
Touch (discriminative sensation) Proprioception (joint position and movement senses) Pain.
58
Touch (discriminative sensation) Proprioception (joint position and movement senses) Pain
-
Upload
alexander-richard -
Category
Documents
-
view
221 -
download
0
Transcript of Touch (discriminative sensation) Proprioception (joint position and movement senses) Pain.
Touch (discriminativesensation)
Proprioception (joint position andmovement senses)
Pain
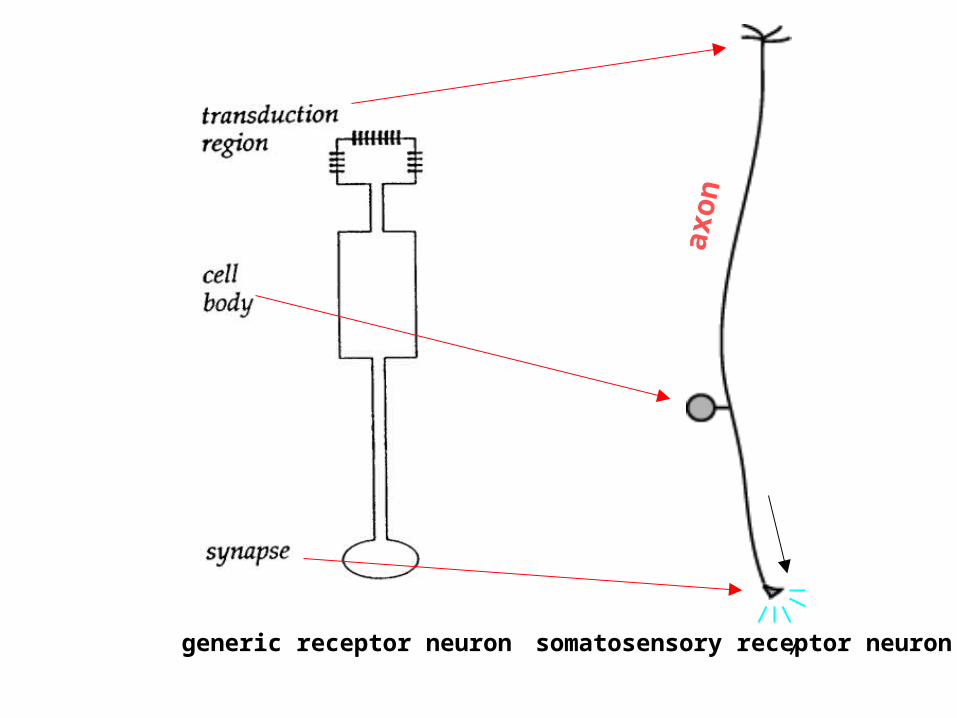
generic receptor neuron somatosensory receptor neuron
axon
Touch
(Axon Ending Types)
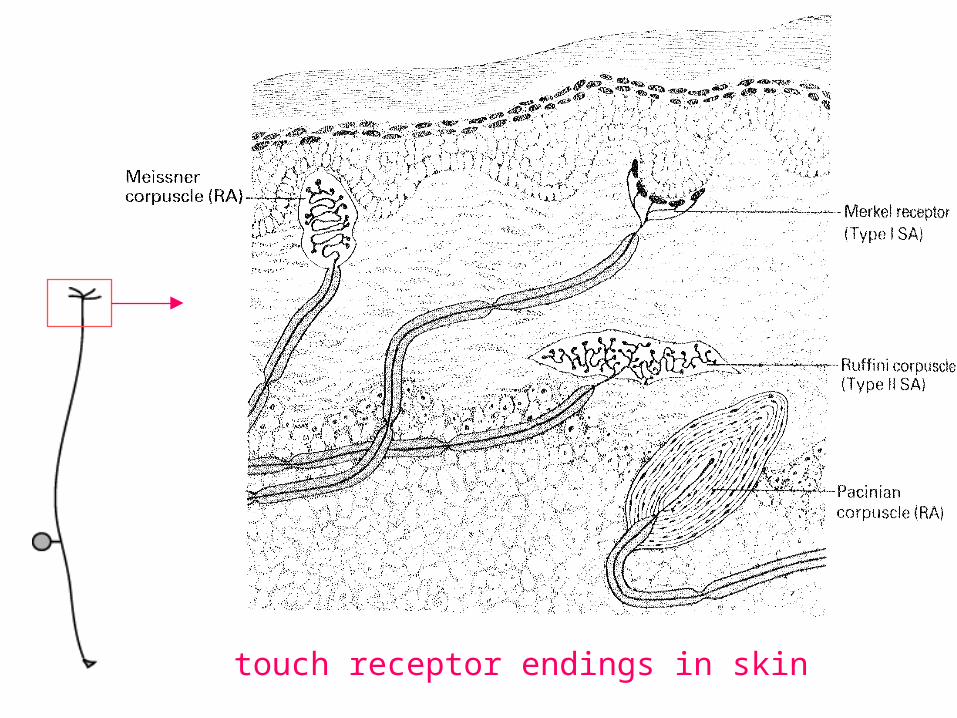
touch receptor endings in skin
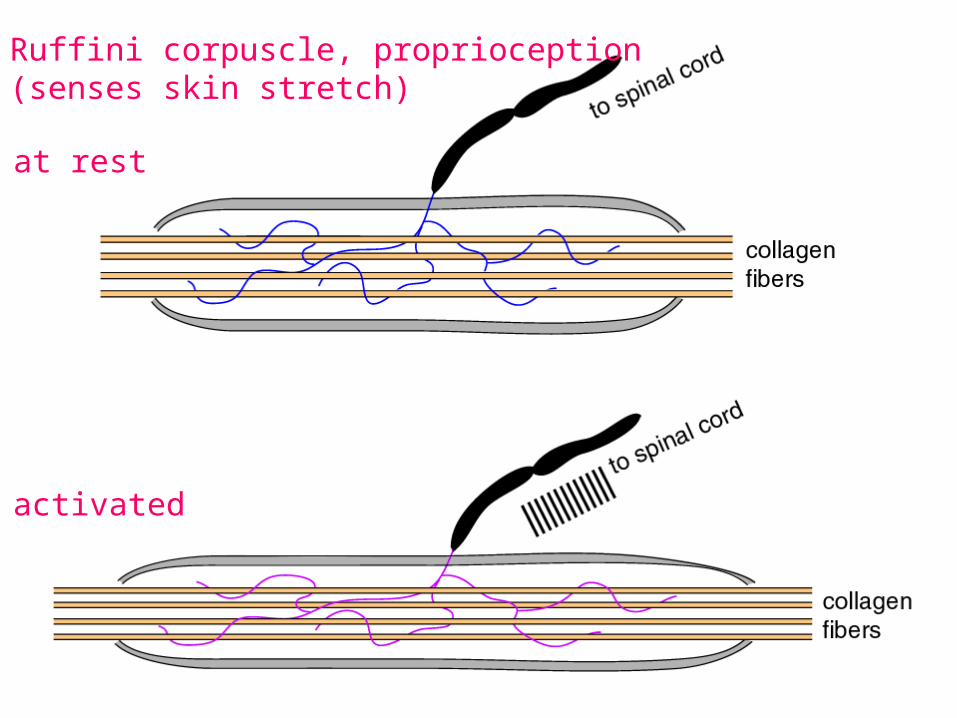
Ruffini corpuscle, proprioception (senses skin stretch)
at rest
activated
Deep touch, vibration Skin stretch sensation
Meissner corpuscle
Merkel disk receptors
Light touch
Touch
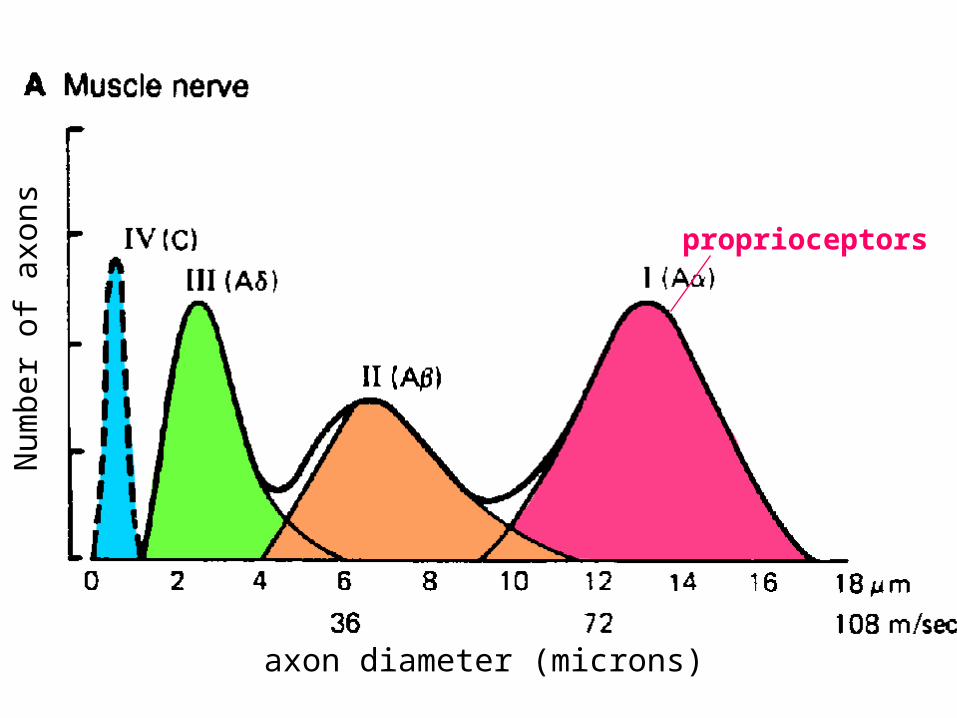
Nerve axon types
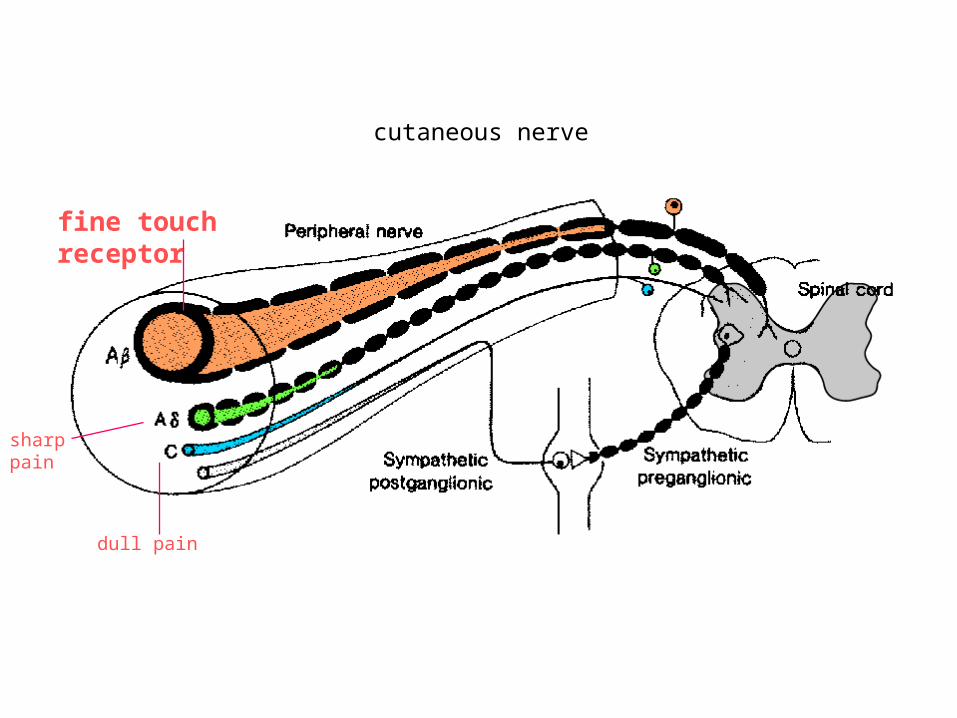
fine touch receptor
cutaneous nerve
dull pain
sharp pain
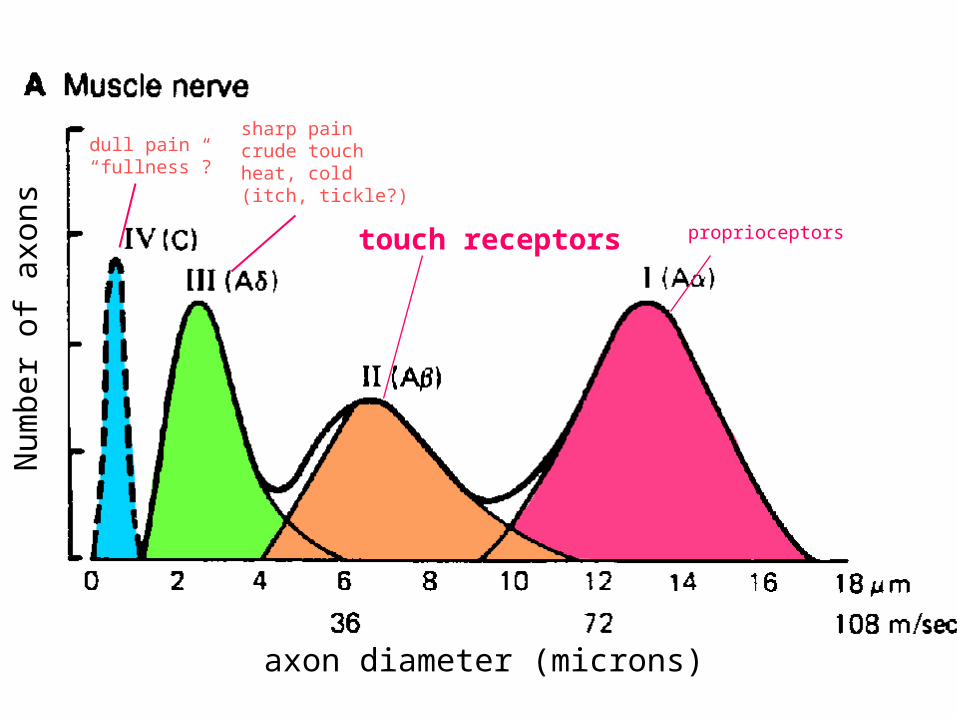
axon diameter (microns)
Num
ber
of a
xons touch receptors proprioceptors
dull pain“fullness”?
sharp paincrude touchheat, cold(itch, tickle?)
Touch
tracts
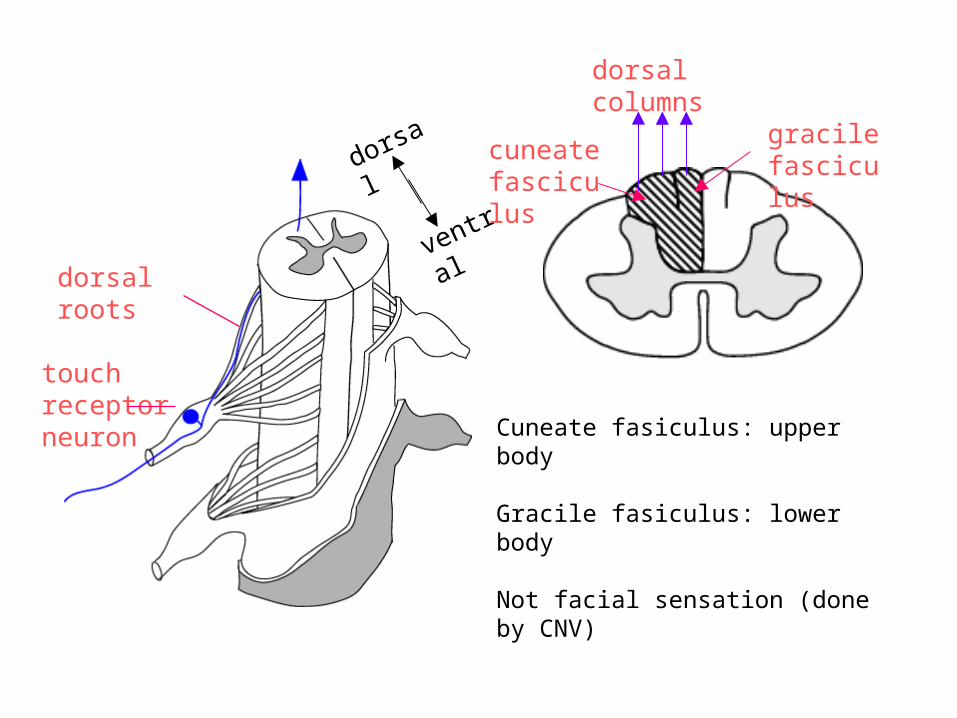
dorsal columns
dorsal
ventral
touch receptor neuron
dorsal roots
cuneate fasciculus
gracile fasciculus
Cuneate fasiculus: upper body
Gracile fasiculus: lower body
Not facial sensation (done by CNV)
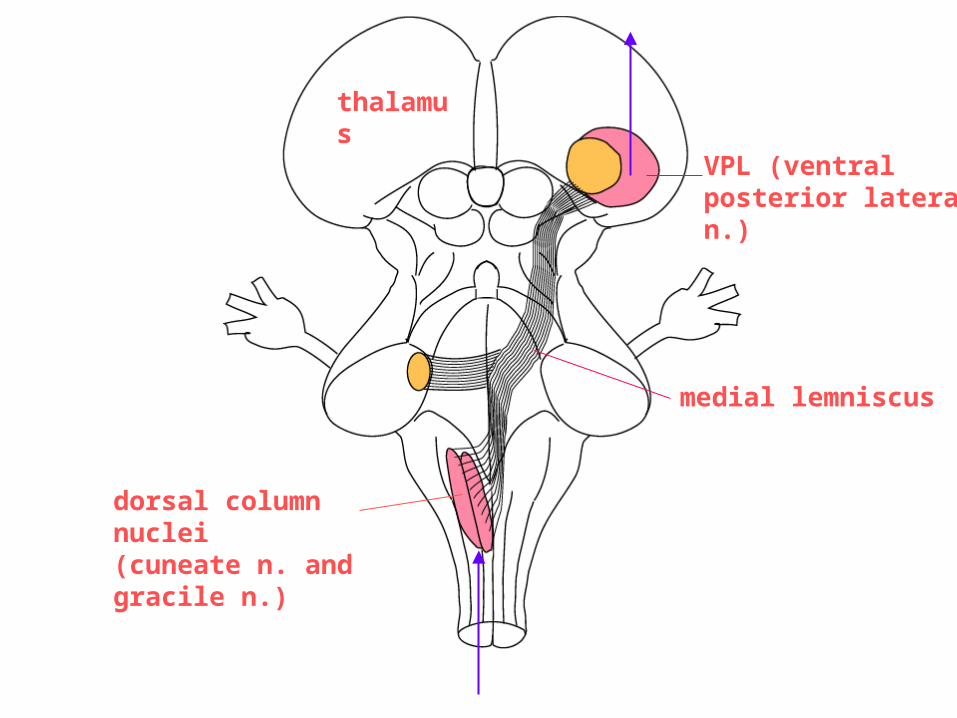
dorsal column nuclei(cuneate n. and gracile n.)
medial lemniscus
VPL (ventral posterior lateral n.)
thalamus
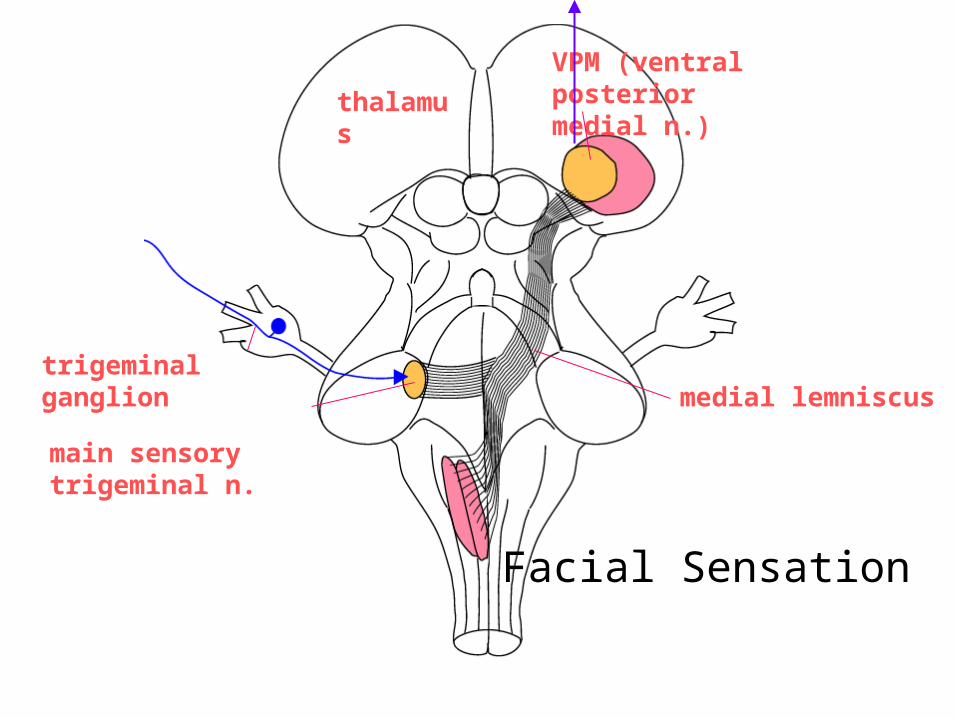
main sensory trigeminal n.
VPM (ventral posterior medial n.)
medial lemniscus
thalamus
trigeminal ganglion
Facial Sensation
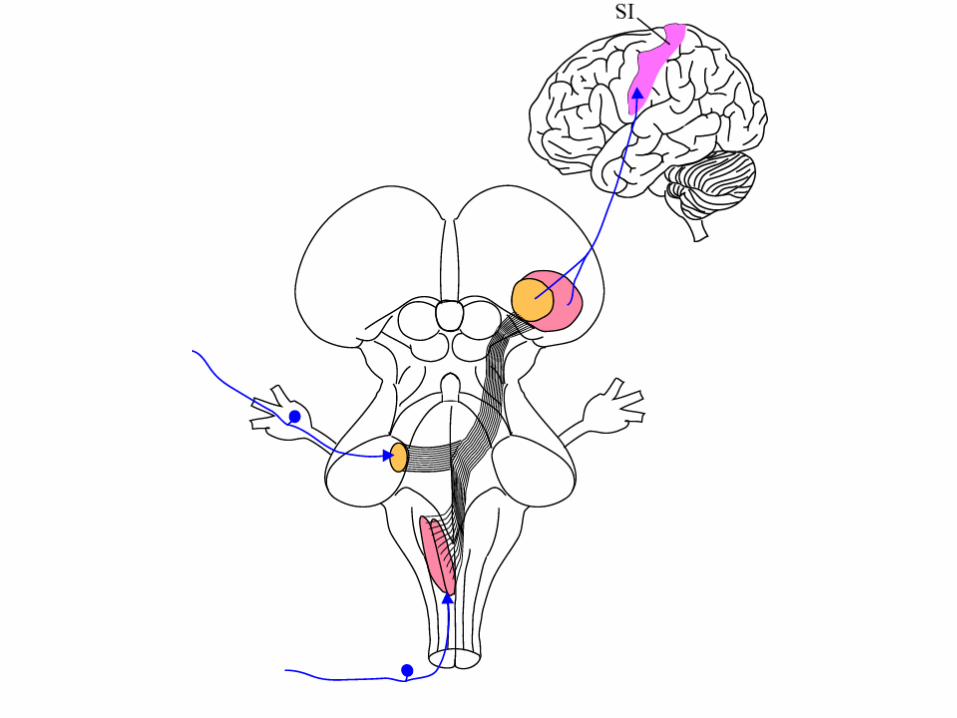
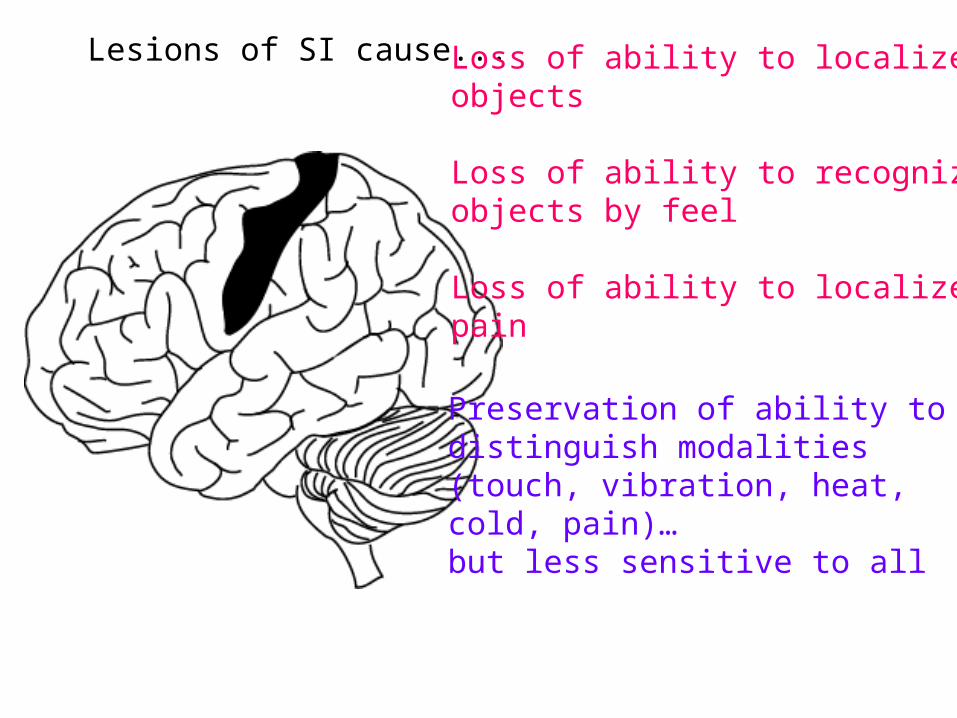
Lesions of SI cause... Loss of ability to localizeobjects
Loss of ability to recognizeobjects by feel
Loss of ability to localizepain
Preservation of ability to distinguish modalities (touch, vibration, heat,cold, pain)…but less sensitive to all
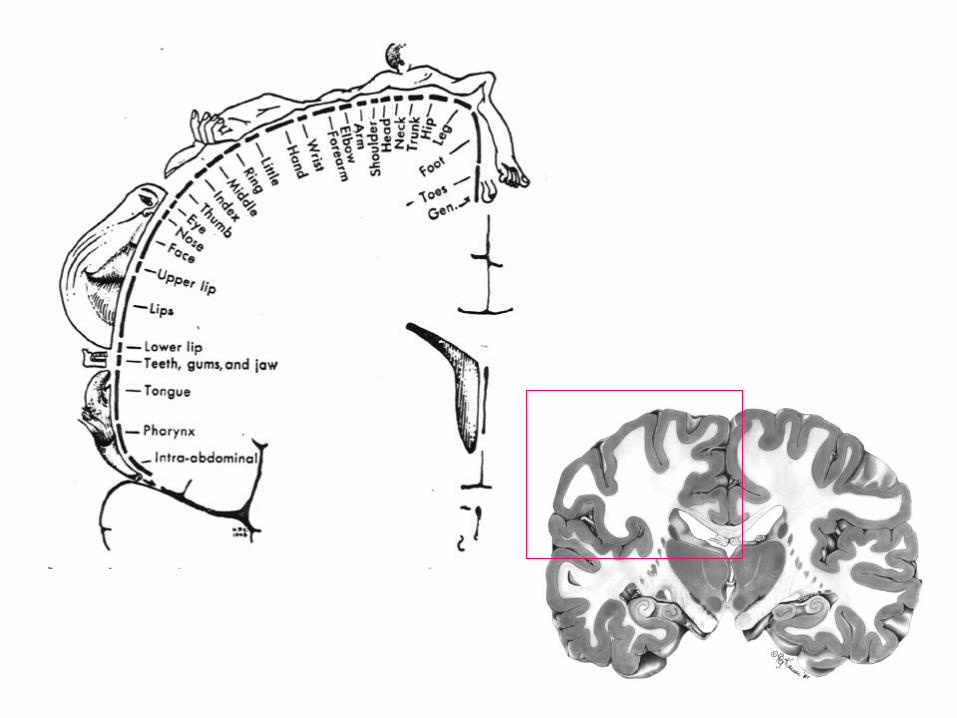
The map in somatosensory cortex is plastic
Lesions of PNS vs CNS
• Lesion of PNS axon = regeneration and regrowth
• Lesion of CNS axon = complete cell death
Proprioception
axon diameter (microns)
Num
ber
of a
xons proprioceptors
Golgi tendon
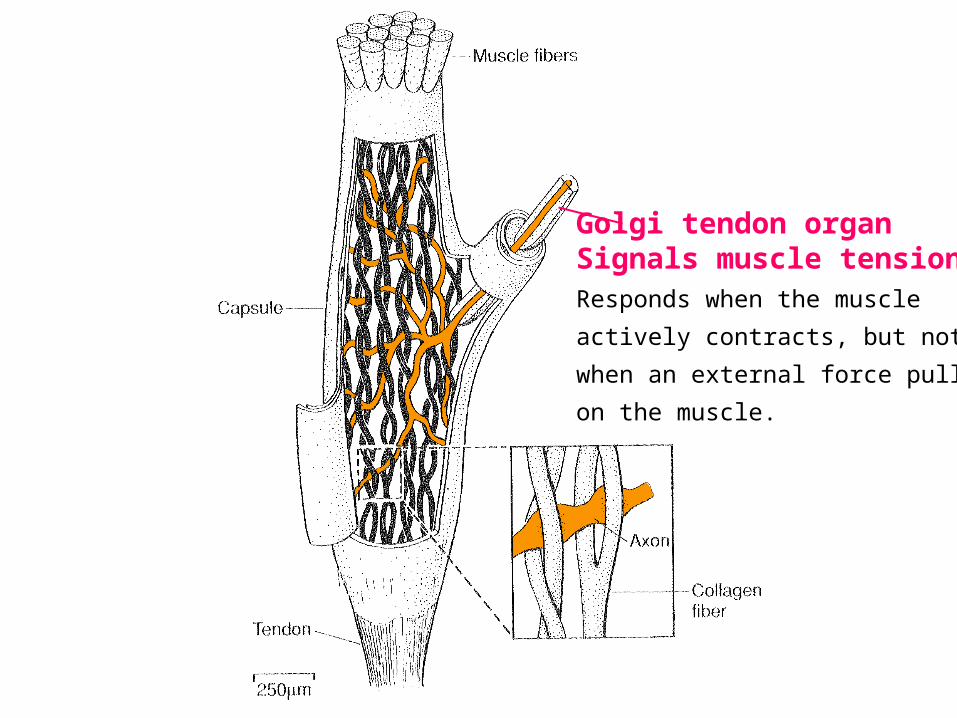
Golgi tendon organSignals muscle tensionResponds when the muscle
actively contracts, but not
when an external force pulls
on the muscle.
Spindle afferents: sense muscle length
… it reports the difference between desired and actual length
Active relaxation of muscle: no intrafusal lengthening. No spindle afferent response
Passive stretch: intrafusal muscle fiber lengthens. Spindle fires a response
Proprioceptive information follows 3 pathways...
Local (in spinal cord)
(results in the stretch reflex)
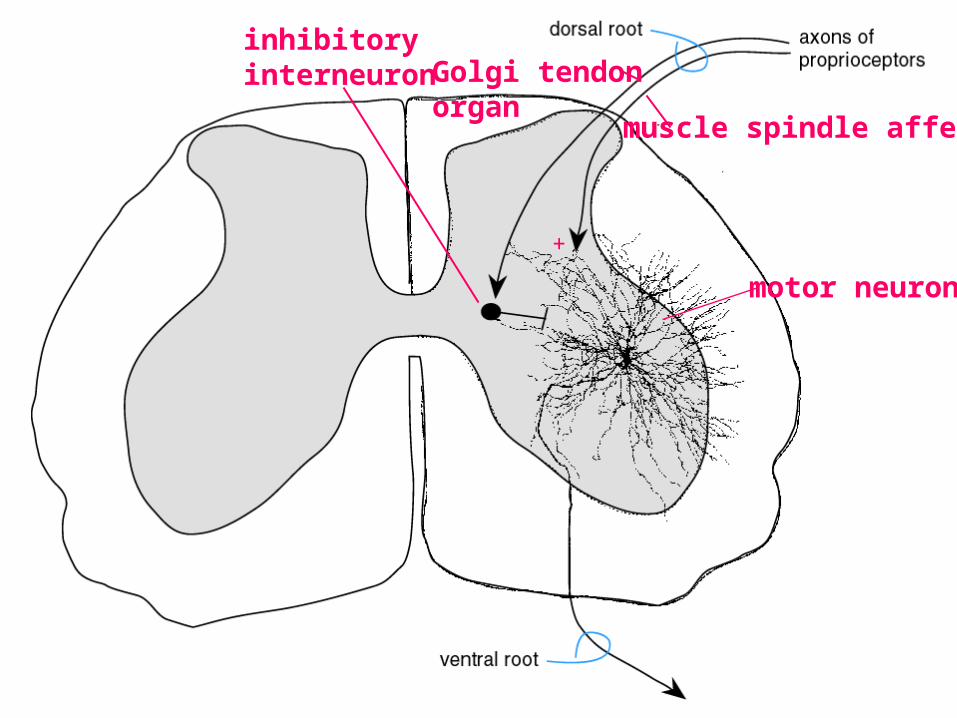
motor neuron
inhibitoryinterneuron
muscle spindle afferent
Golgi tendonorgan
+
Proprioceptive information follows 3 pathways...
To cerebellum
(Keeps the cerebellum informed about the actual movements and allows it to coordinate, smooth and refine movements)
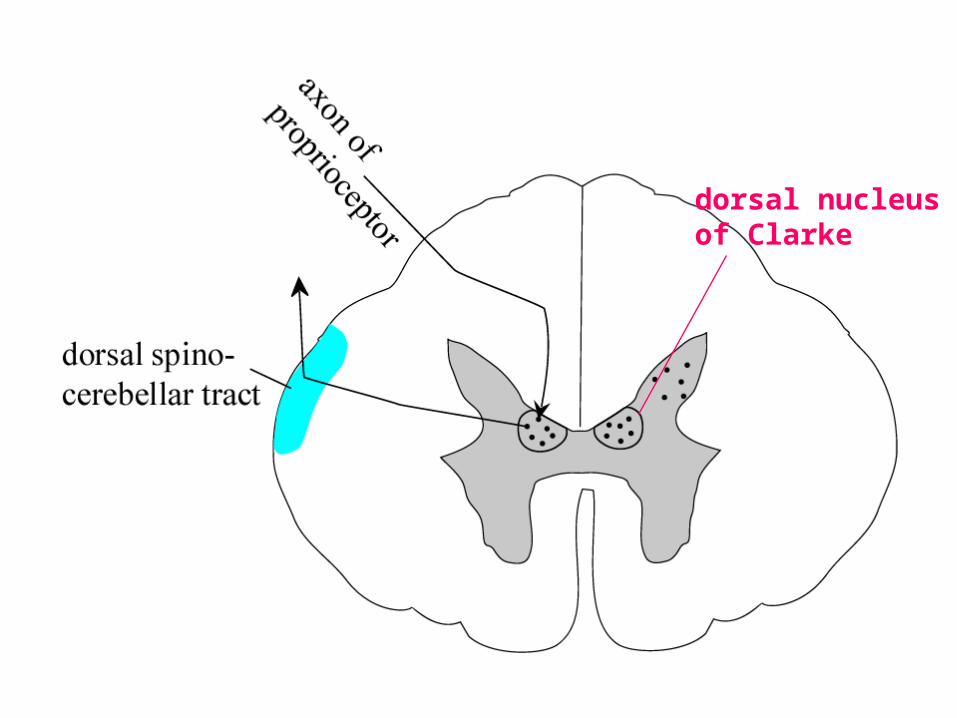
dorsal nucleusof Clarke
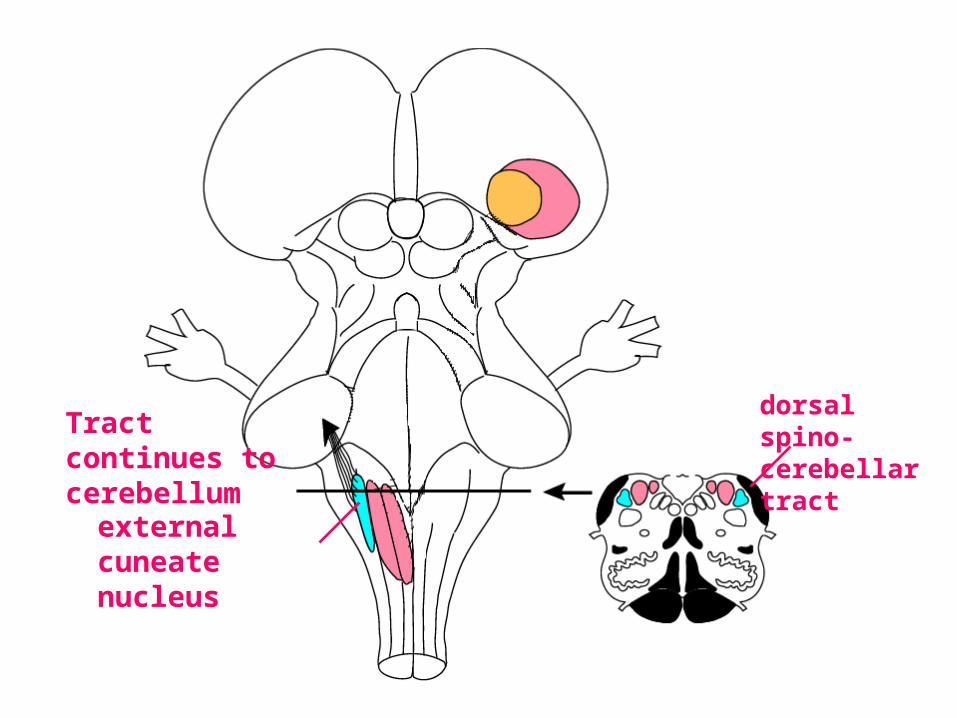
external cuneate nucleus
dorsal spino-cerebellar tractTract continues to
cerebellum
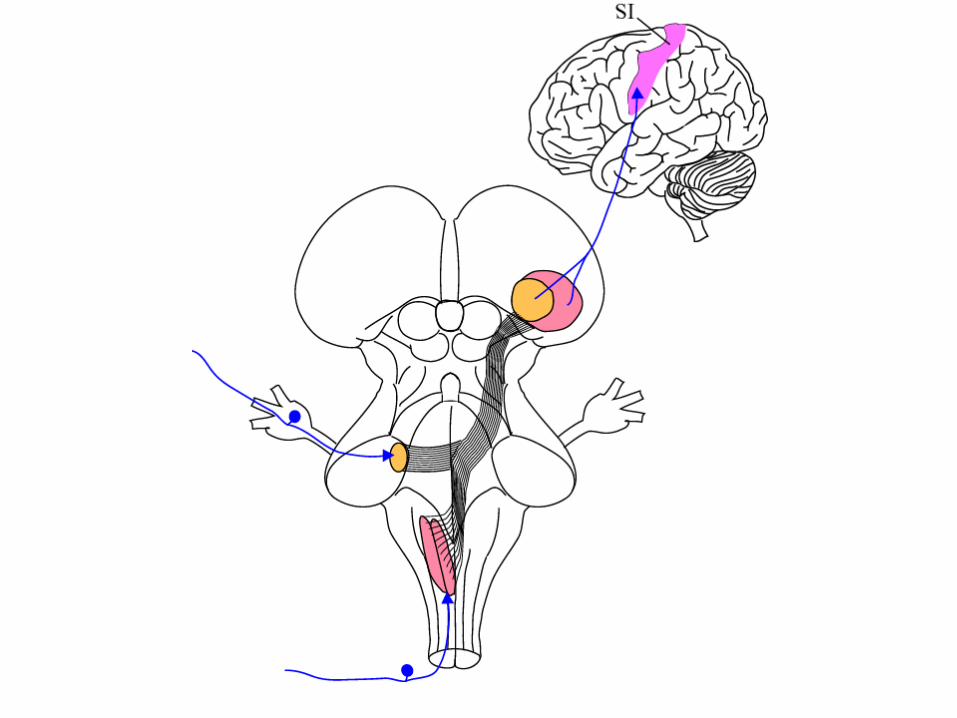
Proprioceptive information follows 3 pathways...
To cerebral cortex
(We can consciously perceive proprioception.)
Pain
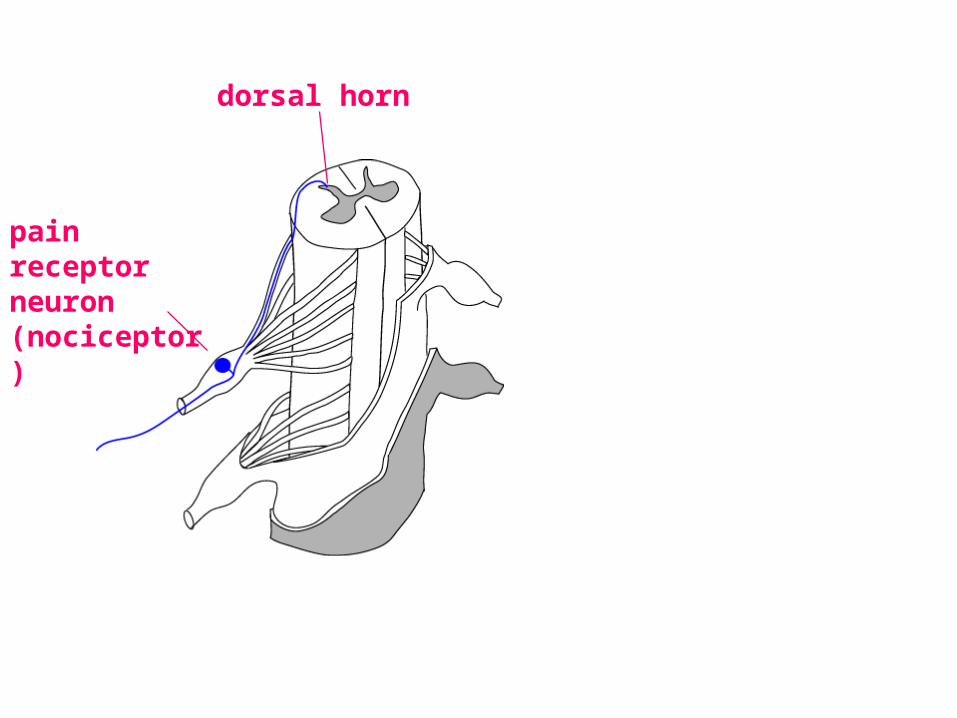
pain receptor neuron(nociceptor)
dorsal horn
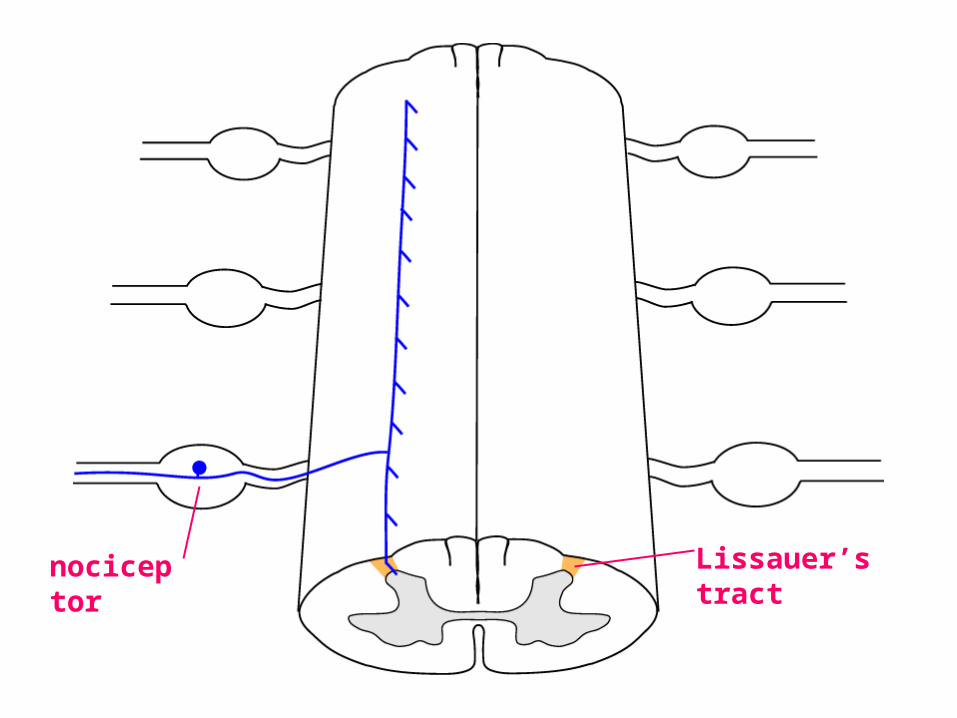
nociceptor Lissauer’s tract
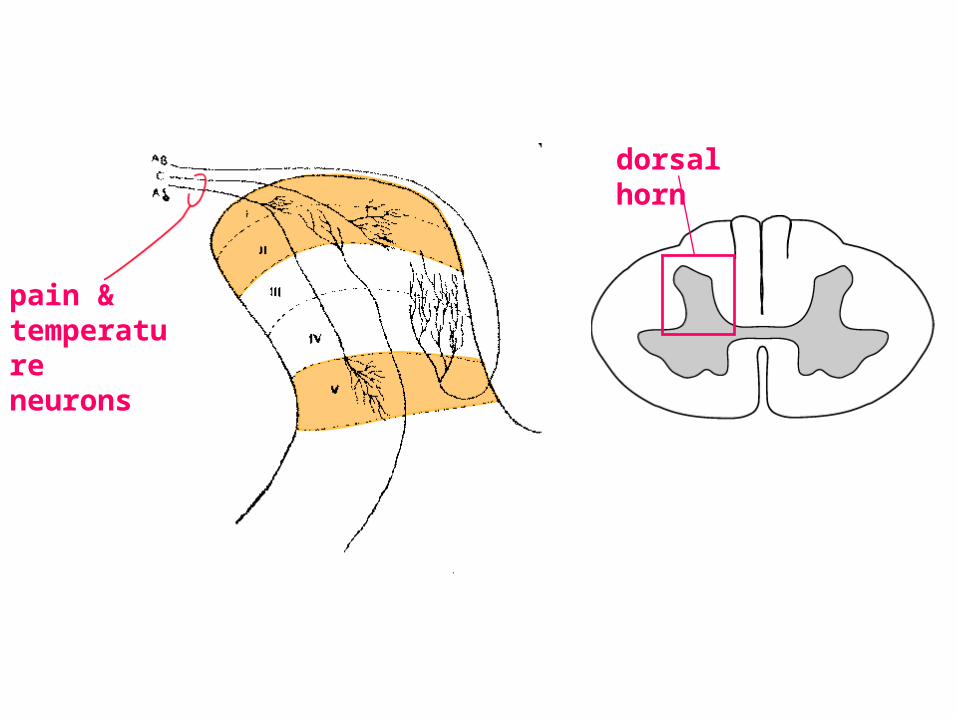
pain & temperature neurons
dorsal horn
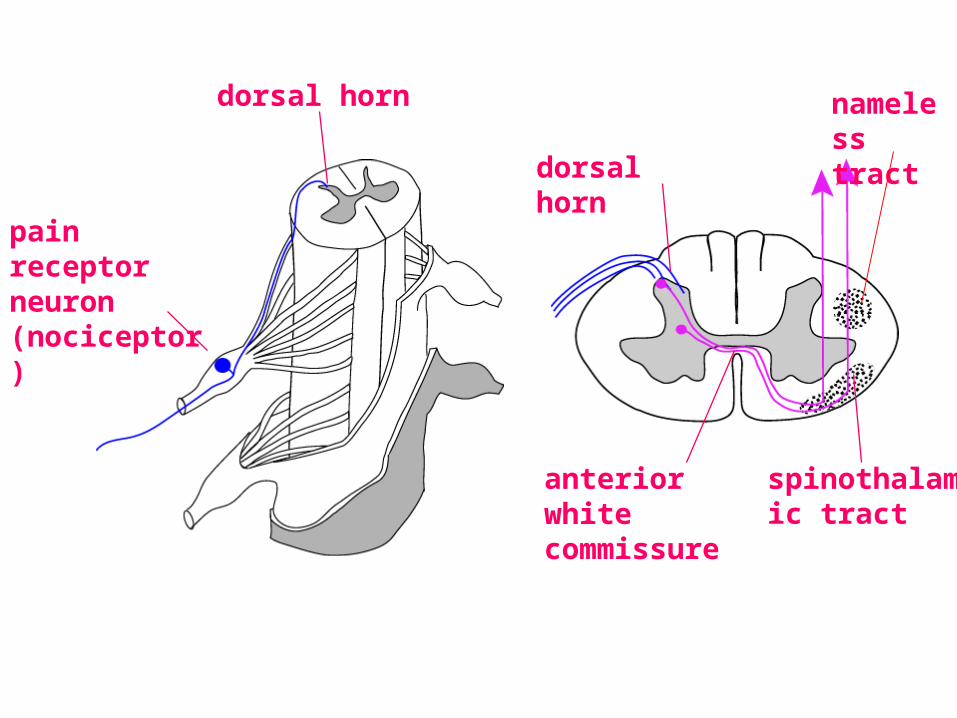
pain receptor neuron(nociceptor)
dorsal horn
dorsal horn
anterior white commissure
spinothalamic tract
nameless tract
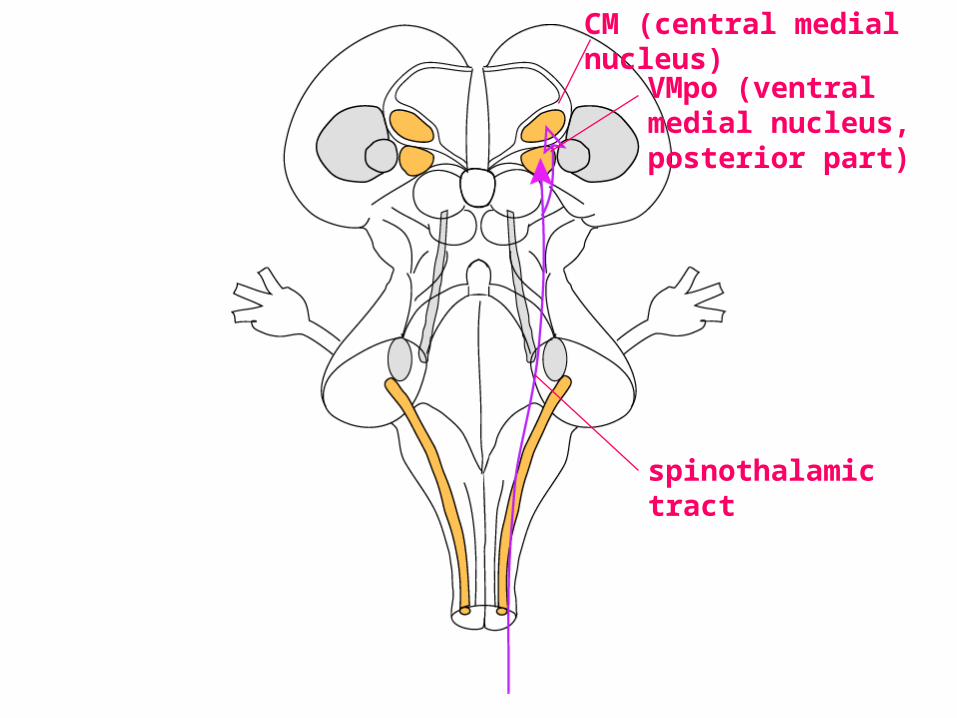
spinothalamic tract
VMpo (ventral medial nucleus, posterior part)
CM (central medial nucleus)
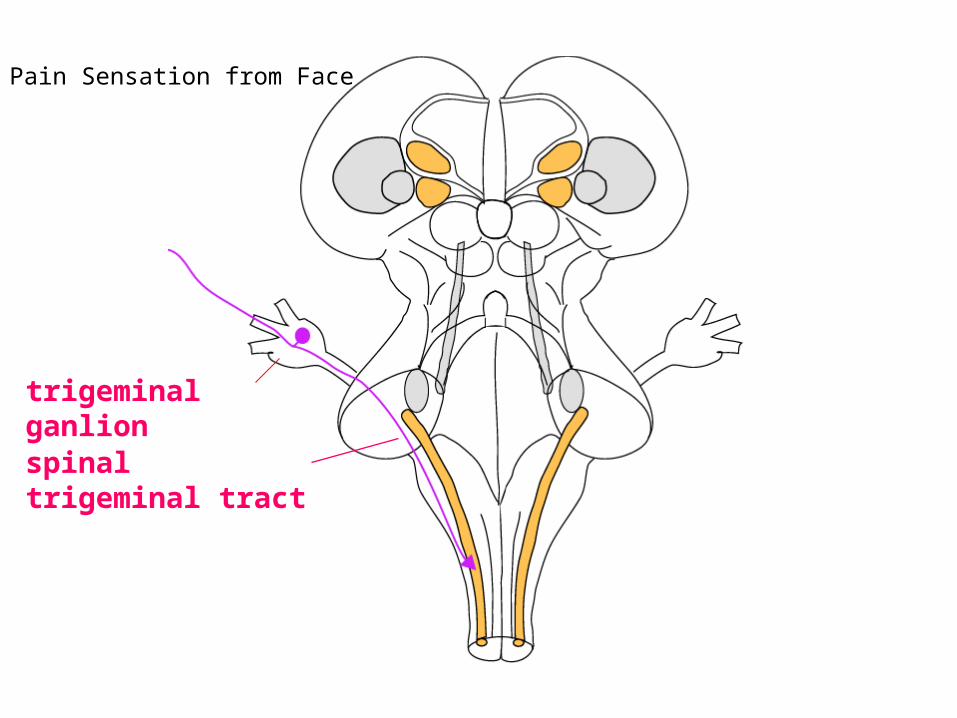
spinal trigeminal tract
trigeminal ganlion
Pain Sensation from Face
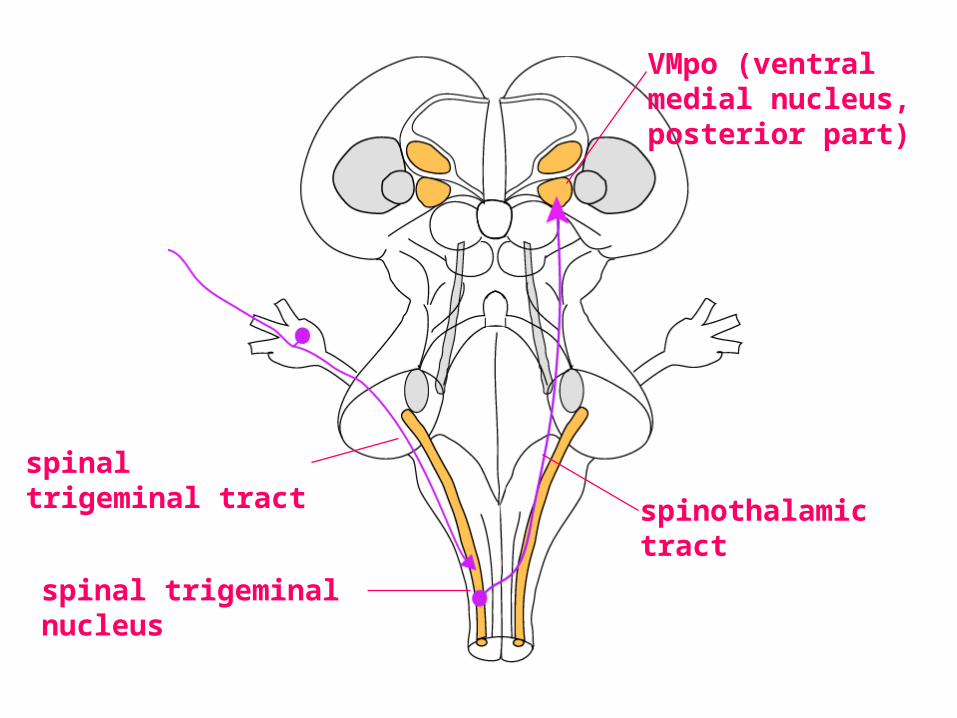
spinothalamic tract
VMpo (ventral medial nucleus, posterior part)
spinal trigeminal tract
spinal trigeminal nucleus
Receptor types in pain-temperature pathway:
sharp pain
dull pain (aching, burning)
heat
cold
crude touch
“fullness” (bladder, stomach, etc.)
itchtickle
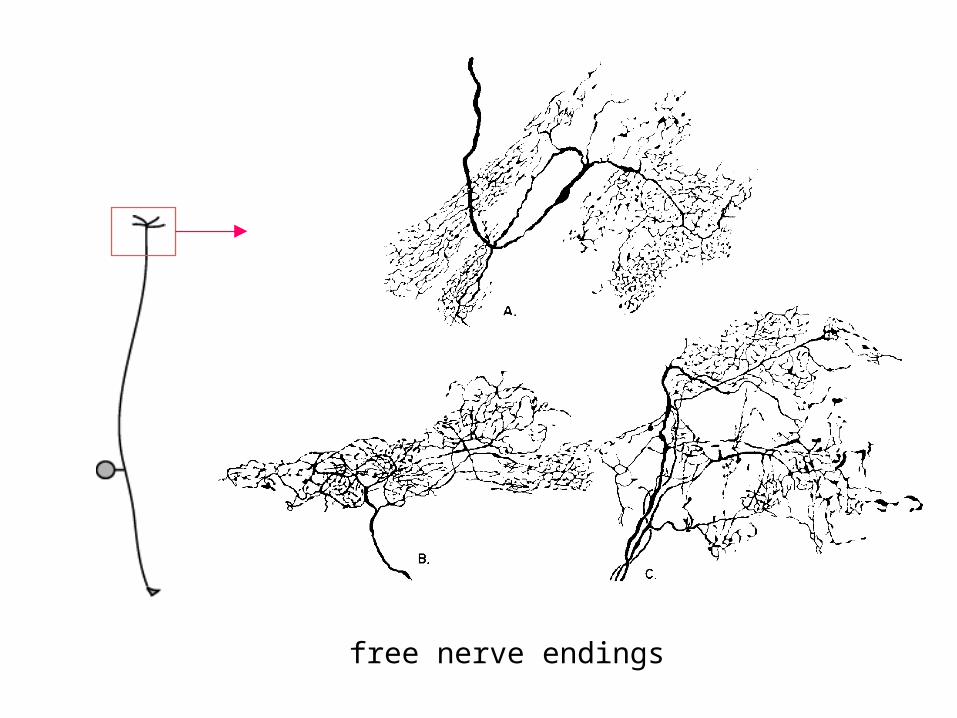
free nerve endings
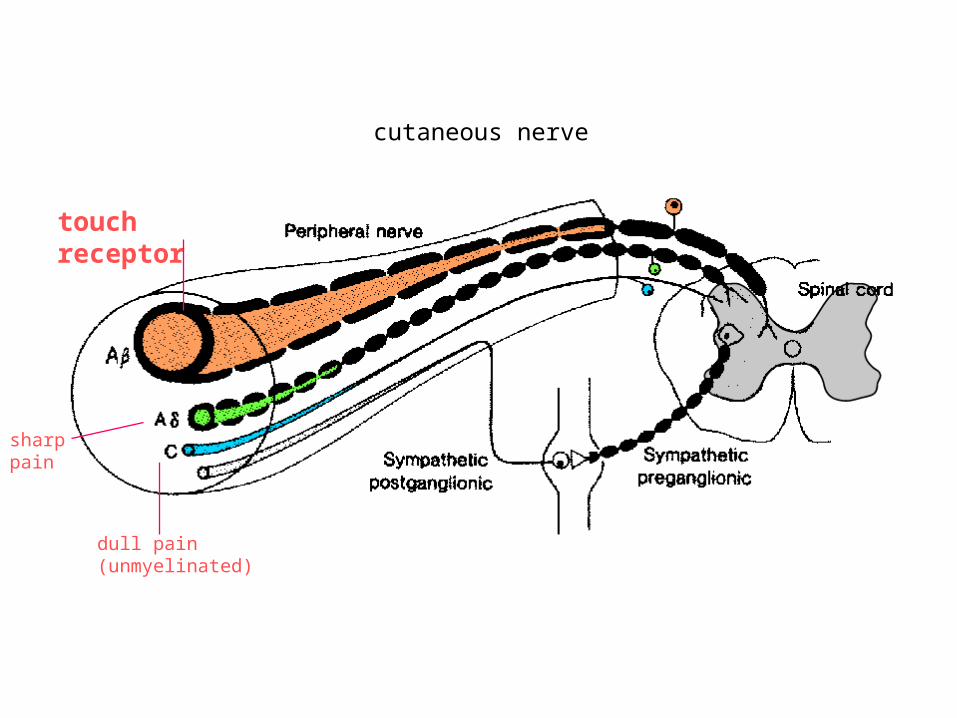
touch receptor
cutaneous nerve
dull pain (unmyelinated)
sharp pain
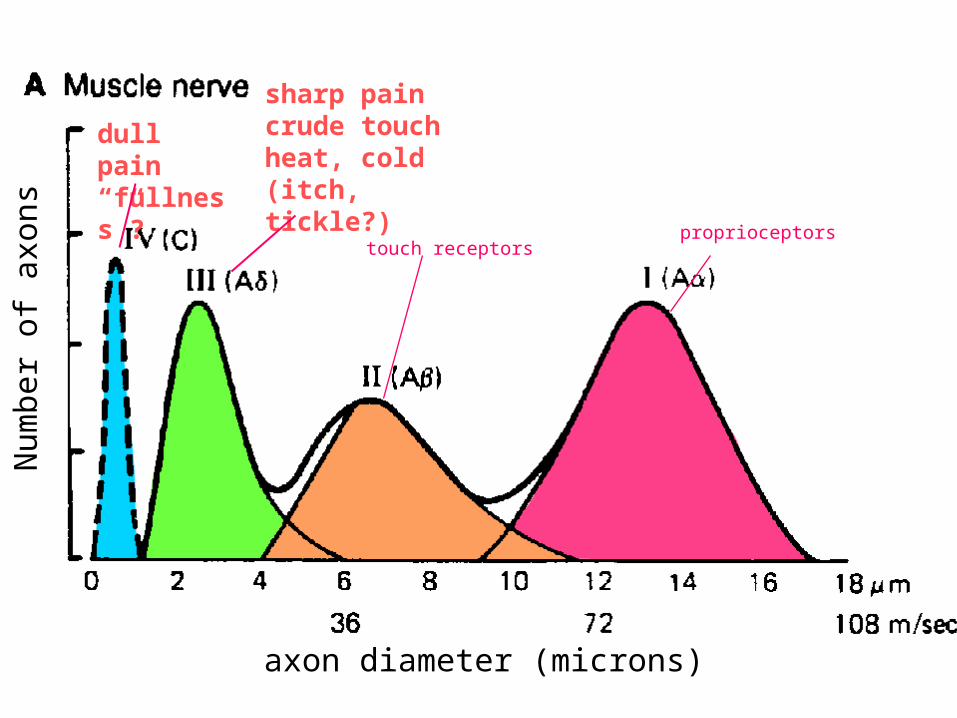
axon diameter (microns)
Num
ber
of a
xons touch receptors
proprioceptors
dull pain“fullness”?
sharp paincrude touchheat, cold(itch, tickle?)
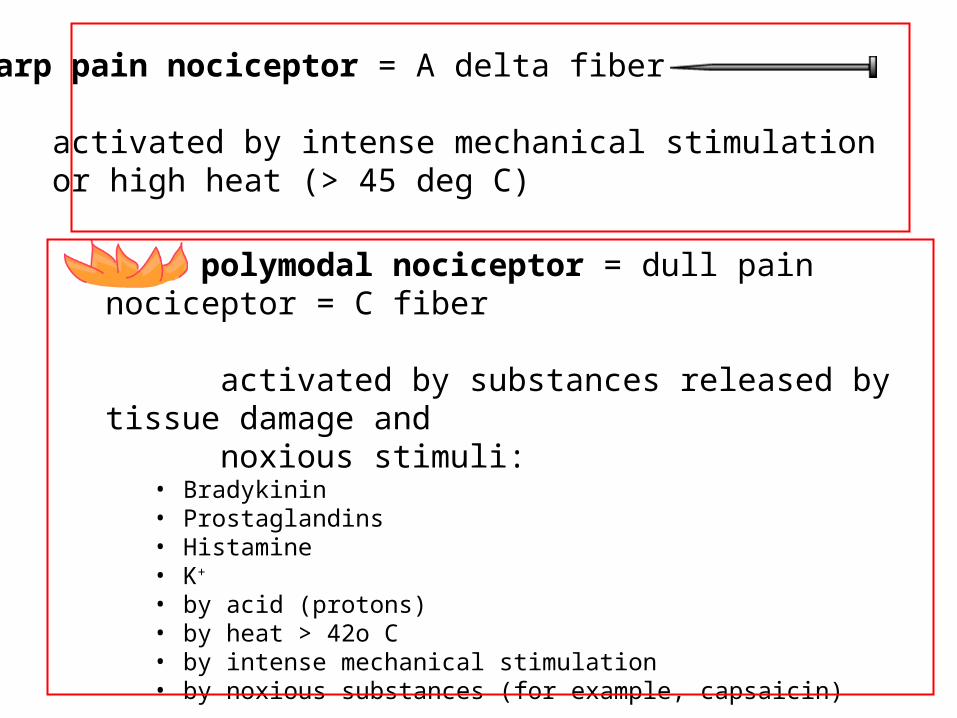
sharp pain nociceptor = A delta fiber
activated by intense mechanical stimulationor high heat (> 45 deg C)
polymodal nociceptor = dull pain nociceptor = C fiber
activated by substances released by tissue damage and noxious stimuli:
• Bradykinin• Prostaglandins• Histamine• K+
• by acid (protons)• by heat > 42o C• by intense mechanical stimulation• by noxious substances (for example, capsaicin)
INNERVATES ALL TISSUE EXCEPT THE BRAIN AND LENS OF EYE
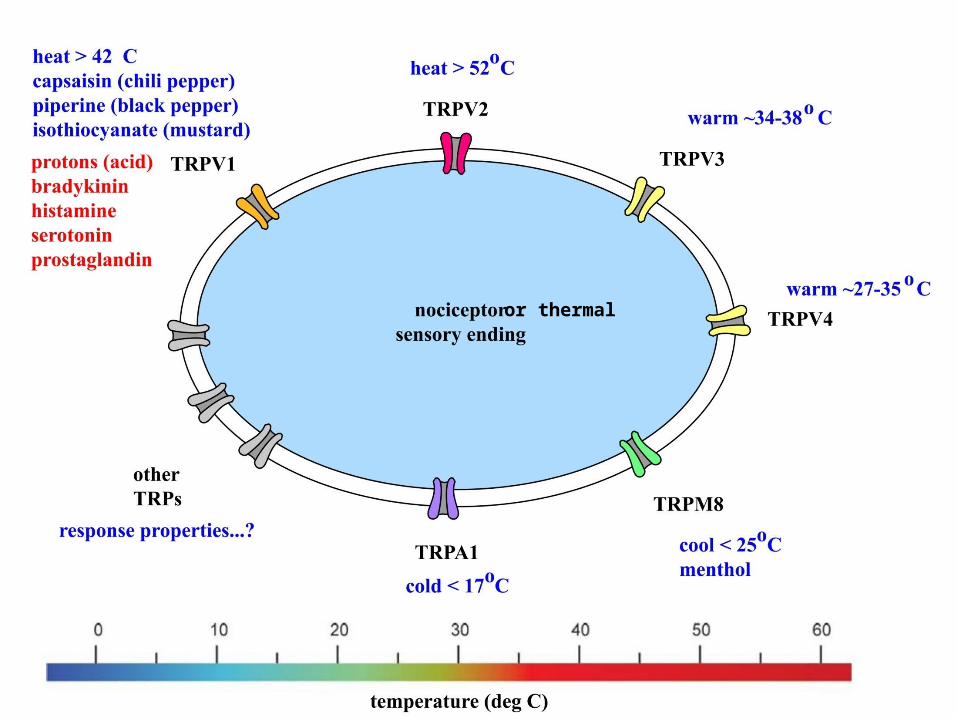
or thermal
• Hyperalgesia: intense pain in response to mildly painful stimulus (pinprick)
• Allodynia: pain in response to completely innocuous stimulus (touch)
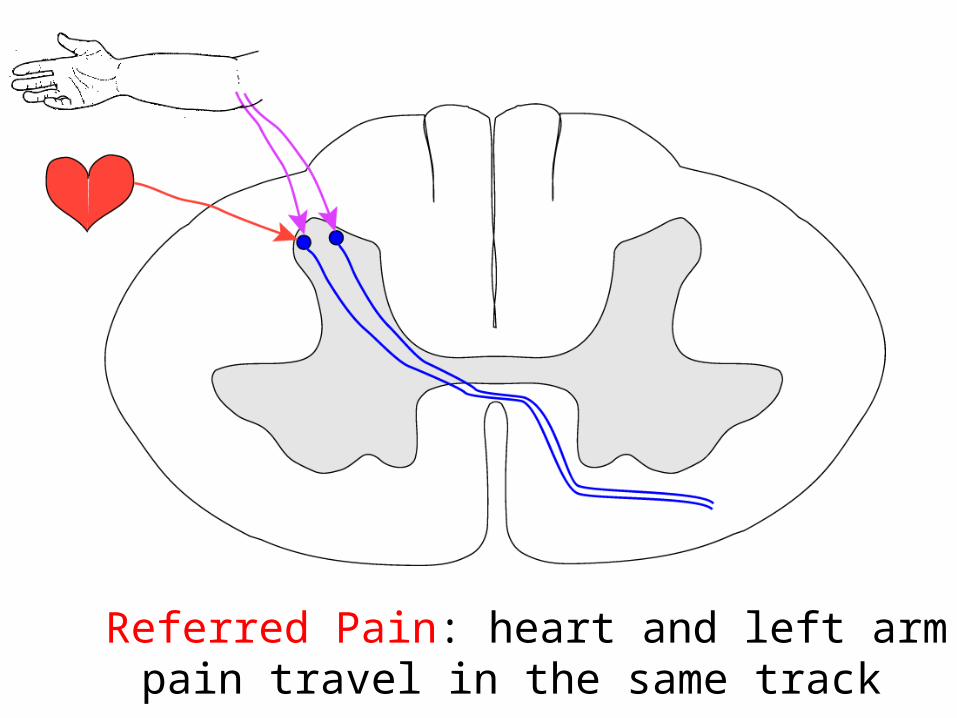
Referred Pain: heart and left arm pain travel in the same track
Descending pain modulation
Neurons of the descending pain modulation system are activated by opium and its derivatives (morphine, etc.)
Endogenous opioid transmitters
• endorphins• enkephalins• dynorphins
• What activates descending pain modulation system?
• STRESS!
• fear
• hunger
• thirst
• fatigue
• prolonged motor activity
• hypnosis
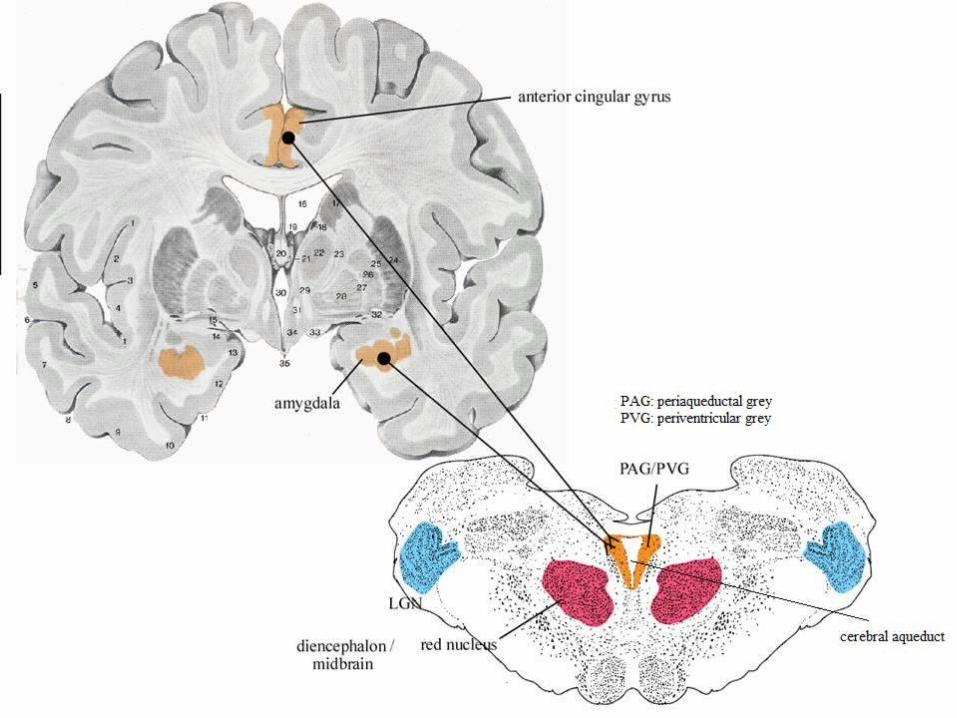
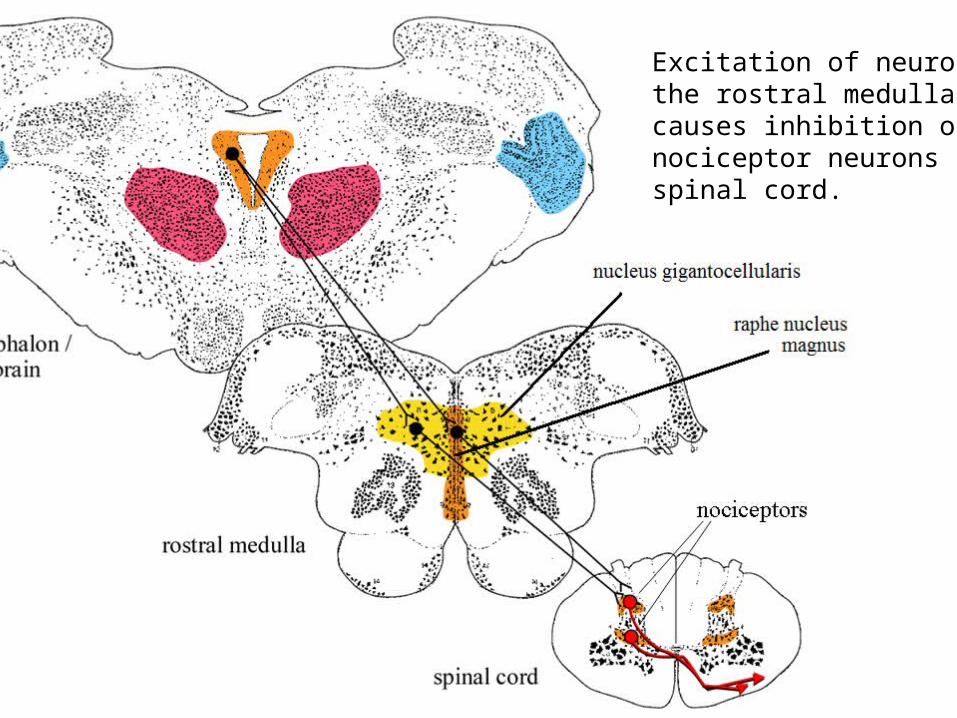
Excitation of neurons in the rostral medulla causes inhibition of nociceptor neurons in the spinal cord.
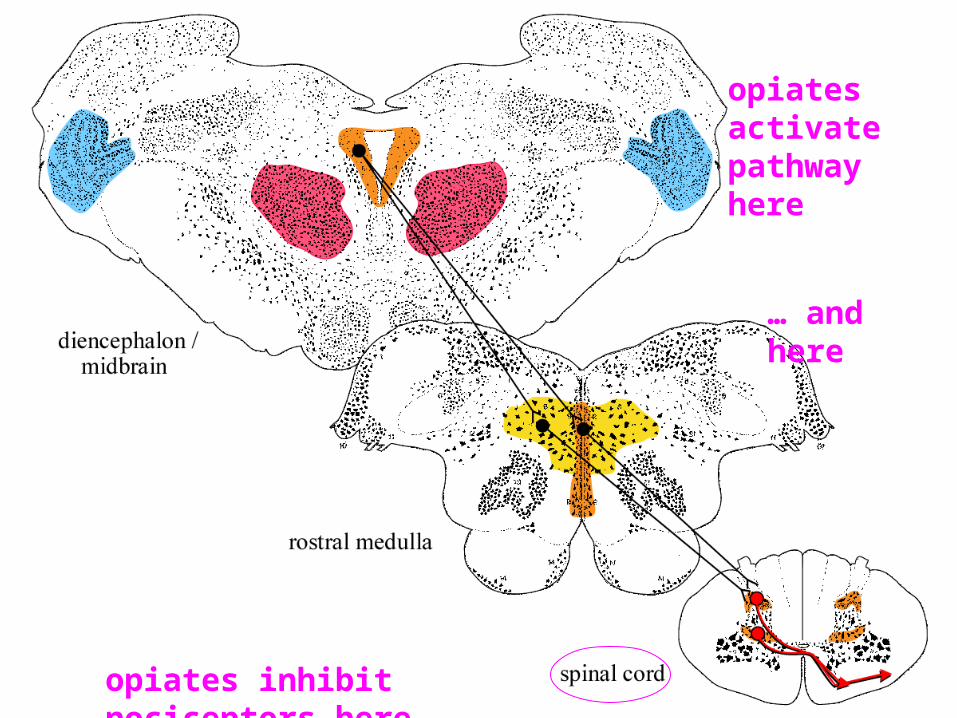
opiates activate pathway here
… and here
opiates inhibit nociceptors here
Neuropathic pain syndromes:
tic douloureux (trigeminal neuralgia)
Chronic facial pain from vessels pinching on the trigeminal nerve. The C fibers are the smallest and easiest to stimulate to fire an AP.
Treatment: Surgery to reroute the offending vessel
Neuropathic pain syndromes:
tabes dorsalis
• The largest axons in the dorsal root ganglia (a beta and proprioceptors) are systematically destroyed.
• The dorsal columns degenerate. • Patient looses discriminative touch and
proprioception. • Locomotion becomes awkward and stumbling.• Also suffers from “lightening-like” stabbing pain
Neuropathic pain syndromes:
thalamic pain
• Spontaneous burning or crushing pain on one side of the body
• May be from lesion in VMpo or MD???• Narcotic meds not effective• electrical stimulation of precentral gyrus can
improve symptoms
Neuropathic pain syndromes:
phantom limb pain
• Narcotics not very effective• From reorganization of the somatoscopic
maps?


















