Transthoracic needle biopsy for suspected thoracic malignancy in elderly patients using CT guidance
4
Clinical Radiology (1998) 53, 116-I 19 Transthoracic Needle Biopsy for Suspected Thoracic Malignancy in Elderly Patients Using CT Guidance T. S. BROWN and P. KANTHAPILLAI* Departments of Diagnostic hnaging and *Respiratory Medicine, Bradford Hospitals NHS Trust, Bradford Royal Infirmary, Bradford, UK There are few reports of transthoracic needle biopsy (TNB) in elderly (> 70 years) patients although there is some evidence that age may be a risk factor in developing pneumothorax. We report our experience of 38 patients, age range 70-90 years, who underwent computed tomography (CT)-guided TNB for suspected malignancy of the chest, with particular reference to sensitivity and complication rate following the procedure. The biopsy was obtained using either a spinal needle or, if appropriate, a core of tissue was obtained using a cutting needle. The biopsy showed evidence of malignancy in 27 patients. Pneumothorax occurred in 10 of 40 biopsies. Two patients with pneumothorax required pleural drains; one was discharged the following day and the other required drainage for 3 days. Haemoptysis was not a problem but occurred as a transient postbiopsy event in three patients. In 26 of 40 (65%) episodes the patients were sent home within 24h of the diagnostic procedure. It is thus quite possible to undertake the procedure on a day case basis. CT- guided TNB is a safe and reliable procedure in elderly patients with suspected chest malignancy and is well tolerated. Brown, T.S. & Kanthapillai, P. (1997). Clinical Radiology 53, 116-119. Transthoracic Needle Biopsy for Suspected Thoracic Malignancy in Elderly Patients Using CT Guidance Accepted for Publication 9 May 1997 The indications for transthoracic needle biopsy (TNB) in patients with suspected chest malignancy are now well established [1,2]. The complications of haemoptysis and pneumothorax are well known; air embolism and seeding of tumour along the needle track are both rare complications [2-5]. There are few absolute contraindications but a patient who fails to breath hold on demand or is fidgety should not be considered for the procedure [3,6]. Bleeding is the most serious and life threatening complication. Patients with bleeding disorders needing TNB can usually have coagula- tion abnormalities corrected as part of the pre-procedure work up. Pulmonary hypertension theoretically places the patient at increased risk of haemorrhage but some authors [2,3] suggest that such patients can safely undergo the procedure. Patients with a reduced forced expiratory volume in 1 s (FEV1) have an increased pneumothorax rate [7,8]. However, patients with advanced emphysema can undergo lung biopsy [3]. Pneumothorax may not be well tolerated by patients with an FEV1 of less than 11 and the procedure should be undertaken in such patients with cau- tion [6]. Age is reported as a risk factor in developing pneumothorax by some authors [2,5]. We report a retrospective study on the use of computed tomography (CT)-guided TNB in 38 elderly patients with reference to sensitivity, complicating pneumothorax and patient tolerance. Correspondence to: Dr T. S. Brown, Department of Diagnostic Imaging, Bradford Hospitals NHS Trust, Bradford Royal Infirmary, Duckworth Lane, Bradford BD9 6RJ, UK. 1998 The Royal Collegeof Radiologists. PATIENTS AND METHODS The notes of 38 patients (20 males and 18 females) with an average age of 75.3 years (range 70-89 years), who had TNBs between 1994 and 1996 were studied retrospectively. Patients were referred from the Chest, Medical or Geriatric units. Forty procedures were performed. One investigator (TSB) or a trainee under his direct supervision performed all the biopsies. The procedure was explained to the patients by the radiologist in the imaging department before the examination, after already having had it explained to them on the ward, where formal signed consent had been obtained. They were warned about the possibility of a pneumothorax and all offered the chance to withdraw from the procedure. Routine clotting screens were not performed. Patients were scanned on a Siemens Somatom Plus scanner. Initially, discontinuous 10mm slices were used but, more recently, the protocol has been changed to spiral acquisition with contiguous 10 mm reconstructions from the thoracic inlet to the adrenals. Where necessary, additional slices were taken with the patient in an appropriate position to identify the most direct approach to the lesion. Unco- operative or dyspnoeic patients did not undergo biopsy and neither did patients who were unable to reproduce their respiratory excursion, with the result that the skin marker and lesion did not appear on the same image. If the lesion could be approached without traversing aerated lung, an 18 G Temno needle (Bauer Medical, Inc., Clearwater, FL, USA) was preferred (Fig. 1), otherwise a 20 G or 22 G spinal needle was used, depending largely upon the presence or absence of signs of emphysema (Fig. 2) on the siting scans.
Transcript of Transthoracic needle biopsy for suspected thoracic malignancy in elderly patients using CT guidance

Clinical Radiology (1998) 53, 116-I 19
Transthoracic Needle Biopsy for Suspected Thoracic Malignancy in Elderly Patients Using CT Guidance
T. S. BROWN and P. KANTHAPILLAI*
Departments of Diagnostic hnaging and *Respiratory Medicine, Bradford Hospitals NHS Trust, Bradford Royal Infirmary, Bradford, UK
There are few reports of transthoracic needle biopsy (TNB) in elderly (> 70 years) patients although there is some evidence that age may be a risk factor in developing pneumothorax. We report our experience of 38 patients, age range 70-90 years, who underwent computed tomography (CT)-guided TNB for suspected malignancy of the chest, with particular reference to sensitivity and complication rate following the procedure. The biopsy was obtained using either a spinal needle or, if appropriate, a core of tissue was obtained using a cutting needle.
The biopsy showed evidence of malignancy in 27 patients. Pneumothorax occurred in 10 of 40 biopsies. Two patients with pneumothorax required pleural drains; one was discharged the following day and the other required drainage for 3 days. Haemoptysis was not a problem but occurred as a transient postbiopsy event in three patients.
In 26 of 40 (65%) episodes the patients were sent home within 24h of the diagnostic procedure. It is thus quite possible to undertake the procedure on a day case basis. CT- guided TNB is a safe and reliable procedure in elderly patients with suspected chest malignancy and is well tolerated. Brown, T.S. & Kanthapillai, P. (1997). Clinical Radiology 53, 116-119. Transthoracic Needle Biopsy for Suspected Thoracic Malignancy in Elderly Patients Using CT Guidance
Accepted for Publication 9 May 1997
The indications for transthoracic needle biopsy (TNB) in patients with suspected chest malignancy are now well established [1,2]. The complications of haemoptysis and pneumothorax are well known; air embolism and seeding of tumour along the needle track are both rare complications [2-5]. There are few absolute contraindications but a patient who fails to breath hold on demand or is fidgety should not be considered for the procedure [3,6]. Bleeding is the most serious and life threatening complication. Patients with bleeding disorders needing TNB can usually have coagula- tion abnormalities corrected as part of the pre-procedure work up. Pulmonary hypertension theoretically places the patient at increased risk of haemorrhage but some authors [2,3] suggest that such patients can safely undergo the procedure. Patients with a reduced forced expiratory volume in 1 s (FEV1) have an increased pneumothorax rate [7,8]. However, patients with advanced emphysema can undergo lung biopsy [3]. Pneumothorax may not be well tolerated by patients with an FEV1 of less than 11 and the procedure should be undertaken in such patients with cau- tion [6]. Age is reported as a risk factor in developing pneumothorax by some authors [2,5].
We report a retrospective study on the use of computed tomography (CT)-guided TNB in 38 elderly patients with reference to sensitivity, complicating pneumothorax and patient tolerance.
Correspondence to: Dr T. S. Brown, Department of Diagnostic Imaging, Bradford Hospitals NHS Trust, Bradford Royal Infirmary, Duckworth Lane, Bradford BD9 6RJ, UK.
�9 1998 The Royal College of Radiologists.
PATIENTS AND METHODS
The notes of 38 patients (20 males and 18 females) with an average age of 75.3 years (range 70-89 years), who had TNBs between 1994 and 1996 were studied retrospectively. Patients were referred from the Chest, Medical or Geriatric units. Forty procedures were performed.
One investigator (TSB) or a trainee under his direct supervision performed all the biopsies. The procedure was explained to the patients by the radiologist in the imaging department before the examination, after already having had it explained to them on the ward, where formal signed consent had been obtained. They were warned about the possibility of a pneumothorax and all offered the chance to withdraw from the procedure. Routine clotting screens were not performed.
Patients were scanned on a Siemens Somatom Plus scanner. Initially, discontinuous 10mm slices were used but, more recently, the protocol has been changed to spiral acquisition with contiguous 10 mm reconstructions from the thoracic inlet to the adrenals. Where necessary, additional slices were taken with the patient in an appropriate position to identify the most direct approach to the lesion. Unco- operative or dyspnoeic patients did not undergo biopsy and neither did patients who were unable to reproduce their respiratory excursion, with the result that the skin marker and lesion did not appear on the same image. If the lesion could be approached without traversing aerated lung, an 18 G Temno needle (Bauer Medical, Inc., Clearwater, FL, USA) was preferred (Fig. 1), otherwise a 20 G or 22 G spinal needle was used, depending largely upon the presence or absence of signs of emphysema (Fig. 2) on the siting scans.

THORACIC NEEDLE BIOPSY 117
RESULTS
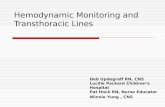
Fig. 1 - Squamous carcinoma of the right upper lobe in contact with the chest wall. Absence of an air gap made this suitable for biopsy with an 18 G Temno needle (patient 11).
Fig. 2 - Computed tomography shows areas of lung destruction caused by emphysema. The biopsy pathway should avoid this area, if possible.
Local anaesthetic was injected using care to avoid traver- sing the pleura on no more than one occasion, thus lessening the chance of a complicating pneumothorax. Needle choice was always made by TSB in the light of the siting images. Two passes into the lesion were usually made, but if there was evidence of severe emphysema on the siting images, only a single pass was made. Technical staff from the pathology department were present to prepare smears on slides and save any clot for embedding in wax. If core samples were taken pathology staff were not called to the department; the specimens were put in formalin and sent directly to the laboratory.
A CT-slice was taken on completion of the biopsy, at the biopsy level, to check for an immediate pneumothorax and, if present, the patient was returned to the ward with a large erect PA chest film. All patients were sent back to the X-ray department for a chest X-ray after 4 h, to look for extension of an existing pneumothorax, or the development of a delayed one.
Table 1 gives details of age, sex, biopsy result, needle size, complicating pneumothorax and, where recorded, FEV1 as a percentage of predicted.
Twenty males (average age 74.5 years) and 18 females (average age 76.4 years) were studied. The incidence of pneumothorax as a whole in the series was 25% [four males, one twice (20%) and five females (27%)]. All pneu- mothoraces occurred at the time of the biopsy, there were no delayed episodes. One patient had a pneumothorax on two occasions in spite of using a thinner needle at the second attempt. Three patients had a small haemoptysis immedi- ately after the biopsy.
Five patients with an FEV 1 of below 11 (mean percentage predicted 39.7%) had six biopsies. All were referred by senior chest doctors who felt that, despite evidence of severe obstructive pulmonary disease, it was important to obtain a tissue diagnosis. Of these, one patient with an FEV1 of 0.951 developed a pneumothorax but did not require a pleural drain. Another patient with an FEV1 of 0.761 had a second biopsy because of failure to obtain an adequate sample at the first attempt and suffered no pneumothorax with either. Four pneumothoraces occurred in patients with an FEV1 greater than 70% of the predicted value, an incidence of 50%. Three episodes of pneumothorax occurred in 17 biopsies (18%) on patients with an FEV1 of less than 70% of the predicted value (mean = 55.0%).
Twenty-three procedures were undertaken using a 20 G needle with five episodes of pneumothorax (22%); of 13 episodes in which a 22G needle was used four pneu- mothoraces occurred (31%). One patient who underwent a biopsy using a Temno needle developed a pneumothorax requiring a pleural drain.
Twenty-seven patients were admitted on the day of the biopsy on 29 occasions; 10 of these were discharged home the same day and a further 13 within 24 h of admission. Two patients had one repeat admission each. Of patients kept in for longer than 24 h, two, both with small pneumothoraces, were kept for 4 days. One admitted to dysphagia after the biopsy and was investigated as an in-patient and the other was kept in for decision making. A third patient with a pneumothorax had a chest drain removed at 3 days but stayed in for a further 10 days for palliation.
Eleven patients were investigated as part of an in-patient protocol. The cumulative total of in-patient time prior to the biopsy in this group was 181 days (mean 14 days). Three of these patients went home within 24 h of the TNB. Twenty-six patients had 45 other negative diagnostic tests for malignancy, including 27 bronchoscopies, before the TNB. Of 23 patients who had negative bronchoscopies 18 (78%) had a positive yield from the biopsy. Eleven patients had TNB as the only investigation of the lung lesion. Nine of 11 were admitted on the day of the test. Three of 11 went home the same day and another five the following day. Excluding the two patients who had a diagnosis of benign disease, there was a sensitivity of 75% for the diagnosis of malignancy in the remaining 36 patients.
DISCUSSION
The sensitivity of the technique in the diagnosis of malignancy in our series is close to the levels reported in recent reports in the literature [2].
�9 1998 The Royal College of Radiologists, Clinical Radiology, 53, 116-119.

1 18 CLINICAL RADIOLOGY
Table 1 - Details of age, sex, biopsy result, needle size, pneumothorax and FEVI as a percentage of predicted value
Patient Age/sex Biopsy result NeedIe/pneumothorax FEV1 (%)
1 70/M Adeno 20/+ 69.8 2 76/F Myeloma 20/ - - - 3 75/F Adeno 20/+ 65.0 4 75/M No malignancy 22/ - - - 5 71/M Non-sclc 18/+ drn 73.7 6 76/F Squamous 22/ - - - 7 73/M Adeno 20 / - 66.9 8 80/M No malignancy 20/ - - - 9 73/M Inad 20/ - 82.0
10 71/M Squamous 20/ - 45.8 11 75/M Squamous 18/- 30.7 12 75/F Squamous 20/ - 42.7 13 77/F Benign 22/+ - - 14 72/F Squamous 20/ - 34.2 15 72/M Failed x 2 20,22/++ 70.6 16 74/M Squamous 20/ - - - 17 81/M Poorly diff 20/- 66.3 18 7 I/M squamous 22 / - 51.4 19 71/M Inad 22 / - - - 20 70/F Squamous 20/ - - - 2l 70/F Inad 20/+ - - 22 89/F Non-diag 22/ - - - 23 72/F Adeno 22 ,22 / - - 35.3 24 75/M Squamous 20/ - 58.2 25 77/F Malignant 20/+ - - 26 76/F Adeno 22/+ 55.5 27 70/M Poorly diff 20/- 60.1 28 74/F Inflammatory 20/ - 84.3 29 88/F Poorly diff 20 / - 92.8 30 85/M PoorLy diff 22 / - 63.0 31 75/M Adeno 18/- 69.1 32 76/M Squamous 20/+ drn 74.9 33 74/F Adeno 20/ - 64.1 34 76/F Sclc 22 / - - - 35 74/M Non-malig 20 / - 57.2 36 73/F Sclc 18/- 92.0 37 77/M Adeno 22/ - - - 38 85/F Non-malig 20/ - 100.0
Adeno, adenocarcinoma; squamous, squamous carcinoma; sclc, small cell lung carcinoma; poorly dill poorly differentiated carcinoma; inad, specimen inadequate for diagnostic purposes; non-rnalig, non-malignant; din, pleural drain.
The incidence of pneumothorax reported by Sinner [5] in patients over 70 years old was 43%. An increase in the incidence of pneumothorax has been reported in patients who had evidence of obstructive pulmonary disease, com- pared with those with normal lung function studies [7-11]. Neither age nor evidence of obstructive lung disease predis- posed patients in our series to pneumothorax. The incidence of this complication was well within the ranges reported else- where [1-4,6,12]. In those patients who might have been at risk because of obstructive pulmonary disease, with an FEV1 of less than 70% of the predicted value, the incidence of pneumothorax was no greater than in the group as a whole. Patients with severe obstructive lung disease (an FEV1 of < 11) might not tolerate a pneumothorax well. Such an event may be associated with significant disability and require timely intervention in the imaging department [3,8]. It is difficult to explain the 50% incidence of pneumothorax in eight patients who had an FEV1 greater than 70% of the predicted value. It is possible that small target lesions or long needle tracks might account, in part, for the higher than expected incidence of pneumothorax [7,13,14] but neither of these were measured in this series.
We agree with Tarver [6] that patients with an FEV1 of less than 11 should be carefully considered before under- going the procedure, but that such patients should not be automatically excluded.
The use of CT enables the radiologist to plan an approach to the lesion avoiding large vessels and bullae and thereby reduce potential complications. It also has the very real advantage of showing the exact position of the needle tip in the target lesion (Fig. 3).
Fluoroscopy does not offer the same route planning and this may account for the higher pneumothorax rate in earlier reports. CT increases the confidence of those undertaking TNB, and because of this the number of TNBs has increased [ 15]. An increase in the reported incidence of pneumothorax following CT biopsies may be because attempts are being made on more difficult lesions requiring multiple passes and an extended biopsy time [2]. There is no doubt that the use of CT in this institution has increased the number of guided lung biopsies and has encouraged us to include patients in their eighth and ninth decades.
Pneumothorax increases in relation to the bore of the needle [1,6]. Bias in the selection of needle size probably explains the increased incidence of pneumothorax in the thinner needle group. The thin needle was chosen because it was felt that the patient was at risk of a pneumothorax when the initial siting images were viewed, and the needle choice was expected to lessen the chance of a compli- cating pneumothorax. Garcia-Rio et al. [7], using 25 G needles, report an overall pneumothorax occurrence of 19%.
�9 1998 The Royal College of Radiologists, Clinical Radiology, 53, 116-119.

THORACIC NEEDLE BIOPSY 119
Fig. 3 - The beam hardening artefact caused by the needle tip confirms its position within the lesion.
TNB provides a rapid pathway for the diagnosis of malignant lung lesions, avoiding other tests and hospital stays, thus reducing costs [4]. Our results indicate that elderly people can cope well with TNBs. There is no evidence that they are at increased risk of suffering com- plications. Not only in the interests of reducing patient costs but also to avoid the charge of ageism, we argue that those with a suspected peripheral malignancy, or following a negative bronchoscopy, should be offered the opportunity of a CT-guided TNB.
REFERENCES
1 Perlmutt LM, Johnston WW, Dunnick NR. Percutaneous thoracic needle aspiration: a review. American Journal of Roentgenology 1989; 15:451-455.
2 Salazar AM, Westeott JL. The role of transthoracic needle biopsy for the diagnosis and staging of lung cancer. Clinics in Chest Medicine 1993;14:99-110.
3 Weisbrod GL. Transthoracic percutaneous lung biopsy. Radiologic Clinics of North America 1990;28:647-655.
4 Weisbrod GL. Transthoracic percutaneous fine-needle aspiration biopsy in the chest and mediastinum. Seminars in lnterventional Radiology 1991;8:1-14.
5 Sinner WN. Complications of percutaneous transthoracic needle aspira- tion biopsy. Acta Radiologica Diagnosis 1976;17:813-828.
6 Tarver RD, Conces DJ. Interventional chest radiology. Radiologic Clinics of North America 1994;32:689-709.
7 Garcia-Rio F, Pino JM, Casadevall Jet al. Use of spirometry to predict risk of pneumothorax in CT-guided needle biopsy of the lung. Journal of Computer Assisted Tomography 1996;20:20-23.
8 Kazerooni EA, Hartker FW III, Whyte RI et al. Transthoracic needle aspiration in patients with severe emphysema. A study of lung trans- plant candidates. Chest 1996;109:616-619.
9 Johnsrude IS, Silverman JF, Weaver MD et al. Rapid cytology to decrease pneumothorax incidence after percutaneous biopsy. American Journal of Roentgenology 1985;144:793-794.
l0 Fish GD, Stanley JH, Miller KS et al. Postbiopsy pneumothorax: estimating the risk by chest radiography and pulmonary function tests. American Journal of Roentgenology 1988;150:71-74.
11 Poe RH, Kalay MC, Wicks CM et al. Predicting risk of pneumothorax in needle biopsy of the lung. Chest 1984;85:232-235.
12 Sider L, Davis TM. Hilar masses: evaluation with CT-guided biopsy after negative bronchoscopic examination, Radiology 1987;164:107- 109.
13 Kazerooni EA, Lim FT, Mikhail A et al. Risk of pneumothorax in CT- guided transthoracic needle aspiration biopsy of the lung. Radiology 1996;198:371-375.
14 Vitulo P, Dore R, Cervefi I etal. The role of functional respiratory tests in predicting pneumothorax during lung needle biopsy. Chest 1996;109:612-615.
15 Morrissey B, Adams H, Gibbs AR et al. Percutaneous needle biopsy of the mediastinum: review of 94 procedures. Thorax 1993;48:632-637.
�9 1998 The Royai College of Radiologists, Clinical Radiology, 53, 116-1 t9.