Advancing COPD treatment strategies with evidence- based ...
Upload
mohamed-essamCategory
view
1.881download
2
TREATMENT OF MPGNWhat is the evidence?
byMohamed Essam

Before we start• MPGN may be either 1ry or 2ry• All patient should be treated with standard
supportive antiproteinuric and antihypertensive measures including ACEi and ARBs.
• 1ry MPGN incidence rate is declining as reported by a systematic review of literature published in NDT 2011 where it was found to be 0.2/100,000 population/year.(1)


1ry MPGN
www.kdigo.org
KDIGO

Kidney Disease: Improving Global Outcomes
www.kdigo.org
(2)

Kidney Disease: Improving Global Outcomes
www.kdigo.org

In Adults
Asymptomatic Non
Nephrotic range
proteinuriaNormal renal
functionsNo specific treatment
Close FU / 3m
Nephrotic syndrome
Or Impaired renal functions
6m CST(Prednisone 1mg/kg BW/day)
+/- Cytotoxic drugs
Considerable reduction of proteinuria
Continue CST at the minimal effective dose
If no response within 3m
Stop CSTR with Cyclosp, Tac or
MMF(3)
RPGN with diffuse crescents
Pulse steroids and Cyclophosphamides+/- plasmapheresis
Comprehensive clinical nephrology, 2010, P. 267-268
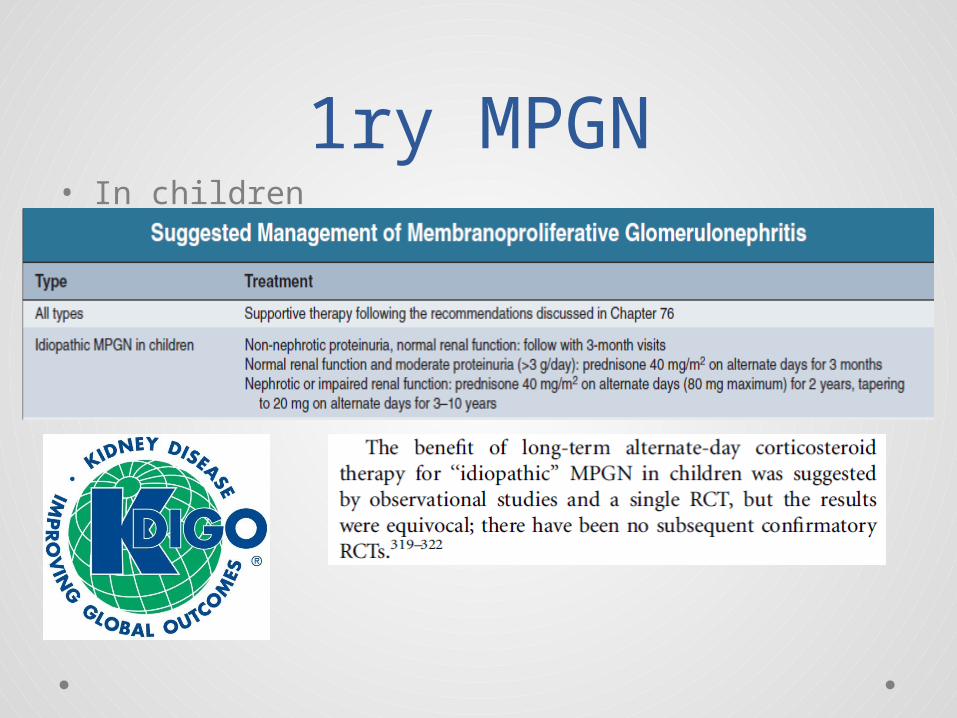
1ry MPGN• In children

2ry MPGN
• Treatment of the cause.• We will concentrate on HBV, HCV associated
MPGN.

Kidney Disease: Improving Global Outcomes
www.kdigo.org
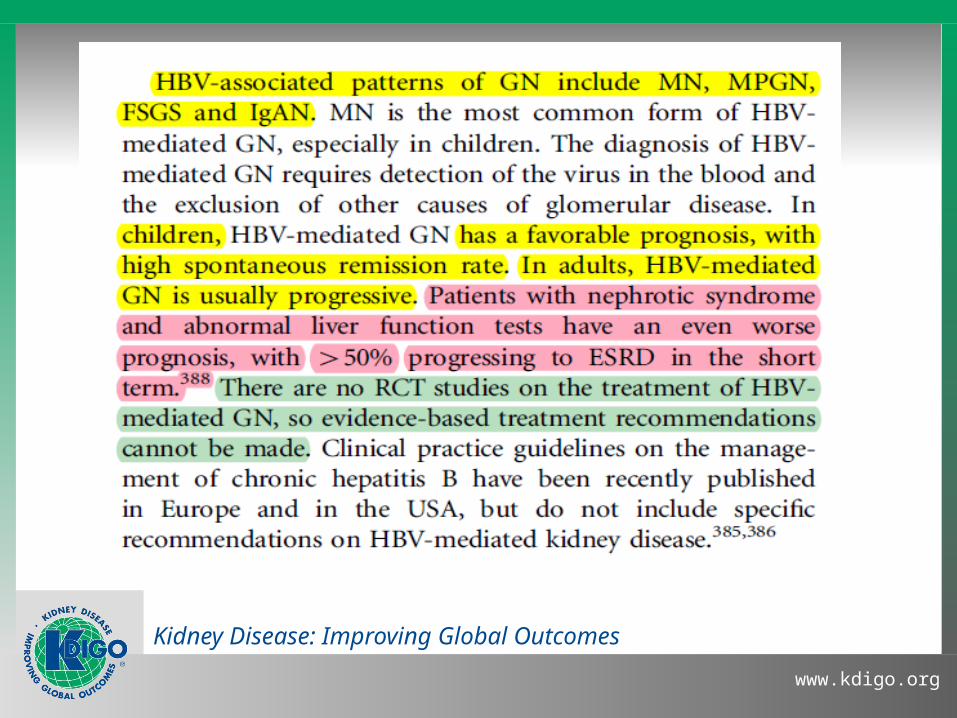
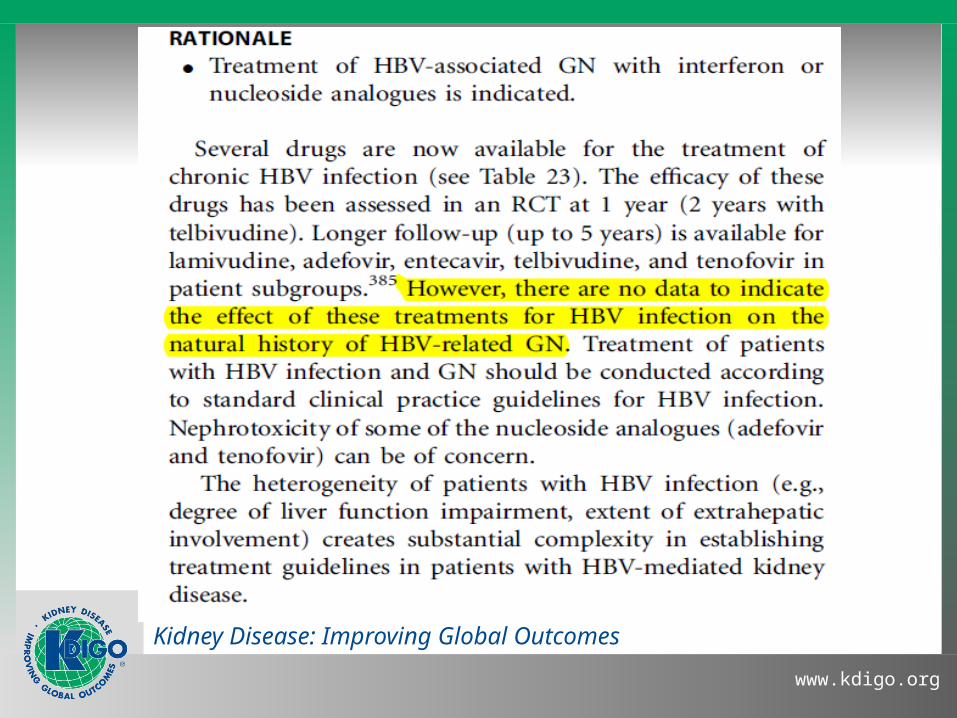
HBV Associated MPGN
Comprehensive clinical nephrology, 2010, P. 268

Kidney Disease: Improving Global Outcomes
www.kdigo.org
Kidney Disease: Improving Global Outcomes
www.kdigo.org
Kidney Disease: Improving Global Outcomes
www.kdigo.org

(4)

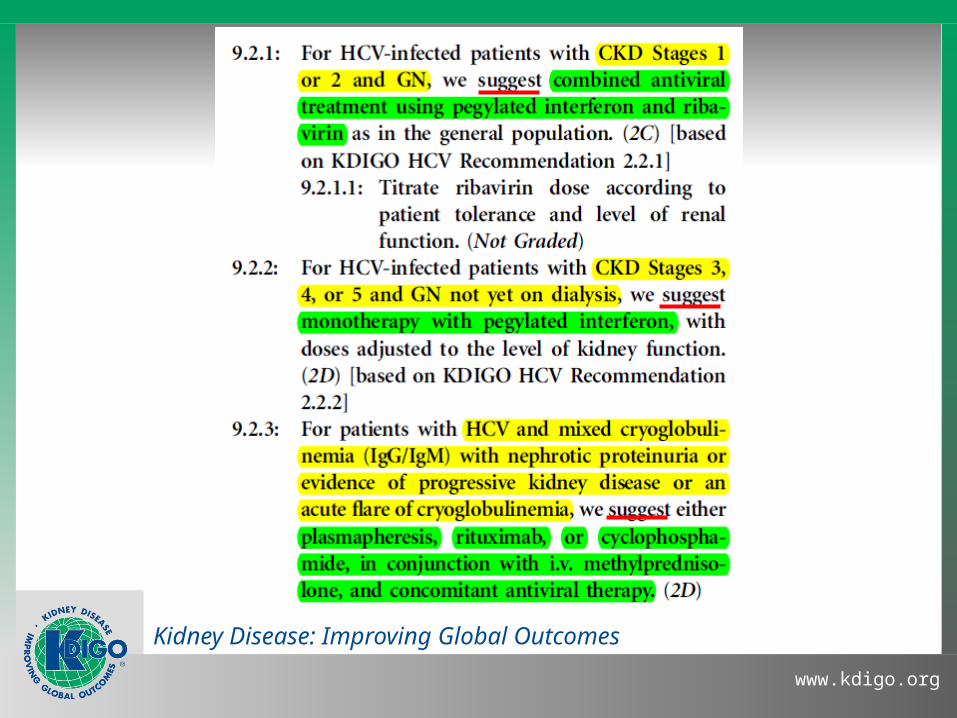
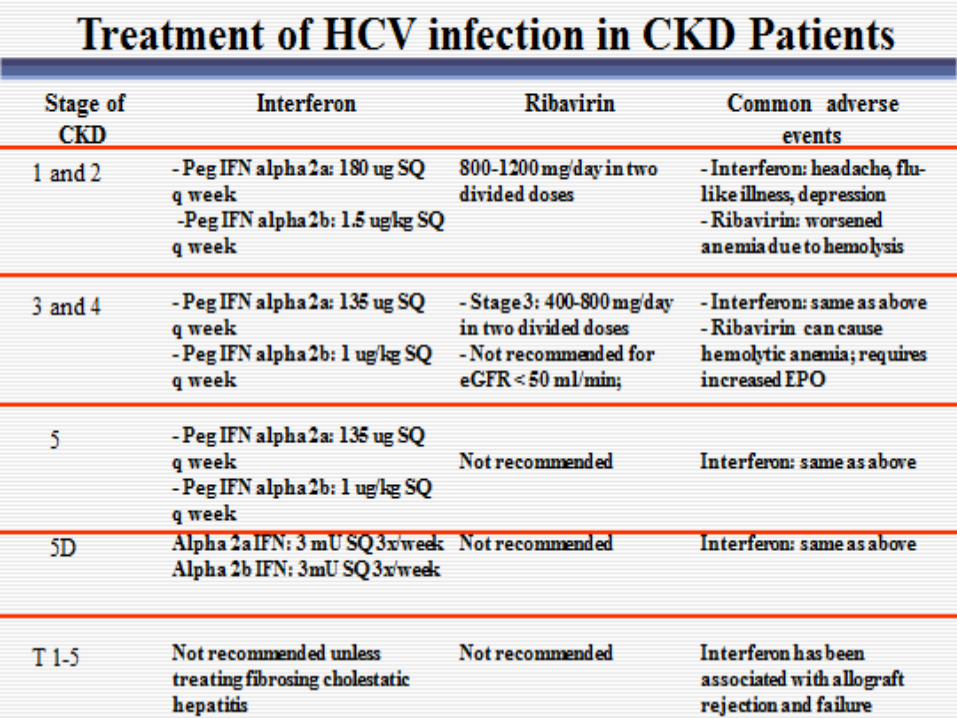
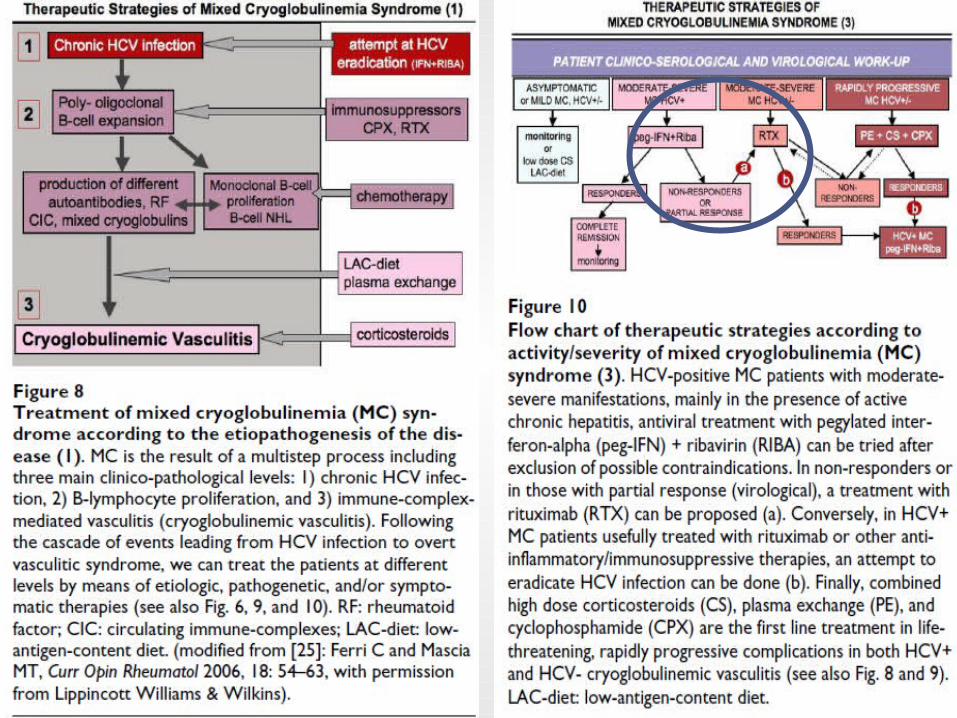
HCV Associated MPGN and Cryoglobulinemia
Kidney Disease: Improving Global Outcomes
www.kdigo.org

Kidney Disease: Improving Global Outcomes
www.kdigo.org
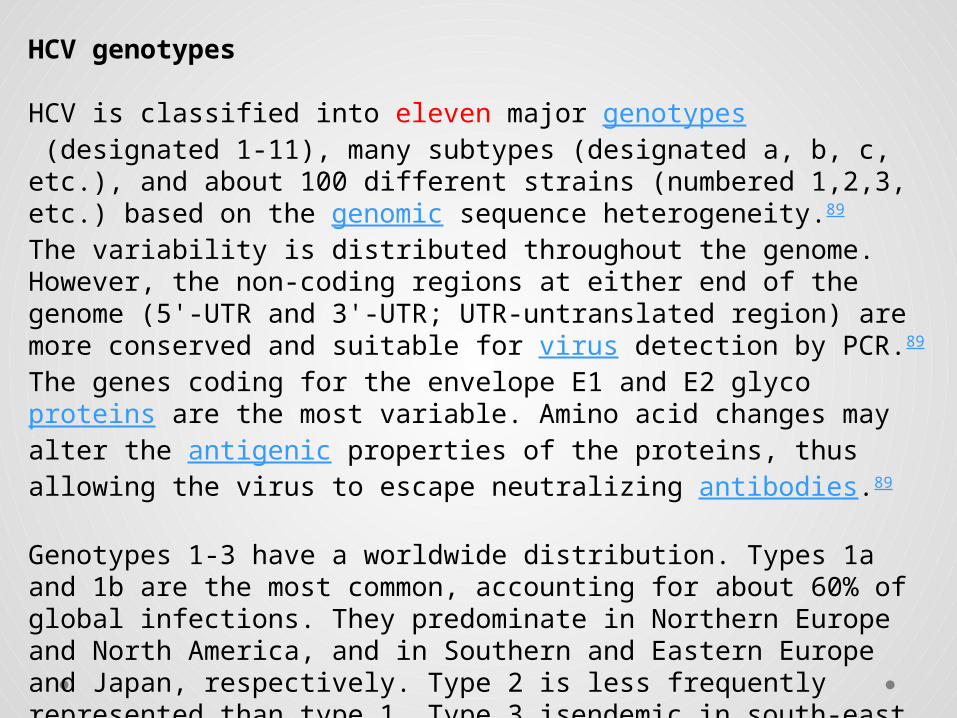
HCV genotypes
HCV is classified into eleven major genotypes (designated 1-11), many subtypes (designated a, b, c, etc.), and about 100 different strains (numbered 1,2,3, etc.) based on the genomic sequence heterogeneity.89
The variability is distributed throughout the genome. However, the non-coding regions at either end of the genome (5'-UTR and 3'-UTR; UTR-untranslated region) are more conserved and suitable for virus detection by PCR.89
The genes coding for the envelope E1 and E2 glycoproteins are the most variable. Amino acid changes may alter the antigenic properties of the proteins, thus allowing the virus to escape neutralizing antibodies.89
Genotypes 1-3 have a worldwide distribution. Types 1a and 1b are the most common, accounting for about 60% of global infections. They predominate in Northern Europe and North America, and in Southern and Eastern Europe and Japan, respectively. Type 2 is less frequently represented than type 1. Type 3 isendemic in south-east Asia and is variably distributed in different countries. Genotype 4 is principally found in the Middle East, Egypt, and central Africa. Type 5 is almost exclusively found in South Africa, and genotypes 6-11 are distributed in Asia.39, 58, 94, 103
PEGylation is the process of covalent attachment of
polyethylene glycol (PEG) polymer chains to another
molecule, normally a drug or therapeutic protein.. The
covalent attachment of PEG to a drug or therapeutic protein
can "mask" the agent from the host's immune system
(reduced immunogenicity and antigenicity), and increase the
hydrodynamic size (size in solution) of the agent which
prolongs its circulatory time by reducing renal clearance.
PEGylation can also provide water solubility to hydrophobic
drugs and proteins.

Contraindications to Treatment with
Iterferon Alfa and Ribavirin
Side Effects of Treatmetn with Interferon Alfa and
Ribavirin
Kidney Disease: Improving Global Outcomes
www.kdigo.org
Kidney Disease: Improving Global Outcomes
www.kdigo.org
Kidney Disease: Improving Global Outcomes
www.kdigo.org
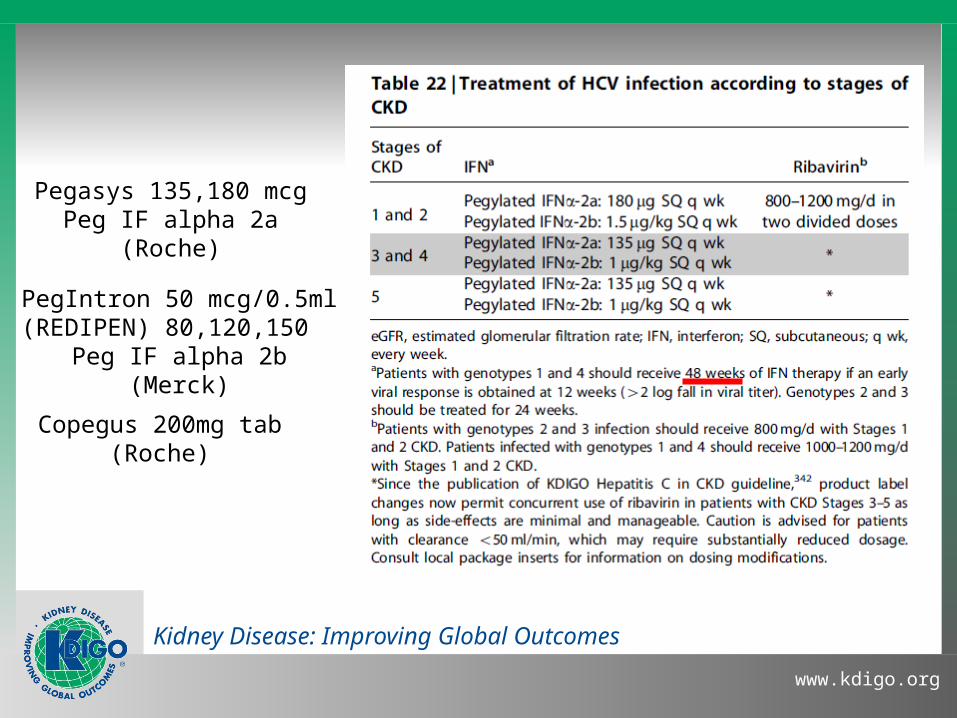
Pegasys 135,180 mcgPeg IF alpha 2a
(Roche)
PegIntron 50 mcg/0.5ml(REDIPEN) 80,120,150
Peg IF alpha 2b(Merck)
Copegus 200mg tab(Roche)

Clinical Practice Guidelines for the Diagnosis, Prevention and Management of Hepatitis C in
CKD
(5)

Management

Kidney Disease: Improving Global Outcomes
www.kdigo.org
(Int J Artif organs) March 2007

Kidney Disease: Improving Global Outcomes
www.kdigo.org

Kidney Disease: Improving Global Outcomes
www.kdigo.org

(6)

Rituximab, the monoclonal anti-CD20 antibody thatselectively targets the B cells, seems to be as least as
efficient as cyclophosphamide. Because it is also bettertolerated, it should be preferred to cyclophosphamide.
(7)

Cases
Kidney Disease: Improving Global Outcomes
www.kdigo.org
1- 45 years old patient presented to renal clinic worried about what he read on the internet about effect of HCV on his kidney,,,
He has normal renal functions, normal urine analysis, Not diabetic or hypertensive.
USS reveals normal kidney,,,
What would you do for this patient?
And what’s your evidence?
Kidney Disease: Improving Global Outcomes
www.kdigo.org
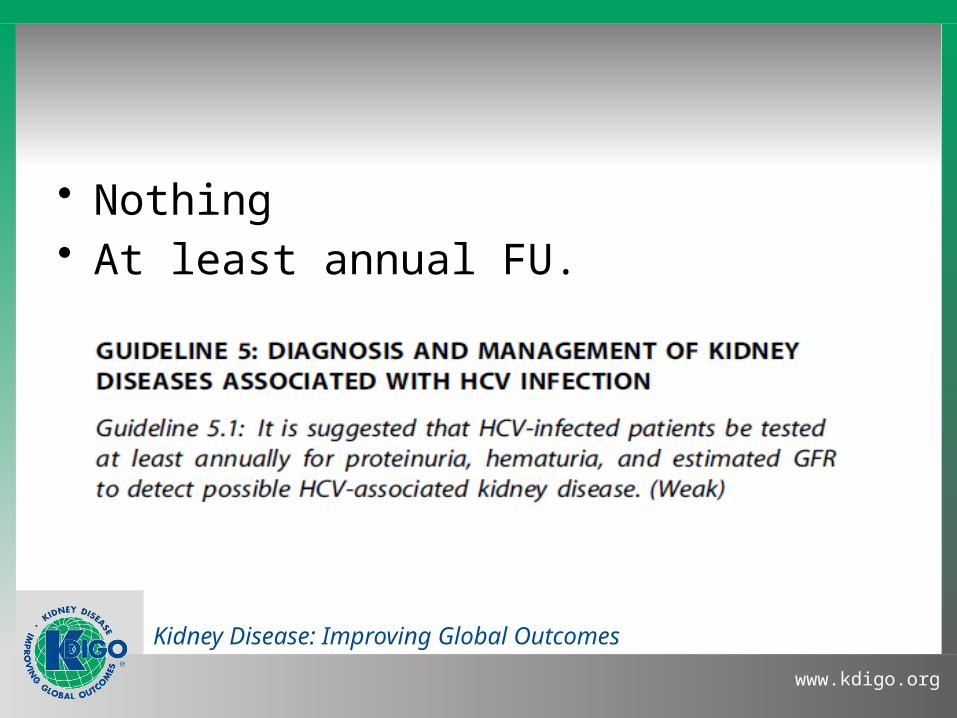
• Nothing• At least annual FU.
Kidney Disease: Improving Global Outcomes
www.kdigo.org
2- 40 y old HCV +ve patient presented with mild LL edema, renal functions are normal, urinary protein/cr ratio 2gm/day, Rh factor negative, Cryo negative.
What would you do for this patient?
And what’s your evidence?
Kidney Disease: Improving Global Outcomes
www.kdigo.org
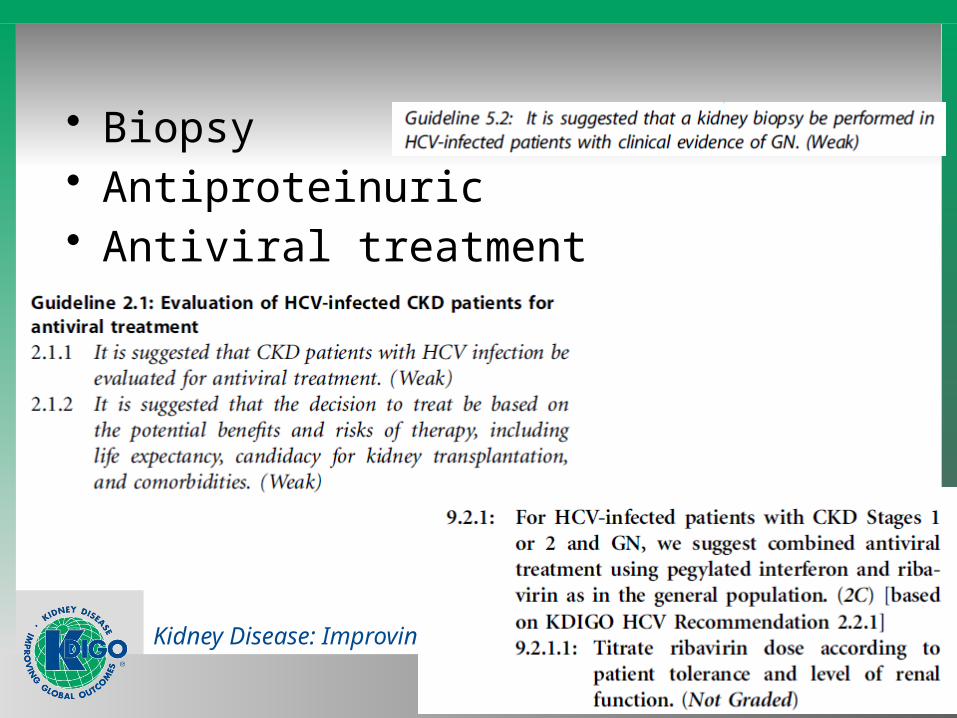
• Biopsy• Antiproteinuric• Antiviral treatment
Kidney Disease: Improving Global Outcomes
www.kdigo.org
• 43 y old male patient presented with HTN, rash on LL, edema +++, oliguria
• Ix: Cr was 5 (with previous history Cr 1 since 2 month done on routine check)
• Urine revealed hematuria, proteinuria
(active sediment)
What would you do for this patient?
And what’s your evidence?

Kidney Disease: Improving Global Outcomes
www.kdigo.org
• Pulse steroids• Cyclophosphamide or Rituximab• Plasma exchange

Kidney Disease: Improving Global Outcomes
www.kdigo.org
• 42 years old female patient presented with 2+ LL edema , renal impairment Cr 2.5,
• Urinary proteins 4 gm/day. She had HCV diagnosed 2 years ago
What would you do for this patient?
And what’s your evidence?
Kidney Disease: Improving Global Outcomes
www.kdigo.org
• Area of debate.• Antiviral for sure with dose modification.• ??? Immunosuppression or not • May be :
Antiviral ……. And if non responder :
Rituximab ???!!!

Kidney Disease: Improving Global Outcomes
www.kdigo.org
• Thank you