
Transport stakeholder meeting
53
Transport and Health JSNA Stakeholder workshop Angelique Mavrodaris Emmeline Watkins Iain Green Public Health 19/11/2014
-
Upload
cambridgeshireinsight -
Category
Health & Medicine
-
view
517 -
download
0
Transcript of Transport stakeholder meeting
Transport and Health JSNAStakeholder workshopAngelique MavrodarisEmmeline WatkinsIain Green
Public Health
19/11/2014

WELCOME AND INTRODUCTIONS
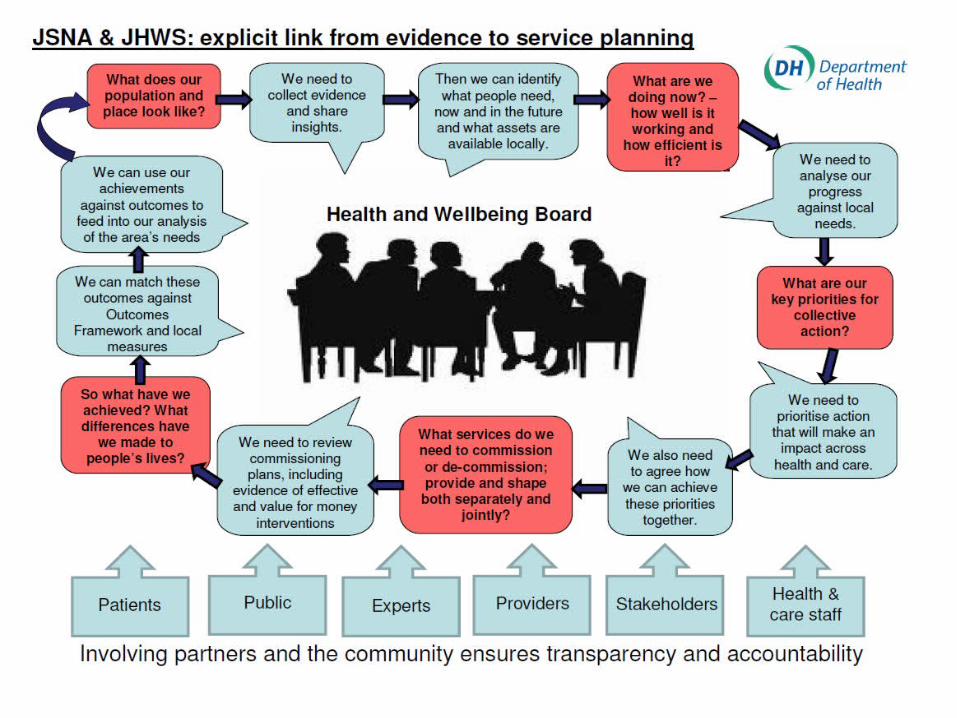
WHAT IS A JSNA?

Joint Strategic Needs Assessment (JSNA)
Commissioners & LA jointly describe health, care & wellbeing needs & service delivery
Focus on:• Outcomes• Partnership working• Consultation
Drives commissioning process
The Local Government and Public Involvement in Health Act (2007) required upper tier LA’s to produce a JSNA’s - Health & Social Care Act 2012 gave this duty to Health & Wellbeing Boards, with an additional statutory duty to prepare a joint health & wellbeing strategy to identify the needs identified in the JSNA
Statutory Background
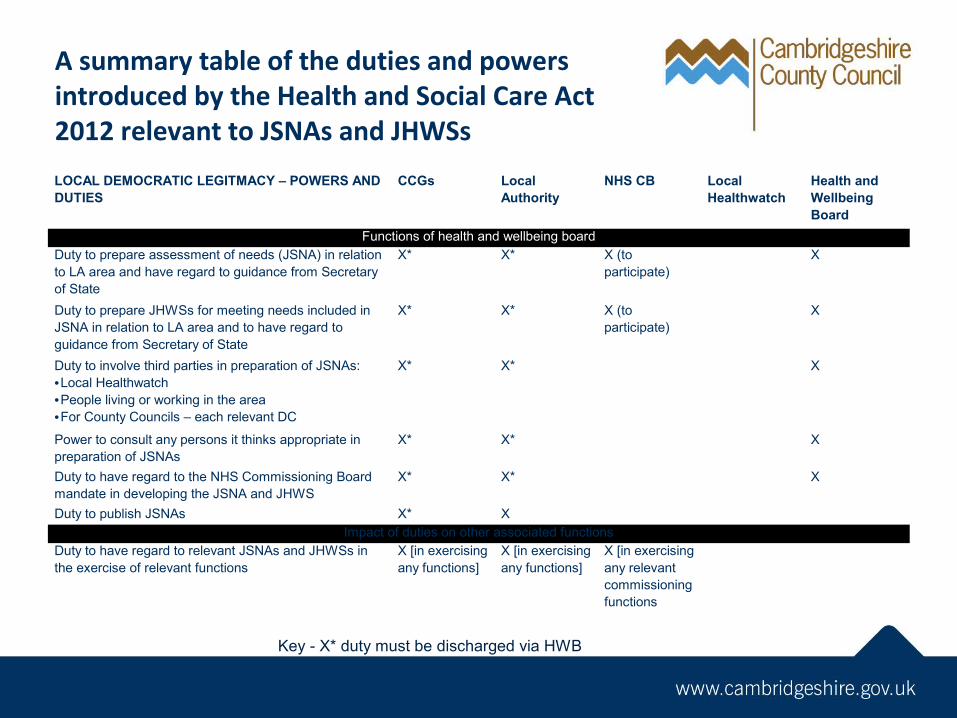
A summary table of the duties and powers introduced by the Health and Social Care Act 2012 relevant to JSNAs and JHWSs
Key - X* duty must be discharged via HWB
LOCAL DEMOCRATIC LEGITMACY – POWERS AND DUTIES
CCGs Local Authority
NHS CB Local Healthwatch
Health and Wellbeing Board
Functions of health and wellbeing boardDuty to prepare assessment of needs (JSNA) in relation to LA area and have regard to guidance from Secretary of State
X* X* X (to participate)
X
Duty to prepare JHWSs for meeting needs included in JSNA in relation to LA area and to have regard to guidance from Secretary of State
X* X* X (to participate)
X
Duty to involve third parties in preparation of JSNAs:•Local Healthwatch•People living or working in the area•For County Councils – each relevant DC
X* X* X
Power to consult any persons it thinks appropriate in preparation of JSNAs
X* X* X
Duty to have regard to the NHS Commissioning Board mandate in developing the JSNA and JHWS
X* X* X
Duty to publish JSNAs X* X Impact of duties on other associated functions
Duty to have regard to relevant JSNAs and JHWSs in the exercise of relevant functions
X [in exercising any functions]
X [in exercising any functions]
X [in exercising any relevant commissioning functions
JSNA ImpactProvide clearer idea of what is neededDeliver what people wantEvidence decisions – enable
stakeholders to but into changeIdentify best interventionsEnsure range of interventions available &
accessibleInform more effective & economic
configuration of services
BACKGROUND AND AIMS OF TRANSPORT AND HEALTH JSNA
Background and context
The purpose of this JSNA is to support HWB Priority 5, focus areas 1&3: Create a sustainable environment in which communities can flourish:
Develop and maintain effective, accessible and affordable transport links and networks, within and between communities, which ensure access to services and amenities and reduce road traffic accidents;
Encourage the use of green open spaces including public rights of way, and activities such as walking and cycling’.
The JSNA will also gather information on long distance transport to specialist hospital services
Linking to other counties (e.g. NCC) and PHE to ensure a regional approach where appropriate
Transport and Health JSNA priority areasAccess and health: An evaluation of transport and
social/geographical isolation in Cambridgeshire and the impact on health; directly or due to barriers in accessing specialist and every day care.
Active transport: Evaluation of transport strategies and initiatives that promote physical activity such as utilitarian walking and cycling and impact on health
Air pollution: An evaluation of Cambridgeshire air quality, hot spots and their impact on long-term conditions such as asthma and COPD and their life course
For each topic
Evidence review Assessment of local status and need
Local access and transport data Overlaid with information on health,
deprivation and demand
Identification of inequalities, gaps and opportunities
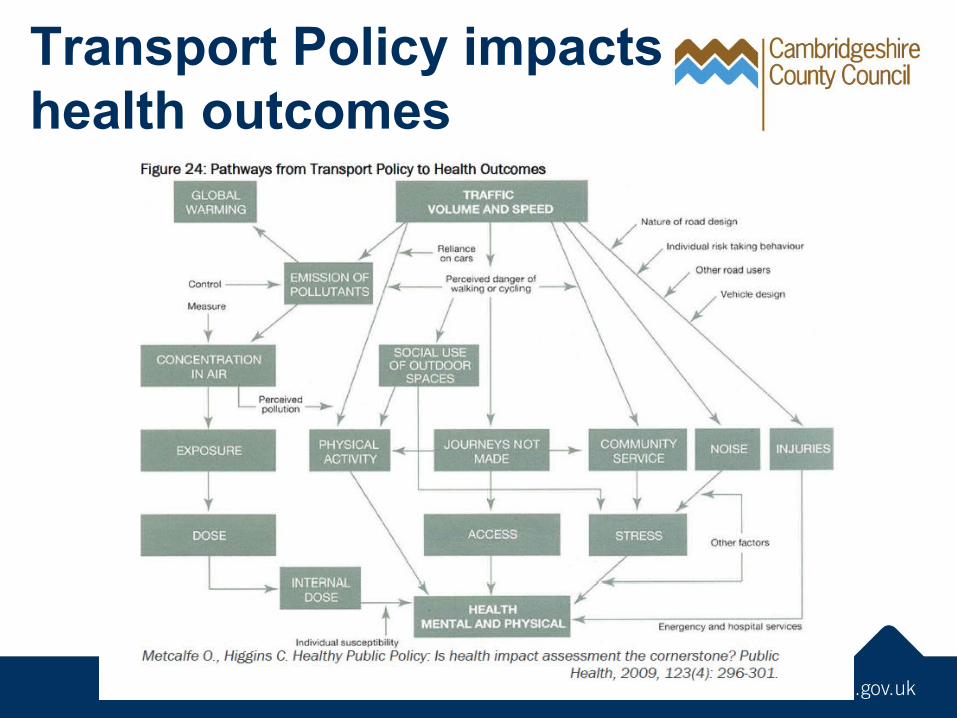
Transport Policy impacts health outcomes
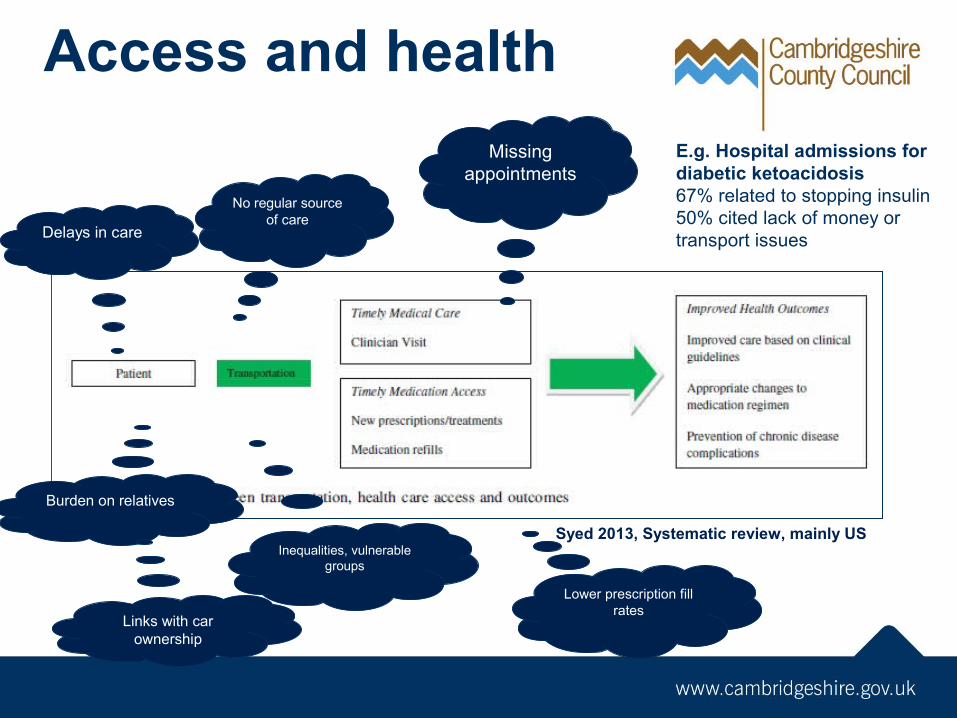
Syed 2013, Systematic review, mainly US
Missing appointments
Delays in care
Burden on relatives
No regular source of care
Links with car ownership
Inequalities, vulnerable groups
Lower prescription fill rates
E.g. Hospital admissions for diabetic ketoacidosis 67% related to stopping insulin50% cited lack of money or transport issues
Access and health
What can we find out locally? Access issues
Availability, eligibility, awareness, use of various transport types Travel time to key health services in rural and urban areas in
Cambridgeshire
Impact of current transport arrangements on patient and carer quality of life
Assessment of need for long-distance transport
What the JSNA adds: Transport data will be overlaid with potential impact on health E.g. mapping of health demand, vulnerable groups, inequalities, high
disease prevalence areas with access issues
Active transport and health NICE local government briefing: walking and cycling (Jan
2013) ensuring there is a network of paths for walking and cycling between places
locally reducing road danger and perception of danger ensuring local strategy, policy and planning support walking and
cycling using local data, communication and evaluation to develop
programmes including practical support, information about options focus on key settings recognising the health benefits
Models to show health impact of walking/cycling initiatives
What can we find out locally? Assessment of current active transport in
Cambridgeshire Rates of walking and cycling
Identification of local gaps, inequalities and opportunities
RTAs covered by C&P Road Safety Partnership Potential for building on this by analysis of
Vulnerable users e.g. pedestrian, >75 years Slight injuries
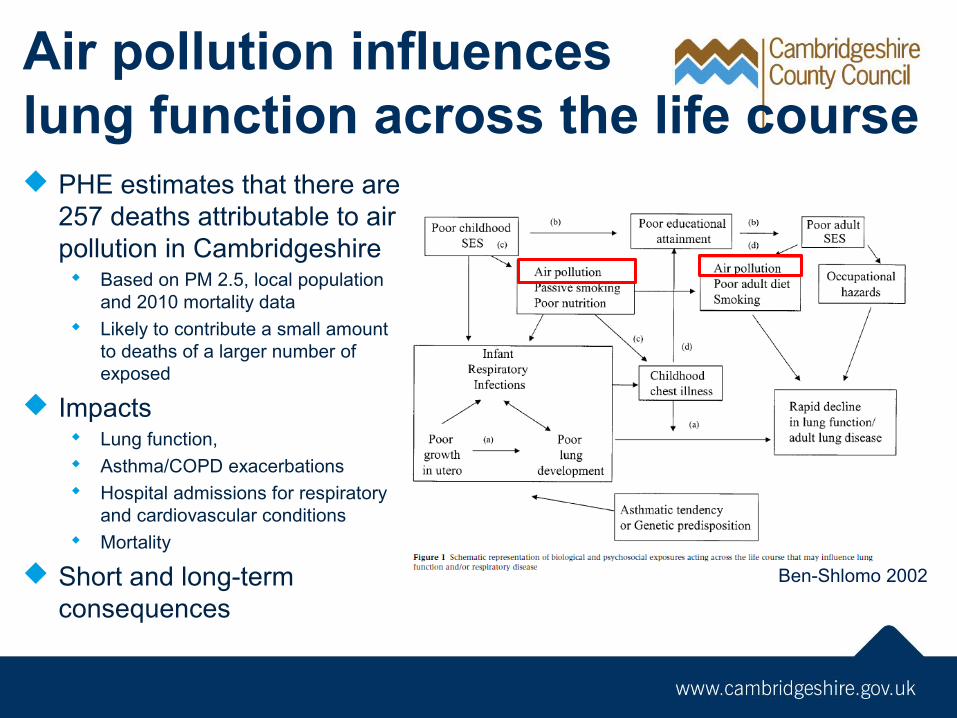
Air pollution influenceslung function across the life course PHE estimates that there are
257 deaths attributable to air pollution in Cambridgeshire Based on PM 2.5, local population
and 2010 mortality data Likely to contribute a small amount
to deaths of a larger number of exposed
Impacts Lung function, Asthma/COPD exacerbations Hospital admissions for respiratory
and cardiovascular conditions Mortality
Short and long-term consequences
Ben-Shlomo 2002
What can we find out locally?Assessment of current and future hot spots in
Cambridgeshire and their potential health impact on nearby development New growth Road changes Timeline for Air Quality Strategy for City, South and Hunts has
been delayed to allow for JSNA evidence
Identification of vulnerable groups and potential health impact
WHERE COULD YOU USE HEALTH DATA?
Where could you use transport and health data?
Create a timeline showing activities in the next 2 years where you could use transport and health evidence What sort of information would be useful? What are the deadlines for this work?
Flip charts and post-its available for timelines
Feedback on timelines
TRANSPORT, ISOLATION AND HEALTH
Wendy Otter
Fenland District Council
Overview – Fenland District
• Around 20,000 people live in villages or more sparsely populated areas in Fenland
• 22% of residents are of retirement age, higher than the national average
• Around 20% of households within the district do not own a car
• Public transport availability varies across Fenland but for many of our smaller communities is limited.
Transport & Health Issues• People can’t get to medical appointments,
especially hospital appointments. • Cost of transport• Reliance on family and friends• Older people often have more complex health
needs but also complex travel needs • A lack of transport Information• A lack of useable transport information• Health problems can often be sudden - A change
in circumstances for transport
Addressing the Barriers 1How did we set about addressing the transport and health issues in Fenland & Why? •Evidence:
– to address a situation you have to fully understand what the problem actually is
– Mapping – addresses of concessionary fare pass holders, bus stops and bus routes, and locations no more than 400metres from a bus stop
– 2011 research to understand the access to healthcare needs of patients in Fenland
– 2013 Audits of car and cycle parking. Assessment of surgeries in relation to bus stops & services
Addressing the Barriers 2• Stakeholders – Understanding who needed to be
involved. Working with colleagues to build relationships with our GP surgeries and the 2 community hospitals. Just under 1500 questionnaires were returned in 2011
• A lack of transport Information – Where do I find out about transport?
• A lack of useable transport information – new ways to present information:– Fenland Transport Directory– Getting from A to B Case Studies
Addressing the Barriers 3• Making information available - Where do people go to access information? - Different people access information in different ways - Information therefore has to be available in many ways
Current Issues
• Early and late appointments are an issue due to a lack of public and community transport
• Hospital appointments especially those further away from Fenland e.g. Cambridge & Norwich
• Eligibility for NHS Patient Transport – many people are no longer able to access patient transport
• Affordability• Opportunities to link NHS transport and public transport
• Any Questions?
Transport, isolation and health
What are the key transport barriers to accessing services from your viewpoint?
How do these impact on health?
Post-its and flip charts provided
Prioritise
Have a look at the issues/barriers that all tables have identified
Which are the most important issues You have 5 sticky dots to put against topics
you feel are most important Distribute, or put all dots on one topic…
TEA!
Feedback on access
Solutions
Each table has been given a key barrier to accessing services How could this be addressed? What works/doesn’t work
Post-its and flip charts provided
Feedback on solutions
ACTIVE TRANSPORT
Dr Jenna Panter
Centre for Diet and Activity Research
CEDAR
Ongoing initiatives in Cambridgeshire List active transport initiatives in
Cambridgeshire Focus on utilitarian active transport (Leisure walking/cycling initiative is being
captured through Naturally Healthy)
Please indicate if there is data available
Several A3 tables available per group
Active transport initiativesName of initiative
Cycling/walking
Area covered
Date launched
Data available
Contact
What works?
Why have initiatives been successful? What have been the barriers? Has health impact been included in
evaluation?
Post-its and flip charts provided
Feedback
AIR POLLUTION

Marcus Bell
Cambridgeshire Pollution Prevention Group
Local Air Quality Management - LAQM
The Environment Act 1995 sets out a framework for LAQM.
This requires every local authority to systematically review the air quality within their boundaries against a set of air quality objectives.
LAQM sets out a reporting structure in the form of annual review and assessment, where councils must assess the likelihood of achieving the air
quality objectives for key pollutants.
The EC has formally launched infraction proceedings against the UK for
breach of the nitrogen dioxide air quality limit values under
The Government powers under the Localism Act 2011 to transfer this fine
on to Local Authorities that have failed to carry out responsibilities under LAQM.
LAQM annual review and assessment• A staged investigation into pollutant levels with progressively more
in-depth study depending on the likelihood of exceeding the specified objective for any given pollutant.
• The first round of review and assessment began in 1998 with each round taking around three years. The first stage is to undertake an updating and screening assessment (USA) to identify any changes since the previous round which may lead to the exceedence of the air quality objectives (AQOs) .
• If the USA highlights that an exceedance is likely then a detailed assessment of the pollutants and locations of concern is necessary. The aim of the detailed assessment is to determine the magnitude and extent of any likely exceedences of the AQOs. If the USA indicates that all AQOs will be met then the local authority simply proceeds to a progress report.
• District Councils operate networks of non continuous monitors (such as diffusion tubes ) as well as continuous monitors, checking concentrations of pollutants 24hrs day.
Air Quality Management Areas (AQMA)
• Where an AQO is unlikely to be met the local authority must designate an air quality management area (AQMA) and draw up an air quality action plan setting out measures to be introduced in pursuit of the air quality objectives.
• Following declaration of an AQMA, a further assessment needs to be carried out to confirm that the AQMA declaration is justified, that the appropriate area has been declared, to ascertain the sources contributing to the exceedence and to calculate the magnitude of reduction in emissions required to achieve the objective. This information can be used to inform an Air Quality Action Plan, which will identify measures to improve local air quality.
• Some local authorities develop regional AQAPs. Defra have endorsed preparation of a Joint Air Quality Action Plan for the AQMAs within Cambridge City, Huntingdonshire District Council and South Cambridgeshire District Council. There are no AQMAs in East Cambridgeshire but the Station Road area is being looked at and will be affected by Southern Bypass.
• Over 220 local authorities have declared AQMAs, mainly for exceedences of the annual average objective for nitrogen dioxide and also, to a lesser degree, the short term objective for PM10. Road transport sources are the main cause of AQMA declarations.
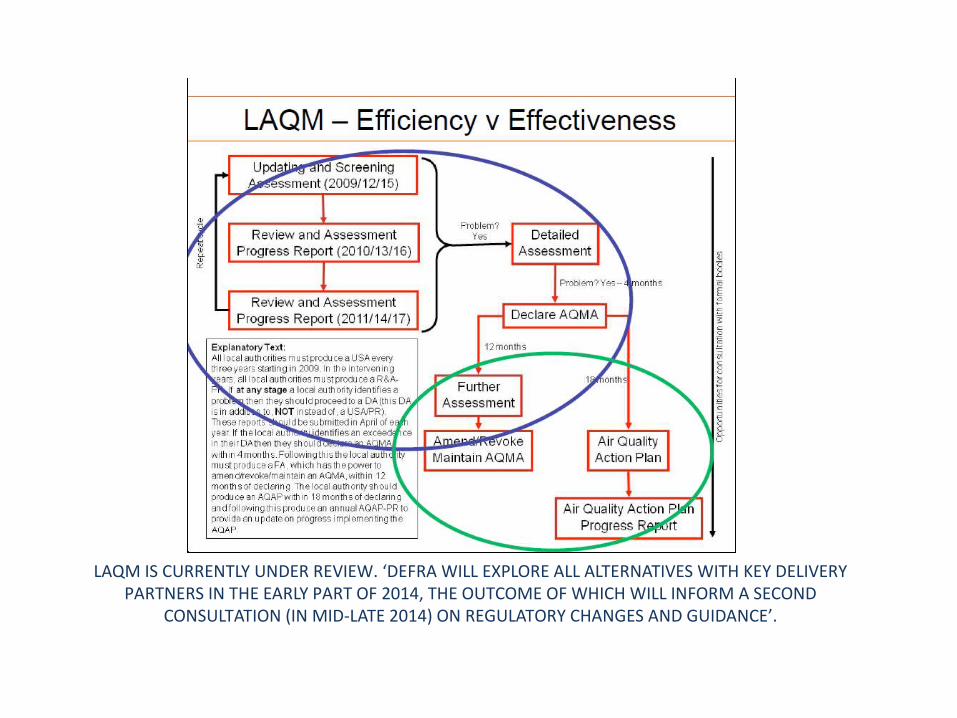
LAQM IS CURRENTLY UNDER REVIEW. ‘DEFRA WILL EXPLORE ALL ALTERNATIVES WITH KEY DELIVERY PARTNERS IN THE EARLY PART OF 2014, THE OUTCOME OF WHICH WILL INFORM A SECOND
CONSULTATION (IN MID-LATE 2014) ON REGULATORY CHANGES AND GUIDANCE’.
Local air pollution issues
What are the key local issues around air quality?
How can this be addressed through transport and planning?
What health data is needed to help drive this?
Flip charts and post-its available
Feedback
Next steps – producing the JSNA togetherSpecific Working Groups
Data and modelling Accessibility Active Transport Air pollution
Evidence review/data analysis work streams November-February 2015
Additional stakeholder meetings in 1Q 2015JSNA to Health and Wellbeing Board in April 2015