
Treatment of Habit and Tic Disorders Rachel Valleley, Ph.D. Munroe-Meyer Institute.
53
Treatment of Habit and Tic Disorders Rachel Valleley, Ph.D. Munroe-Meyer Institute
-
Upload
martha-mathews -
Category
Documents
-
view
223 -
download
1
Transcript of Treatment of Habit and Tic Disorders Rachel Valleley, Ph.D. Munroe-Meyer Institute.

Treatment of Habit and Tic Disorders
Rachel Valleley, Ph.D.Munroe-Meyer Institute

Overview
Habits vs. Tics DSM Criteria Assessment Treatment options:
Medication Habit Reversal
Case Example

Habits
“frequent, repetitive behaviors that cannot be explained by physiological causes and appear to serve no identifiable physiological function”
Examples: nail biting, nail picking, trichotillomania, thumb sucking, hair twirling
Tics
“sudden, brief, involuntary, rapid, nonrhythmic, repetitive movements or utterances that are purposeless and stereotypic”
Examples: eye blinking, facial grimacing, shoulder shrugging, throat clearing, coughing, growling, sniffing

DSM Diagnoses
Habits: Stereotypic Movement Disorder Trichotillomania
Tics: Transient tic disorder Chronic motor or vocal tic disorder Tourette’s disorder

Habits
Stereotypic Movement Disorder Trichotillomania

Stereotypic Movement Disorder
Repetitive, seemingly driven, & nonfunctional motor behavior
Interferes with normal activities or results in self-inflicted bodily injury
Not accounted for by other disorders (e.g., OCD, tics, trichotillomania)
Not due to substance or general medical condition
Lasts longer than 4 weeks

Trichotillomania
Recurrent pulling out of one’s hair, resulting in noticeable hair loss
Sense of tension immediately before pulling out the hair or resisting the behavior
Pleasure, gratification, or relief when pulling out hair
Not better accounted for by other disorder or medical condition
Causes clinically significant distress or impairment

Demographics of Trichotillomania
Prevalence: 0.6% Non-clinical hair pulling (10-13%)
Age of Onset: 13.1 yrs More frequent in females Onset if often precipitated by
stressful life event (e.g., divorce, loss, academic pressures)

Scalp (80.6%)

Brow (43.5%)
Lash (47.3%)
Hair Pulling Episodes
Touching, manipulating region before pull Can range from brief sessions with only a
few hairs lost to sessions lasting several hours with hundreds of hairs pulled
Occurs in solitude but children do in front of family
Increased pulling during periods of stress, relaxation, or distraction
May be unaware they are pulling their hair and thus do not experience tension or relief

More often use dominant hand for pulling
Consequences of Hair Pulling
Post pull: play with hair Result in total absence of hair, bald
spots, or thinning of hair Most serious consequence occurs
when patients eat the hair and form hairballs in the stomach. Results in all kinds of complications like anemia, loss of appetite, nausea, vomiting

Comorbid Conditions
Most Common Anxiety Mood disorders
OCD: Some speculation that it is related to OCD

Tic Disorders
Transient tic disorder Chronic motor or vocal tic disorder Tourette’s disorder

Transient tic disorder
Single or multiple motor &/or vocal tics Occur many times a day, nearly every day
for at least 4 weeks but not longer than 12 consecutive months
Causes marked distress or impairment Onset prior to 18 Not due to substance/medical condition Do not meet criteria for other tic disorder
Chronic motor or vocal tic disorder
Single or multiple motor OR vocal tics but not both
Occur many times a day, nearly every day or intermittently for over 1 year, no more than 3 consecutive months tic free
Causes marked distress or impairment Onset prior to 18 Not due to substance or medical condition Do not meet criteria for Tourette’s
Tourette’s disorder
Both multiple motor & one or more vocal tics have been present but do not have to be at same time
Occur many times a day (usually in bouts), nearly every day or intermittently for over 1 year, no more than 3 consecutive months tic free
Causes marked distress or impairment Onset prior to 18 Not due to substance or medical condition

Impairment from Habit or Tic
Common impairments/distress Physical Social

What causes or maintains habits/tics?
Physical Trauma Automatic reinforcement
Positive Negative
Social reinforcement Very limited data on functional
analysis of habits and tics

Mechanisms involved in Trichotillomania
Negative reinforcement Tension Arousal reduction Negative affective states
Automatic reinforcement Sedentary (watching TV, getting ready
for bed) Contemplative (homework, reading)

Assessment Considerations
Rule out medical problem Comorbid condition or habit? Distress or impairment? Observation Self-monitoring Permanent products High probability situations Ratings scales available

Empirically Supported Treatments
Medication Haldol Pimozide Clonidine Anafranil & Prozac for Trichotillomania
Behavioral Procedures Habit Reversal

Medication
Haldol: Tourette’s Relieves symptoms up to 70-80% of
patients. Short term side effects Long Term side effects
Pimozide Clonidine

Behavioral Procedures
Massed negative practice Punishment Reinforcement Relaxation Training Function-Based Treatments Habit Reversal

Massed negative practice
Requires the individual to perform each tic accurately & effortfully for a specified amount of time

Punishment
Time out Trichotillomania
Topical creams Sensory Extinction: e.g., gloves Increasing effort: e.g., wrist weights

Reinforcement
Differential reinforcement of other behaviors or differential reinforcement of alternative behaviors

Relaxation Training
Reducing tension before the occurrence of tics
No data to support as sole treatment for tics

Function-Based Treatments
Determining the function of the tic to tailor treatment. Is the tic occurring to escape something
aversive or due to social attention provided, or is it occurring due to the sensory
stimulation provided?

“Complete Habit Reversal”
Originally developed by Arin & Nunn (1973)
Consisted of 10-13 steps components Simplified Habit Reversal: only 4
components necessary 90-100% reduction of tics that
maintained over 12 months Has been found effective for many types
of habits and tics

Simplified Habit Reversal
Awareness Training Competing Response Training Relaxation Training (optional) Social Support
Awareness Training
Increase awareness of when habit is occurring by:
Practice habit/tic in front of mirror Focus on how muscles/body feels while
engaging in habit Have child identify times when habit
occurs Prompt child when habit occurred Keep data on habit occurrence

Competing Response Training
Teach an incompatible behavior for when habit occurs
Select competing response Practice competing response in front of
mirror Use competing response when urge for
habit occurs Use competing response in situations
when habit is likely to occur After habit occurs, practice competing
response for one minute

Relaxation Training (optional)
Reduce stress or anxiety if related to habit
Practice daily Options
Progressive muscle relaxation Visual imagery Breathing exercises
Social support
Parents provide feedback and encourage child to use habit reversal procedure
Provide feedback to child to become aware of habit occurrence
Encourage competing response Add reinforcement procedure if
necessary

Reinforcement
Parents could reinforce: Awareness training practices Use of the competing response Habit free periods of time

Case Example
11 year-old, 5th grade Caucasian male Tourette’s Disorder Special Education for LD in Written
Expression Motor Habit: Tensing face, pulling
arms up, anticipation antecedent Vocal Habit: ‘ah’ added between
words, occurred both in conversation & oral reading
Assessment of Motor Tic
Interview of parent and child Description of tic, duration, frequency Situations more likely to do it in Awareness? Parent response
Parent, Teacher Observation Videotape at home
Treatment of Motor Tic
Habit Reversal Awareness
Watching videotape of self in session Incompatible behavior Social Support
Reinforcement for practices

Assessment of Vocal Habit
Assessment involved: Determining instructional reading level
(5th grade, 91-106 WPM & 95% Comprehension)
Determining base rate of vocal habit while reading (28-29 VHM)
Sampling conversation (13 VHM) Conducting a Brief Reading
Experimental Analysis

Brief Experimental Reading Analysis
Baseline conditions alternated with treatment conditions Repeated Reading Listening Passage Previewing Word Error Correction Reinforcement Phrase Error Correction

Brief Experimental Reading Analysis
0
5
10
15
20
25
30
35
40B
asel
ine R
R
Bas
elin
e RR
LPP
WEC
Bas
elin
e
WEC
Rei
nfor
cem
ent PE
C
Bas
elin
e
PEC
Hab
ist P
er M
inut
e

Intervention
Phrase error correction chosen as intervention
Mother trained Home reading practices (10-20 minutes of
preferred reading & one minute generalization probe) conducted over 2 months
Reading sessions recorded for reliability & treatment integrity
Tokens earned for participation

Results: Pre Integrity Feedback
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10
Home Reading Sessions
Hab
its P
er M
inut
e
In Session Probe
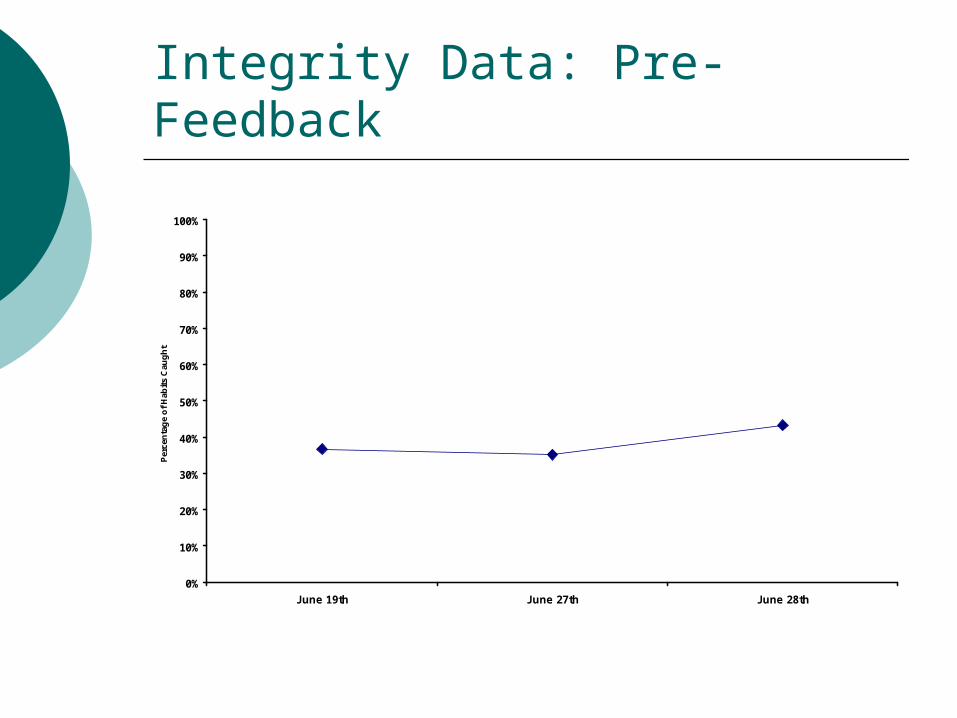
Integrity Data: Pre-Feedback
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
June 19th June 27th June 28th
Per
cen
tag
e o
f H
abit
s C
aug
ht

Results
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25
Home Reading Sessions
Hab
its
Per
Min
ute
In Session Follow up
Home Reading Generalization Probes: Pre Integrity Check
Home Reading Generalization Probes After In Session Integrity Check
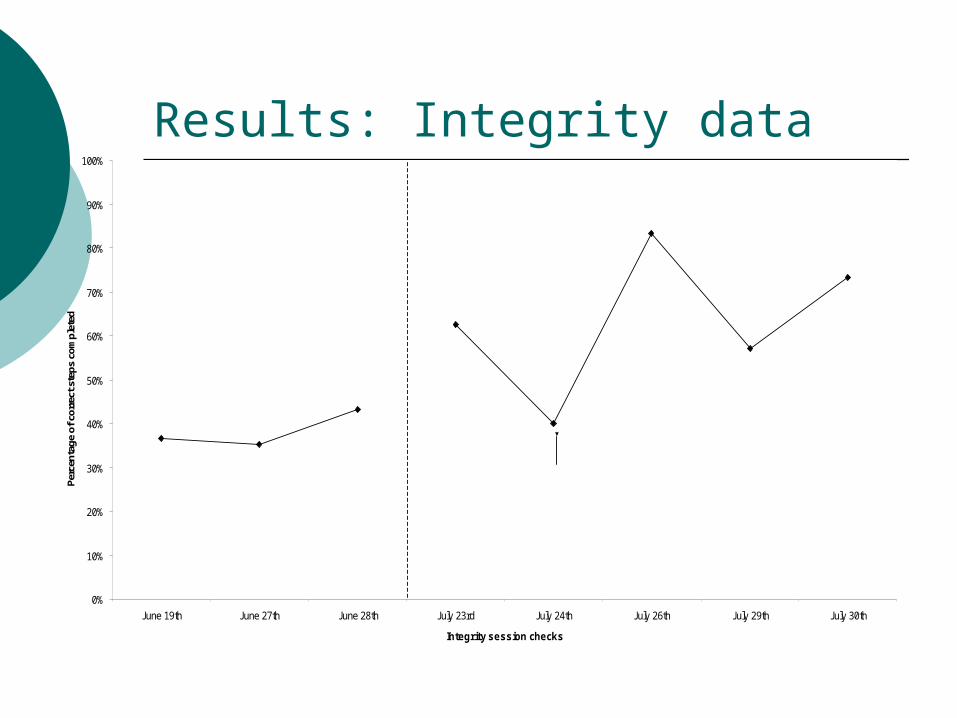
Results: Integrity data
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
June 19th June 27th June 28th July 23rd July 24th July 26th July 29th July 30th
Integrity session checks
Perc
enta
ge o
f cor
rect
ste
ps c
ompl
eted
Pre feedback Post feedback
signif icantly few er habits in session (5)

Results
Decreased rate of oral habit from 28 per minute to 0-1 per minute while reading
Did not impact reading fluency (109 WPM at two month follow up)
Generalized to conversation speech (13 to 1 per minute)

Discussion
Vocal habit conceptualized as dysfluency PEC intervention resembles awareness
training and practice of competing response
Important to collect treatment integrity data
Parents can be trained to conduct these types of interventions & collect data for reliability & treatment integrity

References
Christopherson, E. R., & Mortweet, S. L. (2001). Treatments that work with children: Empirically supported strategies for managing childhood problems. Washington, DC: American Psychological Association
Glaros, A. G., & Epkins, C. C. (1995). Habit Disorders: Bruxism, Trichotillomania, and Tics. In M.C Roberts (Ed.), Handbook of Pediatric Psychology (2nd ed., pp.558-574). New York: The Guilford Press.
Miltenberger, R. G., Fuqua, R. W., & Woods, D. W. (1998). Applying behavior analysis to clinical problems: Review and analysis of habit reversal. JABA, 31, 447-469.

References
Valleley, R. J., Shriver, M. D., & Rozema, S. (2005). Using brief experimental assessment of reading interventions for identification and treatment of a vocal habit. Journal of Applied Behavior Analysis, 38, 129-133
Woods D. W., Miltenberger, R. G. (2001). Tic Disorders, Trichotillomania, and othr repetitive behavior disorders. Norwell, MA: Kluwer Academic Publishers


















