Transformed lymphoma: biology and treatment - … lymphoma: biology and treatment Silvia Montoto...
29
Transformed lymphoma: biology and treatment Silvia Montoto Centre for Haemato-Oncology Barts Cancer Institute www.cancer.qmul.ac.uk
Transcript of Transformed lymphoma: biology and treatment - … lymphoma: biology and treatment Silvia Montoto...

Transformed lymphoma:biology and treatment
Silvia MontotoCentre for Haemato-Oncology
Barts Cancer Institute
www.cancer.qmul.ac.uk

Years
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
0.00
0.25
0.50
0.75
1.00
N =330
Years
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
0.00
0.25
0.50
0.75
1.00
N =330
40
50
60
70
80
90
100
%V
iability
www.cancer.qmul.ac.uk
Observation Experiments Treatment
0
10
20
30
0.01 0.1 1 10 100 1000
Concentration (uM)

Information
Problem
Solution
www.cancer.qmul.ac.uk

Histological transformation (HT)
• Frequent event
• Change in histology
The problem
• Change in clinical course
• Poor prognosis
www.cancer.qmul.ac.uk
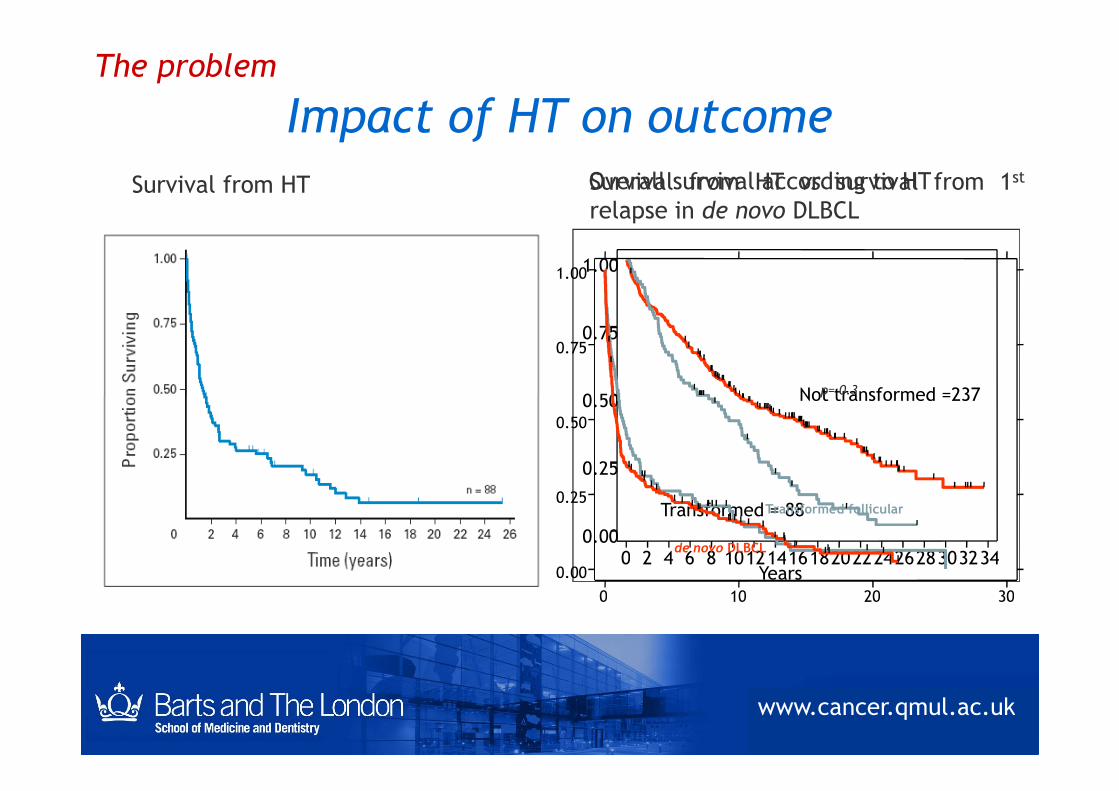
Impact of HT on outcome
Survival from HT
0.50
0.75
1.00
Not transformed =237
Overall survival according to HT
0.75
1.00
p= 0.3
Survival from HT vs survival from 1st
relapse in de novo DLBCL
The problem
Years0 2 4 6 8 10121416182022242628303234
0.00
0.25
0.50 Not transformed =237
Transformed = 88
0 10 20 30
0.00
0.25
0.50
Transformed follicular
de novo DLBCL
p= 0.3
www.cancer.qmul.ac.uk

How to improve the outcome of tFL
• Reduce the risk of HT
– What patients are at high risk of HT?
– Does the initial management impact on the risk ofHT?
The problem
• Improve the response at the time of HT
– Does initial management impact on the outcomeafter HT?
– What is the best treatment at the time of HT?
www.cancer.qmul.ac.uk

Treatment of tFL• Heterogeneous population:
– Number of previous treatment lines
– Type of previous treatment
• Investigational trials:
The problem
• Investigational trials:
– Excluded from FL studies
– Excluded from DLBCL studies
• Data extrapolated from DLBCL studies
www.cancer.qmul.ac.uk
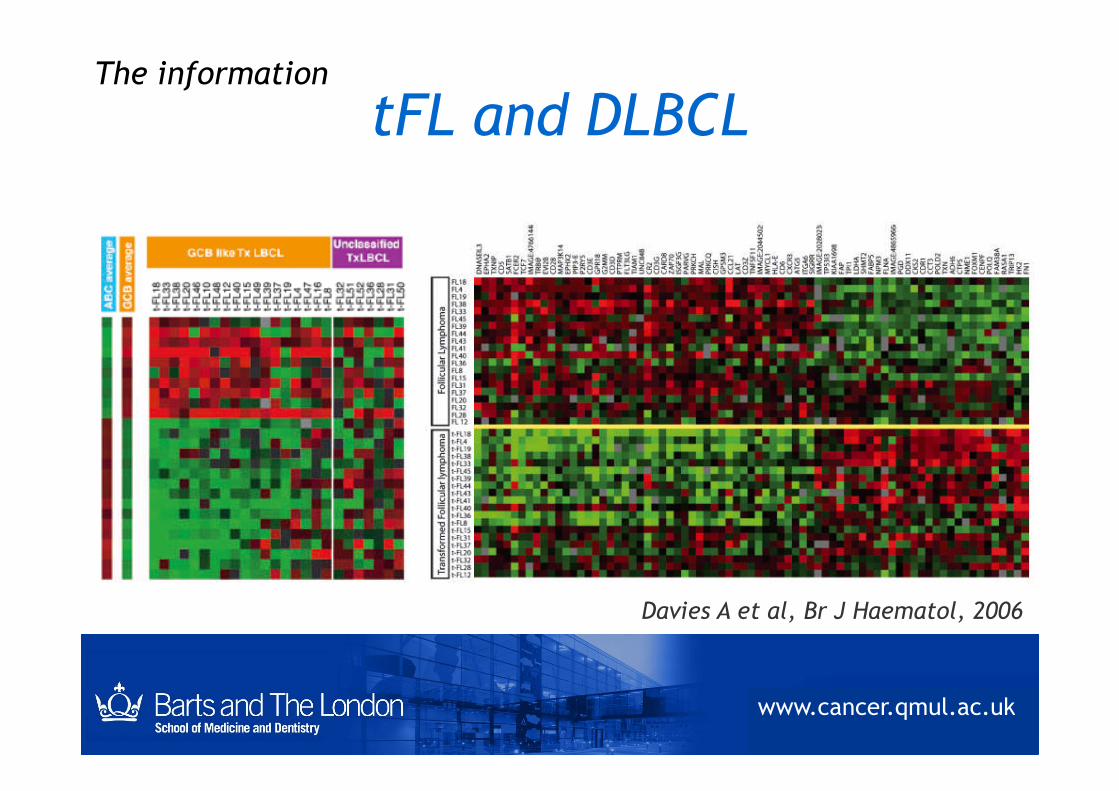
tFL and DLBCLThe information
Davies A et al, Br J Haematol, 2006
www.cancer.qmul.ac.uk

Impact of initial management on the risk of HT
Series Risk of HT
Hubbard (1982) RT ↑ risk of HT
Acker (1983) No impact
The information
Horning (1984) No impact of expectant management
Giné (2006) No impact of CB-CVP vs CHOP
Montoto (2007) Expectant management ↑ risk of HT
www.cancer.qmul.ac.uk

Impact of initial therapy on the risk of HTThe information
Prospective randomised study:PCOP vs PACOP
The addition of doxorubicin doesNOT influence the risk of HT
www.cancer.qmul.ac.uk
Lepage et al, HematologicalOncology, 1990
Al-Tourah et al, JCO, 2008
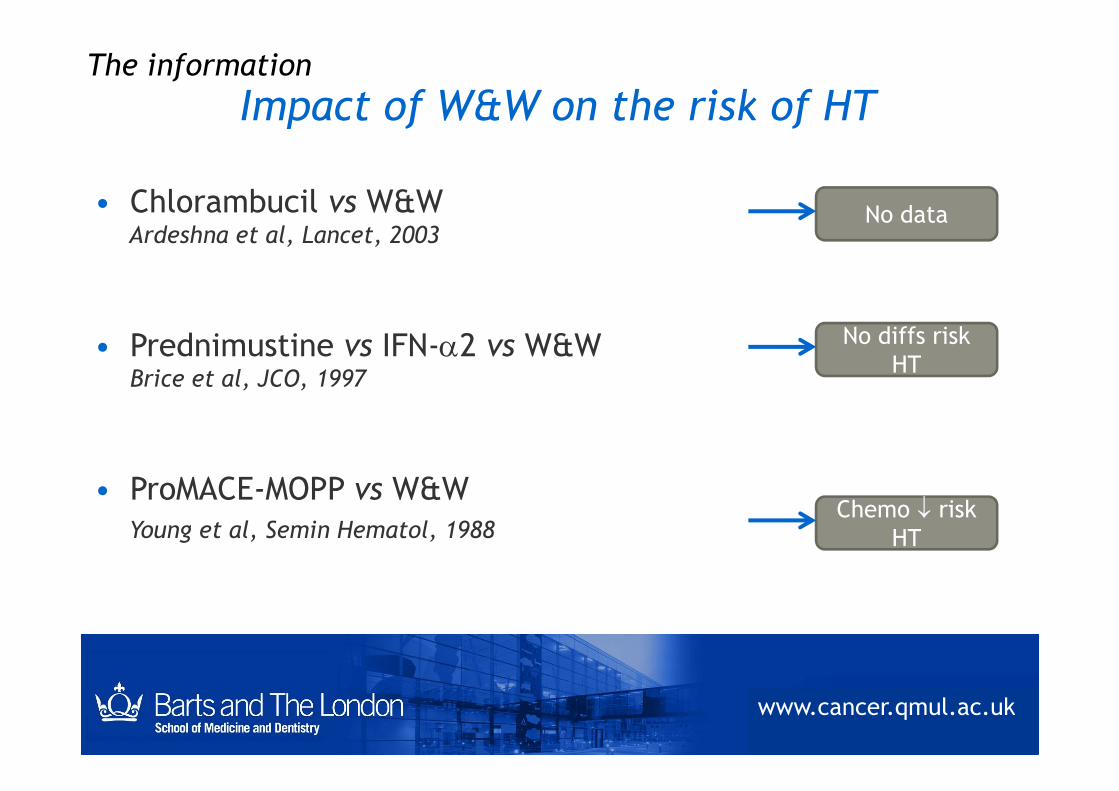
Impact of W&W on the risk of HTThe information
• Chlorambucil vs W&WArdeshna et al, Lancet, 2003
• Prednimustine vs IFN-2 vs W&WBrice et al, JCO, 1997
No data
No diffs riskHT
www.cancer.qmul.ac.uk
• ProMACE-MOPP vs W&WYoung et al, Semin Hematol, 1988
Chemo riskHT

Treatment for HT
= treatment for DLBCL (in most cases) CHOP-R
BUT…CHOP-R already given at the time of HT
The information
AND…outcome of tFL DLBCL at relapse
2nd line chemotherapy for DLBCL?
www.cancer.qmul.ac.uk

Treatment for HTSeries Treatment at HT SFT (median)
Hubbard (1982)63% combinationchemotherapy
11 mo
Yuen (1995) 60% doxo-containing chemo 22 mo
The information
Bastion (1997) 58% CHOP-like 7 mo
Giné (2006)23% CHOP
57% VIA, MINE/ESHAP1.2 yrs
Montoto (2007) 73% doxo-containing chemo 1.2 yrs
www.cancer.qmul.ac.uk

Treatment for HT: CHOP-RThe information
1.0
.8
.6
CHOP-R (N= 23) 5yr OS: 61%
CHOP-like (N= 85) 5yr OS: 33%
Courtesy of Joseph M Connors and Abdul Al-Tourah, unpublished data
www.cancer.qmul.ac.uk
14121086420
.4
.2
0.0
CHOP-like (N= 85) 5yr OS: 33%
p= 0.01

Improvement over timeThe information
www.cancer.qmul.ac.uk
Tam et al, ICML-10 Lugano 2008
• Chemoterapy-naïve patients• Rituximab at HT

Non-CHOP-R treatments for HT
Treatment Series N
(tFL/total)
Previous
rituximab
RR HDT EFS/TTF
MINE/ESHAP Rodriguez
1995
14/92 - 64%
(HT)
No Median TTF: 8mo (HT)
Mini-BEAM Girouard 18/104 - 50% 37% -
The information
Mini-BEAM Girouard
1997
18/104 - 50%
(HT)
37% -
R-EPOCH Jermann
2004
18/50 8/50 68% 61% Median EFS: 12mo (HT)
No detailed data on results with ICE/R-ICE in patients with HT
www.cancer.qmul.ac.uk
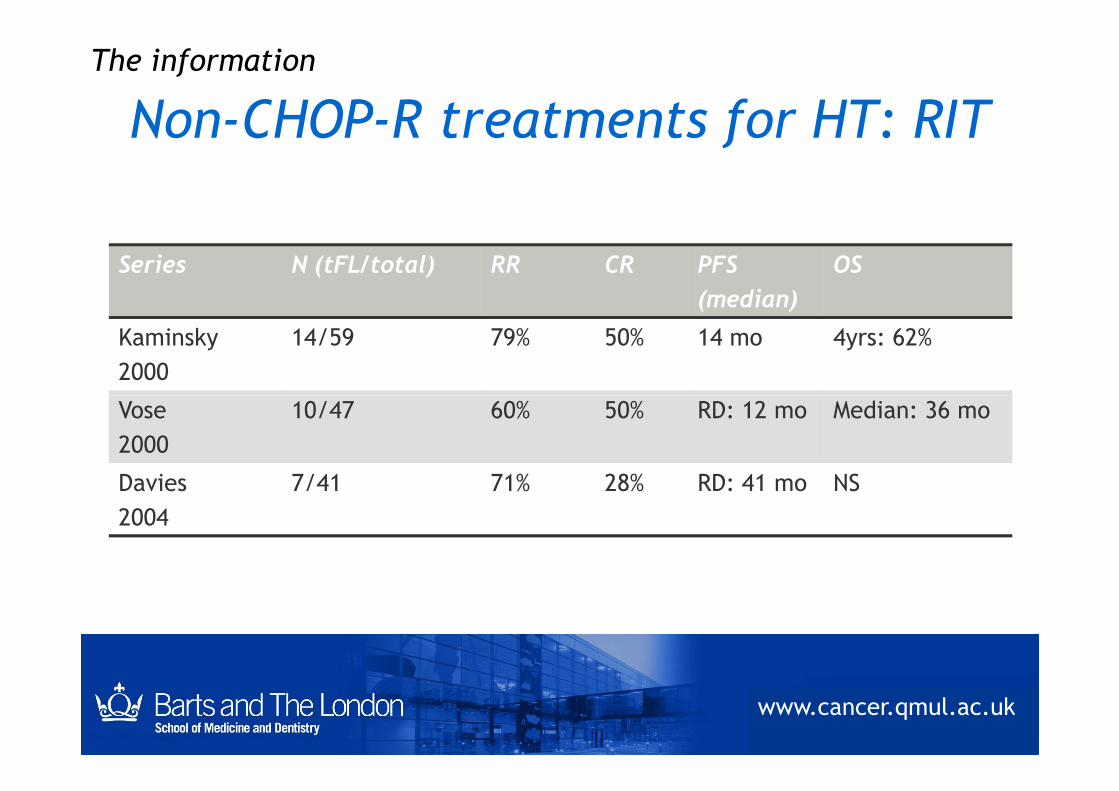
Non-CHOP-R treatments for HT: RIT
Series N (tFL/total) RR CR PFS
(median)
OS
Kaminsky
2000
14/59 79% 50% 14 mo 4yrs: 62%
Vose 10/47 60% 50% RD: 12 mo Median: 36 mo
The information
Vose
2000
10/47 60% 50% RD: 12 mo Median: 36 mo
Davies
2004
7/41 71% 28% RD: 41 mo NS
www.cancer.qmul.ac.uk
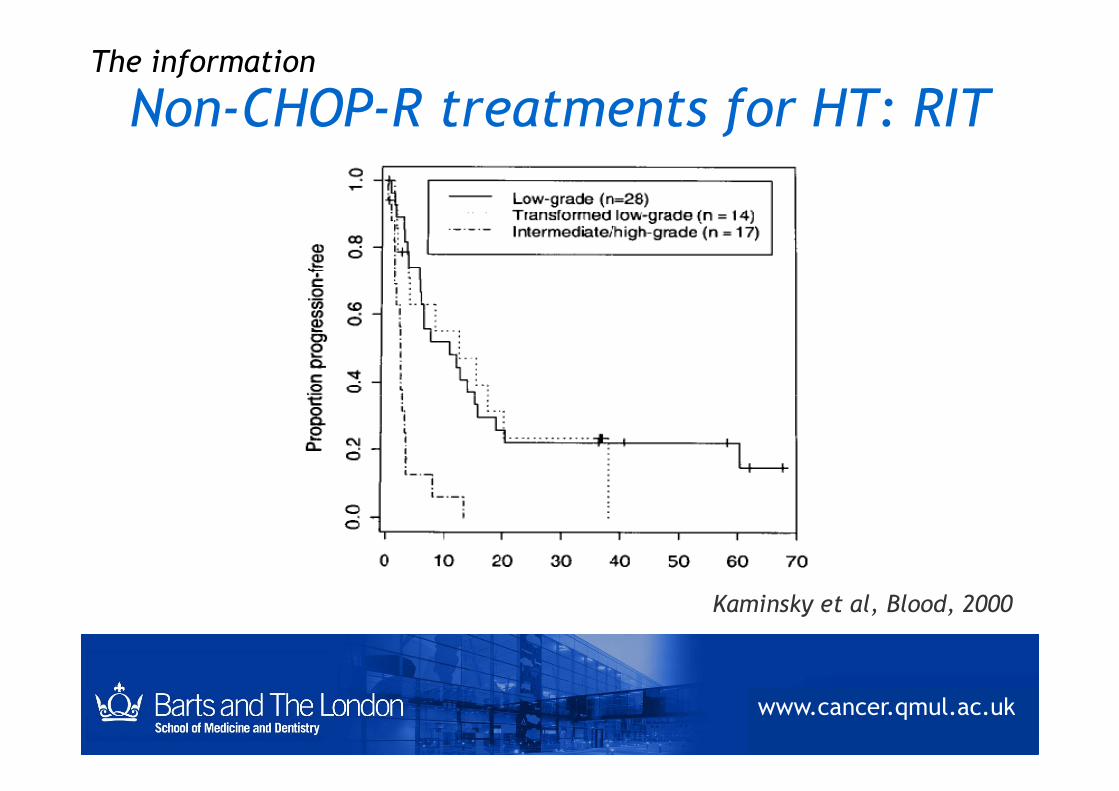
Non-CHOP-R treatments for HT: RITThe information
Kaminsky et al, Blood, 2000
www.cancer.qmul.ac.uk

Non-CHOP-R treatments for HT:lenalidomide
The information
Patients N RR CR/CRu PFS
(median)
All patients 33 45% 21% 5 mo
Czuczman et al, BJH, 2011
www.cancer.qmul.ac.uk
tFL 23 56% 26% 8 mo
tCLL/SLL 7 0 0 2 mo

Treatment for HT: autologous SCT
The information
Williams et al, JCO, 2001
www.cancer.qmul.ac.uk

Treatment for HT: autologous SCTThe information
0.50
0.75
1.00
Pro
babil
ity
FL (N: 50)
Montoto et al, ICML-2011
www.cancer.qmul.ac.uk
Time (years)0 5 10 15
0.00
0.25
p: NS
Pro
babil
ity
tFL (N: 30)
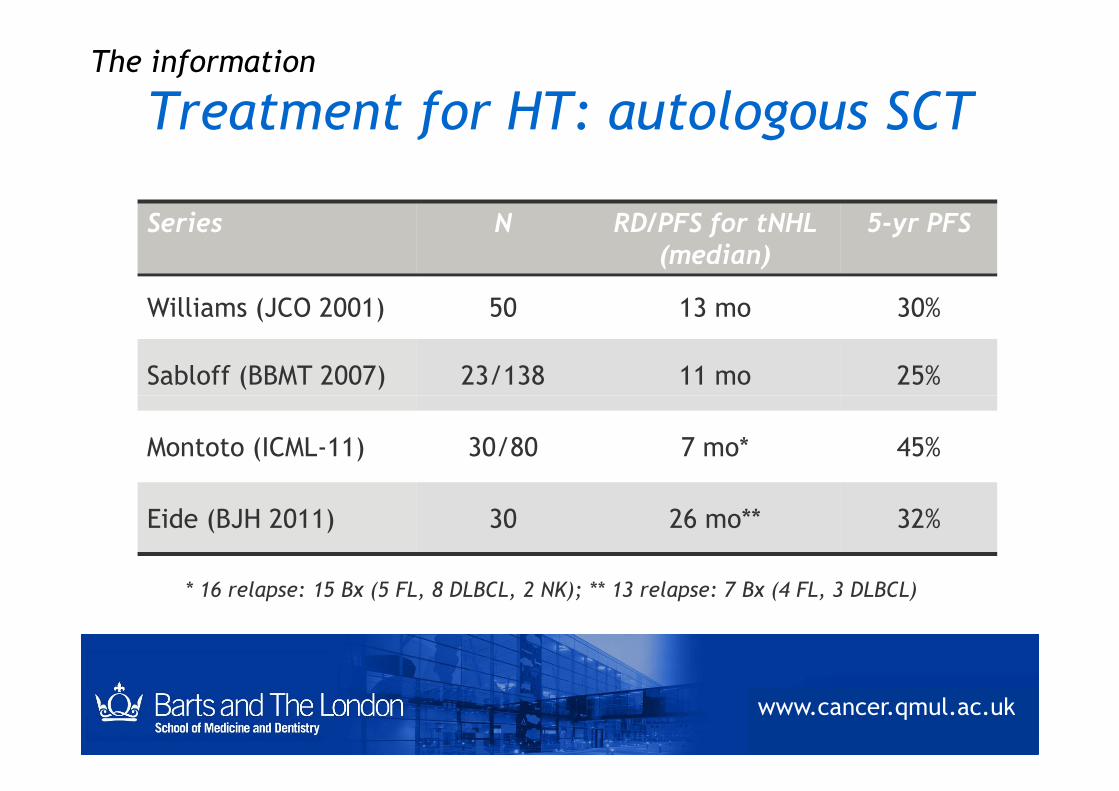
Treatment for HT: autologous SCTThe information
Series N RD/PFS for tNHL(median)
5-yr PFS
Williams (JCO 2001) 50 13 mo 30%
Sabloff (BBMT 2007) 23/138 11 mo 25%
www.cancer.qmul.ac.uk
Montoto (ICML-11) 30/80 7 mo* 45%
Eide (BJH 2011) 30 26 mo** 32%
* 16 relapse: 15 Bx (5 FL, 8 DLBCL, 2 NK); ** 13 relapse: 7 Bx (4 FL, 3 DLBCL)

Treatment for HT: allotransplantThe information
Rezvani et al, JCO, 2008
www.cancer.qmul.ac.uk
Thomson et al, JCO, 2009

Open questions in the treatment of HT
• Do doxo-containing regimens decrease the
risk of HT?
• Do patients NEED doxo-containing regimens
The information
at the time of HT?
• Is HDT necessary for all patients with HT?
• Can something different be done?
www.cancer.qmul.ac.uk

Answers
• Risk of HT as an end-point in randomised
trials
• Include HT in trials for ‘aggressive’
lymphomas
: how to get themThe solution
lymphomas
• Search for specific molecular therapeutic
targets
www.cancer.qmul.ac.uk

Years
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
0.00
0.25
0.50
0.75
1.00
N =330
Years
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34
0.00
0.25
0.50
0.75
1.00
N =330
40
50
60
70
80
90
100
%V
iability
www.cancer.qmul.ac.uk
Observation Experiments Treatment
0
10
20
30
0.01 0.1 1 10 100 1000
Concentration (uM)

What we do at Barts:
Treat as DLBCL:• R-CHOP (if no prior doxo)• 2nd line chemo for DLBCL• HDT unless:
little prior treatmentlocalised disease (?)

Maintenance rituximab for HT?
HT is an exclusion criteria in:
• Studies of maintenance after first-line:
Ghielmini, Blood 2004
Hochster, JCO 2009
The information
Salles, Lancet 2011
• Studies of maintenance at relapse:
Ghielmini, Blood 2004
Van Oers, Blood 2006
www.cancer.qmul.ac.uk

Maintenance rituximab for HT:maintenance rituximab in DLBCL?
The information
After CHOP-R After HDT in first-line
www.cancer.qmul.ac.uk
Haberman et al, JCO, 2006 Haioun et al, Annals of Oncology, 2009