Towards Accessible, Effective and Resilient After … · After hours primary health care ... New...
50
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services Report of the After Hours Primary Health Care Working Party
Transcript of Towards Accessible, Effective and Resilient After … · After hours primary health care ... New...

Towards Accessible, Effective and Resilient After Hours Primary
Health Care Services
Report of the After Hours Primary Health Care Working Party

The After Hours Primary Health Care Working Party
Co-chairs Dr Sharon Kletchko Dr Jim Primrose
Members Dr Tom Bracken Mr John Macaskill-Smith Dr Ben Gray Dr Tim Malloy Ms Linda Dubbeldam Ms Cathy O�Malley (from March 2005) Dr Peter Foley Ms Georgina Paerata Ms Carolyn Gullery Dr Alistair Sullivan Ms Julene Hope Dr Richard Tyler (November 2004 � February 2005) Dr Robert Kofoed Dr Jim Vause Dr Maree Leonard
Project Manager Ms Floss Caughey
Citation: After Hours Primary Health Care Working Party. 2005. Towards Accessible, Effective and Resilient After Hours Primary Health Care Services:
Report of the After Hours Primary Health Care Working Party. Wellington: Ministry of Health.
Published in July 2005 by the Ministry of Health
PO Box 5013, Wellington, New Zealand
ISBN 0-478-29659-2 (Book) ISBN 0-478-29662-2 (Web)
HP 4168
This document is available on the Ministry of Health�s website: http://www.moh.govt.nz

Contents
Executive Summary and Recommendations iv
1 Introduction to After Hours Primary Health Care 1 1.1 New Zealand context 1 2.2 Definition 2 2.3 Guiding principles 2 2.4 The challenge 4
3 Ensuring Access to After Hours Primary Health Care Services 5 3.1 Current access issues 5 3.2 Proposed solutions to ensure access 5
4 Clarifying Roles and Responsibilities for Service Planning and Delivery 7 4.1 Current issues 7 4.2 Proposed actions to clarify roles and responsibilities for effective service planning
and delivery 9
5. Strengthening Resilience 13 5.1 Current issues impacting on resilience 13 5.2 Proposed actions to strengthen resilience 16
Appendices Appendix 1: Terms of Reference: After Hours Primary Health Care Working Party 18 Appendix 2: He Korowai Oranga: Setting a New Direction for Mäori Health 21 Appendix 3: Principles Based Planning Framework for After Hours Primary Health Care 22 Appendix 4: Models of After Hours Primary Health Care: What Works and Where? 30 Appendix 5: Special Needs Grants 41 Appendix 6: Information on Fee for Service Deductions for Casual Visits 42
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services iii
Executive Summary and Recommendations
The After Hours Primary Health Care Working Party (the Working Party) has made 15 recommendations aimed at ensuring accessible and effective after hours primary health care services and strengthening their resilience to meet people�s urgent need for care. The Working Party believes these recommendations, if implemented, will meet the project objectives stated in its Terms of Reference (refer Appendix 1). These are to:
�develop and recommend a national policy framework as it relates to after hours primary health care that:
• provides clarity to practitioners, after hours service providers, Primary Health Organisations (PHOs), District Health Boards (DHBs) and the Ministry of Health about their respective responsibilities for the provision of after hours primary health care; and
• creates an environment that promotes locally developed solutions to the provision of services, particularly over night�.
The Working Party considers that DHBs, in collaboration with PHOs and after hours service providers, must take a lead role in the planning of after hours service development for their districts. This will require exploration of different funding approaches to ensure resilience of these services so that their communities can have confidence that after hours primary health care services will be available to them when they need them. Responsibility for delivering primary health care services that are accessible 24 hours, seven days a week (24/7) should remain with PHOs. PHOs will need to demonstrate to the DHB that they have 24/7 arrangements in place. This can be achieved either by subcontracting with their member practices or by contracting other after hours service providers. It is important that people appreciate that 24/7 primary health care does not mean 24/7 access to routine non-urgent care. After hours primary health care is designed to meet the needs of patients that cannot be safely deferred until regular general practice services are next available. As accessible, effective and resilient after hours services have continued to be an issue for primary health care, DHBs, along with their respective PHOs and after hours service providers, are urged to start planning now.
Recommendations to DHBs
1. DHBs, in collaboration with PHOs and after hours service providers (both PHO member practices and, where applicable, Accident and Medical Clinics) and Emergency Departments (EDs): (a) identify current after hours services and current resources (medical and nursing
workforce and funding from the full range of funding streams as listed in section 5.1)
(b) analyse the service and resource needs, the gap (if any) between these needs and the current services and resources, and any opportunity costs arising
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services iv

(c) develop and implement a planning and funding strategy1 for after hours primary health care for their district, including rural communities, that enables accessible, effective and resilient after hours primary health care services for all service users within current resources
(d) facilitate effective relationships between PHOs and after hours service providers, when requested, as part of the change management process required to achieve sustainable after hours primary health care services.
2. The District After Hours Services Plans should follow as a guide the Principles Based
Planning Framework for After Hours Primary Health Care (Appendix 3); and the information on models of after hours primary health care (Appendix 4), and should: (a) support service models that fully utilise the competencies of the primary care
team and consider the impact of the Health Practitioners Competence Assurance Act 2003 and the concept of scopes of practice
(b) encourage the rationalisation of after hours services in urban areas to provide adequate geographical access, including to services overnight
(c) explore co-location models as an option (d) build professional development into service planning, especially where health
professionals are expected to take on different roles (e) consider the potential for nurses, including nurse practitioners, to strengthen the
workforce capacity for after hours services (f) in relation to the current utilisation of EDs by primary care patients, consider the
opportunity costs to DHBs, equity of access issues and the possible impact on health outcomes in terms of unacceptable delays in accessing services
(g) ensure that any additional assistance for urban after hours services is equitably matched for after hours services in rural areas too distant to participate in or access the urban-based models
(h) collaborate to ensure seamless after hours primary health care across DHB boundaries.
3. As after hours services are an emergent priority, DHBs are urged to commence their
after hours service planning immediately without waiting for the planning requirement to be incorporated into the District Annual Planning (DAP) process for the 2006/07 financial year.
4. DHBs should ensure that Accident and Medical Clinics that are not open 24/7 have an
on call service or formal arrangements in place with other providers to meet their section 882 obligations.
1 A planning and funding strategy is a method to improve the performance of the health system through
proactive planning and funding that considers which interventions should be funded, how they should be funded and from whom (referred to as �strategic purchasing� in the World Health Report 2000, Health Systems: Improving Performance, World Health Organization, 2000).
2 New Zealand Public Health and Disability Act 2000.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services v

Recommendations to PHOs
5. PHOs should work collaboratively with their respective DHB to assist with defining the after hours service needs of their service users and developing a planning and funding strategy that adequately addresses those needs, guided by the Principles Based Planning Framework for After Hours Primary Health Care (Appendix 3).
6. Accountability for 24/7 primary health care service delivery should remain with PHOs.
PHOs must demonstrate to the DHB that they have 24/7 arrangements in place for all service users: (a) by establishing subcontractual arrangements with their member practices that
make their after hours obligations clear and/or (b) by contracting with another provider to provide after hours services.
7. The PHOs� contracts or subcontracts for after hours service provision should:
(a) detail the principle of funding following the patient so that as the increased first contact primary health care strategy funding becomes available, this can be used to improve access to after hours services for their enrolled patients
(b) ensure that eligible enrolled people get access to low cost pharmaceuticals.
Recommendations to the Ministry of Health
8. The Ministry of Health should arrange for the preparation of an after hours primary health care planning and funding strategy, as outlined in Recommendations 1 and 2, to be included as a DAP requirement for DHBs.
9. Once adequate utilisation data is available, the Ministry should review the first contact
capitation formula in collaboration with key stakeholders. 10. The Ministry should review and clarify the policy regarding the use of Services to
Improve Access (SIA) funding to support improved access for high needs populations to after hours primary health care.
11. The Ministry, in collaboration with key stakeholders, should review the existing rural
premium funding (workforce retention funding and reasonable roster funding). Consideration should be given to the impact of changes in after hours service delivery and to compensating those rural providers for whom after hours, particularly overnight services, continue to be an onerous responsibility.
12. The Ministry should give priority to the establishment of an expert sector group to
develop a face to face sector disposition tool. The sector disposition tool would be designed to assist the after hours health professional determine which service � the primary health care service or the ED � patients should most appropriately attend for treatment. The expert sector group should be drawn from the following organisations: New Zealand Faculty Australasian College for Emergency Medicine (ACEM); College of Emergency Nurses of New Zealand (ENNZ); New Zealand College of Practice Nurses (NZNO); Royal New Zealand College of General Practitioners (RNZCGP); Accident and Medical Practitioners� Association (AMPA); New Zealand Rural General Practice Network (RGPN); telephone health advice service; and the ambulance sector.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services vi
13. The Ministry, in collaboration with DHBs, should explore the feasibility of integrating telephone health advice with after hours primary health care services.
Recommendation to the Ministry of Health and Accident Compensation Corporation
14. The Ministry of Health and Accident Compensation Corporation (ACC), in consultation with key stakeholders, should complete the review of Primary Response in Medical Emergencies (PRIME) as a matter of urgency.
Recommendation to Accident Compensation Corporation
15. ACC should investigate options for payment for primary health care services provided in EDs, given the current limitations imposed by the legislation.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services vii
1 Introduction to After Hours Primary Health Care
1.1 New Zealand context
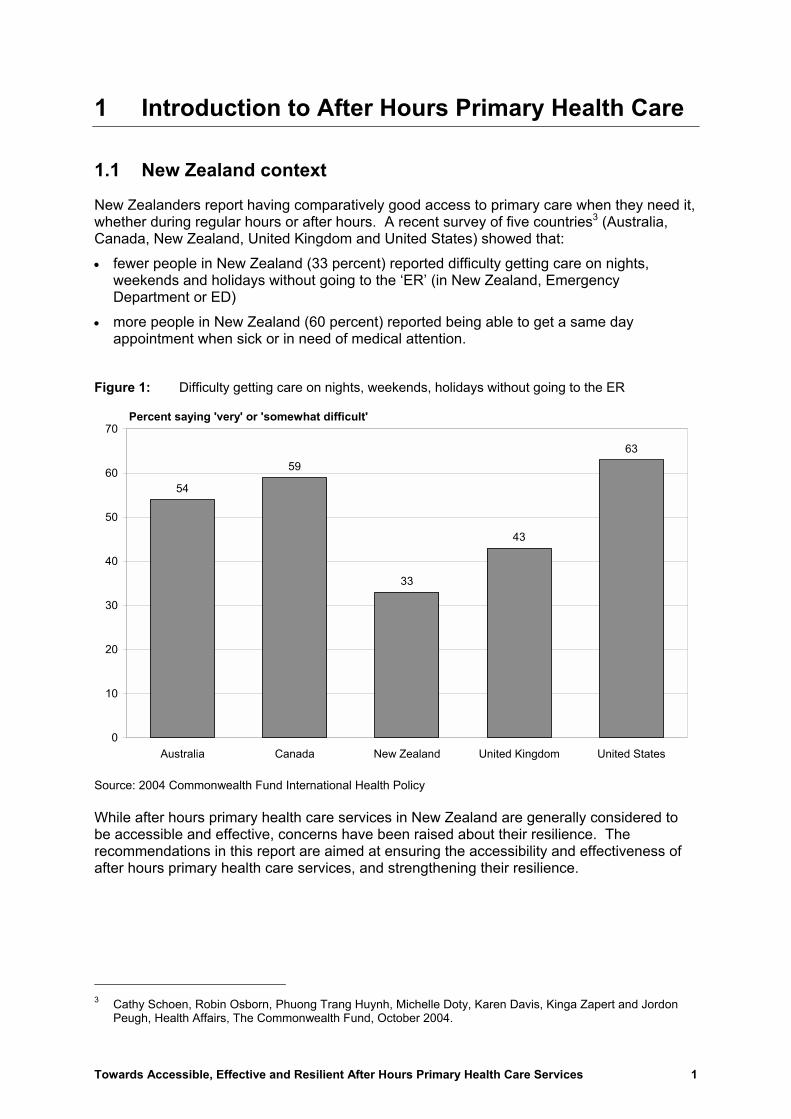
New Zealanders report having comparatively good access to primary care when they need it, whether during regular hours or after hours. A recent survey of five countries3 (Australia, Canada, New Zealand, United Kingdom and United States) showed that: • fewer people in New Zealand (33 percent) reported difficulty getting care on nights,
weekends and holidays without going to the �ER� (in New Zealand, Emergency Department or ED)
• more people in New Zealand (60 percent) reported being able to get a same day appointment when sick or in need of medical attention.
Figure 1: Difficulty getting care on nights, weekends, holidays without going to the ER
54
59
33
43
63
0
10
20
30
40
50
60
70
Australia Canada New Zealand United Kingdom United States
Percent saying 'very' or 'somewhat difficult'
Source: 2004 Commonwealth Fund International Health Policy While after hours primary health care services in New Zealand are generally considered to be accessible and effective, concerns have been raised about their resilience. The recommendations in this report are aimed at ensuring the accessibility and effectiveness of after hours primary health care services, and strengthening their resilience.
3 Cathy Schoen, Robin Osborn, Phuong Trang Huynh, Michelle Doty, Karen Davis, Kinga Zapert and Jordon
Peugh, Health Affairs, The Commonwealth Fund, October 2004.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 1

2.2 Definition
The After Hours Primary Health Care Working Party (the Working Party) has agreed on the following definition of after hours primary health care: After hours primary health care is designed to meet the needs of patients4 which cannot be safely deferred until regular or local general practice5 services are next available.
Figure 2: After hours primary health care
Self Care
After Hours Primary Health Care
Emergency Response
� Regular general practice� Community care (including dental)� Specialist referral
Telephone advice with health professional (eg, Healthline)
Phone 111 Ambulance service and Emergency Department
Disposition assessment6 face to face with health professional
Consultation face to face with health professional
2.3 Guiding principles
The Working Party believes that future planning of after hours primary health care should be guided by three key principles. These are: 1. accessible to patients and their families/whänau 2. effective service delivery 3. resilient with sufficient resources to provide the service so that the community can have
confidence in ongoing service coverage. The diagram below outlines dimensions for each key principle.
4 Patients include both enrolled and casual patients. 5 �Regular general practice services� are those services provided when the practice where the patient is enrolled
is routinely open. 6 Disposition assessment determines which level of care a patient requires, for example primary care or ED.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 2
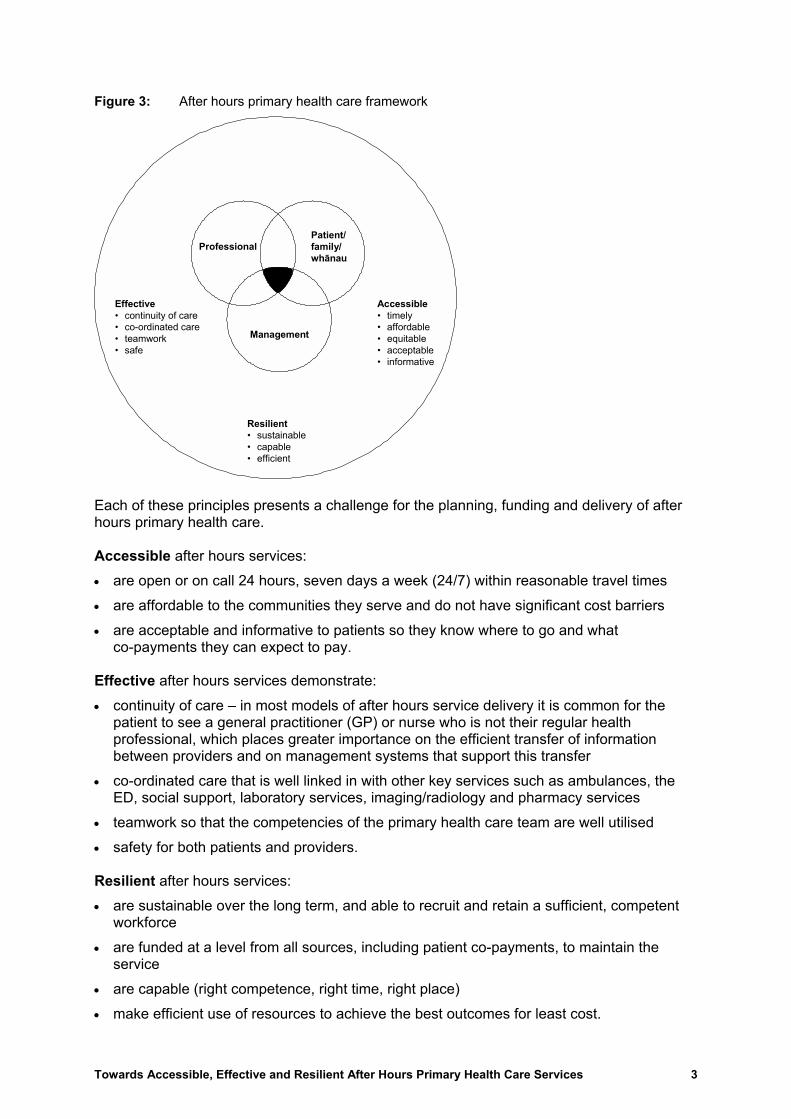
Figure 3: After hours primary health care framework
Effective� continuity of care� co-ordinated care� teamwork� safe
Resilient� sustainable� capable� efficient
Accessible� timely� affordable� equitable� acceptable� informative
ProfessionalPatient/ family/ whänau
Management
Each of these principles presents a challenge for the planning, funding and delivery of after hours primary health care. Accessible after hours services: • are open or on call 24 hours, seven days a week (24/7) within reasonable travel times • are affordable to the communities they serve and do not have significant cost barriers • are acceptable and informative to patients so they know where to go and what
co-payments they can expect to pay. Effective after hours services demonstrate: • continuity of care � in most models of after hours service delivery it is common for the
patient to see a general practitioner (GP) or nurse who is not their regular health professional, which places greater importance on the efficient transfer of information between providers and on management systems that support this transfer
• co-ordinated care that is well linked in with other key services such as ambulances, the ED, social support, laboratory services, imaging/radiology and pharmacy services
• teamwork so that the competencies of the primary health care team are well utilised • safety for both patients and providers. Resilient after hours services: • are sustainable over the long term, and able to recruit and retain a sufficient, competent
workforce • are funded at a level from all sources, including patient co-payments, to maintain the
service • are capable (right competence, right time, right place) • make efficient use of resources to achieve the best outcomes for least cost.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 3

Planning for accessible, effective and resilient after hours primary health care should also be congruent with the key directions of the Primary Health Care Strategy7 and with He Korowai Oranga: Mäori Health Strategy8 which sets a new direction for Mäori health development, building on the gains made over the past decade (refer Appendix 2).
2.4 The challenge
How can New Zealand ensure accessible and effective after hours primary health care services, and strengthen their resilience within available resources � funding, facility and workforce? This challenge has a number of key features. • In rural areas, the smaller workforce teams available to share after hours responsibilities
mean these responsibilities are more onerous to the point where they impact on workforce recruitment and retention.
• During the overnight period, workforce issues generally become more severe. This is because GPs and nurses working during the day are increasingly reluctant to be on call overnight as well and salaried staff expect higher remuneration. (Weekends can pose similar workforce problems for after hours service provision.)
• Low patient numbers presenting after hours in rural areas and overnight in urban areas can mean the service is not financially sustainable within current contracting approaches.
• Higher patient co-payments create access barriers for patients. An unplanned �market� response to these issues can lead to: • a mismatch between public and provider expectations in relation to after hours service
delivery • the expectation that rural people must travel long distances to after hours services • adverse effects on rural workforce recruitment and retention that impact on the availability
of regular daytime primary health care services • closure of overnight services in urban areas • growing inequities for both users and providers of after hours services • increased attendance of primary care patients after hours at hospital-based EDs, incurring
opportunity costs for District Health Boards (DHBs).
7 Minister of Health, The Primary Health Care Strategy, Ministry of Health, February 2001. 8 Minister of Health and Associate Minister of Health, He Korowai Oranga: Mäori Health Strategy, Ministry of
Health, November 2002.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 4

3 Ensuring Access to After Hours Primary Health Care Services
3.1 Current access issues
Growing gap between public and provider expectations � Some people expect primary health care services for routine non-urgent care to be available 24/7. While, through Healthline and other telephone advice services, professional advice is readily accessible 24/7, the available primary health care workforce is stretched to provide after hours primary health care designed to meet the needs of patients whose care cannot be safely deferred until regular general practice services are next available. Risk of service coverage gaps � While rural communities have been most affected by problems in after hours service delivery, some urban areas have been faced with sudden closure of overnight facilities. While the DHBs have seen to it that alternative arrangements have been put in place, the options are often limited by the need to take action immediately. Cost barriers � Fees for after hours primary health care services are often higher than daytime services to reflect the higher cost of service delivery. High fees for after hours services create access barriers for patients, who may delay seeking the urgent primary health care treatment they require. Even when the fees charged are not significantly greater than daytime services, some people on low incomes (such as beneficiaries) may have difficulty meeting an unforeseen expense or are reluctant to attend because of prior bad debts with the after hours service provider. Travel distance and cost � Changes to after hours service delivery that result in communities travelling further to services can be a problem for people without ready access to private transport. This is particularly a problem in areas of high deprivation. (Refer to sections 4.1 and 4.2 for comment on the travel time specified in the PHO Service Agreement.) Access to reduced pharmaceutical co-payments � When Primary Health Organisation (PHO) enrolees access after hours primary health care services that are not part of, or contracted to, their PHO, they do not get reduced pharmaceutical co-payments. Even when the after hours service provider is part of, or contracted to, their PHO, the PHO enrolees may still not get reduced pharmaceutical co-payments because the after hours provider is unable to identify eligible PHO enrolees.
3.2 Proposed solutions to ensure access
Telephone health advice � People throughout New Zealand now have access to free and consistent telephone health advice 24/7 from registered nurses via the Healthline and other telephone advice services. Telephone advice is one important component of a comprehensive after hours service and it can help prevent unnecessary calls to the after hours service provider or unnecessary visits for patients. Telephone services are also an avenue of advice to callers on what after hours services are available in their area and how to access them. (Refer to �Better integrate telephone advice service� in section 4.2 for further comment.)
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 5

Inform the public about appropriate use of after hours services � As part of the implementation of the recommendations of this report and any change management processes that may be required, people need to be well informed about the appropriate use of after hours primary health care services. They need to be encouraged to use after hours services for urgent and necessary primary health care.
Ensure excellent access to regular primary care services � The need for after hours services can be reduced by ensuring excellent access to services during the day. Providing regular clinics during extended hours (evening or weekend) is a way that practices can meet the need for some patients to access primary care services outside working hours while maintaining continuity of care.
Manage service coverage risks � DHBs, in collaboration with PHOs, after hours service providers and EDs, should develop and implement a planning and funding strategy for after hours primary health care for their district, including rural communities.
Apply principle that funding should follow the patient � Funding should follow the patient and this principle should be reflected in the contract between PHOs and after hours service providers. This will allow increased funding, as it becomes available through the roll out of the Primary Health Care Strategy, to be used in ways that improve access to after hours services for the PHOs� enrolled population.
Special Needs Grants (SNGs) for emergency medical treatment � If a patient is having trouble meeting the costs of emergency medical treatment, they may be referred to Work and Income to apply for assistance to meet the cost of that treatment by means of an SNG. The general purpose of SNGs is to provide additional last-resort �safety net� assistance to beneficiaries and low income earners experiencing exceptional financial hardship. After hours service providers should be aware of the availability of SNGs so they can inform patients about them. They also need to be aware that approval of an SNG by Work and Income is required. (Further information about SNGs is provided in Appendix 5.)
Use of Services to Improve Access (SIA) funding � It has generally been considered outside policy for PHOs to apply SIA funding to reduce co-payments for after hours services. However, use of SIA funding has been approved in some instances to support after hours services for high needs populations. The Ministry of Health should review and clarify the policy regarding the use of SIA funding in relation to supporting improved access for high needs populations to after hours primary health care.
Transport assistance � PHOs may apply SIA funding to assist high needs populations with travel costs or with solutions to transport problems to improve access to services.
Access to reduced pharmaceutical co-payments � Where PHOs contract with other providers to provide after hours services for their enrolees, this contract should ensure that eligible enrolled people get access to low cost pharmaceuticals. In order for this to occur, the after hours service provider will need to be able to easily identify the PHO enrolees. As well, the DHB will need to be satisfied that the principle of the funding following the patient has been applied.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 6

4 Clarifying Roles and Responsibilities for Service Planning and Delivery
4.1 Current issues
(a) Current planning of after hours services National level planning � Concerns are expressed by a number of stakeholders that localised solutions in the absence of a national planning framework can lead to a lack of consistency and growing disparities in patient access and expectations of providers across different settings and DHB districts. At a district level � DHBs have tended to respond to after hours service issues affecting service coverage in particular localities. Few DHBs have proactively taken the lead in a comprehensive district-wide approach to planning for after hours service coverage that is accessible, effective and resilient.
(b) Contractual obligations not consistently interpreted or enforced For PHOs � The PHO Service Agreement states the PHO is responsible for providing:
�access to First Level Services on a 24 hour a day, seven day a week basis for 52 weeks a year for all service users.
First Level Services must be available for 95 percent of the enrolled population during: • the normal business day within 30 minutes travel time • after hours within 60 minutes travel time�.
There are concerns that the 60-minute travel time specified in the PHO Service Agreement may become the norm for after hours rather than the maximum travel time applying to the rural context only. While First Level Services are well defined within the PHO Service Agreement, there is varying interpretation regarding the essential components of an after hours primary health care service. For GP members � Not all PHOs have �back to back� agreements in place with their GP members. It was reported that some GPs were not contributing to after hours care and did not experience any imposition of penalties, so others were questioning why they should continue to provide after hours services.
(c) After hours service providers outside PHOs (for example, Accident and Medical Clinics)
A number of Accident and Medical Clinics operate independently of PHOs. They therefore do not receive the additional Primary Health Care Strategy funding received by PHO practices. They continue to receive General Medical Services (GMS) subsidies for eligible patients, which are limited to Community Services Card and High Use Health Card holders and to children and young people under 18 years.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 7

Some of these providers stay open through the night but their Accident Compensation Corporation (ACC) contract (which provides higher funding levels in return for meeting certain quality requirements) requires them to stay open until 8 pm only. In some parts of metropolitan areas there are numerous Accident and Medical Clinics open during the evening period but none open overnight. Accident and Medical Clinics that have recently ceased providing overnight services cite financial sustainability issues as the reason. (d) After hours primary health care services and Emergency Departments The Working Party was asked to advise the Ministry of Health on nationally consistent policy about arrangements for primary health care services provided at hospital EDs. The Working Party makes the following points concerning after hours primary health care services and EDs. • As a general principle, it is considered better for patients to access primary health care
from primary care providers. This is because primary care providers deliver an appropriate level of care and are more likely to achieve the benefits of continuity of care for patients than EDs, which provide episodic care for significant illness.
• Under current policy settings, EDs cannot charge for services, even if the services provided are identified as being primary health care in nature.
• Equity issues arise from the provision of free primary health care services from EDs. While people in urban settings have the option of accessing these free services, rural people living distant from an ED do not have this option available to them and have to pay for after hours primary health care services.
• There are examples of co-location models (refer Appendix 4) where the ED and after hours primary health care service operate from the same site and optimise the use of the available workforce and infrastructure. Where patient charges apply to the primary health care after hours service, it is important that the two services are clearly separated and signposted with clear information to the public about patient charges. The public must be in no doubt that services for emergencies requiring Emergency Department care remain free of charge.
• ACC regulations relating to ACC Public Health Acute Services have a significant impact on the co-located (ED and primary care after hours) model. ACC Public Health Acute Services funding covers �Emergency Department attendances and follow-up emergency department services less then seven days from the original presentation�. However, if the GP service located at the ED is provided under a separate legal entity to the DHB, then ACC will pay for treatment on invoice from the service (although this does not necessarily reduce the risk that ACC will pay twice for these services because of the way the Public Health Acute Services funding is calculated).
• The purpose of the Australasian Triage Scale9 used in EDs is to rate the urgency of patients presenting symptoms. The scale is not appropriate for determining which service (the ED or a primary care provider) people should attend for treatment.
• Some DHBs have agreed that EDs be the after hours primary health care service provider for the overnight period (10 or 11 pm � 8 am) when attendances are low. ED capacity (staff and facilities) must be used for managing emergency needs as the first priority and so may not extend to providing consistent, timely access to people with lower priority needs such as those seeking after hours primary health care. Organising the ED to undertake this role in addition to its first priority role must be carefully considered from a safety, workload, capacity and competency perspective.
9 Australasian College for Emergency Medicine, Patient�s Right to Access Emergency Department Care, Policy
Document, Australasian College for Emergency Medicine, March 2004.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 8

4.2 Proposed actions to clarify roles and responsibilities for effective service planning and delivery
Clarifying responsibilities of key agencies Agency Responsibility for after hours primary
health care As reflected in
DHB • Service coverage � Ensure availability of primary medical services and/or nursing services with medical back-up after hours within 60 minutes of travel for 95 percent of DHB�s population.
2005/06 Service Coverage Schedule
DHB • Identify how it will work with PHOs to ensure all people have appropriate 24 hour access to essential primary services (after hours, First Level Services).
2005/06 Operational Policy Framework
DHB • In collaboration with PHOs, after hours service providers and EDs, develop and implement a planning and funding strategy for after hours primary health care for its district, including rural communities, that enables accessible, effective and resilient primary health care services for all service users within current resources.
Advice in After Hours Primary Health Care Working Party report on how DHBs should work with PHOs to ensure all people have appropriate access to after hours services; Ministry of Health to arrange for inclusion as a District Annual Planning requirement for 2006/07
PHO • Provide access to First Level Services 24/7 for all service users.
• First Level Services must be available for 95 percent of enrolled population after hours within a 60-minute travel time.
PHO Service Agreement.
PHO • Demonstrate to the DHB that it has 24/7 arrangements in place for all service users by establishing subcontractual arrangements with member practices that make their obligations clear or by contracting with another provider to provide after hours services.
Advice in After Hours Primary Health Care Working Party report on how PHOs should deliver on PHO Service Agreement obligations.
PHO • Detail the principle of funding following the patient so that, as the increased first contact primary health care strategy funding becomes available, this can be used to improve access to after hours services for its enrolled population.
• Ensure that eligible people get access to low cost pharmaceuticals.
Advice in After Hours Primary Health Care Working Party report on how PHOs should deliver on PHO Service Agreement obligations.
GP/practice • Provide after hours services or agree with the PHO an alternative arrangement.
Back to back agreement with PHO
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 9

Agency Responsibility for after hours primary health care
As reflected in
Independent after hours service provider (eg, Accident and Medical Clinic)
Either: • provide after hours services for PHO�s
enrolled population and/or • provide after hours services to casual
users.
Contract with PHO and/or Operate under section 88 agreement
ED • Provide secondary level emergency services.
DHB responsibility � service specification for EDs
ED Provide after hours primary health care services either: • as part of co-location arrangement with
primary care services; or • overnight by arrangement as sole after
hours provider.
Agreement between DHB and PHOs/GPs Agreement between DHB and PHOs
A Planning Framework for DHBs and PHOs �The Working Party has developed a Planning Framework for After Hours Primary Health Care based on the key guiding principles of access, effectiveness and resilience (refer Appendix 3). As well, the Working Party has outlined the strengths and weaknesses (in terms of the three guiding principles) of a number of after hours service models that operate in different settings (refer Appendix 4). Appendices 3 and 4 are designed to assist DHBs and PHOs in their planning of after hours services.
DHBs take lead in planning at district level � DHBs are required to identify how they will work with PHOs to ensure all people have appropriate 24 hour access to essential primary services.10 The Working Party considers this requirement would best be met by DHBs, in collaboration with PHOs, taking the lead in developing a planning and funding strategy for after hours primary health care services for all service users within their district. The District After Hours Services Plan should follow as a guide the Principles Based Planning Framework for After Hours Primary Health Care (Appendix 3). The plan should include the following elements: • encouraging the rationalisation of after hours services in urban areas to provide adequate
geographical access, including to services overnight • exploring co-location models as an option • building professional development into service planning, especially where health
professionals are expected to take on different roles • in relation to the current utilisation of EDs by primary care patients, considering the
opportunity costs to DHBs of current utilisation of EDs by primary care patients, equity of access and the possible impact on health outcomes in terms of unacceptable delays in accessing services
• collaborating to ensure seamless after hours primary health services across DHB boundaries • ensuring coverage for casual patients, including visitors to the district.
10 Ministry of Health, 2005/06 Operational Policy Framework.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 10
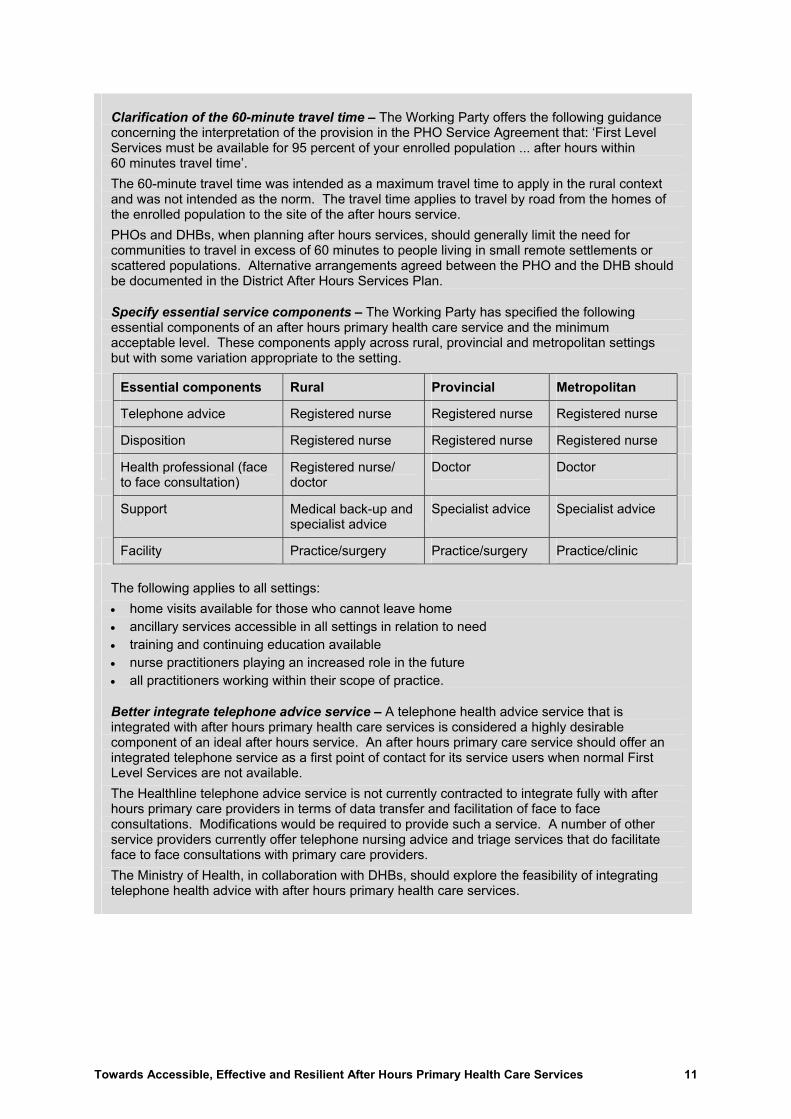
Clarification of the 60-minute travel time � The Working Party offers the following guidance concerning the interpretation of the provision in the PHO Service Agreement that: �First Level Services must be available for 95 percent of your enrolled population ... after hours within 60 minutes travel time�. The 60-minute travel time was intended as a maximum travel time to apply in the rural context and was not intended as the norm. The travel time applies to travel by road from the homes of the enrolled population to the site of the after hours service. PHOs and DHBs, when planning after hours services, should generally limit the need for communities to travel in excess of 60 minutes to people living in small remote settlements or scattered populations. Alternative arrangements agreed between the PHO and the DHB should be documented in the District After Hours Services Plan.
Specify essential service components � The Working Party has specified the following essential components of an after hours primary health care service and the minimum acceptable level. These components apply across rural, provincial and metropolitan settings but with some variation appropriate to the setting.
Essential components Rural Provincial Metropolitan
Telephone advice Registered nurse Registered nurse Registered nurse
Disposition Registered nurse Registered nurse Registered nurse
Health professional (face to face consultation)
Registered nurse/ doctor
Doctor Doctor
Support Medical back-up and specialist advice
Specialist advice Specialist advice
Facility Practice/surgery Practice/surgery Practice/clinic
The following applies to all settings: • home visits available for those who cannot leave home • ancillary services accessible in all settings in relation to need • training and continuing education available • nurse practitioners playing an increased role in the future • all practitioners working within their scope of practice.
Better integrate telephone advice service � A telephone health advice service that is integrated with after hours primary health care services is considered a highly desirable component of an ideal after hours service. An after hours primary care service should offer an integrated telephone service as a first point of contact for its service users when normal First Level Services are not available. The Healthline telephone advice service is not currently contracted to integrate fully with after hours primary care providers in terms of data transfer and facilitation of face to face consultations. Modifications would be required to provide such a service. A number of other service providers currently offer telephone nursing advice and triage services that do facilitate face to face consultations with primary care providers. The Ministry of Health, in collaboration with DHBs, should explore the feasibility of integrating telephone health advice with after hours primary health care services.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 11

Clarify PHO contracting requirements, including with non-PHO providers of after hours services � It is the Working Party�s view that accountability for providing 24/7 primary health care should remain with PHOs. PHOs must demonstrate to the DHB that they have 24/7 arrangements in place for all service users: • by establishing subcontractual arrangements with their member practices that make their
after hours obligations clear and/or • by contracting with another provider to provide after hours services.
The PHOs� contracts for after hours service provision for all service users should: • detail the principle of funding following the patient so that, as the increased first contact
primary health care strategy funding becomes available, this can be used to improve access to after hours services for their enrolled population
• ensure that eligible enrolled people get access to low cost pharmaceuticals.
DHBs and non-PHO providers of after hours services � DHBs should: • include any non-PHO after hours providers in their District After Hours Services Plan • encourage rationalisation of after hours services to enable accessible and sustainable
overnight services • ensure that Accident and Medical Clinics that are not open 24/7 have an on call service or
formal arrangements in place with other providers to meet their section 88 obligations.
After hours primary health care services and Emergency Departments � The Working Party makes the following proposals.
DHBs, in collaboration with PHOs, should involve ED personnel in their District After Hours Services Plan, particularly when considering co-location models of after hours service delivery.
In relation to the current utilisation of EDs by primary care patients, DHBs need to consider the opportunity costs to DHBs, equity of access issues, and the possible impact on health outcomes in terms of unacceptable delays in accessing services.
The Ministry of Health should give priority to the establishment of an expert sector group to develop a face to face sector disposition tool. The sector disposition tool would be designed to assist the after hours health professional determine which service � the primary health care service or the ED � patients should most appropriately attend for treatment. The expert sector group should be drawn from the following organisations: New Zealand Faculty Australasian College for Emergency Medicine (ACEM); College of Emergency Nurses of New Zealand (ENNZ); New Zealand College of Practice Nurses (NZNO); Royal New Zealand College of General Practitioners (RNZCGP); Accident and Medical Practitioners� Association (AMPA); New Zealand Rural General Practice Network (RGPN); telephone health advice service; and the ambulance sector.
As an intermediate option until the sector disposition tool is developed, for patients categorised at the ED as ACEM triage 4 and 5, the health professional should pose an additional question: �What is the probability of this patient deteriorating within the triage times (one hour for triage 4 and two hours for triage 5)?�. If the answer is �extremely unlikely�, the health professional should consider organising alternative primary care provision (if available).
ACC should investigate options for payment for primary health care services provided in EDs, given the current limitations imposed by the legislation.
Once a national sector disposition tool is developed and in place, the policy concerning EDs charging for after hours primary health services should be reviewed.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 12

5. Strengthening Resilience
5.1 Current issues impacting on resilience
(a) Workforce issues The following workforce changes impact on after hours services. Expectations of work/life balance � The future workforce has expectations of a different work/life balance to that of health professionals in the past. General practitioners and nurses working during the day are increasingly reluctant to be on call in the evening and overnight as well. Safety issues are cited as part of the reason for this. Changes in employment arrangements � Historically in general practice, the Principal was the employer and, in order to offer cost-effective care, the Principal provided the uneconomic part of general practice (after hours care) him/herself rather than pay another provider (salaried doctor or nurse) for care that might generate little or no income. With different ownership arrangements (for example, Accident and Medical Clinics, Trusts) and salaried staff becoming more common, these staff expect to be adequately remunerated for working after hours shifts. Wider range of after hours service models � The wide range of after hours service models available today has specific impacts on both the workload and the competency requirements for those involved. The annual reports on the medical workforce published by the Medical Council of New Zealand include �average on call� hours for general practitioners. In 2003, for example, whereas 5 percent of GPs (most likely rural) reported 50 hours or more on call per week, 57 percent (most likely urban) reported no on call hours.11 The average time on call of just under 10 hours per week has remained steady for the years 2000�2003. Expanded role for nurses � Nurses are playing an expanding role in after hours care across all after hours service models. Nurses with appropriate levels of education, experience and competency are maintaining safe and effective after hours services. It is important that nurses providing First Level Services work within a clearly defined scope of practice as members of a team, not in isolation. Professional development � Where health professionals are expected to take on expanded roles in after hours service delivery, it is important to consider scopes of practice and the required competencies. In planning services under new after hours models, associated professional development must be included. For example, for co-location models, nurses may have new or expanded triage and sector disposition responsibilities, and GPs may provide Emergency Department level care in addition to after hours primary health care.
(b) Rural issues Distance to after hours services � Changes in after hours service delivery to enable more resilient services (both after hours and during the day) have in many cases resulted in the need for rural people to travel further to access services. Access to more distant after hours services is a problem for rural people without ready access to private transport. As stated in section 3.2, PHOs can apply SIA funding to assist high needs communities with solutions to transport problems as a way of improving access to after hours services.
11 The New Zealand Medical Workforce in 2003, Medical Council of New Zealand, May 2005.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 13
Workforce issues impact on service delivery � After hours �call burden� is a very important factor impacting on the recruitment and retention of rural GPs and their choice of where to practise. A 2001 survey of the workload of GPs found that workload expressed as responsibility for after hours call is highest (97 percent) for rural areas.12 There have also been reports of nurses working 10 consecutive days or more on call in remote rural areas. The following factors impact on after hours service delivery in rural areas. • Recruitment and retention issues affecting both doctors and nurses mean that many rural
health professionals carry heavy daytime workloads. • The rural workforce (both GPs and nurses) is aging and less able to cope with after hours
responsibilities on top of a busy daytime workload. • More remote rural areas have a small workforce team to draw on so after hours rosters
are more onerous. • The short- and long-term locum placement market is international and very competitive,
especially with regard to price. (While a locum support service is available for rural GPs, there is no similar locum support service available for nurses practising in rural areas.)
• Increased numbers of tourists in rural areas add significantly to after hours call-outs in some rural areas.
Rural practitioners carry unfair share of after hours responsibilities � Some rural providers serve communities located close enough to larger centres for them to participate in large co-operative rosters or to contribute to other after hours service models. Other rural providers serve communities too distant from larger towns for those options to provide their patients with reasonable access to after hours services. A range of after hours models has been developed in rural areas (refer Appendix 4) but most involve heavy on call responsibilities for the doctors and/or nurses involved, who may have heavy workloads during the day as well. Rural practitioners feel they are carrying an unfair burden of after hours services compared with urban practitioners and should receive greater compensation for after hours responsibilities. Expanded role for nurses � Nurses, particularly in more remote communities, are increasingly called on to provide after hours services. There are examples of after hours service models where experienced registered nurses provide first contact care, including after hours, but with access to telephone advice and support when required from a medical practitioner. These nurses are still functioning as part of a team, even if other members of the team are geographically some distance away. However, concerns have been raised where nurses are providing after hours services �by default� in unsupported situations. Ambulance service issues � In rural areas, volunteers are the backbone of the ambulance service or the fire service acting in first response. There is significant variability in the level of training and availability of ambulance personnel. PRIME issues � Rural GPs and nurses who participate as Primary Response in Medical Emergencies (PRIME) responders to ambulance call-outs enhance the emergency response capability in rural areas. Some rural GPs refuse to participate in PRIME, however, out of dissatisfaction with the operation of the scheme, including its workload, remuneration arrangements, and difficulties with accessing PRIME refresher training courses. 12 Antony Raymont, Roy Lay-Yee, Janet Pearson, and Peter Davis, New Zealand general practitioners�
characteristics and workload: The National Primary Medical Care Survey, New Zealand Medical Journal, 2005, Vol 118 No 1215.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 14

(c) Funding issues There is a sector view that the PHO capitation formula does not adequately recognise the cost of after hours care. This is perceived by some providers as a significant problem affecting sustainable service delivery. Funding of after hours services is complex with multiple funding streams that are not specific to the time of day or night. These are: • first contact PHO capitation for PHO enrolees • GMS for casual patients • a rural primary health care premium paid to PHOs with rural practices, which comprises
workforce retention funding and reasonable roster funding. Reasonable roster funding is specific to after hours services but is narrowly targeted at practices experiencing onerous after hours rosters (1:1�1:3) for geographical reasons
• DHB-funded EDs which in some cases are the main after hours primary health care service provider either by arrangement or by default
• funding from some DHBs towards some after hours arrangements to support access and resilience
• ACC fee for service based on the Injury Prevention Rehabilitation and Compensation (Liability to Pay or Contribute to Cost of Treatment) Regulations 2003 and Rural General Practice contract or Accident and Medical Clinics contracts. ED services are funded via the Public Health Acute Services agreement
• PRIME services funded by both Ministry of Health and ACC
• patient co-payments. PHO capitation funding � PHO capitation funding contributes to the cost of 24/7 primary health care. Funding for after hours care is included within the capitation formula for first contact care but is not separately identifiable. The first contact portion of the PHO funding formula is calculated according to average utilisation rates. These are based on: • all subsidised persons, including those attending after hours13 • non-subsidised persons attending general practices, including those attending after hours,
but not those attending Accident and Medical Clinics.14 It is not possible to calculate the portion of attendances that occur after hours (and therefore the portion of PHO capitation funding attributable to after hours) as the time of each attendance is not reported. Cost of after hours care � There has never been a relationship between the level of government subsidy and the cost of after hours service delivery (although there was an additional GMS payment for after hours consultations until 1989). The actual cost of, and cost steps associated with, delivering after hours service are variable according to different settings and service models.
13 Health Funding Authority, General Medical Services payments, Health Benefits Ltd, Health Funding Authority,
New Zealand, 1999. 14 Barry Gribben, The community services card and utilisation of general practitioner services, New Zealand
Medical Journal, 1996, Vol 109 pp 103�5.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 15

If PHOs were to be paid according to the cost of after hours service delivery, multiple sustainable costing models would be required. This would be a very substantive, complex piece of work with uncertain outcome. Fee for service deductions � Fee for service (FFS) deductions when PHO enrolees access after hours care from another provider � for example, an Accident and Medical Clinic � are an issue for some PHOs. PHOs serving urban areas where there are multiple providers of primary health services during the evening period are those most affected by FFS deductions. FFS deductions represent approximately 6 percent of first contact care payment overall but there is wide variation among PHOs and DHBs. FFS deductions are highest among urban enrolees, those aged under 6 or 18 years, and older Pacific and Mäori enrolees. One-quarter of FFS deductions overall are to an after hours service provider (for example, an Accident and Medical Clinic) but the specific proportion varies by DHB. (Refer Appendix 6 for details of FFS deductions.) FFS deductions apply only to Community Services Card and High Use Health Card holders and to children and young people under 18 years. They are not inflation adjusted. (A Casual Deductions Working Party is considering issues relating to casual deductions.) Unsustainable after hours services in some areas � In some areas, the funding currently provided from all sources listed above, including patient co-payments, may not be sufficient to support a sustainable after hours service. A certain level of capacity needs to be maintained even when patient volumes are low. High levels of bad debt, a particular problem in areas of high deprivation, also impact on sustainability. A separate funding allocation for after hours services � Some advocate a separate funding allocation for after hours services as one answer to these funding issues. One option suggested is to �top slice� a portion of PHO capitation at national level (say 6 to 9 percent) and allocate it to after hours services. Given the large variability of casual deductions (refer Appendix 6), however, this approach may disadvantage providers that experience low casual deductions, such as rural providers, or urban providers who are open extended hours.
5.2 Proposed actions to strengthen resilience
(a) Workforce
DHBs, in collaboration with PHOs, through their District After Hours Services Plan should: • support service models that fully utilise the competencies of the primary care team and also
consider the impact of the Health Practitioners Competence Assurance Act 2003 and the concept of scopes of practice
• build professional development into the service planning, especially when developing new after hours service models where health professionals are expected to take on expanded roles � professional development needs to include practice support systems such as peer review, orientation, and standing orders
• consider the potential for nurses, including nurse practitioners, to strengthen the workforce capacity for after hours services.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 16
(b) In rural areas
The following actions should occur to strengthen sustainable after hours services in rural areas. • The Ministry of Health, in collaboration with key stakeholders, should review the existing
rural premium funding (workforce retention funding and reasonable roster funding). Consideration should be given to the impact of changes in after hours service delivery and to compensating those rural providers for whom after hours, particularly overnight, services continue to be an onerous responsibility.
• District After Hours Services Plans should include rural communities and ensure that any additional assistance for urban after hours services in the district is equitably matched for after hours services in rural communities too distant to participate in or access the urban-based models.
• DHBs and PHOs should ensure that where nurses are providing the after hours service in rural areas, they do so as part of a team within a planned service. They need to be experienced registered nurses who have completed PRIME training and/or other advanced practice education. Nurses have also identified the need to access ongoing education, clinical supervision and appropriate medical support.
• The Ministry of Health and ACC, in consultation with key stakeholders, have initiated a review of PRIME. This review needs to include engagement with PRIME providers and be completed with urgency. DHBs and PHOs need to consider linkages between PRIME and the District After Hours Services Plan.
(c) Funding
Address funding issues at district level � Given that funding of after hours services is complex and the actual cost of delivering after hours services is variable according to the particular setting and service model, the Working Party believes it is more productive to address funding issues at district level than at the national level.
The Working Party proposes that DHBs, in collaboration with PHOs, after hours service providers (both PHO member practices and, where applicable, Accident and Medical Clinics) and EDs: • identify current after hours services and current resources (workforce and funding from the
full range of funding streams identified in section 5.1) • analyse the service and resource needs, the gap (if any) between these needs and the
current services and resources, and any opportunity costs arising • develop and implement a planning and funding strategy for after hours primary health care
for their district, including rural communities, that enables accessible, effective and resilient after hours primary health care services for all service users within current resources.
Apply the principle that funding should follow the patient � As stated in section 3.2, the PHOs� contracts or subcontracts for after hours service provision for all service users should detail the principle of funding following the patient. This is so that, as the increased first contact primary health care strategy funding becomes available, this can be used to improve access to after hours services for their enrolled population.
Enter into contractual arrangements to avoid FFS deductions � PHOs that contract with an after hours service provider could negotiate an agreement that delivers additional funding to the after hours service provider for their enrolees, in return for no GMS claims being made for these people.
Between them, a PHO and after hours service provider have all the information they require on the cost of service delivery and the funding available to reach agreement on their local funding arrangements for the provision of after hours services. Depending on local circumstances, payment from the PHO could be based on a percentage of capitation funding, a percentage of gross income, an agreed fixed sum, or a sum per patient seen.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 17

Appendix 1: Terms of Reference: After Hours Primary Health Care Working Party
Background
It is acknowledged that, while New Zealand compares favourably with Australia, Canada, United Kingdom and the United States15 in terms of access to after hours services, in many areas of New Zealand, access to and delivery of after hours care are facing a range of difficulties. Key after hours issues were identified by a Ministry stock-take undertaken during August 2004 based on the responses of District Health Boards (DHBs), national organisations, Primary Health Organisations (PHOs) and after hours service providers. The PHO Service Agreement Amendment Protocol Reference Group (PSAAP) Meeting of 5�7 October 2004 supported the DHBs and Ministry proposal that a working party including key stakeholders be established to address the issue of after hours care and recommended that the working party processes accommodate the urgency of the issues. The Terms of Reference of the Working Party incorporate those proposed by PSAAP.
Project objectives
The purpose of the project is to develop and recommend a national policy framework as it relates to after hours primary health care that: • provides clarity to practitioners, PHOs, DHBs and the Ministry of Health about their
respective responsibilities for the provision of after hours primary health care • creates an environment that promotes locally developed solutions to the provision of
services overnight.
Role of After Hours Primary Health Care Working Party
The After Hours Primary Health Care Working Party will:
(1) make recommendations to the Ministry of Health on: • nationally consistent policy settings as they relate to after hours primary health care
services • nationally consistent policy about arrangements for primary health care services
provided at Hospital Emergency Departments, including patient co-payments and any subsequent impact on PHO capitation funding
(2) make recommendations to the Ministry of Health and ACC on nationally consistent minimum standards that ensure an accessible, quality service
15 2004 Commonwealth Fund International Health Policy Survey can be viewed at http://www.cmwf.org/
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 18
(3) make recommendations to DHBs and PHOs, and, where appropriate, ACC, on: • the funding implications of delivering after hours primary health care and how this
may alter the way that existing funds are distributed • ways of facilitating �flow through,� where appropriate, of lower patient charges for
after hours services, including pharmacy prescriptions • how Accident and Medical Clinics could contribute to the delivery of after hours
services in a PHO environment • solutions appropriate to rural New Zealand that recognise its particular workforce
and access issues • identification of innovative local models, including those that utilise multi-disciplinary
teams, and the need to review those models for consistency against the national policy framework
• any existing contractual requirements as they relate to after hours services and any new contracting approaches that may be required.
Note that the recommendations of the Working Party will need to be developed with the assumption that no further primary health care strategy funding will be available to support after hours services, but there may be opportunities to better utilise available primary health care and DHB baseline funding to support after hours primary health care.
Principles and policy setting
All recommendations must be congruent with the key directions of the Primary Health Care Strategy. These are: • work with local communities and enrolled populations � this means encourage local
solutions that involve consultation with local communities and promote continuity of care • identify and remove health inequalities � this means aiming to reduce access barriers for
populations experiencing health inequalities
• offer access to comprehensive services to improve, maintain and restore people�s health � this means offering access to appropriate after hours services, taking into consideration distance to travel, cost and information to the public
• co-ordinate care across service areas � this means good linkages between primary after hours and secondary Emergency Department services and timely transfer of patient information
• develop the primary health care workforce � this means encourage after hours service models that develop and fully utilise the competencies of the multi-disciplinary primary health care team providing after hours primary health care
• continuously improve quality using good information � this means setting achievable quality standards that can be improved over time.
Build on work already undertaken. Develop a policy direction and framework that is consumer focused, evidence based, system minded and sustainable over time.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 19

Authority of the Working Party
The Working Party has the mandate to make recommendations to DHBNZ, the Ministry of Health, and, as appropriate, ACC. The Working Party has no authority to commit expenditure on behalf of DHBs, DHBNZ, the Ministry of Health or any other organisation.
Chair
The project sponsors will share the role of Chairperson.
Spokespersons
The joint Chairs will be the spokespersons for the Working Party regarding media queries.
Communication with the sector
Relationship with Reference Group The Reference Group will include a wide range of stakeholders such as DHBs (Planning and Funding Managers and Emergency Departments), PHOs, Mäori Reference Group, Healthline, ambulance services, medical and nursing organisations, Accident and Medical Clinics and other stakeholders, including consumer/community groups such as Rural Women, Age Concern, Grey Power, Plunket and others. The role of the Reference Group is to enable wider information sharing among key stakeholders about the work of the Working Party, mainly by email. The Working Party will be consulted on what information should be shared with the Reference Group but the decision will be made by the joint Chairs and their respective organisations.
Communication with other groups The Working Party will share reports and seek feedback from the following groups as appropriate: • the PHO Community Council (once established); and • the Primary Health Care Strategy and PHO Development Taskforce.
6 December 2004
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 20
Appendix 2: He Korowai Oranga: Setting a New Direction for Mäori Health
He Korowai Oranga: Mäori Health Strategy16 sets a new direction for Mäori health development over the next 10 years, building on the gains made over the past decade.
Committed to the Treaty of Waitangi
The Government is committed to fulfilling the special relationship between iwi and the Crown under the Treaty of Waitangi. The principles of Partnership, Participation and Protection (derived from the Royal Commission on Social Policy) will continue to underpin that relationship, and are threaded throughout He Korowai Oranga. Partnership Working together with iwi, hapü, whänau and Mäori communities to develop strategies for Mäori health gain and appropriate health and disability services.
Participation Involving Mäori at all levels of the sector, in decision-making, planning, development and delivery of health and disability services.
Protection Working to ensure Mäori have at least the same level of health as non-Mäori, and safeguarding Mäori cultural concepts, values and practices.
16 Minister of Health and Associate Minister of Health, He Korowai Oranga: Mäori Health Strategy, Ministry of
Health, November 2002.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 21

Appendix 3: Principles Based Planning Framework for After Hours Primary Health Care
Accessible
Dimensions Further explanation Factors to take into account when planning after hours primary health care services
Timely relates to:
• the hours the service is available, both hours open and on call
The PHO Service Agreement states that the PHO will provide access to First Level Services on a 24 hour a day, seven day a week basis for 52 weeks a year for all service users. PHOs must demonstrate to the DHB that they have 24/7 arrangements in place for all service users by: • establishing subcontractual arrangements
with their member practices that make their after hours obligations clear, and/or
• contracting with another service provider to provide after hours services.
• the travel time (by road) the patient needs to reach the service.
The PHO Service Agreement states that First Level Services must be available for 95 percent of the enrolled population after hours within a 60-minute travel time. Justification must be provided when these requirements cannot be met. This justification should include details of alternative arrangements for providing First Level Services as agreed between the PHO and DHB.
Timely
Note the following. • The 60-minute travel time was intended as
a maximum standard to apply in the rural context and was not intended as the norm.
• The travel time applies to travel by road from the homes of the enrolled population to the site of the after hours service.
• PHOs and DHBs should generally limit the need for communities to travel in excess of 60 minutes to people living in small, remote settlements or remote populations.
• Alternative arrangements should be documented in the District After Hours Services Plan.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 22

Dimensions Further explanation Factors to take into account when planning after hours primary health care services
Affordable Affordable means not having significant cost barriers for patients. High patient fees and patient indebtedness act as barriers to access for some people.
It is acknowledged that often patient fees for after hours services will be higher than for regular general practice services to reflect the higher cost of service delivery. However, the following points are also noted. • Every effort should be made to provide low
cost services to all children under six years of age. The PHO Service Agreement states: �We expect that neither you nor any Contracted Provider will charge a co-payment in most situations to children under 6 years between the hours of 8 am and 8 pm, seven (7) days a week.�
• PHO funding should follow the patient so that, as increased first contact primary health care strategy funding becomes available, it can be used to improve access to after hours services for the PHO�s enrolled patients. This principle should be detailed in the contract between the PHO and its after hours service provider (or its subcontract with member practices).
• Where PHOs contract with other providers to provide after hours services for their enrolees, this contract should ensure that eligible enrolled people get access to low cost pharmaceuticals.
Special Needs Grants for emergency medical treatment � If patients are having trouble meeting the costs of emergency medical treatment, they may be referred to Work and Income to apply for assistance to meet the cost of that treatment by means of an SNG. The general purpose of SNGs is to provide additional last-resort �safety net� assistance to beneficiaries and low income earners experiencing exceptional financial hardship. Approval of an SNG by Work and Income is required.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 23

Dimensions Further explanation Factors to take into account when planning after hours primary health care services
Equitable relates to �equal access for equal need� � that is, the service is equally accessible to all the community it serves. Important aspects (other than affordability) are:
• access to transport SIA funding may be used to assist high needs populations with transport costs or with solutions to transport problems to improve access to services, including after hours services.
• physical access to the site of the service for all, including those with disabilities, wheelchairs, pushchairs and ambulance trolleys
All relevant Building Codes must be met.
Equitable
• urban and rural. Equity issues arise from the provision of free primary health care services from EDs. Rural people living at a long distance from the ED do not have this option available to them. DHBs and PHOs should ensure that any additional assistance for urban after hours services is equitably matched for after hours services in rural areas too distant to participate in or access the urban-based models.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 24

Dimensions Further explanation Factors to take into account when planning after hours primary health care services
Acceptability relates to cultural appropriateness. This includes reducing communication barriers for patients, for example, those whose first language is not English or who are hearing impaired.
The Code of Health and Disability Services Consumers� Rights applies to after hours services.
Acceptable
The PHO Service Agreement�s section on cultural values (8.1.2) states that:
�You will work with communities to ensure the Services are delivered in a culturally appropriate and competent manner, ensuring that the integrity of each individual�s culture is acknowledged and respected and that the particular needs of the community are catered for. You will work to reduce barriers to access or communication and work with communities to ensure that Services are safe for all people. You will endeavour to incorporate Mäori principles/ tikanga in to the service delivery process.�
The cultural values for PHOs applies to after hours as well as to regular services.
Informative Essential patient information about after hours services includes the location, opening hours and patient charges.
Public information about after hours services should be available via regular general practice services, clear signage at after hours services, and telephone listings, and in appropriate answerphone messages. People throughout New Zealand now have access to free and consistent telephone health advice 24/7 from registered nurses via Healthline and other telephone health advice services. However, Healthline is not currently contracted to integrate fully with after hours primary care providers in terms of data transfer and facilitation of face to face consultations. Modifications are possible to allow Healthline�s current service to do this. A number of other service providers also currently offer telephone nursing advice and triage services which integrate well with primary care providers. An integrated telephone advice service is considered an important and highly desirable first point of contact component of an ideal after hours primary care service.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 25

Effective
Dimensions Further explanation Factors to take into account when planning after hours primary health care services
Continuity of care
Continuity of care can be viewed from three aspects: 1. relational � an ongoing
relationship with an identified provider
2. informational � accumulated knowledge about an individual supported by transfer of information between providers
3. management � consistent and joined-up care over time and between providers.
PHO enrolment and continuity Enrolment with a PHO provider means that the person intends to use that provider as their preferred provider of First Level health Services. The PHO and provider are �responsible for providing continuity of care for the enrolled patient�.
The District After Hours Services Plan should support continuity of care wherever reasonably practicable. It is considered better for patients to access after hours primary care from primary care providers rather than from EDs. This is because, as well as delivering an appropriate level of care, primary care providers are more likely to achieve the benefits of continuity of care than EDs, which provide episodic care for significant illness. The PHO contract or subcontract for after hours services should include documented arrangements to support continuity of care, including the following. • Information sharing and patient follow-up
should be established. • If possible, the provider of after hours
services should have access to the register of people enrolled with the PHO, including the person�s usual provider or practitioner.
• If possible, the provider of after hours services should have direct access, where necessary, to patients� health care records from their usual provider.
• This usual provider should receive timely information on services provided to its enrolees after hours (unless the patient requests that the information not be shared).
• Wherever possible, this information on services provided to its enrolees after hours should be made available to the usual provider on the next business day.
• In general, after hours providers should only provide short-term advice, medication and support and should refer patients back to their usual provider for ongoing management of the condition.
Co-ordinated care
The after hours primary health care service needs to be well linked in with other key services.
The District After Hours Services Plan should include linkages with key services such as PRIME, the ambulance service (and the fire service where it is acting as first response), the ED, and laboratory, radiology and pharmacy services.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 26

Dimensions Further explanation Factors to take into account when planning after hours primary health care services
Teamwork In the delivery of after hours primary health care, teamwork may refer to the core primary health care team, for example, GPs, nurses, administration staff. In rural areas, the team may be wider to include, for example, ambulance officers (or the fire service acting in first response), ED, and hospital admitting services, where communication is the essence of an effective team response. Teamwork is closely linked with capability, as it is necessary to understand the competencies of team members.
The District After Hours Services Plan should: • support service models that fully utilise the
competencies of the whole primary care team
• consider the impact of the Health Practitioners Competence Assurance Act 2003 and the concept of scopes of practice
• build professional development into service planning, especially when developing new after hours service models where health professionals are expected to take on expanded roles � professional development needs to include practice support systems such as peer review, orientation, and standing orders
• consider the potential for nurses, including nurse practitioners, to strengthen the workforce capacity for after hours services.
In rural areas, the following factors are relevant. • DHBs and PHOs should ensure that where
nurses are providing after hours services, they do so as part of a team within a planned service. These nurses need to be experienced registered nurses who have completed PRIME training and/or other advanced practice education. They also need access to ongoing education, clinical supervision and appropriate medical support.
• DHBs and PHOs need to consider the linkages between PRIME and the District After Hours Services Plan.
Safety Safety issues need to be considered in terms of both: • a safe service for patients • security for the provider.
Safe after hours services for patients are closely linked with teamwork (outlined above) and capability (outlined below). Security arrangements for provider personnel should be in place for both premises and home visits in circumstances where these are considered necessary.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 27
Resilient
Dimensions Further explanation Factors to take into account when planning after hours primary health care services
Sustainable The after hours primary health care service needs to be viable over the long term. Key factors impacting on sustainability are the resources available (workforce and funding) and how well they are utilised. The service needs to be able to recruit and retain a competent workforce large enough to ensure that those providing after hours care are not working unreasonable hours. Achieving this is particularly challenging in rural areas. A certain level of capacity needs to be maintained even when patient volumes are low. This is a particular issue overnight and in rural areas generally.
The District After Hours Services Plan should: • identify current after hours services and current
resources (medical and nursing workforce and funding from the full range of funding streams as listed in section 5.1)
• analyse the service and resource needs, the gap (if any) between these needs and the current services and resources, and any opportunity costs arising
• develop and implement a planning and funding strategy for after hours primary health care for the district that enables accessible, effective and resilient after hours primary health care services within current resources.
PHOs must demonstrate to the DHB that they have 24/7 arrangements in place for all service users by: • establishing subcontractual arrangements with their
member practices that make their after hours obligations clear; and/or
• contracting with another service provider to provide after hours services for their enrolled populations.
These contracts need to detail the principle of funding following the patient. PHOs that contract with an after hours service provider could negotiate an agreement that delivers additional funding to the after hours service provider for their enrolees, in return for no GMS claims being made for these people. Depending on local circumstances, payment from the PHO could be based on a percentage of capitation funding, a percentage of gross income, an agreed fixed sum, or a sum per patient seen. Reasonable roster funding is a targeted resource applied to PHOs serving rural localities where, for geographical reasons, GPs and nurses providing First Level Services are experiencing onerous on call arrangements (1:1�1:3 rosters). Workforce retention funding is allocated to PHOs serving rural communities to assist with creating favourable working conditions including time off-duty, and a supportive professional working environment for the rural primary health care workforce.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 28
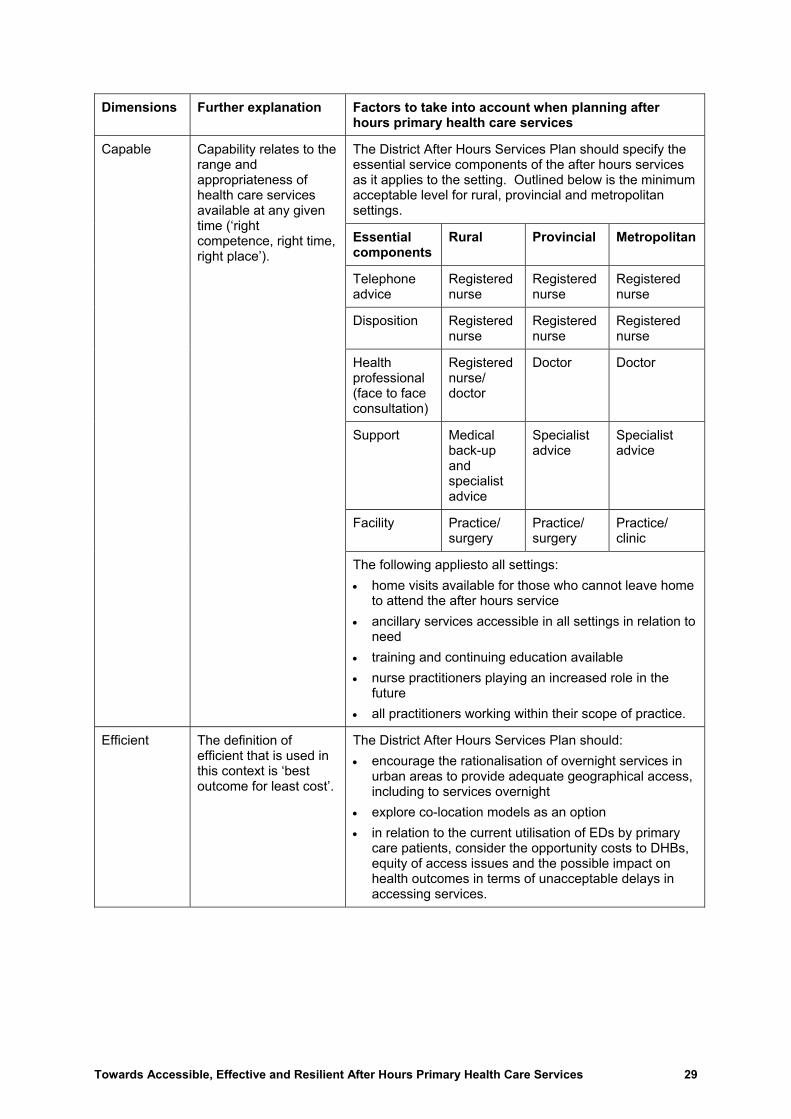
Dimensions Further explanation Factors to take into account when planning after hours primary health care services
The District After Hours Services Plan should specify the essential service components of the after hours services as it applies to the setting. Outlined below is the minimum acceptable level for rural, provincial and metropolitan settings.
Essential components
Rural Provincial Metropolitan
Telephone advice
Registered nurse
Registered nurse
Registered nurse
Disposition Registered nurse
Registered nurse
Registered nurse
Health professional (face to face consultation)
Registered nurse/ doctor
Doctor Doctor
Support Medical back-up and specialist advice
Specialist advice
Specialist advice
Facility Practice/ surgery
Practice/ surgery
Practice/ clinic
Capable Capability relates to the range and appropriateness of health care services available at any given time (�right competence, right time, right place�).
The following appliesto all settings: • home visits available for those who cannot leave home
to attend the after hours service • ancillary services accessible in all settings in relation to
need • training and continuing education available • nurse practitioners playing an increased role in the
future • all practitioners working within their scope of practice.
Efficient The definition of efficient that is used in this context is �best outcome for least cost�.
The District After Hours Services Plan should: • encourage the rationalisation of overnight services in
urban areas to provide adequate geographical access, including to services overnight
• explore co-location models as an option • in relation to the current utilisation of EDs by primary
care patients, consider the opportunity costs to DHBs, equity of access issues and the possible impact on health outcomes in terms of unacceptable delays in accessing services.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 29
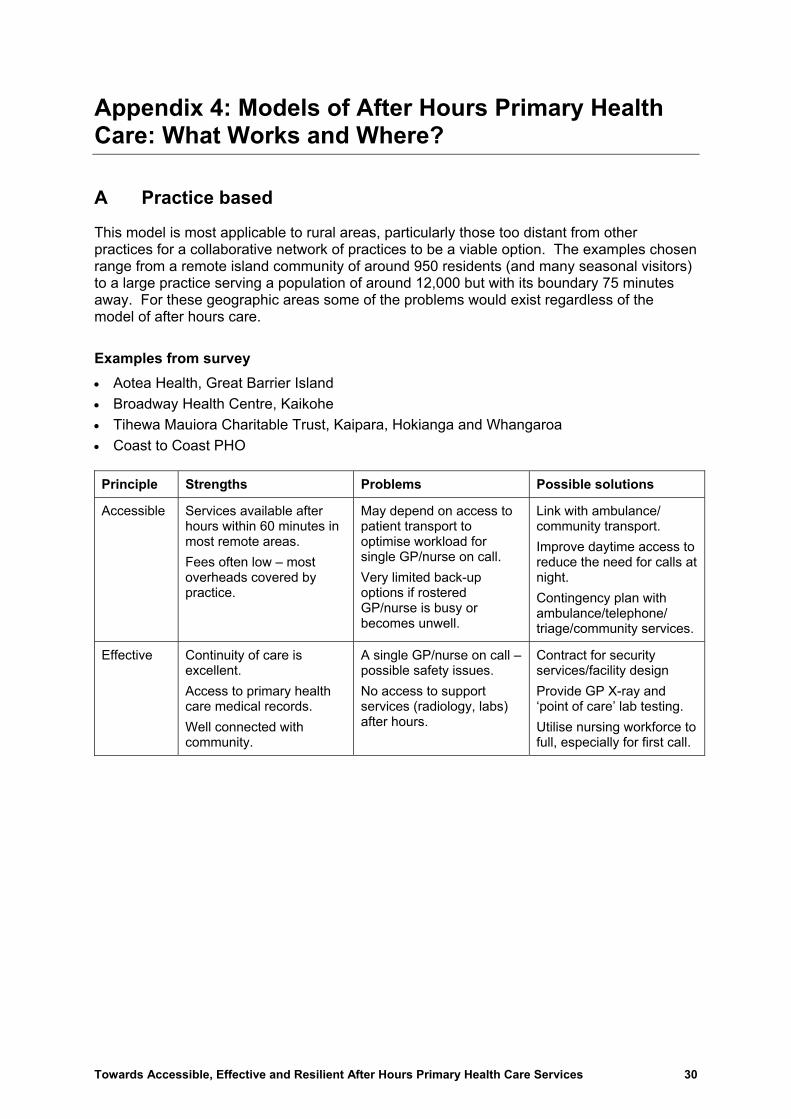
Appendix 4: Models of After Hours Primary Health Care: What Works and Where?
A Practice based
This model is most applicable to rural areas, particularly those too distant from other practices for a collaborative network of practices to be a viable option. The examples chosen range from a remote island community of around 950 residents (and many seasonal visitors) to a large practice serving a population of around 12,000 but with its boundary 75 minutes away. For these geographic areas some of the problems would exist regardless of the model of after hours care.
Examples from survey • Aotea Health, Great Barrier Island • Broadway Health Centre, Kaikohe • Tihewa Mauiora Charitable Trust, Kaipara, Hokianga and Whangaroa • Coast to Coast PHO Principle Strengths Problems Possible solutions
Accessible Services available after hours within 60 minutes in most remote areas. Fees often low � most overheads covered by practice.
May depend on access to patient transport to optimise workload for single GP/nurse on call. Very limited back-up options if rostered GP/nurse is busy or becomes unwell.
Link with ambulance/ community transport. Improve daytime access to reduce the need for calls at night. Contingency plan with ambulance/telephone/ triage/community services.
Effective Continuity of care is excellent. Access to primary health care medical records. Well connected with community.
A single GP/nurse on call � possible safety issues. No access to support services (radiology, labs) after hours.
Contract for security services/facility design Provide GP X-ray and �point of care� lab testing. Utilise nursing workforce to full, especially for first call.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 30

Principle Strengths Problems Possible solutions
Resilient Fee for service deductions (�clawback�) are not an issue. Reasonable roster funding provided to PHOs with practices experiencing 1:1�1:3 rosters, and has enabled the expansion of the primary care team to include an additional GP on Great Barrier Island.
After hours rosters are onerous for a single practice. Recruitment, retention, cost of locums. Employing a locum may not be cost-effective for only one practice at weekends, and not available after hours on weekdays. In some areas, high numbers of visitors place high demands on weekend after hours call with extra costs incurred by the practice.
Expanded role for nurses and ambulance services. Telephone triage (eg, Healthline) may prevent unnecessary call-outs so may encourage community to make full use of these services. Funders/providers include a weighting for after hours call when deciding workforce requirements. Specific after hours fee schedules for casuals. Ministry of Health reviews rural premium funding.
B Collaborative network of practices
This model is most applicable to rural areas where sharing rosters with practices in neighbouring small towns still supports reasonable access (ie, within 60 minutes of travel).
Examples from survey Te Tai Tokerau PHO Northland Wairoa PHO Tikapa Moana PHO, Waiheke Island Rural Canterbury PHO Partnership Health PHO Hurunui Kaikoura PHO Principle Strengths Problems Possible solutions
Accessible Service provided from within (extended) local area.
Several facilities for after hours � patients may be confused about where to access care. Patients may attend local rural hospital after hours to avoid paying fees. There may still be a limited number of GPs/nurses for the roster.
As for practice-based model, plus: • combine practices in
single facility • roster shared clinic late
weekday and weekend surgery among practices to reduce after hours call-outs.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 31

Principle Strengths Problems Possible solutions
Effective Potentially good communication with patient�s own GP/nurse. Reasonable roster funding was provided to enabled GPs to work no more than 1 in 4 weekends.
Equity and sustainability of the roster may damage teamwork across practices.After hours call-out rates are highly variable. Access to labs/X-ray may still be a problem.
As for practice-based model, plus: • PHO could accept
responsibility for publishing a �fair� roster
• first and second call rosters so there is back-up for busy times
• utilise nursing workforce to full, especially for first call.
Resilient Best use of existing facilities and workforce. GPs in collaboration manage or avoid �clawback�. Reasonable roster funding provided to PHOs with practices experiencing 1:1�1:3 rosters, and has reduced weekend after hours on call for some rural GPs.
Rosters may still be considered onerous. Rural hospitals rely on GPs for maintenance of 24 hour cover as availability of Medical Officers of Special Scale diminishes.
As for practice-based model, plus: • develop joint venture
after hours service (extend collaboration beyond one PHO);
• integrate after hours primary health care service with rural hospital services where possible.
C Dedicated after hours facility � Accident and Medical Clinic
This model involves an independent organisation operating a dedicated 24/7 after hours facility with doctors and nurses who are employed on contract or salary. It is typically financially sustainable in large urban areas where there is sufficient demand. Some Accident and Medical Clinics (A&M) outside major urban centres are reportedly experiencing serious sustainability problems.
Examples from survey East Health A&M Coastcare A&M Wanganui A&M Clinic Shore Care A&M White Cross A&M at Whangarei/Manaia PHO White Cross A&Ms in Auckland/Tamaki PHO
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 32

Principle Strengths Problems Possible solutions
Accessible Good access in urban areas � purpose-built facilities. Most charged a $10 surcharge for overnight services � appears low for the extra costs involved. Some A&Ms (ie, White Cross at Whangarei and Auckland) have entered into arrangements with PHOs to enable lower charges for their enrolees.
Most A&Ms have high patient charges for their patients, particularly for unsubsidised adults. Patient charges may dissuade those on lower incomes from attending the A&M service and may lead them to attend ED instead. Some A&Ms are not open overnight and so patients may call out GPs or attend ED. Eligible PHO enrolees may not receive benefit of $3 prescription charges.
PHOs� contracts for after hours service provision detail the principle of funding following the patient so that, as the increased first contact primary health care strategy funding becomes available, it can be used to improve access for their enrolled patients. DHBs ensure that A&Ms that are not open 24/7 have an on call service or formal arrangements in place with other providers to meet their section 88 obligations. PHOs enter into arrangements with A&Ms so their enrolees receive access to low cost prescriptions.
Effective Typically good communication with patient�s GP/nurse for continuing care. May have labs, X-ray, pharmacies.
Requires dedicated facility, may not be available or affordable.
DHB joint ventures for facilities. Collaboration with local PHOs.
Resilient Relieves or avoids pressure on GPs to provide after hours services. Can be an efficient resilient model in a large urban setting with high volumes.
FFS deductions are a significant issue for practices in the A&M catchment area. High costs of 24/7 employed staff including for public holidays and paid leave etc. Difficulties recruiting and retaining doctors to work the overnight shift. May provide primary care during work hours, compromising local practice viability.
PHO enters into arrangements with A&M so there are no FFS deductions. A&Ms diversify � home visits etc. A&Ms increase use of nurses. A&M service provider makes alternative arrangements for overnight services or provides them from limited sites.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 33
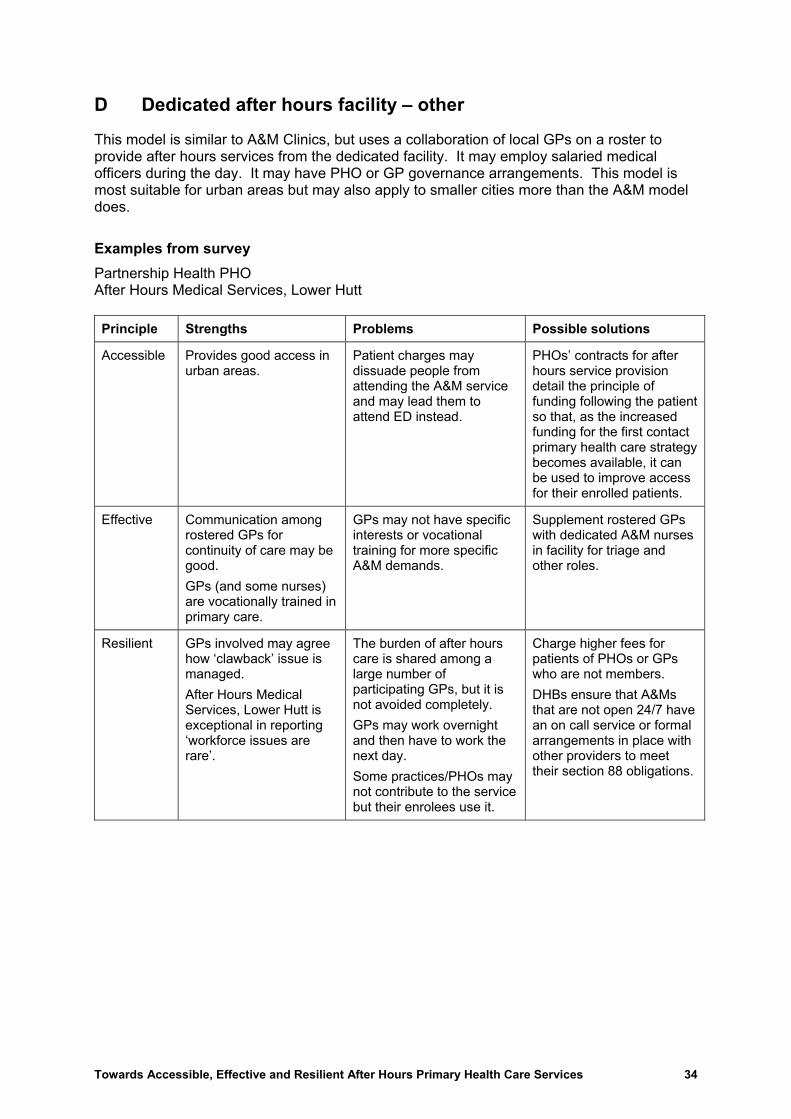
D Dedicated after hours facility � other
This model is similar to A&M Clinics, but uses a collaboration of local GPs on a roster to provide after hours services from the dedicated facility. It may employ salaried medical officers during the day. It may have PHO or GP governance arrangements. This model is most suitable for urban areas but may also apply to smaller cities more than the A&M model does.
Examples from survey Partnership Health PHO After Hours Medical Services, Lower Hutt Principle Strengths Problems Possible solutions
Accessible Provides good access in urban areas.
Patient charges may dissuade people from attending the A&M service and may lead them to attend ED instead.
PHOs� contracts for after hours service provision detail the principle of funding following the patient so that, as the increased funding for the first contact primary health care strategy becomes available, it can be used to improve access for their enrolled patients.
Effective Communication among rostered GPs for continuity of care may be good. GPs (and some nurses) are vocationally trained in primary care.
GPs may not have specific interests or vocational training for more specific A&M demands.
Supplement rostered GPs with dedicated A&M nurses in facility for triage and other roles.
Resilient GPs involved may agree how �clawback� issue is managed. After Hours Medical Services, Lower Hutt is exceptional in reporting �workforce issues are rare�.
The burden of after hours care is shared among a large number of participating GPs, but it is not avoided completely. GPs may work overnight and then have to work the next day. Some practices/PHOs may not contribute to the service but their enrolees use it.
Charge higher fees for patients of PHOs or GPs who are not members. DHBs ensure that A&Ms that are not open 24/7 have an on call service or formal arrangements in place with other providers to meet their section 88 obligations.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 34

E Co-located � Emergency Department and after hours primary health care
This model shares some of the characteristics of the dedicated after hours facility, but is co-located with a hospital ED. This model is most applicable to smaller cities where a separate dedicated after hours primary health care facility is not sustainable and there are mutual benefits in the ED and the after hours primary health care service sharing facilities and workforce.
Examples from survey Wairau Hospital/Wairau Accident and Medical Trust, Blenheim Hawera Hospital/South Taranaki Medical Trust, Taranaki Principle Strengths Problems Possible solutions
Accessible One site for all after hours services. Good access from primary health care after hours service to ED and hospital staff if required in emergencies. Hospital/ED medical records may be available for continuity of care.
Compromises viability of after hours mobile services, so GP home visits may not be available. Patients may be, initially at least, resistant to co-payments for a service located at the ED where they expect services to be free of charge.
Effective community consultation. Patient information, clear signage at co-located facility. Consistent application by staff of access criteria direct to ED. Flexibility for practices that have in place acceptable alternative after hours arrangements for their patients not to participate.
Effective Reduces over-utilisation of ED by primary care patients. Closer working relationships between health professionals working in primary and secondary health services. Quality assurance, workforce development and some equipment may be shared with hospital services. Good access to labs/ radiology and specialist opinion.
Patients assigned to the GP service who decline to pay and who then leave may have a significant clinical problem that requires ED services or admission. Careful planning for administrative services, including for fee collection, is required. Where GPs provide ED cover, they will need extra training. GPs may experience fatigue after busy overnight shift.
A sector disposition tool should be developed nationally to assist the health professional at the first point of contact of the co-location model to rapidly and consistently distinguish primary care patients (who are charged for service) from ED patients (who are not charged). Clear accountability for standards and professional development. GPs arrange workload so do not work a full day in their practice after working overnight.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 35
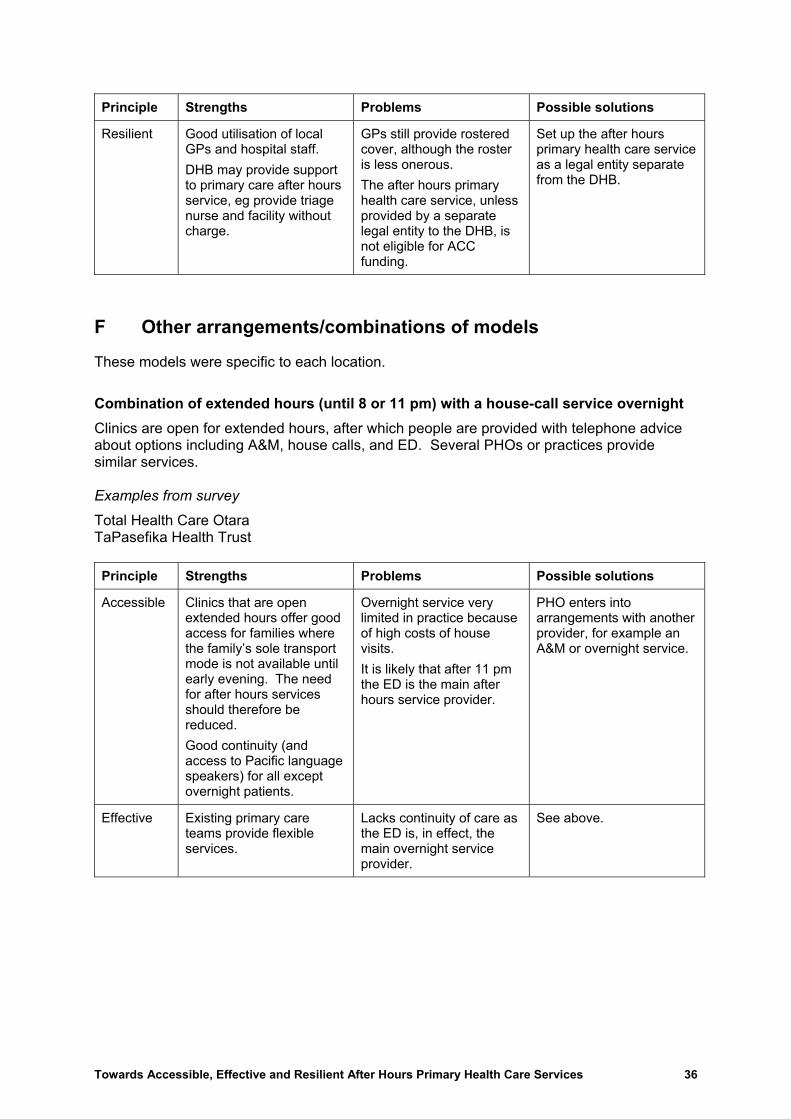
Principle Strengths Problems Possible solutions
Resilient Good utilisation of local GPs and hospital staff. DHB may provide support to primary care after hours service, eg provide triage nurse and facility without charge.
GPs still provide rostered cover, although the roster is less onerous. The after hours primary health care service, unless provided by a separate legal entity to the DHB, is not eligible for ACC funding.
Set up the after hours primary health care service as a legal entity separate from the DHB.
F Other arrangements/combinations of models
These models were specific to each location.
Combination of extended hours (until 8 or 11 pm) with a house-call service overnight Clinics are open for extended hours, after which people are provided with telephone advice about options including A&M, house calls, and ED. Several PHOs or practices provide similar services. Examples from survey
Total Health Care Otara TaPasefika Health Trust Principle Strengths Problems Possible solutions
Accessible Clinics that are open extended hours offer good access for families where the family�s sole transport mode is not available until early evening. The need for after hours services should therefore be reduced. Good continuity (and access to Pacific language speakers) for all except overnight patients.
Overnight service very limited in practice because of high costs of house visits. It is likely that after 11 pm the ED is the main after hours service provider.
PHO enters into arrangements with another provider, for example an A&M or overnight service.
Effective Existing primary care teams provide flexible services.
Lacks continuity of care as the ED is, in effect, the main overnight service provider.
See above.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 36

Principle Strengths Problems Possible solutions
Resilient Retains ownership within primary care.
Evening rosters may be onerous for staff. Extended hours may not be financially sustainable. Incentives to effectively transfer workload to ED by not providing affordable overnight service.
Arrange flexible working hours and roster. Enter into shared arrangements for overnight services with other PHOs or after hours service providers.
Collaborative network included extended hours using an existing practice facility This model uses a collaboration of GPs and nurses from a single existing practice facility with extended hours of operation (for example, one GP, one nurse and one receptionist at the centre 5�10 pm weekdays and a GP on call after 10 pm). A nurse provides triage as part of the after hours service. Example from survey
Pukekohe Family Health Centre (PFHC) Principle Strengths Problems Possible solutions
Accessible A single site � patients know where to go � with excellent access up to 10 pm.
Co-payment for the after hours service is high. Staff may not be available for public holidays.
Seek to increase number of contributing practices to increase demand and lower costs per patient. Specific arrangements for public holidays (may include telephone triage).
Effective A team (GP and nurse) available at the practice until 10 pm. Continuity of care � copies of notes sent to regular health provider. May have radiology and pharmacy on site.
Consider a nurse triage service after 10 pm (still need to have a doctor available on call).
Resilient Practice takes responsibility for the roster. GPs are paid an hourly rate. Efficient use of an existing facility.
GPs still sharing a roster for after hours and on call overnight, with risk of fatigue. Surrounding rural practices may be reluctant to join and compromise their access to workforce retention funding.
Seek to increase the number of contributing practices. Ministry of Health reviews rural premium funding.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 37

Nurse triage system with GP telephone support This model is being used in response to a serious and prolonged GP shortage (three GPs: 10,000 people) in a high-need rural area remote from an ED or dedicated facility. The nurse accesses after hours telephone advice from GPs from 5�10 pm weekdays, and from 8 am � 10 pm weekends and public holidays. Otherwise after hours medical advice is from the nearest ED (45 km away). The area is well resourced with nurses (12) � there is a six-bed hospital unit. Example from survey
Opotiki Principle Strengths Problems Possible solutions
Accessible Patients have a single pathway after hours. Care retained within the practice team. There is no patient co-payment for nurses� care.
If the patient needs to see a doctor urgently overnight, must travel to nearest ED.
Optimise ambulance and any community transport arrangements
Effective Nurse triage calls are audited by the GPs, and internally by the nurses. GP telephone advice is available.
Nurses cannot prescribe, even for straightforward clinical problems.
Develop protocols and standing orders for nurse prescribing. Recruit more GPs to increase support to nurses after hours among a larger roster of GPs.
Resilient Reduces GP workloads and demands. Works well with remote rural hospital beds.
Roster may be onerous for fewer nurses. Requires good access to continuing nursing education to maintain professional standards.
Maintain or increase continuing nursing education.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 38

Nurse-led after hours services This model applies in remote rural areas. Examples from survey
South Westland Roxburgh Medical Centre (weekends only, 5 pm Friday � 9 am Monday) Principle Strengths Problems Possible solutions
Accessible Access to after hours service is maintained in a remote area where the workforce is small
Effective The nurses are experienced registered nurses with PRIME or equivalent advanced practice training. The nurses have the support of a nurse co-ordinator (Roxburgh) and clinical nurse leader (South Westland) as well as working relationships with other key health providers in the area.
Nurses may be expected to undertake excessive on call with insufficient time off. (In South Westland they work a roster of 10 days on and four days off.) There may be insufficient medical back-up.
DHB or PHO employs additional nurses or nurse locum to enable adequate time off. It is important that nurses providing First Level Services after hours work as part of a team with appropriate medical back-up and support arranged from a doctor familiar with the local area.
Resilient The nurse-led weekend service at Roxburgh has supported the recruitment and retention of GPs in the area by providing regular time off. Nurses can provide a cost-effective service for a small population (South Westland).
Nurses undertaking extra responsibilities may expect higher reimbursement.
DHBs, PHOs and practices, when considering the option of nurse-led after hours services for remote communities or weekend cover in rural areas, need to build in the cost of reimbursement, relief, training and other support of nurses.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 39

ED provides telephone triage and all after hours services overnight (after 11 pm) for whole district Other after hours primary health care arrangements apply up till 11 pm and there is also home visiting. Example from survey
Palmerston North ED Principle Strengths Problems Possible solutions
Accessible An overnight service is provided from a single site. Patients can access telephone advice and a doctor or nurse direct overnight. Can follow-up with ED attendance and admission if required. There is no co-payment for services overnight.
Patients from outlying areas may need to travel some distance to ED.
PHOs consider using SIA funding to assist high need populations with transport to overnight service.
Effective Improved relationships with GPs who are free of overnight after hours responsibilities. Access to hospital records, and potential for hospital follow-up.
ED requires extra capacity to deliver additional overnight services. May increase expectation that ED is the provider of all services. Influx of attendances prior to GP surgeries closing starting at 9 pm creates bottlenecks at ED. The free service at the ED may be a disincentive to see the regular GP during regular hours.
Involve GPs in ED, or provide co-located facility. Provide better information back to GP and system for arranging appointments with GP in morning.
Resilient Excellent utilisation of hospital resources for a relatively small number of patients overnight. Service is funded by subscription from GPs � all revenue used for nurse/medical salary for night duty.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 40

Appendix 5: Special Needs Grants
Work and Income may grant a Special Needs Grant to meet the cost of emergency medical treatment. This provision is made, with other provisions, under the Special Needs Grant Programme, 1998. The general purpose of SNGs is to provide additional last-resort �safety net� assistance to beneficiaries and low income earners experiencing exceptional financial hardship. An applicant must satisfy eligibility conditions and limits, including income limits and cash asset limits. If the person can meet the cost from other resources, Work and Income will not grant an SNG. In considering an application for an SNG, Work and Income must also be satisfied that an emergency situation exists, which has given rise to an immediate need. This provision is for up to a maximum of $300 per treatment (not per visit) and includes doctor�s fees, prescription charges or hospital. One treatment could require more than one visit, but the limit applies to all visits required for that treatment. Grants cannot be made to pay or reimburse the �ACC surcharge� charged by medical providers. This SNG is non-recoverable, and more than one grant may be made in a 52-week period.
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 41
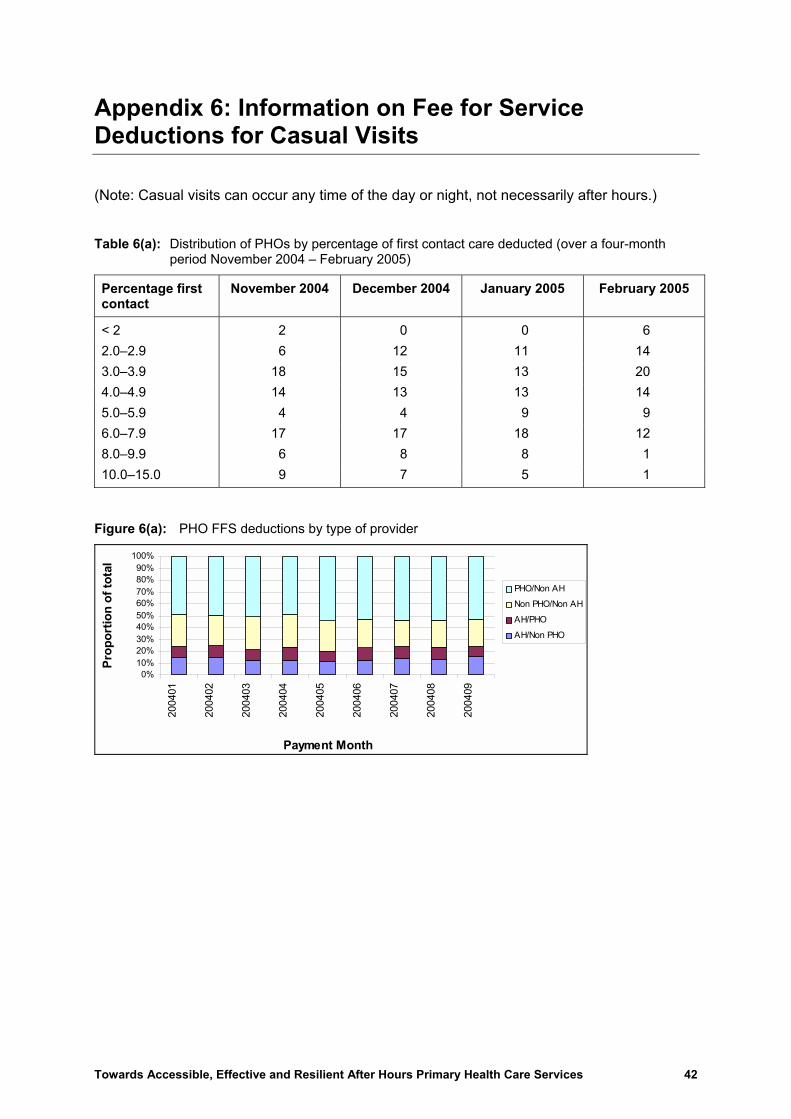
Appendix 6: Information on Fee for Service Deductions for Casual Visits
(Note: Casual visits can occur any time of the day or night, not necessarily after hours.)
Table 6(a): Distribution of PHOs by percentage of first contact care deducted (over a four-month period November 2004 � February 2005)
Percentage first contact
November 2004 December 2004 January 2005 February 2005
< 2 2 0 0 6 2.0�2.9 6 12 11 14 3.0�3.9 18 15 13 20 4.0�4.9 14 13 13 14 5.0�5.9 4 4 9 9 6.0�7.9 17 17 18 12 8.0�9.9 6 8 8 1 10.0�15.0 9 7 5 1
Figure 6(a): PHO FFS deductions by type of provider
0%10%20%30%40%50%60%70%80%90%
100%
2004
01
2004
02
2004
03
2004
04
2004
05
2004
06
2004
07
2004
08
2004
09
Payment Month
Prop
ortio
n of
tota
l
PHO/Non AH
Non PHO/Non AH
AH/PHO
AH/Non PHO
Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 42

Towards Accessible, Effective and Resilient After Hours Primary Health Care Services 43
rovider type and by DHB Figure 6(b): FFS deductions by pFFS Deductions by Provider Type
0%
20%
40%
60%
80%
100%
Auck
land
DH
B
Bay
of P
lent
y D
HB
Cant
erbu
ry D
HB
Cap
ital C
oast
DHB
Coun
ties
Man
ukau
DH
B
Haw
kes
Bay
DH
B
Hut
t DH
B
Lake
s DH
B
Mid
Cen
tral D
HB
Nels
on M
arlb
orou
gh D
HB
Nor
thla
nd D
HB
Ota
go D
HB
Sout
h Ca
nter
bury
DHB
Sout
hlan
d DH
B
Taira
whiti
DHB
Tara
naki
DH
B
Wai
kato
DH
B
Wai
rara
pa D
HB
Wai
tem
ata
DHB
Wes
t Coa
st D
HB
Wha
ngan
ui D
HB
DHB
% o
f FFS
Ded
uctio
ns (J
an04
-Sep
t04)
AH/Non PHOAH/PHONon PHO/Non AHPHO/Non AH
Figure 6(c): Comparison of GMS-funded visits by patient age � Accident and Medical Clinics and other primary providers
30%
23%
47% 18+6�17Under 6
61%14%
25%
18+6�17Under 6