
Toxoplasmosis- Dr. Ndaos3.amazonaws.com/prealliance_oneclass_sample/9eA3vbAGz3.pdf · Eimeria...
49
1 Parasitology Final Study Guide (Post MT Material) Toxoplasmosis- Dr. Ndao: Aside: Chagas Disease can be transmitted up to 3-4 generations. Parasites: Some of the parasites that we will discuss are bioterrorism organisms; if they are dumped into our water supply, the way that we treat our water will not kill them. There is a way to treat a Toxoplasmosis (Toxoplasma gondii) infection, but it is difficult. 33-50% of us are already infected with this parasite. When women get pregnant, often the dormant parasite becomes active. Life Cycle: The life cycle is very simple compared to other parasites. T. gondii can infect any warm-blooded vertebrate, including cats. But important is that most infection is through intermediate hosts; this is when the asexual stage of the parasite occurs. Intermediate hosts would include humans. The definitive host has the sexual stage of the parasite, therefore the gametes and the oocysts are in the felines. HINT: When diagnosing, it is important that you would not look in the feces of intermediate hosts to try and find oocysts. In intermediate hosts, you need to be looking for sero-positivity. In this case we would be looking for IgM (more recent), IgG (exposed a while ago).
Transcript of Toxoplasmosis- Dr. Ndaos3.amazonaws.com/prealliance_oneclass_sample/9eA3vbAGz3.pdf · Eimeria...

1
Parasitology Final Study Guide (Post MT Material)
Toxoplasmosis- Dr. Ndao:
Aside: Chagas Disease can be transmitted up to 3-4 generations.
Parasites:
Some of the parasites that we will discuss are bioterrorism organisms; if they are dumped into our water supply, the way that we treat our water will not kill them.
There is a way to treat a Toxoplasmosis (Toxoplasma gondii) infection, but it is difficult.
33-50% of us are already infected with this parasite. When women get pregnant, often the dormant parasite becomes active.
o Only in France and Austria is there mandatory Toxo screening for pregnant women o Aside: Trichimonas foetus and Trichimonas vaginalis are also problems
There is only ONE species for Toxoplasmosis. o It is part of the phylum Apicomplexa
Toxoplasma:
Domain = Eukaryota
Kingdom = Chromalveoata
Superphylum = Alveolata
Phylum = Apicomplexa
Class = Coccidia o Other Coccidian parasites:
Eimeria species, Sarcocystis species, Neospora species, Cryptosporidium species All Eukaryotes, unicellular, intracellular
Order = Eucoccidiorida
Family = Sarcocystidae
Genus = Toxoplasma
Species (ONLY ONE) = T. gondii
Toxoplasma is a food and water borne pathogen. The development of oocytes that are shed with the definitive host (cat) feces and contaminate the encironment.
Toxoplasma gondii:
A protozoan parasite that was first described in 1908 in Tunis by Nicolle (also got the Nobel Prize for typhus) and Manceaux in the gundi (Ctenodoactylus gundi), whch is an African rodent. The same year it was described in Brazil by Splendore in rabbits.
In 1909, the organism was named Toxoplasma gondii.
Several decades passed before the pathogenic role of T. gondii in humans was discovered: o The first recorded congenital case = 1923 o The first recorded adult case = 1940
1948: Sabin and Feldman serological dye test (the standard basis for diagnositic tests).
Beginning of the 1970s: whole parasite life cycle described by Frenkel and Hutchinson.
Life Cycle:
The life cycle is very simple compared to other parasites.
T. gondii can infect any warm-blooded vertebrate, including cats. But important is that most infection is through intermediate hosts; this is when the asexual stage of the parasite occurs. Intermediate hosts would include humans. The definitive host has the sexual stage of the parasite, therefore the gametes and the oocysts are in the felines.
HINT: When diagnosing, it is important that you would not look in the feces of intermediate hosts to try and find oocysts. In intermediate hosts, you need to be looking for sero-positivity. In this case we would be looking for IgM (more recent), IgG (exposed a while ago).

2
o HOWEVER sometimes when you get infected the IgM can remain in the body for up to 2 years. So you can take a blood sample and look for it. You can also look for Ag-Ig binding in a blood sample.
So the oocysts are only in cats, and the intermediate hosts have 4 sporozoites. Most intermediate hosts might have the dormant bradyzoites, which may be activated later. Intermediate hosts can be infected by cat litter, or by meat (raw, undercooked) from other intermediate hosts. Infected water is another way.
When your immune system is down, tachyzoites cross the placenta and the baby will get the disease. There is even ocular toxoplasmosis, and it can also get into the brain.
Contamination:
Occurs mainly by the oral route. o 1. Ingestion of raw or partly cooked meat (especially pork, lamb, or venison) thatcontains tissue
cysts of bradyzoites. Hand-to-mouth contact after handing undercooked meat, or from using utensils
contaminated by raw meat that contains tissue cysts. o 2. Ingestion of oocyst-contaminated cat feces through hand-to-mouth contact:
Unwashed vegetables, gardenine, cleaning a cat litter box, contact with child sandboxes, touching anything that has come into contact with cat feces.
o 3. Drinking water that is contaminated with oocysts (sporozoites). o 4. Transplacental infection in utero (tachyzoites) o 5. Transplantation of an infected organ (bradyzoites in tissue cysts) or blood transfusion
(tachyzoites- rare).
T. gondii is a major zoonotic pathogen:
There is a huge reservoir in intermediate hosts.
Prevalence in humans: o ~30% of the human population is seropositive. o Up to 60% in Quebec (especially Nunavilk Inuit), Nunavut, Western Europe o Depends mostly on nutritional habits (where undercooked meat is traditionally eaten), and on
contact with cats.
Prevalence in animals: o ~10% in pork, ~40% in sheep/lamb, and 20-63% in goats (Quebec, 2000).
Toxoplasmosis is usually benign:
An average of 30% of the population is seropositive for Toxoplasma, but very few have developed clinical symptoms because the immune response is usually very efficient.
o First line of defense is the innate immune system (neutrophils, DCs, macrophages). These become activated, release IL-12, IFN-gamma, and try to get rid of the infection there.
o But the parasite interacts with the immune system in order to survive.
Acute toxoplasmosis can be asymptomatic, but flu-like symptoms are often observed (1-3 weeks post-infection).
The acute phase (virulent tachyzoites) fades in a few days to weeks, leading to the latent stage of the infection (bradyzoite tissue cysts), which is normally asymptomatic.
o The parasite does not want to come in and kill you right away; this is not very helpful for the parasite.
Any nucleated cell can be infected by the tachyzoites.
Toxoplasmosis is not benign in two cases: o 1. In the case of immunocompromised patients (HIV/AIDS, transplant or cancer patients on
immunosuppressive therapy), toxoplasmosis can develop. The most notable manifestation is the toxoplasmic encephalitis, which is fatal without drug treatment.
o 2. If a primary infection with T. gondii occurs during pregnancy, tachyzoites can cross the placenta, possibly leading to hydrocephaly, microcephaly, intracranial calcification and chorioetinitis, with the possibility of miscarriage or intrauterine death. Ocular toxoplasmosis may occur later in life.
Infection in the 1st trimester: incidence of transplacental infection is low (15%) but disease in neonate is most severe.

3
Infection in the 3rd trimester: incidence of transplacental infection is high (65%) but infant is usually asymptomatic at birth.
Clinical toxoplasmosis in vulnerable groups: common denominator = compromised immunological mechanisms.
o 1. AIDS patients: symptomatic phase when CD4 T cell count < 200 cells/microlitre due to tissue cyst reactivation- toxoplasmic encephalitis (TE).
When the bradyzoites are shifted to tachyzoites (because it is sensed that the host is lacking IFNgamma or IL12 for example).
When there is stress/HSP, then the tachyzoite will go back to the bradyzoite. o 2. Allograft organ recipients: immunosuppressive therapy is necessary to tolerate the allograft,
but high risks of tissue cyst reactivation. o 3. Patients on prolonged corticosteroid therapy: powerful anti-inflammatory drug to suppress
inflammatory disorder. o 4. Fetus (incmpetent immunological mechanisms): transplacental transmission of tachyzoites.
The tachyzoite of T. gondii: the
acute/invasive/proliferative stage.
6-7 micrometers in length, 2-3 micrometers in width.
Replicate intracellularly in any nucleated cell.
T. gondii sub-cellular organelles:
When the parasite invades, they will form a parasitophore/vacuole so that they are protected.
Some stage-specific surface antigens (SAG) are present, so when you want to diagnose, it is easy to find something immunogenic in the host.
o Adhesins: (SAG1, SAG2, SAG2b, SAG3, etc): GPI-anchored proteins, which act as redundant receptors for binding or self-proteoglycans on various host cells.
Toxoplasma has a complete set of canonical eukaryotic organelles (nucleus, secretory pathway, etc) plus TWO endosymbionic organelles (mitochondrion, apicoplast). The parasite contains an “apical complex” of specialized cytoskeletal elements and secretory organelles (micronemes, rhoptries). Rhoptries and the microneme are secretory vesicles that help to invade host cells. It also contains an inner membrane complex.
Replication is by endodyogeny: assembly of two daughter cells within a mother cell, therefore they divide in exponential form.
The bradyzoite of T. gondii; the dormant, chronic stage.

4
Morphologically similar to tachyzoites, but have distinct antigenicity and physiology (different set of SAG surface antigens).
Granules of amylopectine (reserve of carbohydrates)
Bradyzoites reside in tissue cysts, which are derived from a parasitophorous vacuole + a cyst wall – 10 to 200 micrometers.
The dormant stage found in muscles (infective stage), brain, persist for the lifetime of the host.
The bradyzoite tachyzoite interconversion is central in the pathogenesis of Toxoplasma gondii. Reactivation into tachyzoites occurs in immnosuppressed patients (brain- Toxoplasmic encephalitis (TE), retina- Ocular toxoplasmosis, heart, etc). Unlike tachyzoites, bradyzoites are resistant to low pH and host digestive proteases (in the stomach).
Tachyzoite Bradyzoite: low pH, high pH, heat shock, mitochondrial inhibition, presence of NO o Common denominators between the stresses that induce conversion to the bradyzoite: induction
of HSP, phosphorylation of the alpha subunit of eukaryotic initiation factor-2 (TgIF2alpha).
Bradyzoite Tachyzoite: lack of NO, lack of IFN-gamma, lack of TNF-alpha, lack of T cells, lack of IL-12
The sporozoite/oocyst of T. gondii: the sexual stage:
Oocyst, oval, ~13 micrometers in size, resistant stage- viable in moist soil- 18 months.
A product of the sexual cycle (micro and macrogametes), which occurs in the intestinal cells of definitive hosts (cats).
Passed out in the feces by definitive host/carnivores (cat) feces 10-14 days after infection.
Each sporulated oocyst contains 8 sporozoites (~5 days) o The 8 sporozoites inside the oocysts are in sporocysts. Each sporocyst has 4, so therefore there
are two sporocysts in each oocyst.
Infective to humans and other herbivore hosts
HINT: present in the oocysts of the definitive host.
The oocyst is the spore stage of certain protists. o The oocyst wall may be compared to the exoskeleton of insects, or to the cuticle of nematodes:
it is essential for survival. o Because of the oocyst wall, they are very resistant to dessication and chemical disinfection. o Oocysts can survive for lengthy periods of time outside of a host (months to years in a moist
environment). o Because they are so hard to kill, there are several outbreaks.
Resistance:
Physical agents (UV, dessication, freezing)
Chemical agents (ozone, bleach, iodine, ethanol, formalin, salts) Persistence:
18 months in soil, 54 months in water
The coccidian oocyst: characteristics o The oocyst is unsporulated and non-infectious when excreted; it contains a single,
undifferentiated cytoplasmic mass and is essentially the zygote stage of the parasite surrounded by a protective wall.
o At appropriate temperatures and humidity, sporulation occurs by meiotic division. During this process the cytoplasm divides into a characteristic number of sub-masses (secondary sporoblasts), which develop a resistant wall and are termed sporocysts. Within the sporocysts, the infectious stages (sporozoites) are formed. The sporozoites are thus protected by both the oocyst and sporocyst walls.
o Must be sporulated for the infectious stage.
The oocyst of T. gondii is infectious to virtually all warm-blooded vertebrates, including humans.
Oocyst shedding by cats: o Cats can shed oocysts in their feces for several weeks after the initial contamination (usually by
feeding on infected rodent): However, oocysts become infectious 1-2 days after shedding, after sporulation. It is estimated that only ~2% of cats shed oocysts at any one time

5
Oocyst shedding does not reoccur even after repeated exposure to the parasite Oocysts have been detected on cut fur, but not in an infectious form; direct infection
from handling cats is believed to be very rare.
Waterborn transmission of protozoan parasites:
At least 325 water-associated outbreaks of parasitic protozoan disease reported. North American and European outbreaks account for 93% of all reports, ~2/3 of all reports occurred in North America.
SPECIES # OF CASES % OF CASES
Giardia duodenalis 132 40.6%
Cryptosporidium parvum 165 50.8%
Entamoeba histolytica 6 1.8%
Cyclospora cayetanesis 9 2.8%
Toxoplasma gondii 3 0.9%
Water borne contamination can be by sewage, point source (storm drains) or runoff (non-point source pollution).
Wildlife are also susceptible to waterborne toxoplasmosis o Otters in California (38%), due to contaminated freshwater runoff in coastal waters
It is a Category B Biodefense pathogen (threat to the public water supplies)
Immune Response against T. gondii:
In immune competent hosts: o Predominantly controlled by cell-mediated immunity o Humoral immunity also involved
During both acute (mostly innate immune system) and chronic (mostly adaptive immune system) phase of toxoplasmosis:
o CD8+ T cells are major effectors o CD4+ T cells are crucial for regulation of the immune response o NK and macrophages are the first lines of defense during the early phase o IL12 is cricual for the induction of an efficient Th1 response against T. gondii.
Produced by DCs especially, but also macrophages and neutrophils. Th1 response could cause tissue damage because of NO, TNF, etc (cytokine storm).
Those with Crohn‟s disease or IBD suffer a lot because of this. This results in necrosis (pan-ileitis) of the small intestine.
o The major effector: IFNgamma Activates both haematopoietic and non-haematopoietic effector cells, which restrict
parasite intracellular growth/kill intracellular parasites. o Other important effectors (depending on cell types and host species):
ROS and NO metabolites (IFNgamma dependent) Tryptophan starvation (IFNgamma dependent) p47 GTPases (IFNgamma dependent) TNFalpha, IL6, IL1: synergy
Type 1 innate immunity: o Innate recognition by TLR 11 and MyD88 (important), DC releases IL-12, NK releases IFN-
gamma, macrophages execute intracellular killing.
Diagnosis of Toxoplasmosis:
Because T. gondii is intracellular in the host, it is usually difficult to demonstrate the presence of parasites in clinical material.
Acute infection is assessed by serology (IgG and IgM). o IgG Abs usually appear 1-2 weeks after the initiation of infection, reaching peak titres in 6-8
weeks, then gradually decline over 1-2 years. o Titres, usually at low levels, probably persist for life. Some correlate with severity of illness.
ELISAs are now abailable are are preferred, as live parasites are not required to carry out the serology assay.

6
Intra-uterine and cerebral disease can be diagnosed by PCR.
Prevention:
When people are infected, there are still bradozoites after treatment. So it is hard to treat!
Toxo is considered to be the 3rd leading cause of death attributed to foodborne illness in the USA. (Costing $7 billion/year in the USA).
Prevention: o Avoid undercooking meat o Wash fruit and vegetables o Avoid soil contact o Avoid drinking untreated water o Avoid cats if pregnant (controversial) o Empty litterbox daily
Pregnancy precautions: o Blood test initially to determine whether or not the woman was exposed/is at risk.
(-): monthly serological testing is advisable (treatment during pregnancy dramatically decreases the risk of passing the parasite to the fetus)
o Systematic screening: Italy, France, Austria o Regional screening programs: Belgium, Canada (Nunavit, Nunavik Inuit), Germany, Switzerland
Treatments:
Acute: o Pyrimethamine: interferes with folic acid synthesis by inhibiting the enzyme DHFR; an
antimalarial medication o Sulfadiazine: sulfonamide antibiotic (folic acid synthesis) used in combination with
pyrimethamine o Clindamycin: lincosamide antibiotic used most often for people with HIV/AIDS (interferes with
protein synthesis) o Spiramycin: macrolide antibiotic used most often for pregnant women (interferes with protein
synthesis)
Chronic: o Tissue cysts are resistant to most treatments o Some studies in the mouse model have shown some results with:
Atovaquone and Clindamycin
Why is Toxoplasmosis so successful?
Intracellular: protected from Abs, etc.
Can infect any nucleated cell in warm-blooded vertebrate

7
Chronic infection in immune privileged areas
Intracellular niche (vacuole) is resistant to fusion with the host cell lysosomes
T. gondii manipulates host-cell processes (apoptosis, cytoskeleton, etc)
Also manipulates host cell immune effectors (downregulation of antigen presentation to T cells, upregulation of anti-inflammatory mechanisms, use of DCs and neutrophils to cross blood brain barrier.
HOWEVER, hosts are rarely killed. A balanced host-parasite interaction is established, and is necessary for T. gondii survival, persistence and transmission.
Schistosomiasis- Dr. Ndao
See notes attached.

8
Trichinellosis- Dr. Ndao:
While Schistosoma was a helminth, Trichinella is a nematode. It is the smallest nematode, and it looks like a
virus (even though nematodes are round worms).
Trichinellosis, the proper term of trichinosis or trichiniasis, trichinelliasis caused by the smalles nematode parasite of humans (Trichinella).
Unrecognized disease for thousands of years
Food-borne zoonosis (undercooked emat, which will release the larvae that will infect the intestines).
Prevalence of swine trichinellosis and the incidence of human greater in developing countries (China, Thailand, Mexico, Argentina, Bolivia, some central European countries)
Not recognized for a long time, because the acute infection symptoms are inflammation, which goes away. Later on a cyst can remain in the muscle for years.
Most nematodes have eggs (eg: ascaris), but with this parasite there are NO eggs in the stool.
Main epidemiological features of Trichinella:
SPECIES DISTRIBUTION MAJOR HOSTS REPORTED FROM HUMANS
T. spiralis (most common) Cosmopolitan Domestic pigs, wild mammals
Yes
T. britovi Eurasia Wild mammals Yes
T. murrelli North America Wild mammals Yes
T. nativa Arctic Bears, walrus Yes
T. nelsoni South-East Asia Hyenas, felids Yes
T. pseudospiralis* Cosmopolitan Wild mammals, birds Yes
T. papuae* Papua New Guinea, Thailand
Wild pigs, crocodiles Yes
T. zimbabwensis* Zimbabwe, Ethiopia, Mozambique
Crocodiles No
* = non-encapsulated species (HINT)

9
Problem with diagnosis is that when you take serum in acute phase, you do not see any Abs. You have to repeat the serology later on.
Trichinella in humans:
SPECIES RESERVOIRS
T. spiralis Pig
T. nativa Polar bear, walrus
T. britovi Fox, pig, wild boars, horses, jackals, cat
T. pseudospiralis Pig
T. nelsoni Bush pigs, warthogs
Can infect all mammals, birds and reptiles. But humans are the only ones who suffer with the disease. Animals get cysts but have no problems. Most of the reservoirs are pigs.
Distribution:
T. spiralis is very widespread, while T. pseudospiralis is in North America, Europe and Asia as well as Tasmania.
HINT: T. nativa is up north
Characteristics of Trichinella species:
SPECIES DISTRIBUTION CHARACTERISTICS (HINT)
T. spiralis Cosmopolitan High reproductive capacity (only one), no freezing resistance
T. nativa Arctic regions Low reproductive capacity, freezing resistance* (really need to cook
meat)
T. pseudospiralis Cosmopolitan Low reproductive capacity, no freezing resistance, no capsule*
T. nelsoni Africa Low reproductive capacity, no freezing resistance
T. britovi Temperate zone Low reproductive capacity, freezing resistance
Trichinella: an unusual nematode!
World‟s largest intracellular parasite
Non-host specific
The smallest worm among the nematodes
One of the most widespread and clinically important nematode in the world
Same individual serves as both definitive and intermediate host
The worm that would be a virus... o Trichinella was described for the first time in 1835 by Owen from a cadaver muscle in London o Raillet baptized this non-segmented soundworm nematode Trichinella spiralis in 1895. o Nematodes are usually host specific but trichinella is able to adapt to a variety of hosts. o The infection has a worldwide distribution, including the Arctic, temperate lands and the tropics. o Puerto Rico and Australia are free of trichinellosis. o Juveniles are carried away by the hepatoportal system through the liver, the heart, the lungs and
the arterial system. They are found in all tissues. o Eventually they reach the skeletal muscle.
LIKE A VIRUS, they penetrate individual fibres. LIKE A VIRUS, they subvert and redirect the host activities to their own sirvival. LIKE A VIRUS, they alter gene expression of the host cell from that of a contractile fiber to that of a nurse cell.
o There are no eggs produced by the parasite.
Life Cycle:

10
Humans are infected mostly by eating undercooked meat that has cysts (containing larvae).
Males and females will mate; after several populations the male dies and the females release the juveniles, that migrate everywhere, sometimes even in the CNS.
Remember: cysts in the muscle, juveniles into the body, mating, juvenile release, moving through out the body.
What causes pathology is the adult worm threading through the intestinal epithelium.
Biological features:
During its life cycle, Trichinella larvae undergo 4 molts over a period of 30 hours developing into adults.
The female measures 3 mm in length, while the male measures 1.5 mm in length.
The newborn larvae measure 0.8 mm in length.
Patency begins 5 days after mating. Males can cpulate several times and die shortly after adult females release life offspring.
The larvae are carried away by the hepatoportal system, which distributes them throughout the body.
They are found in all tissues and muscles.
Like viruses, the larvae alter the gene expression of the host cell. They are able to change the vocation of the contractile fibre to that of a nurse cell and they become intra-cellular parasites. In other words, they enter fibrocytes, forming a cyst. Then can survive for more than 20 years in this way.
Steps leading to encystation:
1. Larvae enter the muscle fibre cell 2. Fibre loses its myofilaments 3. Fibre nuclei enlarge 4. Fibre smooth ER increases 5. Fibre mitochondria degenerates 6. Encapsulation of the unit (not the 3 that do not do this, however example T. pseudospiralis) with
collagen secreted by neighbouring fibroblasts. a. Calcification of the encysted larvae occur in about 18 months. Encysted larvae can stay alive for
years (even upon death of the host). They can be seen by X-ray.
Stichosome:
11
The stichosome consists of a row of discoid cells containing secretory granules. It can be found in the larvae.
These cells are called stichocytes and they secrete antigens into the nurse cell-parasite complex during nurse cell formation.
It has been hypotheisez that secretory-excretory substances from the stichocytes not only are immunogenic but mediate alteration of host gene expression.
Invasion of muscles:
Some muscles are much more heavily invaded than others, but we do not know why.
Most invaded muscles are: o Eye, tongue, masticatory muscles, diaphragm, intercostals, arms and legs.
Nurse cells do not form in the heart muscle cells. They do not encyst in smooth muscles. Myocarditis is transitory.
Nurse cells do not form in the nervous system (CNS).
However, larvae can be found migrating everywhere.
Invasion of muscles is accompanied by an intense inflammatory reaction.
Edema develops 14 days after penetration of the muscle cell.
The inflammatory reaction is raised after the release of secretory-excretory antigens.
Aside: when the larvae are released into the small intestine, you expect to get as the main clinical sign myopathy and cramps/diarrhea. When you have the larvae form cysts in muscles, the main sign that you will get is body aches and inflammation especially. Eosinophils are good indicators of helminth infections. IL5 helps to bring out the larvae in order to kill them.
o In terms of an immune response, you would expect more of a Th1 response (it is like a virus, remember). Keep in mind that Eosinophils play a major role in the clearance of Trichinella.
Resistance to infections may be classified into 3 categories:
1. Innate resistance: a. Natural resistance to infection. For example, Trichinella is not infective to fish, or amphibians. In
addition the genetic background of the host has an influence on the outcome of the infection. Mechanisms of innate immunity like mucus acts as a barrier.
2. Non-specific acquired immunity: a. Resistance acquired after a first contact with an unrelated infectious agent or an immunogenic
substance. i. Ie: since you want a Th1 response, you want to have had a previous Th1 response, so
that when you get infected with Trichinella your body is ready to mount a Th1 response. b. A first infection with Mycobacterium tuberculosis will prtect against trichinellosis. Acquired
immunity to Trichinella is of the Th1 type and Mycobacterium stimulates a Th1 type of immune response. Likewise, mice infected with Toxoplasma, which also stimulates a Th1 type immune response, are protected against Trichinella.
3. Specific Acquired Immunity: a. Resistance acquired after a first contact with the same infectious agent. In trichinellosis both the
Th1 and Th2 type of immunity are playing a role. b. Serum antibodies of the IgM, IgG and IgE isotypes are detected. IgA antibodies are detected in
the gut. c. T cells and ADCC are also playing a role.
Eosinophil induction, recruitment and products during Trichinella spiralis infection:
Eosinophils play a major role. Trichinella antigen will stimulate the DCs and the classical macrophage.
In the end, IL3, IL5 and GM-CSF is important. IL5 is extremely important to drain eosinophils in the site of infection.
With AAM (alternatively-activated macrophages), Ym1 and Arg1 are chemoattractants, and eotaxin and galaectin help the eosinophil to migrate in the site of infection.
If you have a lot of eosinophils, this is good, but also bad for the host due to tissue balance. You really need a balance.
Key point: eosinophils play a major role in the clearance of Trichinella.

12
See picture on next page.
Pathogenesis and Symptoms:
Pathogenesis is following the 3 stages of development. o Intestinal Stage:
Worms migrating in the intestinal epithelium cause traumatic damage to the tissues. Inflammation causes nausea, vomiting, sweating and diarrhea.
o Migrating larvae: Juveniles damage blood vessels resulting in localized edema. They may cause
pneumonia, encephalitis eye damage, etc. o Muscle:
Formation of the nurse cell causes muscle pain, difficulty in breathing and swallowing. Presence of eosinophilia and edema in tissues.
NOTE: in the acute phase, you cannot do a muscle biopsy looking for larvae because it is too early. You can look for cysts later on. You must look for IgG, etc.
o 4 cardinal features of acute trichinellosis: fever, orbital oedema, myalgia and eosinophilia. o Nailbed haemorrhages are also a frequent sign of acute trichinellosis.
Diagnosis:
Subclinical cases go undetected. Adult worms cannot be detected in stool specimens.
Migrating juveniles cannot be detected.
Muscle nurse cell are detected by biopsy. o Muscle larvae are easily seen early in the muscle by crushing the tissue between micrscopic
slides. You can also use pepsin to digest muscle and look for the larvae.
Serology is not very sensitive as a method in the acute phase. PCR is useful in epidemiological studies.
Treatment:
Basically given to relieve the symptoms by using analgesics and immunosuppressive drugs like prednisone and cortocosteroids to reduce the inflammation.
o Keep in mind: immunosuppression no good for Toxoplasma.
There is no treatment to actually treat the infection.

13
Crocodylus porosus = the estuarine crocodile. T. papuae have been identified in 1/3 of villagers in the South-West corner of Papua New Guinea. The source for humans is the wild pig. T. zimbabwensis has been recorded in 40% of farmed Nile crocodiles (Crocodylus niloticus).

14
Ascaris and Larva Migrans- Dr. Ndao:
Both of these are nematodes as well.
Intestinal nematodes:
All nematodes that are parasitic in humans have: o Separate sexes (male smaller than female) o Egg production varies from species to species o Number of eggs vary from few (Strongyloides stercoralis) to >200,000 (Ascaris lumbricoides).
Life Cycle:
Five successive stages; 4 larval stages and the adult.
In most cases, the 3rd stage large is the infective stage
Eggs and larvae lining the intestine are passed outside in the feces or may be deposited on the preianal skin by the female worm.
Eggs are fully embryonated or require an extended periof of egg embryonation in the soil.
In some cases, eggs are infective when swallowed or will hatch in the soil and initiate infection by skin-larval penetration (eg: L3 Strongyloides can penetrate into the skin).
Ascarid parasites: Intestinal Parasites:
PARASITE HOST DISEASE
Ascaris lumbricoides Man Ascariasis
Ascaris suum Pig, man Ascariasis
Toxocara canis Dog Toxocariasis
Toxocaris catis Cat Toxocariasis
A. suum can infect humans but is not pathogenic. The ones that infect dogs and cats can also actually infect humans.
Development of ascarids:
4 larval stages (L1-L4)
Larval morphology resembles adult worms
Transition from one laval stage to the next requires shedding of surface cuticle (molting)
Most species undergo 4 molts
Aside: in eggs, there is a lipid layer that is very tough and sticky
Ascaris Life Cycle:
If you swallow an unfertilized egg, you will not be infected. Once you ingest a fertilized egg, this is where the life cycle starts. These eggs will hatch in the intestine and will migrate to the lungs.
They will then go to the heart and through the portal vein, go back to the lungs, and then to the intestine.
The adult will remain in the intestine.
There will be mating between the females and the males and eggs will be produced.
Between the ingestion of an egg, development of adults, and the release of the eggs, this takes up to 3 months.
Clinical Features:
Lung phase: 5-6 days after exposure o Pneumonitis (Loeffler‟s pneumonia) due to penetration of lung capillaries by juvenile parasite
causing hemmorhage

15
Intestinal phase: 2-3 months after infection o Abdominal pain, diarrhea o Malapsorption of nutrients o Stunted growth, cognitive impairment o Intestinal obstruction by high worm numbers
Wandering worms: cause pathogenesis; this is what is really bad, and causes children to die. o Intestinal perforation: peritonitis o Blockage of bile ducts o Obstruction of respiratory tract o Liver abscess
Aside: we have ascaris here; it is not just a tropical disease.
Epidemiology of Ascaris:
>1.3 billion people infected
Prevalent in tropical countries and socio-economically depressed areas of Europe, Latin America, Asia o 73% of all infections in Asia o In some areas, 100% of people are infected
Transmission by ingestion of contaminated food, water/soil o Using human feces are fertilizer contaminated vegetables
High infection rates in children o 3.2% of children in the Soviet Union had eggs in nasal mucus o In S.E USA, 20-60% of children infected
Intensity of infection peaks in 5-15 year olds
Eggs are incredibly resistant to chemicals: o Example: resistant to 2% formalin and 50% HCl, Nitric/Sulfuric Acid
Due to the lipid layer of the eggshell
Eggs are thus long-lived in the soil- up to 15 years o Eggs are sticky o Eggs found on German bank notes (1949) o Eggs can be transmitted by windborne dust
In China (1947), it was estimated that 18,000 tons of eggs were excreted by humans!
1014
eggs/day worldwide more than 10 trillion (female ascaris can excrete more than 200,000
eggs per day)
Diagnosis and Chemotherapy:
Eggs in feces o Female produced 200,000 eggs per day o Finding eggs is simple o Female produced 60,000,000 more more during her life span
Chemotherapy using Benzimidazoles (eg: Mebendazole) or Ivermectin
Benzimidazoles bind to tubulin and block muscle action
Being on the drugs increase both weight gain and apetite
Immune Response:
You would expect this to be a Th2 response.
They did a study in Equador looking at the responses, using uninfected and infected individuals. o The infected individuals had higher responses to larval antigen (expected) o Increased frequency of IL4 and IL5 producing peripheral blood mononuclear cells in infected
subjects. There was less IL10 and IFN-gamma in the infected.
Ratios of frequency of PBMC producing Th1/Th2 cytokines:
GROUP IL4/IFN-GAMMA RATIO IL5/IFN-GAMMA RATIO
Uninfected 0.7 0.6
Infected 7.6 (p<0.001) 9.6 (p<0.001)

16
Therefore infection increases the ratio of cells producing Th2 to Th1 cytokines
Conclusions:
In human Ascaris infection: o See increased frequency of PBMC producint Ag-specific IL4 and IL5 o No effect on frequency of PBMC producing IL10 or IFN-gamma o Higher ratio of Th2/Th1 PBMCs o No effect on IGN-gamma levels o Th2 cytokine secretion among individual with significant exposure to A. lumbricoides might have
an impact on the susceptibility to pulmonary infections with M. tuberculosis. L3/L4 are lung-stage parasites
In children, what causes pathogenicity is malnutrition and obstruction.
ALSO, Ascaris infections decrease the amount of IgE (while increasing Eosinophils), especially anti-Ascarid IgE.
Aside: worms secrete eggs, which eventually make it to the trachea, which are swallowed again.
Visceral Larva Migrans:
Baylisascaris procyonis o Found in raccoons (Procyon lotor) and causes serious disease in humans (North America) o Larva invade the eyes (Ocular larva migrans), spinal cord and brain (neural larva migrans) and
in the intestine (VLM) o No effective treatment.
Gnathostoma spinigerum o Found in dogs and cats. Endemic in China, the Philippines o Humans infected by the ingestion of raw or poorly cooked or pickled freshwater fish, chicken,
birds, frogs or snakes. o Larva migration including pulmonary, GI, urogenital, ocular, otohinolaryngeal and cerebral
tissues
Strongyloides stercoralis o Very bad parasite, can sit in the host for up to 3 decades o Once you get any corticoid therapy that stimulates the larvae, they will invade the host and
destroy the organs
Toxocariasis: visceral larval migrans (VLM):
Caused by infection of humans with ascarids of dogs (T. canis) or cats (T. catis)
Transmission by ingestion of embryonated Toxocara eggs in food or in soil o Eggs are long-lived, like Ascaris
If the larvae do not develop to the adult stage: o They wander through the body o Migrate to soft tissues (liver, brain) or eye o Can cause blindness
Toxocara life cycle:
A dog less than 5 weeks or more than 5 weeks have different cycles.
In the left cycle, there is no developmental arrest. You can find eggs and larvae in the stool of puppies that are infected.
In the adult dog, there is arrest of development. Pregnant dogs can reactivate the arrested larvae (think: toxoplasma). Also like toxoplasma, the larvae can cross the placenta and infect the baby.

17
What causes pathogenesis is really the wandering of the larvae.
Clinical Features:
Systemic VLM: o Due to invasion of soft tissues by wandering larvae o Pathogenesis includes
Hepatomegaly Pulmonary and neurological symptoms Eosinophilia (high levels)
Ocular Toxocariasis: o Due to invasion of the eye tissues by the larvae o Juveniles cause chronic inflammation and granulomas of the retina (may cause blindness)
Epidemiology:
Worldwide parasite, including North America o Highest incidence in children
Infected dogs/cats increase risk of infection o in USA:
20% of all adult dogs infected 98% of all puppies infected ie: risk of exposure is high
o in Halifax: 26% of dogs, 25% of cats, 56% of puppies
Seroprevalence in children: o Up to 7.3% in USA. o 34% in Ireland o 50-80% in developing tropical countries
Diagnosis and Chemotherapy:
Fecal egg counts
ELISA using ES antigens
High eosinophilia is suggestive
Treated with Mebendazole
Regular de-worming of dogs and cats is essential!
Dispose of feces
Clean up after your dog
Aside: nodules are indicative of toxocariasis (eg: in the liver). Most pediatricians do not think about Toxocariasis when they see these liver nodules. But since many of the main symptoms of Toxocariasis are nonspecific or nonexistent, identification of hepatic nodules is important.
Now, physicians in the US are using parasites to modulate Th1 diseases (eg: Crohn‟s or IBD). One such parasite is Trichuris suis. It is not toxic to humans. Since people tend to develop Th2 responses when infected with parasites, this helps with disease.
Aside: ascaris worms can be about 20 cm in total. 1.4 billion people infected.
Filariasis- Dr. Ndao:
Filaria:

18
A roundworm
Adult filaria live in the body cavities, lymphatics, and subcutaneous tissues.
Embryos (microfilaria) live in the blood or dermis
All require an insect or a crustacean vector
Microfilaria are 150-350 micrometers long
Adults are 2 cm-12 cm (4-10 micrometers wide)
PARASITES GEOGRAPHIC DISTRIBUTION
VECTOR TYPE OF DISEASE
Blood: Wuchereria bancrofti Brugia malayi Brugia timori Lao lao Mansonella ozzardi Mansonella perstans
All tropics S.E Asia Timor, Indonesia African forest areas New world, Caribbean All tropics
Mosquito Mosquito Mosquito Deer fly Midge Midge
Lymphatic filariasis Lymphatic filariasis Lymphatic filariasis Eye worm
Skin: Onchocerca volvulus Mansonella streptocerca Dracunculus medinensis
Africa, Yemen, Central and South America Central Africa East and West Africa
Black fly Midge Cyclops
River blindness Guinea worm
You will never see adults in the blood, only embryos (microfilaria). Lao Lao is in Africa mostly, and Oncocherca was brought to the Americas by slaves.
Location of adult worms in vertebrate hosts:
Lymphatic group: o Wuchereria bancrofti (95% of lymphatic filariasis) o Brugia malayi o Brugia timori
Cutaneous group: o Loa loa o Onchocerca volvulus
Body cavity group: o Mansonella persistans o Mansonella ozzardi
Wuchereria bancrofti and Brugia malayi (Lymphatic filariasis, elephantiasis)
Lymphatic filariasis:
Wichereria bancrofti: o Males: 4-5 cm in length o Females: 6-10 cm in length o Microfilaria: ensheathed o Definitive host: human (no other natural reservoir) o Vector: mosquito (many species, eg: Anopheles, Aedes, Culex)
Brugia malayi: o Males: 1-2 cm long o Females: 8-10 cm long o Microfilaria: ensheathed o Definitive host: humans and monkeys o Vector: mosquitoe (many species, eg: Aedes and Culex)
120 million people infected, 90% = Bancroftian filariasis. 44 million develop pathology
Endemic to: Central Africa, Nile Delta, Turkey, India, SE Asia, East Indies, Philippines, Oceanic Islands Australia, South America.
Epidemiology:

19
120 million people infected o 90% Wuchereria o 10% Brugia
44 million develop pathology
Found in 80 countries
1.2 billion (20% of the world) at risk
Infections: o 33% in India o 33% in Africa o 33% in Asia/Pacific/Americas
When people are infected, there are parasites in the lymph.
Life Cycle:
When mosquitoes bite, they release the L3 larvae that develop, migrate to the lymphatic system where they turn into adults, females and males.
People can be asymptomatic but have microfilaria in peripheral blood for up to 10 years.
TPE = tropical pulmonary eosinophilia
If you are infected with W. bancrofti, and you come here and go to the doctor, be aware if they take blood in the daytime. Unless they put oxygen or something in the blood, they will see nothing. You can only ever see something at night. Some microfilariae are only released in the blood with medication. This is especially with W. bancrofti.
Clinical states of W. bancrofti:
1. Asymptomatic 2. Inflammatory
a. Lymphangitis i. Arms 25% ii. Legs 11%
b. Epididimitis, funiculitis 42% c. Filarial fevers d. Orchitis e. Filarial abscess
3. Obstructive (both social and psychological problems) a. Elephantiasis (main feature) b. Chyluria
i. Milky fluid due to presence of white lymph from a ruptured dilated lymphatic vessel in the excretory urinary tract (milky urine, containing chyle)
c. Hydrocele i. Collection of serious fluid in the cavity of the Tunica vaginalis testis ii. Caused by lymphatic dysfunction
d. Chylocele i. White lymph fluid in the cavity of the Tunica vaginalis testis, caused by rupture of dilated
lymph vessel e. Acute filarial lymphagitis (AFL): Caused by the death of the adult worm
4. Tripical pulmonary eosinophilia (TPE)
Progression of Clinical Pathology in Lymphatic filariasis:
INCUBATION PHASE FROM INFECTION TO APPEARANCE OF MICROFILARIA
LARGELY SYMPTOMLESS
Acute or inflammatory phase (skin is tight and red due to microfilariae
in the peripheral blood)
Females reach maturity release microfilaria
-Intense lymphatic inflammation, chills, fever and toxaemia
-Swollen lymph nodes, lymphadenitis, orchitis, hydrocele,
epidymitis

20
Obstructive phase Blockage of lymphatic ducts inflammation of lymph nodes and
wall
-Lymph node backs up and lymph passes into surrounding tissue -Followed by fibrosis, chyluria,
elephantiasis
Diagnosis:
Travel history is important to maximize the best type of specimen and optimal collection time for filarial infection
Direct examination (thick or thin smear) o Thin: you can see morphology o Thick: screening
Knotts concentration technique
Millipore filtration
Antigen capture o Coating a play with MoAbs o Better than looking for Abs (coating plate with Ag) because looking for Ag tells you about a
current infection, while looking for Abs looks for a past or chronic infection. HINT.
Presence of microfilariae: finger prick (blood smears), skin snips
Circulating filarial antigen (CFA) (Wuchereria) o IgG4 ELISA tropical eosinophilia syndrome
Antifilarial Abs (IgG and IgE)
IgG4 to recombinant antigen
Treatment:
Diethylcarbamazine (DEC) o Sensitizes microfilaria to phagocytosis o Optimal dose does not clear all the microfilaria and only a proportion of adult worms are killed o 70-80% reduction in reansmission using DEC*
Ivermectin o Acts by hyperpolarization of glutamate-sensitive channels. Glu-Cl receptors (specific to parasite
receptors) and chloride channel permeability. This paralyzes the worm. 90% reduction in transmission using Ivermectin Up to 99% reduction in transmission using DEC + Ivermectin best treatment
o Aside: used a lot in the North for helminth infections, but you need to go through Health Canada to use this drug. This is because it was made to be used on animals.
Albendazole (W. bancrofti) o It acts by inhibiting the polymerization of beta tubulin and microtubule formation o It binds to beta-tubulin, thus preventing microtubule polymerization. It is specific for parasite
tubulin. o Albendazole + Ivermectin is also a good drug combination (results in fever microfilaria than
albendazole + DEC)
Control:
Chemotherapeutic control has three main objectives: o Reduced mortality o Reduced transmission o Interrupt transmission (vector control)
Vector control is difficult
Avoidance from being bitten: o Mosquito nets, repellents, avoidance of habitats during peak biting times for the vector (rainy
season)
Global Program to Eliminate LF (WHO):
Objectives: o To eliminate transmission of infection

21
Single dose, two drug regimen o To alleviate and prevent suffering and diability
Secondary infections: since the immune system is pushed towards a Th2 response, secondary infections might not be properly targeted. Also, because of infection in the leg and the scrotum and breaking/stretching of skin, you are susceptible to bacterial infection.
Eliminating LF:
WHO, in collaboration with major pharma companies and over 35 organizations, launched an international elimination program (Global Alliance to Eliminate LF)
http://www.filariasis.org
The program relies on breaking transmission through yearly mass treatments of entire communities with the antihelmintic drugs Albendazole (GSK) in combination with Diethylcarbamazine or Ivermectin (Merck).
o A “good news” partnership
Effective Immunity: a balance between pro-inflammation and anti-inflammation:
Filarial molecules activate both pro-inflammatory and anti-inflammatory reactions.
Although promoting Th2-type responses, little allergic disease is found in areas where helminth infections are endemic
W. bancrofti study to identify blocking Abs in human sera: o Madras, India; endemic for W. bancrofti o MF group = no clinical disease but mf present in blood
Both groups had anti-filaria IgG o CP group = have chronic lymphatic pathology
Looked for blocking IgG in sera o Assay: blocking of histamine release from IgE sensitized basophils
Look for positive correlations with IgG isotypes Attempt to deplete blocking IgGs from human sera
o (Basically looking at the correlation between IgG and blocking Ab).
o It was found that blocking IgG levels were higher in asymptomatic MF patients
It was IgG1 and IgG4 that had the most significant differences between the groups
IgG1 higher in CP group (lower in MF), IgG4 higher in MF
o IgG4 levels correlate with blocking activity in MF serum
o Depletion of IgG4 leads to reduction in blocking activity in MF sera by 53-81%
Induction and Regulatory properties of IgG4 in human filariasis:
o The cells enter and secrete IgG4, and this will help becase the people will be asymptomatic but will have MF in the blood.
o In the case of high IgE and IgG1, they cause the death of MF and they release the endosymbiotic Wolbachia, which is bacteria that causes pathology.
Good news: drug treatment over the past 4 years has dramatically reduced prevalence of infection. o Moderate transmission rate from 47% to 1%. High transmission rate from 77% to 5%.
Aside: LF was targeted for elimination in 1997 when the World Health Assembly called on all endemic countries to “strengthen efforts towards eliminating” the disease. The global program to Eliminate Lymphatic Filariasis

22
(GPELF) was established in 1999 with the objective of interrupting transmission of the parasites in all endemic countries y 2020.
Loa Loa, “Loiasis”, “Eye Worm”, “Calabar Swellings”
Comared to Onchocerca, it is found only in the tropical forests of Africa.
Transmitted by a fly called Chrysops. Life cycle is the same with all filaria. They can live up to 70 years but this parasite can be found in the blood during the daytime (unlike W. bancrofti).
Common symptoms:
- Calabar swelling
- Can be observed in the eye (eye worm)
Onchocerca volvulus; “River Blindness”
The parasite, when in the blood, in the female form can release up to 2000 MF. When people are infected because they have nodules, it is very easy to diagnose. The fly transmits the disease (Simulium). It is also endemic in South America; it was thought to be brought there by slaves.
Cutaneous filariasis:
Onchocerca volvulus (Onchocerciasis) o 30 million infected, 120 million people live
in endemic areas o 270,000 with blindness and 500,000 with
severe visual impairement
Loa loa
Mansonella streptocara
Clinical Signs of Disease:
Skin Lesions o Edema o Pruritus o Papules o Scab-like eruptions o Altered pigmentation o Lichenification: skin is very tense
Skin nodules (containing thousands of MF)

23
Eye lesions o Punctate keratitis o Pannus formation: when people become blind; slow progressive degenerative disease of the
cornea o Corneal fibrosis o Glaucoma o Optic Atropy
There is also hanging groin and scrotal elephantiasis
Dermatitis can also lead to secondary bacterial infection (due to itching) followed by thickening, discoloration and cracking of the skin (lichenification)
Pathology:
Associated with a long-standing host inflammatory response to proteins from live, dead and/or dying MF o When parasites die they release proteins that cause disease
Inflammatory responses mediated by eosinophils
When O. volvulus invades the cornea, it causes inflammation of the sclera, cornea, iris and retina
Fibrosis leads to blindness 7-9 years later
Difference between this parasite and Lao Lao is that while in Lao Lao you can see the parasite in the eye, here you can see snowflake-like opacities and sometimes the parasite forming inside.
Burkino Faso: about 46% of infected men and 35% of infected women went blind due to onchocerciasis.
Chad: Highest number of blind in the world due to onchocerciasis.
Diagnosis:
Microfilaria; skin snip (using oculoscleral forceps) o If negative, the Mazzotti test is used: DEC patch = itching
Detection of filarial antigen
Detection of anti-filarial Abs (O. volvulus IgG4)
Complete blood cell count- eosinophilia
Treatment:
Nodulectomy
Chemotherapy: o Diethylcarbamazine is more toxic (therefore it is important to differentiate between Lao Lao and
Onchocerca) o Ivermectin:
Well-tolerated, action on microfilariae, reduces recundity in adult, female worms
African Perspective:
Onchocerciasis control program (OCP) = 1974
Aerial application of insecticide
Ivermectin
African program for Onchocerciasis control (APOC) – 1995
Effective and self-sustaining community directed treatment (CDTI)
American Perspective:
93% of infections in Mexico, Guatemala and Venezuela
6% of infections in Ecuador, Brazil, Colombia
Strategy favours elimination
Simulium are inefficient vectors
Ivermectin can interrupt transmission
The Onchocerciasis Elimination Program for the Americas (OEPA) – 1992

24
Strongyloides and Echinococcus- Dr. Ndao:
See attached notes (and maybe skim ppts).
Cryptosporidiosis- Dr. Ndao:
Water-borne disease; people are infected with oocysts. The oocysts have 4 sporozoites that are released. When people are infected, therefore, they can be infected for life (especially those with HIV or immune suppression). There is only one compound approved by the FDA, and it is very controversial.
Species names of Cryptosporidium:
C. parvum: humans, cattle, sheep, goat
C. hominis: human, monkey
C. canis: dog, human
C. muris: mice, human and cattle
C. meleagrides: turkey, human
C. baleily: chicken
C. nasorum: fish
C. serpentis: snake
There is no definitive host (not host specific). The disease causes diarrhea.
OOCYSTS SHED BY: INFECTIVE TO:
Cattle Cattle, cats, goats, sheep, rats, humans, dogs, pigs, rabbits and mice
Cryptosporidiosis:
Zoonotic (and anthropozonotic- human to human transmission) o Therefore it is difficult to eradicate
Various species cause illness in humans
Causes diarrheal outbreaks
Most at risk: children and the immunosuppressed as well as the elderly
It is a major threat to the quality of surface water and the environment. Farm animals can release the oocysts into the environment. People say that the disease is also food-borne; fruits and vegetables can be contaminated and can infect people.
C. parvum control: HINT
Oocysts are viable in: o Potassium dichromate* o Chloroform o Ether o Ammonia o Sodium hydroxide o Buffered hypochlorite o Potassium permanganate
Oocysts are killed by: o Freezing o Boiling for 30 minutes
o Hydrogen peroxide o Ozone (limits: Kitchener-Waterloo outbreak) o Oo-cide (Ammonia + sodium hydroxide + biocide)

25
All research for this is done with oocysts multiplied in the cow. They store the oocysts in potassium dichromate.
Epidemiological considerations:
Zoonose
Anthropozoonose
Arthropods
Manure used as fertilizer
Waterborne disease
Foodborne disease
Airborne disease (some airborne infections have been reported)
Life Cycle:
People ingest oocysts containing 4 sporozoites. They are released inside the intestine.
Excystation requires reducing conditions, pancreatic enzymes, bile salts- release of 4 sporozoites
Differentiation into spherical trophozoites- develop into Type 1 meronts (schizonts) that contains 6-8 merozoites (released)
o This is the first way to auto-infection (trophozoite merozoite trophozoite) and is hard to differentiate under the microscope.
Type 1 meronts invade nearby cells and develop into Type 2 meronts or into trophozoites to complete the asexual cycle.
Merozoites similar in morphology and function to the sporozoites.
Sexual stage: Type 2 meronts differentiate into male microgamonts or female microgamonts. Male microgamonts release microgametes that can fertilize microgametes inside the female microgamonts.
Generation of two types of oocysts o Thin-walled autoinfectious oocysts (10-20%) o Thick-walled oocysts (80%) shed in stool (released)
Aside: the best way to kill C. parvum in water is important (HINT).
Morphology:
Oocysts are 4-6 micrometers wide.
Composed of tough environmentally-resistant wall enclosing 4 sporozoites (HINT: differentiate this from Toxoplasma)- resistant to disinfections
o The oocyst wall is unique with a suture at the end. The suture dissolves during excystation, opeining the wall to 4 sporozoites.
Opportunistic and intracellular
Infects gastrointestinal and respiratory epithelial cells o There is colonization of the villi of the small intestine
Taxonomy:
Cryptosporidium is classified in the phylum Apicomplexa (apical complex has polar rings, micronemes and subpellicular microtubules). All parasites in this group are referred to as coccidia.
The species of coccidia developing in the GI tract of vertebrates include Eimeria, Isospora, Cyclospora and Cryptosporidium.
Those developing extra-intestinally include Neospora, Sarcocystis and Toxoplasma.
Organelles:
Sporozoites and merozoites appear similar to those of other coccidia with the same organelles. o Organelles like: rhoptries, micronemes, electron dense granules, nucleus and ribosomes.
They do not have polar rings, mitochondria and micropores.
Apical organelles of C. parvum and their functions in invasion.

26
o Micronemes: rod-like structures. Micronemal proteins are important in host cell localization, gliding motility and ligand-receptor attachment to host cells. Several classes of proteins are associated with micronemes:
GP900, TRAP-C1, CpSCRP and ABD reactive protein. o Rhoptries: club-shaped membrane-bound organelles. C. parvum have a single rhoptry. Rhoptry
proteins are involved in transforming the host-cell membrane into a parasitophorous vacuole membrane.
o Dense granules: involved in host cell modification following invasion. DG proteins are released from the parasite surface into the PV.
o Micronemes might secrete their proteins through the rhoptry duct.
Transmission:
The transmission is transmitted by the fecal-oral route via the oocyst stage.
C. parvum is a zoonosis lacking host specificity.
Transmission increases with: o Person-to-person contacts o Person-to-animal contacts o Drinking contaminated water
Factors contributing to the spreading of Cryptosporidiosis: o Contamination of the environment
Urban and agricultural effluents Farm and domestic animals, and wildfire
o Immunological status of the host Other infectious agents Ageing of the population Immunosuppressive drugs Stress
o Style of living Day care centres Contact with animals
Groups at risk: o Workers, veterinarians, farmers, medical personnel, day care centres o Immunodeficient people: congenital, acquired, infectious or drugs, malnutrition o Social factors: family, sexual activities, children (day care), pet owners, travelers, drinking non-
filtered water If you are travelling in an endemic area and do not have bottled water, you must filter
your water with a filter smaller than 4 micrometers.
Analysis of water samples for the prevalence of oocysts: o At least 50 litres of water must be filteres (1 micrometer porosity) o Wash the filter with water o Centrifugation o Staining o Microscope o Efficacy about 6.3%
Note: it is not just in endemic areas (tropics) where outbreaks occur. Eg: Canadian outbreak, source = municipal water. Pools are also implicated in waterborne outbreaks.
The 1993 Wilwaukee Outbreak was the biggest outbreak. o From March 23rd to April 9th
100x increase in C. parvum oocysts found in the water treatment plant 403,000 residents contracted the disease Diarrhea, fever, abdominal cramps and vomiting were the main symptoms Over 54 deaths from the high risk group This was very bad for the economy, as people could not go to work.
Total cost of this outbreak = $96,244,000 o C. parvum was classified as a bioterrorism organism class B o One oocyst is enough to infect people.

27
Review of the life cycle. See lecture recording to fill it in. Aside: the thin infects the host. Otherwise the merozoite becomes the trophozoite and the life cycle is kept at that stage.
The parasite has a tropism for the ileum and the jejunum.
How do Cryptosporiduum species interact with the host?
Initial interaction via receptors o CSL o CP47
Attach by anterior pole o Invagination o Microfilament-dependent
Causes damage to apical surface of the cell
C. parvum, compared to other species that cause diarrhea, do not go deep. They stay at the epical surface of the cells. This is opposite to giardia and amobiasis (which can also cause perforations).
Pathology:
HOST TISSUES
Birds Respiratory tract
Fish and Reptiles Intestinal tract
Mammals: a) Immunocompetent
b) Immunodeficient
Intestinal tract
Pancreas, liver, respiratory tract, gall and urinary
bladders
Organisms can have the parasite everywhere. Immunodeficient people will have this for life. There is no good treatment.
Mechanisms have been advanced to explain the pathogenesis of diarrhea induced by Crypto
In patients having large volume of diarrhea (70 bowel movements per day) secretory processes of the parasites or immune cells appear to play an important role.

28
o Metabolites secreted by Cryptosporidium o Inhibition of glucose-stimulation affecting Na-absorption o Increased production of mucosal prostaglandin which can inhibit NaCl absorption leading to
secretory diarrhea Prostaglandin will inhibit NaCl absorption, causing the watery diarrhea.
o Leukocytes can produce high levels of prostaglandins o Alterations in intestinal permeability due to the immune response to the parasite.
ie: Increased secretions of cytokines like IFN-gamma and transforming growth factor (TGF)
What causes diarrhea? o Absorption is impaired
Electroneutral (NaCl) Electrogenic (co-transport)
o Secretion is enhanced Active Cl- or HCO3-
Basically the Cl moving out and the stopping of Na moving in o Causes:
Toxins, pathogenadherence/invasion, stimulate immune response
How to Crypto cause diarrhea? o Inflammation
Prostaglandin is related to inflammation and also secretion of TNFalpha
o Increase in intracellular permeability o Inflammation in submucosal layer o Profuse watery diarrhea
Diarrhea is osmotic o Damage to epithelial cells:
Villus blunting and atrophy hyperplasia
Immune Response:
Crypto resides at the apical surface of intestinal epithelial cells and does not invade deeper layers of the human GI mucosa
Nevertheless, moderate to severe infections stimulate both innate and acquired immunity
There is mucosal inflammation with the presence of macrophages and neutrophils at the site of infection.
In other words, there is a classic immune response to infectious agents o Both innate and acquired immunity can help the patient
Innate: macrophages and neutrophils can invade the site of infection
There is controversy regarding DCs. People think that it is mainly the macrophages and the neutrophils that are the main components
Innate immunity: o Mediated by immune cells present at the epitheial and sub-epithelial levels.
Cytokines: cells express the pro-inflammatory IL-8. It is also a neutrophil attractant Prostaglandin: produced by epithelial cells, may serve to influence their biological
function Nitric oxide: major component of the innate immune response, produced from argenine
by the enzyme nitric oxide synthase (NOS)
This NO is what can really harm the parasite.
Adaptive immunity: o T lymphocytes o Helper T cells
Both of the T cells are importing (helper T and Th1) because people can have lots of Abs against C. parvum but still get infected.
o Th1, Th2 o B cells o Ab responses
Acquired immunity:

29
o The role of acquired immunity in resistant to, and clearance to, Crypto infection has been studied in mouse models in which B and T cell populations were depleted.
o B cells: Patients develop both serum and secretory Abs but these specific Abs are not
successful in eliminating infection.
Humoral Abs: o In the mouse model, B-cell deficient neonatal mice can clear the infection, indicating that the
role of Abs is minor in the control of infection. o Humoral immunity is not an absolute requirement for clearing the infection. It plays a secondary
role in combination with other host factors.
Cell-mediated immunity: o The clearance of the infection in humans correlates with the CD4 T-cell population, not the
CD8 T cells. o Likely, athymic mice and SCID mice are not able to eliminate the infection. o The relation existing between CD4 T cell populations and Crypto explains why AIDS patients
are seriously affected by Crypto infection.
Th1-Th2 Response:
Th1 Th2
IFN: - Prevent initiation and limit infection - Expression = recovery TNFalpha: - Upregulation during infection - Redundant role? IL12: - Remains controversial IL18: - Important for clearing - Th1/Th2 balance
Role of this response is less clear. IL4: - Depletion = longer shedding
Strong early Th1 response, late Th2 may help clearing.
Diagnostic tools:
Microscopy: o Acid fast stain o Fluorescent
Endoscopic biopsy
Immunodiagnosis o Immunofluorescence assay (NOT confirmatory of active infection) o ELISA (NOT confirmatory of active infection)
PCR-based assays: o RT-PCR to quantify oocysts in stool o PCR- standard and multiplex o Loop-mediated isothermal DNA amplification (colorimetric) o Oligometric gold nanoparticle networks
Usually those invected with C. parvum can now use a fast assay called “lateral flow” that can detect the infection in 30 minutes.
Treatment Options:
Self-limiting infection
Unless immunosupressed o Treatments are most important

30
There are no good treatments for C. parvum. o Chronic diarrhea can lead to malabsorption of antiretroviral drugs in HIV patients
Taking Imodium reduces motility. They also need to be rehydrated (eg: with fruit) to compensate for the loss of water.
Treatments: o Anti-motility agents
Imodium o Rehydration therapy
Glutamine-based better than glucose o Drugs
Drug of choice: o Nitazoxanide (only one approved by the FDA but still controversial in the field, due to mixed
results. This is not a good enough drug!) Broad spectrum
Parasites, bacteria and viruses How it works:
Inhibits pyruvate:ferredoxin/flavodoxin oxidoreductases (PFOR) required for anaerobic respiration
Important for parasites without mitochondria
Treatment of HIV-infected patients: o Outcome is inversely related to CD4+ T cell count o Nitazoxanide (FDA approved) + HIV cocktail o Protease-inhibitor-based regiments
Correlated to increase survival o Nucleoside inhibitors
Some increased survival o Parmomycin:
Aminoglycoside (inhibits protein synthesis) Partial efficacy in AIDS patients (20-25%)
May relieve some diarrhea
Allows absorption of antiretroviral drugs) o Rifamycin derivatives:
Blocks DNA-dependent RNA synthesis Least active (used because in the field, we are desperate) Can be used for prophylaxis, or in combination with other antiparasitic drugs
o Drugs often result in clearance but not cure o When CD4+ T cell counts decrease, infection reappears o Need for new drugs
Small molecules preventing surface receptor binding o Prevention is critical
Taenia Solium- Dr. Ndao:
Class: cestoidea- Tapeworm. This disease is endemic in all countries in the world where they raise pigs. When humans defecate outside, the pigs eat human feces, and this is now they get infected. This can be up to 8 meters. Also, with this worm the adult is in the human. In other hydatid diseases, the humans get infected by the oocysts.
Epidemiology:
Cysticercosis is primarily a rural disease
Several factors have been identified in Mexico, Central and South America explaining its high incidence. o Poor sanitation, lack of latrines, inadequate fecal disposal facilitates egg ingestion and
cysticercosis. o Dietary habits, inadequate boiling of pork products containing cysticerci/larvae leads to taeniasis o Open air fecalism in rural areas- pigs consume human feces and over time build up a heavy
load of cysticerci

31
o Pigs deliberately placed in courtyards to clean up human feces- same result as open-air fecalism
The worms can release eggs (thick, can survive for months) or parts of the worm in the feces. This parasite can also spread with contact from human to human.
It is hard to diagnose by looking at the stool of humans. Most people are diagnosed by MRI X-ray. This disease was therefore under-reported until 1990, when people got access to X-Rays and CT scans.
Prevalence:
Prevalence of T. solium infection in South and Central America, and sub-saharan Africa and Asia are infected
It is also prevalent in some Eastern countries in Europe
Pork Tapeworm:
Scolex, neck and proglottid (has eggs)
Remember, hydatid can release up to 1000 eggs
T. solium causes neurocysticercosis mainly. When people have the disease, they can release gravid proglottids, which have have up to 50,000 eggs inside. These proglottids have male and female inside.
This is opposite to others; this is very short. The hydatid is localized mainly in the liver and the lungs. The form that we have up North is mainly in the lungs.
This worm invades the GI tract and forms a cyst in the muscles. Based on the life cycle, if you do not eat pork, you can still get infected from soil.
o It was demonstrated in New York that Jewish Orhtodox people got infected (they never eat pork)
Here, the adult and the larvae is in the host (definitive host = human). But for the hydatid, the definitive hosts are dogs.
Adult worm:
The proglottids come from under the scolex
The scolex is ~1 mm, with suckers and 2 rows of hooklets
New proglottids arise from the base of the scolex
Cestode Tegument: EM section:
Cestodes lack GI tracts
Adults live in small intestine
Tegument metabolically active, impermeable to peptides, proteins and macromolecules but it acquires nutrients by active transport, pinocytosis and diffusion. Tegument is very compact.
Tegument microtriches/villi (~1 micrometer)- actively absorbs amino acids, sugars, vitamins and fatty acids (pinocytosis)
Taenia tegument performs three functions: o Absorptive o Excretory o Digestive
Contact digestion: carried by 2 sets of enzymes on villi: intrinsic, extrinsic
Ovum:
~Spherical, ~45 micrometers, brownish shell, contains onchosphere, egg is hardy, survives for months in moist soil

32
Ingestion of ova Cysticercosis
Hatched onchosphere/hexacanth embryo: ~30 micrometers in diameter; 6 hooks and a pair of secretory glands open laterally; both facilitate onchosphere mucosal invasion.
Aside: very difficult to differentiate the eggs between T. solium and E. granulosis.
Infection and Course of Infection:
3 modes of infection: o Egg ingestion: drinking water or consumption of raw vegetables. o Autoinfection: finger to mouth; due to poor personal hygiene o Reverse peristalsis of gut content: eggs and proglottids from the small intestine forced into
stomach- pepsin, pancreatic trypsin and bile salts facilitate egg hatching- can cause massive cysticercosis. Onchosphere anchors to intestinal mucosa, lyse enterocytes- enter blood vessels in lamina propria- enter portal circulation and peripheralize.
Aside: Strongyloides can also stay in the intestine for 2-3 decades, and can give autoinfection (L3 is autoinfective).
ALSO; pig feces does not infect humans. This is a difference between Echinococus and T. solium.
ASIDE: Which parasite can infect babies? Toxoplasmosis. Is it possible to diagnose Toxoplasmosis by looking at the feces of the patient? No. It must be diagnosed by looking at blood smears, looking for tachyzoites and bradyzoites. Bradyzoites form cysts, and are reactivated when women get pregnant.
Histogenesis of onchosphere:
Surrounding host tissue most likely to determine histogenic fate of the sequestered onchosphere:
o Cystic type of cysticercus develops in compact denser surroundings- muscle, sub-cutaneous tissues or brain parenchyma.
o Branched racemosus type cysticercus develops in open spaces- subarachnoid space or
ventricles of the brain.
Cysticercus larva:
Onchosphere differentiates into cystic form in dense tissues.
Oval; 1 x 0.5 cm; invaginated scolex, neck and bladder.
Cysticercus blocks host attack: Taeniastatin and polysulfated polysaccharides; black inflammatory cells binding and complement activation.
Intact tissue cysticeri induce mild inflammation- survives for years
Ruptured cyst release antigens, and induce intense tissue inflammation tissue lysis and edema; cause clinical symptoms particularly in NCC
SO, what really causes the problems are the larvae. If you have the worm in the GI tract of the patient, it is not a problem. But when the larvae start to circulate, this is bad. The larva can go into the brain. When the larvae circulate, the host tries to protect itself, and inflammation as well as complement activation can result. This will harm the host.
Parenchymal Cysticercosis:
Clinical systems dependent on the number of cysticerci, their brain location and their viability. o A few parenchymal cysts may cause partial/segmental localized paralysis- drugs can be used
(PZQ, albendazole+ corticosteroid) o Multiple parenchymal cysts compromise CSF circulation- increased intracranial pressure- NO
treatment recommended.
Racemosus type: ventricular/meningeal:
Onchospheres differentiate into racemosus forms into hollow locales- subarachnoid space or brain ventricles.

33
Racemosus type: 6-10 cm in size, lacks scolx, grows like a bunch of grapes: cyst fluid highly inflammatory (very immunogenic when cysts rupture).
Incurable when located at the base of the brain.
Clinical Picture:
Non-CNS: sub-cutaneous, muscular, etc: asymptomatic to mildly symptomatic
CNS-involvement: benign to life-threatening outcome. o Depending on the position of the cysts, you might not be able to do anything. Most of the time
the patient dies.
Ventricular/meningeal racemosus cysticercosis: o Usually a severe course o Ruptured cyst-antigen release causes exaggerated inflammation and liquefication necrosis
in surrounding tissues: Meningitis, ventricular accumulation of CSF- cause intracranial hypertension
(hydrocephalus), seizure, blindness o Cysticercus at the base of the brain- is generally inoperable, with fatal consequences within
5 years. o Immunocytochemistry of the brain lesion shows localized inflammation around damaged cysts:
gamma-delta T cells, macrophages, eosinophils, neutrophils, NK cells and type 1 cytokines
Diagnosis:
Combination of neuro-imaging, serology or biopsy: o Computed tomography/magnetic resonance imaging:
Detects space-occupying lesions- cysticercosis included in the differential diagnosis along with tuberculoma, bacterial/fungal abscess/tumor metastasis/congenital cysts
o Western Blot: highly specific, a 10kDa recombinant cysticercus antigen is in use in developing countries to rule out other clinical conditions.
Most of the time CT or MRI are used. Western Blot used by Dr. Ndao and te CDC Atlanta. They use 5 different proteins (eg: thrombin-treated T. solium metacestode protein), and if one is reactive from the patient, then that patient has cysticercosis.
Summary:
Humans are the only definitive hosts of T. solium
Adult Taenia: small intestine, can live up to 25 years o Infection variably subclinial, rare diarrhea or weight loss (most people are asymptomatic) o Gravid segments found in feces/perianal area- signals infection
Ingestion of Taenia eggs by humans may lead to generalized or neurocysticercosis
T. solium Mexican strain- neurogenic (most people with seizures have the Mexican strain); Asian strain mostly sub-cutaneous cysticercosis
Diagnosis: biopsy, serology, brain-imaging or radiology
Treatment: Cysticidal drugs; Praziquantel and Albendazol- mainly used against parenchymal cysts; main draw back- vigorous inflammatory response in brain parenchyma
o Cortocoid is recommended to eliminate inflammation
The best thing would be to try to find a vaccine for pigs
Giardia- Dr. Ndao:
Development forms of food-borne protozoan parasites implicated in the establishment of infection:
PARASITE SPECIES INGESTED FORM ADHESIVE/INVASIVE FORM
MAIN CONTAMINATED SOURCE
T.cruzi Trypomastigote Trypomastigote Fruit juice
T. gondii Oocyst Sporozoite Soil/water

34
Cyst Meat
Cryptosporidium sp. Oocyst Sporozoite Water
E. histolytica Cyst Trophozoite Food/Water
G. intestinalis Cyst Trophozoite Water
Protozoan parasites and their interactions with the human intestinal mucosa:
AD = adhesive disk
AO = apical organelles
MJ = moving junction
PV = parasitophorous vacuole
IR = inflammatory response
LP = lamina propria
Some parasites reamin in the apical portion, like cryptosporidium. With Entamoeba, most people get diarrhea and dysentery when they get it. With dysentery diarrhea, there is blood in the stool. This parasite also goes to the liver (extra-intestinal parasite).
Biological features:
Giardia are eukaryotic organisms because they possess the hallmark organelles including nuclei, ribosomes, lysosomal vacuoles and multiple linear chromosomes.
Giardia intestinalis (aka G. lamblia or G. duodenalis):
An intestinal protozoan parasite of vertebrates and is a significant gllbal cause of endemic and epidemic diarrhea worldwide.
The most common enteropathogen worldwide and while not necessarily a fatal infectious agent in itself, Giardia plays a role in the millions of deaths occurring annually, especially in developing countries, due to diarrheal illness
Can affect several million people, and we have it here (not just in developing countries). Several outbreaks are in developing countries as well. The disease can kill especially for those who are HIV positive.
About 1/3 of people in developed countries have had giardiasis- affects about 2% of adults and 6-8% of children.
Most commonly diagnosed intestinal parasite in USA and in Canada, especially among travelers. Most cases are in the summer- better weather conditions.
o The best way to diagnose would be to look at the stool under a microscope. o Important: when people have diarrhea, stool analysis is always useful.
In the USA, about 20,000 cases/year but incidence is about 2 million. Can be fatal for individuals with compromised immune systems (HIV, transplant patients, young and elderly).
Worldwide prevalence of acute infection between 20-30%.
Russia, E. Europe, Turkey, SE Asia, Central America, Sub-Saharan Africa
History:
1681: Antony Van Leeuwenhoek found it in his own stool.
1859: Lambl is publishing for the first time a good illustration of the Giardia cell.
1888: Blanchard gives the species name lamblia.
1914: Some soldiers in WWI are diagnosed with the infection.

35
1921: Dobell suggests that Giardia should be considered as a pathogen.
1926: Miller reports that Giardia might be responsible for malabsorption in infected children.
1954: Rendtorff R.C. confirms that the presence of Giardia in infected patients is associated with diseases.
Biology and life cycle:
It is a flagellated protozoan
Inhabits the upper part of the small intestine
It has a direct life cycle
The cyst is the infective stage
They can survive in water at 4 degrees C for at least 3 months
About 10 cysts are sufficient to infect humans
Picture: this is the trophozoite, and remember that the parasite lives in the upper part of the small intestine. The cyst is the infective stage (the trophozoite cannot live long outside). The cysts can survive up to 3 months at 4 degrees. It was shown that 10 cysts are enough to infect humans. In the case of cryptosporidium, one is enough.
Cyst:
Resistant to chlorine.Viable for several months in surface water.
Not resistant to freezing. o Remember: some species (eg: Trichinella) are resistant to freezing for 2-3 decades in meat.
Simensions- 6 to 10 micrometers. Elliptically shaped.
The cyst wall is composed of fibrous components containing polymers of galactosamine and proteins.
Stomach acids induce the excystation process.
Biological features:
It is an ancient eukaryote! o Two nuclei (lack nucleoli) o Absence of functional mitochondria o Lack peroxisomes o Altered golgi apparatus o Dependent on anaerobic respiration
After ingestion of cyst, two trophozoites emerge in the duodenum and attach to the host‟s small intestinal mucosa.
They multiply by binary fission in the lumen of the intestine. They colonize the small bowel.
Some of the trophozoites encyst and are released with the fecal materials.
People believe that this might be an ancient eukaryote because it is lacking nucleoli and the mitochondria is not functional.
Remember in cryptosporidium, there are 4 sporozoites. In this case there are 2 trophozoites that can emerge in the small intestine. They replicate by binary fission (like in the case of Toxoplasma). The cyst at the end is released with the fecal matter.
The trophozoites:
Four pairs of flagella originating from the basal bodies located near the nucleus.
Median body unique to the Giardia cell
Virus and bacteria are found in the cytoplasm (endosymbionts) same as Entamoeba
Ventral Disc:
Made of a complex of microtubules and fibrous structures and serves as organelles of attachment

36
The structure is rich in tbulin, term giardin.
Species of Giardia:
G. duodenalis/lamblia/intestinalis Human
G. muris Rodent
G. agilis Amphibian
G. ardae Great blue heron
G. microti Voles
Animal Models:
Mice and its natural parasites Giardia muris have been used to study the biology, acquired immunity, etc in the laboratory. Can grow trophozoites in culture very easily.
The gerbil G. lamblia model has been used to study the epidemiology and pathology of the disease
G. lamblia has been reported to be nfective to adult mice o Best to use G. muris in mice to set up animal model
Mode of contamination:
Transmission: o Drinking contaminated water o Contaminated rivers, lakes, (run-off, floods). Was known as Beaver Fever. o Ingesting contaminated food o Person-to-person contact
Most provinces check their water ever 1-2 weeks.
Anthropoonosis: person-to-person spread
Giardia and the environment: o Besides humans, G. lamblia infects a wide range of mammals which act as a reservoir (eg:
cattle, sheep, beavers, muskrats, and rats)- important for transmission. Cysts can also be found in soil. An infected person can shed up to 1 billion cysts per day! Up to 10 billion trophozoites can be released per day as well. There have even been reports of people releasing 200 million cysts per day, which is bad for day cares.
So there are domestic (sheep, pigs, etc) animal cycles and sylvatic (moose, buffalo, etc) animal cycles, and then through surface water it goes into humans
Giardia contamination in Canadian water samples:
Giardia contamination in Canadian water samples
SAMPLES NUMBER ANALYZED POSITIVE SAMPLES
NUMBER %
Raw drinking water 1,173 245 20.9
Treated drinking water 423 77 18.2
Raw sewage 164 119 72.6
Total # 1,760 441 25.1
Even after treatment of water, it will still have some giardia, depending on the treastment. This is in Canada. No need to memorize all the numbers!
Clinical Symptoms:
Most people (90%) unaware- no symptoms
Symptoms appear at about 6-15 days and may last for 2-6 weeks o This is when the infection is very heavy
Loss of apetite and weight loss very common (50%)
Malabsorption and dehydration is a complication and can be serious in babies
Can be a problem in child-care setting, swimming pools, etc o Swimming pools are also a source for C. parvum

37
SYMPTOMS USA % (N = 324)
Diarrhea 96
Weakness 72
Weight loss 62
Abdominal pain 61
Nausea 60
Steatorrhea 57
Flatulence 35
Vomiting 29
Fever 17
Fever is mostly associated with Entamoeba.
Pathology:
The infection can be asymptomatic or the cause of a severe enteropathy with malapsorption o Pathology in the small bowel can be evaluated by measuring the villus to crypt ratio o During the acute phase of the infection:
Decrease of the height of the villi Increase in the height of the crypt
Giardiasis can be: acute and self-limiting or chronic o The reasons to explain these above variations are not known
Malapsorption is the characteristic of the pathology in giardiasis. This occurs dueing the acute phase of the infection and disappears after elimination of the trophozoite from the small intestine.
o This is the key point here. When people are infected, like any disease, people can have the acute phase and the intermediate phase (depending on the disease) followed by the chronic phase. Most of the protozoan parasites have an intermediate phase (Chagas disease does).
o When people have acute phase, this is when most of the time people go to the clinic because they feel sick. If the physician is not aware of certain diseases, they will check for some diseases and send you home.
Eg: people die of Dengue because it is thought to be influenza. This is fine if you have only Dengue, but if you also have hemorrhagic fever, you could die.
o Therefore it is important to help the physician out and tell them about travel history, etc.
There are three distinct phases in the life cycle:
1. A latent period a. When you feel nothing
2. An acute phase a. Symptomatic
3. An elimination phase a. This is in the case of
Giardia, because there are tons of trophozoites and cysts in the stool.
Giardia and immunity:
INNATE IMMUNITY ADAPTIVE IMMUNITY
1. Presence of mucus in the small intestine acts as a barrier for invasion of mucosal tissue.
2. Normal human milk can kill Giardia trophozoites.
1. Both the humoral and cell-mediated immune responses are playing a role.
2. A local inflammatory reaction develops in the small intestine mucosa (in the upper digestive tract, where
38
the giardia stays).
3. The number of plasma cells present in the crypt increases. They are producing mainly IgA antibodies,
which play a large role in clearing of the parasite.
Both IgM and IgA bearing cells are prominent.
The IgM plasma cells are prominent in the early phase of the infection.
The IgA plasma cells are prominent during the acute phase of the infection
Circulating Abs are found in the blood but are not useful for protection or for diagnosis
So when people are infected, the best way to diagnose is to use the stool, not using serum. A lot of biotech companies are developing tests that can diagnose within 15-30 minutes.
Diagnosis:
ELISA (not very helpful)
Stool examination for trophozoites and cysts (usually 3 samples)
PCR detection of different isolates
Treatment:
DRUG EFFICACY SIDE EFFECTS
Metronidazole (treatment of choice, also used for Entamoeba)
90% Nausea, vomiting, metallic taste, rashes, vertigo, urticaria
carcinogenis.
Tinidazole 90% Same side effects
Ornidazole 90% Same side effects
Quinacrine 90% Nausea, vomiting
Furazolidone 80% Nausea, vomiting
Paromomycin 55% Nephrotoxicity
Metronidazole: selectively binds to and damages DNA in anaerobic protozoa (Giardia, Ameba, Trichomonas vaginalis). Also highly active against anaerobic gram-negative bacteria (Bacteroides fragilis, C. difficile, H.
pylori). Also inhibits aldehyde dehydrogenase, which breaks down alcohol.
CDC Guidelines:
To prevent and control infection with the Giardia parasite, it is important to: o Practice good hygiene (especially in child-care facilities) o Avoid water (drinking or recreational) that may be contaminated (avoid unfiltered water)
Giardia is larger than Crypto, so you can use a filter. You can also boil water. o Avoid eating food that may be contaminated (especially when travelling) o Prevent contact and contamination with feces during sex
Entamoeba histolytica- Dr. Ndao:
Intestinal Protozoa (just know the ones we have discussed):
PATHOGENIC COMMENSAL (NON-PATHOGENIC)
Entamoeba histolytica Giarbid lamblia Balantidium coli
Dientamorba fragilis Cryptosporidium parvum Enterocytozoon bieneusi
Septata intestinalis Cyclospora cayetanensis
Entamoeba hartmani Entamoeba dispar
Entamoeba coli Endolimax nana
Iodamoeba butschlii Chilomastix mesnili
Trichomonas hominis Lastocystis hominis

39
Isospora belli
With E. dispar, you need to be aware that when you diagnose Entamoeba, it is impossible to differentiate beween E. dispar and E. histolytica. Before, provincial labs had to send all samples somewhere else, and now (because of PCR) they do not have to.
Amebiasis is caused by E. histolytica:
Leish, 1875 reported the first cause of amebiasis in a patient suffering from chronic dysentery
Councilman and Lafleur, 1891 describes the pathological and clinical aspects of amebic liver abscess.
There are 6 species of Entamoeba: o E. histolytica o E. coli o E. dispar o E. gingivalis o E. hartmanni o E. polecki
If you are lucky, you may see inclusion of red cells, and then this is E. histolytica and not E. dispar.
E. histolytica vs. E. dispar:
Brumpt 1949, proposed to establish a new species of Entamoeba to designate the amobae that are not pathogenic.
In 1993, it was decided that the invasive form will be called E. histolytica.
The non-invasive form was to be called E. dispar
These to ameobae can NOT be distinguished by microscopic observation
E. histolytica:
Worldwide distribution. Amebisis is the 3rd most common parasitic death in the world (70-100,000 deaths per year).
o When people are infected they could get it in the liver, leading to abscesses.
500 million people are infected
Can be waterborne
Found in regions of the world with poor sanitation
Mexico, Central and South America, Africa, South Asia o More endemic to developing countries due to poor sanitation
Modes of infection: o Water, food o Flies can act as passive vectors o Can be sexually transmitted o Person-to-person contacts
Epidemiology: o Humans are the only source (not a zoonosis) Leishmania is a zoonosis o Fecal-oral transmission o E. histolytica/dispar:
Developing countries is ~10% E. histolytica Developed countries is ~1% E. histolytica
AMOEBIASIS:
1. Asymptomatic carrier state (most people are asymptomatic) 2. Acute amoebic dysentery 3. Amorbic liver abscess 4. Amoboma
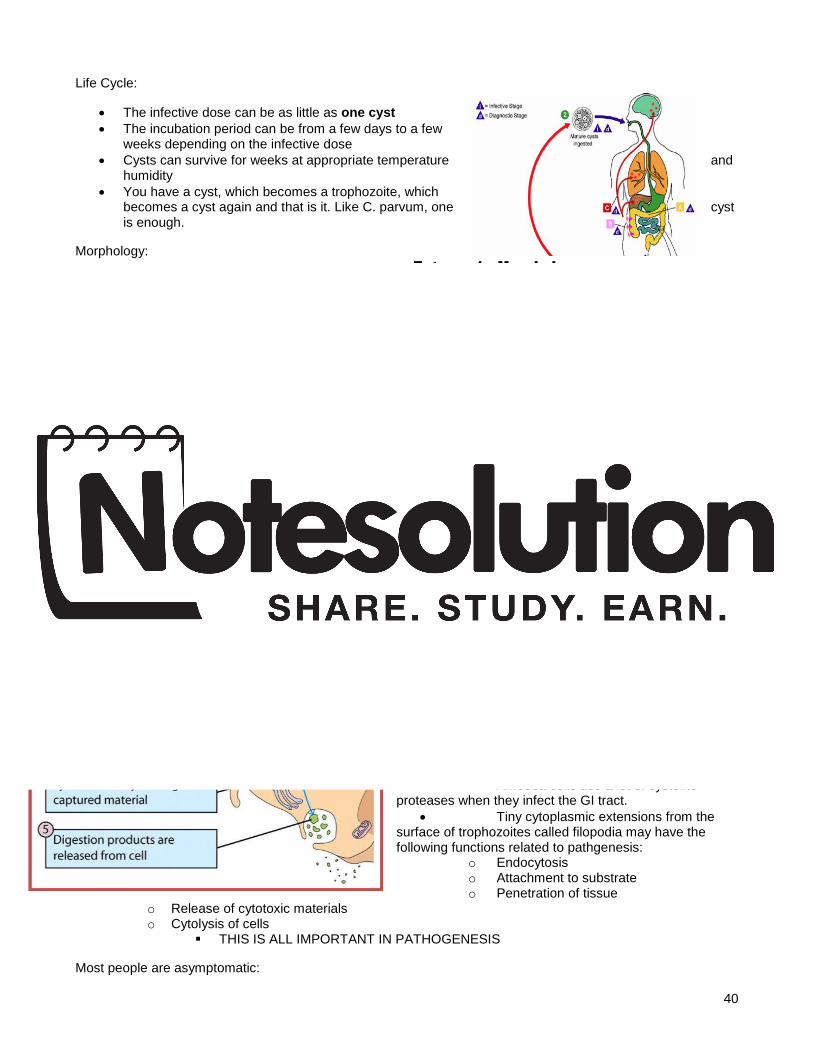
40
Life Cycle:
The infective dose can be as little as one cyst
The incubation period can be from a few days to a few weeks depending on the infective dose
Cysts can survive for weeks at appropriate temperature and humidity
You have a cyst, which becomes a trophozoite, which becomes a cyst again and that is it. Like C. parvum, one cyst is enough.
Morphology:
If you are lucky, you can see some ingested RBC.
Pseudopods help for movement
When cysts are formed, you might find 1-4 rings of nuclei inside
Cytoplasmic structures:
Nucleus: o Nuclear membrane contains
numerous pores. The inner surface membrane is lined with peripheral chromatin.
Endosome: o Located in the center of the nucleus.
Probably contains DNA
Vacuoles: o They occupy a great proportion of the cytoplasm. They vary between 5-9 micrometers in size. o They contain cellular debris, RBC, bacteria - feeding
Amoeba cells can live and multiply indefinitely within the crypts of the mucosa of the large intestine.
They are able to invade the mucous layer, which constitute a major non-specific defense immune mechanism
They feed on starches and mucous secretions and interacting metabolically with enteric bacteria
They initiate tissue invasion when they hydrolyze mucosal cells and absorb the pre-digested products. At this atage they no longer need to feed on bacteria.
Amoeba cells use a lot of cysteine proteases when they infect the GI tract.
Tiny cytoplasmic extensions from the surface of trophozoites called filopodia may have the following functions related to pathgenesis:
o Endocytosis o Attachment to substrate o Penetration of tissue
o Release of cytotoxic materials o Cytolysis of cells
THIS IS ALL IMPORTANT IN PATHOGENESIS
Most people are asymptomatic:

41
Presentation: o Diarrhea to dysentery with blood and mucous (diarrhea may or may not be bloody) o Fever (compared to Giardia, people can have fever) o Abdominal pain (since it goes to the liver)
Diagnosis: o Amoebic (hematophagous trophozoites and cysts) in stool o Patchy inflammation seen on colonoscopy o Serology- Abs in serum o Stool PCR- detection of parasite DNA in stool o Antigen capture- detection of parasite protein in stool (lateral flow- gives results in 15-30
minutes)
Pathology:
Intestine: o Remarkable and unique ability to hydrolyze host tissues with their active proteases present on
the surface membrane of the trophozoite. Protease contributes a lot to pathology
o Lesions are found in the carcum, appendix, or colon. They may heal. o If perforation of the colon occurs, there is a peritonitis that can lead to death. o Amoeboma = granuloma obstructing the bowel
Liver: o Hepatic amebiasis occurs when trophozoites enter the mesenteric veinule and travel to the liver
through the hepatic portal system. o Only about 5-10% of infections will affect the liver. Formation of abscesses will occur.
Symptoms of Ameobic colitis:
SYMPTOMS PERCENTAGE
Diarrhea 100%
Dysentery 99%
Abdominal pain 85%
Fever 68%
Dehydration 5%
Length of symptoms 2 to 4 weeks
Larger percentage of fever here than in Giardia.
Treatment:
Choice of antimicrobials: o Cholera:
Children Azithromycin, TMP/SMX, furazolidone, or Norfloxacin Adult Doxycycline 300 mg once, or tetracycline 500 mg daily x 3 days
o Bacterial dysentery: Children Ciprofloxacin 500 BID x 2 days, azithromycin, or ceftriaxone Adult Ciprofloxacin 15 mg/kg BID x 2 days, or azithromycin, or ceftriaxone 50-100
mg/kg daily i.m. for 2-5 days o Giardia:
Metronidazole, tinidazole, nitrazoxanide, or parmomycin o Amoeba:
Metronidazole or tinidazole, followed by iodoquinol or paromomycin
Mechanisms of cytotoxicity:
Several mechanisms have been advanced to explain the pathogenicity of virulent strains of Entamoeba.

42
o 1. Direct contacts with the host tissues: Example: adherence to the host cell by the release of adhesin molecules
o 2. Release of soluble toxic metabolites Example: Amoebapore are capable of forming a hole in a target cell
o 3. High enzymatic activities of the amoebas Example: enzymes released by the parasite damaging the host cell
o 4. Interfering with the immune response of the host Antigens released by the amoeba cell can lead to:
Inflammatory reaction
Allergies
Immunosuppression
Over-stimulation of cytokines
Formation of immune complexes
Formation of auto-Abs (very bad for the host)
Amoeebic killing:
The immune system can kill the amoebic cell: o 1. Macrophages activated by cytokines can kill Entamoeba trophozoites. The killing mechanism
is contact-dependent and is mediated by both oxygen and oxygen-dependent mechanisms. o 2. Cytotoxic T lymphocytes (CD8+) are active and their activities are dependent of released
lympho-cytotoxins since direct contacts of amoebas with cytotoxic lymphocytes are not always active.
o 3. Abs don‟t seem to play a major protective role This is the same with C. parvum
o 4. Ab-dependent cell-mediated cytotoxocity (ADCC) is not an active mechanism to kill the parasite.
o 5. Lysis of amoebas has not been observed with either immune serum alone or with complement. Threfore the Th2-type of immune response is not playing a major role against amorbiasis.
ENTERIC AMOEBAE OF HUMANS
TROPHOZOITE PSEUDOPODIA CYST NUCLEUS # OF NUCLEI
E. histolytica 25 microns 15-60 microns
Active
Finger-like 12 microns 10-20 microns Chromatid bar
Central endosome
1-4
E. coli 25 microns 15-40 microns
Sluggish
Short, blunt 17 microns 10-33 microns
Eccentric endosome
1-8
E. gingivalis 15 microns 5-35 microns
+/- Active
Blunt None Central endosome
?
Endolimax nana 10 microns 6-25 microns
Sluggish
Short, blunt 9 microns 5-14 microns
Large endosome
1-4
Iodamoeba butschlii
10 microns 6-25 microns
Sluggish
Short, blunt 10 microns 5-18 microns
Large endosome
1
Dientamoeba fragilis
10 microns 6-25 microns
Active
Thin None Central endosome
?
Just for our information.
Amebiasis of the skin:
This infection arises by direct spread of a primarr abscess

43
The patient could have been erroneously operated for a perforated duodenal ulcer and no anti-amorbic drugs were given- this is bad!
Prevention:
Wash hands! Good sanitary practices!
When travelling, do not eat raw vegetables
Boil water
Parasite Chemoterapy- Dr. Geary:
Infectious diseases:
*Encounter Filter o First goal: limit access of pathogen (vector) to host o Geographic isolation; bed nets; no swimming; filter water; DDT; wash hands
*Compatibility Filter o Immune response handles most parasite species o Physiological/biochemical barriers to establishment o Drugs and vaccines are add- on to compatibility filters
There are more parasites than any other kind of animals; the host restricts many kinds of parasites. There are 200 or so malaria species, and about 4 infect people. Why? Most hosts restrict most parasites; there is a counter filter. We do not intercept with the parasites, we do not come into contact with them. The other is that we prevent the encounter with the disease.
The compatibility filter is that, although we could be infected with some parasites, they do not take. There could be a receptor missing, a nutrient missing, or the innate immune system is good at killing it.
Drugs and vaccines do not prevent the infection per se, but they prevent the infection from being more successful.
Parasite chemotherapy:
Goals of chemotherapy for parasitoses: o 1. Prevention of symptomatic infection (prophylaxis)
Eg: with malaria, we really only have prophylactic drugs. It doe not prevent infection, it prevents success of infection.
o 2. Cure of established infection o 3. Reduction in pathology o 4. Prevention of transmission
Key concepts/terms: o Mechanism of action: drug receptors
Before you can talk about which drug helps for which parasite, you need to have a feel for the drug mechanism itself
How a drug works at a molecular level; drug may interact with protein, nucleic acid, membrane, etc to cause an effect.
Eg: a lot of anti-cancer drugs work at the level of DNA. Some of the action of drugs is called non-specific.
o Receptor: Protein target for the drug. A “receptor” is generally an enzyme, a protein that responds
to a neurotransmitter/hormone to cause a change in cellular function, an ion channel, or a structural protein.
o Agonist vs. Antagonist o Potency: IC50 vs. ED50: intrinsic vs. clinical potency
Intrinsic potency: in a perfect world, how potent is this drug against an animal? In drugs, concentrations are given as mass per unit volume. But doses are given as mass per unit mass.
When something is very potent, this means that it kills at a low dose o Efficacy: maximal possible response

44
o Selectivity: therapeutic index; selective toxicity It is easier to kill bacteria than parasites because parasites are eukaryotes Therapeutic index is the dose that is effective vs. the dose that is toxic. In bacteria, it is diagnosis-basis treatment. With parasites, it is mass treatment; they do
not diagnose. In this case, the drug must be very safe. If you are sick then you can tolerate a little risk to be cured. But if you are not sick and do not have the parasite, you get the pill anyways. So it must be really safe.
o Spectrum We are consumer-driven medical treament societies. We do not want to wait for
diagnosis, we want the pill now. You want one pill that kills every bacteria known to man. This is the same with parasites; we want treatments that can be administered without diagnosis at the species level.
o Resistance Whenever you put pressure on a population, you will develop resistance.
Drug receptors:
May be enzymes with specific inhibitors o Examples:
Dihydrofolate reductase (DHFR) is a key enzyme in purine synthesis. It is needed for the one-carbon transfer that converts dUMP to dTMP for DNA synthesis. Drugs that inhibit DHFR are useful in many chemotherapy applications. DHFR differs between mammals, bacteria and protozoa.
Trimethaprim targets this receptor. In malaria parasites, inhibitors of DHFR have helped, specifically Pyrimethaine. This drug is one of several that inhibits the function of DHFR.
May be ion channels gated by neurotransmitters: acetylcholine (ACh), glutamate, GABA o Regulate neuromuscular function in metazoan parasites o Agonists activate the receptor; antagonists block it o Many ion channels are ion-gated. Nicotinic acetylcholine receptor is the most common one.
This is a target for mant anti-parasitic drugs. They take advantage of small structural differences between other nicotinic receptors and ours, and cause paralysis.
o Also, in our bodies our GABA receptors are very important. Entirely dependent on the function of GABA receptors is drinking alcohol. The
pharmacology of these proteins is well understood. Nicotine is an agonist because it acts like acetylcholine. But there are also things that block the channels, antagonists. These are used in parasite treatment.
May be structural proteins: tubulin equilibrium is disrupted by benzimidazole antiparasitic agents. Microtubules form key cable networks in the cell for organelle movement, shape and division.
o Tubulin is a structural protein in the cell; alpha and beta subunits form dimers, which polymerize to form microtubules. Many drugs have been developed to affect the functions of microtubules. Some drugs prevent their depolymerization; they stabilize the network (eg: Tamoxifen; anti-breast cancer drug).
Benzimidazole is important in worm treatment, and they target tubulin.
May not be a traditional macromolecules (protein or nucleic acid): o Malaria parasites digest Hb to make room for their growth in erythrocytes. Left over is the heme
moiety, which is toxic to membranes and which the parasite sequesters in hemozoin crystals in the food vacuole. Chloroquine accumulates to high levels in the food vacuole and binds to hematin, keeping it in solution and toxic.
May be non-specific: poison the parasite before the host o Amphotericin forms ion channels in cell membranes. Has slightly higher affinity for membranes
containing ergosterol (fungi, kinetoplastids like Leishmania) than cholesterol (mammals). Amphotericin B is mainly used as an anti-fungal, typically for life-threatening systemic
fungal infections (not topical treatments). It punches holes. It is a dangerous drug but it can be given safely and it important in the
treatment of Leishmaniasis. o Some drugs are just poisonous. They are still important in some aspects of chemotherapy, only
less than they used to be.

45
Melarsoprol is used for malaria, but it contains arsenic. The parasite will be poisoned a little more than the host.
Suramin was a complex drug used to treat onchocerciasis since it killed the adult parasite. It killed 5% of people, and is no longer used.
Stibophen is used in Leishmaniasis still, but it is a poisonous metal (antimonial)
These drugs all affect the function of many proteins. Heavy metals act on –SH groups. Very low TI values.
Principles of Chemotherapy:
Key concepts: mechanism of action o *Lethal vs. static effects (more of an issue with antibiotics)
Tetracycline and related drugs are bacteriostatic Penicillin and related drugs are bacteriocidal
A pathogen is only successful in the host when it transmits, but essential to this is replication. When it infects a host from which it cannot be transmitted, this is a dead-end host. In parasite treatment, some drugs are lethal and some are static. Some for worms in the gut are paralytic. If worms cannot maintain their hold, they are swept out.
o *Immune effectors: Several antiparasitic drugs require a functional immune response for full efficacy; this is
akin to a „static‟ effect
Praziquantel and schistosomes
Stibophen and Leishmania o HIV complicates treatment of visceral Leishmaniasis
Some drugs require the immune system to wrok just like they do with bacteria. About 200 million people have schistosomiasis. We do not treat it on a case base: we go into a village and know that the incidence is 30% due to fecal smears, and we give Praziquantel to all the children. Its efficacy depends on the function of the immune system, so those who are immune=suppressed do not respond as well.
Co-infection with HIV is bad because the parasite tends to be more aggressive and the infection is worse.
The drug that we use to treat filariasis is Ivermectin. If we put the parasite in solution with Ivermectin, nothing much happens. But what it does is that it stops the parasite from secreting proteins that modulate the immune system.
Onchocerca volvulus, or the causative agent of elephantiais can survive in the host for a long time. The parasite makes it so that the host cannot see it. Ivermectin enables the host to see the parasite.
o *Paralysis vs. Poison: helminthes and arthropods Ivermectin: pharynx Classantel: ATP Levamisole: somatic muscle Consequences of drug exposure depend on worm location. When we look at helminthes and arthropods, arthropods are the vectors of some of the
parasites. Therefore they become important to control. These drugs are to treat helminths, and they are paralytics.
Ivermectin paraslyzes the helminth‟s ability to secrete proteins into the host. Ivermectin is good for everything except hookworm (N. America?). Ivermectin also paralyzes the pharyns from opening, so the parasite cannot eat or move.
Closantel paralyzes the function of mitochondria. It is not used in humans, but works well in parasitized animals.
Levimisole paralyzes filarials as well.
Efficacy is the maximal response obtainable with a drug.
Potency is an estimate of how much drug is needed to cause a given effect. o IC50 = the concentration of a drug required for 50% inhibition in vitro o EC50 = the plasma concentration required to obtain 50% of a maximum effect in vivo. o ED50 = the dose of a drug required for 50% efficacy (eg: a cure) in vivo
Dose-response curve:

46
„Response‟ can be in % or in absolute units. „Dose‟ is in mg/kg or similar unit. A similar cirve for studies done in culture is called a concentration-response curve and the X-axis has units of concentration (usually molarity)
Graph: the curve goes to 100% at a high dose, and around the middle is 50%. Response can be % cure or % reduction in log bacterial presence. We can also measure it in absolute measurements if we are looking at blood pressure, for example.
Spectrum: the range of infectious agents addressed by a drug. Broad spectrum drugs require less diagnostic investment and keep costs low.
o This is a common concept in bacterial chemotherapy. o Humans and animals often suffer polyparisitism: better to use a single drug than multiple drugs.
Incidence of polyparisitism is around 25% (~2 billion people) with worms. Most of the people have more than one species. So we want one drug that gets rid of everything.
o Compliance (how well the patient adheres to the treatment) is a key factor in efficacy and resistance.
If you only take enough medication to feel better, the ones that are still hanging around form the basis of the resistant population. This has been tested rarely, actually.
Resistance: loss of potency of a drug in a population of parasites as a result of selction of individuals with alleles that confer protection from toxic consequences. It is a heritable phenotype. Continued selection leads to greater resistance and possible loss of efficacy.
o Exposure of populations to any pressure selects tolerant or resistant individuals; this is inescapable.
o Alleles are versions of genes. We start with the assumption that alleles that cause resistance are rare. But since they have selective advantage, they dominate the population. It is inheritable because it is a change in the DNA. This is an un-escapable result of chemotherapy.
o Resistance is selection of existing very low abundance variants (many parasite populations have high mutation rates and effective population sizes: mutations in every gene occur in every generation).
Variant alleles may confer gain of function or loss of function phenotypes on the protein.
Alleles are not mutants. Some parasites (malarial, gut, etc) are in large numbers. Many genomes are exposed and they are not good at DNA replication. So variations in genes exist in every population for every gene.
A variant is rare in a population because individuals who have it are at a fitness deficit. In order for the allele to become fixed in a population, we usually have compensatory mutations that are ameliatory. Very common are non-specific mutations in biotransformative processes.
o Mechanisms of resistance: Target alteration:
Beta-tubulin, DHFR (may require compensatory mutations to become fixed in the population).
Biotransformative:
Inactivate the drug (or fail to activate it); block import or accelerate export (common in anti-parasitic drugs).
o Understanding resistance: monitor, alter regimen, respond with resistance-recersing strategies.
*Clinical pharmacology (the science of drug movement and concentration in the body): o Drugs must reach the site of infection in sufficient concentration for sufficient time to cause the
death or disablement of the parasite. o What governs the ability of a drug to do this?
ADME: Absorption, Distribution, Metabolism, Excretion
Cmax; t1/2; AUC, route of administration; bioavailability; P450; conjugation If you give a needle in an endemic area, you need to
worry about the reuse of said needles. If you give a pill, not much gets absorbed by the body in the end.
Pharmacokinetics: o What happens to a drug when it enters the body? o Drug elimination: urine or feces; unchanged or metabolized
(cytochrome P450l conjugation, lipophilicity is the key).
Bioavailability:

47
o Drugs administered i.v = 100% bioavailable o Injections via i.m. or s.c. route: slower, but usually 100% o Oral: rarely 100%, influenced by food, transit time, etc.
Drug Safety:
Selective toxicity: o Is the receptor present in the host and parasite?
Therapeutic index: o An absolute measure of safety; not concerned with receptors. o It is the degree of shift in a graph
Selective toxicity does not equal safety! Eg: in malaria, arteminisin must be used in combination only.
Origin and discovery of antiparasitic drugs: Paul Ehrlic = the father of parasite treatment. Salversan was the first antibiotic, for syphilis. Its active compound was arsenic.
Parasites were the first know infectious agents (fleas, lice, ticks; tapeworms, ascarids) and earliest targets for chemotherapy: mercury, sulphur, nicotine, etc.
Many drugs came from nature: quinine, artemisinin Many other are strictly synthetic: sulfas, levamisole, pyrimethamine, benzimidazoles Some are made by microbes: ivermectin, amphotericin Many are derivatives of natural products: chloroquine and other quinoline-containing antimalarials In the past 100 years, parasites were targets for drug discovery: colonication of Africa, WWII In the past 40 years, efforts to discovery drugs for human parasites diminished markedly Veterinary parasite drug discovery increased markedly In the past 10 years, interest in discovery of drugs for human parasites („neglected diseases‟) has
increased again: Gates, DNDi, OWH, TDR/WHO
48
HINTS AND INFORMATION FOR THE EXAM:
QUESTIONS:
1. Larva migrans can be caused by
a. Strongyloidis
b. Shistosoma
c. Trichinella
d. Toxocara
e. Bayliascaris
i. A,d,c
ii. A,b,d
iii. A,c,e
iv. A,d,e
2. In which of the following helminths the stichocytes are present?
a. Ascaris lumbricoides
b. T. saginata
c. T. solium
d. Fasciola hepatica
e. None of the above
3. In ascaris, the following clinical features are observed:
a. Migration of larva to the eye and epilepsy
b. Deposition of the eggs in the eye by migrating larval parasites
c. Two phases involving larval invasion through the skin and adult worm migration in the tissues
d. Three phases involving infection in the lung, infection in the intestine and parasites
wandering in the tissue
e. Two phases involving wandering worms that migrate out of the skin into the eye
4. Patients with strongyloidis and HTLV-1 co-infection when compared to HTLV-1 negative subjects with
strongyloidies have:
a. Increased IL5 responses
b. Reduced IL5 responses
c. Increased IFN gamma production
d. Increased TNF alpha production
e. Decreased numbers of regulatory T cells
[Nematode (round- subclasses = whip (trichuris), hook or thread), cystode (no GI tract, flat, have up to 2-20 m in size), trematode (most of the time are liver flukes, they usually go to the liver) or protozoan parasite]
Toxoplasma: prosozoan parasite
Schistosoma (liver fluke): trematode
Trichinella: nematode (smallest one)
Ascaris: nematode (round worm)
W. bancrofti/Brugia (LF): nematodes
Strongyloidis: nematode
Echinococcus: cystode (smallest one) no GI tract
Cryptosporidium parvum: protozoan parasite
Taeniasis: cystode (no GI tract)
Chagas (T. cruzi): protozoan parasite
Malaria: protozoan parasite
Leishmania: protozoan parasite

49
Giardiasis can be:
1. Transmitted by some wild animals
2. Water borne
3. Food borne
4. Person to person
5. All of the above
During the acute and chronic phase of toxoplasmisis, which components of the immune system is the major effectors:
1. DCs
2. NK cells
3. Macrophages
4. CD8+
5. None of the above
Nurse cells of trichinella larvae are found in:
1. Smooth muscles
2. Heart
3. CNS
4. Striated Muscles
5. CSF
In North America, Echinoccocosis is caused by:
1. Echinococcus granulosis genotype G5
2. E. vogeli
3. Granulosis genotype G8
4. E. Oligarthrus


















