Tranexamic Acid for MRT?
1
www.mountainmedicine.co.uk Tranexamic Acid for Mountain Rescue Dr Jo Organ Trauma Fellow, Royal London Hospital Dr Linda Dykes Consultant in EM Ysbyty Gwynedd, Bangor Minimum Maximum Casualties with TXA-eligible injury 94 + with eligible on-scene physiology 21 41 and then looking at how quickly the ey’d have got T TXA... Not at hospital by 1 hr post-injury 17 18 Not at hospital by 3 hr post-injury 3 4 Not at hospital by 6 hr post-injury 1 2 Not at hospital by 8 hr post-injury 0 1 Does Mountain Rescue need CRASH-2 too? AIM UK Mountain Rescue Teams (MRTs) administer drugs according to the Mountain Rescue England & Wales (MREW) formulary. In 2014, MREW added IV Tranexamic Acid (TXA) to their formulary, although IV access skills are generally unavailable to MRTs unless their casualty carers happen to be doctors/ paramedics/nurses. TXA should be given as soon as possible after injury, with a maximum time window of three hours. Our ED receives more mountain casualties than any other unit in the UK, so we sought to estimate the proportion of mountain casualties eligible for onscene TXA by MREW formulary criteria. METHOD The Bangor Mountain Medicine database (1051 casualties brought to Ysbyty Gwynedd following contact with MRTs and/ or RAF SAR 2004–2014) was interrogated for injuries which might cause significant haemorrhage. Onscene observations were reviewed to identify CRASH2 eligible 1 patients. Due to unrecorded data, numbers are represented as “minimum” where inclusion criteria were met and “maximum” where exclusion criteria were not. CONCLUSION TXAeligible mountain casualties in Snowdonia are rare (24%). Almost all arrive in hospital within three hours of injury & therefore don’t need MRT to administer TXA at scene in order to meet the time window in which to give the drug. Only 34 casualties in this 11year series arrived at hospital more than 3 hours postinjury and hence we conclude that MRT administration of TXA is not necessary, and numbers would be too low to support maintaining the IV access skills of MRT lay medics. Should an IVtrained HCP happen to be responding as an MRT medic, it would be reasonable for them to administer TXA, but not at the expense of delaying evacuation to hospital. We acknowledge that this data may not be transferable to mountain areas with longer transit times to hospital. However, in Snowdonia, we estimate that it would take 160 years for MRT casualty carers to save one life using TXA at scene by delivering the drug at scene within one hour of injury cf. casualties getting their TXA within three hours from hospital staff or a SAR helicopter paramedic. RESULTS Photo: Fiona Moore 1. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH2 randomised controlled trial. The CRASH2 collaborators. The Lancet, Vol. 377, No.9771, p10961101 REFERENCE
-
Upload
ysbyty-gwynedd-emergency-department -
Category
Documents
-
view
123 -
download
5
description
Poster presentation from Traumacare 2015. Photo courtesy of Fiona Moore
Transcript of Tranexamic Acid for MRT?
-
www.mountainmedicine.co.uk
Tranexamic Acid for Mountain Rescue
Dr Jo OrganTrauma Fellow,Royal London Hospital
Dr Linda Dykes Consultant in EMYsbyty Gwynedd, Bangor
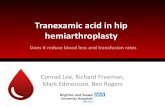
Minimum Maximum
Casualties with TXA-eligible injury 94
+ with eligible on-scene physiology 21 41
and then looking at how quickly theyd have got TXA...and then looking at how quickly theyd have got TXA...and then looking at how quickly theyd have got TXA...
Not at hospital by 1 hr post-injury 17 18
Not at hospital by 3 hr post-injury 3 4
Not at hospital by 6 hr post-injury 1 2
Not at hospital by 8 hr post-injury 0 1
Does Mountain
Rescue need CRASH-2 too?
AIMUK Mountain Rescue Teams (MRTs) administer drugs according to the Mountain Rescue England & Wales (MREW) formulary. In 2014, MREW added IV Tranexamic Acid (TXA) to their formulary, although IV access skills are generally unavailable to MRTs unless their casualty carers happen to be doctors/paramedics/nurses. TXA should be given as soon as possible after injury, with a maximum time window of three hours. Our ED receives more mountain casualties than any other unit in the UK, so we sought to estimate the proportion of mountain casualties eligible for on-scene TXA by MREW formulary criteria.METHODThe Bangor Mountain Medicine database (1051 casualties brought to Ysbyty Gwynedd following contact with MRTs and/or RAF SAR 20042014) was interrogated for injuries which might cause significant haemorrhage. On-scene observations were reviewed to identify CRASH2-eligible 1 patients. Due to unrecorded data, numbers are represented as minimum where inclusion criteria were met and maximum where exclusion criteria were not.
CONCLUSIONTXA-eligible mountain casualties in Snowdonia are rare (2-4%). Almost all arrive in hospital within three hours of injury & therefore dont need MRT to administer TXA at scene in order to meet the time window in which to give the drug. Only 3-4 casualties in this 11-year series arrived at hospital more than 3 hours post-injury and hence we conclude that MRT administration of TXA is not necessary, and numbers would be too low to support maintaining the IV access skills of MRT lay medics. Should an IV-trained HCP happen to be responding as an MRT medic, it would be reasonable for them to administer TXA, but not at the expense of delaying evacuation to hospital.We acknowledge that this data may not be transferable to mountain areas with longer transit times to hospital. However, in Snowdonia, we estimate that it would take 160 years for MRT casualty carers to save one life using TXA at scene by delivering the drug at scene within one hour of injury cf. casualties getting their TXA within three hours from hospital staff or a SAR helicopter paramedic.
RESULTS
Photo: Fiona Moore
1. The importance of early treatment with tranexamic acid in bleeding trauma patients: an exploratory analysis of the CRASH-2 randomised controlled trial. The CRASH-2 collaborators. The Lancet, Vol. 377, No.9771, p1096-1101 REFERENCE