
Tracheobronchopathia osteochondroplastica - CORE · The aetiology of TO remains obscure....
4
RESPIRATORY MEDICINE (1997) 91, 499-502 Tracheobronchopathia osteochondroplastica C. N. MEYER*, M. DBSSING* AND H. BROHOLM+ *Medical Department P and ‘Department of Pathology, BispebjevgHospital, Copenhagen, Denmark A case of tracheobronchopathia osteochondroplastica (TO) was diagnosed in a 6%year-old male with prolonged cough. A bronchoscopy revealed multiple nodular excrescences along the anterolateral wall of the trachea and main bronchi. Tissue specimens showed pronounced change of bronchial cartilage with massive mineralization diagnostic for TO. The literature on the subject is reviewed here. The aetiology and pathogenesis is unknown. The severity of TO range from no symptoms to severe dyspnoea, haemoptysis or pneumonitis. Treatment is seldom necessary. However, in severe cases, bronchoscopic removal of obstructing excrescences and surgery has been performed with therapeutic effect. Differential diagnosis of nodular excrescences includes amyloidosis, endobronchial sarcoidosis, calcificating lesions of tuberculosis, papilomatosis and tracheobronchial calcinosis. Awareness of the condition as a differential diagnosis to neo-plasms is important, to avoid unnecessary surgery or chemotherapy. RESPIR. MED. (1997) 91, 499-502 _-_;" - ._._. -.--.- _.-,,_._ __.;.. "I__".-_"."_-, I " -. Introduction Tracheobronchopathia osteochondroplastica (TO) is a rare disorder of the laryngotracheobronchial tree. The condition is benign, characterized by submucosal nodules containing combinations of cartilaginous, osseus, haemopoietic tissue and calcified acellular protein matrix, protruding into the bronchial lumen. In pronounced cases, the bronchoscopic picture is characteristic, described as beaded, spiculated, rock garden, cobble-stoned or stalactite grotto appear- ance. The overlying mucosa is often the site of squamous metaplasia and typically the posterior wall is spared (1). The first cases were described by Rokitansky (1855) Luschka (1856), and Wilks (1857) and since then, approximately 300 cases have been reported (2). Many cases are asymptomatic, and before the advents of bronchoscopy, it was mainly diagnosed incidentally post mortem. Symptoms may, however, be present as productive or non-productive cough, haemoptysis, dyspnoea, dryness of the throat, recurrent pulmonary infections or ozaena (3). Only rarely can TO be suspected from a conventional chest X-ray. Tomography and CT-scanning can be suggestive (4) but final verification requires biopsy. Received 27 December 1995 and accepted in revised form 20 August 1996. Correspondence should be addressed to: C. N. Meyer, Medical Department M-7721 Rigshospitalet, Tagensvej 20, 2200 Kbh N, Denmark. 0954-6111/97/080499+04 $12.00/O Case Report A 6X-year-old male presented with prolonged fatigue and a history of 8 months of recurrent cough with greenish sputum. Intermittently, he had experienced night sweats, chest pain provoked by deep breath, and a fever of 3940°C but had not received any kind of treatment. He had a tobacco consumption of lo-15 cigarettes since the age of 20 years. A middle lobe atelectasis had been diagnosed 6 yr previously. Supplementary tomography at that time did not reveal any tumour or bronchial stenosis, and was interpreted as chronic middle lobe syndrome. A chest X-ray obtained 2 yr later was normal. Three weeks prior to admission, a chest X-ray again showed a middle lobe atelectasis. This was confirmed by CT-scanning. In addition, several nodular excres- cences were seen prominating into the right main bronchus, the left superior bronchus and inferior lobe bronchus, and a rather diffuse thickening surround- ing the middle lobe bronchus. At bronchoscopy, multiple pale nodular excrescences 4-7 mm in size were observed beneath the vocal cords, extending into both main bronchi causing stenosis of the middle lobe bronchus. The nodules were distributed along the anterolateral wall of the trachea and the main bronchi, sparing the membranous wall of the trachea. The mucosa was intact. Biopsies revealed respiratory epithelium with a slightly thickened basal lamina with underlying elas- toid degeneration, without deposits of amyloid ;(;I 1997 W. B. SAUNDERS COMPANY LTD
Transcript of Tracheobronchopathia osteochondroplastica - CORE · The aetiology of TO remains obscure....

RESPIRATORY MEDICINE (1997) 91, 499-502
Tracheobronchopathia osteochondroplastica
C. N. MEYER*, M. DBSSING* AND H. BROHOLM+
*Medical Department P and ‘Department of Pathology, Bispebjevg Hospital, Copenhagen, Denmark
A case of tracheobronchopathia osteochondroplastica (TO) was diagnosed in a 6%year-old male with prolonged cough. A bronchoscopy revealed multiple nodular excrescences along the anterolateral wall of the trachea and main bronchi. Tissue specimens showed pronounced change of bronchial cartilage with massive mineralization diagnostic for TO. The literature on the subject is reviewed here. The aetiology and pathogenesis is unknown. The severity of TO range from no symptoms to severe dyspnoea, haemoptysis or pneumonitis. Treatment is seldom necessary. However, in severe cases, bronchoscopic removal of obstructing excrescences and surgery has been performed with therapeutic effect. Differential diagnosis of nodular excrescences includes amyloidosis, endobronchial sarcoidosis, calcificating lesions of tuberculosis, papilomatosis and tracheobronchial calcinosis. Awareness of the condition as a differential diagnosis to neo-plasms is important, to avoid unnecessary surgery or chemotherapy.
RESPIR. MED. (1997) 91, 499-502
_-_;" - ._._. -.--.- _.-,,_._ __.;.. "I__".-_"."_-, I " -.
Introduction
Tracheobronchopathia osteochondroplastica (TO) is a rare disorder of the laryngotracheobronchial tree. The condition is benign, characterized by submucosal nodules containing combinations of cartilaginous, osseus, haemopoietic tissue and calcified acellular protein matrix, protruding into the bronchial lumen. In pronounced cases, the bronchoscopic picture is characteristic, described as beaded, spiculated, rock garden, cobble-stoned or stalactite grotto appear- ance. The overlying mucosa is often the site of squamous metaplasia and typically the posterior wall is spared (1). The first cases were described by Rokitansky (1855) Luschka (1856), and Wilks (1857) and since then, approximately 300 cases have been reported (2). Many cases are asymptomatic, and before the advents of bronchoscopy, it was mainly diagnosed incidentally post mortem. Symptoms may, however, be present as productive or non-productive cough, haemoptysis, dyspnoea, dryness of the throat, recurrent pulmonary infections or ozaena (3). Only rarely can TO be suspected from a conventional chest X-ray. Tomography and CT-scanning can be suggestive (4) but final verification requires biopsy.
Received 27 December 1995 and accepted in revised form 20 August 1996. Correspondence should be addressed to: C. N. Meyer, Medical Department M-7721 Rigshospitalet, Tagensvej 20, 2200 Kbh N, Denmark.
0954-6111/97/080499+04 $12.00/O
Case Report
A 6X-year-old male presented with prolonged fatigue and a history of 8 months of recurrent cough with greenish sputum. Intermittently, he had experienced night sweats, chest pain provoked by deep breath, and a fever of 3940°C but had not received any kind of treatment. He had a tobacco consumption of lo-15 cigarettes since the age of 20 years. A middle lobe atelectasis had been diagnosed 6 yr previously. Supplementary tomography at that time did not reveal any tumour or bronchial stenosis, and was interpreted as chronic middle lobe syndrome. A chest X-ray obtained 2 yr later was normal. Three weeks prior to admission, a chest X-ray again showed a middle lobe atelectasis. This was confirmed by CT-scanning. In addition, several nodular excres- cences were seen prominating into the right main bronchus, the left superior bronchus and inferior lobe bronchus, and a rather diffuse thickening surround- ing the middle lobe bronchus. At bronchoscopy, multiple pale nodular excrescences 4-7 mm in size were observed beneath the vocal cords, extending into both main bronchi causing stenosis of the middle lobe bronchus. The nodules were distributed along the anterolateral wall of the trachea and the main bronchi, sparing the membranous wall of the trachea. The mucosa was intact.
Biopsies revealed respiratory epithelium with a slightly thickened basal lamina with underlying elas- toid degeneration, without deposits of amyloid
;(;I 1997 W. B. SAUNDERS COMPANY LTD
500 C. N. MEYER ET AL
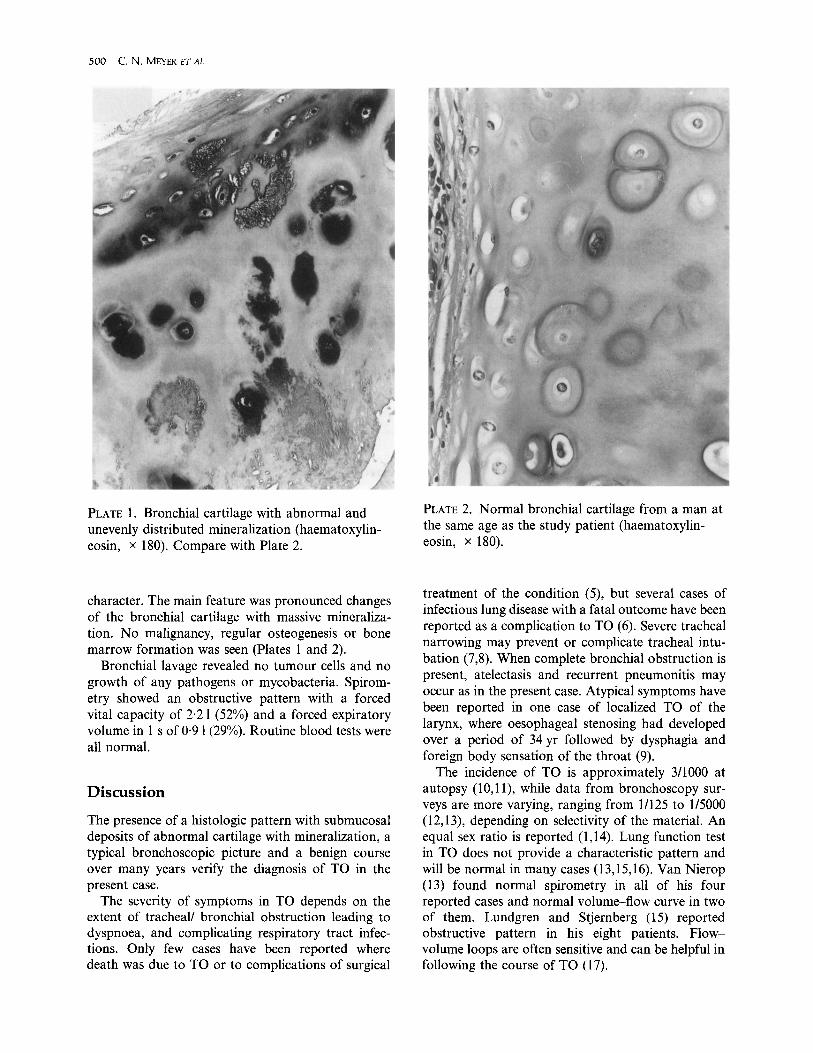
PLATE 1. Bronchial cartilage with abnormal and unevenly distributed mineralization (haematoxylin- eosin, x 180). Compare with Plate 2.
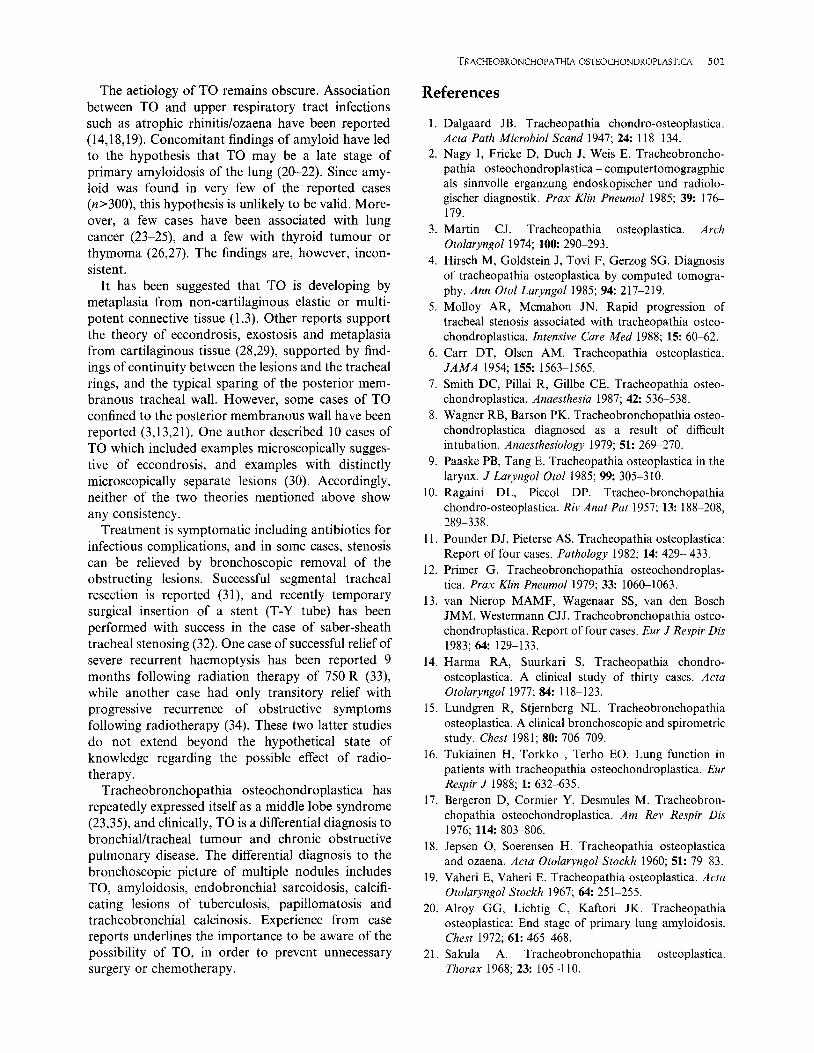
character. The main feature was pronounced changes of the bronchial cartilage with massive mineraliza- tion. No malignancy, regular osteogenesis or bone marrow formation was seen (Plates 1 and 2).
Bronchial lavage revealed no tumour cells and no growth of any pathogens or mycobacteria. Spirom- etry showed an obstructive pattern with a forced vital capacity of 2.2 1 (52%) and a forced expiratory volume in 1 s of 0.9 1(29%). Routine blood tests were all normal.
Discussion
The presence of a histologic pattern with submucosal deposits of abnormal cartilage with mineralization, a typical bronchoscopic picture and a benign course over many years verify the diagnosis of TO in the present case.
The severity of symptoms in TO depends on the extent of tracheal/ bronchial obstruction leading to dyspnoea, and complicating respiratory tract infec- tions. Only few cases have been reported where death was due to TO or to complications of surgical
PLATE 2. Normal bronchial cartilage from a man at the same age as the study patient (haematoxylin- eosin, x 180).
treatment of the condition (5), but several cases of infectious lung disease with a fatal outcome have been reported as a complication to TO (6). Severe tracheal narrowing may prevent or complicate tracheal intu- bation (7,8). When complete bronchial obstruction is present, atelectasis and recurrent pneumonitis may occur as in the present case. Atypical symptoms have been reported in one case of localized TO of the larynx, where oesophageal stenosing had developed over a period of 34 yr followed by dysphagia and foreign body sensation of the throat (9).
The incidence of TO is approximately 3/1000 at autopsy (10,l l), while data from bronchoscopy sur- veys are more varying, ranging from l/125 to l/5000 (12,13), depending on selectivity of the material. An equal sex ratio is reported (1,14). Lung function test in TO does not provide a characteristic pattern and will be normal in many cases (13,15,16). Van Nierop (13) found normal spirometry in all of his four reported cases and normal volume-flow curve in two of them. Lundgren and Stjernberg (15) reported obstructive pattern in his eight patients. Flow- volume loops are often sensitive and can be helpful in following the course of TO (17).
The aetiology of TO remains obscure. Association between TO and upper respiratory tract infections such as atrophic rhinitis/ozaena have been reported (14,18,19). Concomitant findings of amyloid have led to the hypothesis that TO may be a late stage of primary amyloidosis of the lung (20-22). Since amy- loid was found in very few of the reported cases (n>300), this hypothesis is unlikely to be valid. More- over, a few cases have been associated with lung cancer (23-25), and a few with thyroid tumour or thymoma (26,27). The findings are, however, incon- sistent.
It has been suggested that TO is developing by metaplasia from non-cartilaginous elastic or multi- potent connective tissue (1,3). Other reports support the theory of eccondrosis, exostosis and metaplasia from cartilaginous tissue (28,29), supported by find- ings of continuity between the lesions and the tracheal rings, and the typical sparing of the posterior mem- branous tracheal wall. However, some cases of TO confined to the posterior membranous wall have been reported (3,13,21). One author described 10 cases of TO which included examples microscopically sugges- tive of eccondrosis, and examples with distinctly microscopically separate lesions (30). Accordingly, neither of the two theories mentioned above show any consistency.
Treatment is symptomatic including antibiotics for infectious complications, and in some cases, stenosis can be relieved by bronchoscopic removal of the obstructing lesions. Successful segmental tracheal resection is reported (31), and recently temporary surgical insertion of a stent (T-Y tube) has been performed with success in the case of saber-sheath tracheal stenosing (32). One case of successful relief of severe recurrent haemoptysis has been reported 9 months following radiation therapy of 750 R (33), while another case had only transitory relief with progressive recurrence of obstructive symptoms following radiotherapy (34). These two latter studies do not extend beyond the hypothetical state of knowledge regarding the possible effect of radio- therapy.
Tracheobronchopathia osteochondroplastica has repeatedly expressed itself as a middle lobe syndrome (23,35), and clinically, TO is a differential diagnosis to bronchial/tracheal tumour and chronic obstructive pulmonary disease. The differential diagnosis to the bronchoscopic picture of multiple nodules includes TO, amyloidosis, endobronchial sarcoidosis, calcifi- eating lesions of tuberculosis, papillomatosis and tracheobronchial calcinosis. Experience from case reports underlines the importance to be aware of the possibility of TO, in order to prevent unnecessary surgery or chemotherapy.
TRACHEOBRONCHOPATHIAOSTEOCHONDROPLASTICA 501
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
11.
18.
19.
20.
21.
Dalgaard JB. Tracheopathia chondro-osteoplastica. Acta Path Microbial Stand 1947; 24: 118134. Nagy I, Fricke D, Duch J, Weis E. Tracheobroncho- pathia osteochondroplastica - computertomogragphie als sinnvolle erganzung endoskopischer und radiolo- gischer diagnostik. Prax Klin Pneumol 1985; 39: 176- 179. Martin CJ. Tracheopathia osteoplastica. Arch Otolaryngol 1974; 100: 290-293. Hirsch M, Goldstein J, Tovi F, Gerzog SG. Diagnosis of tracheopathia osteoplastica by computed tomogra- phy. Ann Otol Laryngol 1985; 94: 217-219. Molloy AR, Mcmahon JN. Rapid progression of tracheal stenosis associated with tracheopathia osteo- chondroplastica. Intensive Care Med 1988; 15: 60-62. Carr DT, Olsen AM. Tracheopathia osteoplastica. JAMA 1954;155: 1563-1565. Smith DC, Pillai R, Gillbe CE. Tracheopathia osteo- chondroplastica. Anaesthesia 1987; 42: 536538. Wagner RB, Barson PK. Tracheobronchopathia osteo- chondroplastica diagnosed as a result of difficult intubation. Anaesthesiology 1979; 51: 269-270. Paaske PB, Tang E. Tracheopathia osteoplastica in the larynx. J Laryngol Otol 1985; 99: 3055310. Ragaini DL, Piccol DP. Trachea-bronchopathia chondro-osteoplastica. Riv Anat Put 1957; 13: 1888208, 289-338. Pounder DJ, Pieterse AS. Tracheopathia osteoplastica: Report of four cases. Pathology 1982; 14: 429- 433. Primer G. Tracheobronchopathia osteochondroplas- tica. Prax Klin Pneumol 1979; 33: 1060-1063. van Nierop MAMF, Wagenaar SS, van den Bosch JMM, Westermann CJJ. Tracheobronchopathia osteo- chondroplastica. Report of four cases. Eur J Respir Dis 1983;64: 129-133. Harma RA, Suurkari S. Tracheopathia chondro- osteoplastica. A clinical study of thirty cases. Acta Otolaryngol 1977; 84: 118-123. Lundgren R, Stjernberg NL. Tracheobronchopathia osteoplastica. A clinical bronchoscopic and spirometric study. Chest 1981; 80: 706-709. Tukiainen H, Torkko , Terho EO. Lung function in patients with tracheopathia osteochondroplastica. Eur Respir J 1988; 1: 632-635. Bergeron D, Cormier Y, Desmules M. Tracheobron- chopathia osteochondroplastica. Am Rev Respir Dis 1976; 114: 803-806. Jepsen 0, Soerensen H. Tracheopathia osteoplastica and ozaena. Acta Otolaryngol Stockh 1960; 51: 79983. Vaheri E, Vaheri E. Tracheopathia osteoplastica. Acta Otolaryngol Stockh 1967; 64: 251-255. Alroy GG, Lichtig C, Kaftori JK. Tracheopathia osteoplastica: End stage of primary lung amyloidosis. Chest 1972; 61: 465468. Sakula A. Tracheobronchopathia osteoplastica. Thorax 1968;23: 105-l 10.

502 C. N. MEYER ET AL.
22. Jones AW, Chatterji AN. Primary tracheobronchial amyloidosis with tracheopathia osteoplastica. Br J Dis Chest 1977; 71: 268-272.
23. de Wall N, Roggenbuck C, Endres P, Hau T. Tracheo- bronchopathia osteochondroplastica und koexistentes mukoe-pidermoidkarzinom der lunge: Fallvorstellung. Pneumologie 1992; 46: 7477.
24. Dalgaard JB. Lungecancer ved tracheopathia chondro- osteoplastica. Nerd Med 1955; 53: 572-575.
25. Kissler W, Wierich W, Meessen D. Tracheobroncho- pathia osteochondroplastica und bronkialkarzinom. Prax Klin Pneumol 1977; 31: 660-663.
26. Morita S, Yokoyama N, Yamashita S et al. Tracheo- pathia osteochondroplastica complicated with thyroid cancer: case report and review of the literature in Japan. Jpn J Med 1990; 29: 637-641.
27. Kishikawa M, Nagashima Y. Tracheobronchopathia osteoplastica complicating thymoma. Jpn J Thorac Dis 1978; 16: 347-351.
28. Pounder DJ, Pieterse AS. Tracheopathia osteoplastica: A study of the minimal lesion. J Pathology 1982; 138: 235-239.
29. Young RH, Sandstom RE, Mark GJ. Tracheopathia osteoplastica. J Thorac Cardiovasc Surg 1980; 79: 537- 541.
30. Way SPB Tracheopathia osteoplastica. J Clin Path 1967; 20: 814820.
31. O’Reilly RR, Marty AT. Tracheopathia osteoplastica: case report. Ml Med 1978; 143: 497498.
32. Patterson GA, Grill0 HC, Mark EJ. Case records of the Massachusetts General Hospital. Case 461992. N Eng J Med 1992; 21: 1512-1518.
33. Clerf LH. Tracheopathia osteoplastica. Ann Otol Rhino1 Larjmg 1944; 53: 839-844.
34. Howland WJ, Good CA. The radiographic features of tracheopathia osteoplastica. Radio1 1958; 71: 847-850.
35. Hodges MK, Israel E. Tracheobronchopathia osteo- chondroplastica presenting as right middle lobe col- lapse. Chest 1988; 94: 841-844.


















