Seeing with sound II: - Doppler Ultrasound & Obstetrical Ultrasound Background Image: .

532
Transcranial Doppler Ultrasound Findings inMiddle Cerebral Artery Occlusion
M. Kaps, MD, M.S. Damian, MD, U. Teschendorf, and W. Dorndorf, MD
We evaluated the efficacy of transcranial Doppler ultrasonography in 23 patients suffering fromacute middle cerebral artery occlusion. The diagnosis of occlusion was most suggestive when allbasal arteries except the affected middle cerebral artery were detectable. Enhanced blood flowvelocity in the anterior cerebral artery due to leptomeningeal collateralization was used as acorroborating criterion. With frequent follow-up examinations, we monitored reperfusion of theMl segment resulting from recanalization or embolus migration in 16 patients. Those patientsundergoing recanalization within days after onset of the first symptoms revealed variableclinical courses and lesion patterns on computed tomography, indicating the crucial impor-tance of early and efficient leptomeningeal collateral blood supply. Transcranial Dopplerultrasonography was able to exclude middle cerebral artery occlusion with accuracy, whichprovides important clinical information. However, distal branch occlusions could not bedetected with sufficient exactness. (Stroke 1990^1:532-537)
Transcranial Doppler ultrasonography (TCD)can provide the diagnosis of middle cerebralartery (MCA) main stem occlusion under
specific circumstances. This opens new vistas forresearch regarding the frequency, course, and prog-nosis of MCA occlusion. The noninvasive TCDmethod permits examination of patients unfit forangiography during the acute phase of stroke and atshort intervals. The aim of our study is to describeTCD criteria allowing the diagnosis of MCA occlu-sion and to present TCD follow-up findings observedduring MCA recanalization.
Subjects and MethodsTwenty-three patients suffering from acute MCA
occlusion (Table 1) received a complete clinical andcomputed tomographic (CT) work-up. Criteria forMCA occlusion were derived from 11 patients whounderwent angiography (patients 1-11). Twentypatients (4-23) received follow-up studies starting^24 hours after clinical onset; 18 (patients 6-23)were consecutive during 6 months. The diagnosis ofMCA occlusion was confirmed in the consecutiveseries by angiography (patients 6-11), necropsy(patients 12 and 13), or retrospectively, follow-upTCD examinations showing reperfusion of the MCA(patients 14-21). In these eight patients, CT was
From the Department of Neurology, Justus-Liebig-UniversitatGiessen, Federal Republic of Germany.
Address for correspondence: Priv. Doz. Dr. med. M. Kaps,Neurologische Universitatsklinik, Am Steg 14, D-6300 GieBen,Federal Republic of Germany.
Received August 17, 1989; accepted October 31, 1989.
repeated to exclude the possibility of hemorrhageinto the infarcted brain tissue. Two patients (22 and23) had certain MCA occlusion, with a proven car-diac source of emboli, simultaneous arterial occlu-sions in multiple other organs, and clinical and CTfindings compatible with embolic MCA occlusion.Five patients (4-6, 18, and 19) suffered additionalcarotid artery occlusion.
In the consecutive series, follow-up TCD studieswere carried out daily during the first week, every 3days during the second week, and weekly until dis-charge in cases with persistent abnormal blood flowvelocities. Death prohibited follow-up in six patients.
The basal cerebral arteries were investigated using astandard pulsed 2-MHz Doppler device (TC 2-64 B,EME, Uberlingen, FRG) in accordance with acceptedcriteria1 Extracranial continuous-wave (CW) Dopplersonography was carried out in all 23 patients.
ResultsFigure 1 shows criteria for the diagnosis of MCA
occlusion. Conventional CW Doppler sonography ofthe extracranial cerebral arteries must precede everyTCD study because extracranial carotid stenoses andocclusions cause considerable changes in intracranialhemodynamics.
Having ruled out extracranial occlusive disease,demonstration of the basal arteries of the asymp-tomatic side is advisable initially. As physiologicblood flow conditions are to be expected there,information can be obtained regarding ultrasoundpenetration of the temporal bone and depth of thecontralateral MCA (assuming symmetry).
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

Kaps et al TCD in MCA Occlusion 533
TABLE 1. Characteristics of 23 Patients Suffering From Middle Cerebral Artery Occlusion Investigated by TCD
Pl/age/sex
1/44/M
2/24/F
3/56/M
4/50/M*
5/40/F*
6/44/M*
7/49/M
8/49/M
9/34/F
10/34/F
11/45/M
12/74/M
13/81/M
14/73/M
15/67/M
16/63/M
17/82/M
18/68/M*
19/78/M*
20/77/F
21/77/F
22/55/F
23/67/M
Confirmed by
Angiography
Angiography
Angiography
Angiography
Angiography
Angiography
Angiography
Angiography
Angiography
Angiography
Angiography
Necropsy
Necropsy
TCD Follow-up
TCD Follow-up
TCD Follow-up
TCD Follow-up
TCD Follow-up
TCD Follow-up
TCD Follow-up
TCD Follow-up
Multiple embolism
Multiple embolism
Tinw
7 days
2 days
1 day
4 days
Recanalization
; Velocity increase
None
No recanalization
No follow-up
11 days
>7 weeks (stenosis?)
None
No recanalization within 4 weeks
17 days
2 days
12 days
2 weeks
7 days
1 day
1 day
1 day
4 days
7 days
3 days
9 days
>4 weeks (stenosis?)
28 days
Persistent (stenosis?)
None
No recanalization
No recanalization
—
—
33 days
—
25 days
None
8 days
—
No recanalization
No recanalization
Lesion pattern
Multiple branches
LSA
Multiple branches
Multiple branches
Branch
LSA
LSA
-
LSA+branch
LSA
Branch
Complete
Complete
No classification
Complete
LSA
Complete
LSA
LSA
Branch
LSA
LSA
Complete
Neurologic deficit
Severe
Moderate
Severe
Severe
Mild
Severe
Moderate
Moderate
Moderate
Moderate
Mild
Died
Died
Died
Died
Severe
Died
Moderate
Severe
Severe
Severe
Moderate
Died
TCD, transcranial Doppler ultrasonography, Pt, patient; M, male; F, female; increase, >50% greater than contralateral (duration notdetermined when patient died); LSA, lenticulostriate arteries.
•Additional ipsilateral carotid occlusion.
The next step is to identify the distal segment of theinternal carotid artery (ICA), the anterior cerebralartery (ACA), and the posterior cerebral artery(depth settings 50-75 mm). This procedure is the mostimportant prerequisite since it guarantees the exis-tence of an appropriate acoustic bone window. Com-pression tests may contribute to artery differentiation.
Starting from the intracranial ICA or from theACA, one must now search for the MCA by short-ening the ultrasound focusing depth in a stepwisefashion (depth settings 35-40 mm) with rovingchanges of direction of the ultrasound beam. If thispainstaking procedure fails to uncover an ultrasoundsignal related to the MCA, occlusion of the arterymust be suspected. A characteristic finding corrobo-rating the diagnosis of MCA occlusion is acceleratedblood flow in the Al segment of the ACA due toactivation of leptomeningeal anastomoses.
The diagnosis of MCA occlusion secondary to alodging embolus is complicated when there is addi-tional obliteration of the extracranial ICA or of thesiphon. Under these circumstances, increasedorthograde blood flow in the ipsilateral ACA is not tobe expected and the lack of an MCA signal may beexplained by hemodynamic reasons as well. Very lowblood flow velocities (<10 cm/sec) are not detectablefor technical reasons. Under these circumstances,confirmation of periocclusive MCA artery-to-artery
embolism is possible, retrospectively, if MCA recan-alization and sufficient collateralization via basalcommunicating arteries can be demonstrated (Figure2, patient 6).
Follow-up studies were conducted repeatedly dur-ing the acute period after occlusion; recanalization ofthe MCA could be monitored by TCD in 16 cases(Table 1). Recanalization occurred gradually; a high-frequency stenotic signal indicating a partially patentlumen was subtle at first, but later the TCD signs ofMCA stenosis became more obvious. Furtherincreases in the vascular lumen led to decreases inblood flow velocity in the Ml segment. Finally,turbulent signal irregularities disappeared (Figure 3).Recanalization was seen in this series of 20 patientsuntil 17 days after stroke onset. Augmented bloodflow velocity in the Ml segment disappeared between11 days and 4 weeks after onset. Three patients (14,15, and 17) died after recanalization of the MCAsecondary to temporal herniation after developingextensive postischemic edema. In three patients (5,8,and 10; Figure 4), blood flow velocity enhancementpersisted for weeks. Unfortunately, it was not possi-ble to repeat angiography to demonstrate a residualMCA stenosis in these patients.
In another patient with carotid occlusion (15),blood flow velocity enhancement was seen at theinitial TCD examination 2 days after onset of the first
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

534 Stroke Vol 21, No 4, April 1990
MCAocclusion
zs
trrt
Ml
.IPS21
06,?
1-3d 4d 7d 9d 17d
net
3d
-1"1H
' ' • :^^»r>tn. ' -«
i i i i i res by guest on M
ay 30, 2018http://stroke.ahajournals.org/
Dow
nloaded from

Kaps et al TCD in MCA Occlusion 535
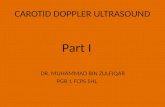
FIGURE 1. Criteria for diagnosis of left middle cerebralartery (MCA) occlusion. All basal arteries except MCA aredetectable by transcranial Doppler ultrasonography. Bloodflow velocity is enhanced in ipsilateral Al segment of anteriorcerebral artery due to activated leptomeningeal anastomoses.Brief compression of common carotid artery (bar in lower lefttracing) elicits increasing blood flow in PI segment of ipsilat-eral posterior cerebral artery.
hemispheric symptoms. Periocclusive embolization ofthe proximal MCA and subsequent thrombus migra-tion was diagnosed, taking into account the finding ofextensive multiple MCA branch infarction on CT.
Differentiating postischemic hyperemia fromresidual MCA stenosis during recanalization causedconsiderable problems. Hemorrhagic transformationcausing clinical deterioration in relation to arterialrecanalization was not observed (under conditions ofhemodilution therapy and 300 mg/day aspirin).
DiscussionOne prerequisite for the TCD diagnosis of MCA
occlusion is a viable acoustic bone window, allowingexamination of uninvolved basal cerebral arteries.Time, patience, and some experience are needed tobe sure that an MCA signal is really lacking.
According to the literature, difficulties due toinsufficient ultrasound penetration through the tem-poral bone arise in up to 30% of cases depending onage, sex, and race. In personal prospective TCDstudies currently including 80 consecutive patientsadmitted ^24 hours after acute stroke, we have 35%drop-outs due to insufficient ultrasound penetration.Furthermore, false-positive diagnosis of MCA occlu-sion may result from a tortuous course of the arteryand is possible when the MCA branches verticallyfrom the siphon.
The recorded Doppler shift is at first unable todifferentiate residual MCA stenosis from increasedblood flow velocity due to decreased peripheral arte-riolar resistance (i.e., postischemic hyperperfusionsyndrome). A combination of both phenomena dur-ing recanalization seems likely. On the basis of onlyone TCD examination shortly after stroke, one musttake care not to misdiagnose reactive hyperemia asMCA stenosis because erroneous conclusions regard-ing pathogenesis would result. However, significantobstruction of the main stem of the MCA causes a"resistance profile" in the feeding ICA, whereas
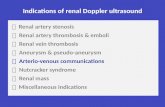
FIGURE 2. Recanalizing right (R) middle cerebral artery(MCA) occlusion with concomitant internal carotid artery(ICA) occlusion (patient 6). Diagnosis can be establishedretrospectively by follow-up transcranial Doppler ultrasonog-raphy. Top: Stenotic signal related to Ml segment on day 4,indicating reperfusion, disappearing thereafter. Due to ICAocclusion, dampened pulse curve with decreased pulsatilityindex (PI, 0.39) persists in spite of good collateralization.Bottom: Left (L) MCA as reference.
reactive hyperemia leads to increased blood flowvelocity even proximal to the Ml segment. The latteris sometimes so pronounced that velocity enhance-ment after intracranial arterial recanalization can bedetected by extracranial CW Doppler sonography.2
Thus, calculating the relation between blood flowvelocity in the MCA and that in the ipsilateral ICA3
may help differentiate MCA stenosis from hyperemiaafter recanalization.
Enhancement of blood flow velocity was notdetectable by TCD in all patients undergoing recan-alization. Partial blockade of the peripheral vascularbed persisting after distal migration of clot fragmentsmay be an explanation.
Patients with MCA occlusion persisting at least 1day revealed highly variable clinical courses andlesion patterns on CT. This was independent of laterspontaneous recanalization, indicating the crucialimportance of early collateral blood supply by lep-tomeningeal anastomoses.4 Five patients featuredtypical "deep" subcortical CT infarcts, which areconsidered to result from proximal MCA trunk occlu-sion and blockade of lenticulostriate end arteries.
Shortly after ischemic stroke, increased or dimin-ished blood flow velocity compared with the oppositeside can frequently be observed in the affected MCA.As the normal ranges of blood flow velocity in thecerebral arteries are wide (mean±SD in the MCA62±12 cm/sec)1 and as side differences of up to 20%are not necessarily pathologic, clear-cut limits forphysiologic and pathologic blood flow velocities aredifficult to establish. Follow-up studies are especiallyhelpful in this respect since reactive hyperemiadecreases over time, enabling the correct diagnosisby TCD retrospectively. We classified a >50%increase in blood flow velocity as abnormal.
Exclusion of an MCA occlusion can also be ofmajor importance, influencing further diagnostic andtherapeutic strategies.5 This information is generallyobtained by TCD with minimal delay and consider-able accuracy.
The small number of cases in our series does notallow us to precisely estimate the sensitivity of TCDin the diagnosis of MCA occlusion. Moreover, state-ments concerning the diagnostic reliability of TCD inpatients with MCA occlusion are biased if the exam-inations are performed in awareness of the clinicaland CT findings, which is to be supposed from apractical point of view. Distal MCA branch occlu-sions cannot be diagnosed by means of TCD sincethere is no reliable way to investigate these segmentsof the artery.
Angiography remains the gold standard for verify-ing MCA occlusions diagnosed by TCD. However,angiography is seldom indicated during the acutephase of stroke. TCD is even more expedient con-cerning follow-up studies of recanalization. Individ-ual angiograms can deliver only one-time informa-tion, initially showing MCA occlusion, later possiblyshowing stenosis; after recanalization, angiography isof no diagnostic value. This may explain occasional
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

536 Stroke Vol 21, No 4, April 1990
4h 24h 48h 7d 12d 16d 28d
mmm mm®
12 h 7d 12 d 18 d 22 d 32d 39d
IS
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

Kaps et al TCD in MCA Occlusion 537
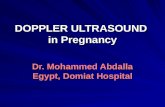
FIGURE 3. Patient 9, 34-year-old woman suffering fromcardiac embolism. Top: Recanalization of internal carotidartery beginning 24 hours after clinical onset. Initially stenoticsignal is prominent; 28 days later transcranial Doppler ultra-sound signal is symmetric and normal on both sides. Differ-entiating stenosis from postischemic hyperemia is difficult.Bottom: Right (R) middle cerebral artery (MCA) as reference.PI, pulsatility index.
discrepancies between angiography and TCD studiescarried out at different times. It is also possible thatocclusion on an angiogram appears as severe stenosison TCD.6 A single angiogram shortly after strokecannot differentiate primary atherosclerotic MCAstenosis from recanalizing embolic occlusion, whichis relevant for further therapeutic strategies.
FIGURE 4. Top: Late recanalization of right (R) middlecerebral artery (MCA), starting 12 days after clinical onset inpatient 10. Five weeks later unequivocal blood velocityenhancement is demonstrable (residual stenosis?). Bottom:Normal left (L) MCA as reference. Note different scales! PI,pulsatility index.
References1. Aaslid R, Markwalder TM, Nornes H: Noninvasive transcranial
Doppler ultrasound recording of flow velocity in basal cerebralarteries. / Neurosurg 1982;57:769-774
2. von Reutern GM: Einsatzmoglichkeiten der Ultraschall-Doppler-Sonographie hirnversorgender Arterien im Rahmender internistischen Intensivmedizin. Intensivmedizin 1987;24:2-7
3. Seiler RW, Weber M, Grolimund P: Evaluation of posttrau-matic cerebral vasospasm by TCD. From the Second Interna-tional Conference on Transcranial Doppler Sonography,Salzburg, Austria, 1988. Neurosurgery (in press)
4. Bozzao L, FantozzixLM, Bastianello S, Bozzao A, Fieschi C:Early collateral blood supply and late parenchymal brain dam-age in patients with middle cerebral artery occlusion. Stroke1989;20:735-740
5. Halsey JH: Progressive lacunar infarction with demonstratedpatency of the middle cerebral artery. Stroke 1986;17:1028-1030
6. Kaps M, Oehler KU: Diagnostische Moglichkeiten der trans-kraniellen Dopplersonographie bei intrakraniellen atheroma-tosen Pseudoocclusionen, in Widder B (ed): Dopplersonographiebei zerebrovaskuldren Erkrankungen. Heidelberg, Springer-Verlag, 1987, pp 41-45
KEY WORDS • ultrasonics • arterial occlusive diseasescerebrovascular disorders
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from

M Kaps, M S Damian, U Teschendorf and W DorndorfTranscranial Doppler ultrasound findings in middle cerebral artery occlusion.
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 1990 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/01.STR.21.4.532
1990;21:532-537Stroke.
http://stroke.ahajournals.org/content/21/4/532World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer available in the
Permissions in the middle column of the Web page under Services. Further information about this process isOnce the online version of the published article for which permission is being requested is located, click Request
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Stroke Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 30, 2018
http://stroke.ahajournals.org/D
ownloaded from