TOXOPLASMOSE CONGÊNITA MANEJO CLÍNICO
41
TOXOPLASMOSE CONGÊNITA MANEJO CLÍNICO Liú Campello Porto – ESC/HRAS/HMIB www.paulomargotto.com.br 1
description
TOXOPLASMOSE CONGÊNITA MANEJO CLÍNICO. Incidência de Toxoplasmose Congênita no DF por 1000 nascidos vivods , Casos Notificados, de 1996 a 2001. 1996 – 41 not, 28 conf. 1997 – 77 not, 30 conf. 1998 – 86 not, 6 conf. 1999- 68 not, 24 conf. 2000- 68 not, 31 conf 2001 – 93 not,17 conf. - PowerPoint PPT Presentation
Transcript of TOXOPLASMOSE CONGÊNITA MANEJO CLÍNICO

TOXOPLASMOSE CONGÊNITAMANEJO CLÍNICO
Liú Campello Porto – ESC/HRAS/HMIB
www.paulomargotto.com.br 1

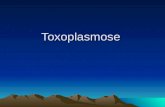
Incidência de Toxoplasmose Congênita no DF por 1000 nascidos vivods , Casos Notificados, de 1996 a 2001
1996 – 41 not, 28 conf. 1997 – 77 not, 30 conf. 1998 – 86 not, 6 conf. 1999- 68 not, 24 conf. 2000- 68 not, 31 conf 2001 – 93 not,17 conf
0,9
1,71,8
1
1,4
2,1
0
0,5
1
1,5
2
2,5
1996 1997 1998 1999 2000 2001
21/04/23 Liú Campello Porto - HRAS - ESCS
2

TOXOPLASMOSE CONGÊNITADIAGNÓSTICO SOROLÓGICO
Orientações básicas
-Escolha do teste e do laboratório controle de qualidade (S e E=95% ?) repetir exames no mesmo laboratório acompanhamento de valores de IgG quantificação dos testes
21/04/23 Liú Campello Porto - HRAS - ESCS
3

TOXOPLASMOSE CONGÊNITADIAGNÓSTICO SOROLÓGICO
MÉTODOS MANUAIS
Títulos
IF > 1/1024
HI IgG>1/16
IgM +
MÉTODOS AUTOMATIZADOS
Índices•
ELISA > 300
MEIA RIA QUIMIOLUMINESCÊNCIA ELETROQUIMIOLUMINESCÊNCIA
IgM > 0,65 UI/ml IgM > 3,00 UI/ml (> correlação
com TC)
21/04/23 Liú Campello Porto - HRAS - ESCS
4

TOXOPLASMOSE CONGÊNITADiagnóstico Sorológico na Gestante
Interpretação complexa
– IgM + até 3 anos (Wilson; Mcauley,1999)
– IgM falso -
-baixa S
-transmissão 3º trim
– IgM falso +– IgM anti-Ac
maternos– “escape
placentário”
– IgA (+ 18 m)
– IgE (+8 m)
– Avidez (1º trim)
21/04/23 Liú Campello Porto - HRAS - ESCS
5

TOXOPLASMOSE CONGÊNITA
Definição de caso de toxoplamose gestacional (Lebech, 1996)
21/04/23 Liú Campello Porto - HRAS - ESCS
6
IgG - IgG +
Infecção confirmada
Infecção provável IgG IgM +>16 sem
Infecção possível IgG +IgM +< 16 sem
IgG IgM -> 16 sem
Infecção improvávelIgG IgM - +
IgG IgM -< 16 sem
IgG ?

TOXOPLASMOSE CONGÊNITA
Tratamento Fetal
Tratamento intrauterino previne transmissão e sequelas?
- SIM- precoce (McLeod R, Kieffer F, 2009)
–Inconclusivo (SYROCOT, 2007)
–aumento de CR em não tratados (Wilson, 1980; Phan et al, 2008)
21/04/23 Liú Campello Porto - HRAS - ESCS
7

Liú Campello Porto - HRAS - ESCS 8
Variável Modelo Univariado
Modelo final ajustado2
OR IC95% Valor p OR
(ajustado) (IC 95%) Valor p Teste
Classificação da gestante
0.002
Confirmado 6.65 (2.47a 17.91) 0.000 9.59 (341 a 26.94) <0,001
Provável 1.08 (0.53 a 2.20) 0.841 1.51 (0.73 a 3.17) 0.267
Possível 2.22 (0.97 a 5.08) 0.058 1.97 (0.85 a 4.56) 1.112
Improvavel/ Não classificada (ref.)
Tratamento pré-natal 0.002
Sim (ref.) Não 2.77 (1.54 a 4.97) 0.001 3.01 (1.61 a 5.64) 0.001
Não informado 2.44 (0.66 a 9.08) 0.182 2.68 (0.68 a 10.56) 0.159
Tipo de tratamento 0.005
Esquema 1 (ref.) Esquema 2 ou 3 0.22 (0.03 a 1.68) 0.144 0.19 (0.02 a 1.51) 0.115
Tratado e não informado o tipo 0.63 (0.08 a 5.02) 0.663 0.43 (0.05 a 3.76) 0.444
Não tratado (somado 20 pacientes que não informaram)
2.25 (1.23 a 4.10) 0.008 2.36 (1.24 a 4.46) 0.008
Trimestre de início do tratamento 0.004
1º trim (ref.)
2º trim 2.15 (0.54 a 8.55) 0.279 2.13 (0.52 a 8.67) 0.291 3º trim 3.89 (1.02 a 14.89) 0.048 3.34 (0.85 a 13.17) 0.085
Não tratados ou não informados 6.07 (1.83 a 20.14) 0.003 6.24 (1.83 a 21.22) 0.003
Duração do tratamento 0.001
Completo 0.35 (0.19 a 0.65) 0.001 0.33 (0.17 a 0.64) 0.001 Outro (ref.)
21/04/23

TOXOPLASMOSE CONGÊNITA
Diagnóstico clínico
90% assintomáticos
Coriorretinite– 40% dos
assintomáticos (Porto, 2009)
– 85% infância
40% adolescência (Wilson,1980)
21/04/23 Liú Campello Porto - HRAS - ESCS
9

21/04/23 Liú Campello Porto - HRAS - ESCS
10
TOXOPLASMOSE CONGÊNITA
Diagnóstico Clínico
DOENÇA NEONATAL SEVERA (10%)
MICRO/MACROCEFALIA CORIORRETINITE
MACULAR BILATERAL

TOXOPLASMOSE CONGÊNITA
Manejo Clínico RN
Caso Suspeito
Mãe
IgM +
RN
Sintomático IgG+
Assintomático IgM +
21/04/23 Liú Campello Porto - HRAS - ESCS
11
Sorologia para toxoplasmose (IgG e IgM), teste de triagem neonatal
Hemograma Completo Fundo de olho Exame de LCR Rx de crânio US de crânio

TOXOPLASMOSE CONGÊNITA
Acompanhamento ambulatorial
21/04/23 Liú Campello Porto - HRAS - ESCS
12

TOXOPLASMOSE CONGÊNITA
Acompanhamento ambulatorial
21/04/23 Liú Campello Porto - HRAS - ESCS
13

TOXOPLASMOSE CONGÊNITA
Tratamento pós-natalDROGA DOSE TEMPO
PIRIMETAMINA 1 mg/Kg/diaAssintomáticoSintomático
1 mg/Kg/dia 2a-4a-6a
2 meses6 meses
Até 1 ano
SULFADIAZINA 80-100 mg/Kg/dia
12/12 h
1 ano
ÁC.FOLÍNICO 10mg/dia 2a-4a-6a
1 ano
PREDNISONA 1 a 2 mg/kg/dia Processo inflamatório
21/04/23 Liú Campello Porto - HRAS - ESCS
14

TOXOPLASMOSE CONGÊNITA
Tratamento pós-natal
PROCESSO INFLAMATÓRIO DROGA
RETINOCOROIDITE PREDNISONA 1 a 2 mg/kg/dia(repetir FO a cada 7 dias)
HIPERPROTEINORRAQUIA (> 1 g/dL) PREDNISONA 1 a 2 mg/kg/dia(repetir PL a cada 7 dias)
21/04/23 Liú Campello Porto - HRAS - ESCS
15

TOXOPLASMOSE CONGÊNITA PREVENÇÃO
PRIMÁRIA:
teste sorológico precoce,orientação higieno-dietética
SECUNDÁRIA: investigação e tratamento da gestante
TERCIÁRIA: investigação (testes sorológicos, triagem neonatal) e tratamento do RN
21/04/23 Liú Campello Porto - HRAS - ESCS
16

TOXOPLASMOSE CONGÊNITA
Prevenção primária
VERDURAS CRUAS
80% SIM Londrina (Lopes et al, 2009)DF (Porto L, 2010)
CARNE MAL COM FEZES DE GATO
20% SIM (Porto L, 2010)
21/04/23 Liú Campello Porto - HRAS - ESCS
17

1821/04/23 Liú Campello Porto - HRAS - ESCS

TOXOPLASMOSE CONGÊNITA
Casos Clínicos

TOXOPLASMOSE CONGÊNITACaso Clínico 1
P.J.N. Admitido aos 32
dias de vida Tratamento:
esquema tríplice anti-toxoplasma
ANTEC DA CRIANÇA:
RNT+AIG; assintomático Exames realizados ao
nascimento Sorologia
IgG = 490
IgM = neg
US= normal FO = normal
21/04/23 Liú Campello Porto - HRAS - ESCS
20

TOXOPLASMOSE CONGÊNITA
Caso Clínico 1
ANT. GESTACIONAIS
G3 P3 Ao consultas PN> 6 sem registro de
sorologia para toxoplasmose em gestações anteriores
Tratamento: espiramicina do 4º mês até o parto
Infecção Provável
21/04/23 Liú Campello Porto - HRAS - ESCS
21

TOXOPLASMOSE CONGÊNITACaso Clínico - 1
Evolução : assintomático
Conduta: alta para atenção primária
21/04/23 Liú Campello Porto - HRAS - ESCS
22

TOXOPLASMOSE CONGÊNITA
Caso Clínico 2
P.L.O.N. Admitido aos 20
dias Medicação: sem
esquema tríplice anti-toxoplasma
Sem queixas.
ANTEC DA CRIANÇA: RNT+AIG; assintomático
EXAMES REALIZADOS ao nascimento
Sorologias– IgG = 430 – IgM = 0,3
FO= normal Rx crânio= normal Teste de triagem
neonatal = negativo21/04/23 Liú Campello Porto - HRAS -
ESCS23

TOXOPLASMOSE CONGÊNITA
Caso Clínico 2
ANTECEDENTES
GESTACIONAIS
G4 P4 Ao PN= 3X sem registro de
sorologia para toxoplasmose em gestações anteriores
Tratamento: espiramicina do 5º mês até o parto
Caso confirmado
21/04/23 Liú Campello Porto - HRAS - ESCS
24

TOXOPLASMOSE CONGÊNITA
Caso Clínico 2
Mantido sem medicação Evolução : assintomático
Conduta: alta para atenção primária
SOROLOGIA TOXO 1 mês 5 meses 8 meses
IgG (VR=10 UI/ml)
IgM (VR=0.65 UI/ml)
155
NEG
26 14
Liú Campello Porto- HMIB-ESCS
2521/04/23

TOXOPLASMOSE CONGÊNITA
Caso Clínico 3
I.F.C.S. Medicação:
usando esquema tríplice desde nascimento
ANTEC DA CRIANÇA:
RNT+AIG
Assintomático
EXAMES REALIZADOS ao nascimento
-Sorologia
IgG = 68 UI
IgM = negativo - Resultado de IgM 22 dias de
vida = 4,3 UI/ml -FO = normal -US = normal -RX CRÂNIO = normal -LCR = normal
21/04/23 Liú Campello Porto - HRAS - ESCS
26

TOXOPLASMOSE CONGÊNITA
Caso Clínico 3
Antec Obstétricos G2 P0 C2 Ao Medicação: 3º mês
ao parto
Caso confirmado
21/04/23 Liú Campello Porto - HRAS - ESCS
27

TOXOPLASMOSE CONGÊNITA
Caso Clínico 3
Acompanhamento Multidisciplinar Tratamento por 12 meses com
esquema tríplice -HC mensal -FO trimestral
21/04/23 Liú Campello Porto - HRAS - ESCS
28

TOXOPLASMOSE CONGÊNITACaso Clínico 4
L.M.T.A.O Admitido aos 32
dias
Medicação= sem esquema tríplice anti-toxoplasma
Sem queixas.
ANTEC DA CRIANÇA:
RNT+AIG; Assintomático
EXAMES REALIZADOS ao nascimento
Sorologia
– IgG = 2923 (VR=3)
– IgM 0,19 (VR= 0,8)
-FO = normal -US = normal -RX CRANIO = normal -LCR = não realizado -TC = não realizada
21/04/23 Liú Campello Porto - HRAS - ESCS
29

TOXOPLASMOSE CONGÊNITACaso Clínico 4
ANTECEDENTES GESTACIONAIS G3 P3 C0 A0 PN= 5X sem registro de sorologia para toxoplasmose em
gestações anteriores
Tratamento: não
Liú Campello Porto- HMIB-ESCS
3021/04/23

TOXOPLASMOSE CONGÊNITACaso Clínico 4
ANTECEDENTES GESTACIONAIS
G3 P03C0A0 n. consultas PN= 5X
sem registro de sorologia para toxoplasmose em gestações anteriores
Tratamento: não
Caso Provável
21/04/23 Liú Campello Porto - HRAS - ESCS
31

TOXOPLASMOSE CONGÊNITACaso Clínico 4
ACOMPANHAMENTO:
Assintomático Suspensa medicação aos 2 meses
Liú Campello Porto- HMIB-ESCS
3221/04/23

TOXOPLASMOSE CONGÊNITACaso Clínico 5
D.D.P.B
Medicação: usando esquema tríplice desde nascimento
ANTEC DA CRIANÇA: RNT+AIG EXAMES REALIZADOS ao
nascimento
Sorologia
IgG> 300
IgM = neg -FO = normal -US = dilatação biventricular
4.5 mm -RX CRÂNIO = normal -LCR = normal -
21/04/23 Liú Campello Porto - HRAS - ESCS
33

TOXOPLASMOSE CONGÊNITACaso Clínico 5
Antec Obstétricos
G1 P1 C0 Ao
Medicação: espiramicina do 7º mês até o parto
Caso Possível
21/04/23 Liú Campello Porto - HRAS - ESCS
34

TOXOPLASMOSE CONGÊNITACaso Clínico 5
Acompanhamento Assintomático Suspensa medicação aos 2 meses
Liú Campello Porto- HMIB-ESCS
3521/04/23

TOXOPLASMOSE CONGÊNITACaso Clínico 6
M.I.R.S
Medicação = nega uso
ANTEC DA CRIANÇA RNT+ GIG;
assintomático EXAMES REALIZADOS ao
nascimento Sorologia
– Triagem neonatal
IgM reag.
ELISA : 2,06 UI/ ml
21/04/23 Liú Campello Porto - HRAS - ESCS
36

TOXOPLASMOSE CONGÊNITACaso Clínico 6
Antec Obstétricos G3 P1 C2
Sem tratamento
Liú Campello Porto- HMIB-ESCS
3721/04/23

TOXOPLASMOSE CONGÊNITACaso Clínico 6
Acompanhamento– Presença de nistagmo. Não fixa o olhar– Baço = palpável a 1 cm RCE– Fígado= palpável a 2 cm RCD
FO: OD= CR macular cicatrizada OE= condensação vítrea em foco
peripapilar, sem vitreíte Solicito TC de crânio e HC Esquema tríplice para toxoplasmose
Liú Campello Porto- HMIB-ESCS
3821/04/23

TOXOPLASMOSE CONGÊNITACaso Clínico 6
Acompanhamento – 2 meses aos 4 meses– Presença de nistagmo. Não fixa o olhar– Baço = não está mais palpável – Fígado= impalpável – Reflexos presentes
. Resultado de TC de crânio Hiperatenuações corticais medindo 03 mm
Sistema ventricular de dimensões normais. (Toxoplasmose calcificada?)
Liú Campello Porto- HMIB-ESCS
3921/04/23

Nota do Editor do site, Dr. Paulo R. Margotto
Consultem também em www.paulomargotto.com.br (Infecções Perinatais
Crônicas)
Do livro Assistência ao Recém-Nacido de Risco, ESCS, Brasília,3a Edição,
2013,
Toxoplasmose congênitaAutor(es): Liu Campello Porto