Traumatic Brain Injury
103
Traumat Traumat ic ic Brain Brain Injury Injury
description
Traumatic Brain Injury. The effects of trauma to the skull and brain, during closed head injury depend upon a number of factors: (a) the shape of the objects causing the trauma, (b) the force of the impact, (c) whether the head is in motion at the time of impact. - PowerPoint PPT Presentation
Transcript of Traumatic Brain Injury

Traumatic Traumatic Brain Brain InjuryInjury

The effects of trauma to the skull and brain, The effects of trauma to the skull and brain, during closed head injury depend upon a during closed head injury depend upon a number of factors: number of factors:
(a)(a) the shape of the objects causing the the shape of the objects causing the trauma,trauma,
(b)(b) the force of the impact, the force of the impact,
(c)(c) whether the head is in motion at the time whether the head is in motion at the time of impact.of impact.

Traumatic brain injury (TBI)
An external mechanical force,An external mechanical force, possibly leading to permanent or possibly leading to permanent or
temporary impairments of temporary impairments of :: cognitive, cognitive, physical, physical, psychosocial functions psychosocial functions with an associated diminished or with an associated diminished or
altered state of consciousnesaltered state of consciousness.s.

Young people Young people Low-income individuals Low-income individuals Unmarried individuals Unmarried individuals Men (2:1 vs. women)Men (2:1 vs. women) Individuals with previous history of substance Individuals with previous history of substance
abuse abuse Individuals with previous TBIIndividuals with previous TBI
High Risk PopulationsHigh Risk Populations

Brain injury results from:Brain injury results from:
Direct injury to brain tissueDirect injury to brain tissue
External forces applied to External forces applied to outside of skull transmitted to outside of skull transmitted to the brainthe brain
Movement of brain inside skullMovement of brain inside skull
Traumatic Brain Injury (TBI)Traumatic Brain Injury (TBI)

Thus the Thus the mechanismsmechanisms of closed head injury of closed head injury are either due to are either due to contactcontact phenomena (usually resulting in focal phenomena (usually resulting in focal
lesions) or lesions) or acceleration/decelerationacceleration/deceleration phenomena phenomena
(principally causing diffuse axonal injury (principally causing diffuse axonal injury (DAI).(DAI).
It is important to realize that severe brain It is important to realize that severe brain damage can occur in the damage can occur in the absence of easilyabsence of easily visible external injuryvisible external injury and vice versa, and and vice versa, and that focal and diffuse lesions may occur in that focal and diffuse lesions may occur in isolation or be combined.isolation or be combined.

HEAD INJURIES / BRAIN INJURIESHEAD INJURIES / BRAIN INJURIESHEAD INJURIES / BRAIN INJURIESHEAD INJURIES / BRAIN INJURIES
CONCUSSIONCONCUSSION
DIFFUSE AXONAL INJURYDIFFUSE AXONAL INJURY
EEPIDURALPIDURAL
SUBDURALSUBDURAL
SUBARACHNOIDSUBARACHNOID
PARENCHYMALPARENCHYMAL
COUP/CONTRE COUPCOUP/CONTRE COUP
FOCAL/MULTIFOCALFOCAL/MULTIFOCAL
INTRAVENTRICULARINTRAVENTRICULAR

CONTACT PHENOMENA &/OR ACC/DEC CONTACT PHENOMENA &/OR ACC/DEC INJURYINJURY
PRIMARY PRIMARY DAMAGEDAMAGE
FOCALFOCAL DIFFUSEDIFFUSE
FRACTURESFRACTURES
CONTUSIONSCONTUSIONS
LACERATIONSLACERATIONS
HEMORRHAGESHEMORRHAGES
DIFFUSE AXONAL DIFFUSE AXONAL INJURYINJURY
(DIFFUSE BRAIN INJURY)(DIFFUSE BRAIN INJURY)
EPIDURALEPIDURAL
SUBDURALSUBDURAL
SUBARACHNOIDSUBARACHNOID
PARENCHYMALPARENCHYMAL
COUP/CONTRE COUPCOUP/CONTRE COUP
FOCAL/MULTIFOCALFOCAL/MULTIFOCAL
INTRAVENTRICULARINTRAVENTRICULAR
HEMATOMASHEMATOMAS

Concussion is caused by Concussion is caused by deformity of the deep deformity of the deep structures of the brainstructures of the brain, leading to widespread , leading to widespread neurologic dysfunctionneurologic dysfunction that can result in that can result in impaired consciousnessimpaired consciousness or or comacoma..
Concussion is considered a mild form of Concussion is considered a mild form of diffuse axonal injurydiffuse axonal injury..
ConcussionConcussion

DIFFUSE AXONAL INJURY (DAI)DIFFUSE AXONAL INJURY (DAI)

Diffuse axonal injuryDiffuse axonal injury
- Diffuse axonal injury is characterized by Diffuse axonal injury is characterized by extensive generalized damage to the white extensive generalized damage to the white matter of the brainmatter of the brain..
- Strains during high-speed Strains during high-speed acceleration/deceleration produced in lateral acceleration/deceleration produced in lateral motions of the head may cause the injuriesmotions of the head may cause the injuries..
- Diffuse axonal injury also could occur as a Diffuse axonal injury also could occur as a result of ischemiaresult of ischemia..

Diffuse axonal injuryDiffuse axonal injury, in its mildest form , in its mildest form is probably responsible for concussion, but is probably responsible for concussion, but if severe is associated with if severe is associated with prolonged prolonged unconsciousness from the moment of unconsciousness from the moment of injuryinjury. .
The mechanism is one of The mechanism is one of widespread widespread tearing of axonstearing of axons due to shearing forces due to shearing forces during during acceleration/deceleration acceleration/deceleration of brain. of brain.
While focal injuries such as contusions, While focal injuries such as contusions, lacerations and intracranial hematomas, are lacerations and intracranial hematomas, are usually readily apparent radiologically, DAI usually readily apparent radiologically, DAI is more subtle. is more subtle.

CONSCIOUSNESS DISTURBANCECONSCIOUSNESS DISTURBANCEIN DIFFUSE BRAIN INJURYIN DIFFUSE BRAIN INJURY
Mild concussion : LOC - transient
Cerebral concussion : LOC <6hrs
Mild DAI : LOC 6-24 hrs
Moderate DAI : >24 hrs
Severe DAI : days-weeks
LOC:Loss of ConsciousnessDAI: Diffuse axonal injury

PATHOMORPHOLOGY OF DAIPATHOMORPHOLOGY OF DAI
•Corpus callosum & brainstem most commonly affected
•Spheroids appear when coma exceeds 6 hrs
•Only detectable at LM level after 24 hours
•Evanescent - days to weeks
INVISIBLE ON CT/MR SCAN

Morphology of DAI
Axonal spheroids

-Epidural HematomaEpidural Hematoma-Subdural HematomaSubdural Hematoma
A.A. Dural associated Dural associated hematomashematomas

Epidural HematomaEpidural Hematoma
Normally the dura is fused with the Normally the dura is fused with the periosteum on the internal surface of the periosteum on the internal surface of the skull. Dural arteries, most importantly the skull. Dural arteries, most importantly the middle meningeal artery, are vulnerable to middle meningeal artery, are vulnerable to injury, particularly with temporal skull injury, particularly with temporal skull fractures in which the fracture lines cross fractures in which the fracture lines cross the course of the vessel. In children, in the course of the vessel. In children, in whom the skull is deformable, a temporary whom the skull is deformable, a temporary displacement of the skull bones leading to displacement of the skull bones leading to laceration of a vessel can occur in the laceration of a vessel can occur in the absence of a skull fracture. absence of a skull fracture.

Epidural HematomaEpidural Hematoma
The extravasation of blood under arterial pressure can The extravasation of blood under arterial pressure can cause the dura to separate from the inner surface of cause the dura to separate from the inner surface of the skull .the skull .
The expanding hematoma has a smooth inner The expanding hematoma has a smooth inner contour that compresses the brain surface. contour that compresses the brain surface.
When blood accumulates slowly patients may be When blood accumulates slowly patients may be lucid for several hours before the onset of neurologic lucid for several hours before the onset of neurologic signs. signs.
An epidural hematoma may expand rapidly and is a An epidural hematoma may expand rapidly and is a neurosurgical emergency requiring prompt drainage.neurosurgical emergency requiring prompt drainage.

Epidural HematomaEpidural Hematoma
More often, a tear in the More often, a tear in the middle meningeal middle meningeal arteryartery causes this type of hematoma. causes this type of hematoma. When hematoma occurs from laceration of an When hematoma occurs from laceration of an
artery, blood collection can cause rapid artery, blood collection can cause rapid neurologic deteriorationneurologic deterioration..



Two-thirds of epidural hematomas are in Two-thirds of epidural hematomas are in the the temporo-parietal regiontemporo-parietal region and they and they usually have a biconvex or lentiform usually have a biconvex or lentiform configuration. configuration.
Epidurals are limited by the firmer Epidurals are limited by the firmer attachment of the dura at the suture attachment of the dura at the suture margins, but they may cross the midline.margins, but they may cross the midline.

Epidural hematomaEpidural hematoma


Subdural hematomaSubdural hematoma
Subdural hematoma tends to occur in patients Subdural hematoma tends to occur in patients with injuries to the with injuries to the dural (dural (corticalcortical)) veins or pial veins or pial arteryartery in severe TBI in severe TBI..
The associated mortality rate is high, The associated mortality rate is high, approximately 60-80%.approximately 60-80%.
They occur most frequently over the They occur most frequently over the convexitiesconvexities, covering the entire hemisphere , covering the entire hemisphere and are manifested clinically by fluctuating and are manifested clinically by fluctuating levels of consciousnesslevels of consciousness. .



Subdural hematomas, both acute and chronic, Subdural hematomas, both acute and chronic, are most often caused by bleeding from are most often caused by bleeding from torn torn bridging dural veinsbridging dural veins. .
Subdural hematomas are less frequently Subdural hematomas are less frequently associated with skull fractures, but more associated with skull fractures, but more frequently associated with frequently associated with parenchymal brain parenchymal brain damage. damage.
The subdural space is a more freely The subdural space is a more freely communicating space and the hematomas form communicating space and the hematomas form a crescentic shaped layer over the brain a crescentic shaped layer over the brain surface. surface.

Instead, they extend along the dura of the falx Instead, they extend along the dura of the falx into the interhemispheric fissure and onto the into the interhemispheric fissure and onto the tentorium, which epidurals cannot do. tentorium, which epidurals cannot do.
Both epidural and subdural hemorrhages Both epidural and subdural hemorrhages occur within the confined space of the bony occur within the confined space of the bony calvarium and calvarium and compress the adjacent braincompress the adjacent brain, , often requiring emergency evacuation.often requiring emergency evacuation.

In alcoholic or elderly patientsIn alcoholic or elderly patients with cerebral with cerebral atrophy, atrophy, SDH'sSDH's are often bilateral are often bilateral and may and may occur after insignificant or even unnoticed occur after insignificant or even unnoticed trauma. trauma.

bridging veins are more susceptible to tearing when there is cortical atrophy

Chronic subdural hematomasChronic subdural hematomas are usually are usually related to a related to a slower venous bleedslower venous bleed without without accompanying cerebral parenchymal injury. accompanying cerebral parenchymal injury.
These collections are more often These collections are more often biconvexbiconvex, , rather than the crescentic shape of acute rather than the crescentic shape of acute subdural hematomas. subdural hematomas.

Subdural hygromasSubdural hygromas or effusions or effusions consist of collections of CSF in the consist of collections of CSF in the subdural spaces, subdural spaces, presumably due to a presumably due to a traumatic traumatic
arachnoid teararachnoid tear or they may also or they may also develop develop following ventricular following ventricular shunting. shunting.
They may accumulate slowly during the They may accumulate slowly during the first few days following head trauma, first few days following head trauma, especially in the pediatric population.especially in the pediatric population.

CContusions ontusions && LLacerationacerationss
ContusionsContusions are focal areas of are focal areas of cortical cortical hemorrhagic necrosishemorrhagic necrosis occurring at the occurring at the crest of a gyrus and are said to be the crest of a gyrus and are said to be the hallmark of closed head injury;hallmark of closed head injury; they may they may occur occur : : at the site of impact at the site of impact (coup lesions),(coup lesions), or or at a point opposite at a point opposite (contrecoup lesions).(contrecoup lesions).

Contusion/laceration of the brain may be Contusion/laceration of the brain may be accompanied by pure accompanied by pure intracerebral intracerebral hematomahematoma,, often multiple, mainly involving often multiple, mainly involving temporal and frontal regionstemporal and frontal regions. .
A distinction is made between contusions A distinction is made between contusions and lacerations: and lacerations: Contusions Contusions (contusio cerebri)(contusio cerebri) :: the pia is intact the pia is intact, , LLacerationsacerations (laceratio cerebri) (laceratio cerebri) :: the pia- the pia-
arachnoid and underlying brain tissue are tornarachnoid and underlying brain tissue are torn..

CoupCoup--Contrecoup Contrecoup CContusionsontusions
A combination of A combination of vascular and tissue damagevascular and tissue damage leads leads to cerebral contusionto cerebral contusion..
Coup contusionsCoup contusions occur at the area of direct impact occur at the area of direct impact to the skull and occur because of the creation of to the skull and occur because of the creation of negative pressure when the skull, distorted at the negative pressure when the skull, distorted at the site of impact, returns to its normal shapesite of impact, returns to its normal shape..
Contrecoup contusionsContrecoup contusions are similar to coup are similar to coup contusions but are located opposite the site of contusions but are located opposite the site of direct impactdirect impact..

Most of the energy of impact from a small Most of the energy of impact from a small hard object tends to dissipate at the impact hard object tends to dissipate at the impact site, leading to a coup contusionsite, leading to a coup contusion..
On the contrary, impact from a larger object On the contrary, impact from a larger object causes less injury at the impact site since causes less injury at the impact site since energy is dissipated at the beginning or end energy is dissipated at the beginning or end of the head motion, leading to a contrecoup of the head motion, leading to a contrecoup contusioncontusion..

Coup – contracoupCoup – contracoup injury injury


CORTICAL CONTUSIONSCORTICAL CONTUSIONS

Traumatic intracerebral Traumatic intracerebral / intraventricular/ intraventricular hemorrhageshemorrhages
Probably they result from tearing of the Probably they result from tearing of the vessels themselves by mechanical forcesvessels themselves by mechanical forces. .

VASCULAR INJURIESVASCULAR INJURIES
Traumatic Traumatic carotid cavernous fistulascarotid cavernous fistulas can result can result from an injury to the carotid artery at the level from an injury to the carotid artery at the level of the cavernous sinus. of the cavernous sinus.
This causes a This causes a high flow arterial venous shunthigh flow arterial venous shunt and often results in painful unilateral pulsating and often results in painful unilateral pulsating exopthalmosexopthalmos as a result of increased flow in a as a result of increased flow in a retrograde direction in the superior opthalmic retrograde direction in the superior opthalmic veinvein (v. ophthalmica superior)(v. ophthalmica superior). . This can lead to This can lead to visual lossvisual loss..

Traumatic dissections of the Traumatic dissections of the carotid or carotid or vertebral arteries in the neckvertebral arteries in the neck can cause can cause strokestroke. .
This can be due to strangulation or whiplash This can be due to strangulation or whiplash mechanisms which may tear the intima. mechanisms which may tear the intima.
Typically the carotid is dissected usually Typically the carotid is dissected usually just proximal to entering the petrous bone at just proximal to entering the petrous bone at about the C1-C2 level. about the C1-C2 level.

Post-traumatic pseudoaneurysmsPost-traumatic pseudoaneurysms can can occur as a result of vascular injuries occur as a result of vascular injuries intracranially. intracranially.
Vascular spasmVascular spasm can occur as a result of can occur as a result of subarachnoid hemorrhage. subarachnoid hemorrhage.

CEREBROVASCULAR CEREBROVASCULAR DISEASE (CVD)DISEASE (CVD)
CVD REFERS TO ANY ABNORMALITY OF THE CVD REFERS TO ANY ABNORMALITY OF THE BRAIN RESULTING FROM A PATHOLOGICAL BRAIN RESULTING FROM A PATHOLOGICAL
PROCESS INVOLVING BLOOD VESSELS, PROCESS INVOLVING BLOOD VESSELS, CAUSING INADEQUATE OXYGENATION OF CAUSING INADEQUATE OXYGENATION OF
BRAIN TISSUEBRAIN TISSUE

CLASSIFICATIONCLASSIFICATION
HYPOXIC ENCEPHALOPATHYHYPOXIC ENCEPHALOPATHY an overall (GLOBAL) reduction in an overall (GLOBAL) reduction in
blood flow to the brainblood flow to the brain STROKE (focal lesion)STROKE (focal lesion)
sudden onsetsudden onset rapid evolutionrapid evolution focal neurologic deficitfocal neurologic deficit

STROKESTROKEThe typical clinical features include a sudden onset and rapid evolution (minutes/hours) of a focal neurological deficit (indicative of focal damage to the brain).

STROKESTROKE:: CLASSIFICATION CLASSIFICATIONISCHEMIC ISCHEMIC
STROKESTROKEHEMORRHAGIC HEMORRHAGIC
STROKESTROKE
oror
BRAIN BRAIN INFARCTIONINFARCTION
oror
INTRACEREBRAL INTRACEREBRAL BLEEDINGBLEEDING
THE CLINICIAN MUST THE CLINICIAN MUST MAKE THIS DISTINCTION MAKE THIS DISTINCTION
IN ORDER TO TREATIN ORDER TO TREAT
CT/MR SCAN ALLOWS DISTINCTIONCT/MR SCAN ALLOWS DISTINCTION

IIt is important to draw a distinction between t is important to draw a distinction between ischemic stroke, ischemic stroke, which refers to a focal cessation of blood supply which refers to a focal cessation of blood supply
due to due to vascular occlusionvascular occlusion, resulting in, resulting in necrosisnecrosis of tissue (cerebral infarction) of tissue (cerebral infarction)
and hemorrhagic stroke, and hemorrhagic stroke, a term applied to a term applied to rupturerupture of a cerebral blood of a cerebral blood
vessel resulting in spontaneous vessel resulting in spontaneous intracranial intracranial hemorrhage.hemorrhage.
In both instances, subsequent secondary events In both instances, subsequent secondary events such as such as brain swellingbrain swelling and and shifts (herniation) shifts (herniation) result in result in progressive comaprogressive coma and are the cause of and are the cause of deathdeath. .

I. Ischemic stroke I. Ischemic stroke (CEREBRAL INFARCTION)(CEREBRAL INFARCTION)
Although there are many variations regarding the Although there are many variations regarding the evolution, site, size and shape of cerebral infarcts, evolution, site, size and shape of cerebral infarcts, certain patterns emerge based on an interplay of certain patterns emerge based on an interplay of hemodynamic & etiological factors: hemodynamic & etiological factors: (a) (a) the site of the occlusionthe site of the occlusion (eg. distal/proximal/end (eg. distal/proximal/end
artery), in relation to the presence and efficacy of a artery), in relation to the presence and efficacy of a collateral blood supply (eg. anatomical variations, collateral blood supply (eg. anatomical variations, diseased and collateral vessels).diseased and collateral vessels).
(b) (b) type of occlusiontype of occlusion - in general, thrombosis leading to - in general, thrombosis leading to gradual occlusion will allow adaptation of anastomoses, gradual occlusion will allow adaptation of anastomoses, while while emboli produce sudden occlusion.emboli produce sudden occlusion.

CAUSES OF BRAIN INFARCTIONCAUSES OF BRAIN INFARCTION
Atherosclerosis + thrombosisAtherosclerosis + thrombosis EmboliEmboli Stenosis + hypoperfusionStenosis + hypoperfusion Vascular spasmVascular spasm Arterial dissectionArterial dissection Vasculitis/vasculopathyVasculitis/vasculopathy CompressionCompression Vascular “degeneration”Vascular “degeneration”

CAUSES OF BRAIN INFARCTIONCAUSES OF BRAIN INFARCTION
EMBOLIEMBOLI ATHEROMAATHEROMA COMPRESSIONCOMPRESSION
THROMBUTHROMBUSS

Pathology of the Ischemic strokePathology of the Ischemic stroke
Initially all cerebral infarcts are relatively Initially all cerebral infarcts are relatively ""palepale" (dusky red to yellowish-white) in " (dusky red to yellowish-white) in appearance, appearance,
and on CT show up as a and on CT show up as a hypodensehypodense, initially , initially non-enhancing area. non-enhancing area.
Associated brain swelling (Associated brain swelling (edemaedema), with ), with midline shiftmidline shift may be present. may be present.

ISCHEMIC “STROKE”ISCHEMIC “STROKE”
BRAIN BRAIN INFARCTIONINFARCTION
PALE/ANEMICPALE/ANEMIC
RED/HEMORRHAGIC
DO NOT CONFUSE “HEMORRHAGIC INFARCT” DO NOT CONFUSE “HEMORRHAGIC INFARCT”
WITH “HEMORRHAGIC STROKE”WITH “HEMORRHAGIC STROKE”

In some instances, In some instances, re-perfusion of damaged re-perfusion of damaged vesselsvessels results in the production of a results in the production of a hemorrhagic infarcthemorrhagic infarct. .
This is seen most commonly with infarction This is seen most commonly with infarction due to due to embolisationembolisation, where there is subsequent , where there is subsequent fragmentation/lysis of the embolus. fragmentation/lysis of the embolus.
The hemorrhagic appearance is usually The hemorrhagic appearance is usually confined to grey matter and enhances confined to grey matter and enhances brilliantly on CT. brilliantly on CT.
Venous infarcts and those associated with Venous infarcts and those associated with brain herniations are also usually hemorrhagic brain herniations are also usually hemorrhagic in appearance. in appearance.

A MINORITY OF INTIALLY PALE A MINORITY OF INTIALLY PALE INFARCTS BECOMEINFARCTS BECOME
RED RED (HAEMORRHAGIC)(HAEMORRHAGIC)
EMBOLIEMBOLI
HERNIAHERNIA
VENOUSVENOUS

VENOUS INFARCTVENOUS INFARCT
HEMORRHAGICHEMORRHAGIC

INFARCT - EVOLUTIONINFARCT - EVOLUTION

INFARCT - EVOLUTIONINFARCT - EVOLUTION
AFTER +/- 3 DAYSAFTER +/- 3 DAYSGLIGLIAAL REACTIONL REACTION

INFARCT - EVOLUTIONINFARCT - EVOLUTION
LIQUEFACTION BEGINS AT +/- 10 DAYS LIQUEFACTION BEGINS AT +/- 10 DAYS
& CONTINUES FOR WEEKS - MONTHS& CONTINUES FOR WEEKS - MONTHS
MACROPHAGMACROPHAGESES

DISSECTIONDISSECTION
ICA THROMBUSICA THROMBUS

If the patient survives, liquefaction of the If the patient survives, liquefaction of the necrotic brain tissue necrotic brain tissue (liquefactive necrosis)(liquefactive necrosis) begins at +/- 3 days, histology shows: begins at +/- 3 days, histology shows: sheets of compound granular corpuscles sheets of compound granular corpuscles
(macrophages), (macrophages), eventually resulting in the production of a cystic eventually resulting in the production of a cystic
cavity (without mass effect), surrounded by glial cavity (without mass effect), surrounded by glial tissue. tissue.

Correlation of etiology and topographyCorrelation of etiology and topography: : Cerebral thrombosisCerebral thrombosis is the most common is the most common cause of cerebral cause of cerebral
infarction, infarction, usually occurs at a point where the vessels wall has been usually occurs at a point where the vessels wall has been
damaged. damaged. Important underlying processes:Important underlying processes:
hypotension (Watershed infarct), hypotension (Watershed infarct), atherosclerosis,atherosclerosis, vascular injuryvascular injury (polyarteritis nodosa, fungal infection)(polyarteritis nodosa, fungal infection). .
Affected Vessels (most common):Affected Vessels (most common): the internal carotids, the internal carotids, upper vertebral upper vertebral lower basilar arteries. lower basilar arteries.
The resulting infarct may either involve the boundary zone The resulting infarct may either involve the boundary zone between arterial territories (consequent to stenosis without between arterial territories (consequent to stenosis without frank occlusion) or be territorial in nature (with complete frank occlusion) or be territorial in nature (with complete occlusion). occlusion).

Emboli, in contrast to thrombi, usually Emboli, in contrast to thrombi, usually involve smaller vessels, involve smaller vessels, often the terminal branches of the middle often the terminal branches of the middle
cerebral arterycerebral artery The sources of emboli (most common)The sources of emboli (most common)
mural thrombi, mural thrombi, valvular vegetations valvular vegetations ulcerated atherosclerotic plaques. ulcerated atherosclerotic plaques.

Lacunar infarcts: Lacunar infarcts: These are small (cystic) infarcts (1-15 mm These are small (cystic) infarcts (1-15 mm
diameter) diameter) mainly in the pons or deep grey matter of mainly in the pons or deep grey matter of
hypertensivehypertensive individuals individuals the result of the result of lipohyalin degeneration or lipohyalin degeneration or
atherosclerosisatherosclerosis of small vessels <150 microns in of small vessels <150 microns in diameter. diameter. With the advent of CT/MR scans, knowledge of their With the advent of CT/MR scans, knowledge of their
existence has assumed greater importance, particular as existence has assumed greater importance, particular as they may be clinically silent or symptomatic, they may be clinically silent or symptomatic, depending on size and position. depending on size and position.

LACUNAR INFARCTSLACUNAR INFARCTS
HypertensionHypertension LipohyalinosisLipohyalinosis Deep grey matterDeep grey matter PonsPons

II. Hemorrhagic stroke II. Hemorrhagic stroke
(SPONTANEOUS INTRACRANIAL HEMORRHAGE)(SPONTANEOUS INTRACRANIAL HEMORRHAGE)
The following discussion only deals with The following discussion only deals with spontaneous spontaneous (non-traumatic)(non-traumatic) intracranial intracranial hemorrhage, of which there are three major hemorrhage, of which there are three major categoriescategories::
1. INTRACEREBRAL HEMORRHAGE1. INTRACEREBRAL HEMORRHAGE 2. SUBARACHNOID HEMORRHAGE2. SUBARACHNOID HEMORRHAGE 3. INTRA-EXTRACEREBRAL (MIXED) 3. INTRA-EXTRACEREBRAL (MIXED)
HEMORRHAGEHEMORRHAGE (a form of hemorrhage (a form of hemorrhage involving both the parenchyma and subarachnoid involving both the parenchyma and subarachnoid space) space)

CT features of intracranial hemorrhage:
As extravasated blood undergoes As extravasated blood undergoes liquefaction and absorbtion, changes liquefaction and absorbtion, changes occur in its CT appearances:occur in its CT appearances:
Acute stageAcute stage of hemorrhage (0-2 days: of hemorrhage (0-2 days: hyperdensehyperdense), ),
Subacute stageSubacute stage (3-14 days: (3-14 days: isodense isodense) ) Chronic stageChronic stage (>14 days - (>14 days - hypodensehypodense). ).

1. Intracerebral (intraparenchymal) 1. Intracerebral (intraparenchymal) hemorrhagehemorrhage
These hemorrhages may be further These hemorrhages may be further subdivided, as the site of the bleed is subdivided, as the site of the bleed is indicative of the underlying indicative of the underlying pathology: pathology: 1.1. Ganglionic hemorrhage,1.1. Ganglionic hemorrhage,
1.2. Lobar hemorrhage.1.2. Lobar hemorrhage.

1.1. 1.1. Ganglionic region hemorrhageGanglionic region hemorrhage The most common cause of death among The most common cause of death among
cerebrovascular diseases.cerebrovascular diseases. Ganglionic region hemorrhage is almost invariably Ganglionic region hemorrhage is almost invariably
associated with associated with hypertensive arteriolosclerosishypertensive arteriolosclerosis affecting the small penetrating, lenticulo-striate affecting the small penetrating, lenticulo-striate vessels, vessels,
a large a large hematomahematoma,, often often rupture into the ventriclerupture into the ventricle (hemato- (hemato-
hydrocephalus), resulting in hydrocephalus), resulting in rapid deathrapid death.. Approximately 20 % of hypertensive intracerebral Approximately 20 % of hypertensive intracerebral
hemorrhages occur in either the hemorrhages occur in either the cerebellumcerebellum or or brain stembrain stem . .

The brains of hypertensive patients at The brains of hypertensive patients at autopsy (also exhibit):autopsy (also exhibit):
Small orange-yellow slit-like lesions Small orange-yellow slit-like lesions (slit hemorrhages) at the junction of (slit hemorrhages) at the junction of cortex and white matter, or in the basal cortex and white matter, or in the basal ganglia. ganglia.
These represent the scars of old These represent the scars of old circumscribed small hemorrhages.circumscribed small hemorrhages.

1.2. Lobar hematomas1.2. Lobar hematomas
These types of hemorrhages are usually These types of hemorrhages are usually caused by caused by rupture rupture of an of an arterio-venous arterio-venous malformationmalformation (AVM) or angioma. (AVM) or angioma.
However, if the hematoma is present in the However, if the hematoma is present in the frontal or medial temporal lobesfrontal or medial temporal lobes, a , a ruptured berry aneurysmruptured berry aneurysm should also be should also be considered in the differential diagnosis. considered in the differential diagnosis.

Lobar hematomas may also occur in Lobar hematomas may also occur in association with certain association with certain primary primary brain tumorsbrain tumors (notably (notably oligodendroglioma), or oligodendroglioma), or metastasesmetastases (choriocarcinoma & melanoma).(choriocarcinoma & melanoma).
Hemorrhages due to blood Hemorrhages due to blood dyscrasia (eg. in association with dyscrasia (eg. in association with leukaemia or lymphoma) are also leukaemia or lymphoma) are also frequently lobar and may occur at frequently lobar and may occur at any site. any site. They are of variable size and are They are of variable size and are
often multifocal.often multifocal.

Etiopathogenesis of the Etiopathogenesis of the Lobar hematomasLobar hematomas 11. Rupture. Rupture AnywhereAnywhere
arterio-venous arterio-venous malformation (AVM) malformation (AVM)
angiomaangioma in Frontal or Medial in Frontal or Medial
temporal lobes temporal lobes ruptured berry ruptured berry
aneurysmaneurysm
2. Tumors2. Tumors PrimaryPrimary
OligodendrogliomaOligodendroglioma MetastaticMetastatic
choriocarcinomachoriocarcinoma melanomamelanoma
3. Blood dyscrasia3. Blood dyscrasia Leukaemia Leukaemia Lymphoma.Lymphoma.

2. Subarachnoid hemorrhage2. Subarachnoid hemorrhage
Major subarachnoid hemorrhage is most commonly caused by rupture of a berry aneurysm, usually situated at the junction of the Middle
Cerebral Artery/Posterior ComA, or Anterior Cerebral Artery /Anterior ComA.
The exact etiology of these aneurysms is unclear but they are basically developmental in nature.
Although infrequent, it should also be remembered that a ruptured berry aneurysm is also the commonest cause of a spontaneous subdural hemorrhage.

3. Intra-extracerebral (mixed) 3. Intra-extracerebral (mixed) hemorrhagehemorrhage
These hemorrhages can be defined by CT and These hemorrhages can be defined by CT and will have the clinical features common to SAH will have the clinical features common to SAH and lobar hemorrhage. and lobar hemorrhage.
The hematoma is usually peripheral and may The hematoma is usually peripheral and may be associated with a relatively small be associated with a relatively small subarachnoid bleed. subarachnoid bleed.
The common causes are rupture of a The common causes are rupture of a superficially situated superficially situated AVMAVM, or , or mycotic mycotic aneurysmaneurysm (associated with acute infective (associated with acute infective endocarditis). endocarditis).

Arteriovenous malformation (AVM)Arteriovenous malformation (AVM)
An arteriovenous malformation (AVM) is a tangled An arteriovenous malformation (AVM) is a tangled cluster of vessels, typically located supratentorially, cluster of vessels, typically located supratentorially, in which arteries connect directly to veins with no in which arteries connect directly to veins with no intervening capillary bed. intervening capillary bed.
The lesion may be compact, containing a core of The lesion may be compact, containing a core of tightly packed venous loops, or it may be diffuse, tightly packed venous loops, or it may be diffuse, with anomalous vessels dispersed among normal with anomalous vessels dispersed among normal brain parenchyma. brain parenchyma.


AVMs account for approximately 11% of AVMs account for approximately 11% of cerebrovascular malformations.cerebrovascular malformations.
Pial or parenchymal AVMs:Pial or parenchymal AVMs: (most common; (most common; congenital) supplied by the internal carotid or congenital) supplied by the internal carotid or vertebral circulation; vertebral circulation;
Dural AVMs:Dural AVMs: by the external carotid circulation; by the external carotid circulation; secondary to trauma, surgery, thrombosis of an secondary to trauma, surgery, thrombosis of an adjacent venous sinus, or veno-occlusive disease. adjacent venous sinus, or veno-occlusive disease.
Mixed AVMs: Mixed AVMs: (pial+dural)(pial+dural) from both the internal from both the internal and external carotid arteries. and external carotid arteries. A pediatric variant of AVM is the vein-of-Galen A pediatric variant of AVM is the vein-of-Galen
aneurysm, in which an AVM drains to and aneurysm, in which an AVM drains to and dilates the great vein of Galen. dilates the great vein of Galen.

PathologyPathology
AVMs can be found throughout the AVMs can be found throughout the CNS. CNS.
They may be microscopic or large They may be microscopic or large enough to involve an entire hemisphere enough to involve an entire hemisphere of the brain. of the brain.
Most AVMs are small (2-4 cm, 42%) to Most AVMs are small (2-4 cm, 42%) to moderately sized (4-6 cm, 35%). moderately sized (4-6 cm, 35%).

90% are supratentorial and tend 90% are supratentorial and tend to occur at watershed areas, to occur at watershed areas,
10% are infratentorial. 10% are infratentorial. Supratentorial AVMsSupratentorial AVMs
70% are purely pial with no 70% are purely pial with no meningeal or dural vascular supply. meningeal or dural vascular supply.
The remainder of lesions are purely The remainder of lesions are purely dural or a pial-dural mix. dural or a pial-dural mix.
Approximately one half of posterior Approximately one half of posterior fossa AVMs are purely dural or a pial-fossa AVMs are purely dural or a pial-dural mix. dural mix.

Pial AVMs lie within brain parenchyma and derive Pial AVMs lie within brain parenchyma and derive blood from the cerebral arteries, namely blood from the cerebral arteries, namely anterior cerebral artery (ACA), anterior cerebral artery (ACA), middle cerebral artery (MCA),middle cerebral artery (MCA), posterior cerebral artery (PCA). posterior cerebral artery (PCA).
The rapid shunting of blood typical of pial AVMs The rapid shunting of blood typical of pial AVMs is visualized as an abnormal tangle of blood vessels is visualized as an abnormal tangle of blood vessels with early, and frequently rapid, venous drainage, with early, and frequently rapid, venous drainage, uniquely demonstrated by catheter angiography. uniquely demonstrated by catheter angiography.
Most AVMs involving the ACA or its branches are Most AVMs involving the ACA or its branches are purely pial.purely pial.

Intracranial aneurysmIntracranial aneurysm
The common causes: The common causes: hemodynamic induced/degenerative vascular injury, hemodynamic induced/degenerative vascular injury, atherosclerosis (typically leads to fusiform aneurysms), atherosclerosis (typically leads to fusiform aneurysms), underlying vasculopathy (eg, fibromuscular dysplasia), underlying vasculopathy (eg, fibromuscular dysplasia), high-flow states, as in arteriovenous malformation (AVM) high-flow states, as in arteriovenous malformation (AVM)
and fistula. and fistula. Uncommon causesUncommon causes
trauma, trauma, infection, infection, drugs, drugs, neoplasms (primary or metastatic). neoplasms (primary or metastatic).

ClassificationClassification
Saccular aneurysms Saccular aneurysms Developmental/degenerative Developmental/degenerative Traumatic Traumatic Mycotic (infectious process involving the arterial wall)Mycotic (infectious process involving the arterial wall) Oncotic (malignant head and neck tumors) Oncotic (malignant head and neck tumors) Flow-related (aneurysms with AVM) Flow-related (aneurysms with AVM) Vasculopathy-related (SLE; Takayasu; Fibromuscular Vasculopathy-related (SLE; Takayasu; Fibromuscular
dysplasia ) dysplasia ) Drug-related (cocaine, heroin, ephedrine, methamphetamine) Drug-related (cocaine, heroin, ephedrine, methamphetamine)
Fusiform aneurysms Fusiform aneurysms Dissecting aneurysms Dissecting aneurysms

Saccular aneurysmsSaccular aneurysms

Location Location
Anterior circulation aneurysms Anterior circulation aneurysms (85%):(85%): Common locations are the anterior Common locations are the anterior
communicating artery (30-35%),communicating artery (30-35%), internal carotid artery (ICA) at the internal carotid artery (ICA) at the
posterior communicating artery origin posterior communicating artery origin (30-35%), (30-35%),
median communicating artery median communicating artery bifurcation (20%). bifurcation (20%).

Posterior (vertebrobasilar) Posterior (vertebrobasilar) circulation aneurysms (15%):circulation aneurysms (15%): 5% arise from the basilar artery 5% arise from the basilar artery
bifurcation, bifurcation, 1-5% arise from other posterior fossa 1-5% arise from other posterior fossa
vessels.vessels. Common posterior fossa sites include the Common posterior fossa sites include the
superior cerebellar artery and the superior cerebellar artery and the vertebral artery (VA) at the origin of the vertebral artery (VA) at the origin of the posterior inferior cerebellar artery posterior inferior cerebellar artery (PICA). (PICA).
Anterior inferior cerebellar artery Anterior inferior cerebellar artery (AICA) aneurysms are rare. (AICA) aneurysms are rare.


Pathology Pathology
Saccular aneurysmsSaccular aneurysms True aneurysmsTrue aneurysms
they are dilatations of a vascular lumen caused by weakness they are dilatations of a vascular lumen caused by weakness of all vessel wall layers.of all vessel wall layers.
Rounded, berrylike outpouchings Rounded, berrylike outpouchings Arise from arterial bifurcation points. Arise from arterial bifurcation points. The aneurysmal sac itself is usually composed only of intima The aneurysmal sac itself is usually composed only of intima
and adventitia.and adventitia. Lymphocytes and phagocytes may infiltrate the adventitia. Lymphocytes and phagocytes may infiltrate the adventitia. Thrombotic debris is often present in the lumen of the Thrombotic debris is often present in the lumen of the
aneurysmal sac. aneurysmal sac. Atherosclerotic changes in the parent vessel are also common.Atherosclerotic changes in the parent vessel are also common.

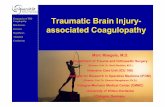
Berry aneurysms typically occur at the bifurcation of cerebral arteries. A berry aneurysm that has been sectioned to reveal the saccular lumen in the center arising off the arterial lumen at the left.

ComplicationsComplications
Subarachnoid hemorrhageSubarachnoid hemorrhage Most aneurysms do not cause symptoms Most aneurysms do not cause symptoms
until they ruptureuntil they rupture


Conditions that have been Conditions that have been associated with increased incidence associated with increased incidence of cerebral aneurysms are as of cerebral aneurysms are as follows: follows: Anomalous vessels Anomalous vessels Coarctation of the aorta Coarctation of the aorta Polycystic kidney disease (10%) Polycystic kidney disease (10%) Fibromuscular dysplasia Fibromuscular dysplasia Connective tissue disorders (eg, Connective tissue disorders (eg,
Marfan, Ehlers-Danlos) Marfan, Ehlers-Danlos) High-flow states (eg, vascular High-flow states (eg, vascular
malformations, fistulae) malformations, fistulae) Spontaneous dissections.Spontaneous dissections.

Intracranial aneurysms are Intracranial aneurysms are multiple in 15-20% of all cases:multiple in 15-20% of all cases: 75% of patients with multiple 75% of patients with multiple
intracranial aneurysms have 2 intracranial aneurysms have 2 aneurysms, aneurysms,
15% have 3, 15% have 3, 10% have more than 3. 10% have more than 3.
A strong female predilection is A strong female predilection is observed with multiple aneurysms. observed with multiple aneurysms. While the overall female-to-male ratio While the overall female-to-male ratio
is 5:1, the ratio rises to 11:1 in is 5:1, the ratio rises to 11:1 in patients with more than 3 aneurysms. patients with more than 3 aneurysms.


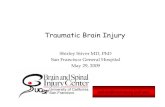
Fusiform aneurysmsFusiform aneurysms

Fusiform aneurysmsFusiform aneurysms
Atherosclerotic aneurysmsAtherosclerotic aneurysms a severe and unusual form of atherosclerosis. a severe and unusual form of atherosclerosis.
Damage to the media results in arterial stretching and Damage to the media results in arterial stretching and elongation that may extend over a considerable elongation that may extend over a considerable length. length. These ectatic vessels may have more focal areas of These ectatic vessels may have more focal areas of
fusiform or even saccular enlargement. fusiform or even saccular enlargement.

Dissecting aneurysmsDissecting aneurysms

In arterial dissections, blood accumulates within the In arterial dissections, blood accumulates within the vessel wall through a tear in the intima and internal vessel wall through a tear in the intima and internal elastic lamina. elastic lamina.
The consequences of this intramural hemorrhage The consequences of this intramural hemorrhage vary. vary. If blood dissects subintimally, it causes luminal If blood dissects subintimally, it causes luminal
narrowing or even occlusion. narrowing or even occlusion. If the intramural hematoma extends into the If the intramural hematoma extends into the
subadventitial plane, a saclike outpouching may be subadventitial plane, a saclike outpouching may be formed.formed.
Thus, uncomplicated dissections do not project Thus, uncomplicated dissections do not project beyond the lumen of the parent vessel, and beyond the lumen of the parent vessel, and dissections with saclike outpouchings are termed dissections with saclike outpouchings are termed dissecting aneurysms. dissecting aneurysms.

Do not confuse these focal Do not confuse these focal aneurysmal dilatations with the aneurysmal dilatations with the pseudoaneurysms that result from pseudoaneurysms that result from arterial rupture and subsequent arterial rupture and subsequent encapsulation of the perivascular encapsulation of the perivascular hematoma. hematoma.
Dissecting aneurysms may arise Dissecting aneurysms may arise spontaneously. spontaneously. More commonly, trauma or an More commonly, trauma or an
underlying vasculopathy such as underlying vasculopathy such as Fibromuscular dysplasia is Fibromuscular dysplasia is implicated. implicated.

Location:Location: Internal carotid arteryInternal carotid artery Vertebral arteryVertebral artery

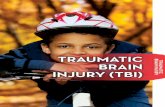
A dissecting aneurysm showing the lumen of blood vessel in relation to the aneurysm.

THANK TOUTHANK TOU