Transcranial Doppler Ultrasound for the Assessment of...
11
TranscranialDopplerUltrasoundfortheAssessmentof IntracranialArterialFlowVelocity-Part1 ExaminationTechniqueandNormalValues M .Hennerici, M .D ., W .Rautenberg, M .D ., G .Sitzer, M .D ., andA .Schwartz,M .D . DepartmentofNeurology,UniversityMedicalSchool,Dusseldorf,FederalRepublicofGermany Henncrlci M, Raurenberg W, SitzerG,Schwartz A . Transcranial Dopplerultrasoundfurtheassessmentofintracranialarterial flow velocity-part . Examinationtechniqueandnormalvalues . Sung Neurol 1987 ;27 :439-48 . Wepresenttheexaminationtechniqueandnormalvalues offlowvelocityfromintracranialbasalcerebralarteries forarecentlydevelopedpulsedDopplersystemoperating at2 MHz emittingfrequency .Peaksystolic,peakdia- stolic,andmeanflowvelocityvaluesareanalyzedfrom fast-Fouriertransformed(FFT)Dopplerspectraatse- lecteddepthsfor50presumednormalsubjectsranging inagefrom22to79years .Interindividualvariationis highforpeakflowbutmoderateformeanflowvelocity values,whichhencearemorelikelytodiscriminatenor- malfromabnormal .Flowvelocityvalueswithinthepos- teriorcerebralartery(PCA)andthebasilarartery(BA) aresignificantlylowerthanintheanteriorcerebralartery (ACA)andthemiddlecerebralartery(MCA),whichis alsouniqueinshowingsignificantlydecreasingvalueswith increasingage :calculatedmeanflowvelocitiesare47 .3 ±13 .6and45 .3t13 .5cruiserintheACA,and58 .4J- 8 .4and44.7±11 .1cm/secintheMCAinpatients<40 yearsand>60years,respectively,but34 .2±7 .8and29 .9 9 .3(PCA)(patients<40yearsandpatients>60years), and34 .9±7 .8and30 .5±12 .4(BA)(patients<40years andpatients>60years) .Anewscanningsystemisintro- duced,whichwesuggestwillreduceinterindividualvari- ationsandimprovetheaccurateseparationofnearbyves- sels,whicharemajorcausesforthecomparativelylarge standarddeviationsatpresent . KEYWORDS : TranscranialDopplerultrasound ;PulsedDop- pler ;Intracranialcerebralarteries ;Cerebralbloodflow AlthoughFreundandKapp[71describedanoninvasive methodforexaminingintracranialarterialpulsationsby ultrasoundin1966,andalthoughduringthelastdecade Addressreprintrequeststo : Dr. M . Hennerici,Neurologische Cniv- ersitatsklinik, Moorensrrasse 5, D-4000Dusseldorf 1, FederalRe- public of Germany . 1987byElsevierSciencePublishingCo .,Inc . SurgNeurol 439 1987 ;27 :439-48 continuous-wave(CW)andpulsed-wave(PW)Doppler techniques(4-10MHz)havebeenextensivelyreported asprovidingaccurateevaluationofextracranialarterial obstructivelesions[3,4,9,11,12,211,theapplicationof noninvasiveultrasoundformeasurementofintracranial cerebralarterialflowhasbeenimpeded,mainlybythe propertiesofbone,whichrepresentanimportantob- stacletothepenetrationofultrasound .Attenuationof theultrasonicwaveneartheskullhasresultedinweak orbarelyreproduciblereflections,makingadequatere- cordingsofbloodflowvelocitiesfromintracranialar- tcricsimpossible . In1982Aaslidetal[2]introducedahigh-energy bidirectionalpulsedDopplersystemoperatingatlower frequencies(1-2MHz),which,forthefirsttime,en- abledareliablemeasurementofflowvelocityfromdis- tinctcerebralarteriesatthebaseoftheskull .Thismethod wassuggestedtobeusefulforevaluationofthecerebral circulationinvascularocclusivediseaseaswellasfor thedetectionofvasospasmaftersubarachnoidhemor- rhage[1,8,15,19) . Thepresentstudydescribestheexaminationtech- niquedevelopedforidentificationoftheintracranial carotid(ICA),middlecerebral(MCA),anteriorcerebral (ACA),posteriorcerebral(PCA),intracranialvertebral (VA), andbasilararteries (BA) . Italsoincludesnormal referencevalues(hithertounknown)of50presumed healthysubjectsfromdifferentaspectsofthefast-Four- iertransformed(FFT)Dopplerspectra. Patients,Methods,and ExaminationProcedure Patients Fiftypresumedhealthysubjects,ranginginagefrom22 to79years(24menand26women),werestudied . Neithertheirhistorynoraneurologicexaminationre- vealedanysignsorsymptomsofcerebrovasculardis- ease .Inaddition,extracranialCW-Dopplerultrasound examinationfortheevaluationofbothcarotidandver- 0090-30]91871$350
Transcript of Transcranial Doppler Ultrasound for the Assessment of...

Transcranial Doppler Ultrasound for the Assessment ofIntracranial Arterial Flow Velocity-Part 1Examination Technique and Normal Values
M. Hennerici, M.D., W . Rautenberg, M.D ., G. Sitzer, M .D., and A . Schwartz, M .D .Department of Neurology, University Medical School, Dusseldorf, Federal Republic of Germany
Henncrlci M, Raurenberg W, Sitzer G, Schwartz A . TranscranialDoppler ultrasound fur the assessment of intracranial arterial flowvelocity-part . Examination technique and normal values . SungNeurol 1987 ;27 :439-48 .
We present the examination technique and normal valuesof flow velocity from intracranial basal cerebral arteriesfor a recently developed pulsed Doppler system operatingat 2 MHz emitting frequency . Peak systolic, peak dia-stolic, and mean flow velocity values are analyzed fromfast-Fourier transformed (FFT) Doppler spectra at se-lected depths for 50 presumed normal subjects rangingin age from 22 to 79 years . Interindividual variation ishigh for peak flow but moderate for mean flow velocityvalues, which hence are more likely to discriminate nor-mal from abnormal . Flow velocity values within the pos-terior cerebral artery (PCA) and the basilar artery (BA)are significantly lower than in the anterior cerebral artery(ACA) and the middle cerebral artery (MCA), which isalso unique in showing significantly decreasing values withincreasing age : calculated mean flow velocities are 47 .3± 13.6 and 45 .3 t 13.5 cruiser in the ACA, and 58 .4 J-8.4 and 44.7 ± 11 .1 cm/sec in the MCA in patients <40years and >60 years, respectively, but 34 .2 ± 7 .8 and 29 .9
9 .3 (PCA) (patients <40 years and patients >60 years),and 34 .9 ± 7.8 and 30.5 ± 12 .4 (BA) (patients <40 yearsand patients >60 years) . A new scanning system is intro-duced, which we suggest will reduce interindividual vari-ations and improve the accurate separation of nearby ves-sels, which are major causes for the comparatively largestandard deviations at present .
KEY WORDS : Transcranial Doppler ultrasound ; Pulsed Dop-pler ; Intracranial cerebral arteries ; Cerebral blood flow
Although Freund and Kapp [71 described a noninvasivemethod for examining intracranial arterial pulsations byultrasound in 1966, and although during the last decade
Address reprint requests to : Dr. M. Hennerici, Neurologische Cniv-ersitatsklinik, Moorensrrasse 5, D-4000 Dusseldorf 1, Federal Re-public of Germany .
1987 by Elsevier Science Publishing Co., Inc .
Surg Neurol
4391987;27 :439-48
continuous-wave (CW) and pulsed-wave (PW) Dopplertechniques (4-10 MHz) have been extensively reportedas providing accurate evaluation of extracranial arterialobstructive lesions [3,4,9,11,12,2 11, the application ofnoninvasive ultrasound for measurement of intracranialcerebral arterial flow has been impeded, mainly by theproperties of bone, which represent an important ob-stacle to the penetration of ultrasound . Attenuation ofthe ultrasonic wave near the skull has resulted in weakor barely reproducible reflections, making adequate re-cordings of blood flow velocities from intracranial ar-tcrics impossible .
In 1982 Aaslid et al [2] introduced a high-energybidirectional pulsed Doppler system operating at lowerfrequencies (1-2 MHz), which, for the first time, en-abled a reliable measurement of flow velocity from dis-tinct cerebral arteries at the base of the skull. This methodwas suggested to be useful for evaluation of the cerebralcirculation in vascular occlusive disease as well as forthe detection of vasospasm after subarachnoid hemor-rhage [1,8,15,19) .
The present study describes the examination tech-nique developed for identification of the intracranialcarotid (ICA), middle cerebral (MCA), anterior cerebral(ACA), posterior cerebral (PCA), intracranial vertebral(VA), and basilar arteries (BA) . It also includes normalreference values (hitherto unknown) of 50 presumedhealthy subjects from different aspects of the fast-Four-ier transformed (FFT) Doppler spectra.
Patients, Methods, andExamination ProcedurePatients
Fifty presumed healthy subjects, ranging in age from 22to 79 years (24 men and 26 women), were studied .Neither their history nor a neurologic examination re-vealed any signs or symptoms of cerebrovascular dis-ease. In addition, extracranial CW-Doppler ultrasoundexamination for the evaluation of both carotid and ver-
0090-30]91871$350

440
Surg Neurol1987 ;27 :439-48
tebral arteries (Debimetre ultrasonique Delalande) andduplex system studies for visualization of the extracra-nial carotid system (Diasonics DRF 400) were used toexclude extracranial arterial disease (for details see ref-erences 10 and 21) . In 16 patients (mean age 67 .5 years,age range 55-79 years) four-vessel arteriograms wereavailable for comparison but did not show any definiteabnormality .
MethodsA microprocessor-controlled directional PW-transcran-ial (TC) Doppler device operating at 2 MHz was usedfor studying the basal cerebral arteries (EME, Uberlin-gen). Using a range-gated transducer, measurements weretaken from selected areas at depths ranging from 25 to125 mm at 5 mm steps, with an optimal focus of theultrasonic beam to a sampling volume of approximately10 mm in length and 4 mm in diameter at a depth ofabout 50 mm . The ultrasonic burst length was 10 µsec,pulse repetition frequencies were 6 .8-18 kHz, high-pass filter was 100 Hz, and the low-pass filter rangedfrom 3 .4 to 9 kHz . The ultrasonic power emitted variedbetween 10 and 100 mW/cm' .
As the angle between the ultrasonic beam and thedirection of the intracranial arteries cannot be deter-mined exactly, estimation of either the Doppler fre-quency shift (Hz) or the Now velocity (cm/sec) computedby a 64-point FFT spectrum analyzer (EME, Uberlingen)is limited . However, optimal recording of the intraar-terial flow provided an angle between the ultrasoundbeam and the axis of the vessel ranging from 0 to 30degrees with its cosine between 1 and 0 .86, which keepsthe maximum error reasonably below 15% . The rela-tionship between Doppler shift frequency (4/) and flowvelocity (r) for measurements performed with an ultra-sonic instrument operating at 2 MHz is given by theequation :
v = 0.039 X Of.
In this respect the MCA is favorably located when thetransducer is placed on the temporal bone, whereas vari-ations of the size and location of the ACA and PCAmay result in less reliable data and even difficulties inrecording from these vessels . The instantaneous peakvelocities in systole and late diastole as well as the av-eraged mean flow velocity were considered for statisticalevaluation from the FFT spectra . Time interval resolu-tion was 25 msec and Doppler signal amplitudes werecoded in a grey scale system (dB) . Measurements wereadjusted to different depths of the sampling volume . Alldata were recorded on a printer (Hewlett-Packard) andstored on video tape (Sharp) .
Examination Procedure
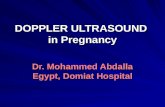
Identification and separation of the basal cerebral ar-teries were performed by determination of flow direc-tion, audio-analysis, depth control of the range-gatedDoppler signals, and occasionally by compression testson the neck arteries . Patients lay comfortably in a supineposition in order to prevent fluctuations of cerebral bloodflow as a result of hypercapnia or hypocapnia ; PCO2 end-tidal values, measured by use of an Engstrom aerometer,were kept constant . Moving the probe in small steps inthe temporal region, preferably at a depth of 50 or 55mm, the ultrasonic window had to be determined first .In most subjects selected, the acoustic window couldeasily be adjusted at a reasonably low signal to noiseratio (recent experience from more than 1500 investi-gations performed in our laboratory indicate that about5%r of subjects are unable to be examined using thetranstemporal approach because of poor ultrasonic bonewindows; in contrast, the transorbital and transnuchalpathways were almost always applicable) . Identificationof the various basal cerebral arteries is then required .The MCA is the easiest to record, at a depth between30 and 60 mm (Figure 1). The main trunk of the MCA(MI segment) and proximal branches (M2 segment) re-veal a flow directed towards the probe . Distal branches(M3 segment) cannot be as confidently recorded becauseof their nearly perpendicular axis to the ultrasound beam .Once the MCA is identified, its course can be trackedby small angle movements of the ultrasonic probe untila Doppler signal in the opposite direction and usuallyof weaker intensity is identified : this signal representsthe ACA (between 60 and 75 mm) .
Tilting the probe caudally, the CI segment of theinternal carotid artery (ICA) can usually be examined .The C2-C4 segments of the carotid siphon can be eval-uated by a transorbital approach in 50-80 mm depthsat a reduced ultrasonic power emitted . The ophthalmicartery may he followed from 30 to 50 mm .
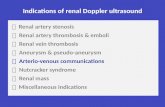
Aiming the probe at a posterior position and slightlycaudal to that of the MCA, the PCA can usually berecorded at depths between 60 and 80 mm (Figure 2) .In the proximal segment (P1) the flow is directed towardsthe probe like in the MCA . The distal segment (P2) aswell as the contralateral PCA-PI segment show flow inthe opposite direction . In contrast to the MCA, thesignal is lost when scanning outwards below 50-55 mm .
Compression tests on the ipsilateral common carotidartery (CCA) may answer the question as to whetherthe PCA is directly supported by the ICA, which canbe seen in about 10-30% of cases [16,20]: in this caseCCA compression would cause a reduction of flow ve-locity . However, if the PCA is supplied by the basilarartery CCA compression would result in an increase of
Hennerici et al

B
A
-> C
50
-> C
70
=> C
75
M C A
ICA
A C A
Figure L Schematic illurtraiiot of the position of the sampleroltnme (A) and /)nee celueiti spectra (B) o/ the AI CA, and the'I'-lrtnttiot of the ICA and the ACC for the transtemporal ap-proaob . Distance between sample rolnme pasi/ton aped the trapni-dncer is indicated tom of depth) below the symbol demo etratingflow direction : F/ou-towards the probe fyi is op . flow away frontthe probe a represented by a dine nward signal. Abbreviation :ICA . internal carotid artery : Aca, anterior communicating artery :A,opht ., ophthalmic artery .

Sr
09
09
SC
06
va
3
Zd
Ld
Zd
Ld
SL
b'z)d
d
H

Transcranial Doppler Ultrasound-Pare 1
Table 1 . Normal Age-Adjusted Calculated Mean - SD Values of TC-Doppler Flow Velocity within the Basal Cerebral Arteries asRecorded from Selected Reference Points
Abbreviations : MCA, middle cerebral artery ; ACA, anterior cerebral artery ; lo-A, posterior cerebral artery, VA, vertebral artery ; BA, basilar artery, nn s ., notsignificant .
7p < 1(02.11, < 11 05)
flow velocity if the posterior communicating artery ispatent .
Common carotid artery compression maneuvers forthe assessment of the anterior communicating arterymay similarly cause marked changes of flow direction,velocity patterns, or both in this vessel and the ACA[21: ipsilateral compression frequently results in an in-verse flow while contralateral CCA compression in-creases the velocity . These tests may be particularlyimportant for evaluation of the collateral capacity in thepresence of extracranial obstructive lesions or for iden-tification of the ACA if morphologic variations are pres-ent, e.g ., aplasia of the A 1 segment (< 1%o) or hypoplasia(3-10%) [16,22}. Compression of the CCA should beavoided if mild compression has already introduced sig-nificant alterations of the cardiac rhythm . In addition,care should be taken to compress the CCA definitelybelow the bifurcation at an area free of atheroma asrevealed by prior CW-Doppler and/or duplex-systemexaminations .
The VA and BA can be easily and most consistentlyrecorded from a nuchal position via the posterior boneand/or the foramen magnum . However, separation ofthese arteries may be limited because of : (1) the variablesite of the vertebrobasilar junction ; (2) anatomical vari-
Figure 2 . Schematic illustration of the position of the sample volume (A)and flow velocity spectra recorded from the PCA (B) and VAIBA (C). (B)In the proximal segment (PI), flow is directed towards the probe (->) tup-wardr) at 80 mm depth, whereas the distal segment (P2) is perfused withinthe direction of the probe (<-) at 60-75 mm depth (upwards) . At the vesselslope simultaneous recordings are obvious from both regmentr (75 mm depth,P2/PI) (C) Plow velocity at 45-60 mm depth is likely to derire from theVA otpwards ; H, whereas beyond 70 rum recordings are from the BA(upwards) . Flow towards the probe (downwards at 50 and 75 mm) probablyoriginates from the PICA and the A ICA, respectmelym
ations in course and length of the BA (approximately33 mm mean value); and (3) variable distances of theBA to the clivus (<90 mm in about 80% and > 100 mmin about 20% of normal subjects) [5,13,22] . In the pres-ence of hypoplasia or aplasia of either of the VAs, sep-aration of the remaining VA from the BA may not bepossible at all . For the same reasons, the depth at whichthe BA can be expected is uncertain . Although signalsrecorded deeper than 80 mm may be estimated to resultfrom the BA, we occasionally identified the confluence
Figure 3 . Age-related dtfferencee of systolic peak flow velocities in the ACAand MCA. Calculated mean values and standard deviations from bothresrelr are indicated according to the depth of recordings . Open .symbols referto the ACA, black symbols refer to the MCA . Subjects younger than 40years are denoted by triangles . subjects older than 60 years by circles .
Surg Neural
4431987 ;27 :439- 4 8
Arteries (depth in mm)
Systolic peakvelocity(cmlsec)
Averaged meanvelocity(cm/sec)
Diastolic peakvelocity(cmlsec)
Age(years)
MCA (50 mm) 94.5 ± 13 .6 58.4 ± 8 .41 45 .6 - 6 .61 <4091.0 ± 16.9~I ns
.57.7 = 11 .5 II ° .s .
44 .3 - 9 .5 11 40-6078.1 ± 15 .0 I" 44.- ± 11 .I 1 31 .9 - 9.1 I' >60
ACA (7() mm) 76.4 - 16.91 47 .3 - 13 .61 36 .0 - 9.01 <4086.4 - 20.1 (I as.
53.1
10.5 1 ns.
4 L 1 - 7_4 11 40-6073 .3 - 20 .3
n. s .45 .3 - 135 I n
. s .34 .2 - 8 .8 I >60
PCA (60 mm) 53 .2 - 11 .31 34 .2 - 7 .81 25 .9 ± 6.51 <4036.6 ± 9 .811 n
. s .28 .7 - 7 . 511
ns .40-6060 .1 - 20 .6I
(n.s.51.() =. 11 .9 29.9 = 9 .3 I n
. s .22.0 - 6 .9 >60
VA1BA (75 tom) 56 .3
7.8) 349- 781 27.0 - 5 .31 <4036.4_ 11.711 n
. s .29 .2 - 8 .4 I 1 n.s .
40-6059.5_ 17.0 1 1 ns .21 .2-9.2 I s50 .9 - 18 .7 I 30 .5 - 12.4 t"
. >60
DEPTHS (mm)
120- 50 55 60 65 70 75
100-100-I
EEU
}t
F 80- t
U0 o'
> 60-
40-

N
140-1 <40
120-
s055
60
5
20
PEAK
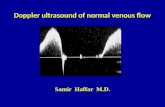
MEANFigure 4 . Range of normal values as recorded at various depths (indicated in numbers in each column) from The MCA of various age groups for the peaksystolic and mean velocities . respectively. Calculated mean values are indicated by the small horizontal bar ., within each column .
Figure 5 . Calculated systolic peak velocity raluet and standard deviations recorded f rom presumed normal subjects of too age groups : people yo urger than40 years (---) and people older than 60 years !-) . Reference depths of recordings are indicated for the MCA, ACA, PCA, and VA/BA . Note the markeddifference of calculated values for The MCA in contrast to the other basal cerebral arteries .
41-60
5
s
AGE GROUPS (YEARS)
>61
55 60 65
65
DEPTHS (mm)
`A 5
s40
41-60
Q
70
1055
m
BA 7075
>61
65
5

Transcranial Doppler Ultrasound-Part I
located as deep as 90 and 110 mm . With regard to thesevariations, identification of other bidirectional signals orsignals toward the probe is difficult, although one mightspeculate whether or not they reflect flow in branchingvessels of the VA/BA [posterior inferior (PICA) andanterior inferior (AICA) cerebellar arteries] (Figure 2C).Compression tests of extracranial carotid or vertebralarteries-the latter being rather difficult to perform foranatomical reasons-are insignificant for this purpose .
In addition, a pulsatility transmission index (PTI)is introduced for a bilateral comparison of the Dopplerspectra recorded. This dimensionless parameter is ex-pressed in percent of the pulsatility indices (PI) of eitherside 1151 as indicated in Table 2 :
PTI = (PI ipsilateral/ PI contralateral) x 100 .
Statistical evaluations were performed using the Wil-coxon test for nonparametric samples .
ResultsDoppler recordings of sufficient intensity to allow re-liable estimation of flow velocities within both MCAs,both ACAs, both PCAs, and the VA/BA are obtainedin 96%, 82%, 88%, and 100%, respectively . Becausesubjects with small ultrasonic bone windows were ex-cluded from this study, these figures will be lower in arandom population. Table 1 summarizes the analyzedmean values and standard deviations of the systolic anddiastolic peak as well as the mean Doppler flow velocitiesas recorded at selected reference depths where the ves-sels considered could be identified most consistently .For all three age-groups the values measured from thereference points of the MCA and ACA revealed a highlysignificant difference (p < 0 .001) from those measuredwithin the PCA and VA/BA, which reflects the majordifference between the carotid and vertebral arterial sys-tems .
Age-related data from the ACA, PCA, and VA/BAshow a slight but nonsignificant increase of all param-eters with increasing age (from <40 to 40-60 years) (p< 0.1) and a decrease for the oldest subgroup . In con-trast, values of all parameters within the MCA decreasedwith age .
Whereas in the MCA peak and mean velocities de-crease with increasing age, values from the ACA nearthe anterior communicating artery increase in older sub-jects (Figure 3) . This increase is probably due to mildatherosclerosis within these small vessels even in pre-sumed normal subjects with normal arteriograms (n =16), and thus should be considered to avoid overesti-mation of pathologic processes .
Interindividual variation is particularly high for thepeak systolic flow velocity as is the range of normal forthese values (Figure 4) . In contrast, standard deviations
Surg Neutral
4451987 ;27 :439-18
Table 2 . Calculated Mean and Standard Deviation ofPulsatility Indices from both MCA, ACA, and PCA in allPresumed Normal Subjects Studied
Abhreviations MCA, middle cerebral artery ; ACA, anterior cerebral artery :PCA, posterior cerebral artery ; n .s .. not stgnihcaot-
"Values are mean ! SD. Pulsatility indices were determined using thefollowing equation. PI - IV, - V, i1/V, 5 , where V, is systolic peak velocity . V iis diastolic peak velocity, and V .,is averaged mean velocityy
of the mean flow velocities are considerably smallerthroughout all the different age groups and less variableto the selected depths of recordings .
As shown in Figure 5, consideration of different pa-rameters, recording sites and age-dependence of flowvelocity are particularly relevant for the MCA . In con-trast to all the other basal cerebral arteries this vesselcan be regularly tracked along a comparatively largecourse at the base of the skull,
No significant difference between flow velocity valuesrecorded from either of bilaterally existing arteries couldbe established provided insonation was similarly possi-ble from both temporal windows, However, interindi-vidual variations are large, as reflected by the data shownin Table 2 .
A recently designed, new pulsed Doppler device, whichenables two-dimensional scanning of the basal cerebralarteries and uses a considerably smaller sample volume(4 x 5 mm) was used for some preliminary studies ina new subjects of this report . As shown in Figure 6 thissystem enables: (1) a stereo assessment of the intra-cranial recording sites with reference to the individualprobe position of the subject examined; (2) demonstra-tion of the topography of the arteries recorded in hor-izontal, sagittal, and frontal planes ; and (3) a sensitivedifferentiation of nearby vessels even if they show thesame flow direction, e.g., distal carotid siphon, proximalMCA, and the posterior communicating artery . In ad-dition, because of the smaller sample volume incorpo-rated, a better delineation can be achieved of small ves-sels that hitherto could not be recorded reliably, e.g .,the posterior communicating and the superior cerebellararteries .
DiscussionAlthough extracranial CW- and PW-Doppler ultrasoundtechniques have been used for the evaluation of bothcarotid and vertebral arterial systems and have gainedacceptance during the last decade t3,4,9,11,12,2 11, both
Arteries Pulsatility index' Regression coefficient U-test
MCA right 0.90 ' 0.24 r = (1 .54 n.s .MCA left 094 ± 0.27ACA right 0.78 3 0.15 r = 0 .6 n.s .ACA left 0.83 ± 0.17PCA right 0.88 ± 0.23 r = 0 ."4 Ills .PCA left 0 .88 ± 0.20

446
Surg Neurol1987 ;27:439-48
Figure 6 . Display of a new two dimensional TC-Doppler device . (beLf)FFT-Doppler spectrum of the right posterior communicating artery . Duringcompression on the ipsilateral common carotid artery the spontaneous alter-nating flow velocity increases indicating its collateral capacity . fK_s_'g_ht)Frontal (upper row) and horizontal (lower row) views of the basal cerebralarteries as recorded from selected positions of the sample volume (-C)) (thisparticular display corresponds to the posterior communicating artery, theDoppler spectra of which are to be seen on the left side) . As the probe isincorporated in a helmet fixed to the patients head, recordings of probeposition, flow velocity (rmlsec), and flow direction (towards the probe : yellowand red; away from the probe: blue and lilac; size of spots corresponds tosignal amplitude), are visualized and stored in a computer .
methods are unable to provide similarly reliable infor-mation about the state of intracranial cerebral arteries .Transcranial Doppler recordings of flow velocity in thebasal cerebral arteries developed by Aaslid et al in 1982[2] have been reported to be useful for the evaluationof intracranial hemodynamic alterations. However, nor-mal reference values have hitherto not been elaborated,because most of the data available result from restrictedsamples of healthy young subjects [1,2,8,15] .
The results presented from 50 patients in differentage classes, who, according to clinical and extracranialultrasound examination and with respect to their history
Hennerici et al
were supposed not to suffer from cerebrovascular dis-eases, show a fairly large variation (peak and mean flowvelocities, PI and PTI) of most of the parameters ana-lyzed from the Doppler FFT spectra . Whereas intrain-dividual variations are reasonably small-and hence sup-port the current use of this method for follow-up studies[ t,8,18,19]-interindividual peak velocity variations arehigh, particularly during systole. Thus, this parameter ishardly suitable for a sensitive differentiation betweennormal and abnormal . This unsuitability is probably dueto the large sample volume used so far [171, which pre-vents definite separation of the vessel considered fromsmaller neighboring vessels . High peak flow velocitieswithin the latter may therefore be superimposed buthidden in the signals recorded from the artery of majorinterest. This assumption is further sustained by prelim-inary observations of multiple superimposed Dopplerspectra from various vessels recorded in patients afterneurosurgical craniectomy . In addition, asymmetries offlow in the tortuous course of the arteries may result inhigh frequency, low amplitude signals, hence dominat-ing the spectrum recorded .
In contrast, measurements of the mean flow velocities

Transcranial Doppler Ultrasound-Part I
are less variable . We therefore suggest this parameterbe given preference . We assume that this parameter isless influenced by high flow velocity but low amplitudesignals originating from small vessels near the main ar-teries under consideration, that it reacts less sensitivelyto minor flow inhomogeneities on the vessel wall, andthat it remains less affected by frequently occurring pulserate differences .
The large variations of normal values in general maybe partly due to a matter of selection : values were takenfrom the same reference points in terms of depths ofultrasound penetration without correction for individualchanges in the anatomy of the circle of Willis . However,this procedure seemed justified at present with regardto the major problems of an unknown angle of inson-ation, the large size of the sample volume, and the in-ability hitherto of tracing the course of recordings . Basedon our recent and still limited experience with a newscanning system, we believe that some of these problemswill be solved by the smaller size of the sample volumeincorporated and the excellent visualization of the areasmeasured, thus increasing the reproducibility of themethod considerably, even if new limitations from aworse signal to noise ratio appear. However, the widevariations of flow velocity values in normal subjects donot restrict the application of this method for evaluationof various types of cerebrovascular diseases, as will heshown in a subsequent contribution in this journal .
Flow velocities measured from the ACA, PCA, andVA/BA are not age-related : whether this is a simpleobservation or results from inconstant angles, insuffi-cient ability to track these arteries, or interindividualvariations in their caliber cannot be answered at present .There is, however, a remarkable tendency toward anincrease of values from younger subjects (less than 40years) to the group between 40 and 60 years, which maybe due to elasticity alterations, increase in vasomotortone, etc . In contrast, decreasing values in subjects olderthan 60 years have been observed, which are probablydue to changes in cerebral autoregulation, dilative ar-teriopathy, the development of nonocclusive athero-sclerosis, etc . In general, the flow velocity values aresignificantly smaller in the posterior cerebral circulationsupplied by the vertebral system (PCA and BA) than inthe ACA and MCA fed by the carotid system . Thisobservation is somewhat surprising although fairly con-sistent, and differs slightly from what one might haveexpected in view of measurements of cerebral bloodflow and blood volume performed by nuclear methods[6] . Because the nuclear methods examine different as-pects of intracranial circulation, we expect further stud-ies to investigate this relationship . The advantages ofTC Doppler examination are its noninvasive, easily re-producible approach for the detection of rapid altera-
Surg Ncurol
4471987 ;27 :439-48
tions of blood supply within the major cerebral arteries,which is impossible with other techniques available to-day. Disadvantages include difficulties in insonating pa-tients with small ultrasound bone windows (about 5%of more than 1500 patients admitted for examination tothis hospital) resulting in either weak signals or a poorsignal to noise ratio . Recordings of the ACA and PCAhave a higher dropout ratio (18%% and 12%, respec-tively), which is suspected to be most likely due to theincidence of abnormalities known to exist in the anteriorbranches of the circle of Willis f 14] and/or less suitabletransmission conditions from the temporal bone probeposition for recordings of these vessels . Both these rea-sons may also be responsible for the less pronouncedvariations of Doppler spectrum parameters with differ-ent age classes in these vessels, which we believe to bean artifact rather than a simple observation . The prelim-inary results of this new technical system, which clearlyimproves examination conditions, are therefore verypromising .
This work was supported by the Deutsche ForschungsgemeinschaftSFB 2001D2 and the Bertelsmann Sufrung, Gutersloh .
References1 . Aaslid R, Huber P, Nornes H . Evaluation of cerebrovascular
spasm with transcranial Doppler ultrasound . J Neurosurg 1984 ;60 :37 -41 .
2. Aaslid R, Markwalder T-M, Norncs H . Non-invasive transcranialDoppler ultrasound recording of flow velocity in basal cerebralarteries. J Neurosurg 1982 ;57.769-74 .
i . Barnes RW, Bone GE, Rcinerrson J, Slaytnaker EE, HokansonDE, Srrandness DE . Noninvasive ultrasonic carotid angiography :prospective validation by contrast arreriography . Surgery 1976 ;80:328-35 .
4 . Barnes RW, Ringers SE, Putney WW. Real-time Doppler spec-trum analysis . Arch Surg 1982;117 :52-7 .
5 . Busch W. Beitrag zur Morphologic and Pathologic der A . basilaris(Untersuchungsergebnisse hei 1000 Gehirnen) . Arch PsychiarrNcrvenkr 1966 ;208:326-44 .
6 . Frackowiak RSJ, Lenzi GL, Jones T, Heather JD . Quantitativemeasurement of regional cerebral blood flow and oxygen metab-olism in man using 150 and positron emission tomography : the-ory, procedure and normal values . J Comput Assist Tomogr 1980;4 :7 27-36.
7 . Freund H-J, Kapp H . Fine Merhode zur Registrierung arteriellerPulsarionen mittels Ultraschall . Pflugers Arch Ges Physiol1966;291 :268-76.
8 . Harders A, Gilsbach JM . Transkranielle Dopplersonographie in,let Neurochirurgie . Ultraschall lived 1984 ;5 :237-15 .
9 . Hennerici M, Auhch A, Sandmann W, Freund H-J . Incidence ofasymptomatic extracranial arterial disease. Stroke 1981 ;12]50-8 .
10. Hennerici M, Freund H-J . Efficacy of CW-Doppler and duplex-system examinations for the evaluation of extracranial carotiddisease . J Clin Ultrasound 1984 :12:155-61 .
It . Keller H, Meier W, Yonekawa Y, Kumpe D. Noninvasive an-giography for the diagnosis of carotid artery disease using Dopplerultrasound (carotid artery Doppler). Stroke 1976;7354-63 .

448
Surg Neurol1987;27:439-48
12 . Keller HM, Meier WE, Kumpe DA. Noninvasive angiographyfor the diagnosis of vertebral artery disease using Doppler ultra-sound (vertebral artery Doppler) . Stroke 1976 ;7:364-9 .
13. Krayenbuhl H, Yasargil MG. Die vaskularen Erkrankungen imGebiet der Arteria vertebralis and Arreria basilaris . Stuttgart :Thieme. 1957 :1-170,
14 . Lang J . Kopf. Ted B, Gehirn- and Augenschadel . In : Lanz-Wachs-muth. Praktische Anatomic 111 . Berlin, Heidelberg, New York :Springer, 1979 .
15 . Lindegaard K-F, Bakke SJ, Grolimund P, Aaslid R, Huber P,Nornes H. Assessment of intracranial hemodynamics in carotidartery disease by transcranial Doppler ultrasound . .1 Neurosurg1985 ;63:890-8 .
16. Mitterwallner von F . Variationsstatistische Untersuchungen anden basalen Hirngefallen . Area Anar(Basel) 1955 ;21:51-88 .
17. Roederer GO, Langlois YE, Chan AW, Primozich J, LawrenceRJ, Chikos PM, Strandness DE . Ultrasound duplex scanning ofthe extracranial carotid arteries : improved accuracy using new
Hennerici et al
features from the common carotid artery . J Cardiovasc Ultrason1982 ; 1 : 373-80 .
18. Schwartz A, Hennerici M . Noninvasive transcranial Doppler ul-trasound in intracranial angiomas. Neurology 1986 ;36:626-35 .
19 . Seiler RW, Grolimund P, Aaslid R, Huber P . Nornes H . Cerebralvasospasm evaluated by transcranial ultrasound correlated withclinicalgrade and CT-visualized subarachnoid hemorrhage . J Neu-rosurg 1986 ;64:594-600 .
20. Sunderland S . Neurovascular relations and anomalies at the baseof the hrain . J Neurol Neurosurg Psychiatr 1948 ;11 :243-54 .
21, Trockel U, Hennerici M, Aulich A, Sandmann W . The superiorityof combined continuous wave Doppler examination over perior-bital Doppler for the detection of extracranial carotid disease . JNeural Neurosurg Psychiatr 1984 ;47 :13-50 .
22. Wollschlager PB, Wollschlager B . The anterior cerebral/internalcarotid and middle cerebral/internal carotid arteries . Area Radio]Diagn 1966 ;5 :615-20 .

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具