Treatment of liver metastases in patients with neuroendocrine tumors
12
Cell Cycle, Cell Death, and Senescence WEE1 Inhibition Sensitizes Basal Breast Cancer Cells to TRAIL-Induced Apoptosis Sireesha V. Garimella 1 , Andrea Rocca 2 , and Stanley Lipkowitz 1 Abstract TRAIL is a member of the TNF super family and has been shown to induce apoptosis in many cancer cell lines but not in normal cells. Breast cancers can be divided into different subgroups on the basis of the expression of estrogen and progesterone receptors, HER-2 amplification, or the lack of these three markers (known as triple-negative or basal-type breast cancer). Our group and others have shown previously that triple- negative breast cancer cell lines are sensitive to TRAIL whereas others are relatively resistant. In an earlier study, we reported that inhibition of WEE1, a cell-cycle checkpoint regulator, causes increased cell death in breast cancer cell lines. In this study, we tested the effects of WEE1 inhibition on TRAIL-mediated apoptosis in breast cancer cell lines. Pretreatment with WEE1 inhibitor or knockdown of WEE1 increased the toxicity of TRAIL in the basal/triple-negative breast cancer cell lines compared with WEE1 inhibitor or TRAIL treatment alone. The enhanced cell death is attributed to increased surface expression of death receptors, increased caspase activation which could be blocked by the pan-caspase inhibitor, Z-VAD-FMK, thereby rescuing cells from caspase-mediated apoptosis. The cell death was initiated primarily by caspase-8 because knockdown of caspase- 8 and not of any other initiator caspases (i.e., caspase-2, -9, or -10) rescued cells from WEE1 inhibitor– sensitized TRAIL-induced cell death. Taken together, the data suggest that the combination of WEE1 inhibitor and TRAIL could provide a novel combination for the treatment of basal/triple-negative breast cancer. Mol Cancer Res; 10(1); 75–85. Ó2011 AACR. Introduction Breast cancer is a heterogeneous group of diseases. Approximately 60% to 70% of breast cancers express estrogen receptors (ER) and/or progesterone receptors (PR), and approximately 20% to 30% of breast cancers have amplified HER-2 and thus express high levels of the HER-2 protein (1, 2). In approximately 15% to 20% of patients with breast cancer, the tumors do not express ER or PR and do not have amplification of HER-2 (1). These are catego- rized as triple-negative breast cancer (TNBC). Molecular classification by expression profiling of primary breast cancers and breast cancer cell lines has determined that the majority of these triple-negative tumors share expression profiles with basal epithelial cells of the breast duct and hence are referred to as basal-like tumors (3–6). Currently, the mainstay of treatment for these tumors is chemotherapy, and patients with these tumors have a poor prognosis (1). Thus, identification of novel, molecularly targeted therapies for triple-negative/basal-like breast cancer would be of great benefit. Studies have shown that TNBCs are defective in dou- ble-stranded DNA repair and, like many other tumor cells, lack the G 1 –S checkpoints (7, 8). WEE1, a tyrosine kinase, serves as a critical component of the response to double-stranded DNA breaks by phosphorylating CDC2, thereby activating the G 2 –M checkpoint and allowing the cells to repair the damaged DNA (9, 10). Therefore breast cancer cells, like other cancer cells, are susceptible to death induced by G 2 –M checkpoint abrogators (11). Previously, we have identified through an RNA interference (RNAi) screen of the human tyrosine kinome that silencing of WEE1 in breast cancer cells resulted in DNA damage, cell- cycle arrest in S-phase, and caspase-mediated cell death (12). TRAIL may have potential use in cancer therapy because of its ability to kill selectively cancer cells over normal cells (13–15). TRAIL binds to its receptors, TRAIL-R1 (TR1, also called DR4) or TRAIL-R2 (TR2, also called DR5) at the cell surface which leads to the recruitment of the adaptor molecule FADD and pro-caspase-8 forming the death- inducing signaling complex (DISC; ref. 16). Pro-caspase-8 Authors' Affiliations: 1 Laboratory of Cellular and Molecular Biology, Cen- ter for Cancer Research, National Cancer Institute, NIH, Bethesda, Mary- land; and 2 Department of Medical Oncology, Scientific Institute of Romagna for the Study and Treatment of Cancer (IRST) Ltd, Meldola (FC), Italy Corresponding Author: Stanley Lipkowitz, Laboratory of Cellular and Molecular Biology, Center for Cancer Research, National Cancer Institute, NIH, 37 Convent Drive, Bethesda, MD 20892. Phone: 301-402-4276; Fax: 301-496-8479; E-mail: [email protected] doi: 10.1158/1541-7786.MCR-11-0500 Ó2011 American Association for Cancer Research. Molecular Cancer Research www.aacrjournals.org 75 on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500
Transcript of Treatment of liver metastases in patients with neuroendocrine tumors

Cell Cycle, Cell Death, and Senescence
WEE1 Inhibition Sensitizes Basal Breast Cancer Cellsto TRAIL-Induced Apoptosis
Sireesha V. Garimella1, Andrea Rocca2, and Stanley Lipkowitz1
AbstractTRAIL is a member of the TNF super family and has been shown to induce apoptosis in many cancer cell
lines but not in normal cells. Breast cancers can be divided into different subgroups on the basis of theexpression of estrogen and progesterone receptors, HER-2 amplification, or the lack of these three markers(known as triple-negative or basal-type breast cancer). Our group and others have shown previously that triple-negative breast cancer cell lines are sensitive to TRAIL whereas others are relatively resistant. In an earlier study,we reported that inhibition of WEE1, a cell-cycle checkpoint regulator, causes increased cell death in breastcancer cell lines. In this study, we tested the effects of WEE1 inhibition on TRAIL-mediated apoptosis in breastcancer cell lines. Pretreatment with WEE1 inhibitor or knockdown of WEE1 increased the toxicity of TRAILin the basal/triple-negative breast cancer cell lines compared with WEE1 inhibitor or TRAIL treatment alone.The enhanced cell death is attributed to increased surface expression of death receptors, increased caspaseactivation which could be blocked by the pan-caspase inhibitor, Z-VAD-FMK, thereby rescuing cells fromcaspase-mediated apoptosis. The cell death was initiated primarily by caspase-8 because knockdown of caspase-8 and not of any other initiator caspases (i.e., caspase-2, -9, or -10) rescued cells from WEE1 inhibitor–sensitized TRAIL-induced cell death. Taken together, the data suggest that the combination of WEE1inhibitor and TRAIL could provide a novel combination for the treatment of basal/triple-negative breastcancer. Mol Cancer Res; 10(1); 75–85. �2011 AACR.
Introduction
Breast cancer is a heterogeneous group of diseases.Approximately 60% to 70% of breast cancers expressestrogen receptors (ER) and/or progesterone receptors (PR),and approximately 20% to 30% of breast cancers haveamplified HER-2 and thus express high levels of the HER-2protein (1, 2). In approximately 15% to 20% of patientswith breast cancer, the tumors do not express ER or PR anddo not have amplification of HER-2 (1). These are catego-rized as triple-negative breast cancer (TNBC). Molecularclassification by expression profiling of primary breastcancers and breast cancer cell lines has determined that themajority of these triple-negative tumors share expressionprofiles with basal epithelial cells of the breast duct and
hence are referred to as basal-like tumors (3–6). Currently,the mainstay of treatment for these tumors is chemotherapy,and patients with these tumors have a poor prognosis (1).Thus, identification of novel, molecularly targeted therapiesfor triple-negative/basal-like breast cancer would be of greatbenefit.Studies have shown that TNBCs are defective in dou-
ble-stranded DNA repair and, like many other tumor cells,lack the G1–S checkpoints (7, 8). WEE1, a tyrosinekinase, serves as a critical component of the response todouble-stranded DNA breaks by phosphorylating CDC2,thereby activating the G2–M checkpoint and allowing thecells to repair the damaged DNA (9, 10). Therefore breastcancer cells, like other cancer cells, are susceptible to deathinduced by G2–M checkpoint abrogators (11). Previously,we have identified through an RNA interference (RNAi)screen of the human tyrosine kinome that silencing ofWEE1 in breast cancer cells resulted in DNA damage, cell-cycle arrest in S-phase, and caspase-mediated cell death(12).TRAIL may have potential use in cancer therapy because
of its ability to kill selectively cancer cells over normal cells(13–15). TRAIL binds to its receptors, TRAIL-R1 (TR1,also calledDR4) or TRAIL-R2 (TR2, also calledDR5) at thecell surface which leads to the recruitment of the adaptormolecule FADD and pro-caspase-8 forming the death-inducing signaling complex (DISC; ref. 16). Pro-caspase-8
Authors' Affiliations: 1Laboratory of Cellular and Molecular Biology, Cen-ter for Cancer Research, National Cancer Institute, NIH, Bethesda, Mary-land; and 2Department of Medical Oncology, Scientific Institute ofRomagna for the Study and Treatment of Cancer (IRST) Ltd, Meldola (FC),Italy
Corresponding Author: Stanley Lipkowitz, Laboratory of Cellular andMolecular Biology, Center for Cancer Research, National Cancer Institute,NIH, 37 Convent Drive, Bethesda, MD 20892. Phone: 301-402-4276; Fax:301-496-8479; E-mail: [email protected]
doi: 10.1158/1541-7786.MCR-11-0500
�2011 American Association for Cancer Research.
MolecularCancer
Research
www.aacrjournals.org 75
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

is cleaved to its active form at the DISC which then cleavesand activates the downstream executioner caspases-3 and -7(16). Active caspase-8 can also cleave the BH3 protein BIDwhich results in activation of the intrinsic mitochondrialpathway of apoptosis and the activation of caspase-9 (17).Work done in animals has shown that TRAIL mediatesregression of cancer xenografts without affecting normaltissues (14). Human phase I studies have shown that TRAILagonists are safe and phase II trials are now in progress (18).Initial reports of TRAIL-mediated apoptosis in breast
cancer cell lines have shown that while TRAIL could induceapoptosis in the MB231 breast cancer cell line, the majorityof cell lines testedwere highly resistant (13, 19–21). The datafrom several groups, including ours, have shown that mostTNBC/basal cell lines and a few of theHER-2–amplified celllines are sensitive to TRAIL-induced apoptosis, but all ER-positive (ERþ) breast cancer cells are resistant to TRAIL-induced apoptosis (22–24). Studies in the literature haveinvestigated the combination of a wide range of chemother-apeutic drugs and radiation with TRAIL agonists to poten-tiate cell death and/or overcome resistance in breast cancercells (24, 25).In this study, we find that loss ofWEE1 function enhances
TRAIL-mediated apoptosis in TNBC/basal breast cancercells. The enhanced apoptosis is mediated by increasedcaspase activation and dependent on the initiator caspase,caspase-8.
Materials and Methods
Cell cultureThe MDA-MB231 (MB231), HCC38, BT549, BT474,
MCF7, Hs578T, and SKBR3 cell lines were obtained fromAmerican Type Culture Collection and BT20 andHCC1937 were obtained from Reinhard Ebner (AvalonPharmaceuticals). American Type Culture Collection celllines are authenticated by short tandem repeat analysis. Onreceiving the cell lines, they were immediately cultured andexpanded to prepare frozen ampule stocks. Cells werepassaged for no more than 2 to 3 months before establishingnew cultures from the early-passage frozen ampules. MB231cells were grown in RPMI-1640 medium supplementedwith 5% FBS, (R5); all other cells were grown in RPMI-1640 medium supplemented with 10% FBS (R10). Allgrowth media contained 100 units/mL of penicillin and100 units/mL of streptomycin.
InhibitorsWEE1 inhibitor II [6-butyl-4-(2-chlorophenyl)-9-hydro-
xypyrrolo[3,4-c]carbazole-1,3-(2H,6H)-dione; Calbio-chem, 681641]; the pan-caspase inhibitor, Z-VAD-FMK(Biomol International, P416) and caspase-3 inhibitor, Ac-DEVD-CHO (Biomol International, P410) were dissolvedin dimethyl sulfoxide (DMSO) and used at 10 or 100 mmol/L concentrations, as described in the text. The glutathione S-transferase (GST)-TRAIL construct and the isolation ofrecombinant GST-TRAIL fusion protein have beendescribed previously (23). The GST-TRAIL protein (at
0.5 mg/mL in culture media) was stored at �70�C inaliquots until used.
Cell viability assaysCellular cytotoxicity was assessed by the MTS assay using
the CellTiter 96 AQueous One Solution Cell ProliferationAssay (Promega Corporation, G3582) as previouslydescribed (23). All MTS measurements were done in repli-cates of 6wells, and each experiment was carried out at least 3times. Results are given as the mean � SEM of at least 3independent experiments.
Trypan blue stainingCells were incubated with Trypan blue stain (Invitrogen,
15250–061) after transfectionwith siRNAor treatmentwithinhibitors and/or GST-TRAIL. Cells that excluded the dye(viable) and cells that retained the dye (dead) were counted.
siRNA transfectionThe WEE1 ON-TARGET plus SMARTpool siRNA
(siWEE1, L-005050–00) and a nontargeting siRNA controlpool (siNEG, D-001810–10) were purchased from Dhar-macon. HCC38 cells were transfected in solution with thesiRNA pool at a final concentration of 50 nmol/L usingOligofectamine (Invitrogen, 12252011; 7 mL/mL). Trans-fected cells were plated in 6-well plates (2 � 105 cells perwell). Eight hours later, one well with the siNEG-transfectedcells and one well with the siWEE1-transfected cells weretreated with 2.5 ng/mLTRAIL. The percentage of dead cellswas determined after 15 hours using Trypan blue stain.Results shown represent mean � SEM of 3 experiments.Other cells in the 6-well plate were used for protein analysis.
Sub-G1 analysisCells (1 � 106) were plated overnight, treated with 10
mmol/L WEE1 inhibitor for 4 hours followed with 100 ng/mLTRAIL for 17 hours. Then, the cells were incubatedwith10 mmol/L bromodeoxyuridine (BrdU; Sigma-Aldrich,5002) for 15 minutes, trypsinized, washed with PBS, andfixed in cold 70%ethanol. Stainingwas conductedwith anti-BrdU-FITC antibody (BD Biosciences, 347583) and 5 mg/mL propidium iodide (Invitrogen, P3566). Flow cytometrywas conducted on a BD FACSCalibur (BD Biosciences) andanalyzed using FlowJo software.
Annexin V stainingAfter treatment with 10 mmol/L WEE1 inhibitor for 4
hours or TRAIL (100 ng/mL) for 17 hours or their com-bination, cells were stained using Annexin V-FITC Apo-ptosis Detection kit II (BD Pharmingen, 51-6710AK) as perthe manufacturer's protocol. Flow cytometry was conductedon a BD FACSCalibur and analyzed using FlowJo software.
Caspase-Glo 3/7 assayCells incubated with Z-VAD-FMK or DEVD-CHO
(100 mmol/L) or DMSO for 1 hour were treated with 10mmol/L WEE1 inhibitor or DMSO for 4 hours, and thenwith 100 ng/mL TRAIL for 2 hours at 37�C. The assay was
Garimella et al.
Mol Cancer Res; 10(1) January 2012 Molecular Cancer Research76
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

done as described previously (12). Results are shown asmean� SEM of 3 independent experiments normalized toDMSO-treated cells.
Flow cytometry for TR1 and TR2MB231 cells treated with DMSO orWEE1 inhibitor (10
mmol/L) for 24 hours were trypsinized into sorter medium(PBS with 1% fetal calf serum and 0.5 mmol/L EDTA and0.02 mmol/L sodium azide). All antibodies used for fluo-rescence-activated cell-sorting (FACS) analysis were pur-chased from R&D Systems. One million cells in 50 mLwere incubated with 10 mL of mouse IgG1-PE (IC002P) ormouse IgG2B (IC0041P) or anti-TR1-PE (FAB347P) oranti-TR2-FITC (FAB6311P) for 45 minutes on ice. TR1andTR2 surface expression wasmeasured by flow cytometryconducted on a BD FACSCalibur and analyzed usingFlowJo software.
Lysate preparation and immunoblottingCell lysates were made, and immunoblotting was con-
ducted as described earlier (23). The following antibodieswere used: caspase-8 (Clone 1C12, 9746), pY15CDC2(4539), CDC2 (9112), caspase-9 (9502), caspase-3(9662), BCL-2 (2872), BCL-xL (2762), and GAPDH(2118) from Cell Signaling Technology; caspase-10(M059–3) from MBL; WEE1 (5285), MCL-1 (819), cas-pase-2 (625), ERK2 (154), HSC70 (7298), and PARP(7150) from Santa Cruz Biotechnology; TR1 (Genetex,28414); TR2 (Prosci Inc., 2019); FLIP (Imgenex, 104);and survivin (R&D Labs, AF886).
StatisticsStatistical comparison of mean values was conducted
using the paired Student t tests. All P values are 2 tailed.
Results
WEE1 inhibition sensitizes breast cancer cells to TRAILtreatmentPreviously, we have shown that WEE1 loss or inhibition
induces cell-cycle arrest and caspase-mediated cell death inbreast cancer cell lines whereas nontransformed cell lines arenot affected (12). This cell death was observed only aftermore than 2 days of WEE1 loss or inhibition. TNBC cellswith a mesenchymal phenotype (so called basal B) are moresensitive to TRAIL than the other subsets of breast cancercells, and this cell death can be observed within less than 24hours of TRAIL treatment (13, 20, 21, 23, 24). We testedthe effect of the combination of WEE1 inhibition onTRAIL-mediated apoptosis using a panel of breast cancercell lines, including basal B/TNBC (MB231, HCC38,MB157, BT549, Hs578T), basal A/TNBC (BT20,HCC1937), HER-2–amplified (BT474, SKBR3) and ERþ
(MCF7, T47D) breast cancer cell lines. In these experi-ments, cells were preincubated with or without WEE1inhibitor II (26) for 4 hours, sub-IC50 doses of TRAIL werethen added, and the viability was assessed 17 hours later byMTS assay. Basal B/TNBC cells were the most sensitive to
the combined treatment. In the basal B/TNBC cells, WEE1inhibition alone caused 20% to 30% decrease in viability,whereas treatment of cells with sub-IC50 doses of TRAILalone caused approximately 5% to 30% loss in viability.However, the pretreatment of cells with theWEE1 inhibitorfollowed by TRAIL treatment resulted in enhanced celldeath (60%–90%) compared with the untreated controls(Fig. 1A). Also, the basal A/TNBC HCC1937 cells and theHER-2–amplified cells were found to be sensitive to theWEE1 inhibitor and TRAIL combination but to a lesserextent than the basal B/TNBC cells. The ERþ cell lines,MCF7 and T47D, were relatively resistant to each agentalone and did not show any effect to the combinationtherapy at these sub-IC50 doses of TRAIL. To assess whetherhigher doses of TRAIL would enhance cell death in theMCF7 cell line, we treated MB231 or MCF7 cells with 10mmol/LWEE1 inhibitor for 4 hours and then with differentdoses of TRAIL for 17 hours ( Fig. 1B). In MB231 cells,pretreatment withWEE1 inhibitor significantly reduced theIC50 of TRAIL (from >1,000 to �8 ng/mL), whereas inMCF7 cells, there was no change in viability in the presenceor absence ofWEE1 inhibitor over the wide range of TRAILconcentrations tested. The WEE1 inhibitor blocked WEE1function as measured by the decrease in the phosphorylationon Tyr15 of CDC2 in both of these cell lines (Fig. 1C).These data indicate that the WEE1 inhibitor significantlyincreases the sensitivity of the basal B/TNBC cells toTRAIL-mediated inhibition, modestly increases the sensi-tivity to TRAIL-mediated inhibition in basal A/TNBC celllines and HER-2–amplified cell lines but does not increaseTRAIL sensitivity in resistant ERþ cell lines.Whereas WEE1 inhibitor II is relatively specific for
WEE1, it is possible that the effects seen above were dueto off-target inhibition of other kinases (26). To confirm thatthe effects of the WEE1 inhibitor were acting throughinhibition of WEE1, we measured the effects of loss ofWEE1 by RNAi on TRAIL-mediated cell death.WEE1 wasknocked down by gene-specific siRNA for 8 hours followedby treatment of cells with TRAIL for 17 hours, and the celldeath was determined by counting dead cells as measured bythe uptake of Trypan blue. WEE1 silencing resulted indecreased WEE1 protein levels and decreased Tyr15 phos-phorylation of CDC2 (Fig. 2A). Silencing ofWEE1 alone for24 hours caused cell death in 10% of the cells, only slightlymore than cells treated with the control siRNA (siNEG; Fig.2B). Treatment of the siNEG-transfected cells with a sub-therapeutic concentration of TRAIL did not significantlyenhance cell death compared with the untreated cells.However, cells in which WEE1 protein has been reducedby siRNA exhibited a 4-fold increase in the percentage ofdead cells when these cells were treated with TRAIL, con-firming that loss of WEE1 function sensitizes cells toTRAIL-induced cell death.
Cell death caused by WEE1 inhibition and TRAIL iscaspase-dependent apoptosisTRAIL acts through the extrinsic death pathway inducing
caspase-mediated apoptosis (16). Previously, we showed that
WEE1 Inhibition and TRAIL Toxicity in Breast Cancer Cells
www.aacrjournals.org Mol Cancer Res; 10(1) January 2012 77
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

WEE1 inhibition causes apoptotic cell death in breast cancercells (12). To determine whether the treatment of WEE1-inhibited cells with TRAIL would cause an increase inapoptosis compared with either of the 2 independent drugs,we measured the fraction of cells with sub-G1 DNA contentusing propidium iodide (Fig. 3A) and the Annexin V–positive cells ( Fig. 3B) by FACS analysis. The combinationof WEE1 inhibitor and TRAIL resulted in a significantlyincreased percentage of cells with sub-G1 DNA contentcompared with each of the other treatments or untreatedcells (P < 0.01; Fig. 3A). WEE1 inhibition alone signifi-cantly increased the percentage of cells with sub-G1 DNAcontent (P < 0.005), suggesting that there is increased DNAdamage in cells treated with WEE1 inhibitor as we havepreviously shown (ref. 12; Fig. 3A). TRAIL treatment aloneresulted in a borderline increase in the percentage of cellswith sub-G1 DNA content (P ¼ 0.07). Also, the combina-
tion treatment increased the percentage of AnnexinV–positive cells significantly compared with any of the singletreatments or untreated cells (P < 0.0005; Fig. 3B). Underthese conditions, neither WEE1 inhibitor nor TRAIL aloneresulted in a significant increase in Annexin V–positive cells.Caspase activation is a key step in apoptosis induced by
TRAIL receptors and WEE1 inhibition (12, 13). Cellstreated with WEE1 inhibitor, TRAIL, or with both in thepresence or absence of the pan-caspase inhibitor Z-VAD-FMK were stained with Trypan blue and counted forthe number of dead cells. In the TNBC cell lines, MB231(Fig. 4A) and HCC38 (Fig. 4B), WEE1 inhibition orTRAIL treatment alone resulted in approximately 10% to15% dead cells whereas the combined treatment resulted in40% to 50% dead cells. Pretreatment with Z-VAD-FMKcompletely abrogated the induction of cell death by WEE1inhibition, TRAIL treatment, and the combination.
MCF7MB231
IB: pY15 CDC2
IB: CDC2
IB: HSC70
++ -WEE1 inhibitor -
+ +-TRAIL -
++ --
+ +--
MB231 MCF7
A
B
C
TNBC/Basal-like
Basal B Basal A
HER-2 amplified ER+
0
20
40
60
80
100
120
T47DMCF7SKBR3BT474HCC1937BT20Hs578TBT549MB157HCC38MB231
% v
iab
ilit
y
DMSO TRAIL WEE1 inhibitor WEE1 inhibitor and TRAIL
*
*
**
*
**
*#
#
#
0
20
40
60
80
100
120
1,000500250125643216840
TRAIL (ng/mL)
0
20
40
60
80
100
120
1,000500250125643216840
TRAIL (ng/mL)
% v
iab
ilit
y
DMSO
WEE1 inhibitor
DMSO
WEE1 inhibitor
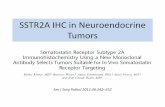
Figure 1. WEE1 inhibition sensitizesbasal breast cancer cells to TRAIL.A, a panel of breast cancer cell lineswere treated with WEE1 inhibitor(10 mmol/L) for 21 hours, withTRAIL for 17 hours, or pretreatedwith WEE1 inhibitor for 4 hours andthen treated with TRAIL for 17hours. HCC38 cells were treatedwith 0.5 ng/mL TRAIL and MB157cells were treated with 50 ng/mLTRAIL. All other cell lines weretreated with 125 ng/mL of TRAIL.Cell viability wasmeasured byMTSassay and is plotted as a percentchange relative to the DMSOcontrol. The combined treatmentwas compared with eithertreatment alone by a 2-tailedStudent t test (�, viability ofcombined treatment less thaneither treatment alone P < 0.05; #,viability of combined treatment notsignificantly different from eithertreatment alone). B, sensitization ofthe triple-negative cell line MB231and ER-positive cell line MCF7 byWEE1 inhibitor was measured atdifferent doses of TRAIL by MTSassay. C, WEE1 inhibition wasassessed by immunoblotting (IB)for pY15CDC2. Total CDC2 andHSC70 are shown as loadingcontrols. All MTS values representthe mean of 3 experiments� SEM.
Garimella et al.
Mol Cancer Res; 10(1) January 2012 Molecular Cancer Research78
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

Together, the results shown in Figs. 3 and 4 are consistentwith the induction of caspase-dependent apoptosis by thecombination of WEE1 inhibitor and TRAIL.
Caspase-8 is the initiator caspaseCaspases are activated by proteolytic cleavage from a
precursor form (pro-caspases) to active cleaved products(27). To investigate the differential activation of caspases byWEE1 inhibitor, TRAIL, or the combination, we measuredthe disappearance of pro-caspase-8, -9, and -3 (Fig. 5A).WEE1 inhibition alone did not result in detectable activationof any of the caspases asmeasured by the loss of the precursors(indicated by the arrows). Treatment with TRAIL aloneresulted in activation of caspase-8 and -3 but no appreciableactivation of caspase-9 (as measured by the loss of theprecursor). Also, there was appearance of the cleaved formof caspase-8 with TRAIL treatment (arrowhead in top panelof Fig. 5A).The combinationofWEE1 inhibitor andTRAILresulted in greater activation of caspase-8 and -3 and alsoactivation of caspase-9 as measured by pro-caspase loss. Also,there is more caspase-8 cleavage product in the cells treatedwith the combination. PARP-1 is cleaved by activated cas-
pase-3 (27). We used loss of full-length PARP-1 (arrow) andthe appearance of cleaved PARP-1 (arrowhead) as a measureof caspase activity ( Fig. 5A, panel 4).WEE1 inhibition alonedid not lead to measurable PARP-1 cleavage whereas TRAILalone resulted in appearance of cleaved PARP-1 (Fig. 5A,panel 4, lanes 2 and 3). The combination ofWEE1 inhibitorand TRAIL treatment resulted in significantly increasedPARP-1 cleavage as measured by loss of the full-lengthPARP-1 and the appearance of more cleaved PARP-1(Fig. 5A, panel 4, lane 4). Thus, the combination of WEE1inhibitor and TRAIL results in greater activation of caspases.We measured upstream (caspase-8) and downstream (cas-
pase-3/7) caspase activity using Caspase-Glo assays to quan-tify the increase in caspase activity inMB231 cells ( Fig. 5B).TRAIL treatment alone resulted in a 2- to 3-fold increase inboth caspase-8 and caspase-3/7 activity whereas WEE1inhibition alone had no significant effect (Fig. 5Bi and ii,respectively, white bars). The combination of WEE1 inhib-itor and TRAIL resulted in an approximately 30% to 40%increase in both caspase-8 and caspase-3/7 activity comparedwith TRAIL alone and in an approximately 4-fold increasecompared with either untreated cells or cells treated withWEE1 inhibitor alone [Fig. 5B (i) and (ii) respectively, whitebars]. Activation of caspase-8 and caspase-3/7was completelyblocked by addition of the pan-caspase inhibitor Z-VAD-FMK [Fig. 5B (i) and (ii) respectively, striped bars]. Caspase-8 can be activated in a retrograde manner by caspase-3 (28).To test whether the increased activity of caspase-8 seen upontreatment of cells with WEE1 inhibitor and TRAIL wasdownstream of caspase-3, we inhibited caspase-3 withDEVD-CHO ( Fig. 5B, black bars). Caspase-3 activity wascompletely blocked byDEVD-CHO for all treatments [ Fig.5B (ii)]. In contrast, caspase-8 activity was only slightlydecreased by the caspase-3 inhibitor [ Fig. 5B (i), black bars].Importantly, the increase in caspase-8 activity induced by thecombination of WEE1 inhibition with TRAIL comparedwithTRAIL alonewasmaintained in the presence ofDEVD-CHO [Fig. 5B (i)]. This suggests that the WEE1 inhibitorincreases TRAIL-induced caspase-8 activation.Caspases are activated by distinct stimuli and the first
caspases activated are known as initiator caspases (24, 27).TRAIL binds to its agonistic receptors (TR1 and TR2) andactivates caspase-8 and/or caspase-10. The caspase assaysabove (Fig. 5B) suggested that the combined treatment ofWEE1 inhibitor and TRAIL initiates caspase activation viacasapse-8. However, it is also possible that WEE1 inhibitionactivates adistinct initiator inadditiontocaspase-8orcaspase-10 and that this accounts for the increase in caspase-3/7activity seen upon treatment with WEE1 inhibitor andTRAIL. To identify the initiator caspase involved in the dualtreatment, eachof theknown initiator caspases (caspase-2, -8,-9, and -10) were silenced using specific siRNAs in MB231cells and then the cells were treated with DMSO, WEE1inhibitor, or TRAIL or the combination ( Fig. 6). Cells werestainedwithTrypan blue, and the dead cells were counted foreach treatment and compared with those of the nontargetingsiRNA (siNEG). In siNEG-transfected cells, the combina-tion ofWEE1 inhibitor andTRAIL resulted in a significantly
A
B
0
10
20
30
40
50
siWEE1siNEG
siRNA (50 nmol/L)
% d
ea
d c
ell
s
Control
2.5 ng/mL TRAILP < 0.005
P < 0.005
IB: WEE1
IB: pY15 CDC2
IB: CDC2
IB: ERK2
NEG NEG WEE1WEE1
2.5 ng/mL TRAIL
siRNA
- - + +
Figure 2. Silencing ofWEE1 by siRNA in the breast cancer cell line HCC38sensitizes the cells to TRAIL-induced cell death. A,Western blot analysesshow the knockdownofWEE1expression anddecrease in pY15CDC2bysynthetic siRNA (50 nmol/L) at 24 hours. Total CDC2 and ERK2 proteinsare shown as loading controls. B, control siRNA (siNEG) or siWEE1-transfected cells were treated with or without TRAIL (2.5 ng/mL) 8 hoursafter transfection. Cell counts with Trypan blue were conducted in thesiNEG or siWEE1-transfected cells in the absence (white bars) or thepresence (black bars) of TRAIL for 17 hours. The values represent meanvalues � SEM of 3 independent experiments. IB, immunoblotting.
WEE1 Inhibition and TRAIL Toxicity in Breast Cancer Cells
www.aacrjournals.org Mol Cancer Res; 10(1) January 2012 79
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

higher percentage of dead cells than either treatment alone oruntreatedcells [Fig.6A(i) and(ii),whitebars], similar to thosepreviously shown in Fig. 4A (black bars). WEE1 inhibitorandTRAILalone resulted ina small increase in thepercentageof dead cells compared with untreated controls [Fig. 6A (i)and (ii), white bars]. Knockdown of caspase-8 resulted in asignificant decrease in the percentage of dead cells when cellswere treated with TRAIL or with the combination ofWEE1inhibitor and TRAIL [Fig. 6A (i) and (ii), black bars].However, knockdown of caspase-2, -9, or -10 did not resultin the inhibition of cell death in the presence of WEE1inhibitor, TRAIL, or the combination [ Fig. 6A (i) and (ii)].The knockdown of each caspase was confirmed by immu-noblotting (Fig. 6B). These studies suggest that caspase-8 isthe key initiator caspase in cell death causedbyTRAIL in cellssensitized by WEE1 inhibition.The decrease in pro-caspase-9 (shown above in Fig. 5A) in
cells treated with WEE1 inhibitor and TRAIL suggests theinvolvement of the intrinsic apoptosis pathway. The intrin-
sic pathway could be activated by caspase-8 or the WEE1inhibitor could be independently activating the intrinsicpathway. To determine whether the activation of the intrin-sic pathway is dependent on initiator caspase-8 or is inde-pendent of it, loss of precursor caspase-9 was monitored incells in which caspase-8 was knocked down (Fig. 6C). Thecombined treatment with WEE1 inhibitor and TRAILresulted in the decrease of both pro-caspase-8 and -9 in thesiNEG-transfected cells (Fig. 6C, lane 4). Strikingly, in theabsence of caspase-8, there was no evidence for a decrease inpro-caspase-9 (Fig. 6C, lane 8). This indicates that in cellstreated with WEE1 inhibitor and TRAIL, the intrinsicpathway of apoptosis is triggered by the activation of theinitiator caspase-8.Altogether, these results indicate that WEE1 treatment
enhances TRAIL-mediated apoptosis through increasedactivation of the initiator caspase, caspase-8.
0
10
20
30
40
50
WEE1 inhibitorTRAILWEE1 inhibitorDMSO
and TRAIL
% S
ub
-G1 c
ell
s
0
5
10
15
20
25
30
WEE1 inhibitorTRAILWEE1 inhibitorDMSO
and TRAIL
% A
nn
ex
in V
–p
os
itiv
e c
ell
s
A
B
Figure 3. WEE1 inhibition followed by TRAIL treatment results inapoptotic cell death in MB231 cells. A, the percentage of cells with sub-G1 DNA content was measured by propidium iodide staining after21 hours of WEE1 (10 mmol/L) inhibition or 17 hours of treatment withTRAIL (100 ng/mL) or pretreatment with WEE1 inhibitor (10 mmol/L) for4 hours followed by TRAIL treatment (100 ng/mL) for 17 hours. Thegraph represents the mean values � SEM of 3 independentexperiments. B, the percentage of Annexin V-positive cells seenfollowing the treatment with WEE1 inhibitor or TRAIL or thecombination of both as described above. The graph represents themean values � SEM of 3 independent experiments.
MB231
0
10
20
30
40
50
60
WEE1 inhibitorTRAILWEE1 inhibitorDMSO
and TRAIL
% d
ead
cell
s
no ZVAD
with ZVAD
HCC38
0
10
20
30
40
50
60
WEE1 inhibitorTRAILWEE1 inhibitorDMSO
and TRAIL
% d
ead
cell
s
A
B
no ZVAD
with ZVAD
Figure 4. Cell death caused by WEE1 inhibitor and TRAIL treatment iscaspase-dependent. (A) MB231 or (B) HCC38 cells were pretreated withDMSO (black bars) or 100 mmol/L Z-VAD-FMK (ZVAD; white bars) for 1hour followed by WEE1 inhibitor (10 mmol/L) for 4 hours and 100 ng/mLTRAIL for 17 hours or both. Cells were then stained with Trypan blue, andthe number of dead cells was counted in each of the treatments.Combined treatment with WEE1 inhibitor and TRAIL resulted in asignificant increase in the percentage of dead cells inMB231 andHCC38compared with either treatment alone or with the DMSO-treated controlcells (P < 0.0005). Pretreatment with Z-VAD-FMK significantly blockedcell death caused by the dual treatment in MB231 and HCC38(comparison of combined treatment with or without Z-VAD-FMK,P < 0.0005).
Garimella et al.
Mol Cancer Res; 10(1) January 2012 Molecular Cancer Research80
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

WEE1 inhibition results in increased levels of theagonistic TRAIL receptorsThe expression of pro-caspase-8, -9, or -3 did not change
uponWEE1 inhibitor treatment (Fig. 5A). Similarly, expres-
sion of FLIP, BCL-xL, survivin, BCL-2, and MCL-1 pro-teins was measured, but no changes in levels of any of theseproteins were observed (Fig. 7A). We measured the tran-scripts of the death receptors afterWEE1 inhibitor treatmentby real-time PCR. A significant increase in the mRNAlevels of TR1 (4-fold) and TR2 (8-fold) at 24 hours wasobserved, compared with the DMSO controls (Fig. 7B). Nosignificant change in the transcript levels was seen at 8 hoursof WEE1 inhibition. In addition to the transcripts, surfaceexpression of the death receptors was assessed by flowcytometry. A 2-fold increase in the TR2 surface expression(P < 0.05) and a 1.5-fold change in TR1 (P ¼ 0.7) surfaceexpression was observed at 24 hours of WEE1 inhibition(Fig. 7C). Thus,WEE1 inhibition increases TRAIL receptorsurface expression, and this increase is likely to account forthe increased activation of caspase-8 upon the treatment ofcells with the combination of WEE1 inhibitor and TRAIL.
Discussion
TNBC is an aggressive subtype of breast cancer whichdoes not benefit from hormone receptor or anti-HER-2–targeted therapies. Patients with TNBC have a poorprognosis relative to those patients with other breast cancersubtypes (1). TRAIL and its agonists have been shown torapidly induce apoptosis in TNBC cell lines with a mes-enchymal phenotype (designated basal B breast cancercells; refs. 21, 23). We have reported that the inhibitionof WEE1, a tyrosine kinase involved in cell-cycle regula-tion, resulted in caspase-dependent apoptotic cell death inbreast cancer cell lines of all subtypes but not in thenontransformed immortalized MCF10A (12). In contrastto the rapid death induced by TRAIL, the loss of WEE1function induces cell death after 72 hours (12). In thisstudy, we show that pretreatment of breast cancer cellswith a WEE1 inhibitor for 4 hours enhanced TRAIL-mediated cell death by 24 hours and that the effects weremost striking in basal B breast cancer cells (Fig. 1). WEE1inhibitor alone caused little observable death at this earlytime point. WEE1 inhibitor increased cell death causedby TRAIL in sensitive cell lines but did not affect theTRAIL-resistant cells unlike other drugs such as histonedeacetylase (HDAC) inhibitors that sensitized even resis-tant cells to TRAIL (29). In other studies of WEE1inhibition, it has been reported that MK-1775, a WEE1inhibitor, enhances the antitumor efficacy of variousDNA-damaging agents such as 5-fluorouracil, doxorubi-cin, camptothecin, and pemetrexed in colon carcinomacells and gemcitabine in pancreatic cancer (30–32) To ourknowledge, our study is the first to show the effects ofusing the WEE1 inhibitor along with TRAIL in cancercells.In this study, treatment with the combination of WEE1
inhibitor and TRAIL resulted in a significant increase in thecleavage of multiple caspases involved in the death receptorpathway. The combination augmented the activation of 2caspases considered initiators: caspase-8 (of the extrinsicdeath pathway) and caspase-9 (of the intrinsic death
IB: PARP-1
IB: Casp-8
IB: Casp-9
IB: GAPDH
IB: Casp-3
WEE1 inhibitor - + - +
TRAIL - - + +
0
1
2
3
4
5
WEE1 inhibitorTRAILWEE1 inhibitorDMSOand TRAIL
Re
lati
ve
ca
sp
as
e-8
ac
tiv
ity
DMSO
DEVD-CHO
Z-VAD-FMK
0
1
2
3
4
5
WEE1 inhibitorTRAILWEE1 inhibitorDMSOand TRAIL
Rela
tive c
asp
ase-3
an
d -
7 a
cti
vit
y
A
B(i)
(ii)
Caspase-8
Caspase-3/7
DMSO
DEVD-CHO
Z-VAD-FMK
Figure 5. Activation of caspases by treatment with WEE1 inhibitor andTRAIL in MB231 cells. A, activation of caspases was monitored byWestern blot analysis. Lysates of MB231 cells obtained from thetreatments (described above) were analyzed for the decrease in theprecursor form ( ) as seen in caspase-8, -9, -3, and PARP-1 or theappearance of the cleaved form (3) as seen in caspase-8 andPARP-1. B, caspase-8, -3, and -7 activities were measured byCaspase-Glo assay. The cells were pretreated with DMSO or0.3mmol/LofDEVD-CHOor100mmol/LofZ-VAD-FMK for 1hour, followedbyWEE1 inhibitor (10 mmol/L) for 4 hours and then with TRAIL (100 ng/mL)for 2 hours after which the caspase activity was measured. Data representmean values � SEM of 3 independent experiments. GAPDH,glyceraldehyde-3-phosphate dehydrogenase; IB, immunoblotting.
WEE1 Inhibition and TRAIL Toxicity in Breast Cancer Cells
www.aacrjournals.org Mol Cancer Res; 10(1) January 2012 81
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

pathway; Fig. 5A). Addition of a pan-caspase inhibitorabrogated the cell death caused by the WEE1 inhibitor andTRAIL, showing that the synergism is due to an increase incaspase activation (Fig. 5B). RNAi-mediated silencing ofinitiator caspases (caspase-2, -8, -9, and -10) showed thatonly caspase-8 was required for the cell death seen by thecombination of WEE1 inhibition and TRAIL ( Fig. 6). Ourdata suggest that the mechanism by which the WEE1inhibitor sensitizes cells to TRAIL-induced apoptosis is byincreasing caspase-8 activation upon the combined treat-ment. Whether there are other mechanisms that contributeto the enhanced activation of caspase-8 by TRAIL in thepresence of WEE1 inhibitor is not known.Sensitization to TRAIL by chemotherapeutic drugs has
been attributed tomultiplemolecularmechanisms includingthe upregulation of TRAIL receptors (33), activation of themitochondrial pathway (34), or enhanced caspase-8 recruit-ment to the DISC (35). DNA-damaging agents such asdoxorubicin, etoposide, and radiation induce TR2 geneexpression via a p53-dependent mechanism (22, 36, 37).Also, HDAC inhibitors were shown to increase the mRNA
and protein levels of TR2 and proapoptotic BCL-2 familymembers. This increase correlatedwith an increase in caspaseactivity and in apoptosis thereby sensitizing TRAIL-resistantand TRAIL-sensitive breast cancer cells to TRAIL (29). Inthis study, we report an increase in transcripts and cell surfaceexpression of TR1 and TR2 levels upon WEE1 inhibition(Fig. 7). We have shown previously that TR2 activation isimportant in inducingTRAIL-mediated apoptosis inTNBCcell lines such as the MB231 cells (23). Also, Zhang andZhang reported that loss of cellular surface expression of TR1and TR2 accounts for resistance to TRAIL and its agonists(38). The increase in TRAIL receptors in cells treated withWEE1 inhibitor is p53-independent asMB231 cells are p53-deficient (6). Sheikh and colleagues have reported p53-independent upregulation of TR2 by genotoxic stressinduced by methyl methanesulfonate (39). A number ofstudies have found that treatments altering the level or activityof antiapoptotic proteins such asBCL-2,BCL-xL, FLIP,NF-kB, or survivin can alter the sensitivity of cells to TRAIL(40–45). However, we did not observe any change in theirlevels uponWEE1 inhibitor treatment alone orwithTRAIL.
0
20
40
60
80
100
WEE1 inhibitorTRAILWEE1 inhibitorDMSO
and TRAIL
% d
ead
cells
siNEG
siCasp-8
siCasp-2
siCasp-9
0
10
20
30
40
50
60
WEE1 inhibitorTRAILWEE1 inhbitorDMSO
and TRAIL
% d
ead
cells
siNEG
siCasp-8
siCasp-10
siN
EG
siN
EG
siC
asp
-8
siC
asp
-2
IB: Casp
IB: GAPDH
siN
EG
siC
asp
-9
siN
EG
siC
asp
-10
IB: Casp-8
IB: Casp-9
siNEG siCasp-8
IB: GAPDH
WEE1 inhibitor
TRAIL
- + - + - + - +
- - + + - - + +
(i)BA
C
(ii)
Figure 6. Caspase-8 is the initiator caspase of apoptotic cell death. A, the initiator caspases-2, -8, -9, and -10 were knocked down independentlyby synthetic siRNA (50 nmol/L) along with the control siRNA (siNEG) in MB231 cells for 48 hours. The cells were then treated with either 10 mmol/LWEE1 inhibitor for 21 hours or with 100 ng/mL TRAIL for 17 hours or pretreated with WEE1 inhibitor for 4 hours followed by TRAIL for 17 hours.Treated cells were stained with Trypan blue, and the dead cells were counted. B, the decrease in the expression of the 4 caspase protein levels by siRNAwas measured by immunoblotting. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) levels are shown as loading controls. C, activation ofcaspase-9 is dependent on caspase-8 activation. Cells transfected with either control (siNEG) or caspase-8 (siCASP8) siRNAs were treated with WEE1inhibitor, TRAIL, or the combination as described above. Activation of caspase-8 and caspase-9 were measured by disappearance of the precursorforms of the caspases. The pro-caspases are indicated by the arrow and the cleaved forms of caspase-8 are indicated by the arrowhead. IB,immunoblotting.
Garimella et al.
Mol Cancer Res; 10(1) January 2012 Molecular Cancer Research82
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

In our previous work, we have shown that the WEE1inhibitor induces a DNA damage signal as measured byincreased amounts of the phosphorylated form of histoneH2AX (gH2AX) that is observed as early as 4 hours aftertreatment with WEE1 inhibitor (12). The gH2AXinduced by WEE1 inhibition is not blocked by caspaseinhibition (12). Also, TRAIL treatment induces theformation of gH2AX. However, this is blocked by caspaseinhibitors (12). Thus, the mechanism leading to the DNAdamage signal by WEE1 inhibition is independent ofcaspase activation, whereas the induction of gH2AX byTRAIL is downstream of and dependent on caspaseactivation (12). Earlier studies have linked DNA damageto TRAIL-induced apoptosis. Silencing of CHK1 orCHK2 in human prostate cancer cells enhances theirsensitivity to the combination treatment of CPT-11 oraphidicolin and Apo2L/TRAIL (46). This occurs byabrogating the proteolysis of CDC25A (a phosphatase)and thereby enhancing the dephosphorylation ofpTyr15 on CDC2 which induces an S-phase arrest. Thisis similar to our model wherein silencing or inhibition ofthe tyrosine kinase WEE1 results in decreased pTyr15 onCDC2 (Fig. 2) and in the arrest of cells in S-phase (shownearlier in ref. 12). Hence, the enhancement of CDC25Aphosphatase activity or the inhibition of WEE1 would beexpected to phenocopy one another. Both result inS-phase arrest and both sensitize cells to TRAIL-mediatedapoptosis.Another mode of sensitization of cells to TRAIL byDNA-
damaging agents is attributed to both the activation andinhibition of ATM kinase. Upon DNA damage, activatedATM/ATR trigger the activation of their downstream targetsCHK1/CHK2 which, in turn, phosphorylate and activateWEE1 kinase. This leads to G2–M arrest. ATM kinaseactivation in response to DNA damage triggers a series ofevents that leads to the proteolytic degradation of cFLIP, anantiapoptotic protein, and sensitization of hepatic carcinomacells to TRAIL (47). In another model, inhibition of ATMby pharmacologic inhibitors or RNAi followed by radia-tion and TRAIL treatment increased the sensitivity ofmelanoma cells to TRAIL because of the upregulationof surface TR2 levels and downregulation of FLIP levels (48).Inhibition ofWEE1 in our study would be expected to workin a mechanism similar to ATM inhibition. Also, in ouranalysis we found upregulation of TRAIL receptors, but wedid not observe a downregulation of FLIP.Our study and other published data suggest that WEE1
inhibition has selective toxicity in cancer cells comparedwithnormal cells (12, 49). This is due, likely in part, to the factthat cancer cells are deficient in the G1 check point andtherefore rely more on the G2–M checkpoint regulated byWEE1 (10). This is an added advantage in combiningTRAIL with the targeted inhibition of WEE1 as both thedrugs show a relative specificity for killing cancer cells.WEE1 inhibitors and the TRAIL agonists are presentlybeing tested in phase I and II clinical trials (25, 50).Therefore, our data suggest that the combination of WEE1inhibition with TRAIL may be a promising therapy for
WEE1 inhibitor - + - +
TRAIL - - + +
IB: BCL-xL
IB: BCL-2
IB: Survivin
IB: MCL-1
IB: HSC70
IB: FLIP
TRAIL-R2 (DR5) mRNA levels
0
2
4
6
8
10
12
WEE1 inhibitorDMSO
Fo
ld c
ha
ng
e i
n t
ran
sc
rip
t le
ve
ls
8 h
24 h
P < 0.05
P < 0.05
A
C
TRAIL-R1 (DR4) mRNA levels
0
1
2
3
4
5
WEE1 inhibitorDMSO
Fo
ld c
ha
ng
e i
n t
ran
sc
rip
t le
ve
ls
P < 0.005P < 0.005
0
0.5
1
1.5
2
2.5
TRAIL-R2TRAIL-R1
Rela
tive s
urf
ace e
xp
ressio
n
DMSO
WEE1 inhibitor
P < 0.05
P = 0.07
B
8 h
24 h
Figure 7. Expression of death receptors and apoptotic proteins with thecombined treatment of WEE1 inhibitor and TRAIL. A, the levels ofpro-/antiapoptotic proteins were assayed by immunoblotting in MB231cell lysates. The cells were either treated with WEE1 inhibitor (10 mmol/L)for 21 hours or with 100 ng/mL TRAIL for 17 hours or pretreated withWEE1 inhibitor (10 mmol/L) followed by 100 ng/mL of TRAIL for 17 hours.B, transcript levels of TR1 and TR2weremeasured by real-time PCRafter8 (white bars) or 24 hours (black bars) of WEE1 inhibitor (10 mmol/L)treatment. The results represent the average of 3 experiments � SEM.ThemRNAexpression ofWEE1 inhibitor treated cells was comparedwiththe other samples as indicated. C, surface expression of TR1 and TR2was measured after 24 hours of WEE1 inhibition by flow cytometry.Surface levels of the receptors after WEE1 inhibition (black bars) werecompared with the DMSO controls (white bars). IB, immunoblotting.
WEE1 Inhibition and TRAIL Toxicity in Breast Cancer Cells
www.aacrjournals.org Mol Cancer Res; 10(1) January 2012 83
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

TNBC/basal breast cancer in the clinic and well worthfurther exploration.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Acknowledgments
The authors thank Marion Nau for critical reading of the manuscript.
Grant Support
This research was supported by the Intramural Research Program of the NationalCancer Institute, Center for Cancer Research, NIH.
The costs of publication of this article were defrayed in part by the payment of pagecharges. This article must therefore be herebymarked advertisement in accordance with18 U.S.C. Section 1734 solely to indicate this fact.
Received October 14, 2011; accepted November 9, 2011; published OnlineFirstNovember 23, 2011.
References1. Brenton JD, Carey LA, Ahmed AA, Caldas C. Molecular classification
and molecular forecasting of breast cancer: ready for clinicalapplication? J Clin Oncol 2005;23:7350–60.
2. Irvin WJ Jr, Carey LA. What is triple-negative breast cancer? Eur JCancer 2008;44:2799–805.
3. Sørlie T, Perou CM, Tibshirani R, Aas T, Geisler S, Johnsen H, et al.Gene expression patterns of breast carcinomas distinguish tumorsubclasses with clinical implications. Proc Natl Acad Sci U S A2001;98:10869–74.
4. Bertucci F, Finetti P, Cervera N, Esterni B, Hermitte F, Viens P, et al.How basal are triple-negative breast cancers? Int J Cancer 2008;123:236–40.
5. Charafe-Jauffret E, Ginestier C, Monville F, Finetti P, Ad�elaïde J,Cervera N, et al. Gene expression profiling of breast cell lines identifiespotential new basal markers. Oncogene 2006;25:2273–84.
6. Neve RM, Chin K, Fridlyand J, Yeh J, Baehner FL, Fevr T, et al. Acollectionof breast cancer cell lines for the studyof functionally distinctcancer subtypes. Cancer Cell 2006;10:515–27.
7. FoulkesWD, Stefansson IM, Chappuis PO, B�egin LR, Goffin JR,WongN, et al. GermlineBRCA1mutations and abasal epithelial phenotype inbreast cancer. J Natl Cancer Inst 2003;95:1482–5.
8. Turner N, Tutt A, Ashworth A. Hallmarks of `BRCAness' in sporadiccancers. Nat Rev Cancer 2004;4:814–9.
9. McGowan CH, Russell P. Human Wee1 kinase inhibits cell division byphosphorylating p34cdc2 exclusively on Tyr15. EMBO J 1993;12:75–85.
10. O'Connell MJ, Raleigh JM, Verkade HM, Nurse P. Chk1 is a wee1kinase in the G2 DNA damage checkpoint inhibiting cdc2 by Y15phosphorylation. EMBO J 1997;16:545–54.
11. Kawabe T. G2 checkpoint abrogators as anticancer drugs.Mol CancerTher 2004;3:513–9.
12. Murrow LM, Garimella SV, Jones TL, Caplen NJ, Lipkowitz S. Iden-tification of WEE1 as a potential molecular target in cancer cells byRNAi screening of the human tyrosine kinome. Breast Cancer ResTreat 2010;122:347–57.
13. Ashkenazi A, Pai RC, Fong S, Leung S, Lawrence DA, Marsters SA,et al. Safety and antitumor activity of recombinant soluble Apo2 ligand.J Clin Invest 1999;104:155–62.
14. Walczak H, Miller RE, Ariail K, Gliniak B, Griffith TS, Kubin M, et al.Tumoricidal activity of tumor necrosis factor-related apoptosis-induc-ing ligand in vivo. Nat Med 1999;5:157–63.
15. Pitti RM,Marsters SA, Ruppert S, Donahue CJ, Moore A, Ashkenazi A.Induction of apoptosis by Apo-2 ligand, a new member of the tumornecrosis factor cytokine family. J Biol Chem 1996;271:12687–90.
16. Ashkenazi A. Targeting death and decoy receptors of the tumour-necrosis factor superfamily. Nat Rev Cancer 2002;2:420–30.
17. Riedl SJ, Shi Y. Molecular mechanisms of caspase regulation duringapoptosis. Nat Rev Mol Cell Biol 2004;5:897–907.
18. Herbst RS, Bajorin DF, Bleiberg H, Blum D, Hao D, Johnson BE, et al.Clinical Cancer Advances 2005: major research advances in cancertreatment, prevention, and screening–a report from the AmericanSociety of Clinical Oncology. J Clin Oncol 2006;24:190–205.
19. Keane MM, Ettenberg SA, Nau MM, Russell EK, Lipkowitz S. Chemo-therapy augments TRAIL-induced apoptosis in breast cell lines. Can-cer Res 1999;59:734–41.
20. Singh TR, Shankar S, Chen X, Asim M, Srivastava RK. Synergisticinteractions of chemotherapeutic drugs and tumor necrosis factor-related apoptosis-inducing ligand/Apo-2 ligand on apoptosis andon regression of breast carcinoma in vivo. Cancer Res 2003;63:5390–400.
21. Buchsbaum DJ, Zhou T, Grizzle WE, Oliver PG, Hammond CJ,Zhang S, et al. Antitumor efficacy of TRA-8 anti-DR5 monoclonalantibody alone or in combination with chemotherapy and/or radi-ation therapy in a human breast cancer model. Clin Cancer Res2003;9:3731–41.
22. Chinnaiyan AM, Prasad U, Shankar S, Hamstra DA, Shanaiah M,Chenevert TL, et al. Combined effect of tumor necrosis factor-relatedapoptosis-inducing ligand and ionizing radiation in breast cancertherapy. Proc Natl Acad Sci U S A 2000;97:1754–9.
23. Rahman M, Davis SR, Pumphrey JG, Bao J, Nau MM, Meltzer PS,et al. TRAIL induces apoptosis in triple-negative breast cancer cellswith a mesenchymal phenotype. Breast Cancer Res Treat 2009;113:217–30.
24. RahmanM, Pumphrey JG, Lipkowitz S. The TRAIL to targeted therapyof breast cancer. Adv Cancer Res 2009;103:43–73.
25. AmmHM,Oliver PG, LeeCH, Li Y,BuchsbaumDJ.Combinedmodalitytherapywith TRAIL or agonistic death receptor antibodies. Cancer BiolTher 2011;11:431–49.
26. Palmer BD, Thompson AM, Booth RJ, Dobrusin EM, Kraker AJ, LeeHH, et al. 4-Phenylpyrrolo[3,4-c]carbazole-1,3(2H,6H)-dione inhibitorsof the checkpoint kinase Wee1. Structure-activity relationships forchromophore modification and phenyl ring substitution. J Med Chem2006;49:4896–911.
27. Cohen GM. Caspases: the executioners of apoptosis. Biochem J1997;326:1–16.
28. Wieder T, Essmann F, Prokop A, Schmelz K, Schulze-Osthoff K,Beyaert R, et al. Activation of caspase-8 in drug-induced apoptosisof B-lymphoid cells is independent of CD95/Fas receptor-ligandinteraction and occurs downstream of caspase-3. Blood 2001;97:1378–87.
29. Singh TR, Shankar S, Srivastava RK. HDAC inhibitors enhance theapoptosis-inducing potential of TRAIL in breast carcinoma. Oncogene2005;24:4609–23.
30. Hirai H, Arai T, OkadaM, Nishibata T, Kobayashi M, Sakai N, et al. MK-1775, a smallmoleculeWee1 inhibitor, enhances anti-tumor efficacy ofvarious DNA-damaging agents, including 5-fluorouracil. Cancer BiolTher 2010;9:514–22.
31. De Witt Hamer PC, Mir SE, Noske D, Van Noorden CJ, Wurdinger T.WEE1 kinase targeting combined with DNA-damaging cancer therapycatalyzes mitotic catastrophe. Clin Cancer Res 2011;17:4200–7.
32. Rajeshkumar NV, De Oliveira E, Ottenhof N, Watters J, Brooks D,Demuth T, et al. MK-1775, a potent Wee1 inhibitor, synergizes withgemcitabine to achieve tumor regressions, selectively in p53-defi-cient pancreatic cancer xenografts. Clin Cancer Res 2011;17:2799–806.
33. Nagane M, Pan G, Weddle JJ, Dixit VM, Cavenee WK, Huang HJ.Increased death receptor 5 expression by chemotherapeutic agents inhuman gliomas causes synergistic cytotoxicity with tumor necrosisfactor-related apoptosis-inducing ligand in vitro and in vivo. CancerRes 2000;60:847–53.
Garimella et al.
Mol Cancer Res; 10(1) January 2012 Molecular Cancer Research84
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

34. NguyenDM,YeowWS, ZiauddinMF,BarasA, TsaiW,ReddyRM, et al.The essential role of the mitochondria-dependent death-signalingcascade in chemotherapy-induced potentiation of Apo2L/TRAIL cyto-toxicity in cultured thoracic cancer cells: amplified caspase 8 isindispensable for combination-mediated massive cell death. CancerJ 2006;12:257–73.
35. Ganten TM, Haas TL, Sykora J, Stahl H, Sprick MR, Fas SC, et al.Enhanced caspase-8 recruitment to and activation at the DISC iscritical for sensitisation of human hepatocellular carcinoma cells toTRAIL-induced apoptosis by chemotherapeutic drugs. Cell DeathDiffer 2004;11 Suppl 1:S86–96.
36. Shankar S, Singh TR, Chen X, Thakkar H, Firnin J, Srivastava RK. Thesequential treatment with ionizing radiation followed by TRAIL/Apo-2Lreduces tumor growth and induces apoptosis of breast tumor xeno-grafts in nude mice. Int J Oncol 2004;24:1133–40.
37. Wu GS, Burns TF, McDonald ER, Jiang W, Meng R, Krantz ID, et al.KILLER/DR5 is a DNA damage-inducible p53-regulated death recep-tor gene. Nat Genet 1997;17:141–3.
38. Zhang Y, Zhang B. TRAIL resistance of breast cancer cells is asso-ciated with constitutive endocytosis of death receptors 4 and 5. MolCancer Res 2008;6:1861–71.
39. SheikhMS, Burns TF, HuangY,WuGS, AmundsonS, Brooks KS, et al.p53-dependent and -independent regulation of the death receptorKILLER/DR5 gene expression in response to genotoxic stress andtumor necrosis factor alpha. Cancer Res 1998;58:1593–8.
40. Fulda S, Debatin KM. Modulation of TRAIL signaling for cancer ther-apy. Vitam Horm 2004;67:275–90.
41. Fulda S, Meyer E, Debatin KM. Inhibition of TRAIL-induced apoptosisby Bcl-2 overexpression. Oncogene 2002;21:2283–94.
42. Guseva NV, Rokhlin OW, Taghiyev AF, Cohen MB. Unique resis-tance of breast carcinoma cell line T47D to TRAIL but not anti-Fas
is linked to p43cFLIP(L). Breast Cancer Res Treat 2008;107:349–57.
43. Keane MM, Rubinstein Y, Cuello M, Ettenberg SA, Banerjee P, NauMM, et al. Inhibition of NF-kappaB activity enhances TRAIL mediatedapoptosis in breast cancer cell lines. Breast Cancer Res Treat 2000;64:211–9.
44. Kim IK, Jung YK, Noh DY, Song YS, Choi CH, Oh BH, et al.Functional screening of genes suppressing TRAIL-induced apopto-sis: distinct inhibitory activities of Bcl-XL and Bcl-2. Br J Cancer2003;88:910–7.
45. Palacios C, Yerbes R, Lopez-Rivas A. Flavopiridol induces cellularFLICE-inhibitory protein degradation by theproteasomeandpromotesTRAIL-induced early signaling and apoptosis in breast tumor cells.Cancer Res 2006;66:8858–69.
46. RayS,ShyamS, FraizerGC,AlmasanA.S-phase checkpoints regulateApo2 ligand/TRAIL and CPT-11-induced apoptosis of prostate cancercells. Mol Cancer Ther 2007;6:1368–78.
47. Stagni V, Mingardi M, Santini S, Giaccari D, Barila D. ATM kinaseactivity modulates cFLIP protein levels: potential interplay betweenDNA damage signalling and TRAIL-induced apoptosis. Carcinogen-esis 2010;31:1956–63.
48. Ivanov VN, Zhou H, Partridge MA, Hei TK. Inhibition of ataxiatelangiectasia mutated kinase activity enhances TRAIL-mediatedapoptosis in human melanoma cells. Cancer Res 2009;69:3510–9.
49. Hashimoto O, Shinkawa M, Torimura T, Nakamura T, Selvendiran K,Sakamoto M, et al. Cell cycle regulation by the Wee1 inhibitorPD0166285, pyrido [2,3-d] pyimidine, in the B16 mouse melanomacell line. BMC Cancer 2006;6:292.
50. Stathis A, Oza A. Targeting Wee1-like protein kinase to treat cancer.Drug News Perspect 2010;23:425–9.
WEE1 Inhibition and TRAIL Toxicity in Breast Cancer Cells
www.aacrjournals.org Mol Cancer Res; 10(1) January 2012 85
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500

2012;10:75-85. Published OnlineFirst November 23, 2011.Mol Cancer Res Sireesha V. Garimella, Andrea Rocca and Stanley Lipkowitz TRAIL-Induced ApoptosisWEE1 Inhibition Sensitizes Basal Breast Cancer Cells to
Updated version
10.1158/1541-7786.MCR-11-0500doi:
Access the most recent version of this article at:
Cited articles
http://mcr.aacrjournals.org/content/10/1/75.full#ref-list-1
This article cites 50 articles, 20 of which you can access for free at:
Citing articles
http://mcr.aacrjournals.org/content/10/1/75.full#related-urls
This article has been cited by 2 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mcr.aacrjournals.org/content/10/1/75To request permission to re-use all or part of this article, use this link
on January 23, 2019. © 2012 American Association for Cancer Research. mcr.aacrjournals.org Downloaded from
Published OnlineFirst November 23, 2011; DOI: 10.1158/1541-7786.MCR-11-0500