Toxicological Myths and Half-Truths
58
Toxicological Myths and HALF-Truths Chris Nickson FACEM Alfred ICU Senior Registrar A Talk by Chris Nickson FACEM Senior Registrar at the Alfred ICU
-
Upload
precordialthump -
Category
Health & Medicine
-
view
1.189 -
download
1
description
The slides for my talk on 'Toxicological Myths and Half-Truths' that was given at the CICM ASM 2013 in Wellington, New Zealand. The theme of the conference was "Down with Dogma: Challenging the Fundamentals of Critical Care"
Transcript of Toxicological Myths and Half-Truths

Toxicological Myths and HALF-Truths
Chris Nickson FACEM Alfred ICU Senior Registrar
A Talk by Chris Nickson FACEM Senior Registrar at the Alfred ICU

Image from h+p://technicalinfodotnet.blogspot.com.au/2012/03/virtual-‐execu@on-‐and-‐emperors-‐new.html
NO CONFLICTS OF INTEREST Talk resources at h+p://liDl.org/11p0o81

Photo by Cavin on Flickr

Glucagon
Calcium, Digoxin & the Stone Heart Theory
Paracetamol Toxicity & Liver Transplanta>on

Glucagon
Calcium, Digoxin & the Stone Heart Theory
Paracetamol Toxicity & Liver Transplanta>on

Glucagon
Calcium, Digoxin & the Stone Heart Theory
Paracetamol Toxicity & Liver Transplanta>on

Glucagon

Glucagone?

Boyd R, Ghosh A. Towards evidence based emergency medicine: best BETs from the Manchester Royal Infirmary. Glucagon for the treatment of symptoma@c beta blocker overdose. Emerg Med J. 2003 May;20(3):266-‐7. O'Connor N, Greene S, Dargan P, Jones A. Glucagon use in beta blocker overdose. Emerg Med J. 2005 May;22(5):391. PubMed PMID: 15843722; PubMed Central PMCID: PMC1726782.

[In toxicology an] evidence basis is often lacking and one therefore needs to rely on a combination of practical experience, case reports and assessment of biological plausibility. There is a sound theoretical basis for the use of glucagon in the cardiovascularly compromised patient who has taken a beta blocker overdose. Glucagon activates adenyl cyclase and exerts an inotropic and chronotropic effect by a pathway that bypasses the beta receptors. …

Each of us has personal experience of the dramatic improvement in cardiovascular parameters that can occur following the administration of glucagon in this clinical situation. …

… Nobody would suggest that naloxone should not be used for opiate overdose yet the evidence base for its use is as flimsy as that of glucagon in beta blocker overdose. We suggest that to attempt to undertake a randomised clinical trial of the use of glucagon in the compromised beta blocker overdosed patient would be unethical. …

Smith GC, Pell JP. Parachute use to prevent death and major trauma related to gravita@onal challenge: systema@c review of randomised controlled trials. BMJ. 2003 Dec 20;327(7429):1459-‐61.
Is glucagon really a
parachute?

Photo by JD Hancock on Flickr
Or is glucagon one
of these?

Show me the evidence!
Photo by Chris Nickson

Photo by zzpa on Flickr

Photo by zzpa on Flickr
Before 1998 some vials of glucagon contained up to 100 units of insulin

Photo by Marianne Perdomo
New dogma?Insulin 6 versus
Glucagon 4

Calcium, Digoxin and the
Stone Heart Theory

Photo by Peregrinari on Flickr

h+p://lifeinthefastlane.com/ecg-‐library/basics/hyperkalaemia/

Calcium, Digoxin Toxicity
and the Stone Heart
Theory
Calcium for hyperkalaemia in digoxin toxicity?
Photo by Gaptone on Flickr

Photo by Melina from Flickr
Beware the Stone Heart!

h+p://www.realmagick.com/digoxin-‐mechanism-‐of-‐ac@on/

What happened to
me?
Photo by Peregrinari on Flickr

She got better

doi:10.1016/j.jemermed.2008.09.027
Selected Topics:Toxicology
THE EFFECTS OF INTRAVENOUS CALCIUM IN PATIENTS WITHDIGOXIN TOXICITY
Michael Levine, MD,* Heikki Nikkanen, MD,†‡ and Daniel J. Pallin, MD†
*Department of Medical Toxicology, Banner Good Samaritan Medical Center, Phoenix, Arizona, †Department of Emergency Medicine,Brigham and Women’s Hospital, Boston, Massachusetts, and ‡Division of Medical Toxicology, Division of Emergency Medicine,
Children’s Hospital, Boston, MassachusettsReprint Address: Michael Levine, MD, Department of Medical Toxicology, Banner Good Samaritan Medical Center,
925 East McDowell Road, 2nd floor, Phoenix, AZ 85006
e Abstract—Background: Digoxin is an inhibitor of thesodium-potassium ATPase. In overdose, hyperkalemia iscommon. Although hyperkalemia is often treated with in-travenous calcium, it is traditionally contraindicated indigoxin toxicity. Objectives: To analyze records from pa-tients treated with intravenous calcium while digoxin-toxic.Methods: We reviewed the charts of all adult patientsdiagnosed with digoxin toxicity in a large teaching hospitalover 17.5 years. The main outcome measures were fre-quency of life-threatening dysrhythmia within 1 h of cal-cium administration, and mortality rate in patients who didvs. patients who did not receive intravenous calcium. Weuse multivariate logistic regression to ensure that no rela-tionship was overlooked due to negative confounders (con-trolling for age, creatinine, systolic blood pressure, peakserum potassium, time of development of digoxin toxicity,and digoxin concentration). Results: We identified 161 pa-tients diagnosed with digoxin toxicity, and were able toretrieve 159 records. Of these, 23 patients received calcium.No life-threatening dysrhythmias occurred within 1 h ofcalcium administration. Mortality was similar among thosewho did not receive calcium (27/136, 20%) compared tothose who did (5/23, 22%). In the multivariate analysis,calcium was non-significantly associated with decreasedodds of death (odds ratio 0.76; 95% confidence interval[CI] 0.24 –2.5). Each 1 mEq/L rise in serum potassiumconcentration was associated with an increased mortalityodds ratio of 1.5 (95% CI 1.0–2.3). Conclusion: Amongdigoxin-intoxicated humans, intravenous calcium doesnot seem to cause malignant dysrhythmias or increase
mortality. We found no support for the historical beliefthat calcium administration is contraindicated in digoxin-toxic patients. © 2011 Elsevier Inc.
e Keywords—digoxin; digoxin toxicity; hyperkalemia;calcium
INTRODUCTION
Digoxin is a cardiac glycoside that is commonly prescribedto patients with congestive heart failure, especially thosewith co-existing atrial fibrillation. Digoxin, like other car-diac glycosides, inhibits the sodium-potassium ATPasepump, thereby increasing the intracellular sodium concen-tration (1–5). The increased intracellular sodium inhibitssodium-dependent calcium transport out of the cyto-plasm, resulting in increased intracellular calcium, andthus increased inotropy. In overdose, digoxin’s inhibitionof the sodium-potassium ATPase frequently results inhyperkalemia (3,6).
In experimental models, calcium potentiates the pos-itive inotropic effects of cardiac glycosides (7). How-ever, in animal models, calcium was found to increasedigoxin toxicity (8–12). This effect was found to bedose-dependent and related to the rate of infusion, butonly at unrealistically high calcium concentrations(10,12). The “stone heart” theory views calcium as the
RECEIVED: 2 July 2008; FINAL SUBMISSION RECEIVED: 16 August 2008;ACCEPTED: 3 September 2008
The Journal of Emergency Medicine, Vol. 40, No. 1, pp. 41–46, 2011Copyright © 2011 Elsevier Inc.
Printed in the USA. All rights reserved0736-4679/$–see front matter
41

20% of pa@ents with
digoxin toxicity died

No difference if IV calcium was given or not
calcium given: 5/23 (22%) died not given: 27/136 (20%) died

No dysrhythmias within 4 hours of IV calcium

Photo by Stefan onFlickr
We need to keep looking…

Only 5 case reports of calcium linked to death in
digoxin toxicity
None are convincing
Bower JO ,Mengle HAK. The addi@ve effect of calcium and digitalis. JAMA 1936 ;106(14):1151–1153

Original animal models were flawed…
Only harmful if calcium
>15 mmol/L

Photo by Nitot from Flickr

Pseudoaxioms
false principles or rules handed down from genera@on to genera@on
and accepted without serious challenge or inves@ga@on
Newman DH: Truth, and epinephrine, at our finger@ps: unveiling the pseudoaxiom. Ann Emerg Med 2007; 50:476–477.

Paracetamol Overdose and
Liver Transplantation

A dilemma Photo by dno1967b on Flickr

Select early
Photo by dno1967b on Flickr

Photo by dno1967b on Flickr
Select early
Risks of surgery Immunosuppression $$$$$ Opportunity cost

King’s College Criteria
for paracetamol-‐induced hepatoxicity
Grady JG, Alexander GJ, Hayllar KM, Williams R. Early indicators of prognosis in fulminant hepa@c failure. Gastroenterology. 1989 Aug;97(2):439-‐45.

pH < 7.3
or, in a 24h period, all 3 of:
INR > 6 (PT > 100s) Cr > 300 mmol/L
grade III or IV encephalopathy
recent modifica@on: lactate >3.5 mM

King’s College Criteria is specific
80-‐90%
but not sensi@ve 60-‐70%

King’s College Criteria
Photo by The PIX-‐JOCKEY on Flickr
What could possibly be wrong with the King’s Criteria?

Evidence and consequences of spectrum bias in studies ofcriteria for liver transplant in paracetamol hepatotoxicity
G.K.A. DING1,2,3 and N.A. BUCKLEY1,4
From the 1Australian National University Medical School, ACT, 2Department of Intensive Care,The Canberra Hospital, 3Department of Intensive Care, The Calvary Hospital, Canberra and4Faculty of Medicine, University of NSW, Australia
Received 31 October 2007 and in revised form 7 April 2008
Summary
Objective: In severe paracetamol hepatotoxicity,orthotopic liver transplant (OLT) is a standardtreatment in patients judged to have a hopelessprognosis. The most commonly used criteria tomake this decision are the King’s College Criteria(KCC). We aimed to compare the expected survivalfor patients who meet the KCC and do not receivetransplant and those who receive OLT.Methods: A systematic review of studies of survivalin patients who met the KCC according to whetherthey were transplanted. Data from these studies wasextrapolated to compare long-term survival with andwithout adjustment for Quality of Life.Results: The survival of patients meeting KCC andundergoing transplant has not been specificallystudied. UK data on transplants for acute liverfailure indicate 1 and 10 year survival rates of 65and 44%, respectively. Survival in those withouttransplant was documented in 15 studies. Theaverage long-term survival rate was 24.9%.
Survival was worse in studies originating in theKing’s unit (13.8 vs. 30.0%). It was apparent that thismay be due to spectrum bias occurring in this muchlarger unit. There was clear evidence that those withthe best prognosis were preferentially transplantedat the Kings liver unit, indicating the criteria mayperform significantly worse at predicting deathwithout transplant than previously estimated. Evenso, for a 20-year-old meeting KCC, the best estimateof life expectancy with transplant (13.5 years) is nobetter than without (13.4 years). Adjustment forquality of life made OLT clearly a worse option.Conclusion: Criteria for OLT that have a muchhigher positive predictive value (for death withouttransplant) are required. Such studies must beconducted only on those who would be consideredsuitable for transplant. Non-orthotopic liver trans-plant may be a preferred option in such circum-stances, although much more data on survival afterthis procedure are required.
BackgroundParacetamol induced liver failure is a serious andpotentially fatal poisoning which occurs commonlyin the United Kingdom. Approximately 100–150people die as a result of paracetamol poisoning, andan estimated 40 000 individuals take paracetamoloverdoses each year.1 In patients who are otherwiseexpected to die, orthotopic liver transplant (OLT)is recommended. OLT is performed in specialist
centers and because this treatment is only clearlyjustifiable in patients who would otherwise die,criteria for determining such patients have beenestablished. If such criteria were perfect, all patientswho would benefit from transplant would beidentified while they were well enough to receivethis major surgery and those that would otherwisesurvive would always be excluded.
Address correspondence to Nick Buckley, Medical Professorial Unit, POW Hospital Clinical School,University of NSW, Level 1, South Wing Edmund Blackett Building, Randwick. 2031, Australia.email: [email protected]
! The Author 2008. Published by Oxford University Press on behalf of the Association of Physicians.All rights reserved. For Permissions, please email: [email protected]
Q J Med 2008; 101:723–729doi:10.1093/qjmed/hcn077 Advance Access published on 7 July 2008
at NT D
ept of Health and Fam
ilies on September 10, 2012
http://qjmed.oxfordjournals.org/
Dow
nloaded from

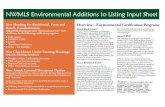
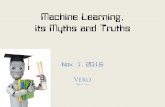
The typical age of paracetamol self-poisoning is20–25 years.4,5 The average life expectancy in thedeveloped world is !80 years. Therefore we model-led the outcome of the decision to transplant a20-year-old on their survival over the next 60 years.Survival rates for transplanted patients beyond 10years for which data are available was extrapolatedby simple arithmetic regression (the same percentageof survivors dieing each year from complications oftheir transplant after year 10 as died between year 1and 10—pale lines in Figure 2). Those who were nottransplanted were assumed to have normal health.Both groups were assumed to also be affected byother causes of mortality equally using data on agerelated mortality in the UK from the WHO GlobalBurden of Disease Project 2001.6
For quality of life assessment, patients survivingwithout a transplant were assumed to have a normalquality of life. So their life expectancy was alsocompared with QALY survival in those with a livertransplant. For such purposes, transplanted individ-uals are estimated to have a quality of life of 0.6compared to a healthy population.7
ResultsThe results of the search strategy are summarizedin Figure 1. Many articles were rejected as theabstracts indicated they could not possibly containoriginal data on this subject. Another 51 articleswere rejected because on review of the original
paper the relevant data was not present (e.g. deathand transplant combined, other severity scorescombined with King’s criteria). Of the 36 articlesidentified in the two searches, 11 were identifiedin both searches and this left a total of 25 articlescontaining relevant data.8–33 Two studies from theKing’s centre had complete overlap with two largerstudies from the same unit and were excludedto prevent major duplication of results.8–11 Onestudy from Birmingham had complete overlap withanother and was excluded.12,13 One study from theScottish Liver Transplant Unit had complete tem-poral overlap with another and was excluded.28,30
Two studies from the Rigshositalet Copenhagen hadcomplete overlap with other studies and wereexcluded.14–19 One study from the RigshositaletCopenhagen had 24 months of 55 months (43%)overlap with another and was excluded.18,32 OneStudy from the Rigshositalet Copenhagen had 1 yearof total 23 years overlap with another (4.3%) andwas included.16,18 The data from two articles fromThe Austin Hospital in Melbourne Australia wererepublished in another later article and wereexcluded.20–22 One Study from Cedars-Sinai hadcomplete temporal overlap with another and wasexcluded.26,31 The two other studies from King’s had3 months of the studies of a total 102 month overlap(2.9%) and were included for analysis.8,9 Data wasextracted from a total of 15 studies8,9,12,16–19,
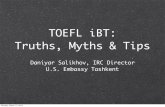
22–25,27,28,31,33 (Figures 1 and 3).From these studies there were 386 patients that
met KCC but were not transplanted and of these96 (24.9%) survived (95% Confidence interval20.8–29.4). The expected survival is shown inFigure 2. The expected survival benefit calculatedas area under curve (AUC) for a 20-year-old with theKCC was similar without a transplant (13.4 years) aswith a transplant (13.5 years). The expected survivalin Quality adjusted life-years in the transplanted
0 10 20 30 40 50 600
50
100
Transplanted
Not transplanted
extrapolation
QALY (transplanted)
extrapolation
Years after transplant
Sur
viva
l %
Figure 2. Estimated survival curves depending on deci-sion to transplant a 20-year-old with KCC for paracetamolinduced liver failure. Pooled data show survival of 24.9%(95% CI 20.8–29.4) in patients meeting KCC who are nottransplanted. Liver transplant recipients after acute liverfailure by comparison have survival at 10 years of 44%(95% CI 38–50). Thus, the odds ratio for 10-year survivalmight be estimated as favouring transplant recipients (OR1.77; 95% CI 1.29–2.40). However, the survival advan-tage becomes increasingly unfavourable with extrapola-tion, and even more so when using QALY.
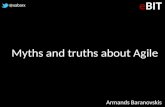
0 25 50 75
*O’Grady JG et al 1991*Bernal W et al 1998*Bernal W et al 2002
Ng et al 2004Anand et al 1997Shakil et al 2000
Detry et al 1999Larson et al 2005Chung et al 2003
Gow et al 1999Donaldson et al 1993
Schmidt 2003Schmidt 2004
Schiodt et al 1996Brandsaeter et al 2002
Died
Lived
Figure 3. Number of people who lived and died aftermeeting KCC for paracetamol induced liver fail-ure.8,9,12,16–19,22–25,27,28,31,33 Asterisk indicate Studyfrom King’s unit.
Liver transplant in paracetamol hepatotoxicity 725
at NT D
ept of Health and Fam
ilies on September 10, 2012
http://qjmed.oxfordjournals.org/
Dow
nloaded from

Survival benefit for a 20-‐year-‐old who meets
King’s College Criteria
13.4 years without transplant 13.5 years with transplant (8.4 QALYs)

Photo by shenamt on Flickr

Why so much dogma?

Flawed understanding of physiology
Poor quality or invalid studies
‘Chinese whispers’
Surrogate outcomes
Publica>on prac>ce distorts science
Difficulty learning to unlearn

Flawed understanding of physiology
Poor quality or invalid studies
‘Chinese whispers’
Surrogate outcomes
Publica>on prac>ce distorts science
Difficulty learning to unlearn

Flawed understanding of physiology
Poor quality or invalid studies
‘Chinese whispers’
Surrogate outcomes
Publica>on prac>ce distorts science
Difficulty learning to unlearn

Flawed understanding of physiology
Poor quality or invalid studies
‘Chinese whispers’
Surrogate outcomes
Publica>on prac>ce distorts science
Difficulty learning to unlearn

Flawed understanding of physiology
Poor quality or invalid studies
‘Chinese whispers’
Surrogate outcomes
Publica>on prac>ce distorts science
Difficulty learning to unlearn

Flawed understanding of physiology
Poor quality or invalid studies
‘Chinese whispers’
Surrogate outcomes
Publica>on prac>ce distorts science
Difficulty learning to unlearn

Which way now?

Eddleston M, et al. The hazards of gastric lavage for inten@onal self-‐poisoning in a resource poor loca@on. Clin Toxicol (Phila). 2007;45(2):136-‐43.

“It is everyone’s responsibility
to find out how to ask ques@ons systema@cally, find answers from
searching the literature, cri@cally appraise the literature and apply
the results to prac@ce”
Bellomo R. The dangers of dogma in medicine. Med J Aust. 2011 Oct;195(7):372-‐3.

Photo by Incurable_hippie on Flickr
The End Talk resources at h+p://liDl.org/11p0o81