


Transforming america educaTion Through innovaTion Technology

Transforming Mental Health Care through Innovation
Ruth Wilson
Provide you with an understanding of how we are introducing and embedding innovation in Mental Health across Yorkshire and Humber
YHAHSN Mental Health team
• Vicky Vanes – Programme Manager
• Khalida Wilson – Programme Manager
• Ruth Wilson – Programme Lead
Our aim today

• Please spend 10 minutes discussing on your table and write your ideas on the post it notes provided
• What are the common themes?
What are the barriers to implementing innovations in mental health?

Our work includes:
• Encourage and support; innovators, use of quality improvement
• Signpost – sources of funding, possible collaborators
• Link health care providers, academia, commissioners and industry
• Work in partnership with local ICS and STPs
• Project management
• Provide evaluation
• Source expertise

Innovation to transform lives for people experiencing mental health challenges
CONNECT
We connect innovations to mental health needs enabling the NHS to use resources effectively and improve peoples lives
DELIVER
We provide solutions to improve the diagnosis, treatment and recovery of patients. These can be national, local or health system based
IDENTIFY
We align our priorities with the mental health needs of our population and national requirements

IDENTIFY – local priorities
National
• NHS England • NICE • Other AHSNs• NIA, ITP
Regional
• ICS/STP Mental Health Programme Boards and
Directors• Mental Health
Commissioners • Urgent and Emergency
Mental Health Network • Y&H Suicide Prevention
Collaborative • Local Universities
Third sector/patient view via YHAHSN
patient involvement
Analysis of population data eg
CYP, University Population, ASD
Local priorities

Use our networks and contacts we connect people with relevantinnovations. To help achieve this for digital innovations we willhold a series of events
CONNECT- people and ideas
24th June 2019 Y&H Mental Health Digital – Introduce a range of innovations that can be used to support mental health service delivery and personalise care
Local priorities will determine what events are next, for example
Subject based innovations – eg
Long Term Conditions
Age based innovations – eg
Children and Young People
Local system required innovations – e.g use of staff
resources
A new model of care using specialist police officers within community
mental health services to help support high intensity users struggling
with complex, behavioural disorders. This improves quality of life for
people and reduces costs to the local health and police systems.
In Yorkshire and Humber:
• The SIM Yorkshire team established in Doncaster is working with 5 high
intensity users.
• We have run workshops in North Yorkshire, Humberside and West
Yorkshire and are supporting local systems to identify the potential for
including the SIM approach in their care pathways for high intensity
users.
National Programme – Serenity Integrated Mentoring(SIM)

Chris Guest- Mental Health Practitioner/ SIMGulshan Akram- SY Police officer/ SIM

• HIU Have Clear Boundaries set.
• HIU appreciate the extra support from Police.
• Consistent Multi-Agency Approach ie A&E, Ambulance, MH and Police.
• HIU is no longer going into crisis before receiving help –Monitored continuously.
• MH and Police based in the same office.
Benefits

• NO 136 admissions
• Reduced GP and A&E admissions.
• Better relationship between Police and the Users
• All agencies are consistent in their approach, have not previously worked in this way.
In the first quarter of SIM Yorkshire:

Source: SIM Yorkshire team

• 24 year old gentleman
• Experience of childhood trauma
• Frequent attendance of NHS service -171 A/E attendance since March 2018- O/D, chest pain
• Various possible mental health diagnosis Emotional unstable personality disorder, PTSD, Anxiety
• Pre-occupied by health anxieties
• Police involvement – charged with assault/ drunk and disorderly
Client A, Case study


Consistent Approach
SIM Plan &
Mentoring
Mental Health Crisis Team
South Yorkshire
Police
Yorkshire Ambulance
Service
A&E

• Promote the spread and adoption of a physical health check template and Elearning module to help primary care deliver physical health checks and therefore improve health for people with a serious mental illness (SMI)
• Funding targeted support to train primary staff in using the template for local ICS/STPs
• Supporting NHS E in further development of the template for primary care
• Evaluating impact of template use, on health checks and interventions for people with SMI
Local Programme – Mental Health Physical Health

You & Your Carewww.bdct.nhs.uk
Improving the Quality of Physical Health Checks for people with SMI
Ruth WilsonProgramme Manager
Yorkshire & Humber, Academic Health Science Network
Kate DaleMental/Physical Health Project Lead (Y&H AHSN)
Bradford District Care NHS Foundation Trust (Honorary)

You & Your Carewww.bdct.nhs.uk
Addressing health inequalities for SMI population initially Bradford & Airedale
• A more specific standardised data entry template based on existing mental health QOF indicator
• Specific to areas of physical health risks prevalent to those with SMI
• More specific tests e.g. blood tests for diabetes, cholesterol, ECG and other appropriate tests
• Auditable across the whole city using the SystmOne primary care information system

You & Your Carewww.bdct.nhs.uk
Health Need FYFVMH• Shorter lifespan, reduced by around 20 years compared to the
general population - one of the greatest health inequalities in England
• Two thirds of these deaths are from avoidable physical illnesses, including heart disease and cancer, many caused by smoking
• Lack of access to physical healthcare for people with mental health problems – less than a third of people with schizophrenia in hospital received the recommended assessment of cardiovascular risk in the previous 12 months

You & Your Carewww.bdct.nhs.uk
Health Need: MH / PH, Audit Findings
• No patients had been given a cardiovascular risk calculation
• This would be a good way to identify high risk people for prevention
• No patients had a blood test for prolactin levels
• Elevated prolactin is a significant and common adverse effect of antipsychotic treatment

You & Your Carewww.bdct.nhs.uk

You & Your Carewww.bdct.nhs.uk
The SystmOne Physical Health Check Template

You & Your Carewww.bdct.nhs.uk

You & Your Carewww.bdct.nhs.uk
IMPACT: Bradford
• Rolled out to all GP practices in Bradford & Airedale
• Replicated on different IT systems
• Replicated in secondary care using RIO
• Rolled out in all in patient areas
• SHARED CARE: Communicated to GP electronically for inpatient discharges

You & Your Carewww.bdct.nhs.uk
Regional & National spread – enabled by Y&H AHSN
“By 2020/21, at least 280,000 people living with severe mental health problems
should have their physical health needs met”
FYFV MH
Priority action for the NHS by
2020 /21
FYFV MH
Project sponsored
and championed
by MH CEOs
across Y&H

You & Your Carewww.bdct.nhs.uk
YEAR 1 PILOT: SWYPFT
https://www.youtube.com/watch?v=2KNaZzEqgnM
You & Your Carewww.bdct.nhs.uk
Real impact for patients
“One of the things that
really impressed us… was
how well integrated it was
into people’s everyday
practice and the way in
which it integrated with
Primary Care”
Adrian Berry, Medical Director at
SWYPFT, August 2016
One pilot site saw a
372%
increase in physical
health checks
targeting
preventable
deaths
reducing
health
inequalities

You & Your Carewww.bdct.nhs.uk
Real impact for patients: YEAR 1 PILOT, SWYPFT
• Adopted RIO Version of Template
• Robust polices and procedures to support PH assessments
• PH clinics operationalised
• Developed training regime
• Improvements can now be monitored
• Strategic intention - roll out to a further 8/10 SWYPFT sites
Within six-weeks
130 patients received a
comprehensive physical health check

You & Your Carewww.bdct.nhs.uk
National Transformation: Health Economics Evaluation

You & Your Carewww.bdct.nhs.uk
National Transformation: Health Economics Evaluation
VALUE
across the
system
with
47,713
health
checks (YHEC, September 2016)
Potential cost saving for
Y&H
£11.3m

You & Your Carewww.bdct.nhs.uk
National Transformation: Template published for use
SystmOne:Template published at the end of December 2015
Over 2,700 GP practices using SystmOne
EMIS Web:Template published May 2016
Over 3,000 GP practices use EMIS Web
Real impact for patients, across the country.

You & Your Carewww.bdct.nhs.uk
National Transformation: Elearning Module
ELearning module to support implementation of robust MH / PH programmes using the Bradford Physical Health Assessment Tool

You & Your Carewww.bdct.nhs.uk
Toolkit for spread
• Incentive schemes for GPs to encourage monitoring of physical health
• Continue efforts to reduce smoking - one of the most significant causes of poorer physical health for this group
• Identify National Champions for MH / PH
Former National Clinical Director for Mental Health Dr Geraldine Strathdee is a major advocate for this
programme

You & Your Carewww.bdct.nhs.uk
Thank you very much for listening
Contact details:
Ruth [email protected]

• Telemedicines and quality improvement project focused on the use of telemedicine in addictions clinics in Humber
• Working across three mental health trusts in South Yorkshire and Bassetlaw to facilitate the implementation of workforce transformation in the ADHD and Autism pathway.
• Scoping work to identify key concerns in patient safety from people with lived experience of mental health and learning disability and their carers across West Yorkshire
Local System Transformation

Dr Soraya MayetConsultant Psychiatrist Humber Teaching NHS FT
Honorary Senior Clinical Lecturer Hull and York Medical School
Opioid Dependence Heroin dependence is a chronic relapsing condition
High risk of death through accidental overdose
Opioid substitution treatment (OST)
Prevents deaths
Reduces and stopping heroin use
Reduces and stops injecting & spread of Hep C and HIV
Reduces criminal offences
Improved effectiveness with psychosocial interventions

Addiction Prescriber Reviews Patients prescribed OST should have an addictions prescriber review
three monthly (DH 2017)
Holistic assessment and medication safety
Non-attendance high in addictions services nationally
Local audit found 53% of patients attended
Quality improvement work increased this to 72%

Improving attendance 100 prescriber appointments missed per month
So fewer appointments available for other patients
Extra costs associated with non attendance
We wanted to look at ways of improving attendance


Could telemedicine help? Use of telecommunications technology to provide clinical health care from
a distance
‘Overcome geographical barriers, and increase access to health care services’
Address challenges in providing accessible, cost effective, high-quality health care (WHO)

Evidence for telemedicine Cost effective
Reduce travel time and costs
Improve access to healthcare
Improve patient satisfaction
But limited research with addictions and none in UK
Why Telemedicine in Addictions?
East Riding of Yorkshire >900 square miles
Hub and Spoke (outreach) Addictions service
Three Hubs in Hull, Bridlington and Goole
Patients seen in spoke sites near home
But few addictions prescribers
Patients mainly travel to Hubs to see prescribers
Some outreach prescriber clinics


Aims
To assess whether telemedicine in addictions:
Increases attendance rates
Improves patient and staff satisfaction
Involves less travel
Reduces costs due to less travel
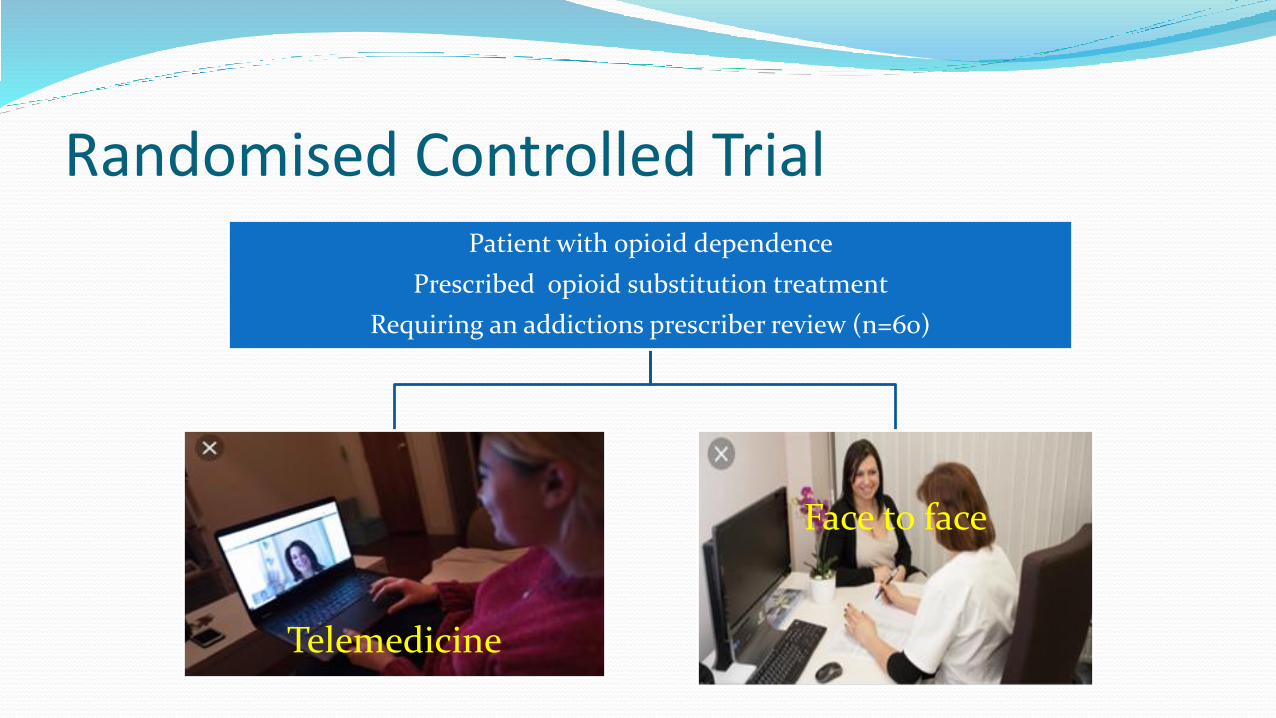
Randomised Controlled TrialPatient with opioid dependence
Prescribed opioid substitution treatment
Requiring an addictions prescriber review (n=60)
Telemedicine
Face to face

Work so far Meetings with collaborators (University of Hull, HYMS)
Patient and Staff Involvement co-produce research design
University of Hull Research Design Service and stats advice
Academic Health Science Network support
Humber Teaching FT Trust governance approvals
IT support for internet at sites, technology and software
Permission for software and software testing completed
Protocol development
Ethical approval application almost complete

To co-produce the research design

Patient Involvement Why do you think patients miss appointments?
They feel unwell
Costs a £9.40 return
Money could be used to “score”
Don’t feel they need appointment
Forget

Patient Involvement What do you think would help patients attend
appointments?
Appointments coincide with payment of benefits
More text alerts
Closer to their home
Afternoon appointment

Patient Involvement What are your thoughts on telemedicine project?
It would cut down travel and less travel time
But might still want a face to face review
Good if you want to reduce dose

Patient Involvement What do you think of the project design?
Overall positive reaction.
Could save NHS money and time
Could help people attend training
Quicker and easier treatment

Funding Yorkshire and the Humber Academic Health Science Network
East Riding of Yorkshire CCG Small Grants
Project not possible without this funding

We work with innovations in Mental Health to accelerate the spread and adoption of those that meet the needs of our local population and their health challenges
Examples can be found here https://www.yhahsn.org.uk/hie/
Working with innovations

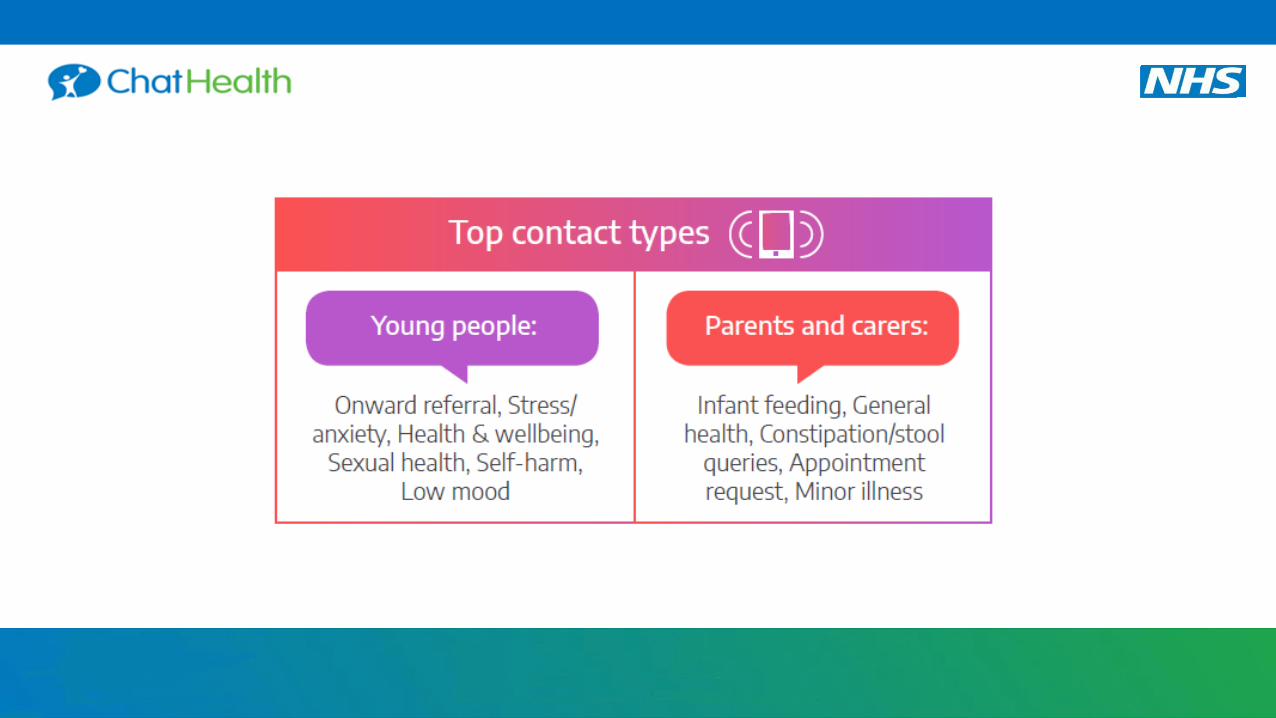
MESSAGING SERVICE

CLINICIAN’S THOUGHTS ON RISK IN MESSAGING …

• Imminent high risk
• 24/7
• Shared responsibility
• Availability changes
• Missed messages
• Excessive record keeping
• Identity verification
CLINICIAN’S THOUGHTS ON RISK IN MESSAGING …
Young people 16-24 yrs MOST likely to report suicidal thoughts. Cases of depression and self harm
have doubled. Number of anti depressants prescribed in the UK is at its highest.

• Imminent high risk
• 24/7
• Shared responsibility
• Availability changes
• Missed messages
• Excessive record keeping
• Identity verification
• Vacancies - 11% and rising
Clinicians thoughts on
risk in messaging

FOLLOW US
PATIENTRECORD

In 2018/2019:
CLINICIAN’S THOUGHTS ON RISK IN MESSAGING …

63
UK spread



Have we broken down any barriers?

• What can you do?
• What can your organisation do?
• Follow our progress - https://www.yhahsn.org.uk/
What can you do?

Thankyou


















