Transfusion Guidelines: Development and Impact … THE TRANSFUSION COMMITTEE blood, and increased...
24
In: Saxena S, ed. The Transfusion Committee: Putting Patient Safety First, 2nd edition Bethesda, MD: AABB Press, 2013 9 Transfusion Guidelines: Development and Impact on Patient Blood Management TIMOTHY HANNON, MD, MBA, AND IRWIN GROSS, MD BLOOD UTILIZATION and blood-related costs are accelerating in the United States at a time when blood compo- nents, hospital labor, and health- care dollars are in short supply. The number of components transfused in the United States was approxi- mately 24 million units in 2008. 1 For the past decade, blood suppli- ers have struggled to meet the demand, while intermittent blood shortages occur. Difficulties in recruiting donors, increases in the cost of testing and processing Timothy Hannon, MD, MBA, Staff Anesthesiologist, Department of Anesthesiology, St. Vincent Hospital Indianapolis, and Chief Medical Officer, Strategic Healthcare Group, Indianapolis, Indiana, and Irwin Gross, MD, Medical Director, Patient Blood Manage- ment and Transfusion Services, Eastern Maine Medical Center, Bangor, Maine Draft 1 -- 3/14/13
Transcript of Transfusion Guidelines: Development and Impact … THE TRANSFUSION COMMITTEE blood, and increased...
In: Saxena S, ed.The Transfusion Committee: Putting Patient Safety First, 2nd edition
Bethesda, MD: AABB Press, 2013
9Transfusion Guidelines: Development and Impact on Patient Blood Management
TIMOTHY HANNON, MD, MBA, AND IRWIN GROSS, MD
BLOOD UTILIZATION and blood-related costs are accelerating in the United States at a time when blood compo-
nents, hospital labor, and health-care dollars are in short supply. The number of components transfused
in the United States was approxi-mately 24 million units in 2008.1 For the past decade, blood suppli-ers have struggled to meet the demand, while intermittent blood shortages occur. Difficulties in recruiting donors, increases in the cost of testing and processing
Timothy Hannon, MD, MBA, Staff Anesthesiologist, Department of Anesthesiology, St. Vincent Hospital Indianapolis, and Chief Medical Officer, Strategic Healthcare Group, Indianapolis, Indiana, and Irwin Gross, MD, Medical Director, Patient Blood Manage-ment and Transfusion Services, Eastern Maine Medical Center, Bangor, Maine
Draft 1 -- 3/14/13
2 THE TRANSFUSION COMMITTEE
blood, and increased skilled-labor costs caused more than a tripling of the price of blood components between 1998 and 2008, creating a hardship for hospitals already deal-ing with thin operating margins and declining reimbursement.2 In hospi-tals, the procurement, storage, pro-cessing, and transfusion of components involves an array of expensive and increasingly scarce resources, resulting in a three- to fourfold increase in the total cost of blood beyond the base cost of its acquisition.3-7
These operational and economic issues are overshadowed by the patient safety implications of inap-propriate transfusion decisions and transfusion errors and the quality management they require. Owing in large part to a lack of formal training in transfusion medicine for most physicians, the administra-tion of components is often guided by emotions, misconceptions, and myths.8 In spite of mounting evi-dence that demonstrates significant harm can result from unnecessary blood transfusions,9-11 several stud-ies document a generalized lack of compliance with appropriate trans-fusion guidelines, as well as tre-mendous variation in transfusion practice both among different insti-tutions and among individual phy-sicians in the same institution.12-20
Better Patient Blood Management through Transfusion Guidelines
In response to the above issues, for-ward-looking hospitals are imple-menting measures that better promote optimal utilization of their blood resources. By reducing varia-tion in transfusion practice and implementing more efficient meth-ods to manage candidates for trans-fusion, hospitals can reduce the need for allogeneic components while improving patient safety and clinical outcomes and reducing costs. Strategies to more efficiently manage blood resources and trans-fusion candidates include preoper-ative anemia management; the judicious use of autologous transfu-sion devices; topical hemostatic agents and systemic drugs that reduce bleeding and the need for certain surgical and anesthetic techniques; intravenous iron and erythropoietic growth factors; and measures to reduce iatrogenic blood loss.21-24
The most challenging, but poten-tially the most effective, method of reducing allogeneic transfusions is to develop systems that promote the use of evidence-based transfu-sion guidelines.25-28 Because the decision to transfuse is made thou-sands of times a day in US hospitals by a multitude of physicians, all with differing backgrounds and

TRANSFUSION GUIDELINES 3
interests in transfusion practice, there is a critical need for active and effective transfusion commit-tees (TCs) to develop, promote, and monitor best practices in blood component therapy. This chapter reviews challenges to the imple-mentation of evidence-based trans-fusion guidelines and offers guidance based on cases of suc-cessful implementation.
Challenges to Changing Physician Practice
In their role as stewards of the blood supply, TCs must function both reactively (ie, providing blood utilization review) and proactively (formulating and implementing effective transfusion guidelines). In this latter role, TCs must serve as agents of change to alter estab-lished patterns of physician behavior.
The Hospital Environment
The many challenges to changing physician practice include environ-mental factors such as poor com-munication between physicians and other members of the health-care team, misalignment among individuals and departments result-ing from different motivation-and-reward systems, a lack of experi-ence in the use of cross-functional
teams, and administrative failure to anticipate and deal with resis-tance.29 Since the first publication of this book, there has been an increasing emphasis on reducing inefficiencies and costs in the US health-care system, along with the implementation of the Patient Pro-tection and Affordable Care Act (“Affordable Care Act,” or ACA). By some estimates, 20% or more of health-care costs are due to waste and inefficiencies, and three key drivers are 1) failure of care deliv-ery, including poor execution or lack of widespread adoption of known best-care processes, 2) fail-ure of care coordination, and 3) overtreatment.30 Because these problems are widespread, many hospitals struggle to implement quality initiatives and departmen-tal reengineering projects. Studies have clearly shown that passive dis-semination of information (“stuff-ing mailboxes”) is an ineffective method of behavioral change,31,32 yet it remains a common practice. Administrators and quality manag-ers are frustrated when they invest considerable time and effort in the development of clinical practice guidelines only to see little change in outcomes after the guidelines have been published.
Staff Resistance
Resistance within organizations is a leading cause of failed change ini-tiatives.33 Common sources of resis-

4 THE TRANSFUSION COMMITTEE
tance include the inertia resulting from previously established prac-tice, negative experience with pre-vious change initiatives, insufficient time for team members to imple-ment the change process, and a lack of resources to effect the change. Resistance to change is both predictable and understand-able; because change represents uncertainty for the organization and for individuals, resistance is a natural response. Acknowledging sources of resistance and actively working toward removing barriers to progress are vital steps in build-ing trust among those involved in changing practice.
In some cases, inappropriate responses to resistance can lead to further problems.33 It is well known that individuals adapt to new ideas at different rates. Rogers is credited with first defining the rate of time required for adoption of novel pro-cesses within a group, by means of a graphed curve that plots the num-ber of adopters over time in a sig-moidal shape similar to that of the spread of an epidemic (Fig 9-1).34-36 For comparative purposes, individ-uals can be classified based on their deviation from the mean adoption time and grouped as inno-vators, early adopters, early major-ity, late majority, and laggards (Fig 9-2).36 When approaching the more conservative physicians in a group with a new concept or practice pat-tern, it is important to recognize that resistance from these individu-
als is predictable and is likely the result of the inertia of established practice, rather than true opposi-tion to the concept itself. Therefore, the best approach to these physi-cians is patience and gentle persis-tence, with the understanding that they will probably not adopt the change until they see other col-leagues leading the way. As such,
Figure 9-1. From a 1943 study show-ing the cumulative number of adopters of a novel process within a group (ie, adoption of hybrid seed corn by farm-ers in two Iowa communities). Reprinted with permission from Rog-
Figure 9-2. Adopter categorization on the basis of innovativeness. Reprinted with permission from Rogers.35

TRANSFUSION GUIDELINES 5
visibility of change efforts by key physician groups and communica-tion of implementation progress are mechanisms to shorten adaption time. Failure to recognize the ten-dency of these individuals to resist change in general can worsen the situation; an antagonistic and overly aggressive approach often leads to genuine opposition. It is also important that clinical and administrative leaders set the expectation that the change effort will be supported and will not go away; otherwise, resistant individu-als may be tempted to simply try and “wait it out.”
Implementing Clinical Practice Guidelines
The Root of Resistance
The Institute of Medicine of the National Academies and other agencies have called for the increased use of clinical practice guidelines to reduce practice varia-tion, improve quality of care, and decrease inefficiencies.29,30,37 Pro-viding such guidance is a major function of hospital TCs. Although the use of transfusion guidelines can improve blood utilization and transfusion outcomes by providing education and guidance for best practice in specific clinical situa-tions, the mere publishing of guide-
lines does nothing to change actual physician practice. Even when the rationale behind practice guide-lines has been given thoughtful consideration and is quite logical, the successful implementation of the guidelines relies heavily upon the emotional reactions and other responses of the physicians affected. Because of this, imple-mentation of practice guidelines first requires changes in percep-tions and attitudes in order to achieve changes in behavior.37
To facilitate attitudinal change, it is important that practice guidelines be internally generated with an expanding process of ownership and “buy-in.” The development of ownership is a process by which stakeholders in the organization are actively involved in shaping the change effort. The process of buy-in builds with a movement toward acceptance and endorsement of the change process by affected individ-uals. In the early stages of guideline implementation, “buy-in” may mean merely that certain key indi-viduals in the group do not actively resist the guidelines.
Key Elements in Implementation
Several published studies have investigated methods to success-fully implement practice guide-lines. This literature31,32,38,39 supports the selection of several conditions that should be met in
6 THE TRANSFUSION COMMITTEE
the process of guideline implemen-tation:1. The guidelines should be based
on scientific evidence, and their application must be meaning-ful in clinical practice (ie, they must be worth the effort).
2. Key local physicians who are responsible for adapting them to local circumstances should formulate the guidelines, and affected users should have the opportunity to critique them.
3. The guidelines should have readily discernible benchmarks or targets for good practice.
4. Active educational efforts should accompany dissemina-tion of the guidelines to all affected health-care providers, and manual or computerized reminder systems should prompt use of the guidelines at points of intervention.
5. Implementation of the guide-lines must include either direct feedback on performance to individual physicians or gen-eral feedback on system perfor-mance.
6. Accountability for adherence to the guidelines must come from peer pressure, administra-tive sanction, and/or financial incentives or disincentives.
Conversely, guideline implemen-tation techniques shown to be inef-fective are those that rely on passive dissemination or voluntary change in practice patterns or that lack an accountability component.32
Key Leaders in Implementation
Once practice guidelines have been formulated, the TC needs to devote a great deal of time and effort to promoting their use. It has been proposed that as much as 90% of total efforts should be spent on guideline implementation and only 10% on development.40 More specifically, educational efforts should target key physicians known to be influential with their peers. Clinicians usually analyze new clinical information by seeking additional information and opin-ions from peers in their local net-work rather than individually reviewing the scientific merits.41
Physician opinion leaders are those physicians informally judged by their peers as educationally influential and trustworthy to evalu-ate new information in the context of the local group norms.41 To lead opinion, a physician must be con-sidered by associates to be techni-cally competent and well integrated with his or her peers in the local medical community.34 It is important to note that opinion lead-ers are informal leaders who are practicing physicians and gener-ally not administrators or authority figures.42 Opinion leaders are also not innovators or early adopters; rather, they are conservative evalu-ators.34 Because their clinical judg-ment is highly valued, physician opinion leaders have the ability to directly or indirectly affect the prac-
TRANSFUSION GUIDELINES 7
tice patterns of their peers. The adoption of new information or technology into one opinion leader’s practice is tremendously influential, because similar adop-tion by peers can occur by leader emulation alone. Concentrating educational and buy-in efforts on physician opinion leaders is an effi-cient and effective method of facili-tating changes in practice.34,41
Case Study: Transfusion Guideline Implementation at St. Vincent Indianapolis Hospital
St. Vincent Hospital is an 800-bed, tertiary care, community hospital in Indianapolis, IN. A comprehensive patient blood management (PBM) program was created in 2001 in response to rising blood utilization and blood costs, disparate patterns in blood use among physicians, and concerns about patient safety. A core element of this program was the formulation and implementa-tion of evidence-based transfusion guidelines by the TC in order to reduce variation and promote best practices in transfusion medicine. A description of the process and the results of the program follow.
The Guideline Revision Process
Following publication of evidence that conservative transfusion strate-gies might be at least as effective as (and possibly even superior to) more liberal transfusion strategies,9 the St. Vincent TC decided to sig-nificantly revise its recommenda-tions for RBC transfusions. Understanding that a transition to this more conservative approach would require major changes in physician attitudes and practice, the TC devised an extensive pro-cess for the formulation, review, and approval of revised transfusion guidelines. The process was specifi-cally designed to build awareness, interest, and buy-in with hospital clinical and administrative leader-ship groups. In addition, the TC began educational efforts about transfusion risks and benefits in tan-dem with the guideline formulation and implementation.
The first step for the TC in the for-mulation of the transfusion guide-lines was to convene a local expert panel to review the transfusion lit-erature. The membership of this panel included respected clinical leaders in anesthesiology, cardiol-ogy, pathology, hematology/oncol-ogy, pediatrics, critical care, cardiac surgery, vascular surgery, and orthopedics, some from out-side the existing TC. Articles reviewed included consensus con-ference recommendations, as well as current clinical trials of transfu-
8 THE TRANSFUSION COMMITTEE
sion strategies, both observational and controlled. The panel then constructed the core recommenda-tions for the hospital’s evidence-based transfusion guidelines cover-ing red cells, platelets, plasma, and cryoprecipitate.
The recommendations of this panel were presented to the TC as a whole for comment, revision, and approval. An interesting phenome-non that occurred during the review process was that TC mem-bers who had been inactive in the past became actively involved and highly participative because they wanted to be certain that their opinions were heard in the guide-lines process.
Following approval by the TC, the transfusion guidelines were pre-sented for review to the Quality Management Committee, which was the largest committee in the hospital and represented a diverse group of clinical and nonclinical departments. Again, the transfu-sion guidelines were openly reviewed before approval.
The final step in the approval process involved the medical exec-utive committee (MEC). A formal presentation was prepared for the MEC; once again, the guidelines were carefully scrutinized before being approved. This final approval step added considerable weight to the enforcement of the guidelines, because compliance was deemed a component criterion for physician recredentialing by the MEC.
The entire process of guideline formulation, review, and approval through an expert panel and three committees took 5 months—a remarkably short time to accom-plish such a major undertaking. Although the process was labori-ous, challenging, and at times con-tentious, the benefit of this meticulous and transparent review of the transfusion guidelines was a sense of ownership and buy-in by key hospital staff. Further, the extensive internal review of the new guidelines proved extremely useful later when they were chal-lenged by individual physicians. In these instances, the process of guideline approval and a list of the relevant clinicians involved in the review process were recounted to support the guidelines.
Education
As previously mentioned, general educational efforts were begun dur-ing the development of the guide-lines, and these efforts were continued through the period of guideline implementation. Medical and surgical departments held meetings, and hospital newsletters disseminated information. The TC actively sought out key physician opinion leaders who had not been involved in the formulation of the guidelines and briefed them through an informal academic detailing process. In addition, the TC made significant efforts to edu-
TRANSFUSION GUIDELINES 9
cate nursing leadership and nursing staff. The TC deemed the inclusion of nursing education efforts particu-larly important, because nurses are generally the interface between physician blood-ordering practices and patients. Nursing staff received education about transfusion risks and benefits, the importance of patient safety measures such as positive patient identification, and the need to “encourage” the use of the new transfusion guidelines in their role as patient advocates.
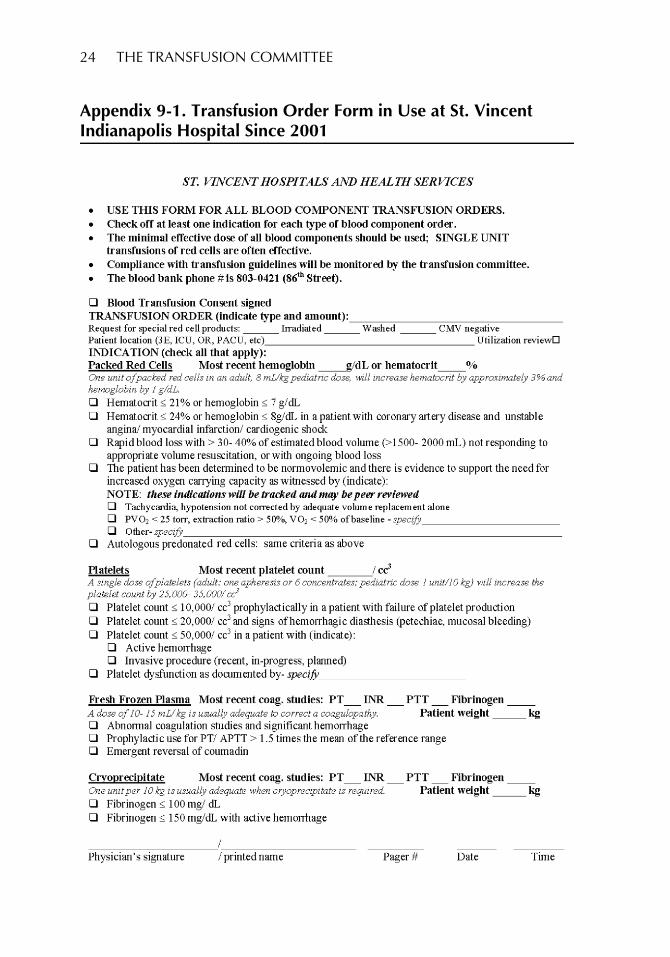
Implementation of a Transfusion Order Form
A critical component of the imple-mentation process required the timely provision of information to support transfusion decisions. Con-sidering the challenges of dissemi-nating information to a large medical staff in a community hospi-tal and the need to provide manual or computerized reminder systems at points of intervention, the TC decided to create a transfusion order form to promote the use of the transfusion guidelines (see Appendix 9-1
The TC used the following ratio-nale to support this form, based on its benefits:1. Awareness/Visibility. To coun-
terbalance sparse attendance at department meetings and grand rounds presentations, the use of a transfusion order form provided a tangible reminder
of the changes the hospital was making in blood utilization. Although the physician response to additional paper-work may have been less than enthusiastic, the implementa-tion of a novel process served to create high visibility for the effort.
2. Education. As previously men-tioned, most physicians do not have formal training in blood component therapy, and remaining current with new research can be challenging when transfusion medicine is not a physician’s area of clini-cal focus. Therefore, the major driver for the creation of the order form was to provide an educational opportunity for physicians. The order form provided approved clinical indications and dosing recom-mendations for RBCs and coagulation-factor therapy (platelets, plasma, and cryopre-cipitate).
3. Compliance/Peer Review. The last major rationale for the inception of the transfusion order form was to improve documentation for blood com-ponent use and to provide a mechanism for peer review through audit and feedback. Although documenting clini-cal indications for blood com-ponent therapy in the medical record is required by accredit-ing organizations such as The

10 THE TRANSFUSION COMMITTEE
Joint Commission and is con-sidered sound practice, a review of the medical records at St. Vincent revealed a lack of adequate documentation in a significant percentage of cases. The transfusion order form allowed physicians to quickly document the patient’s con-sent, pretransfusion physio-logic status, and clinical indication for the transfusion. If the physician chose not to select an approved indication for a component, additional documentation was required. The printed format of the trans-fusion order form allowed for the creation of a carbonless copy, so that one sheet could remain in the chart to serve as documentation, and one sheet could be sent to the blood bank and then the TC. A small sampling of these forms was reviewed each quarter (approx-imately 5% to 10% of cases) for the purposes of peer review and enforcing compliance.
Blood Utilization Benchmarking
In addition to audit of and feedback from the transfusion order form, blood utilization benchmarking was employed by the St. Vincent TC to promote better blood utiliza-tion. Utilization benchmarking is a valuable tool for process improve-ment in health care and should be used as part of a larger quality
improvement tool set that includes metrics, education, and change management strategies. The three purposes of benchmarking are learning from others, identification of performance gaps, and imple-mentation of best practices.43 A sys-tem of peer profiling to compare average blood component transfu-sion rates within major Medicare severity diagnosis-related groups (MS-DRGs) was used. MS-DRGs are defined by the Centers for Medicare and Medicaid Services and are intended to group patients with like procedures or diagnoses for purposes of cost reporting and reimbursement. The MS-DRG sys-tem also contains three levels of patient comorbidity for each proce-dure grouping, so it constitutes a reasonable and standardized method of comparing similar patients across institutions.
The first step in the process was to compare the average number of blood components used per patient, by MS-DRG grouping, to benchmark figures derived from multiple hospitals. In order to reduce the impact of outliers and to provide more meaningful data, a 12-month rolling average was used. This analysis provided hospital leadership with a general overview of blood component utilization in each service line or department and helped to target opportunities for improvement. The second step was to then compare individual physi-cians’ blood component use to that
TRANSFUSION GUIDELINES 11
of their hospital peers. This second evaluation provided a clear view of variability in practice patterns among physicians managing similar patients within the hospital, and generally had greater impact on shaping physician behavior. Although review of individual transfusion decisions through audit and feedback is important, this benchmarking data can provide a more holistic view of PBM prac-tices. Because transfusions, or the lack of them, are often the end result of a series of events (ie, pre-operative preparation, surgical techniques, pharmaceutical use, and adherence to transfusion guidelines), significant deviations from peer norms may represent multiple opportunities for improve-ment. Upon review, if the TC deemed that a physician was over-using components in relationship to his or her peers, the TC sent the benchmark utilization data, along with a supporting letter, to the appropriate clinical department head for discussion with the physi-cian. The role of the TC in these cases was to provide educational support to the department head and physician, rather than to function as a disciplinary body. The use of this blood utilization benchmarking method as a component of a com-prehensive PBM program in a large academic center was recently pub-lished,44 and it is important to note that blood utilization profiling such as this can be used for ongoing pro-
fessional practice evaluation (OPPE).
Program Advancements—Addition of a Transfusion Safety Coordinator
In order to provide support for ongoing education, training, and quality improvement related to blood utilization and transfusion administration safety, St. Vincent created a transfusion safety coordi-nator (TSC) position based on suc-cessful models in Canada and the United Kingdom.8,45 TSCs, also called transfusion safety officers, are specialists that educate clinical staff on transfusion guidelines, safe transfusion administration prac-tices, and protocols that improve PBM. Goals and activities for TSCs include the following46:• Tracking hospital performance
of key processes by active sur-veillance (observation audits) and chart reviews.
• Tracking data on key perfor-mance indicators developed by the TC.
• Participating in an overall pro-gram of transfusion safety error and/or accident reporting (bio/hemovigilance).
• Educating clinical staff (nurs-ing, physician) regarding hospi-tal transfusion guidelines, risks of blood transfusion, and rec-ognition and reporting of trans-fusion reactions.
12 THE TRANSFUSION COMMITTEE
• Providing orientation training for new physician and nursing staff responsible for administer-ing blood in high-usage areas.
• Contributing to continual improvement processes for blood utilization review through transfusion order audit and feedback.
There is a growing body of evi-dence that trained and empowered TSCs provide tangible improve-ments in patient safety, blood utili-zation, and quality of care. After training and deploying TSCs to a hospital network in Ontario, Can-ada, a significant decrease in blood use was experienced, including a 24% reduction of use in knee sur-geries and a 23% reduction of use in coronary artery bypass graft sur-gery. Further, patients that were vis-ited preoperatively by a TSC for preoperative evaluation and ane-mia management were 38% less likely to receive a transfusion dur-ing cardiac surgery.47 Experience to date at St. Vincent has shown the TSC to be a tremendous addition to the TC, as well as the quality man-agement department, by providing a day-to-day resource for promot-ing the overall objectives of safe and effective blood component therapy.
Results of Successful Transfusion Guideline Implementation
The results of the interventions at St. Vincent Hospital were remark-
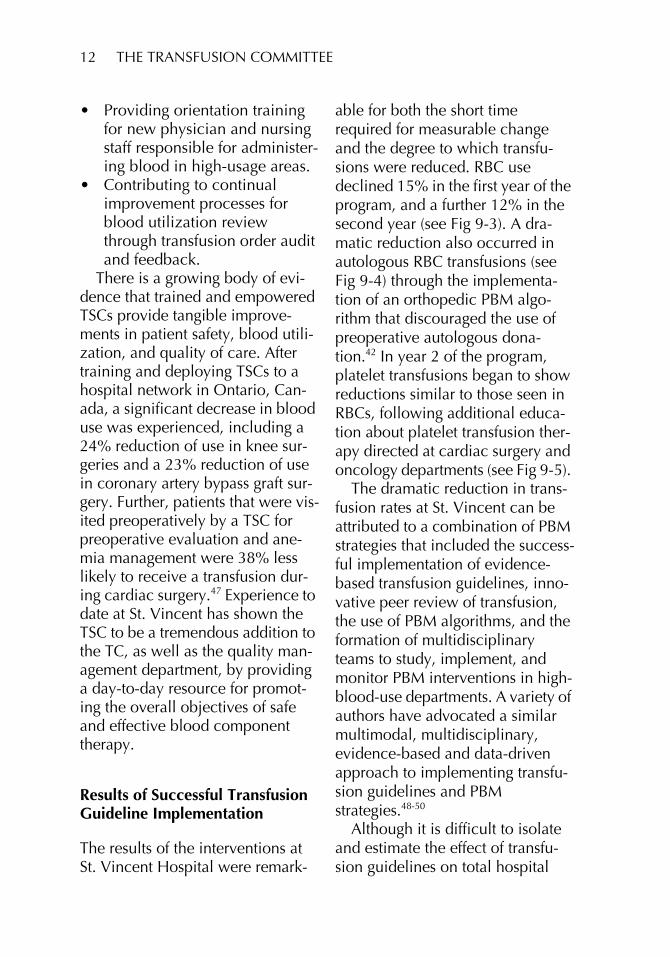
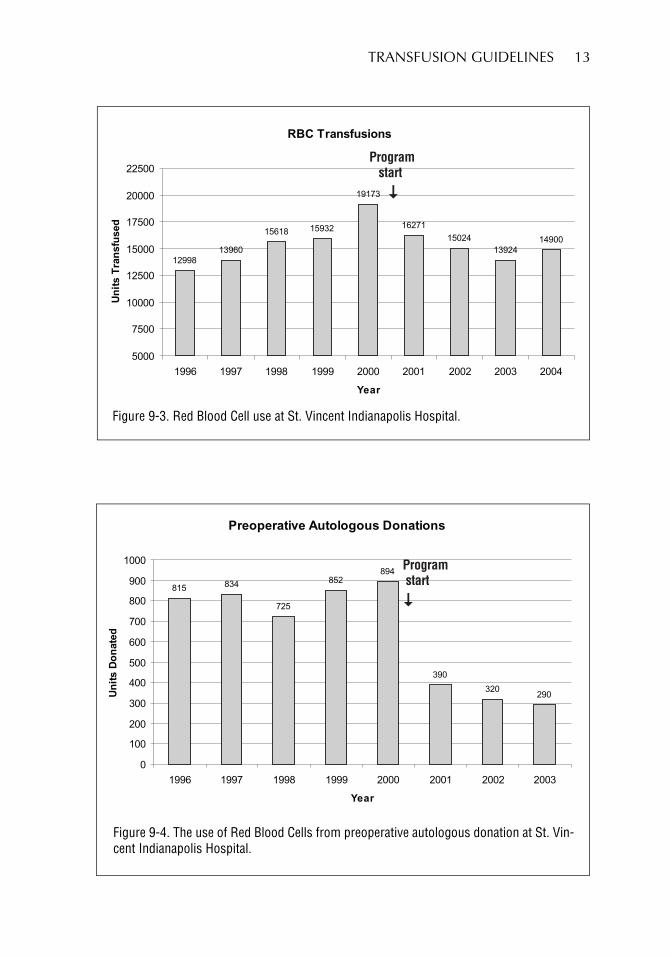
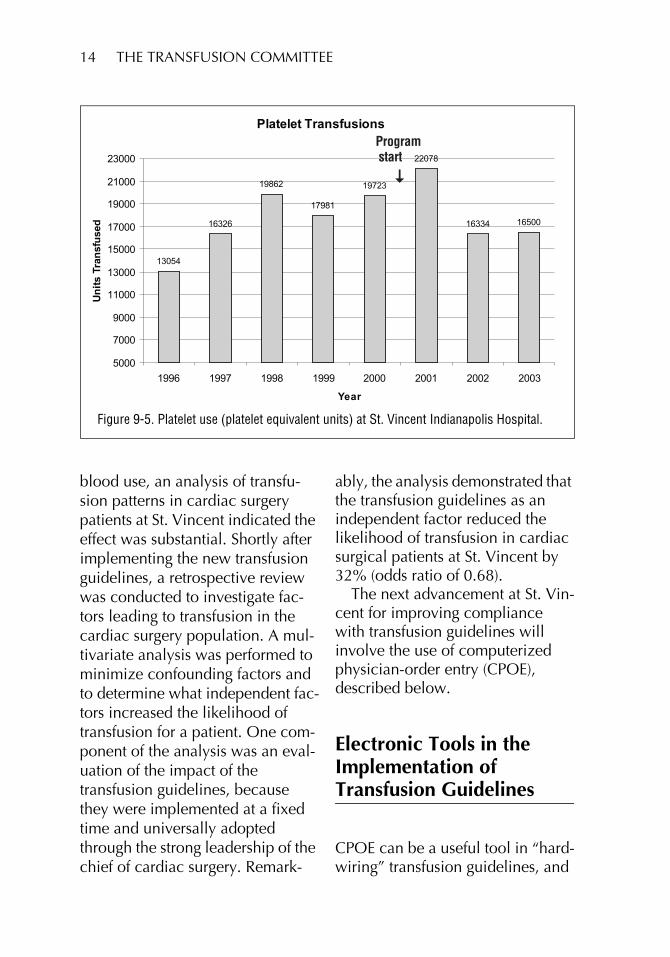
able for both the short time required for measurable change and the degree to which transfu-sions were reduced. RBC use declined 15% in the first year of the program, and a further 12% in the second year (see Fig 9-3). A dra-matic reduction also occurred in autologous RBC transfusions (see Fig 9-4) through the implementa-tion of an orthopedic PBM algo-rithm that discouraged the use of preoperative autologous dona-tion.42 In year 2 of the program, platelet transfusions began to show reductions similar to those seen in RBCs, following additional educa-tion about platelet transfusion ther-apy directed at cardiac surgery and oncology departments (see Fig 9-5).
The dramatic reduction in trans-fusion rates at St. Vincent can be attributed to a combination of PBM strategies that included the success-ful implementation of evidence-based transfusion guidelines, inno-vative peer review of transfusion, the use of PBM algorithms, and the formation of multidisciplinary teams to study, implement, and monitor PBM interventions in high-blood-use departments. A variety of authors have advocated a similar multimodal, multidisciplinary, evidence-based and data-driven approach to implementing transfu-sion guidelines and PBM strategies.48-50
Although it is difficult to isolate and estimate the effect of transfu-sion guidelines on total hospital
TRANSFUSION GUIDELINES 13
RBC Transfusions
12998
13960
15618 15932
19173
16271
15024
13924
14900
5000
7500
10000
12500
15000
17500
20000
22500
1996 1997 1998 1999 2000 2001 2002 2003 2004
Year
Un
its
Tran
sfu
sed
Programstart
�
Figure 9-3. Red Blood Cell use at St. Vincent Indianapolis Hospital.
Preoperative Autologous Donations
815834
725
852
894
390
320290
0
100
200
300
400
500
600
700
800
900
1000
1996 1997 1998 1999 2000 2001 2002 2003
Year
Un
its
Do
nate
d
Programstart
�
Figure 9-4. The use of Red Blood Cells from preoperative autologous donation at St. Vin-cent Indianapolis Hospital.
14 THE TRANSFUSION COMMITTEE
blood use, an analysis of transfu-sion patterns in cardiac surgery patients at St. Vincent indicated the effect was substantial. Shortly after implementing the new transfusion guidelines, a retrospective review was conducted to investigate fac-tors leading to transfusion in the cardiac surgery population. A mul-tivariate analysis was performed to minimize confounding factors and to determine what independent fac-tors increased the likelihood of transfusion for a patient. One com-ponent of the analysis was an eval-uation of the impact of the transfusion guidelines, because they were implemented at a fixed time and universally adopted through the strong leadership of the chief of cardiac surgery. Remark-
ably, the analysis demonstrated that the transfusion guidelines as an independent factor reduced the likelihood of transfusion in cardiac surgical patients at St. Vincent by 32% (odds ratio of 0.68).
The next advancement at St. Vin-cent for improving compliance with transfusion guidelines will involve the use of computerized physician-order entry (CPOE), described below.
Electronic Tools in the Implementation of Transfusion Guidelines
CPOE can be a useful tool in “hard-wiring” transfusion guidelines, and
Platelet Transfusions
13054
16326
19862
17981
19723
22078
16334 16500
5000
7000
9000
11000
13000
15000
17000
19000
21000
23000
1996 1997 1998 1999 2000 2001 2002 2003
Year
Un
its
Tran
sfu
sed
Programstart
�
Figure 9-5. Platelet use (platelet equivalent units) at St. Vincent Indianapolis Hospital.
TRANSFUSION GUIDELINES 15
has been proven to be effective in terms of overall reduction in blood component use.51,52 One pediatric intensive care unit (ICU) had a 52% decrease in RBC transfusions per patient per day after employing CPOE,53 and CPOE was shown to improve compliance with existing transfusion guidelines in a neonatal ICU by 25%.27
The use of paper orders for trans-fusion guidelines can serve as a precursor for successful implemen-tation of CPOE, and subsequently the guidelines become an integral part of electronic decision support. Ideally, the CPOE design should do more than simply recreate an exist-ing paper process for ordering transfusions. CPOE is of greatest value in improving and then hard-wiring physician transfusion prac-tices when clinical decision support (CDS) is incorporated into the design. CDS systems provide physicians (and others) with rele-vant knowledge and patient-spe-cific information to support clinical decision making. This may take the form of references, reminders, alerts, recommendations, and guidelines. These decision support tools work best when they fit into the physician’s workflow and pro-vide clinically relevant information to redirect physicians to an alterna-tive action rather than stopping them without offering an alterna-tive.54 Well-designed CDS systems as part of a CPOE system can help
educate physicians about a hospi-tal’s transfusion guidelines at the point of decision.
The design of the CPOE process can have a profound impact on user acceptance, as well as the degree to which CPOE has a mean-ingful influence on physician deci-sion making. In a retrospective study of the impact of CPOE on compliance with transfusion guide-lines 2 years after implementation, providers indicated the presence of “active bleeding” in 66% of transfu-sion orders that effectively bypassed the CDS. However, medi-cal record review showed that in only 46% of these cases was the presence of bleeding substanti-ated.55 The number and complexity of the input screens may have con-tributed to a lack of user accep-tance and encouraged efforts to avoid the CDS.
In a study of a computerized transfusion decision support sys-tem (CTDSS) for frozen plasma, more than one-third of transfused plasma was given to patients with normal coagulation studies. The CTDSS was not enabled to reject inappropriate transfusion requests, and did not require that an indica-tion be chosen before completing the order. This CPOE process failed to make clinically relevant pre-transfusion coagulation results available on the request screen at the time transfusion was being ordered, limiting its utility.56

16 THE TRANSFUSION COMMITTEE
Elements of Successful Implementation for Electronic Tools
A number of design features may improve the probability of success-ful implementation of transfusion guidelines as part of CDS for CPOE.54,57 Speed and a user-friendly interface are important. Minor changes in the appearance of an input screen can have a major impact on provider actions. The process should fit the user’s work-flow and provide clinically relevant information at the right time within that workflow.51 A recommended practice is to avoid “hard stops” in computerized orders, because these are strongly resisted by physi-cians and often lead physicians to develop work-arounds that circum-vent CDS. Alerts with a hard stop should be reserved for situations that place patient safety at risk. Instead, the preferred actions should be made as easy as possible to execute, while decisions or actions that are discouraged should be made more difficult. The clini-cian should not be able to override critical alerts or barriers but should be allowed to easily exercise clini-cal judgment where appropriate. Changing a physician’s direction is easier than stopping it.54 For exam-ple, redirecting a physician to order vitamin K rather than plasma for
warfarin reversal without having to leave the transfusion order input screen will be more likely to achieve compliance with guide-lines than a hard stop with no alter-native or the need to initiate a new ordering process. Setting defaults to be consistent with guideline recom-mendations offers a path of least resistance and will improve com-pliance with guidelines. Finally, CPOE is most successful when its use is mandatory. With regards to blood component therapy, excep-tions to mandatory use might include urgent or emergency requests for blood in an unstable patient with active bleeding.
Successful implementation of transfusion guidelines does not guarantee that initial changes in clinical practice will be durable. Tethering transfusion guidelines to CPOE facilitates transfusion utiliza-tion review and helps ensure com-pliance. CPOE allows the transfusion service to assign the ordering physician with great accu-racy and avoids attribution of a transfused unit to an admitting or consulting physician who may have had no role in the transfusion decision. The indication for transfu-sion and relevant clinical data should also be captured electroni-cally, facilitating statistical analysis of transfusion practice as well as utilization review.58
TRANSFUSION GUIDELINES 17
CPOE Case Study: The Use of CPOE to Encourage Ordering RBCs as Single Units
Eastern Maine Medical Center (EMMC) is a 375-bed tertiary hospi-tal in Bangor, ME. EMMC imple-mented a comprehensive PBM program in 2007 and used CPOE with CDS as part of a transfusion guideline implementation strategy. One component of that strategy was to encourage single-unit RBC transfusions in stable, nonbleeding patients. Many physicians were taught informally that single-unit transfusions were likely to be inef-fective, and some TCs have used single-unit RBC transfusions as a quality indicator prompting utiliza-tion review.59 Based on the current risk/benefit profile of blood compo-nent therapy, there should be an emphasis on using the minimum effective dose, which is often a sin-gle unit in an otherwise stable patient who has dropped below a transfusion threshold.
EMMC decided that for most patients without significant active bleeding, the appropriate RBC order should be for a single unit, with clinical reassessment before a second unit is ordered. This was promoted through education and hospital policy as established by hospital transfusion guidelines. A significant level of success was achieved by this educational effort, with approximately 60% to 65% of all RBC orders being entered as sin-
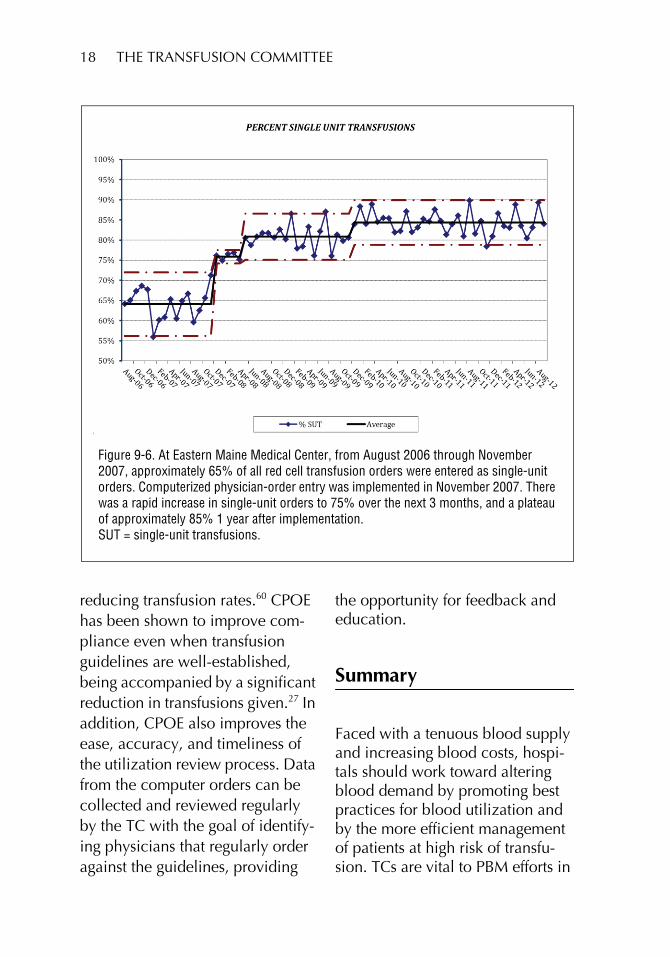
gle-unit orders from August 2006 through November 2007 (Fig 9-6).
In an effort to improve compli-ance, a CPOE process was designed that introduced a barrier to multiunit orders. Specifically, the process required the ordering phy-sician to indicate whether or not the patient had active bleeding. If the patient was not actively bleed-ing, the transfusion ordering “con-versation” within the CDS allowed only 1 unit to be ordered. To order a second unit, the physician needed to begin a new order “con-versation.” This then required addi-tional effort to go through the order process a second time, making it harder to do “the wrong thing.” As seen in Fig 9-6, after implementa-tion of the CPOE process in November 2007, there was a rapid and sustainable increase in the per-centage of RBC orders entered as single-unit orders, to approximately 85%. Further, quality monitoring showed that in patients transfused with only 1 unit, a second unit was ordered within the next 24 hours only 9% of the time (data not shown).
In conclusion, CPOE with CDS is a useful tool when combined with other behavioral interventions to reduce transfusions and assist in the implementation of transfusion guidelines. It may be difficult to dis-cern the independent effect of any one intervention, but in combina-tion these behavioral interventions may have a significant effect on
18 THE TRANSFUSION COMMITTEE
reducing transfusion rates.60 CPOE has been shown to improve com-pliance even when transfusion guidelines are well-established, being accompanied by a significant reduction in transfusions given.27 In addition, CPOE also improves the ease, accuracy, and timeliness of the utilization review process. Data from the computer orders can be collected and reviewed regularly by the TC with the goal of identify-ing physicians that regularly order against the guidelines, providing
the opportunity for feedback and education.
Summary
Faced with a tenuous blood supply and increasing blood costs, hospi-tals should work toward altering blood demand by promoting best practices for blood utilization and by the more efficient management of patients at high risk of transfu-sion. TCs are vital to PBM efforts in
Figure 9-6. At Eastern Maine Medical Center, from August 2006 through November 2007, approximately 65% of all red cell transfusion orders were entered as single-unit orders. Computerized physician-order entry was implemented in November 2007. There was a rapid increase in single-unit orders to 75% over the next 3 months, and a plateau of approximately 85% 1 year after implementation. SUT = single-unit transfusions.

TRANSFUSION GUIDELINES 19
the development of evidence-based transfusion guidelines. Successful implementation of such guidelines requires an organizational commit-ment at all levels and a firm under-standing of the principles involved in formulating and internally mar-keting practice change among phy-sicians. The experiences at St. Vincent Hospital and EMMC dem-onstrate that the impact of these guidelines can be substantial when combined with other methods to manage blood utilization in the most appropriate and systematic manner.
References
1. US Department of Health and Human Services. The 2009 national blood collection and uti-lization survey report. Washing-ton, DC: DHHS, 2011. [Available at http://www.aabb.org/programs/biovigilance/nbcus/Pages/default. aspx (accessed August 28, 2012).]
2. Goodman C, Chan S, Collins P, et al. Ensuring blood safety and availability in the US: Technolog-ical advances, costs, and chal-lenges to payment—final report. Transfusion 2003;43(8 Suppl):3S–46S.
3. Cantor SB, Hudson DV, Lichtiger B, Rubenstein EB. Costs of blood transfusion: A process-flow analy-sis. J Clin Oncol 1998;16:2364-70.
4. Mohandas K, Aledort L. Transfu-sion requirements, risks, and costs for patients with malig-
nancy. Transfusion 1995;35:427-30.
5. Crémieux PY, Barrett B, Anderson K, Slavin MB. Cost of outpatient blood transfusion in cancer patients. J Clin Oncol 2000;18: 2755-61.
6. Shander A, Hofmann A, Ozawa S, et al. Activity-based costs of blood transfusions in surgical patients at four hospitals. Transfu-sion 2010;50:753-65.
7. Hannon TJ, Paulson-Gjerde K. Contemporary economics of transfusions. In: Spiess BD, Spence RK, Shander A, eds. Peri-operative transfusion medicine. 2nd ed. Philadelphia, PA: Lippin-cott Williams and Wilkins, 2006: 13-38.
8. Dzik WH. Emily Cooley Lecture 2002: Transfusion safety in the hospital. Transfusion 2003;43: 1190-9.
9. Hébert PC, Wells G, Blajchman M, et al. A multicenter, random-ized, controlled clinical trial of transfusion requirements in criti-cal care. Transfusion Require-ments in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med 1999;340:409-17.
10. Rao SV, Jollis JG, Harrington R, et al. Relationship of blood transfu-sion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004;292:1555-62.
11. Ferraris V, Davenport DL, Saha SP, et al. Intraoperative transfu-sion of small amounts of blood heralds worse postoperative out-come in patients having noncar-
20 THE TRANSFUSION COMMITTEE
diac thoracic operations. Ann Thorac Surg 2011;91:1674-80; discussion, 1680.
12. Goodnough LT, Johnston MF, Toy PT. The variability of transfusion practice in coronary artery bypass surgery. Transfusion Medicine Academic Award Group. JAMA 1991;265:86-90.
13. Stover EP, Siegel LC, Body SC, et al. Institutional variability in red blood cell conservation practices for coronary artery bypass graft surgery. Institutions of the Multi-Center Study of Perioperative Ischemia Research Group. J Cardiothorac Vasc Anesth 2000;14:171-6.
14. Audet AM, Andrzejewski C, Pop-ovsky MA. Red blood cell transfu-sion practices in patients undergoing orthopedic surgery: A multi-institutional analysis. Orthopedics 1998;21:851-8.
15. Poses RM, Berlin JA, Noveck H, et al. How you look determines what you find: Severity of illness and variation in blood transfusion for hip fracture. Am J Med 1998;105:198-206.
16. Corwin HL, Gettinger A, Pearl RG, et al. The CRIT Study: Ane-mia and blood transfusion in the critically ill—current clinical practice in the United States. Crit Care Med 2004;32:39-52.
17. Bennett-Guerrero E, Zhao Y, O’Brien SM, et al. Variation in use of blood transfusion in coro-nary artery bypass graft surgery. JAMA 2010;304:1568-75.
18. Frank SM, Savage WJ, Rothschild J, et al. Variability in blood and blood component utilization as
assessed by an anesthesia infor-mation management system. Anesthesiology 2012;117:99-106.
19. Tinegate H, Allard S, Grant-Casey J, et al. Cryoprecipitate for trans-fusion: Which patients receive it and why? A study of patterns of use across three regions in Eng-land. Transfus Med 2012;22:356-61.
20. Puetz J, Witmer C, Huang Y-SV, Raffini L. Widespread use of fresh frozen plasma in US children’s hospitals despite limited evidence demonstrating a beneficial effect. J Pediatr 2012;160:210-15.
21. Corwin HL, Parsonnet KC, Get-tinger A. RBC transfusion in the ICU. Is there a reason? Chest 1995;108:767-71.
22. Boucher BA, Hannon TJ. Blood management: A primer for clini-cians. Pharmacotherapy 2007;27:1394-411.
23. Shander A, Javidroozi M, Perel-man S, et al. From bloodless sur-gery to patient blood manage-ment. Mt Sinai J Med 2012;79:56-65.
24. Gombotz H. Patient blood man-agement: A patient-orientated approach to blood replacement with the goal of reducing anemia, blood loss and the need for blood transfusion in elective surgery. Transfus Med Hemother 2012;39:67-72.
25. Carson JL, Hill S, Carless P, et al. Transfusion triggers: A systematic review of the literature. Transfus Med Rev 2002;16:187-99.
26. Goodnough LT, Soegiarso RW, Birkmeyer JD, Welch HG. Eco-
TRANSFUSION GUIDELINES 21
nomic impact of inappropriate blood transfusions in coronary artery bypass graft surgery. Am J Med 1993;94:509-14.
27. Baer VL, Henry E, Lambert DK, et al. Implementing a program to improve compliance with neona-tal intensive care unit transfusion guidelines was accompanied by a reduction in transfusion rate: A pre-post analysis within a multi-hospital health care system. Transfusion 2011;51:264-9.
28. Tavares M, DiQuattro P, Nolette N, et al. Reduction in plasma transfusion after enforcement of transfusion guidelines. Transfu-sion 2011;51:754-61.
29. Committee on Quality of Health Care in America, Institute of Med-icine. Crossing the quality chasm: A new health system for the 21st century. Washington, DC: National Academies Press, 2001.
30. Berwick DM, Hackbarth AD. Eliminating waste in US health care. JAMA 2012;307:1513-16.
31. Oxman AD, Thomson MA, Davis DA, Haynes RB. No magic bul-lets: A systematic review of 102 trials of interventions to improve professional practice. CMAJ 1995;153:1423-31.
32. Smith TJ, Hillner BE. Ensuring quality cancer care by the use of clinical practice guidelines and critical pathways. J Clin Oncol 2001;19:2886-97.
33. Maurer R. Making matters worse. In: Beyond the wall of resistance. Austin, TX: Bard Press, 2005:33-42.
34. Greer AL. The state of the art ver-sus the state of the science. The
diffusion of new medical technol-ogies into practice. Int J Technol Assess Health Care 1988;4:5-26.
35. Rogers EM. Diffusions of innova-tions. 4th ed. New York: Free Press, 1995:258.
36. Berwick DM. Disseminating innovations in health care. JAMA 2003;289:1969-75.
37. Matheny J. Organizational ther-apy: Relating a psychotherapeutic model of planned personal change to planned organizational change. Journal of Managerial Psychology 1998;13:394-405.
38. NHS Centre for Reviews and Dis-semination. Getting evidence into practice. Effective Health Care (Feb) 1999;5(1):1-16. [Available at http://www.york.ac.uk/inst/crd/EHC/ehc51.pdf (accessed Febru-ary 18, 2013).]
39. Davis DA, Taylor-Vaisey A. Translating guidelines into prac-tice. A systematic review of theo-retic concepts, practical experience and research evi-dence in the adoption of clinical practice guidelines. CMAJ 1997;157:408-16.
40. Katterhagen G. Physician compli-ance with outcome-based guide-lines and clinical pathways in oncology. Oncology (Williston Park) 1996;10(11 Suppl):113-21.
41. Borbas C, Morris N, McLaughlin B, et al. The role of clinical opinion leaders in guideline implementation and quality improvement. Chest 2000;118(2 Suppl):24S-32S.
42. Pierson JL, Hannon TJ, Earles DR. A blood-conservation algorithm to reduce blood transfusions after
22 THE TRANSFUSION COMMITTEE
total hip and knee arthroplasty. J Bone Joint Surg Am 2004;86-A:1512-18.
43. De Korne DF, Sol KJC, van Wijn-gaarden JDH, et al. Evaluation of an international benchmarking initiative in nine eye hospitals. Health Care Manage Rev 2010;35:23-35.
44. Marques MB, Polhill SR, Wal-drum MR, et al. How we closed the gap between red blood cell utilization and whole blood col-lections in our institution. Trans-fusion 2012;52:1857-67.
45. Brooks JP. Reengineering transfu-sion and cellular therapy pro-cesses hospitalwide: Ensuring the safe utilization of blood products. Transfusion 2005;45(4 Suppl):159S-71S.
46. Kim JY, Dzik WH, Dighe AS, Lewandrowski KB. Utilization management in a large urban academic medical center: A 10-year experience. Am J Clin Pathol 2011;135:108-18.
47. Freedman J, Luke K, Escobar M, et al. Experience of a network of transfusion coordinators for blood conservation (Ontario Transfu-sion Coordinators [ONTraC]). Transfusion 2008;48:237-50.
48. DeAnda A, Baker KM, Roseff SD, et al. Developing a blood conser-vation program in cardiac sur-gery. Am J Med Qual 2006;21:230-7.
49. Murphy MF, Staves J, Davies A, et al. How do we approach a major change program using the example of the development, evaluation, and implementation of an electronic transfusion man-
agement system? Transfusion 2009;49:829-37.
50. Tinmouth AT, Hare GMT, Mazer CD. The “sticky” business of “adherence” to transfusion guide-lines. Intensive Care Med 2010;36:1107-9.
51. Berner ES. Clinical decision sup-port systems: State of the art. AHRQ publication no. 09-0069-EF. Rockville, MD: Agency for Healthcare Research and Quality, 2009. [Available at http://healthit.ahrq.gov/images/jun09cdsreview/09_0069_ef.html (accessed February 18, 2013).]
52. Brennan PF. CPOE: Sufficient, but not perfect, evidence for taking action. J Am Med Inform Assoc 2007;14:130-1.
53. Adams ES, Longhurst CA, Pageler N, et al. Computerized physician order entry with decision support decreases blood transfusions in children. Pediatrics 2011;127:e1112-19.
54. Bates DW, Kuperman GJ, Wang S, et al. Ten commandments for effective clinical decision sup-port: Making the practice of evi-dence-based medicine a reality. J Am Med Inform Assoc 2003;10:523-30.
55. Scheurer DB, Roy CL, McGurk S, Kachalia A. Effectiveness of com-puterized physician order entry with decision support to reduce inappropriate blood transfusions. JCOM 2010;17:17-26. [Avail-able at http://w.turner-white.com/pdf/jcom_jan10_transfusions.pdf (accessed February 18, 2013).]
56. Chang C-S, Lin Y-C, Wu Y-C, et al. The effects of a computer-

TRANSFUSION GUIDELINES 23
ized transfusion decision support system on physician compliance and its appropriateness for fresh frozen plasma use in a medical center. Am J Clin Pathol 2011;135:417-22.
57. Sittig DF, Krall M, Dykstra RH, et al. A survey of factors affecting clinician acceptance of clinical decision support. BMC Med Inform Decis Mak 2006;6:6.
58. Haspel RL, Uhl L. How do I audit hospital blood product utiliza-
tion? Transfusion 2012;52:227-30.
59. Reece RL, Beckett RS. Epidemiol-ogy of single-unit transfusion. A one-year experience in a commu-nity hospital. JAMA 1966;195:801-16.
60. Tinmouth A, Macdougall L, Fer-gusson D, et al. Reducing the amount of blood transfused: A systematic review of behavioral interventions to change physi-cians’ transfusion practices. Arch Intern Med 2005;165:845-52.
24 THE TRANSFUSION COMMITTEE
Appendix 9-1. Transfusion Order Form in Use at St. Vincent Indianapolis Hospital Since 2001