severe aphasia (scale = 3), or hemianopsia (scale = 2 or 3)
Those with severe deficits (scale > 22) are at increased risk for hemorrhage, & so are also not thrombolytic candidates

3 Cautionary Studies Related to Use of Thrombolytics for Stroke
Schriger et al. 1998: showed CT scans to physicians :–67 % correct by emergency physicians, 83 % correct by neurologists, 83 % correct by radiologists
–"Physicians in this study did not identify cerebral hemorrhage sufficiently to permit safe selection of candidates for thrombolytic therapy"
Engelstein et al. 2000–Set up NINDS criteria stroke protocol but had no eligible candidates for 3 years in a busy E.D.
Katzan et al. 2000–Only 1.8 % of stroke patients received tPA–tPA group mortality was 15.7 % versus 5.1 % nontreated

Other Stroke Thrombolytic Trials With Worse Outcomes in
the Thrombolytic GroupECASS-1 (1995, used tPA)ECASS-2 (1998, used tPA)MAST-I (1995, used streptokinase)MAST-E (1996, used streptokinase)ASK (1996, used streptokinase)ATLANTIS (1999, used tPA at 3 to 5
hours)

Study of Danaparoid Treatment of Acute Stroke
Reported in JAMA 1998TOAST Trial ("Trial of ORG 10172 in Acute Stroke
Treatment")Used danaparoid (ORG 10172), a low molecular
weight heparinoid, bolus then infusion for 7 daysRandomized, double blind, placebo controlled trialEligible if stroke Sx between 1 and 24 hoursEnrollment of 1281 patients 1990 to 1996No significant outcome improvement at 3 months15 intracranial bleeds in ORG group versus 5 in
placebo group

The PROACT 2 Study of Prourokinase for Stroke
JAMA Dec. 1999Prolyse in Acute Cerebral Thromboembolism trial
(PROACT) for strokes < 6 hours symptom durationUsed intraarterial prourokinase (Prolyse) for MCA clots12,323 stroke patients screened & 474 (4 %) had
angiography, and 180 of these were randomized (121 to Rx group & 59 to control group)
No difference in overall mortalityImproved functional scores in treated patientsIntracranial hemorrhage "with neurological
deterioration" in 10 % of treated & 2 % of control patients

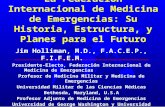
Angiogram of a 54 year old male with a left hemispheric stroke, showing embolic occlusion of the left MCA

The STARS Study of tPA for Stroke
JAMA March 2000Standard Treatment with Alteplase to Reverse
Stroke (STARS)57 centers, 389 patients from 1997 to 1998No control groupPatients refusing tPA not reportedProtocol violations in 32 %3.3 % had symptomatic ICH, 8.2 % had
asymptomatic ICH35 % had good outcome (Rankin score 0 to1) at
30 days

The STAT Study for Treatment of Stroke
JAMA May 2000Stroke Treatment with Ancrod (STAT) trialUsed defibrinogenating agent Ancrod from Malaysian
pit viper72 hour infusion, begun within 3 hours of stroke onsetFollowup doses at 96 and 120 hoursMortality 25 % in both treated & placebo groupsImproved favorable functional status in Ancrod group
(42 % versus 34 %)Symptomatic ICH 5 % vs. 2 %, asymptomatic ICH 19 %
vs. 11 % (both higher in Ancrod group)

Other Agents Being Investigated for Stroke Treatment
Hopefully will be useful in patients with contraindications to thrombolytics or those presenting late, & also be safer
Some act to limit reperfusion injury, & others act to improve or accelerate the neuronal repair process
Some trial agents recently reported out as ineffective :–Selfotel–Cerostat–Tirilizad–Lubeluzole–Citocholine–Antiinflammatory agents

Treatment of Stroke in the E.D. : Summary
Rule out hypoxia & hypoglycemia quickly & provide other supportive care
Activate stroke team early if availableDecide secondary Rx and consultants
based on stat CT scanConsider use of reperfusion agents in
carefully selected patientsObtain rehabilitative services for patient
as soon as acute episode treated