
Transforming Healthcare in the US Virgin Islands….. Primary Healthcare.

Transforming Primary Care at Group Health Cooperative
March 2, 2010 | Robert Reid MD PhD, Group Health Research Institute
2nd National Medical Home Summit, Philadelphia PA

Presentation Goals
• Revitalizing primary care: the medical home imperative
• Defining the medical home at Group Health
• Getting from here to there: implementing practice redesign
• Our medical home learnings
• What’s next at Group Health?
2

About Group Health…
• Integrated health insurance & delivery system • Founded in 1946 • Consumer governed, non-profit • Membership: 628,000 Staff: 9,390 • Revenues (2008): $2.8 billion
• Integrated Group Practice • 26 primary care medical centers • 6 specialty systems, 1 hospital • ~900 physicians
• Contracted network • > 9,000 pracititioners, 39 hospitals
• Group Health Research Institute • 32 investigators • 235 active grants, $34 million (2008)
• Multispecialty Group Practice • 26 primary care medical centers • 6 specialty units, 1 hospital • 960 physicians
• Contracted network • > 9,000 practitioners, 39 hospitals
3

Revitalizing primary care

A little history…
• Since its origin, Group Health organized around primary care base
• Declines in financial performance & membership in early 2000s
• Reforms implemented to improve access, efficiency, productivity
• Reforms resulted in a faster “hamster wheel” (Tufano JGIM 2008;23:1778-83. Conrad HSR 2008;43:1888-1905.)
Defined practice populations Multi-disciplinary teams Specialty care gatekeeping Salaried physicians
“Advanced access” Same-day appointing Leaner primary care teams Direct specialty access EHR implementation Secure email messaging RVU-based productivity incentives (Ralston et al, Med Care Res Rev. 2009;66:703-24.)
5

The medical home imperative
Utilization Trends 1997-2005 by Quarter
Inpatient Days
Specialist Visits
Inpatient Admits
Primary Care Visits
ER Visits
Access & Efficiency Reforms
1997 1998 1999 2000 2004 2005 2002 2003 2001
Freq
uenc
y
6

Inpatient & ER Utilization Trends 1997-2005 by Quarter
Inpatient Days
ER Visits
Inpatient Admits
Access & Efficiency Reforms
1997 1998 1999 2000 2004 2005 2002 2003 2001
The medical home imperative Fr
eque
ncy
7

Increasing primary care physician burnout “...the way in which [care] is structured, it has shifted such an increased
amount of work onto primary care that it is not sustainable … I’m actually looking to get out of primary care because I can no longer work at this pace.”
“ The burnout rate among my colleagues is huge … those of us that have managed to retain some semblance of balance do it by almost unacceptable levels of compromise, either for ourselves or what we define as good enough care.” (Tufano et al, JGIM 2008;23:1778-83)
Looming primary care workforce crisis
• Many positions unfilled
• Full-time practice is now a rarity
• Primary care MDs retiring earlier than specialists
• Exit interviews show most common reason for separation: high workload
The medical home imperative
8

The medical home imperative
There just has to be a better way!
9

Revitalizing primary care
Traditional family practice values
+ 21st century information technology
Supported by consumers, physicians,
health plans, policy makers
The PCMH model:
Whole person care
across lifespan
Personalized, prevention-focused,
coordinated
Until now, little empirical
evidence of its
benefits
10

Revitalizing primary care
Physician - patient
relationship at the core
Coordination & collaboration with patients
Group Health PCMH design principles:
Proactive, comprehensive
care
Patient-centered access
24/7
Efficient, satisfying, effective
11

Revitalizing primary care
Panel size
1,800 2,300 PCMH design:
Clinical teams Desktop time E-technology
Appointments
20 min.
30 min.
12

Medical home change components
• Calls redirected to care teams • Secure e-mail • Phone encounters • Pre-visit chart review • Collaborative care plans • EHR best practice alerts • EHR prevention reminders • Defined team roles
Point-of-care changes • ED & urgent care visits • Hospital discharges • Quality deficiency reports • e-health risk assessment • Birthday reminder letters • Medication management • New patients
Patient-centered outreach
• Team huddles • Visual display systems • PDCA improvement cycles • Salary only MD compensation
Management & payment
PCMH Model
13

Planning and evaluation

PCMH timeline
15

PCMH prototype evaluation
Group Health Research Institute conducted a prospective, before-and-after evaluation comparing Prototype clinic with other Group Health clinics in western Washington
16

PCMH prototype evaluation
Patient experience
Staff burnout
Evaluation measures:
Quality Utilization Cost
17

PCMH prototype evaluation
One year evaluation results available from:
http://www.ajmc.com/issue/managed-care/2009/2009-09-vol15-n9
18

What have we learned?

Patient experience
Goal setting & tailoring
Patient activation & involvement
Helpfulness of office staff
Access
Coordination of care
Shared decision making
Quality of patient-doctor interactions
Year 1
Significantly higher scores for patients at PCMH prototype clinic
Compared to controls:
Difference not significant
PCMH Prototype significantly higher
PCMH Prototype significantly lower 20

** p<0.01
Staff burnout
Marked improvement in burnout levels at PCMH prototype clinic at 1 year
21

Patient Average
100% Performance
75% Performance
50% Performance
Baseline
12 month
Baseline
12 month
Baseline
12 month
Baseline
12 month
Medical Home Control Clinics
Quality of care
Composite measures based on 22 HEDIS indicators measured for each patient
22

Utilization Vi
sits
per
pat
ient
per
yea
r
(Note: mean utilization in first year of PCMH implementation estimated with GLM models, log link, Poisson error, adjusting for age, gender and baseline DxCG scores.)
Medical Home (n=8,094) Other Clinics (n=228,510)
*p<.05 *
*
*
*
*
*
23

Costs
(Note: mean PMPM patient care costs for first year of PCMH implementation estimated with GLM models, identity link, Gamma error, adjusting for age, gender and prior year costs.)
Medical Home (n=8,094) Other Clinics (n=228,510)
* **
*p<.05 ** p<.001
24

Takeaways

Patient-centered primary care saves costs by lowering inappropriate use of emergency care and avoiding preventable hospitalizations.
Investment in a medical home can achieve relatively rapid returns across a range of key outcomes.
The Group Health PCMH evaluation provides some of the first empirical evidence of the benefits of the medical home.
Preliminary analyses suggest that improvements during the first year for the most part were maintained during the second year.
The evaluation has led Group Health to spread the PCMH to all 26 of its medical centers.
PCMH evaluation takeaways
26
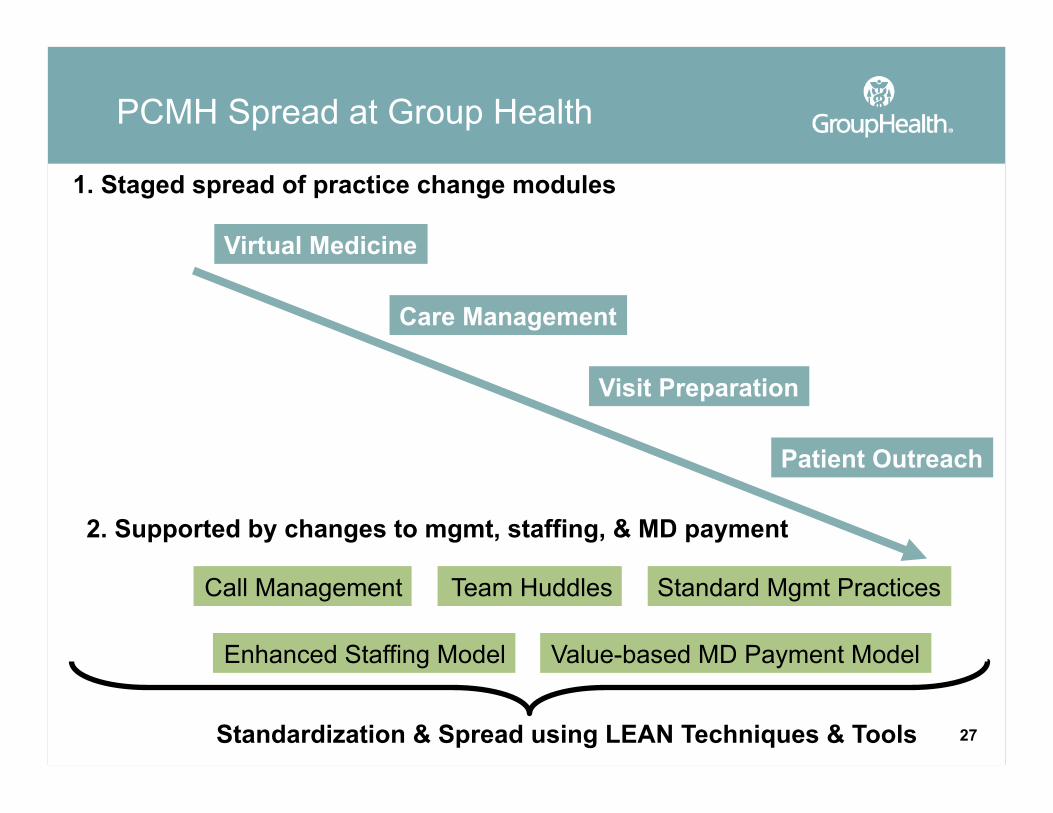
PCMH Spread at Group Health
Virtual Medicine
Care Management
Visit Preparation
Patient Outreach
1. Staged spread of practice change modules
Call Management Team Huddles Standard Mgmt Practices
Enhanced Staffing Model Value-based MD Payment Model
2. Supported by changes to mgmt, staffing, & MD payment
Standardization & Spread using LEAN Techniques & Tools 27

Questions?

Thank you


















