Towards an Australian Approach Stefano Scalzo€¦ · Towards an Australian Approach Stefano Scalzo...
35
Design for Mental Health Towards an Australian Approach Stefano Scalzo A report prepared for the Winston Churchill Memorial Trust of Australia 2016
Transcript of Towards an Australian Approach Stefano Scalzo€¦ · Towards an Australian Approach Stefano Scalzo...
Design for Mental HealthTowards an Australian Approach
Stefano Scalzo
A report prepared for the Winston Churchill Memorial Trust of Australia2016

Cover image : Zentrum fur Psychiatrie, Reichenau by Huber Staudt Architekter (in Associa on with Baulinie Architekter)
1
Dedica on
This report is dedicated to the memory of Mr John Davidson Mitchell King, 1971-2012
Architect, set designer, vocalist and friend.
“Tyrell: The light that burns twice as bright burns half as long, and you have burned so very very brightly Roy”
Blade Runner, 1982 Ridley Sco

2
3
AcknowledgementsThis Report is the culmina on of almost two years eff ort structured around the prepara on, award, undertaking and repor ng of my 50th Anniversary Churchill Fellowship - the catalyst of a signifi cant realignment of my professional life for which I will be forever grateful.
I would like to acknowledge the contribu on of those people whose wisdom, insight, support and eff ort have all con-tributed to making this unique life changing experience possible.
Thank you to Judith Hemsworth and Mario Blandin de Chalain for sponsoring my Churchill Fellowship Applica on and for being such insigh ul and suppor ve colleagues and mentors. Thank you also to Giuseppe Scollo and Ma hew Hercus for facilita ng the exposure of this work amongst Victoria’s network of Mental Health policy experts, carers and administrators.
Thank you too to the many architects who have assisted me prepare for my trip abroad and then provided so gener-ously of their me and wisdom once in their company. Par cular thanks to the Directors and Associates of Tengbom Architects and White Architects, (Sweden), Origo Architects, (Norway), Schmi , Hammel, Larsen Architects and Karlssonark Architects, (Denmark), Huber Staudt Architects and Baulinie Architects, (Germany). Thank you also to the observa ons and clinical perspec ve of Dr Peter Steer, CEO GOSH, (England), Agneta Joreby Jonsson, (Uppsala) and S g- Artur Didriksen, (Bergen).
Further I am forever indebted to the staff , contractors and past Fellows of the Winston Churchill Memorial Trust and thankful for their generous professionalism and assistance shown all along this excep onal journey.
Finally I would like to acknowledge my wife Vanessa Mooney, whose love and support has fi gured so profoundly in this important phase of my life. Thank you for so de ly laying out this document and for being there in so many other ways, for me and our sons Orlando and Clay, whilst I was not.
“Wish we turn back me,
to the good ‘ol days
When our momma sang us to sleep
but now we’re stressed out”
Twentyone Pilots, Blurry Face
4
Table of ContentsDedica on
Acknowledgements
SECTION 011.0 Introduc on
2.0 Execu ve Summary
3.0 Programme
SECTION 024.0 Site visits
4.1 Uppsala Psychiatry by Tengbom Architects 4.2 Ostra Psychiatry by White Architects4.3 Kronstad Psychiatric Centre by Origo Architects4.4 Zentrum fur Psychiatrie Reichenau and Zentrum fur Psychiatrie Friedrichshafen
Psychiatry by Huber Staudt Architekten (in Associa on with Baulinie Architek-ten)
4.5 Psykiatrisygehus Slagelse by Karlsson5.0 On the drawing boards
5.1 Boras Psychiatry by White Architects5.2 Helsingor Hospital Psychiatry by Schmi Hammel Larsen6.0 In support of change
6.1 Academy and Prac ce: a mee ng with Stefan Lundin and Peter Frost6.2 Stefano Boeri and Bosco Ver cale6.3 Looking awry: Historical cues from art and culture
SECTION 037.0 Conclusions and Recommenda ons
7.1 Conclusion7.2 Recommenda ons7.3 Dissemina on of fi ndings
Notes & References
Note on the use of images: The illustra ons of architectural plans included in this report are reproduced with the approval of the respec ve architects for the express purposes of this study only. Also photographic images shown in this report were taken by the author under the direct supervision of clinical staff on the assump on that no consumer rights for privacy were compro-mised. Please note, more comprehensive illustra ons and images of the projects described herein are available on the respec ve architects’ websites.

5
SECTION 1

6
Previous page: Uppsala Psychiatry by Tengbom Architekts
7
1.0 Introduc on“We shape our environments and therea er they shape us.” Winston Churchill
A poignant observa on, u ered by a man said to have struggled with mental illness, which so aptly dis ls the focus of this study: the rela onship between the treatment of people suff ering a mental illness and the architecture that accommodates that treatment.
In Australia today, community awareness of mental health related issues con nues to grow with the 20% or so of people aff ected by some form of mental illness able to receive help every year. Of these people most, “recover well and are able to lead fulfi lling lives in the community- when they receive appropriate ongoing treatment and support”.
However, for 3% of Australians, a mental illness can be debilita ng requiring on going and informed care. For these people and others in our community aff ected by substance abuse, violence and homelessness, a stay in an acute mental health unit may be required to stabilise and treat a cri cal episode.
Although reference to programs and care models is made throughout this Report, they are not the focus of this study. Rather the focus of this study is architecture’s capacity to shape the restora ve environments required to accommo-date the aspira ons of these programs and care models in buildings over mul ple levels.
BackgroundAt its best, the built environment can help heal, as Stefan Lundin and colleagues write in Architecture as Medicine. At worst it conceals the inhumane. And so it did in the later part of last century when asylums erected a hundred years beforehand became symbols of human depravity.
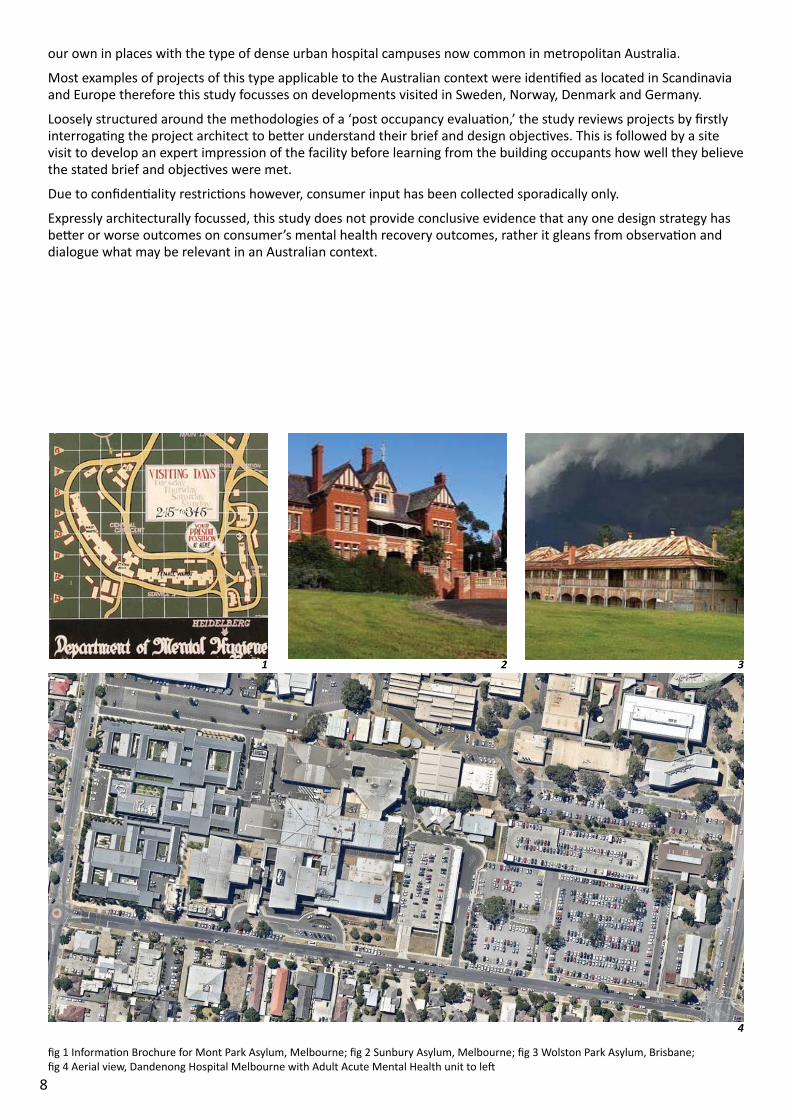
Asylums were originally conceived of as large outer metropolitan landscaped campuses of though ully arranged buildings designed in local styles that tempered the local climate (fi gs. 1-3). The restora ve proper es of the built environment were seemingly well understood.
Over me and away from the public’s gaze however, environments became more custodial than therapeu c and treatments and facili es deteriorated.
By the 1950-60s a world-wide movement that became known as ‘deins tu onalisa on’ sought to end the inhumane prac ces of the asylums and move mental health services back into the community.
From the 1970s large asylums were replaced with smaller psychiatric units developed on acute hospital campuses in recogni on of the co-morbid and emergency nature of acute mental health illnesses. This policy became known as ‘mainstreaming’.
The new units of the 1970-80s were o en mes designed using custodial templates disguised as domes c styled fa-cili es of single level with poor connec ons to outdoor areas. Now well over 30 years old, these same facili es have reached the end of their physical life and are in desperate need of replacement.
During this same 30 year period, care models have become more consumer (mental health pa ent) focussed and recovery orientated. Also during this me, there has re-emerged amongst architects, a renascent interest in the built environment’s capacity to assist healing.
In Australia today, many buildings built during the 1970-80s are being replaced by designs of high amenity. This is being achieved ostensibly through the adop on of building typologies that intertwine built form with landscape. The two most prevalent typologies are courtyard buildings or pavilions in landscape se ngs . In both cases however, buildings remain predominantly single level.
Both these typologies require large site coverage and therefore the rela vely small footprints of the 1970-80s have given way to the sprawling developments of the 2000s. Our metropolitan hospital sites however cannot accommo-date the resultant dispropor onate site coverage given the demands placed on them by other services.
Hassells (Architects) in Future Direc ons in Design for Mental Health Facili es, 2014, foresaw this dilemma when they observed, “… hospital sites are subject to huge pressures on land. It may be possible therefore, that there will be a return to larger, higher and denser building types.”
One solu on to this problem is to build new mental health facili es over mul ple levels incorpora ng the amenity aff orded by landscape access normally associated with single level developments.
Although some interes ng new typologies are emerging, including one designed by the author of this report for Wer-ribee Mercy Hospital in Victoria, there remains the need to gather evidence of how high amenity mental health units can be developed over mul ple levels.
Therefore this study seeks to visit exemplar projects of this type in countries with similar mental health programs to
8
our own in places with the type of dense urban hospital campuses now common in metropolitan Australia.
Most examples of projects of this type applicable to the Australian context were iden fi ed as located in Scandinavia and Europe therefore this study focusses on developments visited in Sweden, Norway, Denmark and Germany.
Loosely structured around the methodologies of a ‘post occupancy evalua on,’ the study reviews projects by fi rstly interroga ng the project architect to be er understand their brief and design objec ves. This is followed by a site visit to develop an expert impression of the facility before learning from the building occupants how well they believe the stated brief and objec ves were met.
Due to confi den ality restric ons however, consumer input has been collected sporadically only.
Expressly architecturally focussed, this study does not provide conclusive evidence that any one design strategy has be er or worse outcomes on consumer’s mental health recovery outcomes, rather it gleans from observa on and dialogue what may be relevant in an Australian context.
1 2 3
4
fi g 1 Informa on Brochure for Mont Park Asylum, Melbourne; fi g 2 Sunbury Asylum, Melbourne; fi g 3 Wolston Park Asylum, Brisbane; fi g 4 Aerial view, Dandenong Hospital Melbourne with Adult Acute Mental Health unit to le
9
2.0 Execu ve SummaryThis Report summarises lessons learnt by Mr Stefano Scalzo, architect, ([email protected], m. 0400 800 071), during his 50th Anniversary Churchill Fellowship exploring the design of high amenity mental health units over mul ple levels.
Stefano is currently Manager of the Design Services Unit of the Infrastructure and Planning Branch of the Sport and Recrea on, Infrastructure, Interna onal Engagement and Department of Housing Division of the Victorian Depart-ment of Health and Human Services.
His role at the Victorian Department of Health and Human Services places him in a unique posi on to be able to dis-seminate the fi ndings of this Report amongst Australian Government Agencies.
This study was undertaken to address specifi cally how mental health units of high amenity are designed in Scandi-navia and Europe over mul ple levels. It is not focussed on the many care models and programs that assist Mental Health suff erers recover from illness today.
The lessons learnt dis l into the following 10 recommenda ons:
1. Mental Health units are ideally developed over mul ple levels so as to minimise building footprint and site cover-age of Hospital campuses
2. Mental Health units are ideally located on Hospital campuses or on urban sites where linkages between the unit, the broader Hospital campus and community can be developed to mi gate against s gma sa on
3. Mental Health units are ideally designed to acheive built environments of high amenity featuring: direct access from clinical spaces to outdoor areas, high levels of daylight penetra on, good acous c a enua on and ease of wayfi nding
4. Wherever Mental Health units are developed as standalone buildings they are ideally designed as either a Stepped Courtyard or Radial Plan type
5. Wherever Mental Health units are designed with courtyards, these are ideally surrounded by residen al accom-moda on in a ‘single’ loaded corridor arrangement to maximise daylight penetra on
6. Mental Health units are ideally designed to facilitate direct access from indoor spaces to landscaped areas with-out the need for ‘managed’ solu ons which impact upon staff effi ciency and consumer percep ons of freedom
7. Mental Health units are ideally designed with disaggregated outdoor areas preferably linked to consumer bed-rooms or recrea on areas that promote individualised amenity
8. Mental Health units are ideally designed to incorporate sound a enua ng features through the use of sound absorbing materials and fi nishes resolved to a high standard architecturally
9. Mental Health units are ideally designed to include local materials and building tradi ons to assist in the cre-a onal of a ‘normal’ place
10. Mental Health units are designed to incorporate an -ligature fi xtures and fi ngs to a standard commensurate with an agreed safety management plan balancing amenity with risk
The following contacts were extremely helpful during the prepara on of and undertaking of this study tour:
Chris ne Hammarling, Director, Tengbom Architects, Chris [email protected]
Stefan Lundin, Director, White Architects, [email protected]
Joachim Staudt, Director, Huber Staudt Architekten, [email protected]
10
3.0 ProgrammeMonth Date Place Ins tute/ Organisa on to be visited
May 25 Melbourne- London Transit
May 26 London Arrival UK
May 27 London Visit Great Ormond Street Hospital CEO Dr Peter Steer
May 28 Cambridge Weekend- Rest Day
May 29 Cambridge Weekend- Rest Day
May 30 Cambridge- Stockholm Transit
May 31 Stockholm- Uppsala Uppsala Psychiatric Hospital
June 1 Stockholm Tengbom Architect- Chris ne Hammering
June 2 Stockholm White Architects- Stefan Lundin
June 3 Stockholm Gothenburg Ostra Psychiatry, Boras Psychiatry- Krister Nilsson, Cris na Caira
June 4 Stockholm-Oslo Transit
June 5 Oslo Weekend- Rest Day
June 6 Oslo Weekend- Rest Day
June 7 Oslo-Bergen Transit
June 8 Bergen Free day
June 9 Bergen Visit Origo Architects- Rikke Charlo e Sundt
June 10 Bergen- Copenhagen Transit
June 11 Copenhagen Weekend- Rest Day
June 12 Copenhagen Weekend- Rest Day
June 13 Copenhagen Visit Schmi / Hamer/ Lassen Architects - Kasper Heiberg Franden
June 14 Slagelse Architecture Design Centre
June 15 Copenhagen Visit Karlssonark Architects- Kristen Karlssonark
June 16 Copenhagen St Herlev Hospital, Poul Gernes
June 17 Copenhagen- Milan Transit- Visit Bosco Ver cale
June 18 Milan Weekend- Rest Day
June 19 Milan Weekend- Rest Day
June 20 Milan- Berlin Transit
June 21 Berlin Visit Hauber Staudt Architects- Joachim Staudt
June 22 Berlin- Friederichshafen Transit
June 23 Friederichshafen Reichenau, Friederichshafen Psychiatry Hospital- Ulrich Glaser
June 24 Friederichshafen- London Transit
June 25 London Weekend- Rest Day
June 26 London- Melbourne Transit
Opposite: Zentrum fur Psychiatrie Friedrichshafen by Huber Staudt Architkter (in Associa on with Baulinie Architekter)

11
SECTION 2
12
4.0 Site VisitsOutlined in this sec on are descrip ons of the six separate sites visited as part of this study. For each site visited, an earlier briefi ng was undertaken with the project architect at their respec ve offi ce either on the same day or on some day preceding the site visit. The strictest confi den ality protocols were followed on each site visit ensuring no consumer was photographed. Wherever possible, consumer refl ec ons on the success or otherwise of the built environment were sought on the site visit along with my key impressions of the site recorded. Inters ngly, in almost all instances, the visits presented an opportunity for the design architect to visit the site accompanied by another architect for the fi rst me some me a er occupa on.
4.1 Uppsala Psychiatry, Uppsala, (Sweden) by Tengbom Architects
Project Descrip onThe Uppsala Psychiatry project is, “Based on the vision of an environment that focuses on the pa ent and demys -fying mental illness ... a building where transparency and integra on are central value.” The 34,000sqm nine level building located on the Uppsala Hospital site, some 1hour’s drive from central Stockholm, collocates all district and regional acute in and out-pa ent mental health services with a dedicated mental health research and emergency care centre.
Designed by Tengbom Architects under the design direc on of Director Chris ne Hammarling and opened in 2013, Uppsala Psychiatry includes 100 beds arranged in 4 accommoda on levels subdivided into 2 x 13 bed pods each shar-ing common administra ve and support spaces. Each accommoda on fl oor includes separately accessed outpa ent consul ng rooms incorpora ng day program and bedroom expansion capacity.
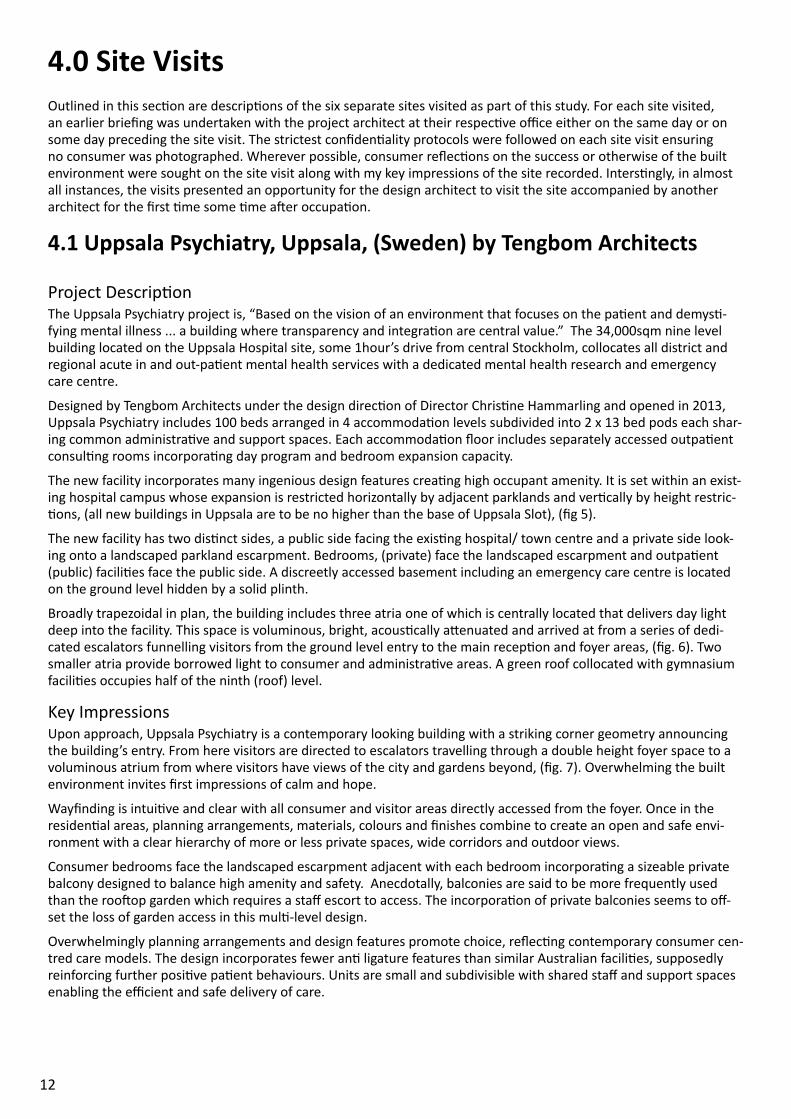
The new facility incorporates many ingenious design features crea ng high occupant amenity. It is set within an exist-ing hospital campus whose expansion is restricted horizontally by adjacent parklands and ver cally by height restric- ons, (all new buildings in Uppsala are to be no higher than the base of Uppsala Slot), (fi g 5).
The new facility has two dis nct sides, a public side facing the exis ng hospital/ town centre and a private side look-ing onto a landscaped parkland escarpment. Bedrooms, (private) face the landscaped escarpment and outpa ent (public) facili es face the public side. A discreetly accessed basement including an emergency care centre is located on the ground level hidden by a solid plinth.
Broadly trapezoidal in plan, the building includes three atria one of which is centrally located that delivers day light deep into the facility. This space is voluminous, bright, acous cally a enuated and arrived at from a series of dedi-cated escalators funnelling visitors from the ground level entry to the main recep on and foyer areas, (fi g. 6). Two smaller atria provide borrowed light to consumer and administra ve areas. A green roof collocated with gymnasium facili es occupies half of the ninth (roof) level.
Key ImpressionsUpon approach, Uppsala Psychiatry is a contemporary looking building with a striking corner geometry announcing the building’s entry. From here visitors are directed to escalators travelling through a double height foyer space to a voluminous atrium from where visitors have views of the city and gardens beyond, (fi g. 7). Overwhelming the built environment invites fi rst impressions of calm and hope.
Wayfi nding is intui ve and clear with all consumer and visitor areas directly accessed from the foyer. Once in the residen al areas, planning arrangements, materials, colours and fi nishes combine to create an open and safe envi-ronment with a clear hierarchy of more or less private spaces, wide corridors and outdoor views.
Consumer bedrooms face the landscaped escarpment adjacent with each bedroom incorpora ng a sizeable private balcony designed to balance high amenity and safety. Anecdotally, balconies are said to be more frequently used than the roo op garden which requires a staff escort to access. The incorpora on of private balconies seems to off -set the loss of garden access in this mul -level design.
Overwhelmingly planning arrangements and design features promote choice, refl ec ng contemporary consumer cen-tred care models. The design incorporates fewer an ligature features than similar Australian facili es, supposedly reinforcing further posi ve pa ent behaviours. Units are small and subdivisible with shared staff and support spaces enabling the effi cient and safe delivery of care.
13
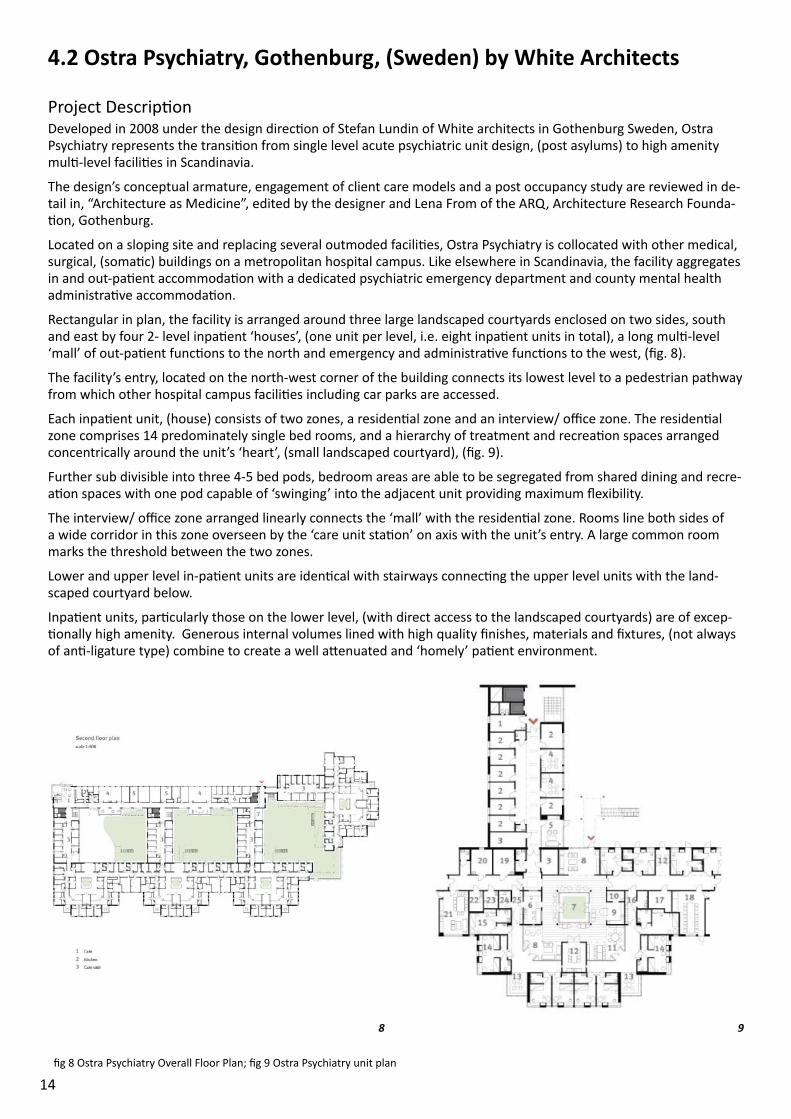
Staff and consumer feedback indicates scope for further improvement including incorpora ng ensuites accessible directly from pa ent bedrooms (i.e. not from corridor) and including more ‘sensory’ in lieu of ‘seclusion’ rooms. No incidences of self-harm have been recorded.
Staff also note that the colloca on of in and out pa ent staff in the one facility has led to improved communica on between care units. The outcomes of this is said to be directly contribu ng to lengths of stay reducing from 21 to 7 days a er moving into the new facility.
Key Lessons Learnt• Excellent site selec on enabling the development of a high amenity design response incorpora ng views of land-
scape and nature whilst providing access to all other Hospital services
• Drama c reduc on in the pa ent length of stay resul ng from the colloca on of in and outpa ent services, (rela- ve to the previous disaggregated Uppsala Psychiatry services)
• Reduc on in the incidence of aggressive behaviours said to be directly a ributable to environmental features including wider than normal corridors
• High levels of pa ent amenity with a hierarchy of pa ent indoor/ outdoor spaces including private balconies provided to each bedroom and collocated roof top garden and gymnasium
• Subdivisible and small (12-13 bed) residen al units providing fl exibility for the segrega on of pa ent cohorts
5
6 7
fi g 5 Uppsala Psychiatry aerial site view; fi g 6 Uppsala Psychiatry entry ; fi g 7 Uppsala Psychiatry arrival sequence
14
4.2 Ostra Psychiatry, Gothenburg, (Sweden) by White Architects
Project Descrip onDeveloped in 2008 under the design direc on of Stefan Lundin of White architects in Gothenburg Sweden, Ostra Psychiatry represents the transi on from single level acute psychiatric unit design, (post asylums) to high amenity mul -level facili es in Scandinavia.
The design’s conceptual armature, engagement of client care models and a post occupancy study are reviewed in de-tail in, “Architecture as Medicine”, edited by the designer and Lena From of the ARQ, Architecture Research Founda- on, Gothenburg.
Located on a sloping site and replacing several outmoded facili es, Ostra Psychiatry is collocated with other medical, surgical, (soma c) buildings on a metropolitan hospital campus. Like elsewhere in Scandinavia, the facility aggregates in and out-pa ent accommoda on with a dedicated psychiatric emergency department and county mental health administra ve accommoda on.
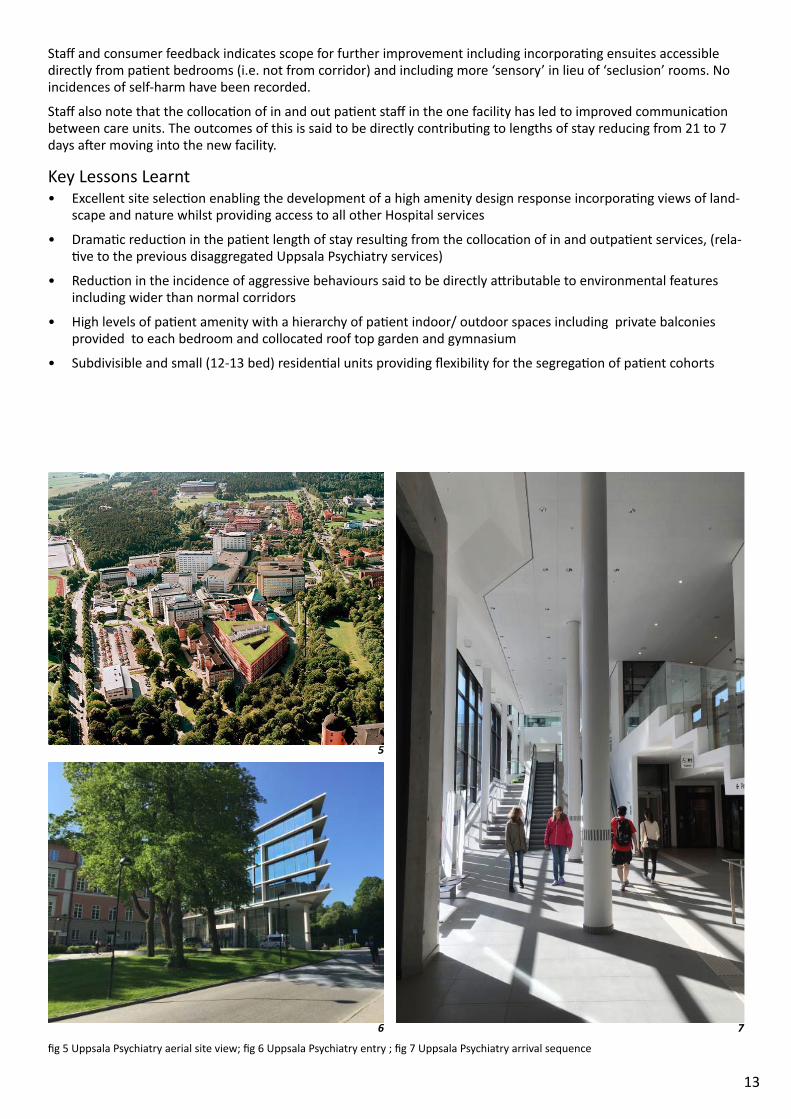
Rectangular in plan, the facility is arranged around three large landscaped courtyards enclosed on two sides, south and east by four 2- level inpa ent ‘houses’, (one unit per level, i.e. eight inpa ent units in total), a long mul -level ‘mall’ of out-pa ent func ons to the north and emergency and administra ve func ons to the west, (fi g. 8).
The facility’s entry, located on the north-west corner of the building connects its lowest level to a pedestrian pathway from which other hospital campus facili es including car parks are accessed.
Each inpa ent unit, (house) consists of two zones, a residen al zone and an interview/ offi ce zone. The residen al zone comprises 14 predominately single bed rooms, and a hierarchy of treatment and recrea on spaces arranged concentrically around the unit’s ‘heart’, (small landscaped courtyard), (fi g. 9).
Further sub divisible into three 4-5 bed pods, bedroom areas are able to be segregated from shared dining and recre-a on spaces with one pod capable of ‘swinging’ into the adjacent unit providing maximum fl exibility.
The interview/ offi ce zone arranged linearly connects the ‘mall’ with the residen al zone. Rooms line both sides of a wide corridor in this zone overseen by the ‘care unit sta on’ on axis with the unit’s entry. A large common room marks the threshold between the two zones.
Lower and upper level in-pa ent units are iden cal with stairways connec ng the upper level units with the land-scaped courtyard below.
Inpa ent units, par cularly those on the lower level, (with direct access to the landscaped courtyards) are of excep- onally high amenity. Generous internal volumes lined with high quality fi nishes, materials and fi xtures, (not always
of an -ligature type) combine to create a well a enuated and ‘homely’ pa ent environment.
8 9
fi g 8 Ostra Psychiatry Overall Floor Plan; fi g 9 Ostra Psychiatry unit plan
15
Key ImpressionsThe ini al impression of Ostra Psychiatry is of a signifi cantly scaled and almost foreboding building; an impression ac-centuated given the building’s entrance is at the bo om corner of a sloping site, (fi g.10).
The foyer albeit generously propor oned and carefully resolved architecturally gives few intui ve way fi nding cues and is not staff ed. The result is a disorienta ng and stark arrivals experience made more diffi cult by the main public circula on spine, the ‘mall’, being two levels above.
Once arrived at, the ‘mall’ is long, (possibly too long) and although bathed in daylight feels impersonal and ins tu- onal. Screening incorporated to block overseeing from here to the landscaped courtyards is being redeveloped and
likely to result in a reduc on of daylight penetra on.
Inpa ent unit entries are not clearly signposted along the ‘mall’ making them diffi cult to fi nd. Once accessed the entry experience is uninvi ng arriving as one does to the interview/ offi ce zone with no natural daylight and overseen by a glazed staff base, (fi g.11).
An a empt to introduce day light into this space, (at the threshold between this and the residen al zone) was lost when an open consumer common room with garden views was reconfi gured into a staff room. The a endant privacy requirements resulted in the view (and daylight) being blocked.
Stepping into the residen al zone, the overwhelming sense is of calm. The many recrea onal and dining spaces ar-ranged around the ‘heart’ feel invi ng, in mate and comfortable. Ceilings are high, fl ooring of a natural parquetry and ligh ng indirect crea ng a dignifi ed ‘homely’ environment.
Bedroom pods, accessed from an elegantly propor oned and detailed ‘enclosed veranda’ (fi g. 12) consist of wide cor-ridors leading to a series of well confi gured bedrooms- some of which have direct garden access.
An -ligature fi xtures and fi ngs are used sparingly throughout so as not to engender an ins tu onal ambience al-though some anecdotal evidence exists that self-harm incidents have occurred.
The amenity of pa ent areas is high, par cularly for those pa ents able to access the landscaped courtyards, (ground level units). The courtyards are generous in scale, variegated and designed to maximise sunlight, (fi g. 13). Access to these spaces from upper units is less successful however, (fi g.14).
Developed as an extruded plan, Ostra Psychiatry lacks the architectural complexity, (evidenced elsewhere in Scan-dinavia and Europe) to sa sfactorily balance pa ent amenity with equitable access. For example, pa ents in upper level units do not have direct access to a landscaped courtyard or ‘heart’.
Stairs connec ng the upper level residen al units with the landscape courtyards require a ‘managed’ solu on; a staff member needs to either accompany the consumer to the courtyard or stand at the top of the stair to oversee the pa ent’s movements whilst in the courtyard. This overt management diminishes, it is said, a consumer’s percep on of freedom whilst impac ng upon staff effi ciency.
Key Lessons Learnt• Ostra Psychiatry is amongst the fi rst psychiatric unit designs of the contemporary era that sets out to achieve
high amenity in support of recovery focussed care models over mul ple levels providing excellent evidence for future projects
• The arrivals and overall way fi nding experiences seem ins tu onal and incongruent, even if generously scaled and highly detailed
• Sophis cated in pa ent unit design, par cularly in the residen al zone with high levels of consumer amenity. The interview and offi ce zone, (ac ng as arrival experience) however is underwhelming
• Well-conceived and detailed landscaped areas par cularly for those consumers with direct access. Less success-ful for upper level units impac ng upon consumer percep ons of freedom and staff effi ciency

16
10 11
12 13
14 15
fi g 10 Facility entry; fi g 11 Unit entry; fi g 12 Enclosed verandah leading to bedrooms, fi g 13 Unit courtyard; fi g 14 Upper level courtyard access; fi g 15 from le , Nurse Unit Manager, Stefano Scalzo and Elin Ri mark of White Architects
17
4.3 Kronstad Psychiatric Centre, Bergen (Norway) by Origo Architects
Project Descrip onLocated in a low socio economic neighbourhood on the outskirts of Bergen, (Norway) Kronstad Psychiatric Centre, designed by Origo Arkitektgruppe’s Rikke Charlo e Sundt represents arguably the future of high amenity mental health units developed over mul ple levels.
As per elsewhere in Scandinavia, Kronstad Psychiatric Centre provides both in and out pa ent accommoda on in a purpose built facility that also includes a dedicated psychiatric emergency department and county level mental health administra on.
Unlike elsewhere however, Kronstad Psychiatric Centre is a stand-alone facility detached from an acute hospital set- ng, (20minutes away). The new facility is located in a harsh inner urban se ng between a major city arterial and
sports grounds with drama c views to Mount Ulrichen.
Developed over seven levels, the new facility incorporates nine roof gardens confi gured over mul ple levels so as to directly serve diff erent residen al, ambulatory and administra ve func ons. These provide a ‘so ’ heart to a building with a ‘hard’ or fortress like exterior designed in direct response to the harsh urban context.
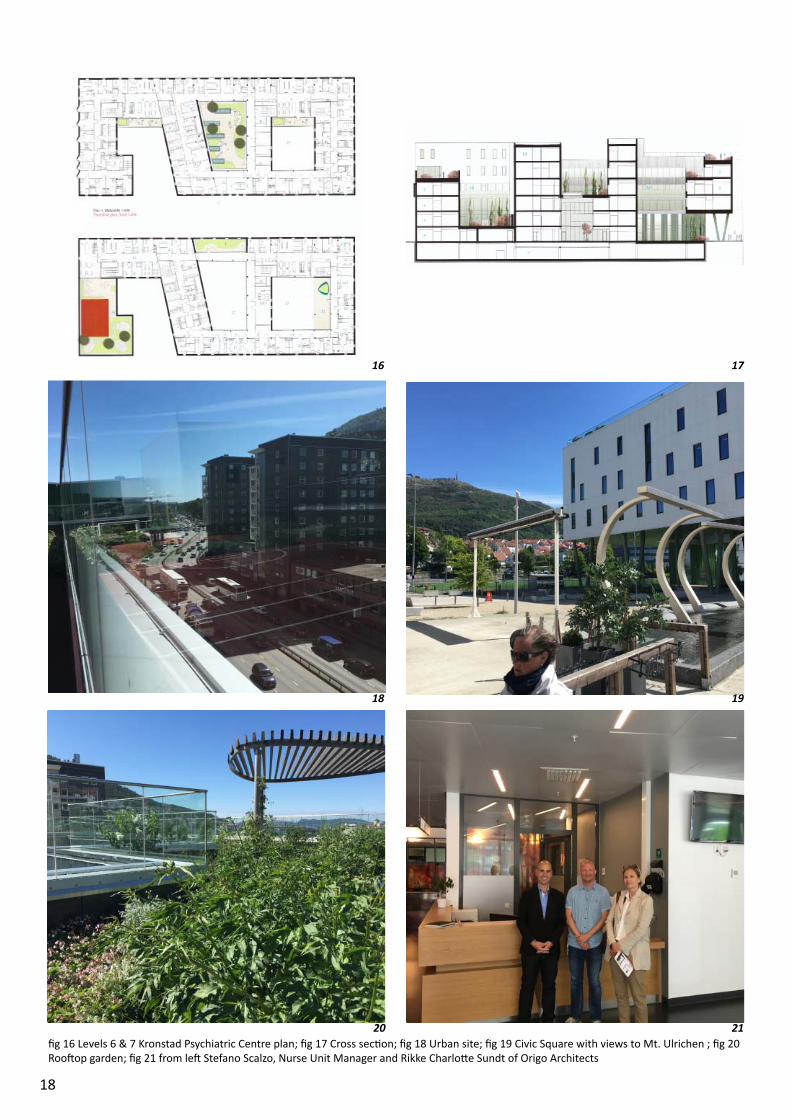
The building’s public func ons are located on the ground and upper ground levels within a permeable ‘green’ podium set back from the site’s northern edge to create a civic square with views to the landscape beyond. This civic gesture serves to normalise the introduc on of a Psychiatric Centre into a residen al area.
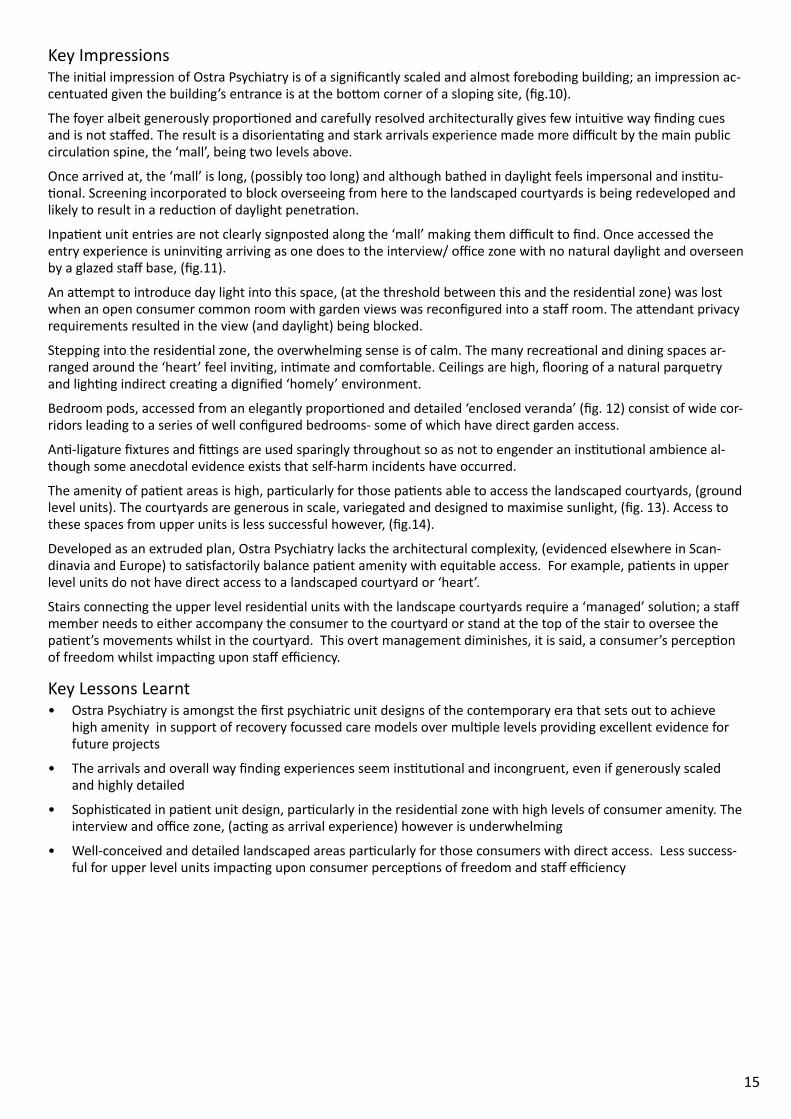
The Centre’s residen al accommoda on is located in a ‘white’ box ar culated with slit windows that rests on top of the green podium. The box’s external solidity gives way to a narrow plan that wraps its way around several courtyard spaces over mul ple levels crea ng a formal complexity only evident from the ‘sports fi eld’ side of the building, (fi gs. 16, 17).
Internally the building is excep onally well resolved architecturally with views through the facility carefully balanced with the provision of day light penetra on and the maintenance of privacy. Materials are carefully selected to a enu-ate noise with fi xtures and fi ngs chosen to promote safety without being overtly of an -ligature type.
Two 16 bed residen al units, further subdivisible into pods of 8 (and 4) include 100% single bedrooms that overlook the sports fi elds adjacent. These include ‘nested’ ensuites and are supported by a hierarchy of recrea on, interview and ac vity spaces capable of ‘swinging’ between pods and sub pods. Each unit has direct access to a landscaped area that includes only a medium height balustrade, (2m).
The top most occupiable level includes a community day stay unit, (Flexible Asser ve Treatment) with mul ple ac v-ity and interview rooms opening onto a vast roof top terrace with spectacular views to the sports fi elds adjacent and Mt Ulrichen beyond.
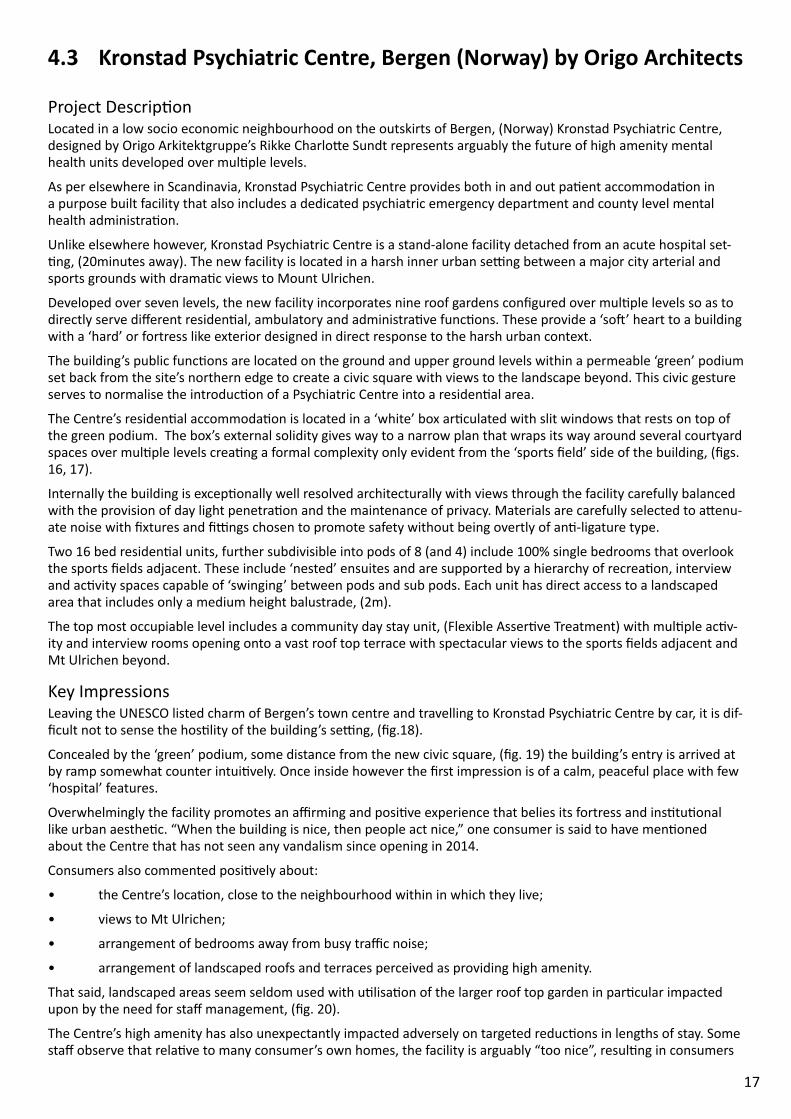
Key ImpressionsLeaving the UNESCO listed charm of Bergen’s town centre and travelling to Kronstad Psychiatric Centre by car, it is dif-fi cult not to sense the hos lity of the building’s se ng, (fi g.18).
Concealed by the ‘green’ podium, some distance from the new civic square, (fi g. 19) the building’s entry is arrived at by ramp somewhat counter intui vely. Once inside however the fi rst impression is of a calm, peaceful place with few ‘hospital’ features.
Overwhelmingly the facility promotes an affi rming and posi ve experience that belies its fortress and ins tu onal like urban aesthe c. “When the building is nice, then people act nice,” one consumer is said to have men oned about the Centre that has not seen any vandalism since opening in 2014.
Consumers also commented posi vely about:
• the Centre’s loca on, close to the neighbourhood within in which they live;
• views to Mt Ulrichen;
• arrangement of bedrooms away from busy traffi c noise;
• arrangement of landscaped roofs and terraces perceived as providing high amenity.
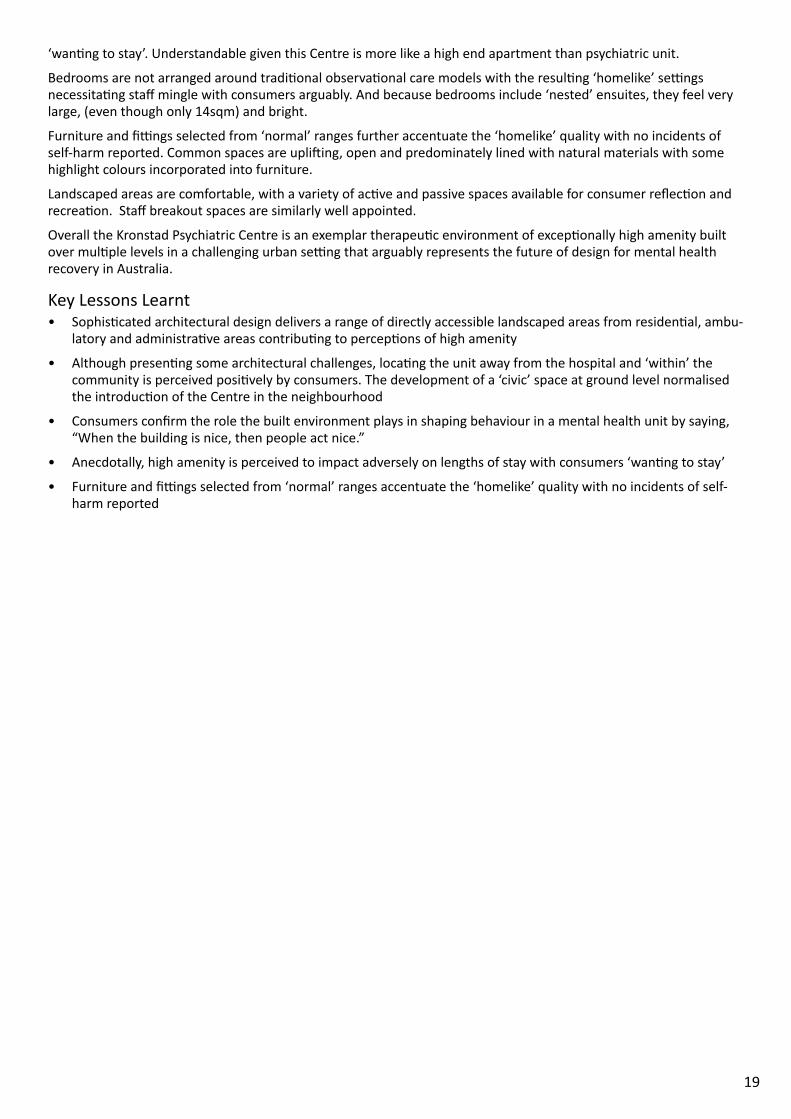
That said, landscaped areas seem seldom used with u lisa on of the larger roof top garden in par cular impacted upon by the need for staff management, (fi g. 20).
The Centre’s high amenity has also unexpectantly impacted adversely on targeted reduc ons in lengths of stay. Some staff observe that rela ve to many consumer’s own homes, the facility is arguably “too nice”, resul ng in consumers
18
16 17
18 19
20 21fi g 16 Levels 6 & 7 Kronstad Psychiatric Centre plan; fi g 17 Cross sec on; fi g 18 Urban site; fi g 19 Civic Square with views to Mt. Ulrichen ; fi g 20 Roo op garden; fi g 21 from le Stefano Scalzo, Nurse Unit Manager and Rikke Charlo e Sundt of Origo Architects
19
‘wan ng to stay’. Understandable given this Centre is more like a high end apartment than psychiatric unit.
Bedrooms are not arranged around tradi onal observa onal care models with the resul ng ‘homelike’ se ngs necessita ng staff mingle with consumers arguably. And because bedrooms include ‘nested’ ensuites, they feel very large, (even though only 14sqm) and bright.
Furniture and fi ngs selected from ‘normal’ ranges further accentuate the ‘homelike’ quality with no incidents of self-harm reported. Common spaces are upli ing, open and predominately lined with natural materials with some highlight colours incorporated into furniture.
Landscaped areas are comfortable, with a variety of ac ve and passive spaces available for consumer refl ec on and recrea on. Staff breakout spaces are similarly well appointed.
Overall the Kronstad Psychiatric Centre is an exemplar therapeu c environment of excep onally high amenity built over mul ple levels in a challenging urban se ng that arguably represents the future of design for mental health recovery in Australia.
Key Lessons Learnt• Sophis cated architectural design delivers a range of directly accessible landscaped areas from residen al, ambu-
latory and administra ve areas contribu ng to percep ons of high amenity
• Although presen ng some architectural challenges, loca ng the unit away from the hospital and ‘within’ the community is perceived posi vely by consumers. The development of a ‘civic’ space at ground level normalised the introduc on of the Centre in the neighbourhood
• Consumers confi rm the role the built environment plays in shaping behaviour in a mental health unit by saying, “When the building is nice, then people act nice.”
• Anecdotally, high amenity is perceived to impact adversely on lengths of stay with consumers ‘wan ng to stay’
• Furniture and fi ngs selected from ‘normal’ ranges accentuate the ‘homelike’ quality with no incidents of self-harm reported
20
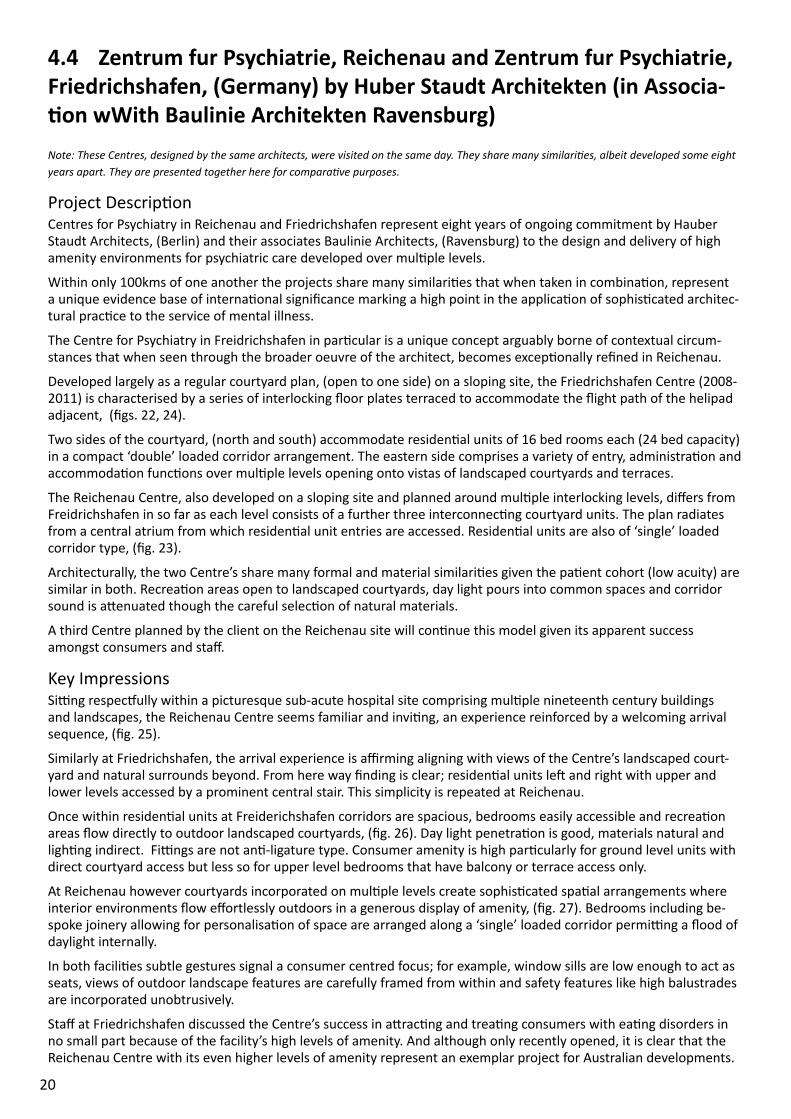
4.4 Zentrum fur Psychiatrie, Reichenau and Zentrum fur Psychiatrie, Friedrichshafen, (Germany) by Huber Staudt Architekten (in Associa- on wWith Baulinie Architekten Ravensburg)
Note: These Centres, designed by the same architects, were visited on the same day. They share many similari es, albeit developed some eight years apart. They are presented together here for compara ve purposes.
Project Descrip onCentres for Psychiatry in Reichenau and Friedrichshafen represent eight years of ongoing commitment by Hauber Staudt Architects, (Berlin) and their associates Baulinie Architects, (Ravensburg) to the design and delivery of high amenity environments for psychiatric care developed over mul ple levels.
Within only 100kms of one another the projects share many similari es that when taken in combina on, represent a unique evidence base of interna onal signifi cance marking a high point in the applica on of sophis cated architec-tural prac ce to the service of mental illness.
The Centre for Psychiatry in Freidrichshafen in par cular is a unique concept arguably borne of contextual circum-stances that when seen through the broader oeuvre of the architect, becomes excep onally refi ned in Reichenau.
Developed largely as a regular courtyard plan, (open to one side) on a sloping site, the Friedrichshafen Centre (2008-2011) is characterised by a series of interlocking fl oor plates terraced to accommodate the fl ight path of the helipad adjacent, (fi gs. 22, 24).
Two sides of the courtyard, (north and south) accommodate residen al units of 16 bed rooms each (24 bed capacity) in a compact ‘double’ loaded corridor arrangement. The eastern side comprises a variety of entry, administra on and accommoda on func ons over mul ple levels opening onto vistas of landscaped courtyards and terraces.
The Reichenau Centre, also developed on a sloping site and planned around mul ple interlocking levels, diff ers from Freidrichshafen in so far as each level consists of a further three interconnec ng courtyard units. The plan radiates from a central atrium from which residen al unit entries are accessed. Residen al units are also of ‘single’ loaded corridor type, (fi g. 23).
Architecturally, the two Centre’s share many formal and material similari es given the pa ent cohort (low acuity) are similar in both. Recrea on areas open to landscaped courtyards, day light pours into common spaces and corridor sound is a enuated though the careful selec on of natural materials.
A third Centre planned by the client on the Reichenau site will con nue this model given its apparent success amongst consumers and staff .
Key ImpressionsSi ng respec ully within a picturesque sub-acute hospital site comprising mul ple nineteenth century buildings and landscapes, the Reichenau Centre seems familiar and invi ng, an experience reinforced by a welcoming arrival sequence, (fi g. 25).
Similarly at Friedrichshafen, the arrival experience is affi rming aligning with views of the Centre’s landscaped court-yard and natural surrounds beyond. From here way fi nding is clear; residen al units le and right with upper and lower levels accessed by a prominent central stair. This simplicity is repeated at Reichenau.
Once within residen al units at Freiderichshafen corridors are spacious, bedrooms easily accessible and recrea on areas fl ow directly to outdoor landscaped courtyards, (fi g. 26). Day light penetra on is good, materials natural and ligh ng indirect. Fi ngs are not an -ligature type. Consumer amenity is high par cularly for ground level units with direct courtyard access but less so for upper level bedrooms that have balcony or terrace access only.
At Reichenau however courtyards incorporated on mul ple levels create sophis cated spa al arrangements where interior environments fl ow eff ortlessly outdoors in a generous display of amenity, (fi g. 27). Bedrooms including be-spoke joinery allowing for personalisa on of space are arranged along a ‘single’ loaded corridor permi ng a fl ood of daylight internally.
In both facili es subtle gestures signal a consumer centred focus; for example, window sills are low enough to act as seats, views of outdoor landscape features are carefully framed from within and safety features like high balustrades are incorporated unobtrusively.
Staff at Friedrichshafen discussed the Centre’s success in a rac ng and trea ng consumers with ea ng disorders in no small part because of the facility’s high levels of amenity. And although only recently opened, it is clear that the Reichenau Centre with its even higher levels of amenity represent an exemplar project for Australian developments.

21
Key Lessons Learnt• The arrival experience must be affi rming and a posi ve experience, preferably with views onto nature
• Landscaped courtyards arranged across mul ple levels provide greater amenity than balcony and terrace spaces
• ‘Single’ rather than ‘double’ loaded corridors allow for greater daylight penetra on and amenity
• Detailed features such as window seat, views out and unobtrusive safety features signal a consumer focus
22 23
24 25
26 27fi g 22 Friedrichshafen plan; fi g 23 Reichenau Plan; fi g 24 Building form ‘stepped’ to accommodate helipad; fi g 25 Reichenau arrival; fi g 26 Inter-nal environment; fi g 27 Sophis cated spa al arrangements
22
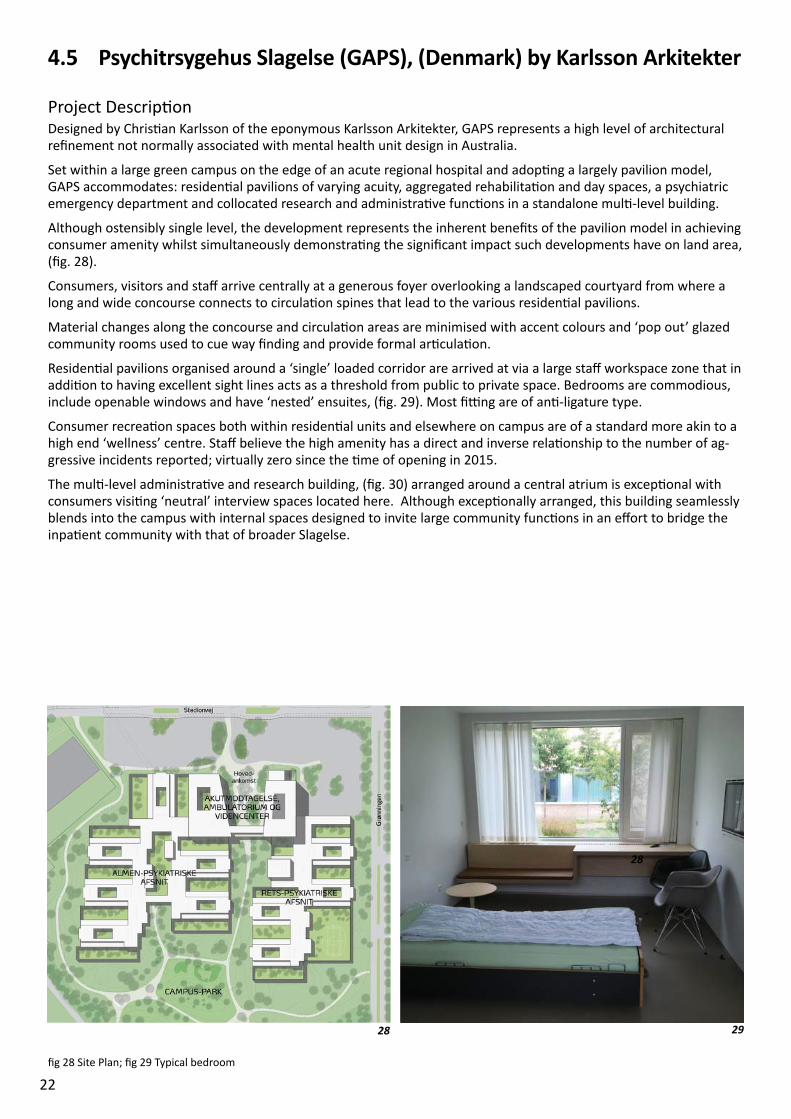
4.5 Psychitrsygehus Slagelse (GAPS), (Denmark) by Karlsson Arkitekter
Project Descrip onDesigned by Chris an Karlsson of the eponymous Karlsson Arkitekter, GAPS represents a high level of architectural refi nement not normally associated with mental health unit design in Australia.
Set within a large green campus on the edge of an acute regional hospital and adop ng a largely pavilion model, GAPS accommodates: residen al pavilions of varying acuity, aggregated rehabilita on and day spaces, a psychiatric emergency department and collocated research and administra ve func ons in a standalone mul -level building.
Although ostensibly single level, the development represents the inherent benefi ts of the pavilion model in achieving consumer amenity whilst simultaneously demonstra ng the signifi cant impact such developments have on land area, (fi g. 28).
Consumers, visitors and staff arrive centrally at a generous foyer overlooking a landscaped courtyard from where a long and wide concourse connects to circula on spines that lead to the various residen al pavilions.
Material changes along the concourse and circula on areas are minimised with accent colours and ‘pop out’ glazed community rooms used to cue way fi nding and provide formal ar cula on.
Residen al pavilions organised around a ‘single’ loaded corridor are arrived at via a large staff workspace zone that in addi on to having excellent sight lines acts as a threshold from public to private space. Bedrooms are commodious, include openable windows and have ‘nested’ ensuites, (fi g. 29). Most fi ng are of an -ligature type.
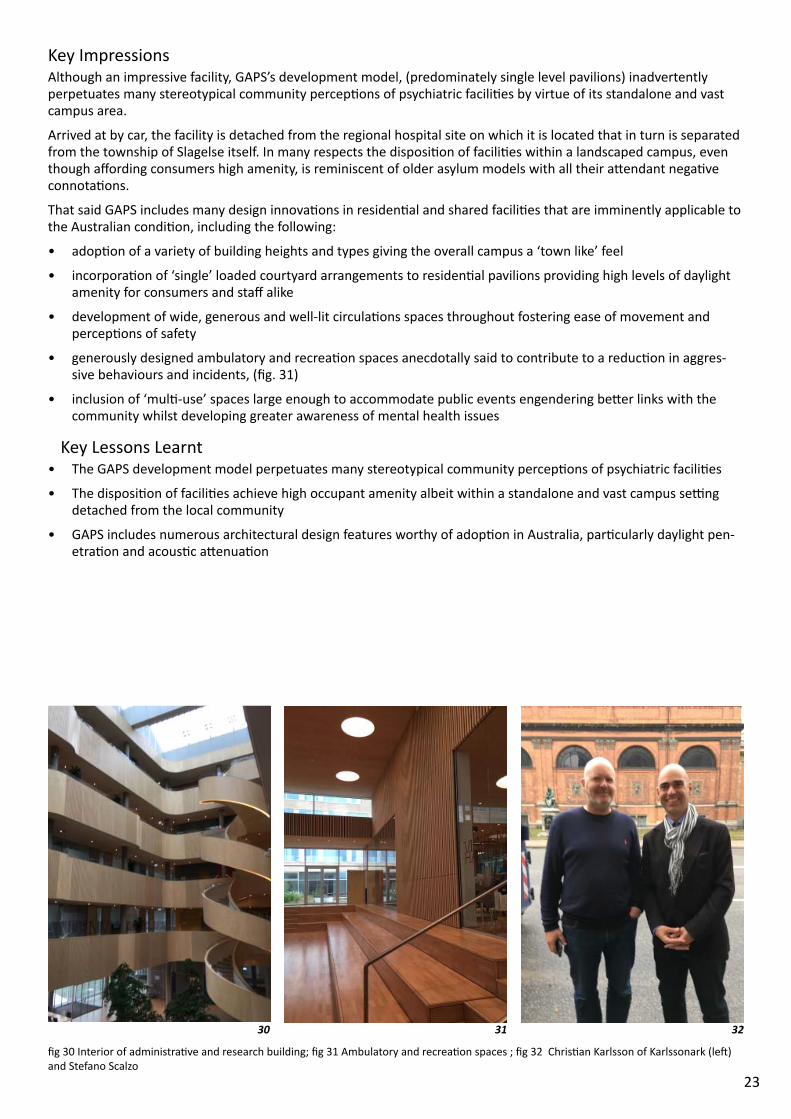
Consumer recrea on spaces both within residen al units and elsewhere on campus are of a standard more akin to a high end ‘wellness’ centre. Staff believe the high amenity has a direct and inverse rela onship to the number of ag-gressive incidents reported; virtually zero since the me of opening in 2015.
The mul -level administra ve and research building, (fi g. 30) arranged around a central atrium is excep onal with consumers visi ng ‘neutral’ interview spaces located here. Although excep onally arranged, this building seamlessly blends into the campus with internal spaces designed to invite large community func ons in an eff ort to bridge the inpa ent community with that of broader Slagelse.
28
28
29
fi g 28 Site Plan; fi g 29 Typical bedroom
23
Key Impressions Although an impressive facility, GAPS’s development model, (predominately single level pavilions) inadvertently perpetuates many stereotypical community percep ons of psychiatric facili es by virtue of its standalone and vast campus area.
Arrived at by car, the facility is detached from the regional hospital site on which it is located that in turn is separated from the township of Slagelse itself. In many respects the disposi on of facili es within a landscaped campus, even though aff ording consumers high amenity, is reminiscent of older asylum models with all their a endant nega ve connota ons.
That said GAPS includes many design innova ons in residen al and shared facili es that are imminently applicable to the Australian condi on, including the following:
• adop on of a variety of building heights and types giving the overall campus a ‘town like’ feel
• incorpora on of ‘single’ loaded courtyard arrangements to residen al pavilions providing high levels of daylight amenity for consumers and staff alike
• development of wide, generous and well-lit circula ons spaces throughout fostering ease of movement and percep ons of safety
• generously designed ambulatory and recrea on spaces anecdotally said to contribute to a reduc on in aggres-sive behaviours and incidents, (fi g. 31)
• inclusion of ‘mul -use’ spaces large enough to accommodate public events engendering be er links with the community whilst developing greater awareness of mental health issues
Key Lessons Learnt• The GAPS development model perpetuates many stereotypical community percep ons of psychiatric facili es
• The disposi on of facili es achieve high occupant amenity albeit within a standalone and vast campus se ng detached from the local community
• GAPS includes numerous architectural design features worthy of adop on in Australia, par cularly daylight pen-etra on and acous c a enua on
30 31 32
fi g 30 Interior of administra ve and research building; fi g 31 Ambulatory and recrea on spaces ; fi g 32 Chris an Karlsson of Karlssonark (le ) and Stefano Scalzo
24
5.0 On the drawing boards - the next wave of designThe following projects represent the future of mental helath unit design in Scandinavia. Each builds on design trends seen in the earlier site visits whilst presen ng some new design innova ons directly applicable to the Australian context.
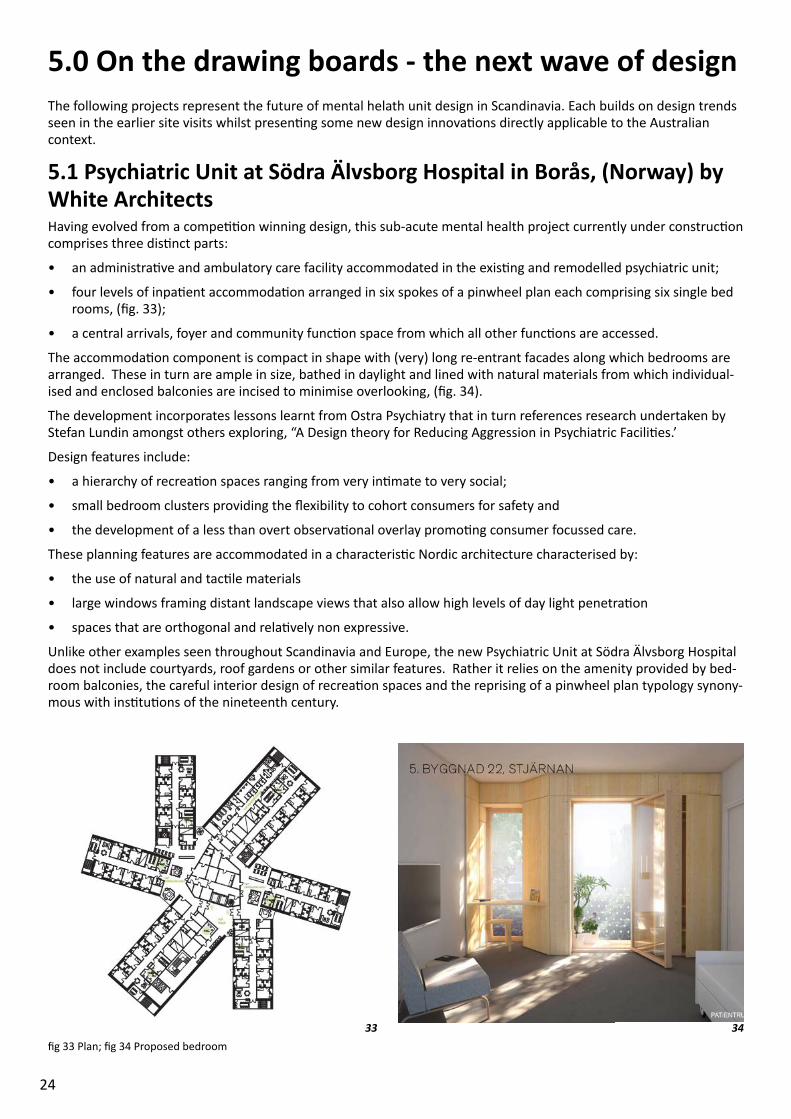
5.1 Psychiatric Unit at Södra Älvsborg Hospital in Borås, (Norway) by White Architects Having evolved from a compe on winning design, this sub-acute mental health project currently under construc on comprises three dis nct parts:
• an administra ve and ambulatory care facility accommodated in the exis ng and remodelled psychiatric unit;
• four levels of inpa ent accommoda on arranged in six spokes of a pinwheel plan each comprising six single bed rooms, (fi g. 33);
• a central arrivals, foyer and community func on space from which all other func ons are accessed.
The accommoda on component is compact in shape with (very) long re-entrant facades along which bedrooms are arranged. These in turn are ample in size, bathed in daylight and lined with natural materials from which individual-ised and enclosed balconies are incised to minimise overlooking, (fi g. 34).
The development incorporates lessons learnt from Ostra Psychiatry that in turn references research undertaken by Stefan Lundin amongst others exploring, “A Design theory for Reducing Aggression in Psychiatric Facili es.’
Design features include:
• a hierarchy of recrea on spaces ranging from very in mate to very social;
• small bedroom clusters providing the fl exibility to cohort consumers for safety and
• the development of a less than overt observa onal overlay promo ng consumer focussed care.
These planning features are accommodated in a characteris c Nordic architecture characterised by:
• the use of natural and tac le materials
• large windows framing distant landscape views that also allow high levels of day light penetra on
• spaces that are orthogonal and rela vely non expressive.
Unlike other examples seen throughout Scandinavia and Europe, the new Psychiatric Unit at Södra Älvsborg Hospital does not include courtyards, roof gardens or other similar features. Rather it relies on the amenity provided by bed-room balconies, the careful interior design of recrea on spaces and the reprising of a pinwheel plan typology synony-mous with ins tu ons of the nineteenth century.
33 34fi g 33 Plan; fi g 34 Proposed bedroom
25
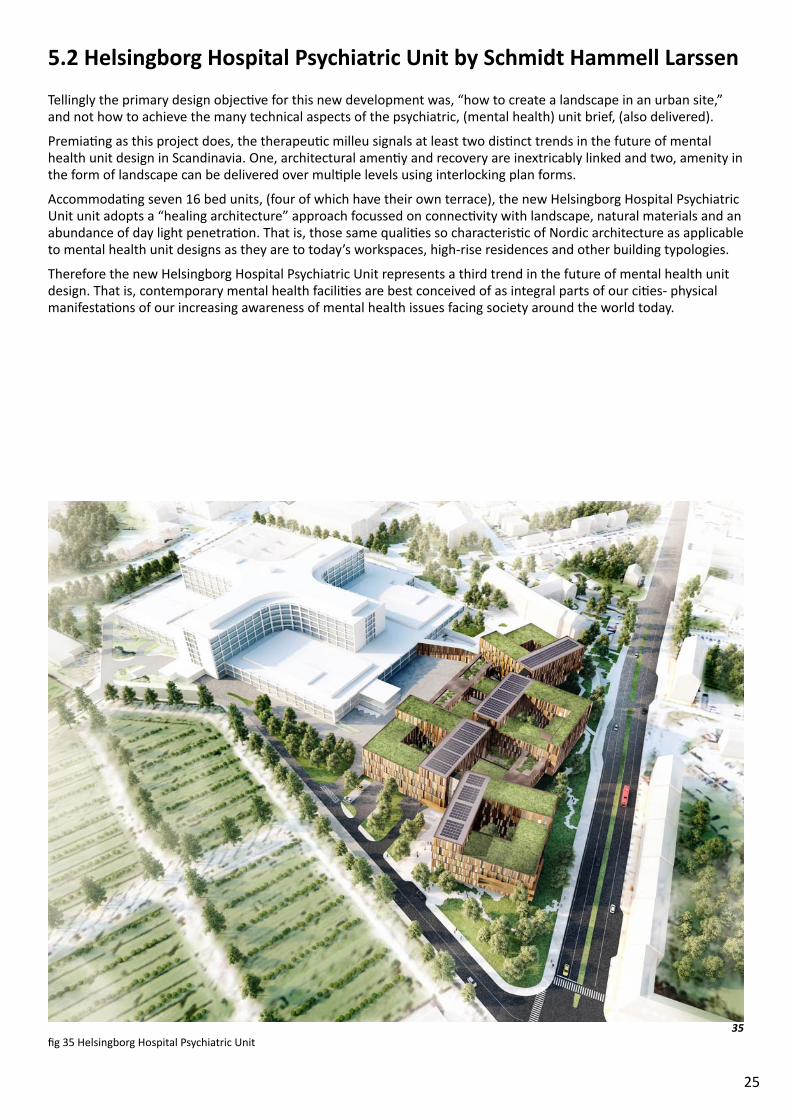
5.2 Helsingborg Hospital Psychiatric Unit by Schmidt Hammell Larssen Tellingly the primary design objec ve for this new development was, “how to create a landscape in an urban site,” and not how to achieve the many technical aspects of the psychiatric, (mental health) unit brief, (also delivered).
Premia ng as this project does, the therapeu c milleu signals at least two dis nct trends in the future of mental health unit design in Scandinavia. One, architectural amen y and recovery are inextricably linked and two, amenity in the form of landscape can be delivered over mul ple levels using interlocking plan forms.
Accommoda ng seven 16 bed units, (four of which have their own terrace), the new Helsingborg Hospital Psychiatric Unit unit adopts a “healing architecture” approach focussed on connec vity with landscape, natural materials and an abundance of day light penetra on. That is, those same quali es so characteris c of Nordic architecture as applicable to mental health unit designs as they are to today’s workspaces, high-rise residences and other building typologies.
Therefore the new Helsingborg Hospital Psychiatric Unit represents a third trend in the future of mental health unit design. That is, contemporary mental health facili es are best conceived of as integral parts of our ci es- physical manifesta ons of our increasing awareness of mental health issues facing society around the world today.
35fi g 35 Helsingborg Hospital Psychiatric Unit
26
6.0 In Support of ChangeAlthough the site visits described in the previous sec on formed the backbone of this study, other interviews and experiences made possible by the Churchill Fellowship, helped to shape a broader understanding of the issues sur-rounding society’s a tudes toward mental health and the concepts informing the design of contemporary mental health facili es.
6.1 Dinner with Stefan Lundin and Peter FrostStefan Lundin, White Architects and Peter Frost, ar s c professor at Chalmers University, Gothenburg con nue to shape the intellectual dialogue informing the design of today’s healthcare se ngs in Sweden.
Key themes discussed include:
• Ostra Psychiatry as exemplary of a renascent awareness of architecture’s capacity to assist recovery from a men-tal illness
• The important role architectural prac ce led research plays in informing the evolu on of mental health unit designs
• Consulta on strategies for design phases that foster evidence sharing and dialogue amongst cross disciplinary groups whilst allowing architectural responses to evolve itera vely
• Contemporary procurement methodologies and their impact on the consulta on strategies described above
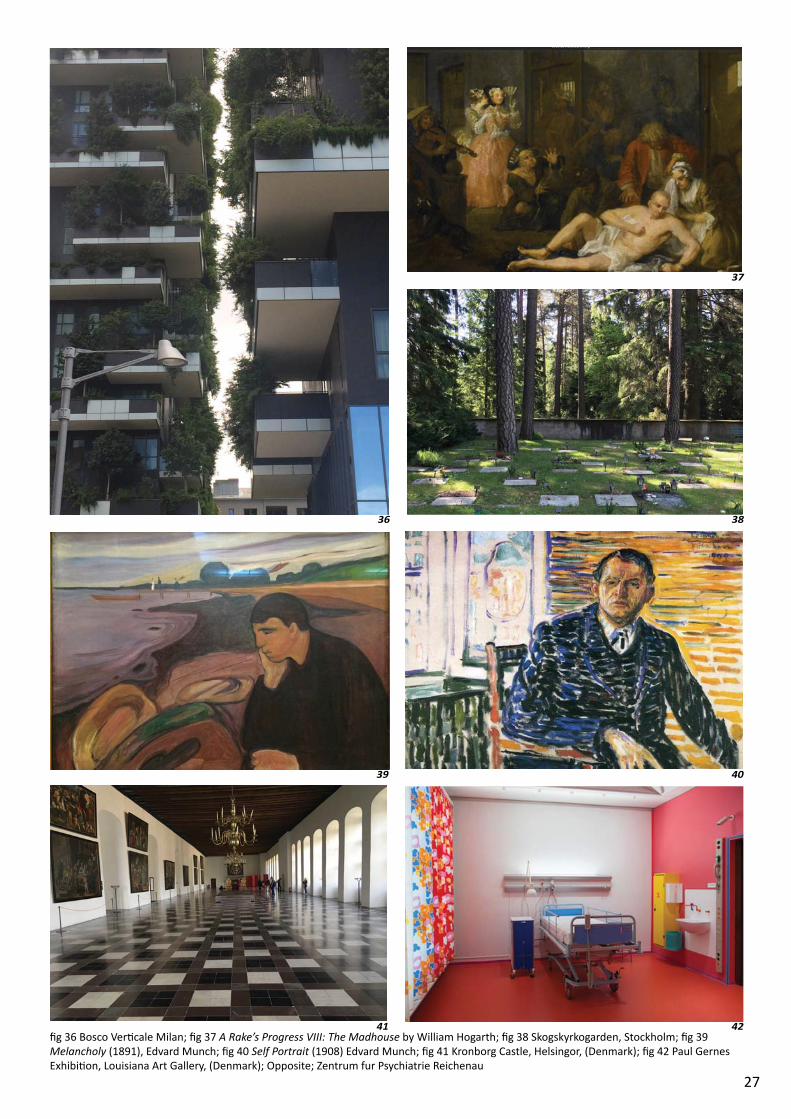
6.2 Bosco Ver cale, MilanCompleted by Stefano Boeri of Boeri Studio, Bosco Vericale won the Council on Tall Buildings and Urban Habitat (CT-BUH) “2015 Best Tall Building Worldwide.” The project symbolises a world wide preoccupa on in improving occupant amenity in today’s dense ci es, (fi g. 36).
The building’s landmark quali es shape the urban renewal of this part of Milan connec ng to improved pedestrian and bicycle pathways, sites for urban agriculture and other mixed use developments. The development’s overall ob-jec ve is to shape more vibrant, safe and diverse urban habitats within a consolidated city footprint.
In the context of this study however, the building also represents a utopian vision for what psychiatric units may be-come; high amenity facili es developed over mul ple levels embeded within the fabric of our vibrant ci es.
6.3 Looking Awry- Notes from Culture and Art
This sec on documents those representa on of mental illness in the history of art and culture that refl ect society’s a tudes to mental health. They provide a cultural backdrop to this study sourced from the many places visited be-tween scheduled site visits and mee ngs.
A Rake’s Progress VIII: The Madhouse by William Hogarth (1697-1764), (England)Seen in Sir John Soane’s Museum, London this picture (fi g. 37) is the fi nal in a series that traces the life of ‘A Rake’, (an opportunist of few morals) through the highs and lows of eighteenth century English life. Rake, pictured in the foreground has fallen to dispair living amongst society’s most desperate and des tute in the Madhouse.
Also pictured, are two elegantly dressed ladies strolling through the Madhouse taking pleasure it would seem, from the inhabitants and there squalor. The picture depicts the accepted social moires of the me where poorly treated and des tute Madhouse inhabitants, gathered elms from visitors encouraged to ‘poke and prod’ them for entertain-ment.
Skogskyrkogarden, Stockholm, (Sweden) Only a short train ride from the centre of Stockholm, Skogskyrkogarden is a remarkable place that unfolds to the view and imagina on along carefully curated pathways. Registered as an UNESCO World Heritage Site in 1994, this unique-ly designed includes landscapes designed by Lewerentz and buildings designed by Asplund (fi g. 38).
An idealised version of the Nordic lanscape, the cemetry is peaceful and reveren al as a place of burial and memory.
27
36
37
38
fi g 36 Bosco Ver cale Milan; fi g 37 A Rake’s Progress VIII: The Madhouse by William Hogarth; fi g 38 Skogskyrkogarden, Stockholm; fi g 39 Melancholy (1891), Edvard Munch; fi g 40 Self Portrait (1908) Edvard Munch; fi g 41 Kronborg Castle, Helsingor, (Denmark); fi g 42 Paul Gernes Exhibi on, Louisiana Art Gallery, (Denmark); Opposite; Zentrum fur Psychiatrie Reichenau
39 40
41 42
28
But in the context of this study however one wonders, “why is it that we aspire for such beauty in death when life for the most vulnerable can be so lacking in basic human amenity.”
Edvard Munch and his famous pain ngs, Oslo and Bergen, (Norway)Munch has been iden fi ed as the ar st, “more so than any other to have given shape to the inner life and psyche of modern man and is thus a precursor in the development of modern psychology.”
His pictures, Melancholy (1891), (fi g. 39), The Scream (1893) and Anxiety (1894) have become recognisable symbols of the aliena on of modern life with each picture rich in subject ma er, symbolism and brooding technique.
By 1908 Munch was ‘verging on madness,’ and underwent a cure of ‘vitalism’ at Professor Jacobson’s Hospital for sev-eral months where he painted a self-potraint, (fi g.40) so unlike his previous ouevre in its vibrancy of color and tech-nique that it marked a recovery of sorts. Munch went on to paint op mis c pictures returning to his earlier themes less regularly.
Kronborg Castle, Helsingor, (Denmark)Made famous by Shakespere, Elsinore (said to have been based on Kronborg Castle), is the backdrop for the seem-ingly demented musings of Hamlet as he plots the downfall of King Claudius who has seized the throne and married Queen Gertrude- the widow of his recently deceased father, (fi g, 41).
Madness is a ruse to enact jus ce on the most powerful by the most weak. The impact Hamlet’s demeted ways has on his most beloved Ophelia however are harrowing as the mighty castle halls echo her distress as she runs through them inconsolable and in tears.
Paul Gernes Exhibi on, Louisiana Art Gallery, (Denmark)Paul Gernes experimented with color fi elds, found objects and ‘poor’ techniques to create vibrant and thought pro-voking ar si c pieces and installa ons. Amongst many other things, he developed a thesis linking color with pa ent recovery leading him in 1968, to be commissioned by St. Herlev Hospital to ‘decorate’ their new acute services build-ing, (fi g. 42).
The result is a unique hospital se ng characterised by polychroma c interior spaces, some of which are reproduced in this gallery retrospec ve of the ar st’s work. Simulataenously overwhelming and hopeful, Paul Gernes’s ‘decora- on’ of St Herlev Hospital confi rms the contribu on art and architecture can make to the every day life of our ins tu- ons.
Michael Jarrell’s Cassandre, Berlin, (Germany)Interpreted by Fanny Ardant accompanied by the Berliner Philharmoniker, Cassandre is the internal monolgues of the the Trojan priestess that is said to ‘represent both an a empt to clarifi ca on and the admission of failure, a marriage of clear realisa on and melancholy.’
The piece swerves and dips through a malestrom of feeling and emo on touching places of raw pain and lucid love. In this study, Cassandre is symbolic of how our psychological well being is shaped by our individual capaci es to en-gage and make sense of the depths of our human experiences and the emo ons they trigger.

29
SECTION 3
30
7.0 Conclusions and Recommenda ons
7.1 ConclusionsCurrently in Australia, many outmoded mental health units built in the 1970s are being replaced by new facili es of high amenity to meet the aspira on of today’s recovery focussed care models.
Many of the new facili es developed over single level incorporate large landscaped areas resul ng in a disporpo on-ally high site footprint that adversly limits the capacity of hospital campuses to accommodate other needs.
Out of necessity new ‘mul ple level’ design models are emergeing in Australia consistent with many of the overseas models visited as part of this study. Of these, four trends emerge that are summarised below as ‘types’ and described with reference to the amenity provided.
In this context, amenity is defi ned as follows:
1. Direct access from internal residen al and clinical areas to landscaped spaces
2. High levels of daylight penetra on
3. High levels of acous c a enua on
4. Ease of way fi nding
Amenity items 1 and 2 vary drama cally in the ‘types’ listed below whilst amenity items 3 and 4 can be adapted to suit each.
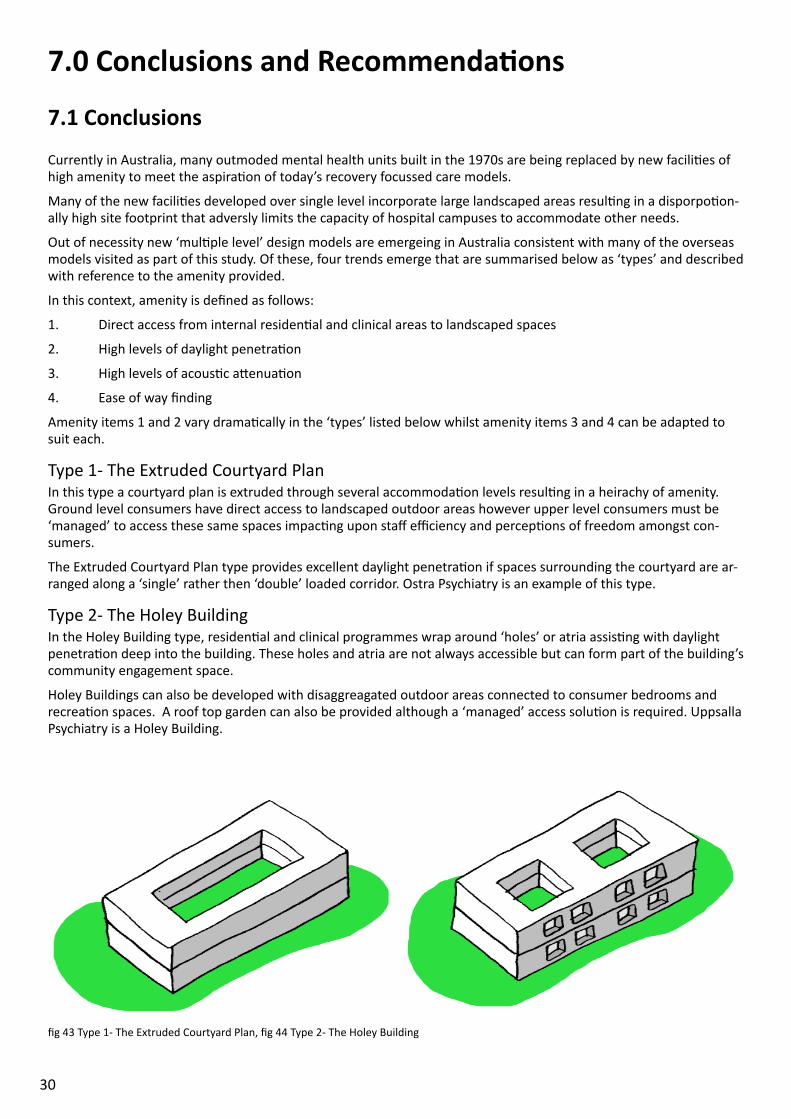
Type 1- The Extruded Courtyard PlanIn this type a courtyard plan is extruded through several accommoda on levels resul ng in a heirachy of amenity. Ground level consumers have direct access to landscaped outdoor areas however upper level consumers must be ‘managed’ to access these same spaces impac ng upon staff effi ciency and percep ons of freedom amongst con-sumers.
The Extruded Courtyard Plan type provides excellent daylight penetra on if spaces surrounding the courtyard are ar-ranged along a ‘single’ rather then ‘double’ loaded corridor. Ostra Psychiatry is an example of this type.
Type 2- The Holey BuildingIn the Holey Building type, residen al and clinical programmes wrap around ‘holes’ or atria assis ng with daylight penetra on deep into the building. These holes and atria are not always accessible but can form part of the building’s community engagement space.
Holey Buildings can also be developed with disaggreagated outdoor areas connected to consumer bedrooms and recrea on spaces. A roof top garden can also be provided although a ‘managed’ access solu on is required. Uppsalla Psychiatry is a Holey Building.
fi g 43 Type 1- The Extruded Courtyard Plan, fi g 44 Type 2- The Holey Building
31
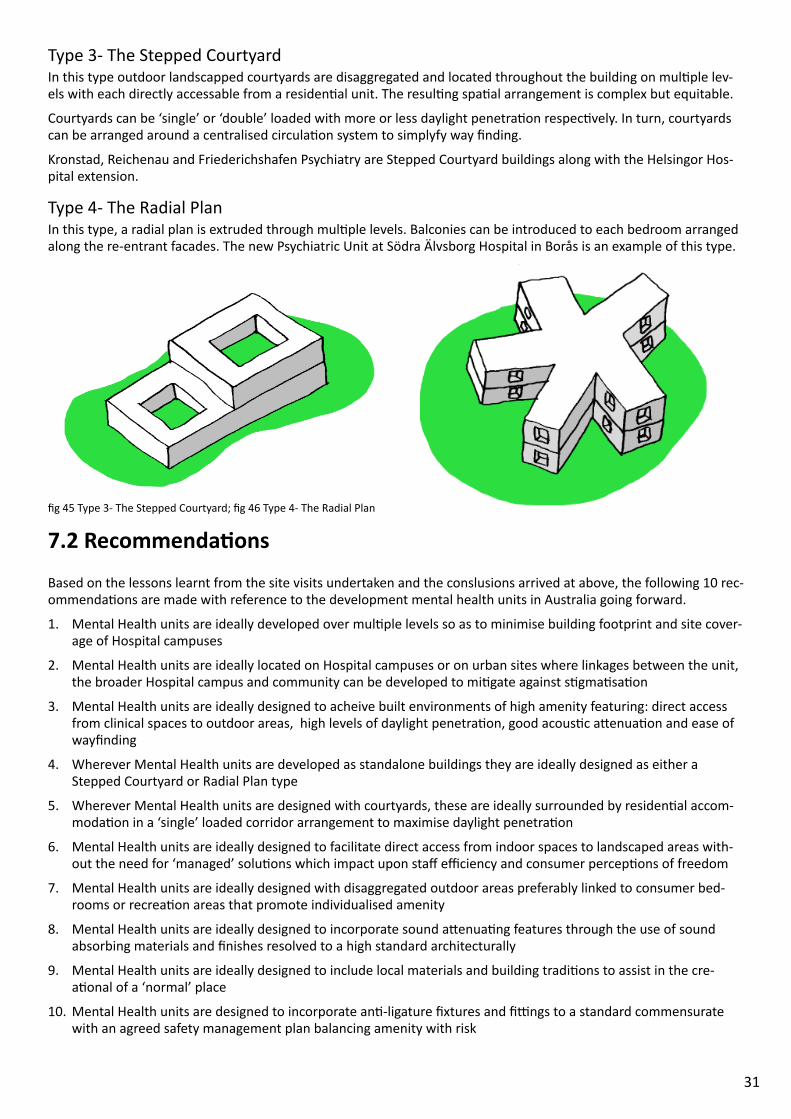
Type 3- The Stepped CourtyardIn this type outdoor landscapped courtyards are disaggregated and located throughout the building on mul ple lev-els with each directly accessable from a residen al unit. The resul ng spa al arrangement is complex but equitable.
Courtyards can be ‘single’ or ‘double’ loaded with more or less daylight penetra on respec vely. In turn, courtyards can be arranged around a centralised circula on system to simplyfy way fi nding.
Kronstad, Reichenau and Friederichshafen Psychiatry are Stepped Courtyard buildings along with the Helsingor Hos-pital extension.
Type 4- The Radial PlanIn this type, a radial plan is extruded through mul ple levels. Balconies can be introduced to each bedroom arranged along the re-entrant facades. The new Psychiatric Unit at Södra Älvsborg Hospital in Borås is an example of this type.
7.2 Recommenda onsBased on the lessons learnt from the site visits undertaken and the conslusions arrived at above, the following 10 rec-ommenda ons are made with reference to the development mental health units in Australia going forward.
1. Mental Health units are ideally developed over mul ple levels so as to minimise building footprint and site cover-age of Hospital campuses
2. Mental Health units are ideally located on Hospital campuses or on urban sites where linkages between the unit, the broader Hospital campus and community can be developed to mi gate against s gma sa on
3. Mental Health units are ideally designed to acheive built environments of high amenity featuring: direct access from clinical spaces to outdoor areas, high levels of daylight penetra on, good acous c a enua on and ease of wayfi nding
4. Wherever Mental Health units are developed as standalone buildings they are ideally designed as either a Stepped Courtyard or Radial Plan type
5. Wherever Mental Health units are designed with courtyards, these are ideally surrounded by residen al accom-moda on in a ‘single’ loaded corridor arrangement to maximise daylight penetra on
6. Mental Health units are ideally designed to facilitate direct access from indoor spaces to landscaped areas with-out the need for ‘managed’ solu ons which impact upon staff effi ciency and consumer percep ons of freedom
7. Mental Health units are ideally designed with disaggregated outdoor areas preferably linked to consumer bed-rooms or recrea on areas that promote individualised amenity
8. Mental Health units are ideally designed to incorporate sound a enua ng features through the use of sound absorbing materials and fi nishes resolved to a high standard architecturally
9. Mental Health units are ideally designed to include local materials and building tradi ons to assist in the cre-a onal of a ‘normal’ place
10. Mental Health units are designed to incorporate an -ligature fi xtures and fi ngs to a standard commensurate with an agreed safety management plan balancing amenity with risk
fi g 45 Type 3- The Stepped Courtyard; fi g 46 Type 4- The Radial Plan
32
7.3 Dissemina on of FindingsThe Conclusion and Recommenda ons made here are best disseminated throughout Australia through the following intergovernmental, academic and industry forums, publica ons, conferences and groups.
• Australasian Health Infrastructure Alliance: an Australia wide inter governmental forum of State Departments of Health that, amongst other things, auspices the development of the Australsian Health Facility Guidelines which set a minimum standard for all Health facili es design including Mental Health facili es across Australia
• Australian Health Design Council: an Australia wide industry forum of expert health design professionals es-tablished principly to assist collate and disseminate evidence pertaining to all aspects healthcare facility design including mental health
• Architecture Australia: Australia’s publica on of record for architectural and design dialogue
• Healthcare Week and Design Speaks, Health: Mul format and annual health facility design conferences includ-ing a Call for Abstracts process, invited interna onal and local Speakers Series and Panel Sesssions a ended by Government and Health Service provider representa ves along with Australian expert health archi ects and designers
• University of Melbourne, Melbourne School of Design, Guest Lectures and Studio Design Sessions: Various op-portuni es to engage in University led academic forums including Guest Lectures, Guest Design Studio Cri ques or Sessional Studio Leader opportuni es in health facility design forums, studio sessions or exchanges
Recently I was appointed to the posi on of Manager, Design Services Unit of the Infrastructure and Planning Branch of the Sport and Recrea on, Infrastructure, Interna onal Engagement and Department of Housing Division of the Vic-torian Department of Health and Human Services.
This gives me a unique opportunity to shape the future of mental health unit design by advoca ng for the recom-menda ons made above amongst Government colleagues and public mental health service providers during the planning, conceptualisa on and delivery of new mental health unit developments throughout Victoria and Australia.
In conclusion, this study summarises the opportuni es available to Australian mental health administrators and architects when conceptualising new mental health units based on consumer focussed and recovery orientated care models. It demonstrates how successfully high amenity designs can be conceived of and delivered in facili es devel-oped over mul ple levels that enable the demands of today’s metropolitan hospital campuses to be met.

33
Notes & References1. How many people experience mental illness?, Sane Australia, accessed 29 August 2016, <h p://www.sane.org>
2. What are the chances of recovering from mental illness?, Sane Australia, accessed 29 August 2016, <h p://www.sane.org>
3. How many people are disabled by mental illness?, Sane Australia, accessed 29 August 2016, <h p://www.sane.org>
4. From, L and Lundin, S (eds) 2010, Architecture As Medicine- The importance of architecture for the treatment outcomes in psychiatry, ARQ, Gothenburg
5. Rosen, A (2006) The Australian experience of de-ins tu onalisa on: interac on of Australian culture with the development and reform of mental health services. Acta Psychiatria Scandinavica, 113 (s429), pp.81-89
6. Dandenong Acute Mental Health Unit, Victoria and the Glenside Mental Health Unit in South Australia are ex-amples of the courtyard and pavilion types respec vely.
7. HASSELL (2014), Future direc ons in design for mental health facili es
8. Psykiatrius Hus, Tengbom, accessed 29 August 2016, <h p://www.en.tengbom.se>
9. Ulrich, R, Borgen, L, Lundin, S, 2012 Toward a design theory for reducing aggression in psychiatric facili es, Arch 12: Architecture| Research| Care| Health, Chalmers, Gothenburg