Transport in Humans. Blood vessels Cross section of an artery Structure vs function.
55
Transport in Humans
-
Upload
brett-wilcox -
Category
Documents
-
view
221 -
download
3
Transcript of Transport in Humans. Blood vessels Cross section of an artery Structure vs function.

Transport in Humans

Blood vessels

Cross section of an artery
Structure vs function

Cross section of a vein
• Structure vs function

Cross section of a capillary
• Structure vs function



Red Blood Cells (erythrocytes)
Bi-concave shape increases surface area and keeps the haemoglobin as close as possible to the membrane
Shape makes them flexible to squeeze along capillaries.
No nucleus or mitochondria, so more room for haemoglobin.
Cannot reproduce, and die after 3 months, so are manufactured in liver, spleen and bone marrow.
White Blood Cells (Leucocytes)Generally larger that erythrocytes, and have a nucleus. Despite having a nucleus, they are short lived (a few days) and are reproduced in the bone marrow.
Are capable of amoeboid movement, so they can squeeze through pores in capillary walls to reach tissues and sites of infection.
Visible when stained, using a light microscope, and fall into two groups.
Granulocytes (having granules in the cytoplasm) and are polymorphonuclear * (?)
Agranulocytes (no visible granules) and are mononuclear, ** (?)
* Looking as though they have more than one nucleus
** Having one definite nucleus

GRANULOCYTES
Neutrophils
70% of all white blood cells.
They squeeze between cells in the capillary wall, and wander through the intercellular spaces.
The move to infection sites in the body, where they engulf and digest disease causing bacteria. (they are phagocytic)

GRANULOCYTES
Eosinophils.
They represent 1.5% of all white blood cells, and get their name from their granules that turn red when stained by Eosine dye
They increase in number in allergic conditions such as asthma or hayfever, and they possess anti-histamine properties.
Their numbers are controlled by stress of various kinds (ie the result of an asthma attack)

GRANULOCYTES
Basophils
They represent 0.5% of all white blood cells andtheir granules stain blue with dyes such as methylene blue.
The cells produce histamine, a chemical found in damaged tissues. Histamine stimulates repair of damaged tissues, so is important, but over production can occur in allergic reactions (and so needs to be controlled)
AGRANULOCYTES
Monocytes
They are formed in the bone marrow, and have a bean shaped nucleus.
They only last 30 hours or so in the blood, after which they leave the capillaries and enter the tissues.
Here they become Macrophages

AGRANULOCYTES
Macrophages
These are phagocytic, and engulf bacteria and other large particles, such as damaged tissue.
They are also involved in the immune system (to be covered later)
Macrophages and Neutrophils (discussed earlier) both act as a first line of defence against bacteria.

LYMPHOCYTES
These make up 24% of all white blood cells, and develop from cells that originate in the bone marrow (although the lymphocytes themselves develop in a gland called the Thymus, and also in lymph tissue (to be discussed later).
There are two types of Lymphocyte, T Cells and B cells that are involved in immune reactions, such as antibody production, graft rejection and killing tumour cells.
Their lifespan ranges from a few days to 10 years or more.

Summary: Create a chart showing the name, function of the cell, and a picture of it
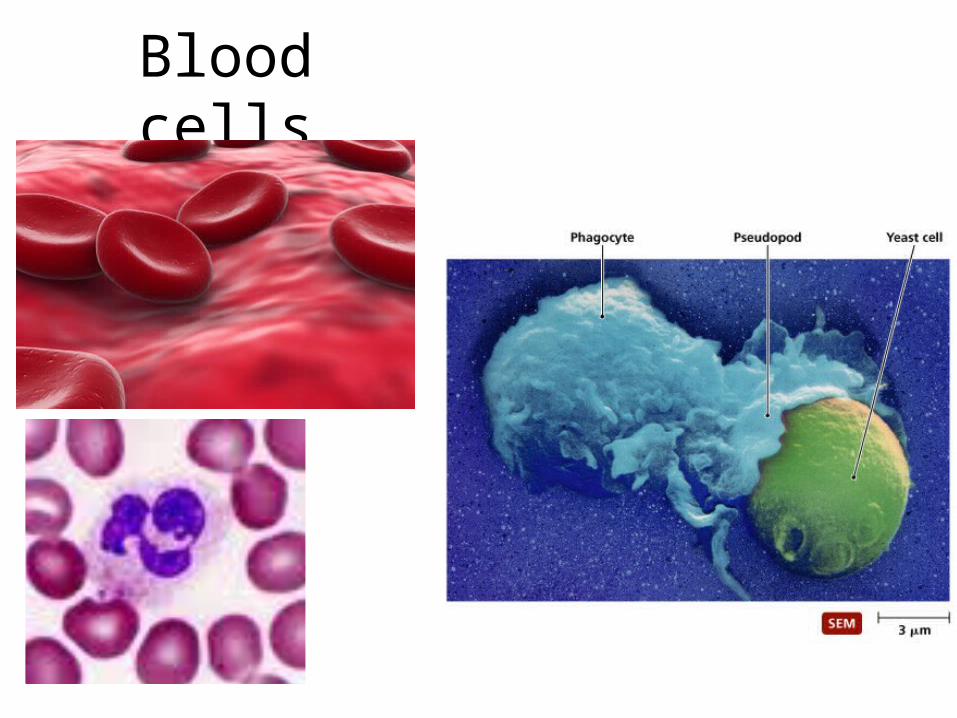
Blood cells
BLOOD PLASMA
This is the fluid that the cells are surrounded by. It contains
Nutrients
Waste Products,
Plasma Proteins

Tissue fluid
• Cells are bathed in tissue fluid• Source of nutrients and oxygen
• Blood at the arterial end is under high pressure which forces water and small molecules out into interstitial spaces (ultrafiltration)
• Proteins are too big to move so they create an osmotic effect which keeps some fluid in the capillary.
• The pressure at the venous end is low so water, waste and carbon dioxide move back in to the capillary.


Lymphatic system
• Not all tissue fluid circulates back into the capillary
• Some drains into the lymphatic system
• Similar in composition to tissue fluid but has more fatty substances
• Works in defence system as well.


Body Fluids: A Comparison

The relationship between Blood, Tissue Fluid and Lymph

Haemoglobin (recap)
It is made up of 4 polypeptide chains (Quaternary structure)Each chain is a globin molecule, and there are 2 chains of alpha-globin, and 2 chains of beta-globin.Molecule is nearly spherical.Hydrophobic R-groups point inwards, and hydrophilic R groups point outwards making it soluble.

Haemoglobin (recap)Interactions of the hydrophobic R groups help hold the molecule into it’s 3-dimentional shape.In Sickle cell anaemia, a glutamic acid molecule (an amino-acid) near the surface of a globin molecule is replaced by valine, which has a hydrophobic R group.The hydrophobic R group makes the whole molecule less soluble and prevents it functioning correctly.

Haemoglobin (recap)Each polypeptide chain contains a haem group.Haem is not made of amino acids, and is called a prosthetic group.Each haem group contains an iron atom, which can bind with an oxygen molecule, 02
Each haemoglobin molecule can therefore carry 8 atoms of oxygen.

Oxygen dissociation curve
• Degree of oxygenation of haemoglobin is determined by the partial pressure of oxygen in the immediate surroundings.
• Partial pressure of a gas is the pressure exerted by that gas in a volume of air.
• At sea level the total atmospheric pressure is 101.3kPa.
• Atmosphere has 21% oxygen so the partial pressure of oxygen is 21% of 101.3kPa, or 21.3kPa.

The curve shows how much haemoglobin is saturated by oxygen at different partial pressures of oxygen

• Note that the curve is sigmoidal because• There is high affinity by each haem group and
oxygen at high partial pressures.• This means that in the lung tissue, where
there is a lot of oxygen, it quickly combines with the haemoglobin

• There is low affinity between each haem group and oxygen at low partial pressures.
• This means that in muscle tissue, where the body needs the haemoglobin to give up its oxygen it will do so easily.

Carbon dioxide
• 5% carbon dioxide is transported in solution
• 10% combines with some of the amino acids in haemoglobin to form carbaminohaemoglobin.
• 85% carried as hydrogencarbonate ions.

• CO2 diffuses into red blood cells and it is changed into carbonic acid by an enzyme called carbonic anyhydrase
• Carbonic acid dissociates to form H+ and hydrogen-carbonate ions.
Write the formulae for these two reactions on p110 of your textbook.

• HCO3- (hydrogencarbonate) ions can
diffuse out of the cell and are then transported in the plasma.
• Chloride ions move in to the red blood cell from the plasma, to maintain electrical neutrality by replacing the hydrogen-carbonate irons that have moved out.
• This is referred to as the Chloride Shift.

• H+ are taken up by the haemoglobin to form haemoglobinic acid (HHb)
• Haemoglobin is therefore acting as a buffer to keep blood from being too acidic by preventing a build-up of H+ ions.
• This also forces haemoglobin to release their oxygen molecules,

Summary of whole process

Bohr Effect
• Oxygen dissociation curve is shifted to the right due to the presence of CO2
• CO2 reduces the affinity of haemoglobin for oxygen
• This means the more CO2 there is, the more O2 is released from the Haemoglobin

Graph:(a) The partial pressure of oxygen in the tissue
(b) At Pco2 = 3kPa Hb has 50% unloaded its oxygen.
(c) At Pco2= 4kPa Hb has approx 80% unloaded its oxygen.
(d) At Pco2= 6kPa Hb has approx 90 % unloaded its oxygen.
Explained in more detail………..

• Adaptations to altitude:
• Prolonged time at altitude results in the following adaptations for the individual
1) Increased vascularisation of the muscle
2) Increases in the concentration of myoglobin (single chain globular protein containing haem, found in muscles)
3) Increased red cell number in blood

Red blood cell count at high altitude
• At high altitudes there is lower atmospheric pressure of oxygen.
• The current number of red blood cells in the body cannot meet the cells demands for oxygen.
• Polycythemia occurs, which is an increase in the bodies red blood cell count.
• It means there is more haemoglobin available to bond with oxygen molecules meaning more oxygen can be transported to the cells in the body, therefore helping to meet the oxygen demands of the body even with less oxygen in the air.

4) Greater number of mitochondria per muscle cell
5) Increases in the concentration of respiratory enzymes
6) Improved buffering of pH and utilisation of lactate ions, (the product of anaerobic respiration). This is called lactate clearance.
More adaptations to altitude:

• An interesting observation in sports medicine has been the realisation that athletes do not need to train at altitude to achieve these effects.
• Rather the key is to recover at altitude which means recovering and sleeping either at altitude or in a hypobaric chamber which can simulate high altitude. It is during recovery that the body adapts to the stresses of exercise and under high altitude recovery conditions it they recover with the above list of 6 adaptations.

The Heart

The heart
Closed, double circulation


Thickness of the walls is related to their functions

The cardiac cycle

Atrial systole
• atrium contracts• blood flows from
atrium to the ventricle

Ventricular Systole
• Ventricles contract• Atrioventricular
valves close• Semi lunar valves
open

Diastole
• whole heart is relaxed

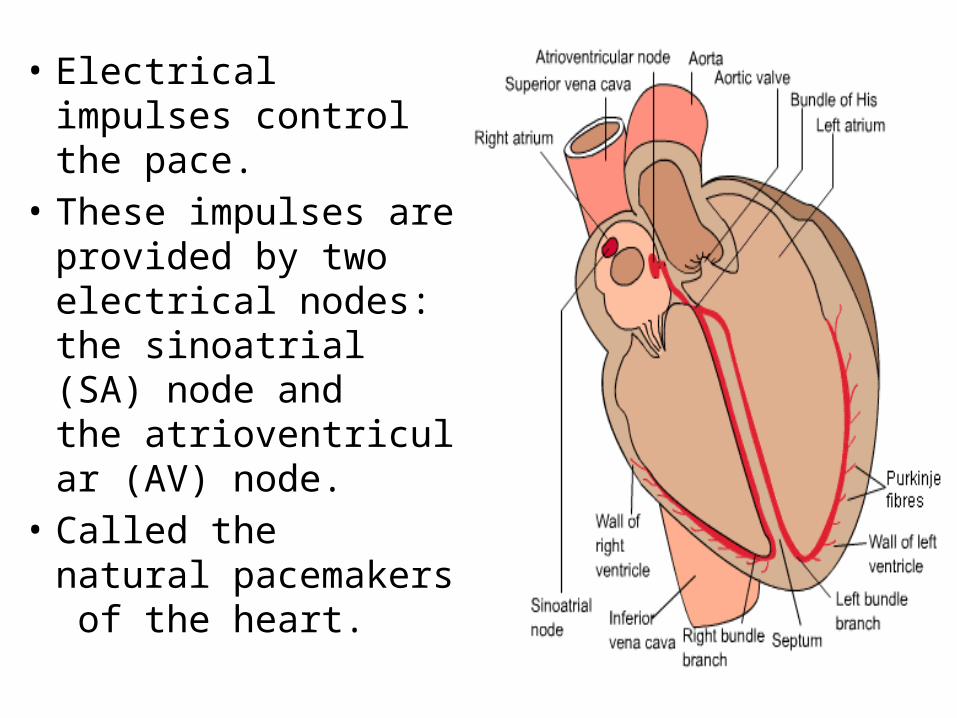
• Electrical impulses control the pace.
• These impulses are provided by two electrical nodes: the sinoatrial (SA) node and the atrioventricular (AV) node.
• Called the natural pacemakers of the heart.

Diastoleno electrical activity during this phase
Atrial SystoleSinoatrial node fires an electrical impulse ,it spreads throughout the right and left atria, causing the muscle to contract and push blood into the ventricles. Towards the end of the atrial systole the electrical impulse reaches and triggers the atrioventricular node.

• Ventricular Systole• The atrioventricular node (after a short delay)
fires an impulse, • it spreads throughout the thick ventricular
muscle, • causing contraction from the bottom of the
ventricles,• pushing blood through the lungs and body.