Transoral resection of supraglottic tumours using microelectrodes (54 cases)
6
1 3 Eur Arch Otorhinolaryngol (2014) 271:2497–2502 DOI 10.1007/s00405-014-3002-x LARYNGOLOGY Transoral resection of supraglottic tumours using microelectrodes (54 cases) Jorge Basterra · Francisco Esteban · Rosa Reboll · Alicia Menoyo · Enrique Zapater Received: 23 December 2013 / Accepted: 4 March 2014 / Published online: 3 April 2014 © Springer-Verlag Berlin Heidelberg 2014 approach using microelectrodes (MEs), so far this is the largest published series of supraglottic tumours operated using this method. From 1989 to 2004, the senior author has used the CO 2 laser transoral technique to resect supra- glottic tumours, being replaced in 2004 by microelectrodes. The basic general principle of this technique is to achieve tissue resections by using MEs (designed by the first author), connected to an electric scalped hand piece and an electro or radiofrequency generator (see “Methods”). The first comparison study of the CO 2 laser and MEs was published by the authors in 2006 [1, 2]. Histopathol- ogy (acute and chronic tissue damage) showed similar results for the CO 2 laser and MEs [3, 4]. Since 2004, sev- eral changes have been introduced in the ME device but the principles of the surgical technique remain the same [5, 6]. In 2006, to evaluate the results of supraglottic surgery using MEs, we designed a prospective multicentre study of patients with supraglottic carcinoma reported from two ENT clinics. The aim of this paper is to present the results of using MEs in supraglottic tumours. Methods The ENT departments are part of academic tertiary referral hospitals with ample experience in oncological head and neck surgery with a population area of 750,000. In our departments, since 2005 (during 2004 only glottic tumours were operated on using MEs technique), transoral resection with ME has been considered the surgical stand- ard treatment for patients with T1, T2, and selected cases of T3 supraglottic carcinomas, with preservation of vocal cord motility, good visual control of the tumour, and extension within the pre-epiglottic space. Abstract We present the oncological and functional results of surgical transoral resection of supraglottic laryngeal car- cinomas using microelectrodes. This prospective multicen- tre trial was conducted from 2005 to 2009. It included 54 patients (23 T1, 14 T2, and 17 T3) with supraglottic cancer, with a follow-up of 2 years. Outcome measurements were: tracheostomy, hospital stay, nasogastric feeding and recur- rences. Four patients required permanent tracheostomies. The mean hospital stay was 8.1 days. Temporary nasogastric feeding was necessary in 13 patients. Postoperative compli- cations included two incidences of haemorrhage requiring surgical intervention and one pneumonia. Four patients out of eight with T3 tumours had regional recurrence; in these cases salvage surgery was performed: two cases by the transoral approach and six total laryngectomies. Clinical results were similar to those obtained with CO 2 laser therapy. We list other advantages of the technique and include a literature review. Keywords Larynx · Cancer · Microelectrodes · Transoral surgery · CO 2 laser Introduction Herein, we present the oncological and functional results of 54 cases of supraglottic tumours transected via a transoral J. Basterra (*) · R. Reboll · E. Zapater ENT Unit, Surgical Department, Valencia Medical School, University of Valencia, University General Hospital, Valencia, Spain e-mail: [email protected] F. Esteban · A. Menoyo ENT Department, Sevilla Medical School, Hospital Virgen del Rocío, University of Sevilla, Sevilla, Spain
-
Upload
francisco-esteban -
Category
Documents
-
view
212 -
download
0
Transcript of Transoral resection of supraglottic tumours using microelectrodes (54 cases)

1 3
Eur Arch Otorhinolaryngol (2014) 271:2497–2502DOI 10.1007/s00405-014-3002-x
LAryngOLOgy
Transoral resection of supraglottic tumours using microelectrodes (54 cases)
Jorge Basterra · Francisco Esteban · Rosa Reboll · Alicia Menoyo · Enrique Zapater
received: 23 December 2013 / Accepted: 4 March 2014 / Published online: 3 April 2014 © Springer-Verlag Berlin Heidelberg 2014
approach using microelectrodes (MEs), so far this is the largest published series of supraglottic tumours operated using this method. From 1989 to 2004, the senior author has used the CO2 laser transoral technique to resect supra-glottic tumours, being replaced in 2004 by microelectrodes. The basic general principle of this technique is to achieve tissue resections by using MEs (designed by the first author), connected to an electric scalped hand piece and an electro or radiofrequency generator (see “Methods”).
The first comparison study of the CO2 laser and MEs was published by the authors in 2006 [1, 2]. Histopathol-ogy (acute and chronic tissue damage) showed similar results for the CO2 laser and MEs [3, 4]. Since 2004, sev-eral changes have been introduced in the ME device but the principles of the surgical technique remain the same [5, 6].
In 2006, to evaluate the results of supraglottic surgery using MEs, we designed a prospective multicentre study of patients with supraglottic carcinoma reported from two EnT clinics. The aim of this paper is to present the results of using MEs in supraglottic tumours.
Methods
The EnT departments are part of academic tertiary referral hospitals with ample experience in oncological head and neck surgery with a population area of 750,000.
In our departments, since 2005 (during 2004 only glottic tumours were operated on using MEs technique), transoral resection with ME has been considered the surgical stand-ard treatment for patients with T1, T2, and selected cases of T3 supraglottic carcinomas, with preservation of vocal cord motility, good visual control of the tumour, and extension within the pre-epiglottic space.
Abstract We present the oncological and functional results of surgical transoral resection of supraglottic laryngeal car-cinomas using microelectrodes. This prospective multicen-tre trial was conducted from 2005 to 2009. It included 54 patients (23 T1, 14 T2, and 17 T3) with supraglottic cancer, with a follow-up of 2 years. Outcome measurements were: tracheostomy, hospital stay, nasogastric feeding and recur-rences. Four patients required permanent tracheostomies. The mean hospital stay was 8.1 days. Temporary nasogastric feeding was necessary in 13 patients. Postoperative compli-cations included two incidences of haemorrhage requiring surgical intervention and one pneumonia. Four patients out of eight with T3 tumours had regional recurrence; in these cases salvage surgery was performed: two cases by the transoral approach and six total laryngectomies. Clinical results were similar to those obtained with CO2 laser therapy. We list other advantages of the technique and include a literature review.
Keywords Larynx · Cancer · Microelectrodes · Transoral surgery · CO2 laser
Introduction
Herein, we present the oncological and functional results of 54 cases of supraglottic tumours transected via a transoral
J. Basterra (*) · r. reboll · E. Zapater EnT Unit, Surgical Department, Valencia Medical School, University of Valencia, University general Hospital, Valencia, Spaine-mail: [email protected]
F. Esteban · A. Menoyo EnT Department, Sevilla Medical School, Hospital Virgen del rocío, University of Sevilla, Sevilla, Spain

2498 Eur Arch Otorhinolaryngol (2014) 271:2497–2502
1 3
We designed a database regarding oncologic and func-tional aspects; data were introduced prospectively and updated monthly and no new patients were accepted into the study after December 2009, for a minimum follow-up of 2 years.
The sample comprised 54 patients (17 T3, 14 T2 and 23 T1), 48 males (88.8 %) and six females (11.2 %). The mean age of the patients at the time of diagnosis was 66.3 years (range 49–85 years).
In the T3 cases that were unsuitable for a transoral approach (extension beyond condition previously indi-cated, or anatomic conditions complicating direct intuba-tion), an external procedure or conservation organ therapy was offered. Patients who had been transorally treated pal-liatively due to distant metastases or concomitant neoplasia were not included in our series. no age limit was imposed prior to surgery. Tumours were classified according to the 2002 TnM classification [7].
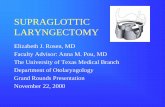
Ultrafine tungsten MEs (Sutter Medizintechnik gMBH, Freiburg, germany) were used for the resections (Fig. 1). Tissue resection was performed in the cutting or coagu-lation mode of the hand piece scalpel depending on the amount of bleeding. From 2005 to 2009 an electrogen-erator (Valleylab Force 2; Pfizer, germany) was used [6]; since 2009 a radiofrequency generator (Curis; Sut-ter Medizintechnik gMBH, Freiburg, germany) has been used. For more technical details see published data [6]. The highest power intensity level, 20 W, was used to resect cartilage, while the lowest (5–10 W) was used to section soft tissues. In all procedures, depending on the amount of bleeding, direct electrocoagulation with MEs or clamping of the vessels with microforceps and coagulation at 35 W was applied.
The numbers of patients with clinical nodes (c-n) were: 8 n2, 3 n1; 43 n0. Bilateral functional neck dissections were performed in the T2–T3 cases; prior to the tran-soral approach to the laryngeal tumour the superior laryn-geal vascular pedicle was ligated during the neck dissec-tion to achieve better haemostasis of the laryngeal field.
Tracheostomy was always performed in cases requiring bilateral neck dissections. In wide supraglottic resections, a nasogastric feeding tube was inserted to prevent aspiration.
Intraoperative frozen tissue sections of the tumour mar-gins were examined postoperatively by a pathologist and classified as affected or negative. Adjuvant postoperative radiotherapy was applied in cases of positive neck nodes and affected resection margins.
All patients were informed regarding the characteristics of the technique, and were made aware of alternative con-servative therapy options. The study design was approved by the Institutional review Boards of both institutions.
Data were analysed using SPSS for Windows, version 14.0. A p value of 0.05 was defined as statistically signifi-cant. The relationship between qualitative variables was analysed using Pearson’s Chi-square test. rates of overall survival, disease-specific survival, laryngectomy-free sur-vival and functional preservation were estimated using the Kaplan–Meier method. Overall survival time was deter-mined as the date of surgery to the date of death. Disease-specific survival was calculated taking into account deaths related to the tumour or complications of the treatment. The end point for larynx preservation was the date of total laryngectomy. The end point for function preservation was the date of total laryngectomy, permanent tracheotomy or requirement for a nasogastric feeding tube.
All patients were informed about the characteristics of the technique and alternative nonsurgical therapies. The study design was approved by the institutional review board at our institution.
Results
Cases were postoperatively staged as follows: 17 pT3, 14 pT2 and 23 pT1. The definitive pathology analysis of the surgical specimen margins was negative for neoplasia in 51 patients (94.4 % of margins were tumour-free) and positive in three cases (5.6 %), two of which were T3 and one was T1.
Fig. 1 a Detail of the tips terminal 3 × 0.3 mm; 90° and 180°. b Microelectrodes and hand piece radiofrequency scalpel

2499Eur Arch Otorhinolaryngol (2014) 271:2497–2502
1 3
Bilateral neck dissections were performed in 31 patients, all T2–T3; no unilateral neck dissections were performed. In 14 patients (25.9 %) adjuvant radiation therapy was indi-cated in the neck and in the primary tumour site.
Tracheostomy was performed in all patients who under-went bilateral neck dissection (31 patients, 57.4 %); four of these patients could not be decannulated postoperatively (7.4 %), due to actinic laryngeal stenosis after radiotherapy.
nasogastric feeding was necessary in 13 patients (24 %); 10 required it for 10 days postoperatively, one 68-year-old patient (T2) 35 days, and another for 90 days, due to chronic pneumonia. The remainder began per oral feeding on the first postoperative day.
Three patients had postoperative complications: two required surgical revision due to early postoperative haem-orrhage from the tumour site and one 68-year-old patient (T2) developed aspiration pneumonia.
The duration of hospital stay (HS) ranged from 1 to 90 days (median 8.1 days); 47 cases remained in the hospi-tal for less than 10 days, see Table 1; in six patients the HS ranged between 10–20 days.
Local recurrences were confirmed in eight patients dur-ing the follow-up period, all of them T3 tumours (14.8 %);
in addition, four patients developed a regional recurrence (three T3n2 and one T1n0), three of whom had also developed a local recurrence. In all cases, laryngeal sal-vage surgeries were performed: two received the transoral approach, and six received total laryngectomies.
Secondary laryngeal tumours developed in six cases: three in the vocal cords (two T1 and one T2), two in the false vocal cord (both T2), and one in the subglottis (T3); five of these patients were treated by transoral surgery, and the patient with the T3 subglottic tumour was treated by total laryngectomy.
In our series, three patients died due to laryngeal carcinoma.
Statistical analysis
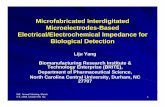
The Kaplan–Meier 5-year overall and disease-specific sur-vival rates were 64.8 and 75.9 %, respectively (Fig. 2).
In the univariate analysis, survival was related to the sta-tus of the cT (p = 0.009), the c-n (p = 0.002), regional recurrences (p = 0.001), and local recurrences (p = 0.040). no significant differences in specific survival related to the local recurrences were found.
Table 1 recorded parameters of the 54 patients (six female and 48 male)
c-N clinical nodes, RT radiotherapy, QT chemotherapy, RT post postoperative radiotherapy
neck dissection 31 bilateral 0 unilateral 23 none
Tracheostomy 31 yes 10 none
none decannulated 4
c-n 1 n2b 7 n2 3 n1 43 n0
Margins 3 affect 51 none
Hospital stay (days) 47; <10 days 6; 10–20 days 1; >20 days
Complications 2 haemorrhage 1 pneumonia
nasogastric feeding 41 none 13 total 10; <10 days 1; 10–20 days 2; >10 days
rt/Qt 14 rt post
Follow-up (months) 16; <24 months 23; 24–60 months 15; >60 months
Local recurrence 8 yes (14,8 %) T1 0 casesT2 0 casesT3 8 cases
46 none
regional recurrence 4 yes 50 none
recurrence treatment 2 transoral surgery 6 total laryngectomy 4 neck dissection
Secondary laryngeal tumours 6 total 3 vocal cord2 false vocal cord1 subglottis
Secondary laryngeal tumour treatment 5 transoral surgery 1 total laryngectomy
Other tumour sites 4 total 1 lung1 uterus1 oesophagus1 rectum
Exitus 16 exitus 13 dead by other causes
Date of total laryngectomy 5; <24 months 2; >24 months
Survival time 9; <24 months 6; >24 months

2500 Eur Arch Otorhinolaryngol (2014) 271:2497–2502
1 3
Total laryngectomy was significantly related to neck dissection (p = 0.015), tracheotomy (p = 0.015), c-n (p = 0.003), stage T (p = 0.000), local recurrences (p = 0.000) and permanent tracheostomy (p = 0.000).
Discussion
Transoral surgeons generally agree that transoral surgery is indicated in supraglottic tumours staging T1 and T2. Most experienced surgeons using this approach also agree that T3 supraglottic tumours are resectable if the surgeon has a good visual control of the tumour on microlaryngoscopy, the larynx mobility is preserved, and the tumour is within the pre-epiglottic space limits.
Our oncological and functional results using MEs are similar to those reported by other authors using CO2 lasers (see ahead) and specifically regarding the recurrence rates and survival times, requirement for permanent tracheos-tomy, time of decannulation, necessity of nasogastric feed-ing, and neck dissection. Important points are discussed below.
recurrences and survival
recurrences after the transoral approach can be treated by the same procedure or by open surgery, depending on the size of the tumour and the surgical criteria. Agrawal [8] described only one patient with local disease recurrence that required total laryngectomy. Vilaseca [9] reported 37.5 % of local recurrences, which were treated by laser
surgery in five patients, partial external surgery in five, and total laryngectomy in 45. Their disease-specific sur-vival rate was 70.2 %, while that in the present study was 75.9 %. We reported a local recurrence rate of 14.8 % in eight patients with T3 tumours. An interesting fact is that no significant differences in specific survival were found according to local recurrences. In glottic tumours similar criteria are followed; Steiner performed six total laryngec-tomies in 21 patients with anterior commissure involve-ment, in contrast to one total laryngectomy in a patient without anterior commissure involvement [10].
Tracheostomy and decannulation
In our series, tracheostomy was performed in 31 patients (57.4 %) with bilateral neck dissections during this proce-dure. We understand that performing a supraglottic resec-tion plus bilateral neck dissection in the same procedure involves major surgical trauma, and no added risk is to be taken when avoiding performing a tracheostomy. In our opinion, it is more convenient to perform laryngeal plus neck dissection in one procedure and perform a tracheos-tomy, than to perform laryngeal and neck dissection in two procedures, avoiding the tracheostomy.
Motta et al. [11] reported that in their series tracheot-omy was performed in only 2.4 % of the patients. Cabanil-las [12] performed neck dissection about 15 days after the primary tumour was removed to minimise the risk of air-way swelling and to reduce the tracheotomy rate. He stud-ied 26 cases of supraglottic cancer treated with transoral oral surgery, three of whom (11.5 %) had tracheotomies
Fig. 2 a Disease-specific survival rates according to Kaplan–Meier analysis. b Overall survival rates according to Kaplan–Meier analysis

2501Eur Arch Otorhinolaryngol (2014) 271:2497–2502
1 3
perioperatively and one an emergency tracheotomy due to postsurgical bleeding. Two of the four tracheotomies were closed and the incidence of permanent tracheotomy was 8 %, similar to that of our patients (7.4 %). Agrawal [8] reviewed 34 cases of supraglottic cancer (T1–T2–n0–n1) that were treated with transoral supraglottic laryn-gectomy followed by postoperative radiotherapy, and only four patients underwent tracheostomy during the initial surgical procedure, all as a consequence of either obstruct-ing tumours or unfavourable anatomy that precluded safe intubation.
In our statistics most tracheostomies are removed early in the postoperative period and no permanent sequelae are reported; thus we do not consider tracheostomy to be a handicap but actually increases the safety, as endolaryngeal bleeding in transorally treated, non-tracheotomised patients is a serious and potentially lethal complication [13]. We treated postoperative haemorrhage in two patients, both of whom required surgical revision under general anaesthe-sia; the revision procedure and haemostasis were routine in both patients. Similar tracheostomy indications were fol-lowed by the senior author while performing transoral sur-gery using the CO2 laser before 2004.
Vilaseca et al. [9] reported an incidence of tumour site bleeding of 13.6 %, and one patient died of massive bleed-ing a few days after surgery.
In our study, the percentage of tracheostomies was higher than in other reports of use of the CO2 laser but this is unrelated to the ME technique, having arisen from the safety criteria. The percentage of permanent postopera-tive tracheostomies in our series (7.4 %) is similar to that reported by other authors using the CO2 laser.
Swallowing
The early postoperative swallowing capacity after tran-soral surgery is always better compared to the transcervical approach, leading to a reduced chance of aspiration. nev-ertheless, long-term results are similar whether transoral or open surgery is performed [8, 12]. In our sample, nasogas-tric feeding was necessary in 13 patients (24 %), most of whom required it for less than 10 days postoperatively, with only one patient needing it for 90 days due to chronic aspi-ration pneumonia. In Agrawal’s series, seven (7 %) subjects required prolonged use of feeding tubes (>15 days post-operatively). One of these patients required feeding tube reinsertion during radiotherapy 8 weeks after surgery and three patients (9 %) did not recover oral feeding [8]. Zei-tels [14] stated that with more extensive supraglottic resec-tions using CO2 laser, temporary aspiration for 1–6 weeks is often expected and preservation of the vestibular folds appears to shorten swallowing rehabilitation.
neck dissection
There is disagreement regarding the indications for uni-lateral or bilateral neck dissection for T2–T3 supraglottic tumours. We have performed bilateral neck dissections in all T2–T3 cases (31 patients, 57.4 %); according to the considerable number of occult metastasis found in cn0 reported by other authors. Vilaseca et al. [9] reviewed the outcomes of transoral laser microsurgery in 147 T3 laryn-geal carcinoma patients, in whom neck dissection was performed in 97 (66.4 %), 54 of these patients had patho-logically postoperative confirmed positive nodes. Even early supraglottic cancer is associated with a high rate of neck metastasis, from 25 to 50 %; and bilateral neck dissection in these patients is associated with reduced recurrence, although cn0 cases may be overtreated in 70–80 % of cases [13]. Motta et al. [11] reviewed the results of transoral laser surgery in 124 patients with T1, T2 and T3 supraglottic tumours. In their study, neck dis-section was performed in 10 cases, and 13 patients had metastatic lymphadenopathy at 1 year following the pri-mary operation (10.4 %). Zeitels et al. [14] also reported a high incidence of occult neck metastasis in T2 and T3 supraglottic cancer cases. For patients with n0 neck status (clinical and radiographic), Agrawal et al. [8] did not perform neck surgery but administered prophylactic radiotherapy.
Most authors have stated that bilateral neck dissection is an adequate therapy for primary cancer of the supraglottic larynx with n0 neck, and we must keep in mind that even T1 supraglottic cancer has a probability of cervical metas-tasis in the range 15–25 %.
Conclusions
To summarise, regarding functional and oncological evalu-ation, the results of ME are similar to those achieved using a CO2 laser.
In the authors’ experience, use of MEs has advan-tages over the CO2 laser such as: improved haemostasis, the angled tip of the ME which allows cutting at a direct angle, improved tactility through the ME, excellent visu-alisation with the high-intensity operating light of the microscope, simplicity of handling, and a significantly lower cost of the equipment. Also, the operating time is shorter (mean operating time: cordectomy 22 min, epi-glottectomy 17 min and supraglottic resection 85 min) due to the excellent cutting capacity of the ME’s tungsten sharp tip (3 × 0.3 mm) [5]. MEs are also more effective than a CO2 laser when sectioning cartilage and debulking a tumour [6].

2502 Eur Arch Otorhinolaryngol (2014) 271:2497–2502
1 3
References
1. Basterra J, Zapater E, Moreno r, Hernández r (2006) Elec-trosurgical endoscopic cordectomy with microdissection elec-trodes: a comparative study with CO2 laser. J Laryngology Otol 120:661–664
2. Basterra J, Frías S, Alba J, Zapater E (2006) A new device for treating laryngeal carcinoma using microdissection electrodes. Laryngoscope 116:2232–2234
3. Basterra J, Frías S, Alba Jr, Pérez A, Zapater E (2006) Compara-tive study of acute tissue damage induced by the CO2 laser versus microelectrodes in cordectomies. Otolaryngol Head neck Surg 135:933–936
4. Zapater E, Frías S, Pérez A, Basterra J (2009) Comparative study on chronic tissue damage after cordectomies using either a CO2 laser or microdissection electrodes. Head neck 31:1477–1481
5. Basterra J, Alba Jr, Bonet M, Zapater E (2010) Endoscopic resection of supraglottic (T1-T2-T3) and glottic (T2-T3) carci-nomas using microdisecciont electrodes. Otolaryngol Head neck Surg 142:449–451
6. Basterra J, reboll r, Zapater E (2011) 83 cases of glottic and supraglottic carcinomas (stage T1-T2-T3) treated with transoral microelectrode surgery. Clin Otolaryngol 36:500–504
7. greene FL, Page DL, Fleming ID, Fritz A, Balch CM, Haller Dg, Morrow M (eds) (2002) American Joint Committee on Cancer:
AJCC Cancer Staging Manual, 6th edn. Springer, new york, ny, USA
8. Agrawal A, Moon J, Davis K (2007) Transoral carbon dioxide laser supraglottic laryngectomy and irradiation in stage I, II and III squamous cell carcinoma of the supraglottic larynx. Arch Oto-laryngol Head neck Surg 133:1044–1050
9. Vilaseca-gonzález I, Bernal-Sprekelsen M, Blanch-Alejandro JL (2010) Transoral laser microsurgery for T3 laryngeal tumours: prognosis factors. Head neck 32:929–938
10. Steiner W, Vogt P, Ambrosch P, Kron M (2004) Transoral carbon dioxide laser microsurgery for recurrent glottic carcinoma after radiotherapy. Head neck 477–484
11. Motta g, Esposito E, Testa D, Iovine r, Motta S (2004) CO2 laser treatment of supraglottic cancer. Head neck 26:442–446
12. Cabanillas r, rodrigo JP, Llorente JL, Suarez C (2004) Func-tional outcomes of transoral laser surgery of supraglottic car-cinoma compared with a transcervical approach. Head neck 653–659
13. rodrigo J, Suarez C, Silver C et al (2008) Transoral laser surgery for supraglottic cancer. Head neck 30:658–666
14. Zeitels S, Koufman J, Davis K, Vaughan C (1994) Endoscopic treatment of supraglottic and hypopharynx cancer. Laryngoscope 104:71–78