Toxicology 3. toxicokinetics Biotransformation: Hepatic-first pass metabolism Xenobiotics absorbed...
41
Toxicology 3. Toxicology 3. toxicokinetics toxicokinetics Biotransformation: Hepatic-first pass metabolism Xenobiotics absorbed from the gastrointestinal tract Exceptions: Mouth (Nitroglycerine, weak base, to be put under the tongue), Colon Extrahepatic metabolism Epithelium of the GI tract Skin lungs
-
Upload
helena-johns -
Category
Documents
-
view
220 -
download
0
Transcript of Toxicology 3. toxicokinetics Biotransformation: Hepatic-first pass metabolism Xenobiotics absorbed...

Toxicology 3.Toxicology 3.toxicokineticstoxicokinetics
Biotransformation: Hepatic-first pass metabolism
Xenobiotics absorbed from the gastrointestinal tract Exceptions: Mouth (Nitroglycerine,
weak base, to be put under the tongue), Colon
Extrahepatic metabolism Epithelium of the GI tract Skin lungs

bioavailability
Ratio of the dose reaching the systemic circulation (0-1)
Bioavailability depends on oral absorption and the first pass metabolism.
Concentration of the molecule in the blood after oral administration/ Concentration of the molecule in the blood after intravenous administration

Distribution:Binding to plasma proteins Plasma protein binding: helps the distribution of a
xenobiotic and prevents its excretion Reversible/irreversible affinity, Kd= concentration of free xenobiotic x
concentration of free binding site/ concentration of occupied binding sites

Species differences in binding to plasma proteins Thyroxine is binding to plasma proteins in humans. 2/3 of
thyroxine molecules are present in the form of thyroglobulin, the remaining molecules bind to albumins or prealbumins.
In rats thyroxine is dissolved in the blood without binding to proteins.
Some xenobiotics induce metabolic enzymes and accelerate the elimination of thyroxine.
In rats: as the level of thyroxine is reduced, the thyroid gland tries to produce more thyroxine by cell proliferation. This can lead to tumours in the thyroid.
In humans: the same xenobiotic will not cause thyroid tumours, because of the protein binding of the thyroxine.

EliminationExretion Biotransformation Ecretion via urine Excretion via the bile Excretion via the lungs Ecretion with mother’s milk, placenta, hair, saliva,
tears…etc,

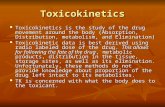
Route of excretion(%)
compound Molecular mass kidney Faeces
Biphenyl 154 80 20
4-monochloro-biphenyl 188 50 50
4,4’-dichloro-biphenyl 223 34 66
2,4,5,2’,5’-pentachloro-biphenyl 326 11 89
2,3,6,2’,3’,6’-hexachloro-biphenyl 361 1 99
Nefron
Ultra-filtration, passive re-Ultra-filtration, passive re-absorption, active tubular absorption, active tubular
secretionsecretion
Table: Molecular mass and the route Table: Molecular mass and the route of some biphenyls in ratsof some biphenyls in rats
Reference: H. B. Mattheus in: Introduction to Biochemical Toxicology (1960)

Enterohepatic circulationEnterohepatic circulation

Effects depend on
Dose Time period of dosing Other molecules present (induction, inhibitionj)
Graded response- measured on a continouos scale Quantal response –measured by counting responders
in a group

Receptor types
Intracellular receptors Cell surface receptors
Receptors with enzyme activity
Receptors leading to a chain of reactions
Receptors triggering a secondary messenger
Ion chanels

Intracellular receptorIntracellular receptor

Tyrosine kinase: a transmembrane receptor having enzyme activityTyrosine kinase: a transmembrane receptor having enzyme activity

Receptor with enzyme activity triggering a chain reactionReceptor with enzyme activity triggering a chain reaction

G-G-protein coupled receptorprotein coupled receptor

Ion chanel receptorIon chanel receptor

ToxicodynamicsEthanol
Absorption: passive diffusion from the whole length of the GI tract Pow= 0,4898 (logPow= -0,31)

Metabolism of ethanol Ethanol
Alcohol dehydrogenase (SER, MFO)
Acetaldehyde Aldehyde dehydrogenase (2 isoforms, in cytosol or
mitochondria)
Acetic acidACSS2 enzyme (Acetyl-coenzymeA synthetase S2, cytosol)
Acetyl-coenzyme A Enzymes of the citrate cycle
3 H2O + 2 CO2 Energy : approximately 1300 kJ/mol

Elimination of ethanol and its metabolites
Ethanol: urine, exhalation, sweat
Acetic acid- urine
Acetyl-coenzyme A- used for biosynthetic processes, biotransformation, like acetilation or as an energy source in the citrate cycle

The elimination rate of ethanol
Rate limiting step: oxydation to acetaldehyde Reaction of 0 grade (KM: 80 mg/l, but much
higher plasma concentration is frequent) Elimination rate: 10 g ethanol/hour, the
elimination of ½ l wine takes 7 hours

Acute effects of ethanol
g/l

For later effects (hangover, intoxication effects) mainly the acetaldehyde is responsible and the free radicals it generates. Free radicals cause oxidative stress and cell death. Two forms of aldehyde dehydrogenase are
present in the cytosol or in mitochondria
In the white population both forms are active while in 50% of Asiatic people the mitochondial enzyme is missing or has a very low activity.

Effects of chronic ethanol exposure
free radicals –cell damage Liver –is the main target organ
Chronic hepatitis Fatty liver (5%-50% lipid content ) Livercirrhosis Liver tumours

Further chronic effects Pancreas
Pacreatitis Tumours
Heart The performance of the heart is reduced (Chronic
cardiomyopathy) Nervous system
Tremors, impairment of the sight and the memory willpower, impaired judgment, emotional lability, outbursts of anger…

Effects on the development
Low birth weightSmall head circumferencenervous system disordersabnormalities of the hippocampus: learning difficultiesSmall cerebellum: motion developmental disordersSmall corpus callosum, hyperactivity, impulsive behavior

Some characteristics of the fetal alcohol syndrome

Dose dependent fetal effects:
Strong drinking: teratogenic effects
Moderate drinking:neurotoxic effects (fetal NOAEL can not be established)

Summary of the chronic effects of ethanol
Toxic for several organs Carcinogenic (I.A.R.C. Cat1A, ) Neurotoxic Teratogenic

Causes of carcinogenesis
Physical (ionizing radiation)Chemical (genotoxic and non-genotoxic carcinogens)Biological (viruses, bacteria, endoparasitic insects, etc.)

Steps of chemical carcinogenesisStep 1 InitiationHighly electrophilic structures, free radicals, organic
cations bind covalently to special nucleophilic binding sites of the DNA and form DNA-adducts
(some critical sites: Guanine C8, N2, N3, O6, Timidine, Uracil O2, O4, N3 position).

Step 2 Fixation: If repair enzymes cut off the altered parts, then DNA
polymerase synthetizes the missing part on the basis of the complementer strand ---the cell remains normal
If the mutation takes place in an inactive part of the DNA, this does not change the functions-the--cell remains normal
The mutation damages seriously the functions of the cell ---the cell dies, the organism remains healthy
if the altered cell survives and divides-the mutation can be fixed.

Capacity of DNA repair in some organs Liver: good Kidney: intermediate Brain: practically missing

Step 3 Promotion: selective increase of the iniciated cells helped by a repeated effect of a promoter within a critical period of time Not a genetic effect The result is a microscopic neoplasia The promoter effect is dose dependent but there
is a limit dose

Some promoters
Mitogens: substances stimulating cell proliferation (endogenous mitogens, like estrogens or other hormones or exogenous mitogens.)
Permanent presence of cytotoxic substances Persisting mechanical effects (irritation) causing
cytotoxicity Blood loss in rats is promoting leukemia

Inhibition of the carcinogenic process
Inhibition of cell division Immune system (macrophags, limphokins) Reduced total energy intake Specific dietary components: Vitamines A, C and
E

Step 4 Progression
For further increase of iniciated cells— often a new mutation is needed. New initiated cell types have to appear which produce angiogenesis factor, helping vascularisation of the micro-tumour
Blood vessels develop in the harmless microtumour ( max.0,5 mm3) and the small tumour starts to grow at an exponential rate.

Step 5 Metastases
The tumour becomes invasive, the cancer cells disseminate through blood and lymph vessels and new, secunder tumours develop at different parts of the body.

Tumour therapy
Surgical therapy Radiotherapy Drug therapy Komplex therapy

Types of anti-cancer drugs
Drugs inhibiting DNA duplication Antimetabolites (Enzyme inhibitors, nucleic acid
synthesis inhibitors: methotrexate, antifolates, pirimidin antagonists, dezoxycyitidine analogs, purine antagonists
DNA alkylating agents :cyclophosphamide (they prevent cell proliferation, but might have serious effects):
Topoizomerase I és II inhibitors ( they inhibit the integration of DNA chains)

Agents that affect the regulation of cell proliferation Mitotic spindle inhibitors: Vinca alkaloids, taxanes,
vinblastine, vinchristine, taxol, taxotere (inhibiting the development of the mitotic spindle)
Hormones and hormone-like compounds, like progesterones, anti-estrogens, aromatase inhibitors, anti-androgens, which inhibit the growth of hormone dependent tumours.
Cytokins (interferons, interleukins): inhance the immune response of the host
Tyrosine kinase inhibitors: they reduce the viability of tumour cells by inhibiting signal transduction
Monoclonal antibodies: they inactivate cell surface receptors

3
Drugs inhibiting vascularisation
Avastine, thalidomide
Anti-metastasis agents
Bisphosphanates: prevent stone metastasis from breast and prostate tumours.

Drugs to improve the quality of life of the patient Filgrastine. Enhances the production of white
blood cells Erithropoetine alpha: helps the proliferation of
erithrocytes Mesna, Amifostine: neutralise the reactive groups
of drugs in the healthy tissues.

Literature recommended
Niesink et al: Toxicology, Principles and applications (1996.) CRC Press, LLC and Open University of the NetherlandsISBN: 0-8493-9232-2
Gyires Klára, Fürst Zsuzsanna: Farmakológia (2007.) Medicina Könyvkiadó Rt., BudapestISBN: 978 963 226 137 9 (I kötet)